Back to Journals » Journal of Pain Research » Volume 19
Monocyte Transmigration Involves in Remifentanil Induced Mechanical Hyperalgesia in Animal Models and a Randomized Controlled Clinical Trial
Authors Zhang R, Ye Z, Chen Q, Zhu Y ![]() , Wang Y, He H
, Wang Y, He H ![]() , Li J
, Li J ![]() , Hu Y, Gan X
, Hu Y, Gan X ![]()
Received 9 June 2025
Accepted for publication 23 March 2026
Published 8 April 2026 Volume 2026:19 545720
DOI https://doi.org/10.2147/JPR.S545720
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Rui Zhang,1,* Zexi Ye,1,* Qianru Chen,1,* Yanling Zhu,1 Yongyi Wang,1 Honglian He,1 Jinfei Li,1 Youjin Hu,2 Xiaoliang Gan1
1Department of Anesthesiology, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat−sen University, Guangdong Provincial Key Laboratory of Ophthalmology Visual Science, Guangdong Provincial Clinical Research Center for Ocular Diseases, Guangzhou, 510060, People’s Republic of China; 2State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat−sen University, Guangdong Provincial Key Laboratory of Ophthalmology Visual Science, Guangdong Provincial Clinical Research Center for Ocular Diseases, Guangzhou, 510060, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoliang Gan, Department of Anesthesiology, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat−sen University, Guangdong Provincial Key Laboratory of Ophthalmology Visual Science, Guangdong Provincial Clinical Research Center for Ocular Diseases, 7 Jinsui Road, Guangzhou, 510060, People’s Republic of China, Email [email protected] Youjin Hu, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat−sen University, Guangdong Provincial Key Laboratory of Ophthalmology Visual Science, Guangdong Provincial Clinical Research Center for Ocular Diseases, Guangzhou, 510060, People’s Republic of China, Email [email protected]
Abstract: Remifentanil−induced hyperalgesia (RIH) complicates postoperative pain management under total intravenous anesthesia. Although monocyte transmigration contributes to neuropathic pain, its role in RIH remains undefined. Here, we investigated monocyte dynamics in RIH through preclinical and clinical studies. In male mice, intraperitoneal remifentanil infusion (4 μg/kg/min, 1 h) induced sustained mechanical hyperalgesia (reduced paw withdrawal thresholds, PWTs) over 48 hours, paralleled by a transient decline in circulating monocytes (3 h post−infusion) and increased macrophage infiltration in paw tissues. Critically, monocyte depletion significantly attenuated RIH, implicating monocytes in its pathogenesis. Translating these findings, a randomized trial of 44 patients undergoing minor surgery under sevoflurane−remifentanil anesthesia (0.3 μg/kg/min) revealed that perioperative flurbiprofen axetil (1 mg/kg) attenuated remifentanil−induced mechanical hyperalgesia (peri−incisional and upper limb regions) at 2 h and 24 h postoperatively (p < 0.05). Mechanistically, flurbiprofen axetil prevented remifentanil−driven reductions in circulating monocytes and suppressed plasma CCL3/G−CSF elevations (p < 0.05), despite unchanged monocytic COX− 2 expression. In vitro, remifentanil (1000 ng/mL) directly promoted peripheral blood mononuclear cell migration (p < 0.05) without affecting viability. Collectively, monocyte transmigration underlies RIH in both animal models and humans, while flurbiprofen axetil counteracts hyperalgesia by retaining monocytes in circulation and modulating chemokine signaling. These translational insights highlight monocyte−targeted strategies as a therapeutic avenue for RIH. In this study, we demonstrated that extravascular migration of circulating monocytes is involved in remifentanil-induced hyperalgesia. Flurbiprofen axetil attenuates remifentanil-induced hyperalgesia, possibly by suppressing monocyte extravasation.
Keywords: hyperalgesia, monocytes, non−steroidal anti−inflammatory drugs, remifentanil
Introduction
Opioids have long been used for the management of perioperative acute pain. Indeed, Remifentanil, one of the most widely used opioids in total intravenous anesthesia (TIVA), is particularly well suited for ambulatory surgery owing to its potent analgesic effect, short context-sensitive half-life, and minimal accumulation during prolonged infusion.1 However, many studies have reported that high-dose remifentanil reduces mechanical pain thresholds and increases postoperative opioid consumption, a phenomenon known as remifentanil-induced hyperalgesia (RIH).2,3 It should be noted that remifentanil-induced hyperalgesia does not appear to be confined to supraclinical or excessively high doses of remifentanil. Evidence from multiple randomized controlled trials and systematic reviews indicates that continuous infusion of remifentanil at clinically routine anesthetic doses may still be associated with postoperative hyperalgesia, higher pain scores, and increased postoperative opioid consumption.4–6 Such alterations in pain sensitivity may exacerbate acute postoperative pain, increase analgesic requirements, and ultimately prolong recovery while imposing an additional burden on healthcare resources.6,7 Consequently, elucidating the underlying mechanisms of RIH and identifying effective preventive or therapeutic strategies remain issues of clear and immediate clinical relevance.
Opioids may influence immune function via the neuroendocrine system. For instance, increased migration of regulatory T (Treg) cells into the brain has been reported in individuals with opioid addiction, potentially mediated by opioid-induced chemokine release from neurons.5 Meanwhile, monocyte transmigration into perivascular tissues has been shown to be closely associated with neuropathic pain.6 These findings suggest that monocyte migration may play an important role in the development of opioid-induced hyperalgesia, such as remifentanil-induced hyperalgesia. However, current evidence regarding immune-mediated mechanisms of opioid-related pain is derived predominantly from neuropathic pain models or studies involving prolonged opioid exposure. Whether short-term perioperative infusion of remifentanil elicits comparable immunological processes remains uncertain. Moreover, existing clinical investigations of remifentanil-induced hyperalgesia have largely focused on analgesic outcomes, whereas the potential contribution of immune cell migration to RIH has received limited attention. Accordingly, further studies integrating experimental models with clinical data are warranted to clarify the role of monocyte migration in perioperative RIH.
Previous clinical studies have demonstrated that preoperative administration of flurbiprofen axetil is more effective than its postoperative administration in preventing the exacerbation of RIH; however, the underlying mechanism remains unclear.8 Several lines of evidence have demonstrated that remifentanil upregulates cyclooxygenase-2 (COX−2) expression in spinal cord, and increased COX-2 levels are associated with the severity of hyperalgesia.7 Flurbiprofen axetil is a nonselective COX inhibitor that reduces pain primarily by inhibiting the synthesis of prostaglandin E2 (PGE2) in the spinal cord.9 Previous studies have also demonstrated the chemotaxis effects of PGE2 on macrophage migration.10 Given the absence of clinically available agents that specifically target monocyte migration, we hypothesized that flurbiprofen axetil may attenuate remifentanil-induced hyperalgesia, at least in part, by modulating monocyte migratory activity.
On the basis of these considerations, this study was undertaken to characterize remifentanil-induced hyperalgesia under clinically relevant anesthetic conditions using animal models and a randomized controlled clinical trial. We further examined the potential role of monocyte migration in RIH and assessed whether flurbiprofen axetil could serve as a preventive intervention. Through the integration of mechanistic and clinical approaches, this work seeks to advance understanding of the pathophysiology and perioperative management of RIH.
