Back to Journals » Drug Design, Development and Therapy » Volume 19
Molecular Pharmacological Interventions for Endometrial Cancer: A Comprehensive Review
Authors Qin W, Qi Y, Li Q, Wang B, Wang J, Ge X, Li Y, Zhang X, Liu K
Received 21 February 2025
Accepted for publication 5 August 2025
Published 27 August 2025 Volume 2025:19 Pages 7381—7392
DOI https://doi.org/10.2147/DDDT.S524181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Wei Qin,1,* Yazhou Qi,2,* Qianwen Li,2,* Bei Wang,2,* Jingmiao Wang,3 Xueke Ge,3 Yanhong Li,4 Xinyue Zhang,4 Kuan Liu4
1Internal Medicine of Integrated Chinese and Western Medicine, Affiliated Hospital of Hebei University, Baoding, People’s Republic of China; 2Department of Gynecology, Affiliated Hospital of Hebei University, Baoding, People’s Republic of China; 3Department of Radiotherapy, Baoding First Central Hospital, Baoding, People’s Republic of China; 4Department of Radiotherapy, Affiliated Hospital of Hebei University, Baoding, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kuan Liu, Affiliated Hospital of Hebei University, No. 212 East Yuhua Road, Lianchi District, Baoding, Hebei, 071000, People’s Republic of China, Email [email protected] Xinyue Zhang, Affiliated Hospital of Hebei University, No. 212 East Yuhua Road, Lianchi District, Baoding, Hebei, 071000, People’s Republic of China, Email [email protected]
Abstract: Endometrial cancer, a common malignancy of the female reproductive system, has a rising incidence and complex clinical management due to its diverse molecular subtypes. This review examines the molecular mechanisms underlying EC, particularly the roles of the Bcl-2 family in apoptosis regulation and estrogen receptor signaling in tumor progression. We explore pharmacological interventions targeting these pathways, including BH3 mimetics and selective estrogen receptor modulators, which show promise but face challenges such as resistance and adverse effects. Additionally, we highlight the potential of natural compounds like curcumin, paclitaxel, and Ganoderma lucidum polysaccharides as adjunctive therapies, demonstrating efficacy in preclinical studies and early-phase clinical trials. This review aims to provide insights into the development of personalized therapeutic strategies for EC and to identify opportunities for optimizing clinical outcomes in future treatments.
Keywords: endometrial cancer, Bcl-2 family, estrogen receptors, natural polysaccharides, therapeutic interventions
Introduction
Endometrial cancer (EC) remains one of the most common gynecologic malignancies worldwide. Despite advances in surgical and adjuvant therapies, the prognosis for patients with high-risk or recurrent disease remains poor.1 Traditionally, EC treatment has been based on clinical and histopathological features; however, these approaches often fail to fully account for the molecular heterogeneity of the disease.2 Recent advances in molecular biology have led to the identification of distinct molecular subtypes of EC, which vary significantly in their prognosis and response to treatment.3 These molecular classifications, such as those described in the new molecular stratification system, underscore the necessity of shifting from traditional histological-based classifications to molecularly-informed approaches for personalized treatment.4 This shift is crucial, as it allows for more accurate predictions of disease behavior and therapeutic response.
Despite these advances, a clear knowledge gap exists in the integration of these molecular insights into routine clinical practice. While molecular markers have the potential to guide therapy, their clinical application remains limited due to a lack of standardized protocols and widespread adoption. This review aims to bridge this gap by synthesizing current molecular approaches in the treatment of EC, evaluating their potential to refine risk stratification, and tailoring therapeutic strategies to the individual patient’s molecular profile.
Background on EC
EC is a malignant tumor that originates from the uterine endometrial epithelium. It ranks among the three most common cancers of the female reproductive system and is the sixth most prevalent cancer worldwide. In recent years, the incidence of EC has been steadily increasing, particularly among younger women, and is strongly associated with metabolic syndrome factors such as obesity, diabetes mellitus, and hypertension.5
Clinically, EC is categorized into two main types: Type I and Type II. Type I EC accounts for over 80% of cases and is linked to excessive estrogen exposure. It typically occurs in premenopausal or early postmenopausal women and is often characterized by low-grade, minimally invasive lesions with a more favorable prognosis, as seen in endometrial glandular cancer.6 In contrast, Type II EC makes up 10% to 20% of cases, is not associated with estrogen, and is most frequently diagnosed in late postmenopausal women.7 This type tends to be high-grade, highly invasive, and is associated with a poorer prognosis, as seen in endometrial infiltrative carcinoma, serous carcinoma, or clear cell carcinoma.
Overview of Molecular Subtypes
Based on the molecular characteristics of EC, it can be categorized into four molecular subtypes:8 (1) Microsatellite instability-high (MSI-H) subtype, accounting for approximately 30%, associated with the inactivation of mismatch repair genes (MMR), predominantly observed in Type I EC, and typically characterized as low-grade, minimally invasive, with a favorable prognosis, similar to endometrial glandular carcinoma; (2) Microsatellite stable/low copy number variation (MSS/low CNV) subtype, accounting for about 40%, linked to mutations or deletions in the PTEN gene, commonly seen in Type I EC, and often characterized as low-grade, minimally invasive, with a positive prognosis, resembling endometrial glandular carcinoma; (3) High copy number variation/p53 mutant (high CNV/p53 mutant) subtype, comprising 10%-20%, correlated with mutations or deletions in the p53 gene, largely detected in Type II EC, frequently manifested as high-grade, highly invasive, with an adverse prognosis, similar to endometrial infiltrative carcinoma, serous carcinoma, or clear cell carcinoma; (4) High copy number variation/POLE mutant (high CNV/POLE mutant) subtype, making up about 10%, connected to mutations in the DNA polymerase ε (POLE) gene, mainly encountered in Type I EC, and largely characterized as low-grade, minimally invasive, with a promising prognosis, reminiscent of endometrial glandular carcinoma.
Traditional Pharmacological Interventions
Currently, therapeutic interventions for EC primarily include surgical procedures, radiotherapy, and pharmacological treatments. For patients with early-stage EC, hysterectomy remains the gold-standard procedure, with a five-year survival rate exceeding 95%. However, for those with advanced or recurrent EC, the risk of surgical complications is elevated, often rendering surgery impractical and resulting in a five-year survival rate of less than 20%.9 As a result, pharmacological interventions become the cornerstone of clinical treatment for patients who are either surgically ineligible or choose to forgo surgery. These pharmaceutical treatments primarily consist of hormone therapy, chemotherapy, and targeted therapies. Hormone therapy utilizes progestogens or anti-estrogenic agents to counteract estrogen-driven EC growth and carcinogenesis.10 Chemotherapy uses agents such as taxanes, platinum compounds, or anthracyclines to inhibit EC cell proliferation and induce apoptosis. Targeted therapies employ inhibitors of the epidermal growth factor receptor (EGFR), vascular endothelial growth factor (VEGF), mammalian target of rapamycin (mTOR), and other targeted pathways to block EC cell signaling. The current advancements and challenges in EC treatment are illustrated in Figure 1.
