Back to Journals » Journal of Pain Research » Volume 19
Modulation of Brain Activity in Patients with Acute Non-Specific Low Back Pain by Wentong Guan Therapy: A Functional Near-Infrared Spectroscopy Study
Authors Fu S, Chen H ![]() , Zhi X, Liu F, Zhang J
, Zhi X, Liu F, Zhang J ![]() , Ren L, Rong M, Wang Y
, Ren L, Rong M, Wang Y ![]()
Received 9 July 2025
Accepted for publication 9 February 2026
Published 13 April 2026 Volume 2026:19 544191
DOI https://doi.org/10.2147/JPR.S544191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor King Hei Stanley Lam
Shifang Fu,1,* Hao Chen,2,3,* Xiaoyu Zhi,1 Fanqi Liu,1 Junfeng Zhang,4 Longsheng Ren,5 Mengying Rong,5 Yanguo Wang1
1Rehabilitation Department, Tianjin University of Traditional Chinese Medicine Second Affiliated Hospital, Tianjin, 300150, People’s Republic of China; 2Acupuncture Department, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, 300193, People’s Republic of China; 3National Clinical Research Center for Chinese Medicine, Tianjin, 300381, People’s Republic of China; 4Brain Disease Department, Tianjin Academy of Traditional Chinese Medicine Affiliated Hospital, Tianjin, 300120, People’s Republic of China; 5Graduate School, Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanguo Wang, Rehabilitation Department, Tianjin University of Traditional Chinese Medicine Second Affiliated Hospital, Tianjin, 300150, People’s Republic of China, Email [email protected]
Background: Wentong Guan Therapy (WTG) integrates techniques from Chinese massage, moxibustion, scraping, and cupping. Its analgesic mechanisms remain unclear. The brain functional network in patients with acute non-specific low back pain (ANSLBP) is impaired, and central nervous system regulation is one of the important mechanisms through which traditional Chinese medicine external therapies alleviate pain and functional impairment in ANSLBP. This study neurophysiologically evaluates WTG’s pain modulation effect on the cerebral cortex in acute non-specific low back pain (ANSLBP).
Methods: Twelve ANSLBP patients received a single WTG session. Subjective pain (Visual Analogue Scale, VAS), pressure pain threshold (PPT) using a force-measuring glove, and cortical hemodynamic changes via functional near-infrared spectroscopy (fNIRS) were assessed pre- and post-treatment. False discovery rate (FDR) corrected multiple comparisons.
Results: Post-treatment, VAS scores significantly decreased (4.75± 1.29 to 3.58± 1.17, p< 0.001) and PPT increased (77.29± 39.83N to 94.58± 39.79N, p< 0.001). No significant brain network differences were found (PFDR> 0.05). Pre-treatment HbO2 concentration in channel 17 (DLPFC) was significant (PFDR=0.042), but post-treatment, no channels showed significance. Channel 33 (Somatosensory Association Cortex, SAC) showed a significant HbO2 change post-treatment (PFDR=0.038). ΔHbO2 in SAC (CH33) negatively correlated with ΔPPT (P=0.045, r=− 0.587).
Conclusion: WTG effectively alleviates ANSLBP. The SAC and DLPFC are involved in WTG’s neuromodulatory analgesic effects. Reduced ΔHbO2 in the SAC may be a potential biomarker for WTG’s analgesia.
Keywords: Wentong Guan therapy, acute non-specific low back pain, functional near-infrared spectroscopy, neuroactivity, somatosensory association cortex, dorsolateral prefrontal cortex
Introduction
Acute non-specific low back pain (ANSLBP) is one of the most common medical conditions. It is characterized by acute onset of low back pain (LBP), limited mobility, and a disease duration of less than 6 weeks.1 The lifetime prevalence of ANSLBP in adults reaches up to 40%, leading to significant socioeconomic costs worldwide.2,3 Approximately, 20% of patients continue to experience symptoms one year post-onset, and 3% remain unable to work, seriously affecting their quality of life, and physical and mental health.4 Therefore, effective treatment during the acute phase is essential to alleviate pain and prevent chronic progression.
International clinical practice guidelines focus on symptomatic treatment for managing ANSLBP, with drug treatment options including non-steroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, or short-term application of weak opioids.5 However, systematic reviews have highlighted limitations of drug treatment. For example, one review indicated that acetaminophen is ineffective for acute low back pain, while skeletal muscle relaxants offer short-term analgesia for acute low back pain but have sedative effects. Opioid use carries risks of adverse reactions such as central nervous system suppression and constipation.6 Certain exercises, kinesiology taping, and electro-physical agents are frequently used in treatment.7 Therefore, non-drug treatments like spinal manipulation, massage, and acupuncture are recommended for the treatment of LBP.8
Numerous studies have shown that traditional Chinese medicine (TCM) rehabilitation therapies such as moxibustion,9 scraping,10 cupping,11 and Chinese massage12 can significantly alleviate pain and improve low back dysfunction in LBP patients. Recent studies indicate that combining multiple therapy techniques is more effective that a single one.13–16 Therefore, the combined application of multiple TCM rehabilitation techniques may improve the treatment efficacy.