Materials and Methods
Animals
Male C57/B6J mice (6−8 weeks old) were purchased from the Institute of Experimental Animals, Sun Yat−sen University (Guangzhou, China). Animals were housed under a 12h light/dark cycle with ad libitum access to food and water. Standard laboratory chow was supplied in pellet form and replenished regularly. Drinking water was supplied via sterilized bottles and changed at regular intervals to ensure cleanliness and adequate intake. The ambient temperature was maintained at 24 °C, with relative humidity controlled at 50−60%. All the experimental procedures were approved by the Institutional Animal Care and Use Committee of Zhongshan Ophthalmic Center of Sun Yat−sen University. (Approval No. Z2021062, issued in 2021), and were conducted in accordance with the relevant national and institutional guidelines.
Monocyte Depletion in Mice and Remifentanil−Induced Hyperalgesia Mice Model
On day 1–3, the male C57/B6J mice of experimental group received daily intraperitoneal injections of clodronate liposomes (1 µg/10 g) for three consecutive days to deplete circulating monocytes. In the control group, male C57/B6J mice received daily intraperitoneal injections of PBS liposomes (1 µg/10 g) over the same three-day period. On day 4, The remifentanil-induced hyperalgesia (RIH) model was established as described previously, with minor modifications. Briefly, mice were anesthetized with isoflurane (2%) delivered in oxygen using a calibrated small-animal anesthesia vaporizer and a nose-cone inhalation system. During anesthesia, remifentanil was administered via continuous intraperitoneal infusion at a rate of 4 μg/kg/min for 1 h using a programmable microinfusion pump connected to a sterile intraperitoneal catheter. Following completion of remifentanil administration, anesthesia was discontinued, and mice were transferred to a temperature-controlled recovery chamber maintained at 30–32 °C with ambient humidity and a standard light environment. Animals were monitored until full recovery of spontaneous activity and were then returned to their home cages with free access to food and water.
Mechanical Pain Threshold Test in Mice
Mechanical pain thresholds of both hind paws were assessed before surgery and on postoperative days 1 and 2 using the von Frey filament test. Before the experiment, mice were habituated to the testing environment for 1 h in a quiet room at room temperature. Each mouse was individually placed in a transparent chamber positioned on a metal mesh floor, allowing unrestricted movement. The hind paw skin of the mouse was stimulated vertically using Von Frey fibers. Each von Frey filament started from 0.4 g. Paw withdrawal in response to stimulation was considered a positive response, and the up–down method was applied to determine subsequent filament forces. Following the occurrence of the first change in response (from positive to negative or vice versa), four additional stimulations were performed. The 50% paw withdrawal threshold (PWT) was calculated using the Dixon formula, as previously described.11
Flow Cytometry for Leukocytes and Tissue Macrophages in Left Paw
After assessment of the final paw withdrawal threshold (PWT), mice were anesthetized with isoflurane, and peripheral blood was collected by cardiac puncture into EDTA-coated tubes. Leukocytes were isolated, washed, and stained with fluorochrome-conjugated antibodies for surface antigen analysis. Mice were then deeply anesthetized and euthanized by carbon dioxide inhalation, followed by transcardial perfusion with phosphate-buffered saline (PBS). Both hind paws were excised at the ankle joints.
The paw tissues were minced and digested in RPMI/HEPES medium (Corning) containing 5 mg/mL collagenase for 1.5–2 h at 37 °C with gentle agitation every 15 min. The resulting cell suspension and remaining tissue fragments were passed through a 70-μm nylon mesh filter using a 5-mL syringe plunger to further dissociate cells. The filter was rinsed with 2 mL of RPMI/HEPES, and the suspension was collected into a 15-mL tube. An additional 10 mL of RPMI/HEPES was added to dilute the collagenase and preserve cell viability. Samples were centrifuged at 500 × g for 5 min, and the cell pellets were resuspended in 1 mL of FACS buffer for flow cytometric analysis.
For Fc receptor blocking, cells were incubated with 0.5 μL of TruStain FcX™ PLUS in 50 μL of FACS buffer for 30 min at room temperature. Cells were then stained with APC-conjugated anti-CD11b antibody (clone M1/70; Elabscience; 5 μL per test) in 50 μL of FACS buffer for 30 min in the dark. After washing, cells were resuspended in 300 μL of FACS buffer. CD11b⁺ cells were sorted using a BD FACSAria cell sorter and collected into RPMI medium supplemented with 2% fetal bovine serum (FBS), followed by resuspension in PBS containing 2% FBS. Flow cytometric acquisition was performed using a BD FACSCelesta or LSR II cytometer (BD Biosciences, San Jose, CA). Data were analyzed using FlowJo software (version 10.6.1; FlowJo LLC).
Clinical Study Design and Participants
This was a single−center, prospective, randomized, single−blind clinical trial. Ethical approval was obtained from the Institutional Review Board of Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangzhou, China (Approval No. 2021KYPJ216). The trial was preregistered at the Chinese Clinical Trial Registry prior to patient enrollment (ChiCTR2200060031; principal investigator: Xiaoliang Gan; registration date: May 15, 2022). This study was conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Patients undergoing corneal transplantation at the Zhongshan Ophthalmic Center of Sun Yat−sen University between June 2022 and April 2023 were screened for enrollment. The inclusion criteria were as follows: (1) male patients aged 18–45 years scheduled for elective corneal transplantation; (2) American Society of Anesthesiologists (ASA) physical status I−II; and (3) body mass index (BMI) between 18−30 kg/m2. Exclusion criteria include: (1) a history of gastrointestinal bleeding, peptic or duodenal ulcer disease, inflammatory bowel disease, coagulation disorders, prior cerebrovascular hemorrhage, known arteriovenous malformations, asthma, or other conditions associated with an increased risk of bleeding related to nonsteroidal anti-inflammatory drug (NSAID) use; (2) known allergy to any medication used in the study; (3) a history of chronic pain or preoperative use of analgesics; (4) use of immunosuppressive agents within the preceding 3 months; (5) exposure to general anesthesia within the previous 3 months; (6) prior ocular or upper limb surgery; (7) severe cardiac arrhythmias, including sick sinus syndrome, second- or third-degree atrioventricular block, bundle branch block, or severe bradycardia (heart rate < 50 beats/min); (8) cardiac insufficiency with a left ventricular ejection fraction (LVEF) < 40%; (9) coronary artery disease or a history of myocardial infarction; (10) severe renal dysfunction (serum creatinine > 2 mg/dL); (11) severe hepatic dysfunction (Child–Pugh class C); and (12) cognitive impairment precluding the ability to understand or respond to study-related questions.
Anesthesia Induction and Maintenance
All patients fasted for at least 8 h before surgery. Before entering the operating room, a general questionnaire was completed, and mechanical pain thresholds around the eyes and both upper limbs were assessed. Standard monitoring, including electrocardiography (ECG), heart rate (HR), noninvasive blood pressure (NIBP), pulse oxygen saturation (SpO2), and bispectral index (BIS), was applied. Peripheral venous access was established and Lactated Ringer’s solution was infused at a rate of 6–8 mL/kg/h.
General anesthesia was induced using propofol (1.5–2.5 mg/kg), remifentanil (1 μg/kg), and cisatracurium (0.2 mg/kg). An optimal size of laryngeal airway mask (LMA) was inserted to facilitate mechanical ventilation. Anesthesia was maintained with sevoflurane (1–2%) and continuous intravenous infusion of remifentanil (0.3 μg/kg/min). Patients were mechanically ventilated with a tidal volume of 6−8 mL/kg with a fresh gas flow 2 L/min of 100% oxygen. The respiratory rate (RR) was adjusted to maintain an end−tidal carbon dioxide partial pressure of 35−45 mmHg (1 mmHg = 0.133 kPa). Depth of anesthesia was maintained within a BIS range of 45–60.
At the end of surgery, sevoflurane and remifentanil were discontinued, and patients were transferred to the post-anesthesia care unit (PACU). The LMA was removed once patients were fully awake and met the following criteria: tidal volume > 6 mL/kg, respiratory rate of 12–20 breaths/min, and the ability to respond to verbal commands.