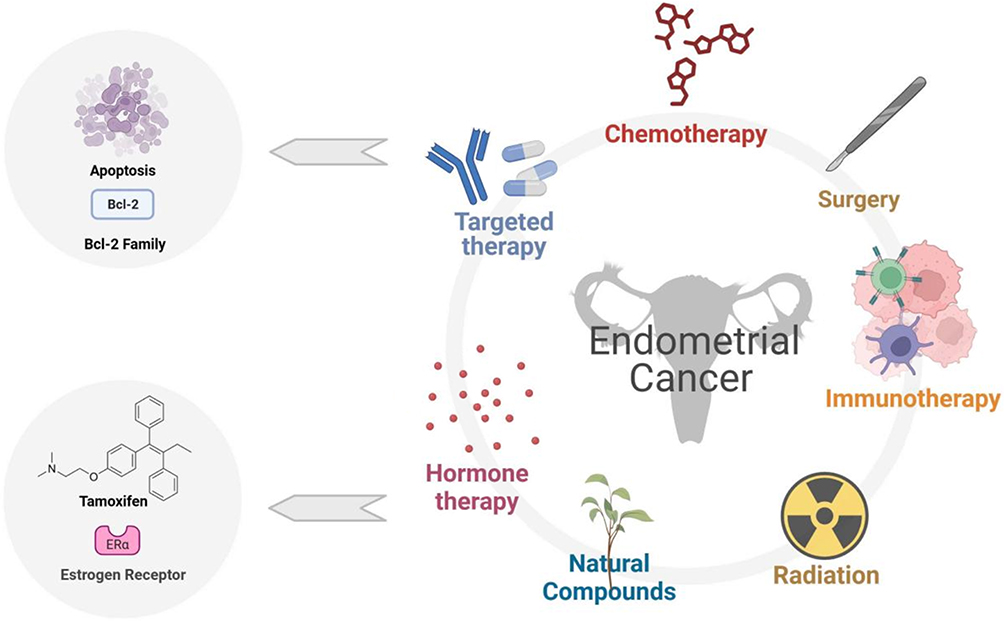 |
Figure 1 Current and emerging therapeutic strategies for endometrial cancer (EC).This figure systematically summarizes six major treatment modalities and their mechanisms: immunotherapy (eg, anti-PD-1/PD-L1 antibodies reactivating T-cell-mediated tumor killing), chemotherapy (paclitaxel/carboplatin inducing apoptosis via DNA damage or microtubule disruption), surgery (primary intervention for early-stage EC with limited efficacy in advanced cases), hormone therapy (tamoxifen modulating ERα activity in a tissue-specific manner), targeted therapy (BH3 mimetics like Venetoclax inhibiting Bcl-2, and mTOR/PI3K inhibitors blocking pro-survival signaling), and natural compounds (Ganoderma lucidum polysaccharides and curcumin synergizing with conventional therapies by regulating p53/Bcl-2 and NF-κB pathways). Arrows indicate potential combination strategies, such as combining immunotherapy with targeted therapy to overcome resistance. |
Chemotherapy and Its Limitations
Chemotherapy involves the use of cytotoxic drugs to eliminate cancer cells or inhibit their growth. It can be administered as a monotherapy or in combination with other agents, depending on the type and stage of EC. Chemotherapy can be delivered via various routes, including oral, intravenous, intramuscular, subcutaneous, or intraperitoneal administration. It may be given preoperatively (neoadjuvant) to shrink tumors and facilitate their removal, or postoperatively (adjuvant) to reduce the risk of recurrence.11 Additionally, chemotherapy can serve as a palliative treatment to alleviate symptoms and improve the quality of life for patients with advanced or metastatic EC.12
Despite its therapeutic benefits, chemotherapy has several limitations. First, it lacks selectivity, which means it can damage normal, healthy cells along with cancer cells, leading to various side effects such as nausea, vomiting, hair loss, fatigue, anemia, infections, and neuropathy. Second, chemotherapy can induce resistance in cancer cells, making them less responsive to subsequent treatments. Third, chemotherapy may increase the risk of developing secondary cancers or other diseases due to its mutagenic and immunosuppressive effects.13 Finally, chemotherapy may be less effective for certain subtypes of EC.14
Hormone Therapy and Targeted Treatments
Hormone therapy involves the use of drugs that interfere with the production or action of hormones that promote the growth of hormone-dependent EC. It can be administered as a monotherapy or in combination with other drugs, depending on the type and stage of the cancer.15 Hormone therapy can be delivered via oral, intravenous, subcutaneous, or intramuscular routes.16 It may be used preoperatively or postoperatively to reduce the risk of recurrence, or as a palliative treatment for patients with advanced or metastatic EC.17
Hormone therapy is typically categorized into two main classes: selective estrogen receptor modulators (SERMs) and aromatase inhibitors (AIs). SERMs are drugs that bind to estrogen receptors (ERs) and block their activity in certain tissues (such as the breast) while activating them in others (such as bone).18 AIs, on the other hand, inhibit the enzyme aromatase, which converts androgens to estrogens in peripheral tissues.19 Examples of SERMs include tamoxifen and raloxifene, while examples of AIs include anastrozole, letrozole, and exemestane. Hormone therapy can be effective in patients with low-grade or hormone receptor-positive EC. However, it may also cause side effects such as weight gain, fluid retention, mood swings, hot flashes, and bone loss.
Targeted Treatments
Targeted treatments are therapies designed to target specific molecules or pathways involved in the growth and survival of cancer cells. These treatments can be administered as monotherapies or in combination with other drugs, depending on the type and stage of EC. Targeted therapies can be delivered orally, intravenously, subcutaneously, or intramuscularly. They may be used either before or after surgery to reduce the risk of recurrence or as a palliative treatment for patients with advanced or metastatic EC.
Targeted therapies utilize drugs that focus on specific molecules or pathways integral to the proliferation and survival of cancer cells.20 These include tyrosine kinase inhibitors (eg, sorafenib or pazopanib), mammalian target of rapamycin (mTOR) inhibitors (eg, everolimus or temsirolimus), angiogenesis inhibitors (eg, bevacizumab),21 and poly (ADP-ribose) polymerase (PARP) inhibitors (eg, olaparib or rucaparib). Targeted therapy can be particularly effective for patients with specific genetic mutations or biomarkers that render their cancer cells sensitive to these agents. However, targeted therapies may also induce side effects such as rash, diarrhea, hypertension, fatigue, or bleeding.