Wentong Guan Therapy (WTG), a non-drug treatment therapy, has been used for various pain and dysfunction conditions in China.17–19 Wentong Guan Therapy is an external TCM technique that that integrates TCM principles of Chinese massage, moxibustion, scraping, and cupping, and thus particularly effective for LBP,20–22 as shown in Figure 1. It exerts its effects through multiple links. When the moxa stick in WTG is ignited, it releases heat, which raises the temperature inside the cup to form negative pressure. The lower opening of the cup adheres to the muscle surface, enabling the functions of cupping and moving cup. When the opening of the cup is repeatedly scraped on the muscle surface, sha spots appear, realizing the function of gua sha (scraping therapy). By using the protrusions on the cup body and the edge of the cup’s lower opening to perform manipulations such as pushing, pressing, pointing, kneading, plucking, and rolling, the function of massage can be achieved.
 |
Figure 1 Wentong Cup. |
Recent studies have primarily focused on patient self- reports, physical examinations, and some serological analyses.21,23 There is a notable lack of neuroimaging research on the mechanism by which WTG regulates brain activity in patients with ANSLBP.
The pain signals caused by low back pain are transmitted in the brain through two pathways, namely the lateral transmission system and the medial transmission system, which convey pain sensory information and emotional information respectively. With the advancement of modern imaging technology, it has been found that abnormal activities in brain regions responsible for sensory, emotional, and cognitive functions are closely associated with acute low back pain. This, to a certain extent, confirms the pain modulation effect of the brain center on LBP-related disorders, including ANSLBP.24 Some scholars have proposed the “low back pain cortex” theory, pointing out that the excitability of the sensorimotor cortex is reduced in patients with acute low back pain,25,26 and the brain activation areas are mainly located in the prefrontal cortex, insula, cingulate cortex, and other regions.27 This suggests that the brain center plays an important role in ANSLBP.
Functional magnetic resonance imaging (fMRI), a classic neuroimaging evaluation technique, accurately records pain-related brain activity.28 However, fMRI requires limiting head and body movement and involves lengthy detection times making it unsuitable for long-term monitoring of patients with LBP. Recently, functional near-infrared spectroscopy (fNIRS), has emerged as a robust non-invasive functional neuroimaging technology with strong resistance to head movements. Compared to electroencephalogram (EEG) and other techniques, fNIRS offers superior robustness and has been increasingly utilized in brain functioning research.
The fNIRS technology measures changes in brain activity and metabolism by detecting concentrations of oxygenated hemoglobin (HbO2) and deoxygenated hemoglobin (HbR) in the cerebral cortex.29 This provides a new method for exploring the brain effect mechanisms underlying WTG. Based on our previous clinical observations and literature review, we hypothesize that WTG can alleviate pain symptoms in patients with acute non-specific low back pain ANSLBP by modulating the brain activity of the somatosensory cortex and prefrontal cortex. In this study, we used fNIRS to assess the cerebral hemodynamic responses of patients with ANSLBP before and after WTG treatment. This approach aims to deepen our understanding of the neurophysiological mechanisms of WTG, thus providing a stronger scientific basis for its clinical application.
Materials and Methods
Participants
We recruited twelve patients diagnosed with ANSLBP who visited the Rehabilitation Department of the Second Affiliated Hospital of Tianjin University of Traditional Chinese Medicine from November 11, 2024 to February 25, 2025, based on the following criteria:
Inclusion Criteria
- Diagnosis of ANSLBP with symptoms persisting for less than six weeks.
- Age between 18–75 years and right-handed, as determined by Edinburgh Handedness Inventory.
- Average Visual Analogue Scale (VAS) score ≥3 over the past week.
- No receipt of other related treatments for ANSLBP in the past month.
- No history of discectomy or other related surgeries.
- Willingness to accept and comply with the treatment schedule and to sign the informed consent form.
Exclusion Criteria
- Presence of scoliosis, ankylosing, spondylitis, bone tuberculosis, tumors, severe osteoporosis, and other orthopedic diseases, or history of acute pain from other causes in the past month.
- 2 History of severe spinal trauma and spinal surgery.
- Contact allergy or moxa smoke allergy.
- Skin damage, allergy, infection, or other conditions at the treatment site unsuitable for WTG.
- Head deformities, scalp damage, inability to wear headgear, or poor fNIRS signals in pre-acquisition.
- Presence of autoimmune diseases, allergic diseases, acute or chronic infectious diseases, or serious medical or mental diseases such as cardiovascular, hematological, and digestive system diseases.
- Participation in other clinical research within the past week.
This research protocol was approved by the Ethics Review Committee of the Second Affiliated Hospital of Tianjin University of Traditional Chinese Medicine (No.2024–032-01). The protocol has been registered with the International Traditional Medicine Clinical Trial Registry and conducted in accordance with the Declaration of Helsinki (ITMCTR2024000666). Written informed consent was obtained from all participants.
