Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Molecular Epidemiology of Human Herpes Virus Type 8 Among Patients with Compromised Immune System in Ouagadougou, Burkina Faso
Authors Biatougou NMB, Ouedraogo MS, Soubeiga ST ![]() , Zohoncon TM, Ouedraogo P, Obiri-Yeboah D
, Zohoncon TM, Ouedraogo P, Obiri-Yeboah D ![]() , Tapsoba ASA, Kiendrebeogo TI
, Tapsoba ASA, Kiendrebeogo TI ![]() , Sagna T
, Sagna T ![]() , Niamba P, Traore A, Simpore J
, Niamba P, Traore A, Simpore J ![]()
Received 8 December 2021
Accepted for publication 1 July 2022
Published 8 July 2022 Volume 2022:14 Pages 311—317
DOI https://doi.org/10.2147/HIV.S353166
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Nakougou Mo&idigr;-bohm Biatougou,1 Muriel S Ouedraogo,2 Serge Theophile Soubeiga,3,4 Theodora Mahoukede Zohoncon,1,5 Paul Ouedraogo,5 Dorcas Obiri-Yeboah,6 Aziz Sidi Aristide Tapsoba,1 Touwendpoulimdé Isabelle Kiendrebeogo,1,3 Tani Sagna,4 Pascal Niamba,2 Adama Traore,2 Jacques Simpore1,3
1Biochemistry and Microbiology Department, Laboratory of Molecular Biology and Genetics (LABIOGENE), University Joseph Ki-Zerbo, Ouagadougou, Burkina Faso; 2Department of Dermatology, Yalgado Ouedraogo Hospital University Centre, Ouagadougou, Burkina Faso; 3Department of Biomedical Research, Biomolecular Research Centre Pietro Annigoni (CERBA), Ouagadougou, Burkina Faso; 4Department of Biomedical and Public Health, Research Institute of Health Sciences (IRSS), Ouagadougou, Burkina Faso; 5Department of Medicine, Saint Thomas d’Aquin University (USTA), Ouagadougou, Burkina Faso; 6Department of Microbiology and Immunology, University of Cape Coast, Cape Coast, Ghana
Correspondence: Serge Theophile Soubeiga, Department of Biomedical and Public Health, Research Institute for Health Sciences (IRSS), P.O. 03. BOX 7047, Ouagadougou, Burkina Faso, Tel +226 70 01 30 58, Email [email protected]
Introduction: Human herpesvirus type 8 (HHV-8) is the main etiological agent of Kaposi’s sarcoma. This virus is frequently associated with immunocompromision. This study aimed to detect HHV-8 in people with compromised immune system.
Patients and Methods: This is a cross-sectional study that included 180 subjects: 179 HIV-infected patients and 1 patient with bullous pemphigoid. Blood samples were taken from all subjects, and swabs of lesions were then taken from individuals with symptoms of Kaposi’s sarcoma. Viral load and CD4+ T lymphocytes count were performed for persons living with HIV and real-time PCR detection of HHV-8 DNA was performed in all subjects in the study.
Results: Among HIV-infected persons, 13.41% had a viral load of more than 10,000 copies/mL, and 22.91% had a CD4+ T lymphocytes count of fewer than 350 cells/μL. A total of four (three HIV-1 infected patients and one patient with bullous pemphigoid) patients (2.22%) had apparent lesions of Kaposi’s sarcoma. In the plasmas and swabs from associated lesions, HHV-8 DNA was found in only two individuals, with an HHV-8 prevalence of 1.11% (2/180) with 0.55% (1/179) in an HIV-infected patient on antiretroviral therapy.
Conclusion: These results exposing low prevalence levels of HHV-8 in HIV-infected patients could be due to the beneficial effect of antiretroviral drugs.
Keywords: HIV, HHV-8, immunocompromised, Kaposi’s sarcoma, Burkina Faso
Introduction
Human herpesvirus type 8 (HHV-8) is the main etiological agent of Kaposi’s sarcoma and has also been associated with multicentric Castleman’s disease and primary effusion lymphomas.1 HHV-8 is one of the most oncogenic known human viruses.2 Kaposi’s sarcoma, often associated with HIV, is an opportunistic infection that occurs predominantly in men, but women, children, intravenous drug users, organ recipients, and people living with HIV (PLWHIV) are at risk of developing this disease.3–5
While WHO estimated in 2020, that 37.7 million people were living with HIV worldwide, the seroprevalence of HHV-8 varies across geographical regions and subpopulations.6,7 This seroprevalence, while relatively low in northern countries, is high in Africa with more than 50% in some countries such as Cameroon.8–10 A high prevalence of HHV-8 is observed in people with immunodeficiencies such as PLWHIV.11 In Burkina Faso, a seroprevalence of 12.15% has been reported in pregnant women infected with HIV.12 However, little information is available. In a context where HHV-8 is endemic in West Africa, having data on the prevalence of this virus in people susceptible to sustained immunocompromision is of great epidemiological importance. This study, therefore, aimed to detect the presence of HHV-8 in patients with HIV and bullous pemphigoid in Burkina Faso.