Immunotherapy and Its Potential
Immunotherapy involves the use of drugs that stimulate the immune system to recognize and attack cancer cells.22 These therapies include immune checkpoint inhibitors (eg, pembrolizumab or nivolumab), which block the signals that normally prevent the immune system from attacking cancer cells,23 and adoptive cell transfer (eg, chimeric antigen receptor [CAR] T-cell therapy), which entails genetically modifying the patient’s own immune cells to target specific antigens on cancer cells. Immunotherapy has shown efficacy in patients with high tumor mutational burden or mismatch repair deficiency. However, it can also lead to side effects, including inflammation of various organs (such as the lungs, liver, kidneys, or thyroid), autoimmune reactions, or cytokine release syndrome.
Role of Apoptosis in EC
Apoptosis and BCL-2 Family
Apoptosis is a highly regulated process of programmed cell death, essential for maintaining tissue homeostasis in multicellular organisms.24 Dysregulation of apoptosis is a hallmark of cancer progression, including EC, as it allows malignant cells to evade death and continue uncontrolled proliferation.25 Among the key regulators of apoptosis, the BCL-2 protein family plays a central role in governing mitochondrial outer membrane permeabilization (MOMP), a critical event in intrinsic apoptotic pathways.26
The BCL-2 family consists of both pro-apoptotic and anti-apoptotic members, classified based on their homology to the BCL-2 homology (BH) domains. Pro-apoptotic members include effectors (BAX, BAK, and BOK), which directly mediate MOMP, and BH3-only proteins (BIM, BID, PUMA, BMF, NOXA, BIK, BAD, and HRK), which function as sensors of cellular stress.27 Anti-apoptotic proteins, such as BCL-2, BCL-XL, MCL-1, BCL-W, and A1, sequester pro-apoptotic effectors, thereby preventing mitochondrial membrane disruption and inhibiting apoptosis (Figure 2).28
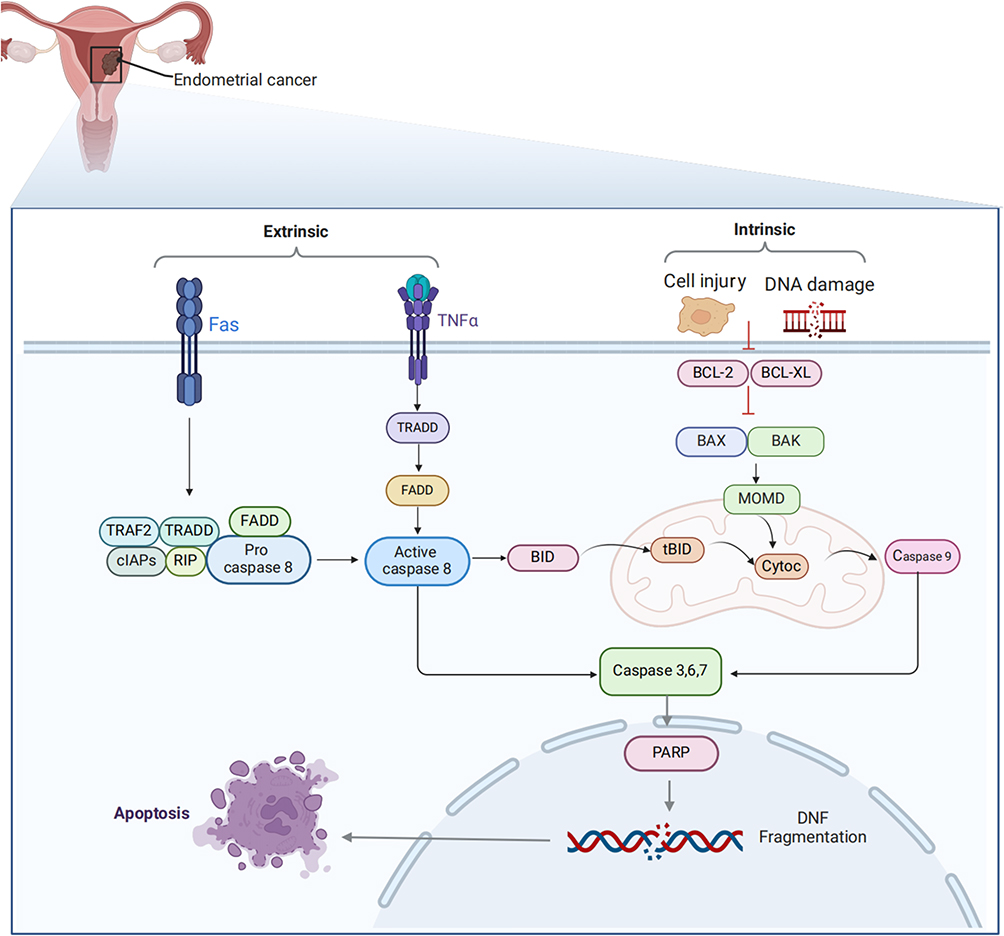 |
Figure 2 Intrinsic and extrinsic apoptosis pathways in EC.This figure details two apoptotic pathways: the extrinsic pathway triggered by death ligands (FasL/TNF-α) activating caspase-8 via the DISC complex, and the intrinsic pathway initiated by cellular stress (eg, DNA damage) through Bcl-2 family proteins (pro-apoptotic Bax/Bak vs anti-apoptotic Bcl-2/Bcl-xL) regulating mitochondrial outer membrane permeabilization (MOMP), leading to cytochrome c release and caspase-9 activation. The pathways connect via caspase-8 cleavage of Bid to generate tBid. This mechanism explains apoptosis resistance due to Bcl-2 overexpression in EC and the therapeutic potential of BH3 mimetics (eg, ABT-199) in restoring apoptotic balance by inhibiting Bcl-2. |
In EC, alterations in the expression of BCL-2 family proteins are frequently observed. Overexpression of BCL-2 and BCL-XL has been associated with chemoresistance, tumor invasion, and poor prognosis.29 Conversely, downregulation of pro-apoptotic members like BAX and PUMA reduces apoptotic signaling, thereby promoting cancer progression.30 Additionally, certain genetic polymorphisms or epigenetic modifications in BCL-2 family genes have been reported to influence the susceptibility to or outcomes of EC.31
Role of Bcl-2 and Bax in Apoptosis
The Bcl-2 family consists of proteins that regulate apoptosis, including pro-apoptotic members such as Bax and Bak, and anti-apoptotic counterparts like Bcl-2 and Bcl-xL. This family plays a pivotal role in the modulation of cell death by influencing mitochondrial membrane permeability, leading to the release of factors like cytochrome c, which activates the caspase pathway and subsequently results in cellular demise.32 Bcl-2 and Bax are among the most crucial members of the family. Their role in regulating apoptosis involves the formation of either homodimers or heterodimers. The balance between Bcl-2 and Bax determines cellular fate—whether the cell survives or undergoes death. A higher Bcl-2/Bax ratio inhibits apoptosis, while a lower ratio promotes it.33
EC is a prevalent gynecological malignancy, and its onset and progression are influenced by various factors, one of which is dysregulated apoptosis. Studies have shown that in EC tissues, Bcl-2 expression levels are significantly higher compared to normal endometrial tissues, while Bax expression levels are markedly lower. This imbalance results in an elevated Bcl-2/Bax ratio, which inhibits apoptosis and promotes tumor growth and invasion.34
Therapeutic Strategies
Two primary therapeutic strategies target the Bcl-2 family: The first involves the use of small molecule inhibitors or antagonists that interfere with the interactions between Bcl-2 family members, aiming to reduce the Bcl-2/Bax ratio and restore apoptosis. The second strategy employs gene therapy or RNA interference techniques to modulate the expression levels of Bcl-2 family members, either by increasing Bax or decreasing Bcl-2 expression, thereby inducing apoptosis.35
Therefore, targeting Bcl-2 family proteins may represent a promising strategy for the treatment of EC. Several drugs targeting the Bcl-2 family have shown encouraging results in clinical trials, including ABT-737, ABT-263 (Navitoclax), ABT-199 (Venetoclax), and AT101. These are BH3 mimetics that bind with high affinity and specificity to BCL-2, BCL-XL, and/or BCL-W, disrupting their interaction with pro-apoptotic proteins and thereby inducing apoptosis.36
Preclinical studies have demonstrated that ABT-737 exhibits potent antitumor activity against EC cell lines. However, its clinical application has been limited due to poor oral bioavailability and dose-limiting thrombocytopenia, which is caused by inhibition of Bcl-xL, a protein crucial for platelet survival.37 To overcome these limitations, ABT-263, an orally bioavailable analog of ABT-737, was developed. In Phase I clinical trials involving patients with advanced solid tumors, Navitoclax demonstrated partial responses in 3% of patients and stable disease in 26%. However, thrombocytopenia remained a major adverse effect, occurring in 40–60% of patients due to Bcl-xL inhibition.38 This thrombocytopenia necessitated dose adjustments, which ultimately limited the drug’s efficacy in clinical settings.