Randomization and Blinding
This was a double-blind randomized trial. Participants who have provided informed consent will be assigned to a treatment group using sequentially numbered, sealed envelopes. On the day of surgery, before induction of anesthesia, an anesthesiologist not involved in the study opened the corresponding envelope, prepared the study medication according to the assignment, and initiated drug administration.
Patients were randomly allocated to either the control group (Group C, n = 22) or the flurbiprofen axetil group (Group F, n = 22). Patients in Group F received an intravenous bolus of flurbiprofen axetil (1 mg/kg) during induction of anesthesia, followed by an additional dose of 1 mg/kg at the end of surgery. Patients in Group C received an equal volume of 0.9% normal saline according to the same administration protocol. All study medications were prepared in identical 10-mL opaque syringes and administered slowly over 1 min for each bolus injection, ensuring blinding of patients and investigators.
Measurement of Mechanical Pain Threshold and Post−Operative Pain
All patients underwent a mechanical pain threshold test using an Electronic von Frey (EvF) device (IITC Life Science, Woodland Hills, CA) at three time points: before anesthesia, 2 h after surgery, and 24 h after surgery. The tip of the probe was first pressed at a right angle against the skin surface, 2 cm above and below the bilateral edge of the orbit, and the applied force was increased at a controlled rate. When the patient felt pain, the probe was removed, and the pain threshold was recorded. The procedure was then repeated on the medial side of each forearm, 3, 6, and 9 cm distal to the middle of the antecubital fold, and the mean of the results at the three sites was calculated. There was a 30s interval between each measurement.
Complete Blood Count Examination, Chemokine Concentration, Expression of COX−2, and Monocyte Viability
Peripheral venous blood was collected from a vein in the non-dominant arm into EDTA tubes before anesthesia in the preoperative waiting area, and 2 h after surgery in the post-anesthesia care unit (PACU) for complete blood count examination and measurements of chemokine concentration. For ex vivo stimulation experiments, 200 μL of whole blood (5 × 106 cells/mL) was added to 24-well plates containing RPMI 1640 medium in the presence of remifentanil (1, 10, 100, or 1000 ng/mL) or normal saline. The samples were incubated at 37 °C in a humidified atmosphere with 5% CO2 for 3 h.
After incubation, cells were harvested, and 10 μL of the cell suspension was mixed with propidium iodide (PI) staining solution to assess cell viability using an automated cell counter.
Plasma concentrations of CCL3 and granulocyte colony-stimulating factor (G-CSF) were quantified using enzyme-linked immunosorbent assay (ELISA). Expression of cyclooxygenase-2 (COX-2) mRNA in peripheral blood mononuclear cells (PBMCs) was measured by quantitative real-time PCR (qRT-PCR), according to the manufacturers’ instructions.
Outcomes
The primary outcome was the incidence of mechanical hyperalgesia at 2 h after surgery. Based on previous studies, hyperalgesia was defined as a reduction of ≥25% in postoperative mechanical pain threshold compared with the preoperative baseline.4,11
Secondary outcomes included numerical rating scale (NRS) scores, blood examination results, plasma concentrations of CCL3 and granulocyte colony-stimulating factor (G-CSF), and cyclooxygenase-2 (COX-2) expression at 2 and 24 h after surgery.
Peripheral Blood Whole Blood Cell Migration Assay
For the Transwell migration assay, 200 μL of whole blood (5 × 106 cells/mL) was added to the upper chamber of a Transwell insert (Corning, USA). The lower chamber was filled with 800 μL of medium containing either normal saline (control) or remifentanil at concentrations of 100 or 1000 ng/mL. Cells were incubated at 37 °C in a humidified atmosphere with 5% CO2 for 3 h. After incubation, non-migrated cells on the upper surface of the membrane were gently removed using a cotton swab.
The inserts were then rinsed with phosphate-buffered saline (PBS), fixed with paraformaldehyde, and stained with crystal violet. Cells that migrated to the lower surface of the membrane were visualized under a microscope, photographed, and quantified using ImageJ software.
Statistical Analysis
In a preliminary experiment involving 10 patients, the incidence of hyperalgesia was 10% in the flurbiprofen axetil group (Group F) and 60% in the control group (Group C). Based on these proportions, the minimum required sample size for a two-sided comparison of proportions was calculated. A sample size of at least 17 patients per group, with a significance level (α) of 0.05, was estimated to provide 80% statistical power. Sample size calculations were performed using IBM SPSS Statistics for Windows (version 23.0; IBM Corp., Armonk, NY, USA) and R software (R Core Team, 2024).
Statistical analyses were performed using SPSS version 23.0 (IBM Corp., Chicago, IL, USA). Data distribution was assessed using the Kolmogorov–Smirnov test and visual inspection of histograms. Normally distributed data are presented as mean ± standard deviation (SD), whereas non-normally distributed data are expressed as median (interquartile range, IQR). Categorical variables are presented as number (percentage). Independent t-tests or Mann–Whitney U-tests were used to compare mechanical pain thresholds, numerical rating scale (NRS) scores, circulating monocyte counts, and COX-2 expression between groups. Categorical variables, including the incidence of hyperalgesia, were analyzed using the Pearson χ2-test or Fisher’s exact test, as appropriate. A two-tailed P value < 0.05 was considered statistically significant.
Ethics Approval and Consent to Participate
The clinical trial component of this study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board of Zhongshan Ophthalmic Center, Sun Yat-sen University (Approval No. 2021KYPJ216). The trial was prospectively registered at the Chinese Clinical Trial Registry (ChiCTR2200060031). Written informed consent was obtained from all participants prior to enrollment.
All animal experiments were reviewed and approved by the Institutional Animal Care and Use Committee of Zhongshan Ophthalmic Center, Sun Yat-sen University (Approval No. Z2021062). All procedures involving laboratory animals were performed in accordance with the National Guidelines for the Care and Use of Laboratory Animals and relevant institutional regulations. Every effort was made to minimize animal suffering and to reduce the number of animals used.
Results
Remifentanil Induces Hyperalgesia in Mice Accompanied by Decreases in Circulating Monocyte
As shown in Figure 1, remifentanil infusion (4 μg/kg/min) resulted in significant decrease in paw withdrawal threshold (PWT) in mice, which persisted for up to 2 days after infusion (p < 0.05). Meanwhile, remifentanil induced a significant reduction in circulating monocyte counts at 3 h post-infusion and a concomitant increase in peripheral macrophage counts in the left paw (all P < 0.05).
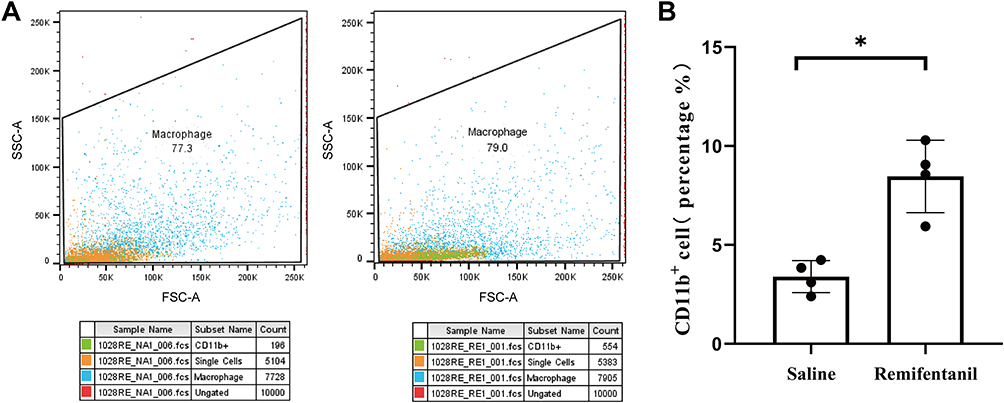 |
Figure 1 (A) Representative flow cytometry plots of CD11b+ cells in hind paw cell suspensions from mice following establishment of the remifentanil-induced hyperalgesia (RIH) model. RIH model group (Remifentanil infusion) vs Sham group (saline infusion) (n=4). (B) Quantitative analysis of CD11b+ cell percentage. |
Depletion of Circulating Monocytes Alleviates Remifentanil−Induced Hyperalgesia
Next, we examined the role of monocyte migration in the hyperalgesia. Depletion of circulating monocytes markedly attenuated the persistent remifentanil-induced reduction in mechanical pain threshold in mice (Figure 2, P < 0.05).