Study Procedure
Participants underwent resting-state and task-based fNIRS scans at two time points: baseline and after one treatment session. Patients were also asked to rate their pain intensity using a VAS. Before the task-based scan, the doctor applied pressure on the patient’s low back tender points to determine the pressure pain threshold, using thois intensity for task-based scan. The test sequence was as follows: resting-state scan, VAS score assessment, pressure pain threshold determination, and task-based scan, as shown in Figure 2.
 |
Figure 2 The procedure of the experiment. |
WTG Treatment
All WTG treatments were administered by a doctor with five years of operating experience in this technique. The patient was instructed to lie prone, and Vaseline was evenly applied to the lower back. The doctor then inserted a moxa stick into the fixing clip at the center of the Wentong Cup and ignited, allowing it to preheat for five minutes. The cup was then placed at an angle against the skin, and the doctor performed scraping along the Du Meridian from bottom to top using a flat push method. This was then followed by scraping from top to bottom along the bilateral bladder meridian until the skin exhibited redness or Sha. Subsequently, the cup was pressed flatly against the skin around Dachangshu (BL25) and Shenshu (BL23), and was rotated and moved in a regular pattern. These were then followed by a press and knead at the acupoints with a dentate of the lower edge of the Wentong cup, as shown in Figure 3. Each treatment session lasted 20 minutes. No adverse events were reported during the WTG treatment study period.
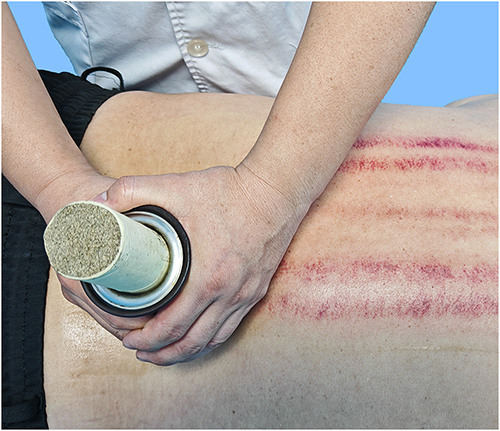 |
Figure 3 Treatment of ANSLBP patient using WTG. |
VAS Score and Pressure Pain Threshold Test
After systematic training and examination, an independent doctor conducted the VAS score assessment and pressure pain threshold test. Patients rated their current pain on a scale from 0 (no pain) to 10 (pain severe enough to seriously affect their lives).
The pressure pain threshold test was performed using an intelligent mechanical collection glove (SK-HTA-01, Guangzhou Shuangkong Technology Co., Ltd). Patients were placed in a prone position with the lower back skin exposed and they were instructed to relax. The doctor identified the most obvious palpable response in the distribution area of the erector spinae myofascial trigger point on the affected side of the patient’s lumbar region30 and marked the spot. If the patient’s pain did not show a lateral tendency, the left lower back was pressed.
The doctor wore the intelligent mechanical collection glove on the right hand, positioning the thumb perpendicular to the patient’s skin surface, and applied pressure slowly and at a constant speed, as shown in Figure 4. When the patient’s pain perception reached a VAS score of five,31,32 the screen value was recorded. The pressure pain threshold test was performed three times, and the average of these results was taken as the final measurement.33 Measurement locations were consistent before and after treatment.
 |
Figure 4 SK-HTA-01 was used to record pain values. (a) Using SK-HTA-01 to press the lower back. (b) The inside of SK-HTA-01 glove. (c) The outside of SK-HTA-01 glove. |
Functional Near-Infrared Spectroscopy Detection and Data Preprocessing
Device Information
A portable fNIRS device (NirSmart II-3000A, Danyang Huichuang Medical Equipment Co., Ltd.) was used to monitor real-time changes in the cerebral cortex HbO2 and HbR. The device included 21 light sources and 15 detectors, forming a total of 47 channels. The arrangement of light sources, detectors, and channels are shown in Figure 5. Following the international standard 10/20 electrode placement system, the setup covered the forehead and bilateral sensorimotor areas. The light source probes used wavelengths of 730nm and 850nm, with a sampling rate of 11Hz. To ensure high-precision data collection, the detector and light source were fixed with black headgear. The average distance between each detector and light source was set to 30 mm. The headgear was adjusted to ensure direct contact between the detectors, light sources, and the scalp. Patients were instructed to close their eyes and avoid engaging in any cognitive activities during the measurement.