ABT-199 was developed to selectively target Bcl-2 while sparing Bcl-xL, thereby reducing the risk of thrombocytopenia. In Phase II clinical trials for chronic lymphocytic leukemia (CLL), Venetoclax achieved an overall response rate (ORR) of 79%, with complete remission in 20% of patients.39 In solid tumors, including EC, Venetoclax has shown promising preclinical results, although clinical data remain limited. Early-phase trials reported manageable side effects, including neutropenia and gastrointestinal symptoms such as nausea and diarrhea.
AT101, a natural Bcl-2 inhibitor derived from gossypol, has been tested in phase II trials for solid tumors, including endometrial and ovarian cancers. In one trial, 13% of patients achieved stable disease, although no significant tumor regression was observed. Side effects included fatigue, nausea, and low-grade hematologic toxicity.40 While AT101 has shown limited efficacy as a monotherapy, its combination with other agents, such as chemotherapy or radiotherapy, is currently being explored for potential synergistic effects.
Role of ER in EC
Role of ER in Tumor Growth and Progression
Estrogen receptors (ERs) are nuclear transcription factors that mediate the effects of estrogen by binding to estrogen-responsive elements (EREs) on DNA, thereby activating or repressing the transcription of target genes. These genes regulate a wide range of biological processes, including cell proliferation, differentiation, and apoptosis.41 ERs play a crucial role in the initiation and progression of hormone-dependent cancers, including EC.42
In EC, ERs exhibit dual roles that depend on their subtype and expression levels. ERα, which is predominantly expressed in low-grade, estrogen-dependent Type I ECs, is associated with tumor differentiation and growth. In contrast, ERβ, expressed at lower levels, appears to counteract the oncogenic signaling mediated by ERα and is linked to reduced invasiveness. Dysregulated ER signaling promotes tumorigenic phenotypes, including enhanced cell cycle progression, angiogenesis, and evasion of apoptosis (Figure 3).43,44
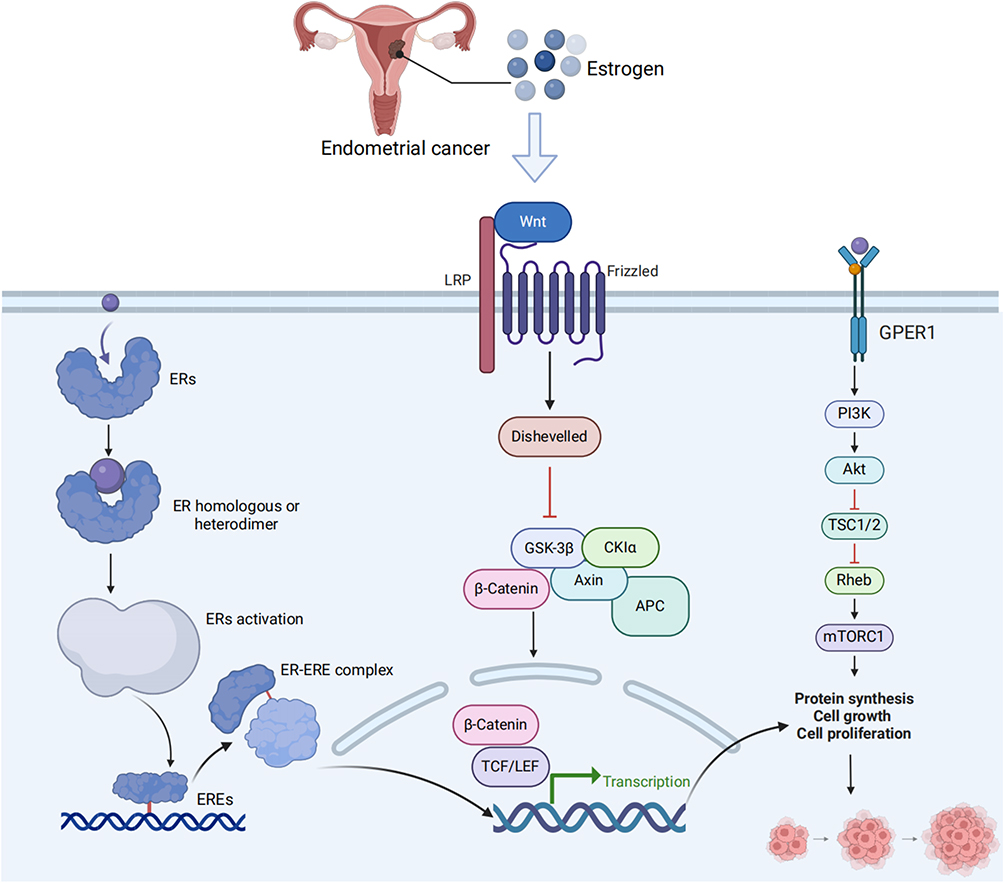 |
Figure 3 Estrogen receptor (ER) signaling and crosstalk with oncogenic pathways in EC.This figure comprehensively illustrates the molecular interplay between estrogen receptor (ER) signaling and key oncogenic pathways in endometrial cancer. The schematic depicts three interconnected networks: (1) Classical ER signaling involving receptor dimerization, ERE binding, and transcriptional regulation; (2) The canonical Wnt/β-catenin pathway initiated by LRP5/6-Frizzled receptor activation, progressing through GSK-3β/CK1α-mediated β-catenin stabilization and culminating in TCF/LEF-dependent transcription; and (3) GPER1-triggered PI3K/Akt/mTOR cascade leading to enhanced protein synthesis and proliferation via Rheb-mTORC1 activation. The diagram particularly highlights pathway crosstalk, including ER-mediated Wnt modulation and GPER1’s non-genomic PI3K activation, which collectively drive tumor progression through convergent regulation of cell cycle and survival mechanisms. These interactions provide mechanistic insights for current therapies (SERMs, mTOR inhibitors) and emerging targeted approaches (Wnt pathway inhibitors), while demonstrating the rationale for combination strategies that simultaneously target multiple signaling nodes in EC treatment. |
Notably, crosstalk between ER signaling and other oncogenic pathways, such as PI3K/AKT and Wnt/β-catenin, exacerbates EC progression. For example, estrogen-mediated activation of PI3K/AKT signaling promotes cell survival and inhibits apoptosis,45 while its interaction with BCL-2 family proteins further suppresses intrinsic apoptotic pathways.46 These findings highlight the importance of targeting ERs in EC therapy. Modulators such as Tamoxifen and aromatase inhibitors show promise, although their dual effects in different tissues require careful therapeutic planning.
