Back to Journals » Infection and Drug Resistance » Volume 12
Molecular typing revealed the emergence of pvl-positive sequence type 22 methicillin-susceptible Staphylococcus aureus in Urumqi, Northwestern China
Authors Yuan W, Liu J ![]() , Zhan Y, Wang L, Jiang Y, Zhang Y, Sun N
, Zhan Y, Wang L, Jiang Y, Zhang Y, Sun N ![]() , Hou N
, Hou N ![]()
Received 25 January 2019
Accepted for publication 21 May 2019
Published 20 June 2019 Volume 2019:12 Pages 1719—1728
DOI https://doi.org/10.2147/IDR.S202906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Wenchang Yuan,1,2,* Jianhua Liu,2,3,* Youchao Zhan,1,* Li Wang,2 Yanqiong Jiang,1 Yanling Zhang,1 Ning Sun,1,4 Ning Hou1,5
1Department of Clinical Laboratory, The Fifth Affiliated Hospital of Guangzhou Medical University, Guangzhou, 510700, People’s Republic of China; 2Department of Clinical Laboratory, General Hospital of Xinjiang Military Region, Urumqi 830001, People’s Republic of China; 3Department of Intensive Care Unit, the Fourth Hospital of Changsha, Changsha 410006, People’s Republic of China; 4State Key Laboratory of Chemical Biology and Drug Discovery, and Department of Applied Biology and Chemical Technology, The Hong Kong Polytechnic University, Hung Hom, Kowloon, Hong Kong, People’s Republic of China; 5School of Pharmaceutical Sciences, Guangzhou Medical University, Guangzhou 511436, People’s Republic of China
*These authors contributed equally to this work
Background: Staphylococcus aureus is among the most common causes of health care- and community-associated infections worldwide. The distributions of different S. aureus clones change over time and also vary geographically. The purpose of this study was to determine the molecular type and antimicrobial resistance profiles of clinical S. aureus strains isolated in Urumqi, Northwestern China.
Methods: A total of 605 clinical S. aureus isolates were collected from Xinjiang Military General Hospital, in Urumqi. Protein A-encoding (spa) typing, multilocus sequence typing, staphylococcal chromosomal cassette mec typing, Panton-Valentine leucocidin (pvl) gene detection, and antimicrobial resistance profiling were performed.
Results: Among these strains, 271 isolates (44.7%) were methicillin-resistant S. aureus (MRSA) and 334 (55.3%) were methicillin-susceptible S. aureus (MSSA). The MRSA strains consisted of 22 spa types and 14 sequence types (STs). ST239-MRSA-III-t030 (73.1%, 198/271) and ST59-MRSA-IV-t437 (11.8%, 32/271) were the most common, and ST22-MRSA-IV-t309 was the rarest (2.02%, 6/271). The MSSA strains consisted of 93 spa types and 29 STs. ST22, ST121, ST398, ST5, ST7, ST188, and ST15 were the main MSSA STs, and ST22-MSSA-t309 was most common (26.0%, 87/334). The pvl gene was present in 20.3% of all S.aureus strains, and 80.8% (88/99) of ST22-MSSA strains harbored the pvl gene. A total of 85.7% pvl-positive ST22-MSSA strains were spa t309 (85/99), and 87.5% of pvl-positive ST22-MSSA strains were from abscesses or wounds (skin and soft tissue infections). All ST239-MRSA strains were resistant to gentamicin (GEN), levofloxacin (LEV), ciprofloxacin (CIP), moxifloxacin (MXF), rifampicin (RIF), and tetracycline (TET). Among the ST59-MRSA strains, over 70.0% were resistant to erythromycin (ERY), clindamycin (CLI), and TET. ST22-MSSA remained susceptible to most antibiotics, but was resistant to PEN (97.0%), ERY (57.6%), and CLI (15.2%).
Conclusion: Our major results indicated that the antimicrobial resistance profiles and pvl genes of S. aureus isolates from Urumqi were closely associated with clonal lineage. ST239-MRSA-III-t030 and pvl-positive ST22-MSSA-t309 were the most common clones in this region of Northwestern China.
Keywords: Staphylococcus aureus, methicillin-sensitive Staphylococcus aureus, methicillin-resistant Staphylococcus aureus, pvl gene, molecular typing
Introduction
Staphylococcus aureus is a potentially dangerous human pathogen that can cause a variety of diseases from skin and soft tissue infections (SSTIs) to systemic infections, such as pneumonia, bacteremia, sepsis, osteomyelitis, and endocarditis.1–3 Since the first report of methicillin resistant S. aureus (MRSA) in the United Kingdom in 1961, the number of MRSA infections has increased rapidly worldwide. MRSA strains are frequently resistant to many different classes of antibiotics owing to the acquisition of the staphylococcal cassette chromosome mec (SCCmec) element. To mediate methicillin resistance, the SCCmec element has to harbor the mecA gene encoding an additional penicillin-binding protein (PBP2A), which has very low affinity for β-lactam antibiotics.4 Understanding the genotypic characteristics of the predominant strains and their antibiotic resistance profiles is helpful to prevent and control the spread of S. aureus. Our previous studies indicated that ST5-MRSA-SCCmec II and ST239-MRSA-SCCmec III were prevalent in most hospitals in China.5 Moreover, ST398, ST7, ST1, ST59, and ST5 were the most prevalent sequence types (STs) among the MSSA isolates.6 Panton-Valentine leukocidin (PVL) is an important exotoxin of S. aureus; it can cause leukocytolysis and tissue necrosis, and has been found to be associated with pneumonia and SSTIs.7
Very few recent studies have examined the molecular epidemiology of S. aureus in Northwestern China. Our general purpose was to provide an initial characterization of the epidemiological and antimicrobial resistance patterns of S. aureus isolates in Urumqi, Northwestern China. Based on our earlier work,5 we hypothesized that ST5-MRSA or ST239-MRSA would be the most common types of MRSA in this region. We also hypothesized that the antimicrobial resistance profiles and pvl genes of S. aureus isolates from Urumqi are associated with clonal lineage.