Materials and Methods
Study Population and Sample Collection
This was a cross-sectional study that ran from December 2018 to July 2019 and involved 180 subjects (179 HIV-infected patients and 1 person with bullous pemphigoid under long-term corticosteroid therapy) followed at Saint Camille Hospital of Ouagadougou (HOSCO), Pietro Annigoni Biomolecular Research Center/Laboratory of Molecular Biology and Molecular Genetics and Yalgado Ouedraogo University Hospital (CHU-YO).
Sociodemographic, paraclinical and therapeutic information were obtained from the clinicians in charge of monitoring these patients. Whole blood was collected from each participant of the study by venipuncture and collected in two EDTA-impregnated tubes. The first blood tube was used to perform the CD4+ T lymphocytes count; the second blood tube was centrifuged at 2000 g for 5 min to collect plasma sample that was stored at −80°C and subsequently used for HIV-1 viral load determination and HHV-8 detection. Also, swab samples were taken from patients with apparent symptoms of Kaposi’s sarcoma.
Determination of HIV-1 Viral Load and CD4+ T Cell Count
HIV-1 RNA was extracted manually using the “Abbott mSample Preparation” kit and amplified using the “Abbott HIV-1TM Real-Time” kit on the Abbott m2000rt thermocycler (Abbott Laboratories, Des Plaines, Illinois, USA) according to the manufacturer’s instructions. CD4+ T lymphocytes count was performed on the FACS Count BD flow cytometer (Grenoble, France) with the “BD FACS Count CD4” reagent according to the manufacturer’s instructions.
Detection of HHV-8 by Real-Time PCR
HHV-8 DNA was extracted from plasma samples and swabs collected from patients in the study using the “DNA Sorb B” kit (Sacace Biotechnologies, Como, Italy) and amplified using the “HHV-8 Real-Time TM” kit on the SaCycler −96 Real-Time PCR thermocycler (Sacace Biotechnologies, Como, Italy), also following the manufacturer’s instructions.
Statistical Analyses
The data collected were entered into Excel 2013 and then analysed using the standard Statistical Package for Social Sciences (SPSS) version 21 and EPI Info version 6.0 software. The statistical significance threshold was set at p < 0.05.
Ethics Considerations
The protocol of this research was approved by the Institutional Ethics Committee of HOSCO and CERBA/LABIOGENE (Deliberation N° 2018-22/X-014) and was conducted according to the Helsinki Declaration. All study participants gave their free and informed consent. Parents or legal guardians of participants under 18 years of age provided informed consent while the participants gave accent. The anonymity and confidentiality of the data collected, and the results were assured. The results were returned to clinicians in charge of monitoring these patients to inform their care.
Results
Socio-Demographic, Paraclinical, and Biological Data
A total of 180 individuals participated in our study. Of these, 174 (96.67%) were HIV-1, 5 (2.78%) were co-infected with HIV-1/HIV-2, and 1 (0.55%) was an immunocompromised person with bullous pemphigoid on long-term corticosteroid therapy.
The predominant sex was female, 77.22% (139/180). The average age of the patients in our study was 44.76 ± 10.75 years with extremes of 8 and 76 years. The most represented age group was over 45 years old for 50.00% (90/180). Among HIV-1-infected persons in our study, 61.45% (110/179) were receiving first-line treatment, although some of these people had changed treatment regimens ranging from 1 to 4 times (Table 1). The average duration of HIV-1 treatment was 7.99 ± 4.42 years with extremes of 3 months and 16 years. The majority, 72.07% (129/179) of HIV-1 infected patients had been on treatment for at least 5 years (Table 1).