Tamoxifen as an ER Modulator
Tamoxifen is a selective estrogen receptor modulator (SERM) that can function as either an antagonist or an agonist of ER, depending on the tissue or cellular context. Initially used for the endocrine treatment of breast cancer, Tamoxifen blocks ER signaling in breast cells, thereby inhibiting tumor growth. However, in endometrial cells, Tamoxifen exhibits estrogenic effects, promoting cell proliferation and differentiation. This dual action complicates and makes the application of Tamoxifen in EC both complex and controversial.16
Clinical Implications of ER-Targeted
Although there is a potential risk of Tamoxifen promoting tumor growth in EC, it remains an effective treatment option in certain situations. For example, in young patients who wish to preserve fertility and have early-stage, ER-positive EC, Tamoxifen can be used as a conservative treatment, particularly when surgery or radio-chemotherapy is contraindicated or ineffective. Tamoxifen can help reduce tumor size, alleviate symptoms, and improve quality of life.47 Additionally, in patients with advanced or recurrent EC, Tamoxifen can serve as palliative care, potentially extending survival and relieving pain. However, the therapeutic efficacy of Tamoxifen varies among individuals, and resistance can develop over time. Therefore, personalized assessment, close monitoring, and potential combination with other treatments are necessary to optimize outcomes.48
The Role of Natural Compounds in the Treatment of EC
Therapeutic Potential of Natural Polysaccharides
Recent research has shown that certain natural compounds exhibit anti-EC activity, making them promising candidates for future therapeutic interventions. Natural polysaccharides, high molecular weight compounds composed of monosaccharides or multiple monosaccharides, are widely found in animals, plants, and microorganisms. These compounds demonstrate a range of biological activities, including immunomodulation, antioxidation, anti-inflammatory, and antitumor effects. Several natural polysaccharides have been shown to inhibit the proliferation of EC cells, induce apoptosis, suppress invasion and metastasis, regulate the cell cycle, and modulate various signaling pathways. For example, polysaccharides derived from Ganoderma lucidum (Reishi mushrooms) induce apoptosis in EC cells by activating the p53 and Bax/Bcl-2 signaling pathways.49 Polysaccharides from Lycium barbarum (Goji berries) inhibit both the proliferation and invasion of EC cells by suppressing the PI3K/Akt/mTOR signaling pathway.50 Additionally, polysaccharides from sea cucumbers reduce the migration of EC cells by downregulating the expression of MMP-2 and MMP-9.51
Mechanism of Action of Natural Compounds
Natural compounds are physiologically active small molecules extracted or synthesized from nature, including plant secondary metabolites, animal toxins, and microbial metabolites. Due to their diverse structures and functions, natural compounds can interact with various targets and pathways involved in tumor initiation and progression. Several natural compounds have been identified as effective in inhibiting the growth and transformation of EC cells or enhancing their sensitivity to radiotherapy and chemotherapy. For example, shikonin, derived from the Lithospermum species, inhibits the proliferation and metabolism of EC cells by activating the AMPK signaling pathway.52 Emodin, derived from the Rheum species (rhubarb), induces apoptosis in EC cells by triggering the ER stress response.53 Curcumin, extracted from Curcuma species (turmeric), enhances the sensitivity of EC cells to cisplatin by modulating the NF-κB signaling pathway.54
Clinical Trials and Results of Treatment Regimens Based on Natural Compounds
Currently, several treatment regimens based on natural compounds are undergoing clinical trials to assess their safety and efficacy in treating EC. Some of these regimens have shown promising results.
Paclitaxel, a natural diterpene compound extracted from the yew tree (Taxus spp)., stabilizes microtubule assembly and inhibits cell division, thereby inducing tumor cell apoptosis. In a Phase III clinical trial targeting recurrent or metastatic EC, the combination of paclitaxel and carboplatin demonstrated significant efficacy. Results indicated that progression-free survival (PFS) was significantly longer in the combination group compared to the carboplatin-only control group (median PFS: 13.3 months vs 8.3 months, p < 0.001). Additionally, overall survival (OS) was improved (median OS: 29.5 months vs 23.7 months). However, adverse effects in the combination group were notable, with 58% of patients experiencing grade 3 or 4 neutropenia and peripheral neuropathy.55
Curcumin, a polyphenolic compound extracted from turmeric (Curcuma longa), is recognized for its anti-inflammatory and anticancer properties. In EC, curcumin enhances tumor cell sensitivity to cisplatin by inhibiting the NF-κB and PI3K/AKT/mTOR pathways. A phase I/II clinical trial evaluating curcumin as an adjunct to chemotherapy found that patients receiving curcumin achieved a disease control rate (DCR) of 67% at 6 months, significantly higher than the control group without curcumin (DCR: 47%, p < 0.05). Side effects were primarily gastrointestinal, including nausea and diarrhea, but overall tolerability was good.54
Ganoderma lucidum polysaccharides (GLPs), which act as immune modulators, induce cancer cell apoptosis by activating the p53 and Bax/Bcl-2 signaling pathways. In a phase II clinical trial involving 40 patients with advanced EC, GLPs alone achieved an objective response rate (ORR) of 15% and a disease stabilization rate (SDR) of 50%. While the monotherapy efficacy was limited, combining GLPs with radiotherapy or chemotherapy resulted in a synergistic effect, increasing the disease control rate to 75%. Adverse effects were mild, including fatigue and rash, with no serious toxic events reported.56
In summary, natural compounds show promise as potential treatments for EC. However, further investigation is required to better understand their mechanisms of action, optimize delivery methods, assess long-term effects, and evaluate safety profiles. In the future, the development of novel therapeutic interventions based on natural compounds may provide EC patients with more treatment options and improved quality of life.