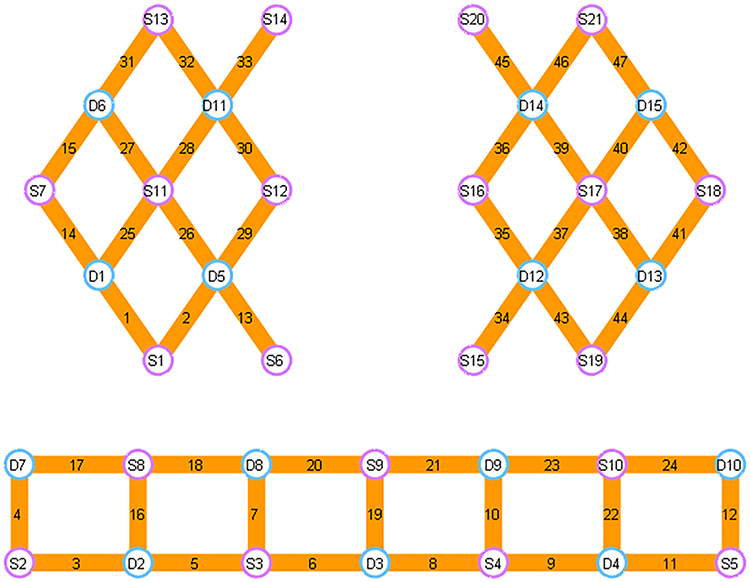 |
Figure 5 Arrangement of light sources, detectors, and channels. |
Resting-State Data Acquisition
Before starting the test, the patient must rest for 5 minutes to adapt to the examination room environment, after which the examination can proceed. Resting-state data should be collected for 8 minutes per session. During the test, patient remains still, avoids cognitive activity, and keeps their eyes closed but must not fall asleep. Resting-state fNIRS measurements were conducted on all patients before and after WTG treatment.
Task-Based fNIRS Data Acquisition
The procedure is divided into two phases: the preparation period and the task period. During the preparation period, the patient remained quiet for 20 seconds. In the task period, the doctor performed “pressing” or “rest” according to the fNIRS system instructions. During the rest phase, the subject remained quiet and minimized cognitive activity. The doctor applied pressure with the intensity measured in the Pressure Pain Threshold Test. Both the compression and rest phases lasted 20 seconds each and were alternated eight times. All patients underwent a task-based fNIRS assessment before and after treatment. The task paradigm is shown in Figure 6.
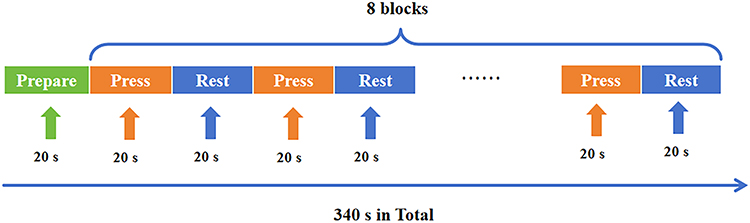 |
Figure 6 The examination procedure of the task-based fNIRS. |
Data Processing
Preprocessing
The fNIRS data were preprocessed using the NirSpark software package (v1.8, Danyang Huichuang Medical Equipment Co., Ltd)., which has been validated in previous studies.34,35 The preprocessing steps included: First, converting raw fNIRS light intensity data into optical density signals. Secondly, detecting and monitoring motion artifacts caused by head movements.36 Thirdly, the optical density signals were filtered with a bandpass filter from 0.01 to 0.1 Hz. Lastly, the filtered optical density signals were converted into relative concentrations of HbO2 and HbR using the modified Beer⁃Lambert law.37 Due to superior signal-to-noise ratio of HbO2 compared to HbR, only the HbO2 data were used for subsequent analysis.38 For patients with the compression site on the right side, data were mirror-flipped across the left and right brain area channels to standardize the compression site as being on the left.
Analysis of HbO2 Concentration Changes
The changes in HbO2 concentration (ΔHbO2) during the compression task and the rest phase were quantified using feature value editing. A one-sample t-test was used to identify channels exhibiting significant ΔHbO2 before and after treatment. A two-sample t-test was used to compare the ΔHbO2 before and after treatment.
Brain Network Functional Connectivity Strength Analysis
Region of Interest (ROI) were defined as detailed in Table 1. Pearson correlation analysis was used to calculate the correlation of HbO2 concentration changes between different channels and ROIs for the resting state. These correlation values were then converted into z-scores using the Fisher r-z transformation and defined as functional connectivity strength.