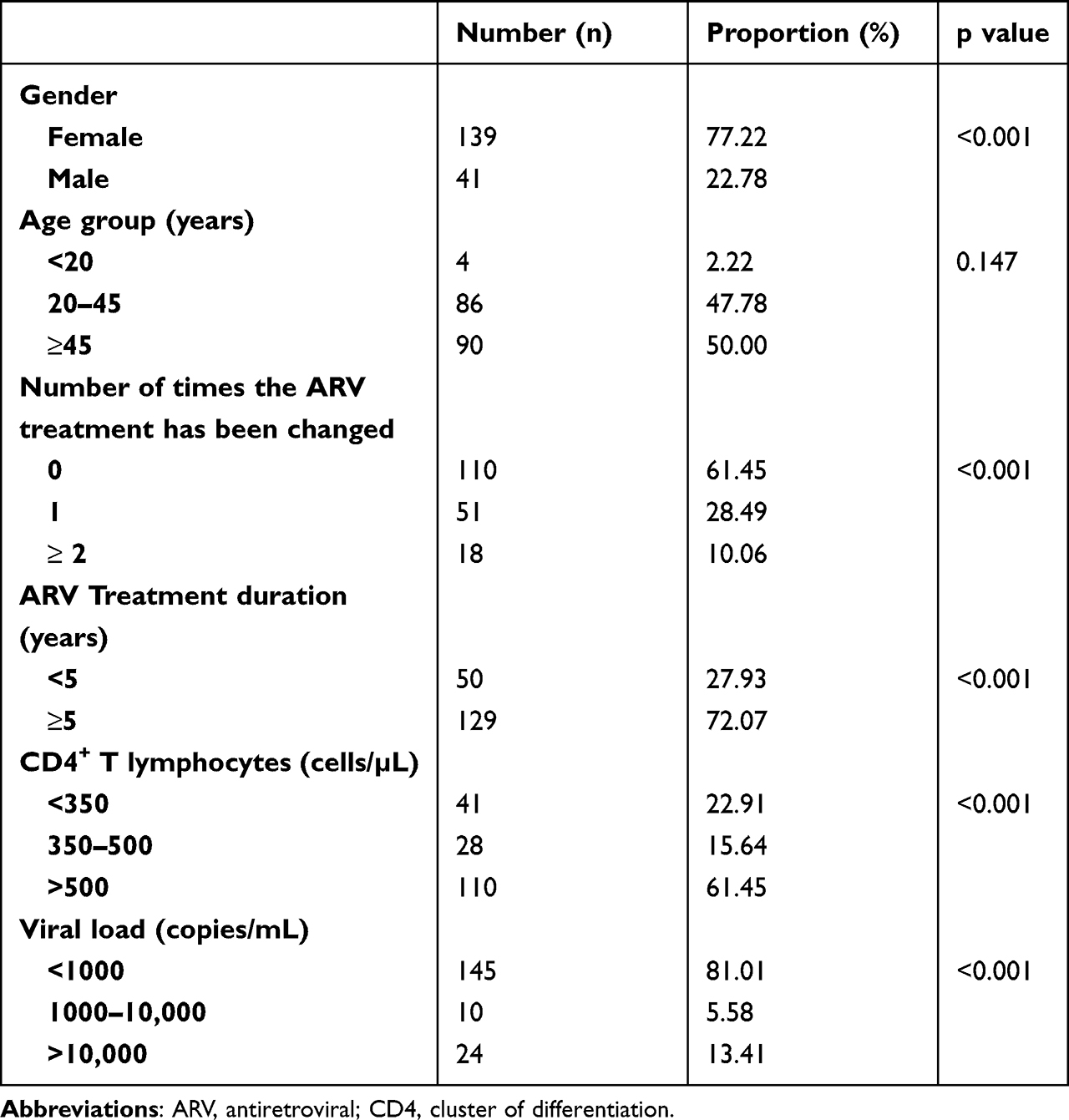 |
Table 1 Summary of Socio-Demographic, Paraclinical and Biological Data |
HIV-1 Viral Load and CD4+ T Lymphocytes Count
The majority (81.01%) of HIV-1 infected persons in our study had viral load <1000 copies/mL, while 13.41% (24/179) had a viral load of more than 10,000 copies/mL (Table 1). Also, 61.45% (110/179) had CD4+ T lymphocytes counts greater than 500 cells/µL while 22.91% (41/179) had CD4+ T lymphocytes counts less than 350 cells/µL. The average CD4+ T lymphocytes count was 658.53 ± 376.82 cells/µL with extremes of 13 cells/µL and 2038 cells/µL.
Association Between Kaposi’s Sarcoma Symptoms and Paraclinical and Biological Parameters
Of the 180 patients in our study, only 4 (2.22%) had apparent symptoms of Kaposi’s sarcoma (ulcerated and/or non-ulcerated lesions on the skin). The presence of lesions was associated with HIV-1 viral load (p<0.001) and duration of treatment (p=0.010). However, CD4+ T lymphocytes count (p=0.373) and treatment change (p=0.637) (Table 2) were not associated with Kaposi’s sarcoma symptoms.