Recent Advances and Future Directions
Ongoing Clinical Trials and Emerging Therapies
Several clinical trials are currently underway to evaluate new pharmacological interventions for EC patients. These include novel combinations of existing drugs, such as chemotherapy with immunotherapy or targeted therapy; new drugs with different mechanisms of action, such as antibody-drug conjugates, bispecific antibodies, or epigenetic modulators; or personalized therapies based on the molecular profile of the tumor, such as tumor-agnostic therapies or basket trials.57 These trials aim to identify new options for patients who do not respond to or relapse after standard therapies, or who have rare or aggressive subtypes of EC.
Omics Background and Research Progress
In recent years, omics technologies have been widely applied in biomedical research, particularly in cancer research, where their importance has become increasingly prominent. Omics, including genomics, transcriptomics, proteomics, and metabolomics, allows for a comprehensive analysis of genetic information, gene expression, protein functions, and metabolic processes from multiple dimensions and levels.58 The advancement of these technologies has enabled in-depth exploration of biological mechanisms at the cellular and tissue levels, driving innovations in cancer diagnosis, prognostic evaluation, and therapeutic strategies.
In the study of EC, omics technologies have become essential tools for uncovering the mechanisms underlying disease initiation and progression. Through high-throughput genomic and transcriptomic analyses, researchers have identified various gene mutations and expression profile alterations associated with EC.59 The genomic landscape of EC is underpinned by genetic alterations, such as mutations in PTEN, PIK3CA, and ARID1A, and chromosomal abnormalities.60 The identification of molecular subtypes—POLE ultramutated, microsatellite instability (MSI), copy number low, and copy number high—illustrates the diverse genetic profiles within EC and underscores the need for subtype-specific therapeutic strategies.61 The integration of multi-omics technologies such as single-cell genomics and spatial transcriptomics has revolutionized our understanding and approach to studying EC and offers a holistic perspective that enhances the ability to identify novel biomarkers and therapeutic targets.62 The translation of these multi-omics findings into personalized medicine and precision oncology is increasingly feasible in clinical practice.63
Conclusion
Summary of Key Findings
EC continues to pose a significant challenge in the realm of women’s health. The rising incidence rates underscore the urgency to develop effective therapeutic interventions. The intricate dance of molecular pathways, especially the interplay between the Bcl-2 family, estrogen receptors, and other molecular markers, has opened new vistas in the treatment landscape. The potential of natural compounds, particularly those from the polysaccharide category, showcases a promising bridge between traditional and modern treatment paradigms. Moreover, the intrinsic relationship between apoptosis and cancer progression further accentuates the importance of targeted therapies that can leverage these natural cellular processes.
Implications for Clinical Practice
The holistic treatment of EC now spans beyond traditional therapies. Modern advances in understanding molecular mechanisms offer an arsenal of tools for clinicians. The insights gained from studies underscore the significance of tailoring treatments based on the specific molecular subtypes of EC. In doing so, the potential for improved patient outcomes becomes more tangible. Natural compounds, especially natural polysaccharides, have emerged as not just complementary alternatives but as potential mainstays in the treatment regimen. Their ability to augment conventional treatments, with possibly fewer side effects, makes them invaluable in clinical practice.
Despite the promising early results, larger clinical trials and biomarker-driven studies are needed to ensure that these therapies are not only effective but also safe for a broad patient population. Understanding the optimal combinations, dosages, and potential resistance mechanisms will be crucial for their successful implementation in clinical practice.
Recommendations for Future Research
The journey in EC research, though filled with breakthroughs, is far from completion. To realize the full potential of recent advances, there is a pressing need to delve deeper into understanding the long-term impacts and the possible latent side effects associated with new interventions. Future research endeavors should prioritize multicentric clinical trials that juxtapose the outcomes of traditional therapies with emerging ones. This will not only offer a clearer picture of optimal treatment pathways but also shed light on potential synergistic effects. Further, a holistic understanding of EC would be incomplete without a detailed exploration of the genetic and environmental variables that act as its bedrock. By unraveling these factors, the medical community can pave the way for truly personalized treatment strategies, ensuring that each patient receives care that is best aligned with their unique genetic and molecular profile.
By embracing a personalized medicine approach—tailored to the genetic and molecular profile of individual patients—we can enhance the precision and efficacy of these emerging cancer therapies, leading to better patient outcomes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Baoding Science and Technology Program (No. 2341ZF150).
Disclosure
All authors declare that there are no conflicts of interest in this work.
References
1. Makker V, MacKay H, Ray-Coquard I, et al. Endometrial cancer. Nat Rev Dis Primers. 2021;7(1):88. doi:10.1038/s41572-021-00324-8
2. Passarello K, Kurian S, Villanueva V. Endometrial cancer: an overview of pathophysiology, management, and care. Semin Oncol Nurs. 2019;35(2):157–165. doi:10.1016/j.soncn.2019.02.002
3. van den Heerik ASVM, Horeweg N, de Boer SM, et al. Adjuvant therapy for endometrial cancer in the era of molecular classification: radiotherapy, chemoradiation and novel targets for therapy. Int J Gynecol Cancer. 2021;31(4):594–604. doi:10.1136/ijgc-2020-001822