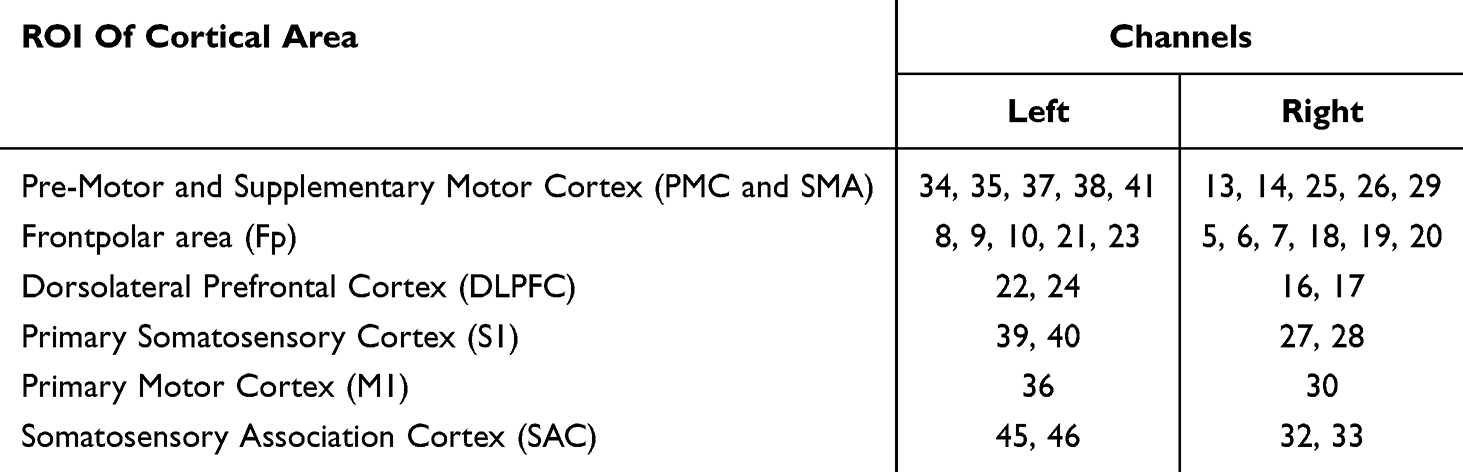 |
Table 1 ROI Settings and Channel Correspondence Table |
Statistical Analysis
Statistical analysis was conducted using SPSS software version 23.0 (IBM SPSS Inc., Chicago, IL, USA). Quantitative data were expressed as mean ± standard deviation ( ± s). The Shapiro–Wilk test was used to assess the normality of the data distribution. For comparisons before and after treatment, paired t-tests were used at p<0.05. Spearman correlation analysis was performed to examine the relationship between HbO2 concentration and clinical data. Multiple comparisons were corrected using the false discovery rate (FDR) method (p < 0.05), thereby adjusting for potential false positives in all results rejecting the null hypothesis.39
± s). The Shapiro–Wilk test was used to assess the normality of the data distribution. For comparisons before and after treatment, paired t-tests were used at p<0.05. Spearman correlation analysis was performed to examine the relationship between HbO2 concentration and clinical data. Multiple comparisons were corrected using the false discovery rate (FDR) method (p < 0.05), thereby adjusting for potential false positives in all results rejecting the null hypothesis.39
Results
Clinical Data
A total of twelve patients with ANSLBP were recruited for the study. The cohort had a mean age of 51.2±15.0 years, ranging from 30 to 72 years, including eight males and four females, all of whom were right-handed. The Body Mass Index (BMI) was 22.97±3.62 kg/m2. Table 2 presents detailed information on each patient’s stimulation side, BMI, VAS scores, and pressure values before and after treatment.
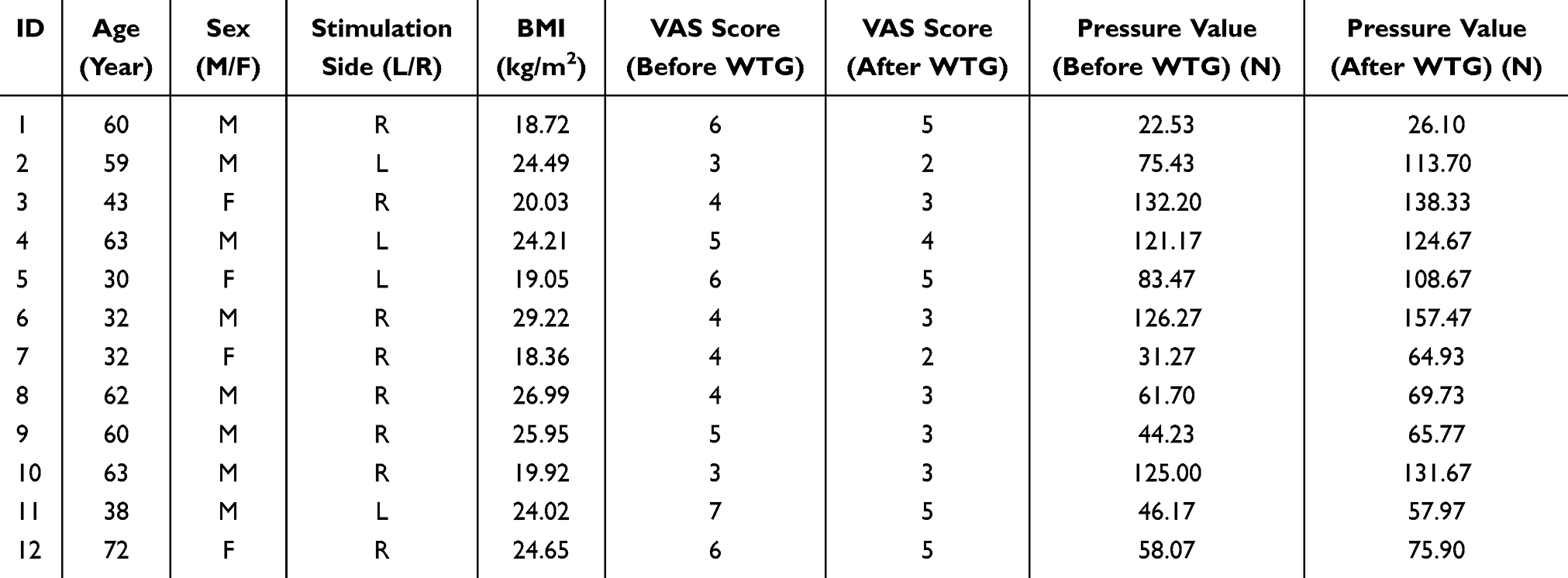 |
Table 2 Demographic Information and Clinical Behavioral Measurement of Participants |
Treatment with the WTG approach had significant effect on both VAS scores and pressure values. As shown in Figure 7, the mean VAS score pos-treatment was 3.58±1.17 (95% Confidence Interval [CI], 2.84 to 4.32), significantly lower than pre-treatment mean VAS score of 4.75±1.29 (95% CI, 3.93 to 5.57), with a t-value of 7.000 and p<0.001. The mean difference in VAS scores was 1.17±0.58 (95% CI, 0.80 to 1.53).