Materials and methods
Bacterial isolates and clinical data
A total of 605 nonduplicate S. aureus strains were collected between 2013 and 2017 from the Xinjiang Military General Hospital, a 1039-bed tertiary care center in Urumqi. Among the S. aureus isolates, 271 (44.7%) were identified as MRSA based on analysis of the femB and mecA genes.8 Strains for community-acquired (CA-) and hospital-acquired (HA-) S. aureus infections were differentiated as previously described.6,9
S. aureus isolates were obtained from individual patients hospitalized in various departments. The isolates were derived from diverse clinical specimens, including abscesses or wounds (n=353, 58.3%; MSSA =204, MRSA =149), respiratory tract secretions (n=176, 29.1%; MSSA =102, MRSA =74), blood (n=52, 8.6%; MSSA =17, MRSA =35), and other fluids (cerebrospinal fluid, urine, synovial fluid, and abdominal fluid: n=24, 4.0%; MSSA =11, MRSA =13).
Antibiotic susceptibility testing
The antibiotic susceptibilities of the S. aureus isolates were determined using the broth dilution method, according to the procedure recommended by the Clinical and Laboratory Standards Institute (CLSI).10 The antibiotics tested were penicillin G (PEN), cefoxitin (FOX), tetracycline (TET), erythromycin (ERY), gentamicin (GEN), vancomycin (VAN), teicoplanin (TEC), clindamycin (CLI), linezolid (LZD), rifampicin (RIF), levofloxacin (LEV), tigecycline (TGC), ciprofloxacin (CIP), moxifloxacin (MXF), quinupristin-dalfopristin (QDA), and trimethoprim-sulfamethoxazole (SXT). CLSI breakpoints were used for interpreting minimum inhibitory concentration. S. aureus ATCC 29213 was used as the standard strain.
spa typing
The variable region (X) of the spa gene of each S. aureus isolate was amplified using PCR as described by Shopsin et al11. The PCR products were sequenced and submitted to the Ridom Spa Server spa type database (
Multilocus sequence typing (MLST)
MLST typing of S. aureus isolates was performed by amplification and sequencing the internal fragments of seven housekeeping genes (arcC, aroE, glpF, gmk, pta, tpi, and yqiL) as previously described.12 The sequences were submitted to the MLST website for S. aureus (
SCCmec typing of MRSA strains
SCCmec typing was performed using a multiplex PCR assay to characterize the mec and ccr gene complexes as previously described.13 MRSA NCTC10442 (SCCmec I), MRSA N315 (SCCmec II), MRSA85/2082 (SCCmec III), MRSA JCSC 4744 (SCCmec IV), and MRSAWZ153 (SCCmec V) were provided by Prof. Fanyou Yu (Wenzhou Medical University) and used as reference standards for SCCmec typing.
pvl gene detection
The pvl genes of all S. aureus isolates were detected by PCR using the primers pvl-1 and pvl-2 as previously described.14 MW2 was used as a reference standard for pvl gene identification.
Statistical analysis
Student’s t-test for continuous variables and Chi-square or Fisher’s exact for categorical variables were used to calculate p values. A p-value below 0.05 was considered statistically significant. Statistical analysis was performed using SPSS 19.0. All susceptibility data and molecular test results were analyzed using WHONET software, version 5.6.
Results
Molecular typing of S. aureus isolates
We analyzed 605 S. aureus isolates. There were 164 (27.1%) community-acquired isolates (including 27 MRSA and 137 MSSA) and 441 (72.9%) isolates associated with health-care infections (including 244 MRSA and 197 MSSA). All S. aureus isolates were analyzed by MLST and spa typing (Tables 1 and 2).
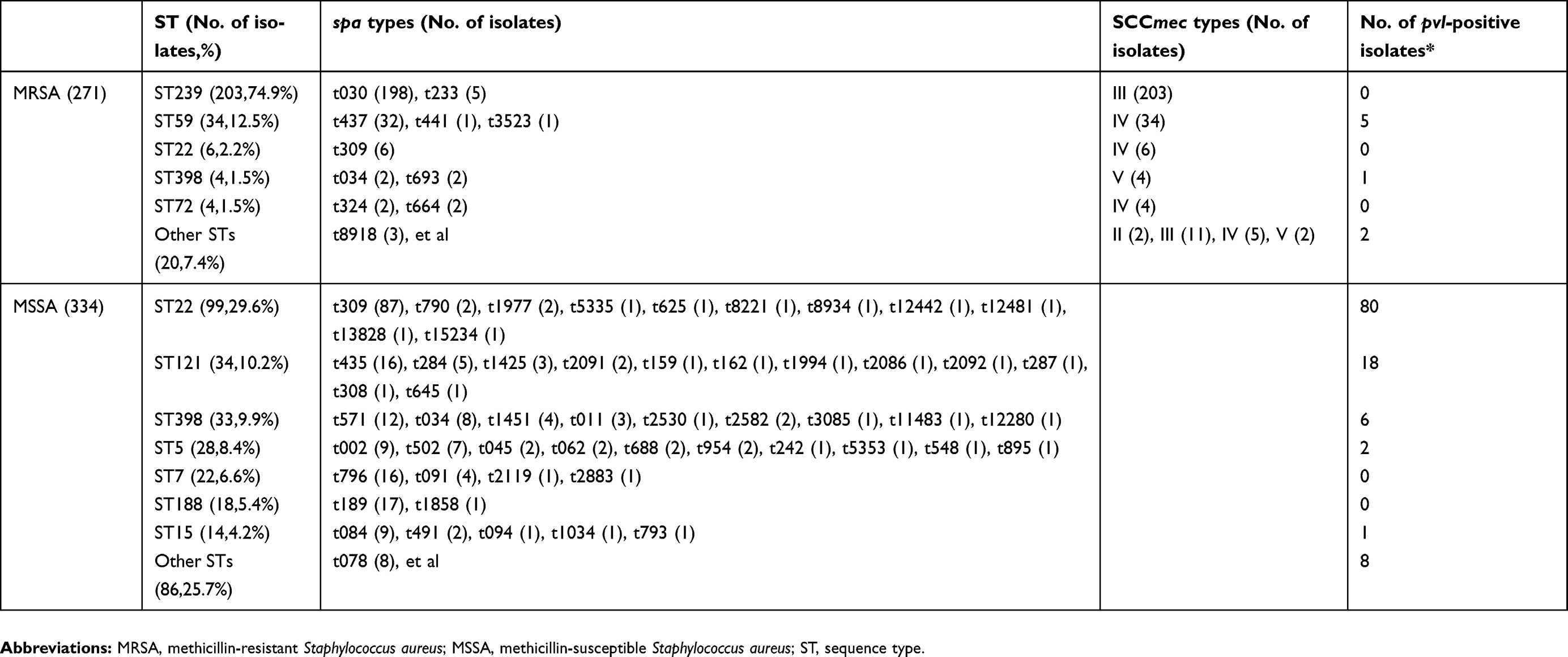 | Table 1 Molecular characteristics of 605 Staphylococcus aureus isolates from Urumqi, Northwestern China |
 | Table 2 Typing results for 605 Staphylococcus aureus isolated from Urumqi, Northwestern China |
There were 14 STs among the 271 MRSA isolates, and the most common clone was ST239 (74.9%, 203/271). This result is consistent with our initial hypothesis that ST239 would be a common strain. The second most common clone was ST59 (12.5%, 34/271).