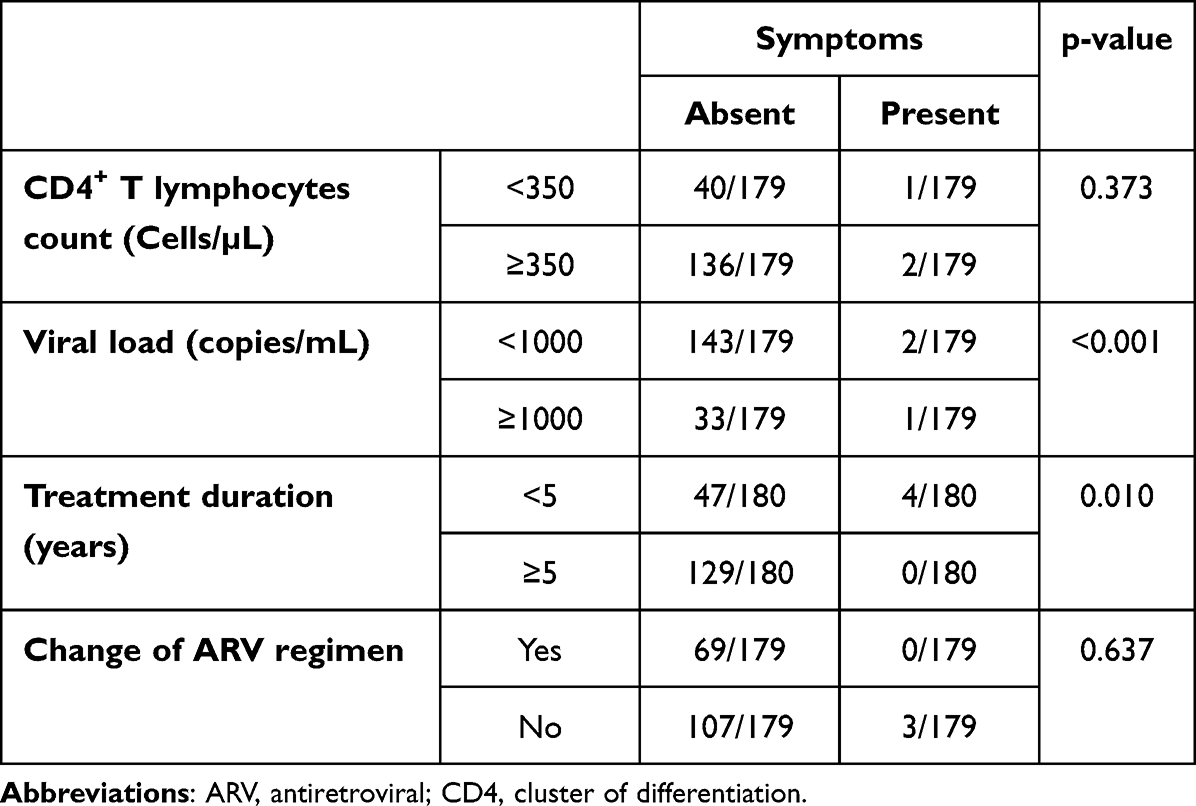 |
Table 2 Relations Between the Apparent Symptoms of Kaposi’s Sarcoma and Clinical and Biological Parameters |
Detection of HHV-8 in the Global Population Study
In our study population, of the four people with apparent symptoms of Kaposi’s sarcoma, two had ulcerated lesions and two were HIV-1 infected patients. HHV-8 DNA was found only in the two individuals with ulcerated lesions, representing an overall prevalence of HHV-8 in our study population of 1.11% (2/180) (Table 3).