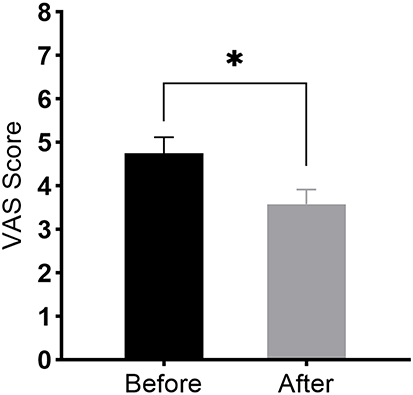 |
Figure 7 The VAS Score between before and after treatment. * P<0.001. |
The pressure values, determined by the average compression measured by mechanical gloves, also showed significant. As shown in Figure 8, the mean pressure value post-treatment was 94.58±39.79 N (95% CI, 51.99 to 102.60), significantly higher than mean pressure value pre-treatment of 77.29±39.83 N (95% CI, 69.29 to 119.86) with a t-value of 4.796 and p<0.001. The mean difference in pressure values was −17.28±12.48 N (95% CI, −25.21 to −9.35).
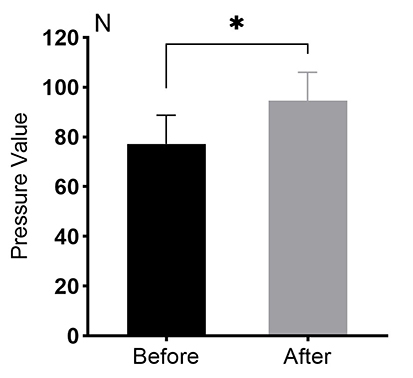 |
Figure 8 The Pressure Value between before and after treatment.* P<0.001. |
Functional Near-Infrared Spectroscopy Data
Reduction in the Strength of Functional Connectivity
The Pearson correlation coefficient, calculated from the HbO2 concentration data, was transformed using the Fisher r-z transformation to define the functional connectivity between channels and ROIs. By analyzing the z-scores of each pair of channels in the time series, a 47×47 correlation matrix was generated for each patient. The results showed that the overall functional connection strength between the channels of the patients was 0.28±0.13 pre-treatment and 0.22±0.10 post-treatment, showing a downward trend (Figures 9 and 10). However, these differences did not remain significant after correction for multiple comparisons (PFDR>0.05).