There were 334 MSSA isolates and 29 STs (5 isolates were non-typable). The most common ST was ST22 (29.6%, 99/334), followed by ST121 (10.2%, 34/334), ST398 (9.9%, 33/334), ST5 (8.4%, 28/334), ST7(6.6%, 22/334), ST188 (5.4%, 18/334), and ST15 (4.2%%, 14/334).
There were 22 spa types among the MRSA isolates, and spa t030 (73.1%, 198/271) and spa t437 (11.8%, 32/271) were the most common. There were 93 spa types among the 271 MSSA isolates, and the five most prevalent were t309 (26.0%,87/334), t189 (5.1%,17/334), t796 (4.8%,16/334), t435 (4.8%,16/334), and t571 (3.6%,12/334).
SCCmec typing indicated that 214 MRSA isolates were SCCmec III and 49 were SCCmec IV; only 1 isolate was SCCmec I, 2 isolates were SCCmec II, and 5 isolates were SCCmec V. The most common ST among the MRSA SCCmec III isolates was ST239 (n=203), and the most common ST among SCCmec IV isolates was ST59 (n=34).
According to the MLST, spa, and SCCmec typing results, the most common clones among MRSA isolates were ST239-MRSA-III-t030 (73.1%, 198/271) and ST59-MRSA-IV-t437 (11.8%, 32/271). One SCCmec I isolate was classified as ST88 and 2 SCCmec II isolates were classified as ST5. The 5 isolates of SCCmec V were classified as ST398 (n=4) and ST630 (n=1). Interestingly, although the major spa type in China was t037, we detected no isolates of this type. Among the 203 ST239 isolates, 198 were spa t030 and five were spa t233. ST5 is also a major MRSA clone prevalent in China, however, only 6.7% of ST5 strains isolated were MRSA in our study. This result is contrary to our initial hypothesis that ST5 would be a common strain. ST1, ST5, ST8, ST22, ST25, ST30, ST59, ST398, ST630, ST641, and ST1289 were identified in both MSSA and MRSA isolates. Among MSSA strains, ST22-t309 (26.0%, 87/334), ST188-t189 (5.1%, 17/334), ST796-t796 (4.8%, 16/334), ST121-t435 (4.8%, 16/334), and ST398-t571 (3.6%, 12/334) were the most dominant clones, and accounted for 44.3% of the tested MSSA strains.
ST239 and ST59 were the predominant MRSA clones among each group of clinical specimens. ST22, ST121, and ST398 were the most common MSSA clones. The proportion of STs differed by clinical samples, but the dominant genotypes were ST239, ST59, ST22, and ST398. ST239 accounted for more than 60.0% of isolates from blood specimens. The distributions of MRSA and MSSA STs among the different specimens are shown in Figure 1. ST239 was the most common in blood samples whereas ST239, ST59, and ST22 were the most frequently found in specimens from abscesses/wounds, sputum, and other fluids. The globally disseminated hypervirulent clone ST121 was the main clone in abscess/wound samples. The proportions of ST239, ST59, ST22, ST398 and others differed by clinical department, ST239 was the predominant MRSA clones in all clinical departments (except pediatrics). As a CA-MRSA clone, ST59 was the most common ST clone in many clinical departments and was the predominant clone causing pediatric infections. ST22 is commonly reported as a MRSA clone in Europe and some Asian countries; however, in this study, most ST22 clones were MSSA, and only six ST22 MRSA isolates were found. ST22 was detected in most clinical departments and was responsible for abscess/wound, sputum, blood, and body fluid infections, suggesting that ST22 can cause both HA- and CA- infections.