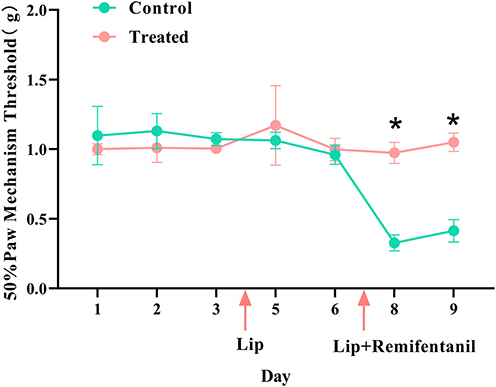 |
Figure 2 Baseline mechanical pain thresholds were measured in mice prior to intraperitoneal administration of clodronate liposomes or PBS liposomes (0.15 mL/kg), followed by a 3-day observation period. Mechanical withdrawal thresholds of the hind paw were assessed at designated time points during the 3-day period. On day 3 post-injection, the remifentanil-induced hyperalgesia (RIH) model was established, and mechanical hypersensitivity was subsequently evaluated (*p<0.05 vs Control group; n=4). |
Flurbiprofen Axetil Did Attenuate RIH
The CONSORT flow diagram illustrates the number of participants who received the allocated interventions. A total of 44 eligible patients were enrolled and included in the final analysis (Figure 3). Baseline patient demographics and surgical characteristics are summarized in Table 1. As shown in Table 1, there were no significant differences between the two groups with respect to age, body mass index, or American Society of Anesthesiologists (ASA) physical status (P > 0.05). In addition, intraoperative remifentanil dosage, duration of surgery, time to laryngeal mask airway (LMA) removal, and time to achieve a post-anesthesia discharge score (PADS) ≥ 9 were comparable between the two groups (P > 0.05).
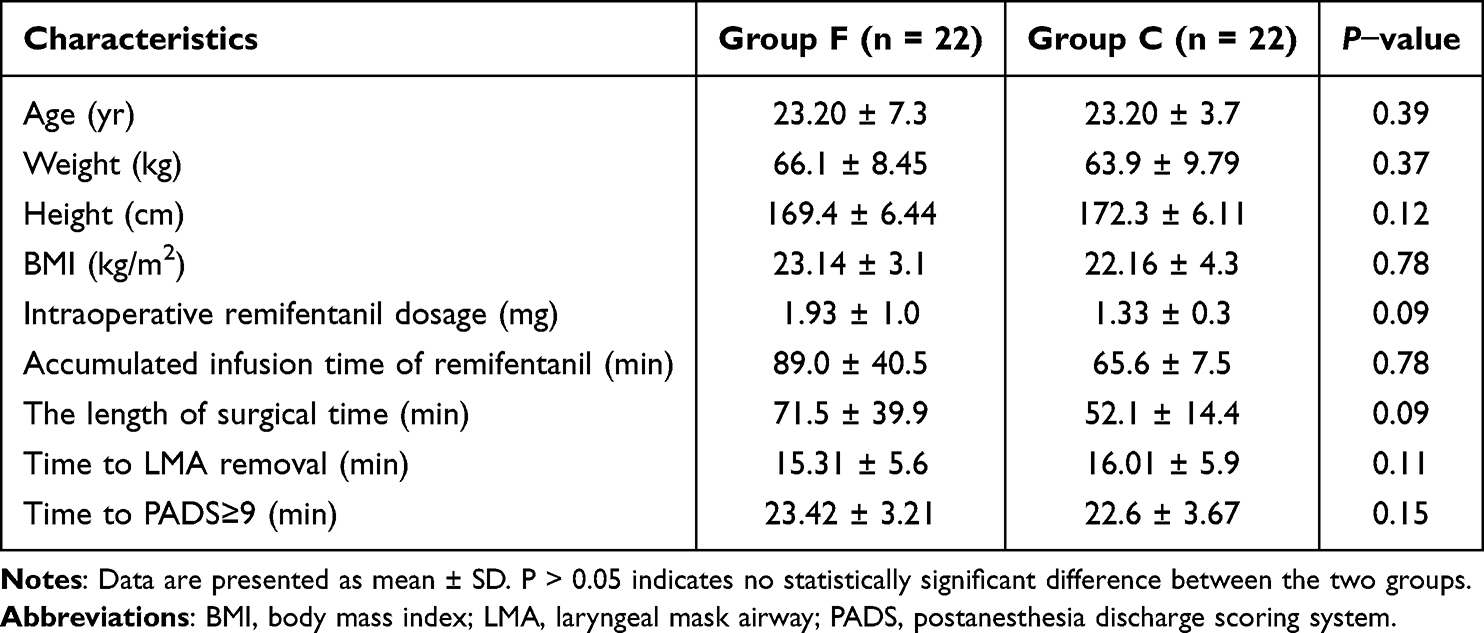 |
Table 1 Comparison of Patient Demographics and Surgical Characteristics Between the Two Groups |
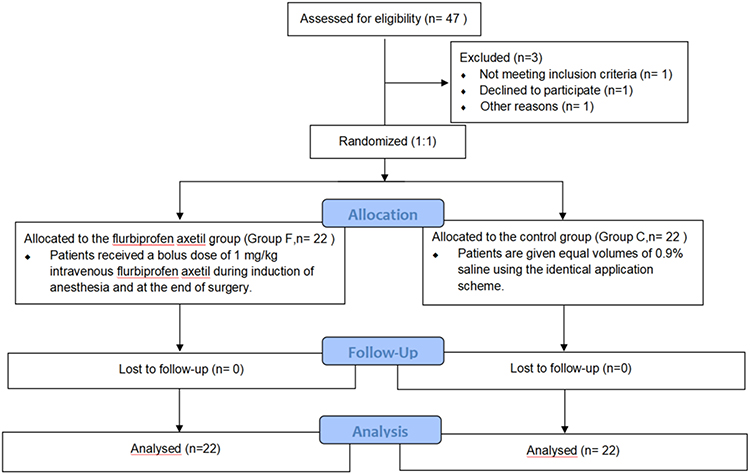 |
Figure 3 CONSORT diagram of patient recruitment. |
As shown in Figure 4A and B, except for the medial and inferior regions of the operative eye, mechanical pain thresholds at all measured sites were significantly higher in the flurbiprofen axetil group than in the control group at 2 h after surgery (P < 0.05). However, no significant differences in mechanical pain thresholds were observed between the two groups at 24 h postoperatively (Figure 4C and D, P > 0.05).