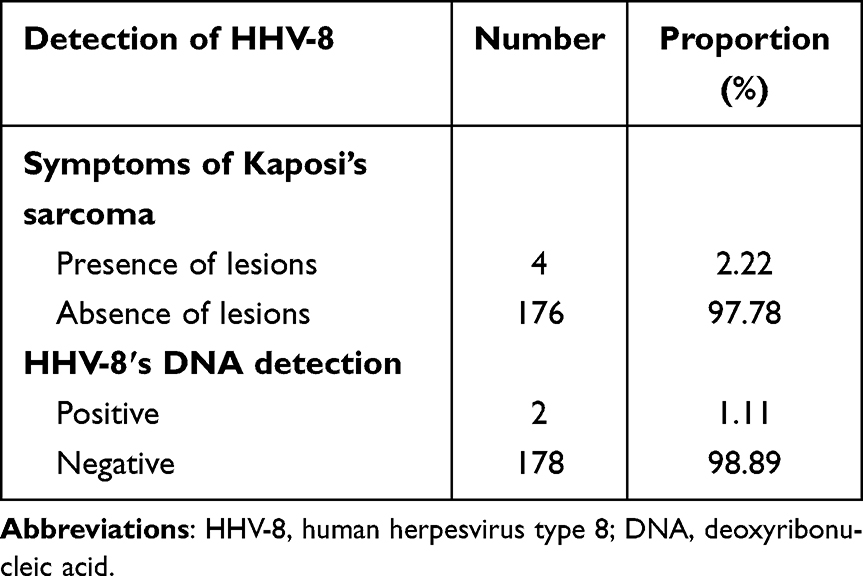 |
Table 3 Apparent Symptoms of Kaposi’s Sarcoma and Detection of HHV-8 DNA |
Detection of HHV-8 in HIV-1 Infected Persons
Among 179 HIV-1-infected persons, 3 had apparent symptoms of Kaposi’s sarcoma. HHV-8 DNA was detected only in one person whose lesions were ulcerated, unlike the other two whose lesions were not ulcerated and who were undergoing chemotherapy (three Oncovin plus Bleomycin cures each). This person also had a very low CD4+ T lymphocytes count (14 cells/µL) and a very high viral load (331, 131 copies/mL). In this person, HHV-8 DNA was not detected in plasma, but rather in swab samples of his lesions (Table 4). The prevalence of HHV-8 among HIV-1-infected patients in our study was 0% (0/179) in plasma and 0.55% (1/179) in lesions.
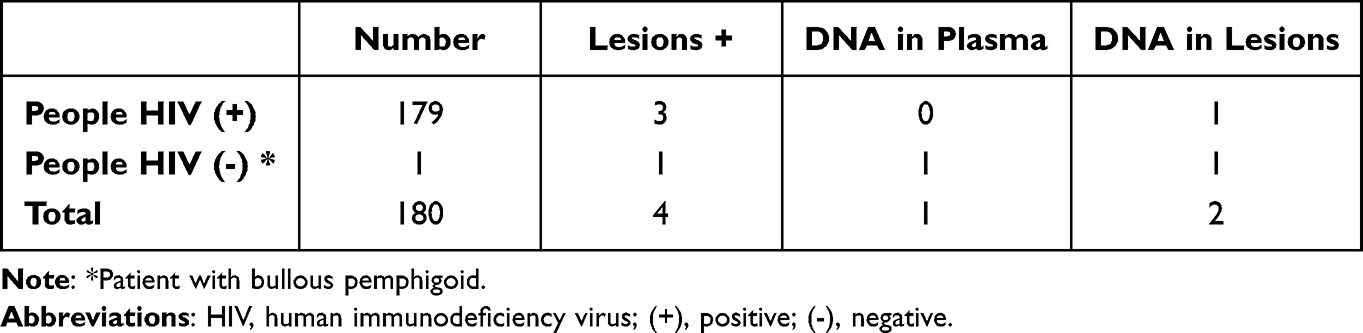 |
Table 4 Detection of HHV-8 DNA by Sample Type |
Detection of HHV-8 in Another Immunocompromised Person
Only one non-HIV-infected patient participated in our study. He was 76 years old and had bullous pemphigoid, for which he had been put on long-term corticosteroid therapy, which was the cause of his immunocompromision. This person had apparent symptoms of Kaposi’s sarcoma that had an ulcerated appearance. HHV-8 DNA was detected in this person’s plasma and ulcerated lesions (Table 4).