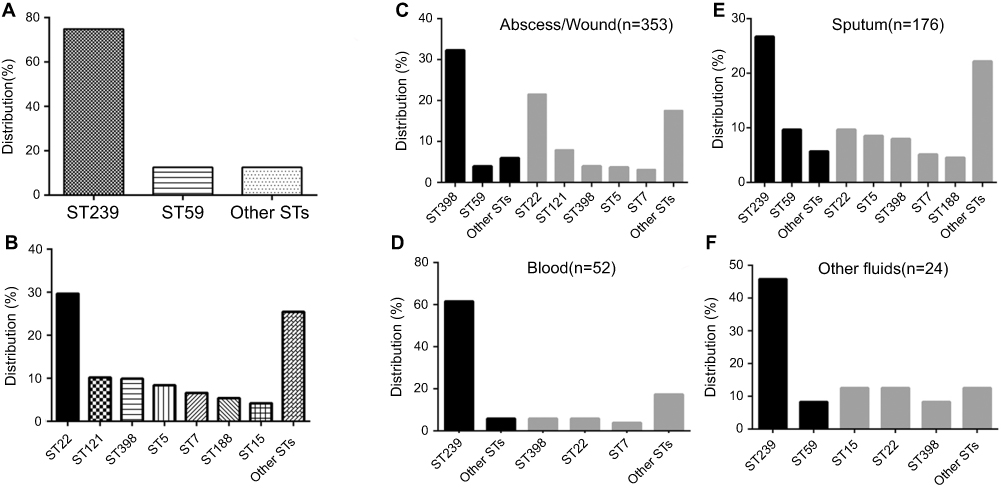 | Figure 1 Prevalence of Staphylococcus aureus STs among different clinical specimens. (A) Proportions of the two predominant MRSA sequence types, ST239 and ST59, among all S. aureus isolates. (B) Proportions of the predominant MSSA sequence types, ST22, ST398, ST121, ST5, ST7, ST188, and ST15, among all S. aureus isolates. (C) Distribution of STs in abscess/wound specimens. (D) Distribution of STs in blood specimens. (E) Distribution of STs in sputum specimens. (F) Distribution of STs in specimens of other fluids. (C–F: black bars indicate MRSA and grey bars indicate MSSA.).Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-susceptible Staphylococcus aureus; ST, sequence type. |
A total of 121 isolates (20.3%, 123/605) were positive for the pvl gene, including 8 MRSA (3.0%, 8/271) and 115 MSSA (34.4%, 115/334) isolates (Table 1). A total of 93.4% (113/121) of pvl-positive strains were from abscesses or wounds associated with SSTIs. The most common STs among pvl-positive isolates were ST22 (66.1%, 80/121), ST121 (14.9%, 18/121), ST59 (9.1%, 11/121), and ST239 (5.8%, 7/121). All of the 80 pvl-positive ST22 isolates were MSSA, and 72 were spa t309 (85.7%, 72/80). Seventy pvl-positive ST22-MSSA strains were from abscesses or wounds associated with SSTIs, five were from sputum specimens, two were from blood specimens, and three were from other fluid specimens.
Antimicrobial susceptibility testing
According to the results of antimicrobial susceptibility tests, all of the isolates were susceptible to VAN, LZD, TGC, and TEC (data not shown). For all S. aureus isolates, it was found that 95.4% were resistant to PEN, 63.6% of isolates were resistant to ERY, 44.8% were resistant to FOX, 44.3% were resistant to CLI, 42.1% were resistant to TET, 40.3% were resistant to GEN, 37.9% were resistant to CIP, 36.2% were resistant to LEV, 35.0% were resistant to MXF, and 7.6% of isolates were resistant to SXT. In addition, the resistance profiles of S. aureus isolates differed with respect to their STs. For ST239, all strains were resistant to PEN, FOX, GEN, LEV, CIP, MXF, RIF, and TET. Interestingly, 22.2% of ST239 strains were susceptible to ERY and CLI, and 77.8% were resistant to ERY and CLI. For the ST59 strains, more than 70.0% were resistant to PEN, FOX, ERY, CLI, and TET. The major MSSA clone ST22 was susceptible to most antibiotics and was only resistant to PEN (97.0%), ERY (57.6%), and CLI (15.2%) (Table 3). In general, the MRSA isolates were more resistant to each antibiotic (except SXT) than the MSSA isolates.
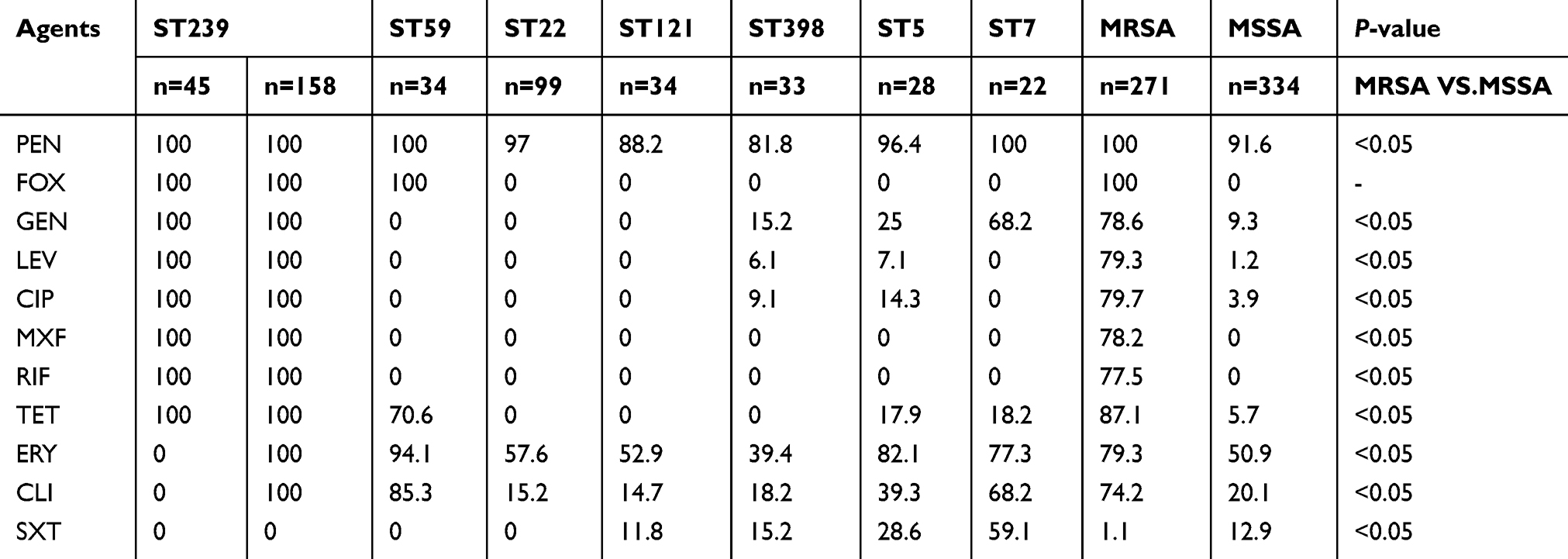 | Table 3 Antibiotic profiles of 605 Staphylococcus aureus isolated from Urumqi, Northwestern China |
Discussion
S. aureus usually undergoes clonal spreading within certain areas. Multiple molecular typing of S. aureus is an important tool in epidemiological studies because the results help to monitor and control staphylococcal infections. Here, we performed an initial comprehensive characterization of the genetic types and antimicrobial resistance profiles of S. aureus isolates in Urumqi, Northwestern China. These initial data suggest the prevalence of MRSA in Urumqi is 44.8%, lower than the mean prevalence rate of MRSA in China (59.8%).5 ST22-t309 was the predominant MSSA clone among all clinical S. aureus isolates. The distribution of MRSA clones seems geographically unique. ST239-III-t030, ST239-III-t037, ST59-IV-t437, and ST5-II-t002 were reported as the major MRSA clones in China.5,15 ST239-III-t030 was dominant in Beijing, followed by ST239-III-t037 and ST5-II-t002.16 ST5-II-t002 was the most common MRSA clone in Shanghai, followed by ST239-III-t037 and ST239-III-t030.17 A previous study in Northeastern China reported the most common MRSA clones were ST5-II-t002 and ST239-III-t030 among HA- and CA-MRSA isolates.9
Our findings suggest that ST239-III-t030 and ST59-IV-t437 were the predominant types of MRSA isolates in Urumqi. Only two ST5-MRSA-II-t002 strains were detected among 271 MRSA isolates, and ST239-III-t037 was not detected. ST239 originated in European countries and has become one of the most widely disseminated MRSA clones in many Asian countries, especially China.18,19 ST239 with the SCCmec type III is the most common MRSA clone in China, and is responsible for more than 50% of MRSA infections.15 It was reported that ST239 is mainly associated with spa t030 and spa t037 types. A comparison of genome phylogeny with spa typing suggested that spa t037 represents the ancestral ST239 spa type, which is distributed worldwide;20 the spa t030 type was only reported in Turkey and the Czech Republic.