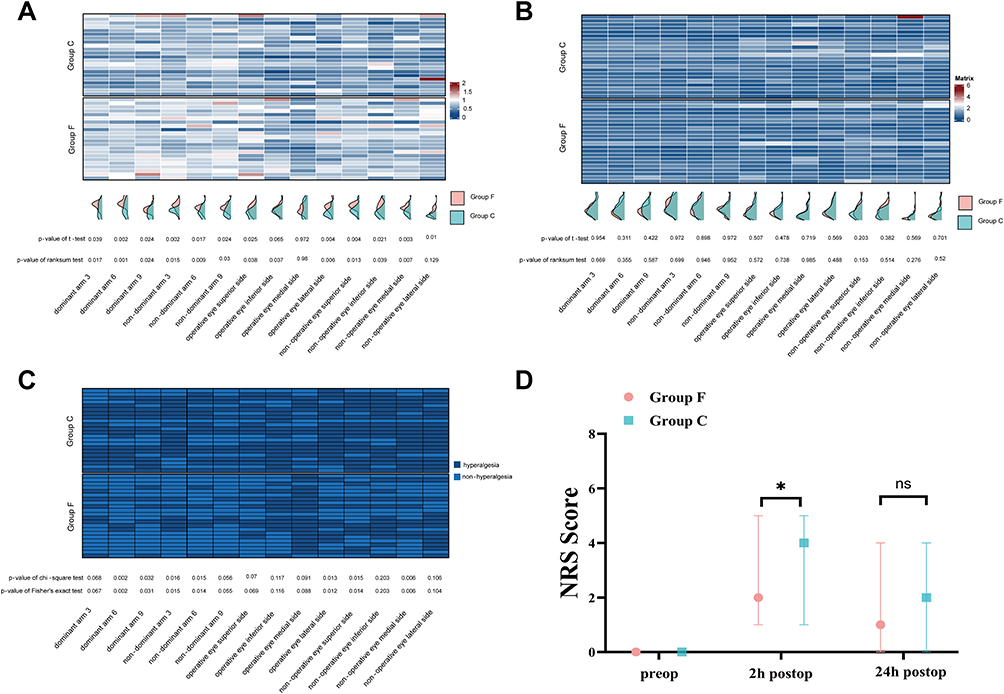 |
Figure 4 (A) Heatmap of the postoperative 2-hour/preoperative mechanical pain threshold at various points; (B) Heatmap of the postoperative 24-hour/preoperative mechanical pain threshold at various points; (C) A binary heatmap constructed based on the criteria that a postoperative 2-hour/preoperative mechanical pain threshold ratio less than 0.75 is defined as remifentanil induced hyperalgesia (RIH); (D) The NRS score of the flurbiprofen axetil group was significantly lower than that of the control group 2 hours after surgery, which became comparable between the two groups 24 hours after operation. |
As summarized in Table 2, remifentanil infusion at a rate of 0.3 μg/kg/min induced mechanical hyperalgesia in 81.8% of patients in the control group. The incidence of remifentanil-induced hyperalgesia (RIH) was significantly reduced in patients receiving flurbiprofen axetil (50%, P = 0.03). By 24 h after surgery, the incidence of RIH was comparable between the two groups (P > 0.05).
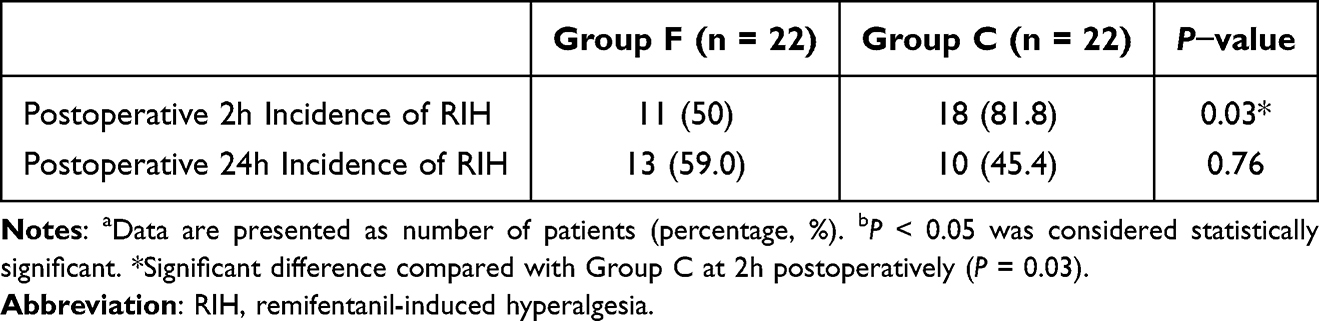 |
Table 2 Incidence of Remifentanil-Induced Hyperalgesia (RIH) in the Two Groups |
Consistent with these findings, a binary heatmap constructed based on the criterion of a postoperative 2-h/preoperative mechanical pain threshold ratio < 0.75 demonstrated a clear between-group difference at 2 h after surgery (Figure 4C).
In addition, numerical rating scale (NRS) scores at 2 h postoperatively were significantly lower in the flurbiprofen axetil group [2.00 (1.00–3.00)] than in the control group [4.00 (2.25–4.75), P = 0.002; Figure 4D. No significant difference in NRS scores was observed between the two groups at 24 h after surgery [1.00 (0.00–2.00) vs 2.00 (1.00–2.00), P = 0.31].
Flurbiprofen Axetil Blocked the Reductions in Circulating Monocyte Count Induced by Remifentanil
As shown in Figure 5, the change in circulating monocyte counts from the preoperative baseline to 2 h postoperatively was significantly reduced in patients receiving remifentanil, as reflected by a negative postoperative-to-preoperative difference. This reduction was significantly attenuated in patients who additionally received flurbiprofen axetil (P < 0.01 for both the independent t-test and Mann–Whitney U-test; standardized mean difference [SMD] = 1.13).
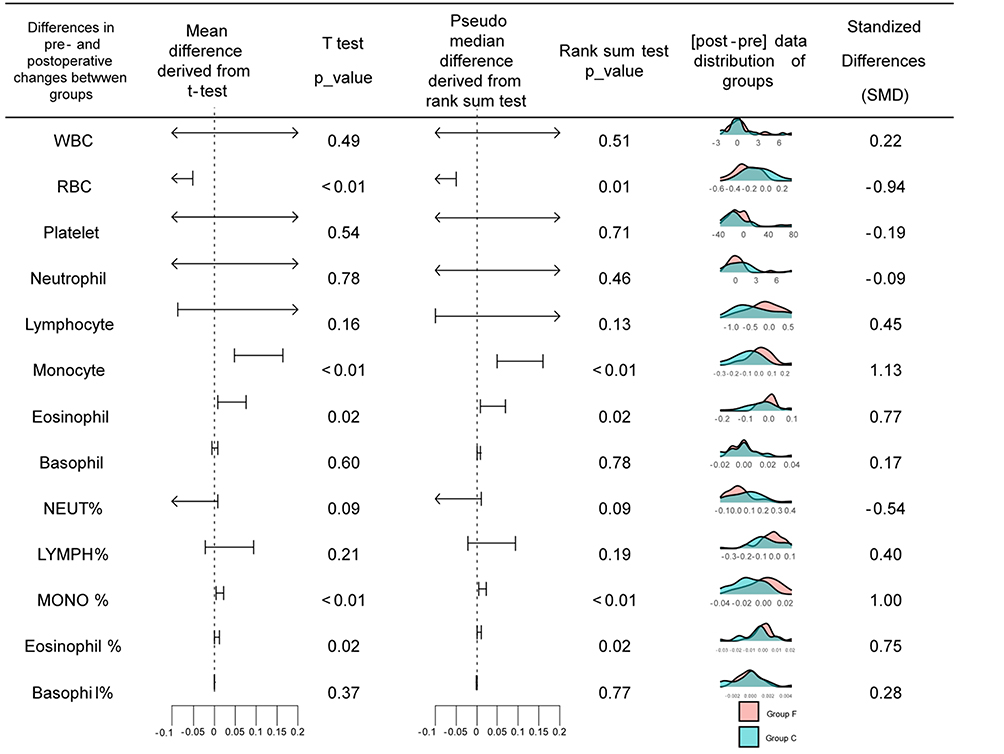 |
Figure 5 The figure summarizes the differential trends in white blood cell lineages and related indices between the two study groups. Differences in changes: The left and middle panels display the mean differences (derived from independent samples t-test) and pseudo-median differences (derived from Mann–Whitney U/Rank sum test) with their corresponding 95% confidence intervals (CIs). Statistical Significance: P-values for both parametric (T-test) and non-parametric (Rank sum test) analyses are provided for each parameter. Parameters such as RBC, Monocyte, Eosinophil, MONO %, and Eosinophil % show statistically significant differences between the groups (P < 0.05). Data Distribution: The density plots represent the distribution of [postoperative - preoperative] delta values for Group F (pink) and Group C (teal). Effect Size: The rightmost column lists the Standardized Mean Difference (SMD) to quantify the magnitude of the difference between groups. Abbreviations: WBC, white blood cell count; RBC, red blood cell count; NEUT, neutrophil; LYMPH, lymphocyte; MONO, monocyte; SMD, standardized mean difference. |
A similar pattern was observed for the proportion of monocytes among total white blood cells, with a significantly smaller postoperative decrease in the flurbiprofen axetil group compared with the control group (P < 0.01 for both tests; SMD = 1.00).