Discussion
The main objective of our study was to determine the prevalence of HHV-8 in a population composed of people suffering from a pathology that could lead to immunocompromision. HIV-1-infected patients (96.67%) were predominant. People co-infected with HIV-1/HIV-2 accounted for only 2.78%. These trends were also reported in 2014 by Sagna et al, who found in their study 92.7% (HIV-1) and 3.4% (HIV-1/HIV-2).13 However, Karfo et al reported in 2018 a lower proportion of HIV-1-infected persons compared to our results (80.9%).14 Females were more representative among HIV-infected patients and this was also the bias reported by Ky-Zerbo et al.15 This same observation was made by WHO in 2017 and shows that women are the most affected by HIV-1.16 The average age of the subjects in our study was 44.76 ± 10.75 years, and the most represented age group which was over 45 years has also been observed in other studies in Burkina Faso.14 The high proportion of individuals in this age group could be explained by the fact that the majority of HIV-infected patients in this study have been followed-up for several years since their diagnosis. Indeed, 72.07% of the patients had more than 5 years of ARV treatment duration. This study revealed also that 81.01% of HIV-1-infected patients had viral load less than 1000 copies/mL compared to 13.41% who had a viral load greater than 10,000 copies/mL. This finding is consistent with some studies conducted in Burkina Faso and Mali in 2008.17 This indicates that ARV treatment is effective in patients of this study. On the other hand, the high viral load values observed in some patients may be due to either poor adherence to treatment and/or virologic failure related to ARV resistance mutations.18 During their ARV treatment, some patients develop HIV drug resistance (HIVDR). HIVDR is caused by changes in the genetic structure of HIV that affect the ability of drugs to block the replication of the virus.19 Good therapeutic education and/or switch regimens are necessary to improve the health of these patients. Actually, to stop HIVDR, WHO recommends that all global stakeholders should promote the availability of optimal drugs to treat HIV infections, support retention in care and optimal adherence to treatment, increase access and use of viral load testing to know if HIV treatment is working, and rapidly switch regimens in cases of confirmed treatment failure.19 Our results regarding CD4+ T lymphocytes were high compared to those reported by Sagna et al.13 This is because most patients in this study (72.07%), had been on antiretroviral therapy for at least 5 years, while in the study conducted by Sagna et al, HIV-1-infected patients were at the beginning of treatment. Indeed, ARV treatment contributes to restoration of the immune system. The low CD4+ T lymphocytes we found, suggesting severe immunocompromision, may reflect poor adherence to treatment of patients, immunological failure of antiretroviral therapy, or temporary loss of sight of patients during their management.20
The prevalence of HHV-8 among HIV-infected patients in our study was very low at 0.55% (1/179). Also, a low prevalence of HHV-8 has been reported by other authors in India (0%) and Brazil (4%) respectively.21,22 However, Ilboudo et al in Burkina Faso reported higher prevalence in 2009 (12.15%), a period where the ARV treatment was not available to all HIV-1-infected.12 This difference may be due to the additional natural immunocompromision of HIV-1-positive pregnant women included in their study. We also noted that the prevalence of HHV-8 in our study was very low compared to the results of the work carried out since 2004 by our predecessors, whose objective was to study the evolution of the prevalence of HHV-8 among different types of immunocompromised populations in Burkina Faso,12,23,24 namely 21.2%, 12.50%, and 12.15%, respectively. This significant reduction in the prevalence of HHV-8 found in our study could be due to the current systematic introduction of antiretroviral treatment for all HIV-1-infected patients as required by WHO recommendations; this was not the case in 2004, 2007, and 2009. This strategy would promote the maintenance of the immune system at a level or restore an immune response capable of controlling HHV-8 replication.25 Protease inhibitors included in antiretroviral triple therapies are also reported to be protective agents against replication of the virus associated with Kaposi’s sarcoma.24 Only one HIV-infected person was HHV-8 coinfected in our study. This person had a very low CD4+ T lymphocytes count (14 cells/µL) and a very high viral load (331, 131 copies/mL), a condition favorable to the development of opportunistic infections such as HHV-8 infection.26
The detection of HHV-8 in ulcerated lesions and not in plasma in only one HIV-1-infected patient could be due to the pathophysiology of HHV-8, which would lead it to specific areas of the body and therefore to the onset of symptoms. Skin lesions of Kaposi’s sarcoma are clinically classified into the patchy, plaque and nodular stage and appear mainly in the extremities, but in more advanced cases appear as multiple ovoid-shaped skin lesions in the trunk symmetrically.27 One case of iatrogenic Kaposi disease was found in our study although this form is very rare and usually described in transplant recipients under immunosuppressive therapy with only a few cases reported in Africa.28–30 This is a 76-year-old person afflicted with an autoimmune disease, bullous pemphigoid, who is on long-term corticosteroid therapy. This result confirms that bullous pemphigoid is a disease that affects the elderly the most. In addition, HHV-8 DNA was found in the patient’s plasma and ulcerated lesions. The detection of HHV-8 DNA in this participant’s plasma may be due to a dampened immune system in response to the long-term high-dose corticosteroid therapy, which is the most commonly used treatment in this type of disease. Interruption of this treatment could lead to a regression of Kaposi’s sarcoma lesions in this participant in our study.29,30
Conclusion
Our study highlighted HHV-8 in a population consisting of people living with HIV and a person with bullous pemphigoid, an autoimmune disease. One case of iatrogenic Kaposi disease has been found in this study. Besides HIV, other diseases inducing immunocompromision are a favorable situation for the development of HHV-8 infection.