Whole-genome sequencing of representative spa t037 strains from Hong Kong and spa t030 strains from Beijing revealed that spa t037 belongs to the traditional Asian clade; in contrast, t030 is clustered closely with strains of the “Turkish clade” from Eastern Europe.21 In China, the first patient with spa t030 MRSA was found in the intensive care unit of Peking Union Medical College Hospital in 2000.22 Since then, the t030 clone has spread rapidly throughout area hospitals and has gradually replaced the spa t037 clone to become the predominant MRSA clone in Beijing. A survey conducted using isolates collected from seven tertiary care hospitals at distinct geographical locations during 2014 revealed that ST239-t030 accounted for 80.1% of the tested MRSA isolates; in contrast, ST239-t037 accounted for only 4% of these isolates.23 These results suggest that spa t030 has successfully replaced spa t037 as the most common MRSA clone in China. A comparative matched pairs study of spa types t037 and t030 found that low fitness cost and characteristic drug resistance phenotype facilitated ST239-III-t030 strains to become the predominant clone in Chinese hospitals.24 However, no spa t037 strains were identified among 203 ST239 isolates studied in this study. Although our results are only from a single hospital, it is possible that spa t030 has completely replaced t037 in Urumqi. In addition, we demonstrated that 77.8% of spa t030 strains showed 100% resistance to eight non-β-lactam antimicrobial agents (GEN, CIP, CLI, MXF, RIF, ERY, TET, and LEV), and 22.2% of t030 strains were susceptible to ERY and CLI. The erm (ermA, ermB, ermC) genes encode products responsible for ERY and CLI resistance in S. aureus isolates. Mutations in the coding or promoter regions of erm genes might contribute to the discordance between phenotype and genotype in some MRSA strains.9,25
ST59 is associated with the spread of CA-MRSA, which is prevalent in the Asia Pacific area, and was recently identified in Europe.26,27 There is geographical difference among the subclones of ST59. In Western Australia, ST59-t437-V and ST59-t976-IV are the predominant clones, whereas in Taiwan and Hong Kong, ST59-t437-V is the most common.28–30 A multicenter study of CC59 MRSA isolates from children in mainland China confirmed that ST59-t437-IV is the predominant clone in CC59 strains among children.31 We found that ST59 was present CA- and HA-MRSA isolates. It was not only the main clone causing pediatric infections but also an important infection-causing clone in other clinical departments, such as burn medicine and neurosurgery. Thus, our results suggest that there is no clear distinction of strain types between CA-and HA-MRSA. In China, some reports pointed out that ST59 clone has already been introduced into hospitals and causes hospital-associated infections.31–33 A number of reports have speculated that CA-MRSA will gradually replace HA-MRSA in future because of the smaller SCCmec element in CA-MRSA may result in increasing adaptability and shortening doubling time as compared with HA-MRSA.34,35 Li et al reported that the population structure of S. aureus causing bacteremia has changed over the past several years in China. The prevalence of ST239-MRSA has significantly decreased and ST59-t437-MRSA has increased from 2013 to 2016 among all MRSA isolates.36 However, our data suggest that ST239-MRSA is still the most common clone responsible for bacteraemia. Thus, at least at our study hospital, there was no trend of a decline in bacteraemia-associated ST239-MRSA, in contrast to other Chinese cities.36
Our initial data indicated the MSSA isolates from Urumqi were genetically diverse, with seven major STs (ST22, ST398, ST121, ST5, ST7, ST188, and ST15) and five major spa types (t309, t189, t796, t435, and t571). Several of these types (ST121, ST398, ST5, ST7, and ST188) have been previously characterized as the predominant molecular types of MSSA in some other cities of China.6,37,38 ST22 has been established as one of the main international STs of MRSA.39 However, ST22 has been detected in MSSA strains from several cities of China. Before 2013, no ST22 clones were reported in China, but ST22 was the most prevalent genotype among MSSA isolates in Chongqing (11.3%) and Beijing (18.2%).38 Our results confirm that ST22 strains (29.6%, 99/334) are the most common group among MSSA isolates in Urumqi. The isolation of ST22 commonly from secretions, blood, sputum, and other body fluids associated with community and nosocomial infections. An investigation of the clinical and molecular epidemiology of S. aureus isolated from pediatricians in Beijing showed that ST22-MSSA was the most predominant ST in community and nosocomial infections in that city.38
Our study found that ST22-MSSA remained sensitive to most antibiotics; 97.0% of isolates were resistant to PEN, 57.6% were resistant to ERY, 15.2% of isolates were resistant to CLI, which is lower than that reported in previous studies.9 This may suggest some differences among ST22 clones from different regions, and the need for further multicenter investigations on the prevalence of the ST22 clone in China. ST398 and ST188 are usually associated with livestock-associated infections among animals and farm workers in many countries.40,41 ST188 is currently found as a common clone among patients with S. aureus SSTIs in Shanghai, Beijing, and Jiangsu in China.6,42,43 We isolated 33 ST398-MSSA and 4 ST398-MRSA strains from various types of samples. Our initial results indicate they were the most common clones in the departments of nephrology, geriatric medicine, neurosurgery, maxillofacial surgery, and pediatrics. This result may indicate that ST398 has become the major prevalent clone in Urumqi. ST188 has a high rate of colonization in the nasal cavity of healthy people and animals and it may cause infection in various animals. In this study, we detected 17 