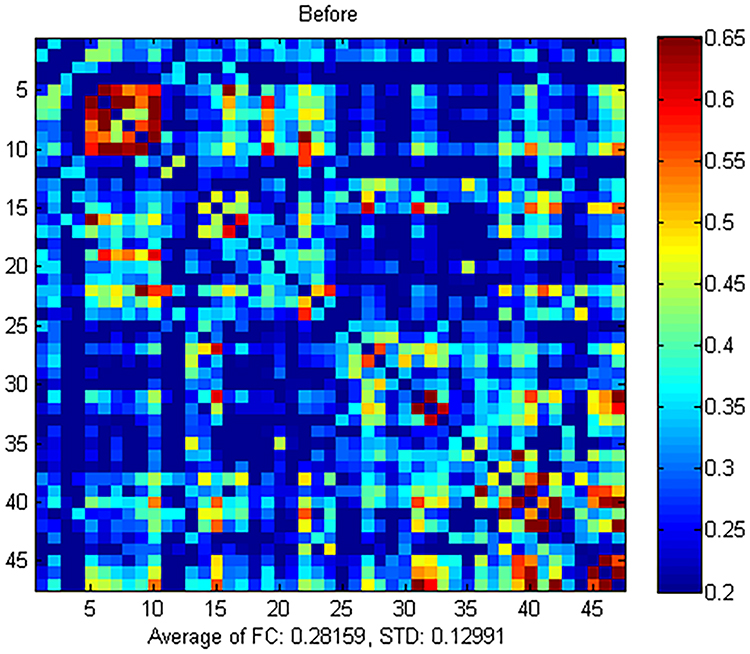 |
Figure 9 Functional connectivity strength between channels before treatment. |
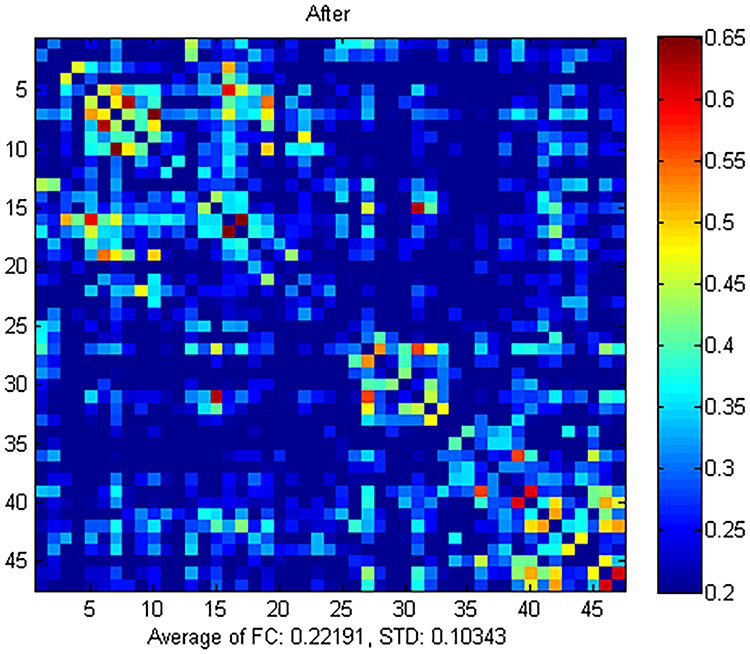 |
Figure 10 Functional connectivity strength between channels after treatment. |
At the ROI level, the bilateral Pre-Motor Cortex (PMC), Supplementary Motor Area (SMA), Frontpolar area (Fp), Somatosensory Association Cortex (SAC), and left Dorsolateral Prefrontal Cortex (DLPFC) all exhibited a decrease in the functional connectivity strength of the homologous ROIs. However, the differences did not pass the FDR correction (PFDR>0.05), as detailed in Supplementary Table 1. For the functional connectivity between ROIs, most connections demonstrated a downward trend, except for an increasing trend observed in the functional connectivity strength between the right DLPFC and the right PMC and SMA, bilateral M1, right SMA, and between the right Fp and the right M1 region. However, none of these results remained significant after FDR correction (PFDR>0.05) as shown in Figures 11, 12, and Supplementary Table 2.
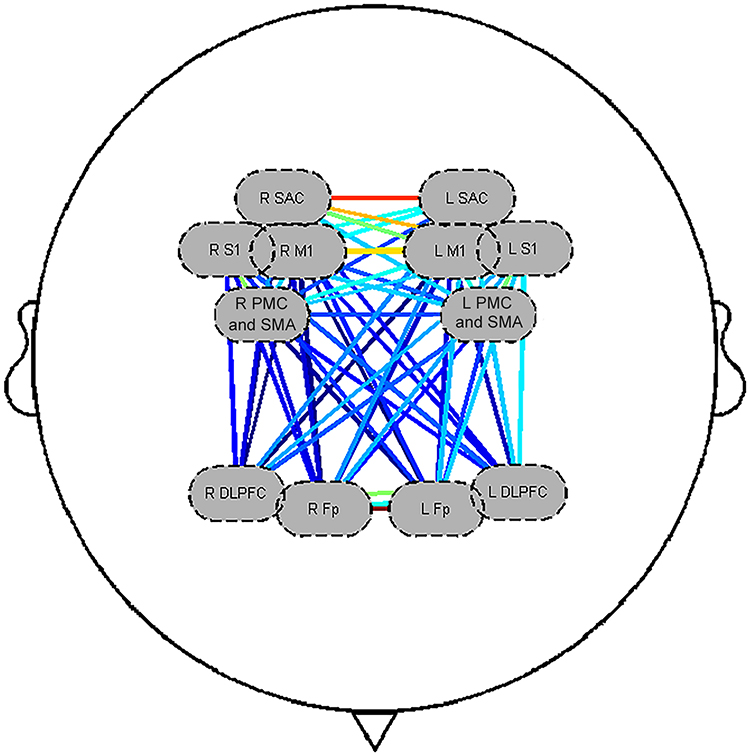 |
Figure 11 Functional connectivity strength between ROIs before treatment. Abbreviations: R, Right; L, Left; DLPFC, Dorsolateral prefrontal cortex; SAC, Somatosensory Association Cortex; PMC and SMA, Pre-Motor and Supplementary Motor Cortex; Fp, Frontopolar area; S1, Primary Somatosensory Cortex; M1, Primary Motor Cortex. |