Acknowledgments
We would like to thank Saint Camille Hospital of Ouagadougou, Pietro Annigoni Biomolecular Research Center/Laboratory of Molecular Biology and Molecular Genetics (CERBA/LABIOGENE), and the dermatology department of University Hospital Yalgado Ouedraogo for their support. We also thank all the patients who agreed to participate in the study.
Disclosure
The authors have no conflicts of interest in relation to this work.
References
1. Cesarman E, Chang Y, Moore PS, et al. Kaposi’s sarcoma-associated herpès virus-like DNA sequences in aids-related body-cavity–based lymphomas”. N Engl J Med. 1995;332(18):1186–1191. doi:10.1056/NEJM199505043321802
2. Moore PS, Chang Y. Why do viruses cause cancer? Highlights of the first century of human tumor virology. Nat Rev Cancer. 2010;10(12):878–889. doi:10.1038/nrc2961
3. Begré L, Rohner E, Mbulaiteye SM, et al. Is human herpès virus 8 infections more common in men than in women? Systematic review and meta-analysis. Int J Cancer. 2016;139(4):776–783. doi:10.1002/ijc.30129
4. Schneider JW, Dittmer DP. Diagnosis and treatment of Kaposi sarcoma. Am J Clin Dermatol. 2017;18(4):529–539. doi:10.1007/s40257-017-0270-4
5. Cavallin LE, Goldschmidt-Clermont P, Mesri EA. Molecular and cellular mechanisms of KSHV oncogenesis of Kaposi’s sarcoma associated with HIV/AIDS. PLoS Pathog. 2014;10(7):5–8. doi:10.1371/journal.ppat.1004154
6. World Health Organization. Data and statistics of HIV/AIDS. 2020. Available from: https://www.who.int/hiv/data/en/.
7. Minhas V, Wood C. Epidemiology and transmission of Kaposi’s sarcoma-associated herpès virus. Viruses. 2014;6(11):4178–4194. doi:10.3390/v6114178
8. Stolka K, Ndom P, Hemingway-Foday J, et al. Risk factors for Kaposi’s sarcoma among HIV-positive individuals in a case-control study in Cameroon. Cancer Epidemiol. 2014;38(2):137–143. doi:10.1016/j.canep.2014.02.006
9. Njiki BJ, Ndom P, Mupang L, Agokeng DS. Séroprévalence du virus de l’herpès humain-8 chez des patients VIH positif à l’hôpital général de Yaoundé - Cameroun [Seroprevalence of human herpes virus-8 in HIV-positive patients at the General Hospital of Yaounde - Cameroon]. Pan Afr Med J. 2015;20(69):1–7. French. doi:10.11604/pamj.2015.20.1.5568
10. Etta EM, Alayande DP, Ramarumo-Mavhandu LG, et al. HHV-8 seroprevalence and genotype distribution in Africa, 1998–2017: a systematic review. Viruses. 2018;10(9):1–17. doi:10.3390/v10090458
11. Altuğlu I, Yolcu A, Öcek ZA, et al. Investigation of Human Herpès virus-8 Seroprevalence in Blood Donors and HIV-Positive Patients Admitted to Ege University Medical School Hospital, Turkey”. Mikrobiyoloji Bulteni. 2016;50(1):104–111. doi:10.5578/mb.10751
12. Ilboudo D, Simpore J, Sanou DS, et al. Mother-to-child HIV and HHV-8 transmission in neonates at saint Camille Medical Center in Burkina Faso. Pak J Biol Sci. 2009;12(12):908–913. doi:10.3923/pjbs.2009.908.913
13. Sagna Y, Koulidiaty J, Diallo I, et al. Profil biologique des patients nouvellement pris en charge pour une infection à VIH à Ouagadougou (Burkina Faso) [Laboratory test features of newly diagnosed adult HIV-Infected patients in Ouagadougou (Burkina Faso)]. Med Sante Trop. 2014;24:307–311. French. doi:10.1684/mst.2014.0381
14. Karfo R, Kabré E, Coulibaly L, et al. Evolution of biochemical and hematological parameters in patients living with HIV/AIDS treated with antiretroviral therapy at the Aboubacar Sangoulé Lamizana General Camp Medical Center. Pan Afr Med J. 2018;8688:1–7.