ST188 isolates in 334 MSSA strains and found that all of the ST188 isolates were spa t189. A previous investigation showed that spa t189 was the most common spa type found among healthy nasal carriers in Northern China.44 Livestock-associated clone ST398 and ST188 are the most prevalent in Urumqi. It is probably because a great number of people who live in this area are engaged in livestock husbandry or related activities.ST121 is mainly distributed in Africa, Asia, and Europe and has been characterized as a hypervirulent clone causing SSTIs.2,45 In the present study, all ST121 clones were MSSA isolates. ST121 was the second most common clone in MSSA infections. In agreement with the results of other studies, we found that 82.4% (28/34) of ST121 clones were isolated from abscesses or wounds.
The presence of the pvl gene in S. aureus strains is associated with abscess formation and tissue necrosis and can enhance inflammatory responses and local infections.46 The pvl-positive strains more often caused SSTI and are comparatively rare in invasive disease.47 Our results indicated the PVL protein was present in MRSA isolates and MSSA isolates. A previous investigation of MRSA from inpatients in China found that 28.6% of isolates were pvl–positive.7 Several other recent studies also showed that about 10% of MRSA isolates were pvl-positive.2,48 Our results showed that only 3.0% of MRSA isolates were pvl-positive, which is very different from these other studies.2,48 However, 34.4% of our MSSA isolates harbored the pvl gene, similar to the prevalences reported by recent studies in Chongqing.38
Our results showed that 93.4% of pvl-positive strains were isolated from abscess/wound specimens associated with SSTIs. We found that a great number of ST22 MSSA strains (80.8%) harbored the pvl gene, similar to the prevalences of pvl as in ST22 MSSA strains isolated from Chongqing (71.4%, 10/14) and Beijing (100%, 6/6). Further investigation of the roles of pvl-positive ST22 isolates using a large collection of MSSA isolates is proposed. In this study, six ST22-MRSA-IV strains were pvl-negative, which is same as a previous study of ST22 in Europe where most strains were pvl negative. However, a recent study showed that pvl-positive CC22-MRSA-IV variant strains are the dominant epidemic (EMRSA-15) variants in Kuwaiti hospitals.49
In conclusion, we performed a comprehensive molecular characterization of S. aureus isolates collected over a 5-year period in a general hospital in Urumqi, Northwestern China. Our findings suggest that ST239-MRSA-t030 and pvl-positive ST22-MSSA-t309 were the most common clones among S. aureus isolates. This study provides the latest information on the molecular epidemiology of S. aureus in Urumqi and also provides a foundation for future epidemiological studies of S. aureus in Urumqi and elsewhere in Northwestern China.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (81401703, 81703333 and 81773720).
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work
Disclosure
The authors report no conflicts of interest in this work.
References
1. Reddy PN, Srirama K, Dirisala VR. An update on clinical burden, diagnostic tools, and therapeutic options of Staphylococcus aureus. Infect Dis (Auckl). 2017;10:1179916117703999. doi:10.1177/1179916117703999
2. Liu Y, Xu Z, Yang Z, Sun J, Ma L. Characterization of community-associated Staphylococcus aureus from skin and soft-tissue infections: a multicenter study in China. Emerg Microbes Infect. 2016;5(12):e127. doi:10.1038/emi.2016.119
3. Xiao Y, Wei Z, Shen P, et al. Bacterial-resistance among outpatients of county hospitals in China: significant geographic distinctions and minor differences between central cities. Microbes Infect. 2015;17(6):417–425. doi:10.1016/j.micinf.2015.02.001
4. DeLeo FR, Chambers HF. Reemergence of antibiotic-resistant Staphylococcus aureus in the genomics era. J Clin Invest. 2009;119(9):2464–2474. doi:10.1172/JCI38226
5. Cheng H, Yuan W, Zeng F, et al. Molecular and phenotypic evidence for the spread of three major methicillin-resistant Staphylococcus aureus clones associated with two characteristic antimicrobial resistance profiles in China. J Antimicrob Chemother. 2013;68(11):2453–2457. doi:10.1093/jac/dkt213
6. Zhao C, Liu Y, Zhao M, et al. Characterization of community acquired Staphylococcus aureus associated with skin and soft tissue infection in Beijing: high prevalence of PVL+ ST398. PLoS One. 2012;7(6):e38577. doi:10.1371/journal.pone.0038577
7. Hu Q, Cheng H, Yuan W, et al. Panton-Valentine leukocidin (PVL)-positive health care-associated methicillin-resistant Staphylococcus aureus isolates are associated with skin and soft tissue infections and colonized mainly by infective PVL-encoding bacteriophages. J Clin Microbiol. 2015;53(1):67–72. doi:10.1128/JCM.01722-14
8. Kobayashi N, Wu H, Kojima K, et al. Detection of mecA, femA, and femB genes in clinical strains of staphylococci using polymerase chain reaction. Epidemiol Infect. 1994;113(2):259–266. doi:10.1017/s0950268800051682
9. Sun DD, Ma XX, Hu J, et al. Epidemiological and molecular characterization of community and hospital acquired Staphylococcus aureus strains prevailing in Shenyang, Northeastern China. Braz J Infect Dis. 2013;17(6):682–690. doi:10.1016/j.bjid.2013.02.007
10.