4. Cuccu I, D’Oria O, Sgamba L, et al. Role of genomic and molecular biology in the modulation of the treatment of endometrial cancer: narrative review and perspectives. Healthcare. 2023;11(4):571. doi:10.3390/healthcare11040571
5. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int, J, Cancer. 2015;136(5):E359–86. doi:10.1002/ijc.29210
6. Chen JG, Zhu J, Parkin DM, et al. Trends in the incidence of cancer in Qidong, China, 1978-2002. Int, J, Cancer. 2006;119(6):1447–1454. doi:10.1002/ijc.21952
7. Lax SF. Molecular genetic pathways in various types of endometrial carcinoma: from a phenotypical to a molecular-based classification. Virchows Arch. 2004;444(3):213–223. doi:10.1007/s00428-003-0947-3
8. Talhouk A, Hoang LN, McConechy MK, et al. Molecular classification of endometrial carcinoma on diagnostic specimens is highly concordant with final hysterectomy: earlier prognostic information to guide treatment. Gynecol Oncol. 2016;143(1):46–53. doi:10.1016/j.ygyno.2016.07.090
9. Lin H, Zhu Y, Ahmad N, Han Q. A scientometric analysis and visualization of global research on brownfields. Environ Sci Pollut Res Int. 2019;26(17):17666–17684. doi:10.1007/s11356-019-05149-3
10. Crosbie EJ, Kitson SJ, McAlpine JN, et al. Endometrial cancer. Lancet. 399(10333):1412–1428. doi:10.1016/S0140-6736(22)00323-3
11. Dexter J, Lips E, DiSilvestro P. Adjuvant therapy in node-positive endometrial cancer: a focus on chemotherapy. Curr Oncol Rep. 2022;24(12):1677–1683. doi:10.1007/s11912-022-01327-8
12. Galaal K, Al Moundhri M, Bryant A, et al. Adjuvant chemotherapy for advanced endometrial cancer. Cochrane Database Syst Rev. 2014;2014(5):CD010681. doi:10.1002/14651858.CD010681.pub2
13. Humber CE, Tierney JF, Symonds RP, et al. Chemotherapy for advanced, recurrent or metastatic endometrial cancer: a systematic review of Cochrane collaboration. Ann Oncol. 2007;18(3):409–420. doi:10.1093/annonc/mdl417
14. Huber D, Seitz S, Kast K, et al. Hormone replacement therapy in BRCA mutation carriers and risk of ovarian, endometrial, and breast cancer: a systematic review. J Cancer Res Clin Oncol. 2021;147(7):2035–2045. doi:10.1007/s00432-021-03629-z
15. Burstein HJ, Lacchetti C, Anderson H, et al. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: American society of clinical oncology clinical practice guideline update on ovarian suppression. J Clin Oncol. 2016;34(14):1689–1701. doi:10.1200/JCO.2015.65.9573
16. Jordan VC. Tamoxifen: a most unlikely pioneering medicine. Nat Rev Drug Discov. 2003;2(3):205–213. doi:10.1038/nrd1031
17. Dowsett M, Cuzick J, Ingle J, et al. Meta-analysis of breast cancer outcomes in adjuvant trials of aromatase inhibitors versus tamoxifen. J Clin Oncol. 2010;28(3):509–518. doi:10.1200/JCO.2009.23.1274
18. Lee SJ, Cha CD, Hong H, et al. Adverse effects of tamoxifen treatment on bone mineral density in premenopausal patients with breast cancer: a systematic review and meta-analysis. Breast Cancer. 2024;31(4):717–725. doi:10.1007/s12282-024-01586-2
19. Wang J, Wang L. The therapeutic effect of dehydroepiandrosterone (DHEA) on vulvovaginal atrophy. Pharmacol Res. 2021;166:105509. doi:10.1016/j.phrs.2021.105509
20. Slomovitz BM, Coleman RL. The PI3K/AKT/mTOR pathway as a therapeutic target in endometrial cancer. Clin Cancer Res. 2012;18(21):5856–5864. doi:10.1158/1078-0432.CCR-12-0662
21. Ray-Coquard I, Pautier P, Pignata S, et al. Olaparib plus bevacizumab as first-line maintenance in ovarian cancer. N Engl J Med. 2019;381(25):2416–2428. doi:10.1056/NEJMoa1911361
22. Sharma U, Tuli HS, Uttam V, et al. Role of hedgehog and hippo signaling pathways in cancer: a special focus on non-coding RNAs. Pharmacol Res. 2022;186:106523. doi:10.1016/j.phrs.2022.106523
23. Ott PA, Hodi FS, Robert C. CTLA-4 and PD-1/PD-L1 blockade: new immunotherapeutic modalities with durable clinical benefit in melanoma patients. Clin Cancer Res. 2013;19(19):5300–5309. doi:10.1158/1078-0432.CCR-13-0143
24. Carneiro BA, El-Deiry WS. Targeting apoptosis in cancer therapy. Nat Rev Clin Oncol. 2020;17(7):395–417. doi:10.1038/s41571-020-0341-y
25. An J, Li L, Zhang X. Curcusone C induces apoptosis in endometrial cancer cells via mitochondria-dependent apoptotic and ERK pathway. Biotechnol Lett. 2021;43(1):329–338. doi:10.1007/s10529-020-03027-4
26. Czabotar PE, Garcia-Saez AJ. Mechanisms of BCL-2 family proteins in mitochondrial apoptosis. Nat Rev Mol Cell Biol. 2023;24(10):732–748. doi:10.1038/s41580-023-00629-4
27. Cheng EH, Wei MC, Ler S, et al. BCL-2, BCL-X(L) sequester BH3 domain-only molecules preventing BAX- and BAK-mediated mitochondrial apoptosis. Mol Cell. 2001;8(3):705–711. doi:10.1016/s1097-2765(01)00320-3
28. Czabotar PE, Lessene G, Strasser A, et al. Control of apoptosis by the BCL-2 protein family: implications for physiology and therapy. Nat Rev Mol Cell Biol. 2014;15(1):49–63. doi:10.1038/nrm3722
29. Konecny GE, Winterhoff B, Kolarova T, et al. Expression of p16 and retinoblastoma determines response to CDK4/6 inhibition in ovarian cancer. Clin Cancer Res. 2011;17(6):1591–1602. doi:10.1158/1078-0432.CCR-10-2307
30. Dorjgochoo T, Xiang YB, Long J, et al. Association of genetic markers in the BCL-2 family of apoptosis-related genes with endometrial cancer risk in a Chinese population. PLoS One. 2013;8(4):e60915. doi:10.1371/journal.pone.0060915
31. Zhang Y, Yan W, Jung YS, et al. PUMA Cooperates with p21 to regulate mammary epithelial morphogenesis and epithelial-to-mesenchymal transition. PLoS One. 2013;8(6):e66464. doi:10.1371/journal.pone.0066464
32. Adams JM, Cory S. The BCL-2 arbiters of apoptosis and their growing role as cancer targets. Cell Death Differ. 2018;25(1):27–36. doi:10.1038/cdd.2017.161
33. Youle RJ, Strasser A. The BCL-2 protein family: opposing activities that mediate cell death. Nat Rev Mol Cell Biol. 2008;9(1):47–59. doi:10.1038/nrm2308
34. Mirakhor Samani S, Ezazi Bojnordi T, Zarghampour M, et al. Expression of p53, Bcl-2 and Bax in endometrial carcinoma, endometrial hyperplasia and normal endometrium: a histopathological study. J Obstet Gynaecol. 2018;38(7):999–1004. doi:10.1080/01443615.2018.1437717
35. Oltersdorf T, Elmore SW, Shoemaker AR, et al. An inhibitor of Bcl-2 family proteins induces regression of solid tumours. Nature. 2005;435(7042):677–681. doi:10.1038/nature03579