15. Ky-Zerbo O, Desclaux A, El Asmar K, et al. La stigmatisation des PvVIH en Afrique: analyse de ses formes et manifestations au Burkina Faso [Stigmatization of PLWHIV in Africa: analysis of its forms and manifestations in Burkina Faso]. Sante Publique (Paris). 2014;26(3):375–384. French. doi:10.3917/spub.139.0375
16. World Health Organization. HIV country profile: 2017; 2020. Available from: https://www.cfs.hivci.org/country-factsheet.html.
17. Boileau C, Nguyen V, Sylla M, et al. Low prevalence of detectable HIV plasma viremia in patients treated with antiretroviral therapy in Burkina Faso and Mali. J Acquir Immune Defic Syndr. 2008;48(4):476–484. doi:10.1097/QAI.0b013e31817dc416
18. Kouéta F, Yé D, Zoungrana A, et al. Echecs du traitement antirétroviral de première ligne chez les enfants infectés par le VIH à Ouagadougou (Burkina Faso) [Failure of first-line antiretroviral treatment among HIV-infected children in Ouagadougou, Burkina Faso]. Med Trop. 2010;70(5/6):517–523. French.
19. World Health Organization. HIV drug resistance; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-drug-resistance.
20. Touré A, Cissé D, Kadio K, et al. Facteurs associés aux perdus de vue des patients sous traitement antirétroviral dans un centre de traitement ambulatoire du VIH à Conakry, Guinée [Factors associated with dropouts of patients on antiretroviral therapy in an outpatient HIV treatment center in Conakry, Guinea]. Rev Epidemiol Sante Publique. 2018;66(4):273–279. French. doi:10.1016/j.respe.2018.04.057
21. Sachithanandham J, Kannangai R, Abraham AM, et al. Human herpes virus-8 infections among subjects with human immunodeficiency virus infection and normal healthy individuals in India. Intervirology. 2013;56:253–257. doi:10.1159/000349890
22. Machado PRL, Farias KJS, Pereira MGM, et al. Human herpès virus 8 (HHV-8) detected by nested polymerase chain reaction (PCR) in HIV patients with or without Kaposi’s sarcoma. An analytic cross-sectional study. Sao Paulo Med J. 2016;134(3):187–192. doi:10.1590/1516-3180.2014.8973010
23. Simpore J, Granato M, Santarelli R, et al. Prevalence of infection by HHV-8, HIV, HCV and HBV among pregnant women in Burkina Faso. J Clin Vir. 2004;31:78–80. doi:10.1016/j.jcv.2004.06.001
24. Ilboudo D, Karou SD, Nadembega WMC, et al. Prevalence of human herpes virus-8 and hepatitis B virus among HIV seropositive pregnant women enrolled in the mother-to-child HIV transmission prevention program at Saint Camille. Pak J Biol Sci. 2007;10(17):2831–2837. doi:10.3923/pjbs.2007.2831.2837
25. Philibert P, Chiche L, Retornaz F, et al. Sarcome de Kaposi associé au VIH: à propos d [HIV-associated Kaposi's sarcoma: a case report illustrating the protective effect of HIV protease inhibitors]. Rev Med Interne. 2017;38:A220–A221. French. doi:10.1016/j.revmed.2017.03.328
26. Malonga GA, Jary A, Leducq V, et al. Seroprevalence and molecular diversity of Human Herpesvirus 8 among people living with HIV in Brazzaville, Congo. Sci Rep. 2021;11:17442. doi:10.1038/s41598-021-97070-4
27. Grayson W, Pantanowitz L. Histological variants of cutaneous Kaposi sarcoma. Diagn Pathol. 2008;3:31. doi:10.1186/1746-1596-3-31
28. Lamchahab M, Oukkache B, Marouan S, et al. Sarcome de Kaposi compliquant une aplasie médullaire [Kaposi sarcoma complicating bone marrow aplasia]. Pan Afr Med J. 2014;18(169):1–6. French. doi:10.11604/pamj.2014.18.169.1351
29. Saihi M, Jebali H, Breik N, et al. Le Sarcome de Kaposi iatrogène: à propos de trois observations [Iatrogenic Kaposi's Sarcoma: about three observations]. French. Rev Med Interne. 2018;39(1):A199. doi:10.1016/j.revmed.2018.03.169
30. El Jouari O, Chaymae J, Senhaji G, et al. Iatrogenic Kaposi sarcoma in an immune competent woman. Int J Cutaneous Disord Med Case. 2018;1(1):1–4.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.