11. Shopsin B, Gomez M, Montgomery SO, et al. Evaluation of protein A gene polymorphic region DNA sequencing for typing of Staphylococcus aureus strains. J Clin Microbiol. 1999;37(11):3556–3563.
12. Enright MC, Day NP, Davies CE, Peacock SJ, Spratt BG. Multilocus sequence typing for characterization of methicillin-resistant and methicillin-susceptible clones of Staphylococcus aureus. J Clin Microbiol. 2000;38(3):1008–1015.
13. Kondo Y, Ito T, Ma XX, et al. Combination of multiplex PCRs for staphylococcal cassette chromosome mec type assignment: rapid identification system for mec, ccr, and major differences in junkyard regions. Antimicrob Agents Chemother. 2007;51(1):264–274. doi:10.1128/AAC.00165-06
14. Lina G, Piemont Y, Godail-Gamot F, et al. Involvement of Panton-Valentine leukocidin-producing Staphylococcus aureus in primary skin infections and pneumonia. Clin Infect Dis. 1999;29(5):1128–1132. doi:10.1086/313461
15. Xiao M, Wang H, Zhao Y, et al. National surveillance of methicillin-resistant Staphylococcus aureus in China highlights a still-evolving epidemiology with 15 novel emerging multilocus sequence types. J Clin Microbiol. 2013;51(11):3638–3644. doi:10.1128/JCM.01375-13
16. Liu Y, Wang H, Du N, et al. Molecular evidence for spread of two major methicillin-resistant Staphylococcus aureus clones with a unique geographic distribution in Chinese hospitals. Antimicrob Agents Chemother. 2009;53(2):512–518. doi:10.1128/AAC.00804-08
17. Song Y, Du X, Li T, Zhu Y, Li M. Phenotypic and molecular characterization of Staphylococcus aureus recovered from different clinical specimens of inpatients at a teaching hospital in Shanghai between 2005 and 2010. J Med Microbiol. 2013;62(Pt 2):274–282. doi:10.1099/jmm.0.050971-0
18. Ko KS, Lee JY, Suh JY, et al. Distribution of major genotypes among methicillin-resistant Staphylococcus aureus clones in Asian countries. J Clin Microbiol. 2005;43(1):421–426. doi:10.1128/JCM.43.1.421-426.2005
19. Feil EJ, Nickerson EK, Chantratita N, et al. Rapid detection of the pandemic methicillin-resistant Staphylococcus aureus clone ST 239, a dominant strain in Asian hospitals. J Clin Microbiol. 2008;46(4):1520–1522. doi:10.1128/JCM.02238-07
20. Harris SR, Feil EJ, Holden MT, et al. Evolution of MRSA during hospital transmission and intercontinental spread. Science. 2010;327(5964):469–474. doi:10.1126/science.1182395
21. Wang Z, Zhou H, Wang H, et al. Comparative genomics of methicillin-resistant Staphylococcus aureus ST239: distinct geographical variants in Beijing and Hong Kong. BMC Genomics. 2014;15:529. doi:10.1186/1471-2164-15-529
22. Chen H, Liu Y, Jiang X, Chen M, Wang H. Rapid change of methicillin-resistant Staphylococcus aureus clones in a Chinese tertiary care hospital over a 15-year period. Antimicrob Agents Chemother. 2010;54(5):1842–1847. doi:10.1128/AAC.01563-09
23. Chen Y, Liu Z, Duo L, et al. Characterization of Staphylococcus aureus from distinct geographic locations in China: an increasing prevalence of spa-t030 and SCCmec type III. PLoS One. 2014;9(4):e96255. doi:10.1371/journal.pone.0096255
24. Shang W, Hu Q, Yuan W, et al. Comparative Fitness and Determinants for the Characteristic Drug Resistance of ST239-MRSA-III-t030 and ST239-MRSA-III-t037 Strains Isolated in China. Microb Drug Resist. 2016;22(3):185–192. doi:10.1089/mdr.2015.0226
25. Sekiguchi J, Hama T, Fujino T, et al. Detection of the antiseptic- and disinfectant-resistance genes qacA, qacB, and qacC in methicillin-resistant Staphylococcus aureus isolated in a Tokyo hospital. Jpn J Infect Dis. 2004;57(6):288–291.