36. Souers AJ, Leverson JD, Boghaert ER, et al. ABT-199, a potent and selective BCL-2 inhibitor, achieves antitumor activity while sparing platelets. Nat Med. 2013;19(2):202–208. doi:10.1038/nm.3048
37. Song JH, Kandasamy K, Kraft AS. ABT-737 induces expression of the death receptor 5 and sensitizes human cancer cells to TRAIL-induced apoptosis. J Biol Chem. 2008;283(36):25003–25013. doi:10.1074/jbc.M802511200
38. Gandhi L, Camidge DR, Ribeiro de Oliveira M, et al. Phase I study of Navitoclax (ABT-263), a novel Bcl-2 family inhibitor, in patients with small-cell lung cancer and other solid tumors. J Clin Oncol. 2011;29(7):909–916. doi:10.1200/JCO.2010.31.6208
39. Wierda WG, Allan JN, Siddiqi T, et al. Ibrutinib plus venetoclax for first-line treatment of chronic lymphocytic leukemia: primary analysis results from the minimal residual disease cohort of the randomized phase II CAPTIVATE study. J Clin Oncol. 2021;39(34):3853–3865. doi:10.1200/JCO.21.00807
40. Baggstrom MQ, Qi Y, Koczywas M, et al. A phase II study of AT-101 (Gossypol) in chemotherapy-sensitive recurrent extensive-stage small cell lung cancer. J Thorac Oncol. 2011;6(10):1757–1760. doi:10.1097/JTO.0b013e31822e2941
41. Winuthayanon W, Hewitt SC, Orvis GD, et al. Uterine epithelial estrogen receptor α is dispensable for proliferation but essential for complete biological and biochemical responses. Proc Natl Acad Sci U S A. 2010;107(45):19272–19277. doi:10.1073/pnas.1013226107
42. Liang J, Shang Y. Estrogen and cancer. Annu Rev Physiol. 2013;75:225–240. doi:10.1146/annurev-physiol-030212-183708
43. Guha P, Sen K, Chowdhury P, Mukherjee D. Estrogen receptors as potential therapeutic target in endometrial cancer. J Recept Signal Trans Res. 2023;43(1):19–26. doi:10.1080/10799893.2023.2187643
44. Yu K, Huang ZY, Xu XL, et al. Estrogen Receptor Function: impact on the Human Endometrium. Front Endocrinol. 2022;13:827724. doi:10.3389/fendo.2022.827724
45. Guo RX, Wei LH, Tu Z, et al. 17 beta-estradiol activates PI3K/Akt signaling pathway by estrogen receptor (ER)-dependent and ER-independent mechanisms in endometrial cancer cells. J Steroid Biochem Mol Biol. 2006;99(1):9–18. doi:10.1016/j.jsbmb.2005.11.013
46. Martin LA, Dowsett M. BCL-2: a new therapeutic target in estrogen receptor-positive breast cancer? Cancer Cell. 2013;24(1):7–9. doi:10.1016/j.ccr.2013.06.006
47. Ushijima K, Yahata H, Yoshikawa H, et al. Multicenter phase II study of fertility-sparing treatment with medroxyprogesterone acetate for endometrial carcinoma and atypical hyperplasia in young women. J Clin Oncol. 2007;25(19):2798–2803. doi:10.1200/JCO.2006.08.8344
48. Thigpen JT, Brady MF, Alvarez RD, et al. Oral medroxyprogesterone acetate in the treatment of advanced or recurrent endometrial carcinoma: a dose-response study by the Gynecologic Oncology Group. J Clin Oncol. 1999;17(6):1736–1744. doi:10.1200/JCO.1999.17.6.1736
49. Hashemi M, Mirdamadi MSA, Talebi Y, et al. Pre-clinical and clinical importance of miR-21 in human cancers: tumorigenesis, therapy response, delivery approaches and targeting agents. Pharmacol Res. 2023;187:106568. doi:10.1016/j.phrs.2022.106568
50. Zhang F, Zhang YY, Sun YS, et al. Asparanin A from Asparagus officinalis L. Induces G0/G1 Cell Cycle Arrest and apoptosis in human endometrial carcinoma ishikawa cells via mitochondrial and pi3k/akt signaling pathways. J Agric Food Chem. 2020;68(1):213–224. doi:10.1021/acs.jafc.9b07103
51. Grybos A, Bar J. The relationships between the immunoexpression of KAI1, MMP-2, MMP-9 and steroid receptors expression in endometrial cancer. Folia Histochem Cytobiol. 2014;52(3):187–194. doi:10.5603/FHC.2014.0022
52. Huang C, Hu G. Shikonin suppresses proliferation and induces apoptosis in endometrioid endometrial cancer cells via modulating miR-106b/PTEN/AKT/mTOR signaling pathway. Biosci Rep. 2018;38(2):BSR20171546. doi:10.1042/BSR20171546
53. Jiang J, Zhou N, Ying P, et al. Emodin promotes apoptosis of human endometrial cancer through regulating the MAPK and PI3K/ AKT pathways. Open Life Sci. 2019;13:489–496. doi:10.1515/biol-2018-0058
54. Soumoy L, Ghanem GE, Saussez S, et al. Bufalin for an innovative therapeutic approach against cancer. Pharmacol Res. 2022;184:106442. doi:10.1016/j.phrs.2022.106442
55. Pignata S, Scambia G, Katsaros D, et al. Carboplatin plus paclitaxel once a week versus every 3 weeks in patients with advanced ovarian cancer (MITO-7): a randomized, multicenter, open-label, Phase 3 trial. Lancet Oncol. 2014;15(4):396–405. doi:10.1016/S1470-2045(14)70049-X
56. Li X, Chen X, Guo J, et al. Lycium barbarum polysaccharides inhibit the proliferation and invasion of endometrial cancer cells via PI3K/Akt/mTOR signaling pathway. Int J Biol Macromol. 2019;140:1090–1098.
57. Makker V, Rasco D, Vogelzang NJ, et al. Lenvatinib plus pembrolizumab in patients with advanced endometrial cancer: an interim analysis of a multicentre, open-label, single-arm, Phase 2 trial. Lancet Oncol. 2019;20(5):711–718. doi:10.1016/S1470-2045(19)30020-8
58. Lin Z, Wang F, Yin R, et al. Single-cell RNA sequencing and immune microenvironment analysis reveal PLOD2-driven malignant transformation in cervical cancer. Front Immunol. 2025;15:1522655. doi:10.3389/fimmu.2024.1522655
59. Clark AJ, Singh R, Leonis RL, et al. Gene co-expression network analysis associated with endometrial cancer tumorigenesis and survival outcomes. Int J Mol Sci. 2024;25(22):12356. doi:10.3390/ijms252212356
60. Kandoth C, Schultz N, Cherniack AD, et al. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67–73. doi:10.1038/nature12113
61. Galant N, Krawczyk P, Monist M, et al. Molecular classification of endometrial cancer and its impact on therapy selection. Int J Mol Sci. 2024;25(11):5893. doi:10.3390/ijms25115893
62. Yu Z, Zhang J, Zhang Q, et al. Single-cell sequencing reveals the heterogeneity and intratumoral crosstalk in human endometrial cancer. Cell Prolif. 2022;55(6):e13249. doi:10.1111/cpr.13249
63. Chen Z, Liang B, Wu Y, et al. Integrating multi-omics data to identify dysregulated modules in endometrial cancer. Brief Funct Genomics. 2022;21(4):310–324. doi:10.1093/bfgp/elac010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.