Elevation of Plasma CCL3, but Not PGE2 May Contribute to Remifentanil Induced Monocyte Transmigration
As shown in Figure 6A and B, remifentanil infusion did not significantly alter cyclooxygenase (COX) mRNA expression in circulating monocytes or plasma prostaglandin E2 (PGE2) concentrations in the control group, and these parameters were not affected by flurbiprofen axetil treatment (P = 0.56).
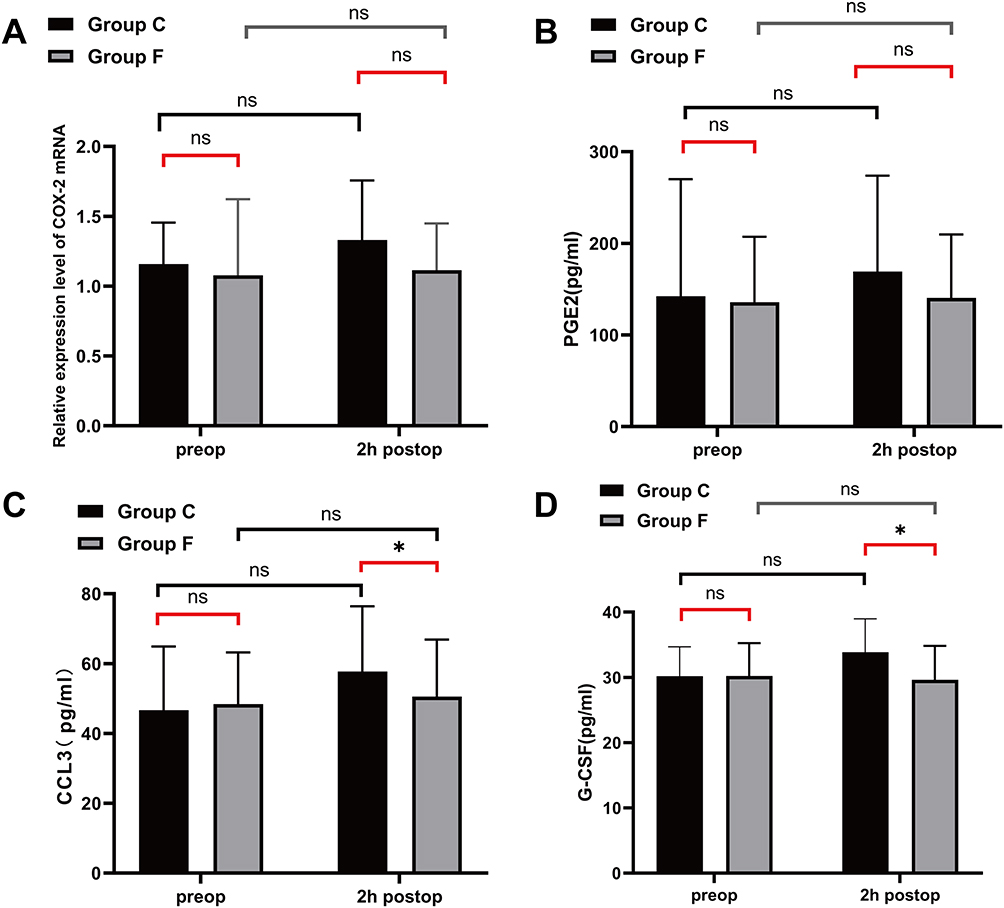 |
Figure 6 (A) Relative expression levels of cyclooxygenase mRNA in whole blood mononuclear cells preoperative and postoperative 2-hour; (B) PGE2 levels in plasma preoperative and postoperative 2-hour; (C) CCL3 levels in plasma preoperative and postoperative 2-hour; (D) G-CSF levels in plasma preoperative and postoperative 2-hour. Data are expressed in terms of mean and standard deviation. *p<0.05 compared with group C. |
In contrast, remifentanil infusion resulted in a modest but significant increase in plasma CCL3 and granulocyte colony-stimulating factor (G-CSF) concentrations within 2 h after surgery. These increases were significantly attenuated by flurbiprofen axetil treatment (P = 0.001 and P = 0.023, respectively; Figure 6C and D).
As shown in Figure 7A, exposure to remifentanil in vitro did not significantly affect total white blood cell counts or cell viability, even at a high concentration of 1000 ng/mL (P > 0.05). In contrast, Transwell migration assays demonstrated a significant increase in peripheral blood mononuclear cell (PBMC) counts in the lower chamber following remifentanil treatment (P < 0.05; Figure 7B).
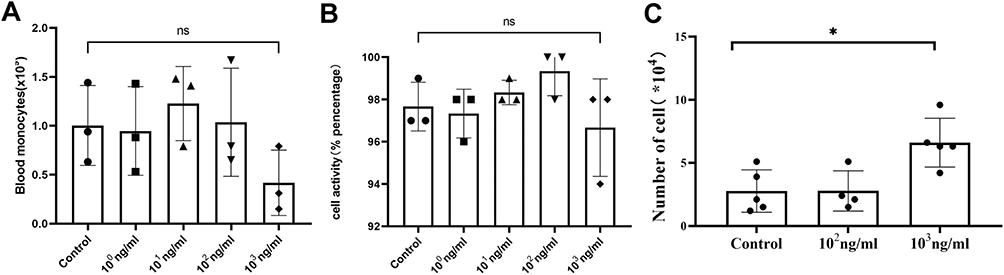 |
Figure 7 (A and B) Changes in the number of monocytes cultured with different concentrations of remifentanil in whole blood for 3 h; (C) Changes in leukocytes activity after 3 h of culture with different concentrations of remifentanil in whole blood. |
These findings suggest that the observed reduction in circulating monocytes is unlikely to result from cell loss or cytotoxicity, but may instead be attributable to remifentanil-induced extravascular migration.