26. Chen CJ, Huang YC, Su LH, et al. Molecular epidemiology and antimicrobial resistance of methicillin-resistant Staphylococcus aureus bloodstream isolates in Taiwan, 2010. PLoS One. 2014;9(6):e101184. doi:10.1371/journal.pone.0101184
27. Glasner C, Pluister G, Westh H, et al. Staphylococcus aureus spa type t437: identification of the most dominant community-associated clone from Asia across Europe. Clin Microbiol Infect. 2015;21(2):163 e161–168. doi:10.1016/j.cmi.2014.09.010
28. Coombs GW, Monecke S, Ehricht R, et al. Differentiation of clonal complex 59 community-associated methicillin-resistant Staphylococcus aureus in Western Australia. Antimicrob Agents Chemother. 2010;54(5):1914–1921. doi:10.1128/AAC.01287-09
29. Ho CM, Ho MW, Lee CY, Tien N, Lu JJ. Clonal spreading of methicillin-resistant SCCmec Staphylococcus aureus with specific spa and dru types in central Taiwan. Eur J Clin Microbiol Infect Dis. 2012;31(4):499–504. doi:10.1007/s10096-011-1338-3
30. Ho PL, Chuang SK, Choi YF, et al. Community-associated methicillin-resistant and methicillin-sensitive Staphylococcus aureus: skin and soft tissue infections in Hong Kong. Diagn Microbiol Infect Dis. 2008;61(3):245–250. doi:10.1016/j.diagmicrobio.2007.12.015
31. Li J, Wang L, Ip M, et al. Molecular and clinical characteristics of clonal complex 59 methicillin-resistant Staphylococcus aureus infections in Mainland China. PLoS One. 2013;8(8):e70602. doi:10.1371/journal.pone.0070602
32. Song Q, Wu J, Ruan P. Predominance of community-associated sequence type 59 methicillin-resistant Staphylococcus aureus in a paediatric intensive care unit. J Med Microbiol. 2018;67(3):408–414. doi:10.1099/jmm.0.000693
33. Peng H, Liu D, Ma Y, Gao W. Comparison of community- and healthcare-associated methicillin-resistant Staphylococcus aureus isolates at a Chinese tertiary hospital, 2012–2017. Sci Rep. 2018;8(1):17916. doi:10.1038/s41598-018-36206-5
34. Maree CL, Daum RS, Boyle-Vavra S, Matayoshi K, Miller LG. Community-associated methicillin-resistant Staphylococcus aureus isolates causing healthcare-associated infections. Emerg Infect Dis. 2007;13(2):236–242. doi:10.3201/eid1302.060781
35. David MZ, Daum RS, Bayer AS, et al. Staphylococcus aureus bacteremia at 5 US academic medical centers, 2008–2011: significant geographic variation in community-onset infections. Clin Infect Dis. 2014;59(6):798–807. doi:10.1093/cid/ciu410
36. Li S, Sun S, Yang C, et al. The changing pattern of population structure of Staphylococcus aureus from Bacteremia in China from 2013 to 2016: ST239-030-MRSA replaced by ST59-t437. Front Microbiol. 2018;9:332. doi:10.3389/fmicb.2018.00332
37. Li X, Fang F, Zhao J, et al. Molecular characteristics and virulence gene profiles of Staphylococcus aureus causing bloodstream infection. Braz J Infect Dis. 2018;22(6):487–494. doi:10.1016/j.bjid.2018.12.001
38. Yang Y, Hu Z, Shang W, et al. Molecular and phenotypic characterization revealed high prevalence of multidrug-resistant methicillin-susceptible Staphylococcus aureus in Chongqing, Southwestern China. Microb Drug Resist. 2017;23(2):241–246. doi:10.1089/mdr.2016.0078
39. Stefani S, Chung DR, Lindsay JA, et al. Meticillin-resistant Staphylococcus aureus (MRSA): global epidemiology and harmonisation of typing methods. Int J Antimicrob Agents. 2012;39(4):273–282. doi:10.1016/j.ijantimicag.2011.09.030
40. Ye X, Fan Y, Wang X, et al. Livestock-associated methicillin and multidrug resistant S. aureus in humans is associated with occupational pig contact, not pet contact. Sci Rep. 2016;6:19184. doi:10.1038/srep19184
41. Smith TC, Thapaliya D, Bhatta S, Mackey S, Engohang-Ndong J, Carrel M. Geographic distribution of livestock-associated Staphylococcus aureus in the United States. Microbes Infect. 2018;20(6):323–327. doi:10.1016/j.micinf.2018.05.004
42. Gu FF, Hou Q, Yang HH, et al. Characterization of Staphylococcus aureus isolated from non-native patients with skin and soft tissue infections in Shanghai. PLoS One. 2015;10(4):e0123557. doi:10.1371/journal.pone.0123557
43. Gu FF, Chen Y, Dong DP, et al. Molecular epidemiology of Staphylococcus aureus among patients with skin and soft tissue infections in two Chinese Hospitals. Chin Med J (Engl). 2016;129(19):2319–2324. doi:10.4103/0366-6999.190673
44. Yan X, Song Y, Yu X, et al. Factors associated with Staphylococcus aureus nasal carriage among healthy people in Northern China. Clin Microbiol Infect. 2015;21(2):157–162. doi:10.1016/j.cmi.2014.08.023
45. Rao Q, Shang W, Hu X, Rao X. Staphylococcus aureus ST121: a globally disseminated hypervirulent clone. J Med Microbiol. 2015;64(12):1462–1473. doi:10.1099/jmm.0.000185
46. Bocchini CE, Hulten KG, Mason EO
47. Shallcross LJ, Fragaszy E, Johnson AM, Hayward AC. The role of the Panton-Valentine leucocidin toxin in staphylococcal disease: a systematic review and meta-analysis. Lancet Infect Dis. 2013;13(1):43–54. doi:10.1016/S1473-3099(12)70238-4
48. Kong H, Fang L, Jiang R, Tong J. Distribution of sasX, pvl, and qacA/B genes in epidemic methicillin-resistant Staphylococcus aureus strains isolated from East China. Infect Drug Resist. 2018;11:55–59. doi:10.2147/IDR.S153399
49. Boswihi SS, Udo EE, Monecke S, et al. Emerging variants of methicillin-resistant Staphylococcus aureus genotypes in Kuwait hospitals. PLoS One. 2018;13(4):e0195933. doi:10.1371/journal.pone.0195933
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.