Discussion
Remifentanil-induced hyperalgesia (RIH) is a well-recognized phenomenon that limits the clinical utility of remifentanil, particularly in total intravenous anesthesia. In the present study, prolonged remifentanil infusion (>1 h) resulted in a significant reduction in mechanical pain thresholds in both mice and patients, accompanied by a marked decrease in circulating monocyte counts. Importantly, depletion of circulating monocytes in mice markedly attenuated remifentanil-induced mechanical hyperalgesia, while administration of flurbiprofen axetil significantly alleviated both the reduction in mechanical pain threshold and the decline in circulating monocytes in patients. Furthermore, in vitro experiments demonstrated that remifentanil, even at high concentrations, did not impair monocyte viability but instead promoted monocyte migration in a Transwell assay. Taken together, these findings suggest that extravascular migration of monocytes contributes to the development of remifentanil-induced hyperalgesia.
Monocytes are the largest white blood cells in peripheral blood and originate from hematopoietic stem cells in the bone marrow. They are characterized by high nonspecific esterase activity and potent phagocytic capacity. Previous studies have implicated monocytes in chronic pain conditions. For example, Merriwether et al reported that monocytes from patients with fibromyalgia produced higher levels of interleukin (IL)-5 and IL-1β following lipopolysaccharide (LPS) stimulation compared with healthy controls.12 In the present study, remifentanil administration was associated with both a reduction in mechanical pain thresholds and a significant decrease in circulating monocyte counts, reflected by reductions in both the percentage and absolute number of monocytes, alongside increased macrophage accumulation in peripheral tissues. Notably, depletion of circulating monocytes markedly attenuated remifentanil-induced hyperalgesia in mice. Consistent with these findings, Mai et al demonstrated that monocyte transmigration into the brain perivascular space plays a critical role in neuropathic pain. Taken together, these observations support an association between remifentanil-related reductions in circulating monocytes and the development of hyperalgesia, potentially mediated by monocyte migration into peripheral or central tissues.
Multiple mechanisms may contribute to the observed reduction in circulating monocyte counts. Previous studies have reported that opioids can decrease the number and functional capacity of peripheral immune cells, partly through the induction of apoptosis.13 In addition, remifentanil has been shown to induce autophagy in certain cell types.14 To explore whether reduced monocyte counts were attributable to cell death, we conducted ex vivo experiments in which whole blood was incubated with remifentanil and cell viability was assessed. Notably, cell viability remained stable across increasing remifentanil concentrations, suggesting that remifentanil-associated monocyte reduction is unlikely to be primarily driven by apoptosis. An alternative explanation is that remifentanil promotes monocyte redistribution rather than depletion. Consistent with this hypothesis, our in vitro Transwell assays demonstrated that remifentanil directly enhanced monocyte transmigration. Taken together, these findings support a role for monocyte/macrophage migration in the development of remifentanil-induced hyperalgesia (RIH).
In previous studies, the precise mechanism of remifentanil-induced hyperalgesia (RIH) has remained unclear, partly because the confounding effects of surgical trauma could not be excluded.15 In the present study, we deliberately selected a minimally invasive intraocular procedure—corneal transplantation, which has limited systemic impact—and an animal model without a surgical procedure to better isolate the mechanism underlying RIH. Mechanical pain thresholds around the surgical field and in both upper limbs were quantitatively assessed using an electronic von Frey device. Consistent with previous reports, high-rate remifentanil infusion reduced mechanical pain thresholds in both upper limbs distant from the surgical site.16,17
Because remifentanil is frequently required in total intravenous anesthesia (TIVA), minimizing remifentanil-induced hyperalgesia (RIH) has become a clinical priority. Previous studies have evaluated pharmacological strategies for preventing RIH. For example, one study showed that paracetamol can attenuate remifentanil-induced hyperalgesia.18 In addition, cyclooxygenase-2 (COX-2) has been implicated in RIH through ephrin-B/EphB signaling pathways.7 Ephrin-B/EphB signaling can regulate COX-2 expression, and inhibition of COX-2 activity has been shown to alleviate RIH.19 In the present study, we found that flurbiprofen axetil not only reduced RIH but also lowered postoperative pain scores after intraocular surgery. This finding is consistent with our previous report showing that flurbiprofen axetil attenuated postoperative pain following oculoplastic surgery.20 However, flurbiprofen axetil did not reduce circulating COX-2 expression in our study, suggesting that additional mechanisms beyond COX-2 signaling may contribute to RIH.
The chemokines CCL3 and granulocyte colony-stimulating factor (G-CSF) play critical roles in promoting monocyte recruitment and extravascular migration.21 After migrating into extravascular tissues, monocytes can differentiate into macrophage precursors and contribute to the regulation of neuropathic pain.22,23 Consistent with this framework, our results showed that remifentanil induced modest but significant increases in CCL3 and G-CSF levels, further supporting a role for monocyte migration in the development of hyperalgesia.
In our study, flurbiprofen axetil attenuated both the development of hyperalgesia and the reduction in circulating monocyte counts. Flurbiprofen axetil is known to exert analgesic effects primarily through inhibition of cyclooxygenase-2 (COX-2) activity in the spinal cord. Beyond its analgesic effects, our findings suggest that flurbiprofen axetil also suppressed CCL3 and granulocyte colony-stimulating factor (G-CSF) levels. Consistent with these observations, previous studies have shown that cyclooxygenase inhibition can reduce immune cell adhesion and migration.24 However, the mechanistic links among COX-2, CCL3, and G-CSF remain to be elucidated and warrant further investigation.
The advantages of this study are the selection of intraocular surgery (corneal transplantation) with a small incision and no interference with the systemic environment; furthermore, the patients do not receive any treatments that may affect the pain threshold (such as 5−HT3 receptor antagonists or dexamethasone). However, this study also has some limitations:1) the practical difficulty of obtaining blood samples for circulating monocyte analysis at 24 hours postoperatively in day-surgery patients limited our ability to capture the full immune dynamics at a potentially critical time point; 2) the relatively small sample size, combined with the exclusive focus on young male subjects and male animal models, constrains the statistical power and generalizability of our findings. This is particularly relevant in the context of pain-immunology research, where significant sex- and age-related dimorphisms are well-established. Consequently, the mechanisms identified here may be specific to this homogeneous young male/male cohort, and our results cannot be directly extrapolated to broader populations, such as females or elderly patients; and 3) the assessment of hyperalgesia relied primarily on qualitative examination of areas surrounding and distant from the surgical site, rather than on quantitative measures of the hyperalgesic area or thermal pain thresholds, which may affect the precision of our hypersensitivity evaluation; and 4) Macrophage accumulation in peripheral tissues was used as a surrogate marker of immune cell recruitment; however, the absence of direct histological or cell-tracking evidence limits definitive conclusions regarding active transmigration.
In conclusion, extravascular migration of circulating monocytes plays a critical role in remifentanil induced hyperalgesia.
Data Sharing Statement
The authors do not intend to share individual de-identified participant data. This decision is based on institutional data governance policies and the scope of informed consent obtained from participants.
Aggregate data supporting the findings of this study are included within the article. No additional study documents will be made publicly available.
Requests for access to data may be directed to the corresponding author and will be considered on a case-by-case basis, subject to institutional approval and applicable ethical and data protection regulations. Such requests may be submitted beginning after publication and will be considered for a period of 12 months.
Acknowledgments
This work was supported by National Natural Science Foundation of China (82571387), and the clinical research project of Zhongshan Ophthalmic Center of Sun Yat−sen University (3030901011175). The sponsors had no role in the study design, survey process, data analysis, or manuscript preparation. Rui Zhang, Zexi Ye, and Qianru Chen are co−first authors for this study. This study was registered at the Chinese Clinical Trial Registry (ChiCTR2200060031, principal investigator: X. Gan, date of registration: May 15, 2022), and can be reached at https://www.chictr.org.cn/showproj.html?proj = 170064.
Author Contributions
Designed the protocol, drafted and revised the manuscript: Rui Zhang, MD; Conduct the study, and edit the manuscript: Zexi Ye, MD., Qianru Chen, MD; Collected the data: Yongyi Wang, BD. Honglian He, MD, Jinfei Li, MD; Analyzed the data.: Yanling Zhu, MD, Zexi Ye, MD; Helped with study conception, reviewing and editing the manuscript: Xiaoliang Gan, MD, PhD. Youjin Hu, MD, PhD. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Rui Zhang and Zexi Ye are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Hadavi SMR, Eghbal MH, Kaboodkhani R, Alizadeh N, Sahmeddini MA. Comparison of pregabalin with magnesium sulfate in the prevention of remifentanil-induced hyperalgesia in patients undergoing rhinoplasty: a randomized clinical trial. Laryngoscope Investig Otolaryngol. 2022;7(5):1360–14. doi:10.1002/lio2.905
2. Vitin AA, Egan TD. Remifentanil-induced hyperalgesia: the current state of affairs. Curr Opin Anaesthesiol. 2024;37(4):371–378. doi:10.1097/ACO.0000000000001400
3. Kern SE, Xie G, White JL, Egan TD. A response surface analysis of propofol-remifentanil pharmacodynamic interaction in volunteers. Anesthesiology. 2004;100(6):1373–1381. doi:10.1097/00000542-200406000-00007
4. Jia Z, Chen Y, Gao T, et al. Nalmefene vs. dexmedetomidine for prevention of postoperative hyperalgesia in patients undergoing laparoscopic gynecological surgery with remifentanil infusion: a randomized double-blind controlled trial. Front Pharmacol. 2023;14:1131812. doi:10.3389/fphar.2023.1131812
5. Zhu Y, Yan P, Wang R, et al. Opioid-induced fragile-like regulatory T cells contribute to withdrawal. Cell. 2023;186(3):591–606.e23. doi:10.1016/j.cell.2022.12.030
6. Mai CL, Tan Z, Xu YN, et al. CXCL12-mediated monocyte transmigration into brain perivascular space leads to neuroinflammation and memory deficit in neuropathic pain. Theranostics. 2021;11(3):1059–1078. doi:10.7150/thno.44364
7. Peng Y, Zang T, Zhou L, Ni K, Zhou X. COX-2 contributed to the remifentanil-induced hyperalgesia related to ephrinB/EphB signaling. Neurol Res. 2019;41(6):519–527. doi:10.1080/01616412.2019.1580459
8. Zhang L, Shu R, Zhao Q, et al. Preoperative but not postoperative flurbiprofen axetil alleviates remifentanil-induced hyperalgesia after laparoscopic gynecological surgery: a prospective, randomized, double-blinded, trial. Clin J Pain. 2017;33(5):435–442. doi:10.1097/AJP.0000000000000416
9. Feng CD, Xu Y, Chen S, et al. Opioid-free anaesthesia reduces postoperative nausea and vomiting after thoracoscopic lung resection: a randomised controlled trial. Br J Anaesth. 2024;132(2):267–276. doi:10.1016/j.bja.2023.11.008
10. Wu J, Bley M, Steans RS, et al. Nicotinamide riboside augments human macrophage migration via SIRT3-mediated prostaglandin E2 signaling. Cells. 2024;13(5):455. doi:10.3390/cells13050455
11. Chaplan SR, Bach FW, Pogrel JW, Chung JM, Yaksh TL. Quantitative assessment of tactile allodynia in the rat paw. J Neurosci Methods. 1994;53(1):55–63. doi:10.1016/0165-0270(94)90144-9
12. Ye Z, Zhu Y, Zhang R, Wang Y, Huang J, Gan X. Effect of multimodal preemptive analgesia of flurbiprofen axetil, nalbuphine, and retrobulbar block on postoperative pain and enhanced recovery in patients undergoing oculoplastic day surgery: a prospective, randomized, double-blinded study. Ophthalmic Plast Reconstr Surg. 2023;39(3):260–265. doi:10.1097/IOP.0000000000002308
13. Merriwether EN, Agalave NM, Dailey DL, et al. IL-5 mediates monocyte phenotype and pain outcomes in fibromyalgia. Pain. 2021;162(5):1468–1482. doi:10.1097/j.pain.0000000000002089
14. Wen S, Jiang Y, Liang S, Cheng Z, Zhu X, Guo Q. Opioids regulate the immune system: focusing on macrophages and their organelles. Front Pharmacol. 2022;12:814241. doi:10.3389/fphar.2021.814241
15. Zhao Y, Mu H, Zhang J, Lu Y. Efficacy and safety of flurbiprofen-axetil combined with nalbuphine pretreatment on remifentanil-induced postoperative hyperalgesia: a randomized clinical trial. Exp Ther Med. 2023;26(4):475. doi:10.3892/etm.2023.12174
16. Luo M, Han X, Li H, Zhou G, Chen H, Gao F. Effects of remifentanil gradual withdrawal combined with postoperative infusion on postoperative hyperalgesia in patients undergoing laparoscopic hysterectomy: a factorial design, double-blind, randomized controlled trial. Drug Des Devel Ther. 2024;18:583–595. doi:10.2147/DDDT.S451913
17. Wu Z, Yu J, Lin Q, et al. Effects of an intraoperative intravenous bolus dose of dexmedetomidine on remifentanil-induced postinfusion hyperalgesia in patients undergoing thyroidectomy: a double-blind randomized controlled trial. Anesth Analg. 2021;132(2):320–328. doi:10.1213/ANE.0000000000005003
18. Guignard B, Bossard AE, Coste C, et al. Acute opioid tolerance: intraoperative remifentanil increases postoperative pain and morphine requirement. Anesthesiology. 2000;93(2):409–417. doi:10.1097/00000542-200008000-00019
19. Hasan MS, Abdul Razak N, Yip HW, et al. Association between intraoperative remifentanil use and postoperative hyperalgesia in adolescent idiopathic scoliosis surgery: a retrospective study. BMC Anesthesiol. 2023;23(1):177. doi:10.1186/s12871-023-02127-8
20. Zhou XL, Wang Y, Zhang CJ, Yu LN, Cao JL, Yan M. COX-2 is required for the modulation of spinal nociceptive information related to ephrinB/EphB signalling. Eur J Pain. 2015;19(9):1277–1287. doi:10.1002/ejp.657
21. Wang M, Guo S, Zhang Y, Zhang Y, Zhang H. Remifentanil attenuates sepsis-induced intestinal injury by inducing autophagy. Bioengineered. 2021;12(2):9575–9584. doi:10.1080/21655979.2021.1997562
22. Ciechanowska A, Pawlik K, Ciapała K, Mika J. Pharmacological modulation of the MIP-1 family and their receptors reduces neuropathic pain symptoms and influences morphine analgesia: evidence from a mouse model. Brain Sci. 2023;13(4):579. doi:10.3390/brainsci13040579
23. Liao MF, Hsu JL, Lu KT, et al. Granulocyte Colony Stimulating Factor (GCSF) can attenuate neuropathic pain by suppressing Monocyte Chemoattractant Protein-1 (MCP-1) expression, through upregulating the early MicroRNA-122 expression in the Dorsal Root Ganglia. Cells. 2020;9(7):1669. doi:10.3390/cells9071669
24. Carvalho TT, Mizokami SS, Ferraz CR, et al. The granulopoietic cytokine granulocyte colony-stimulating factor (G-CSF) induces pain: analgesia by rutin. Inflammopharmacology. 2019;27(6):1285–1296. doi:10.1007/s10787-019-00591-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.