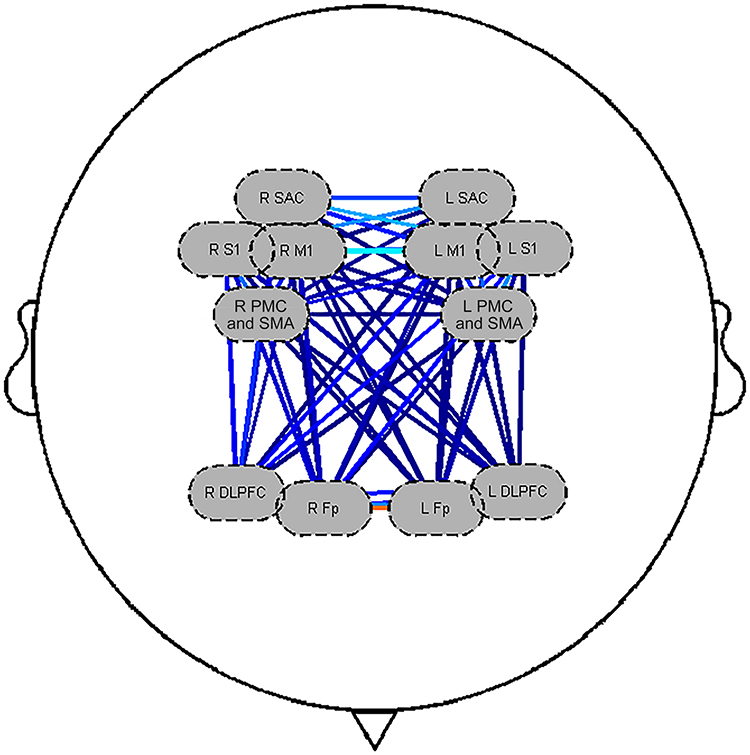 |
Figure 12 Functional connectivity strength between ROIs after treatment. Abbreviations: R, Right; L, Left; DLPFC, Dorsolateral prefrontal cortex; SAC, Somatosensory Association Cortex; PMC and SMA, Pre-Motor and Supplementary Motor Cortex; Fp, Frontopolar area; S1, Primary Somatosensory Cortex; M1, Primary Motor Cortex. |
ΔHbO2 Concentration Reduction
One-sample t-test results showed that the ΔHbO2 concentration in Channel (CH) 17 was 0.029±0.022 mmol/L*mm before WTG treatment, and the difference was statistically significant (t=4.505, PFDR=0.042), as shown in Figure 13. However, there was no statistical significant difference in ΔHbO2 concentration in all channels after treatment (PFDR>0.05), as shown in Figure 14. The ΔHbO2 concentration in CH33 was 0.011±0.017 mmol/L*mm before treatment, while the concentration after treatment was −0.004±0.022 mmol/L*mm. The results of the paired t-test showed that the difference in ΔHbO2 concentration in CH33 before and after treatment was statistically significant (t=4.571, PFDR=0.038), as shown in Figure 15. The corresponding brain regions and MNI coordinate information of the channels are shown in Table 3.
 |
Table 3 The Detailed Information on CH17 and CH33 |
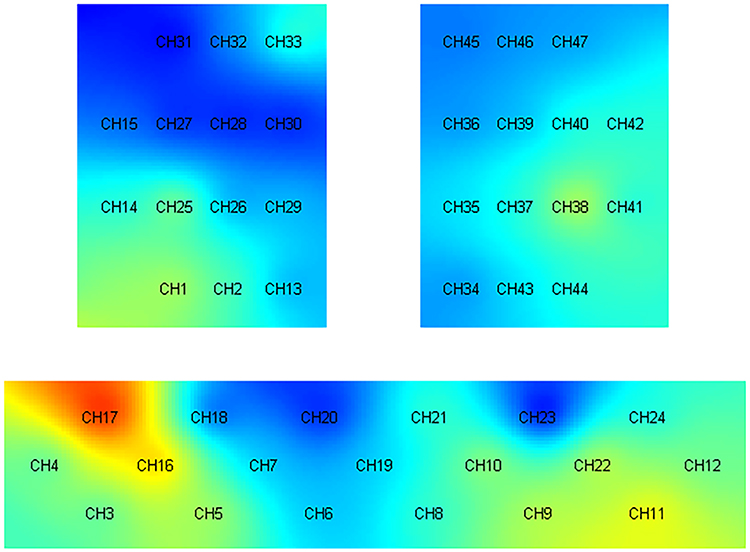 |
Figure 13 T value diagram of ΔHbO2 concentration in each channel before treatment. |
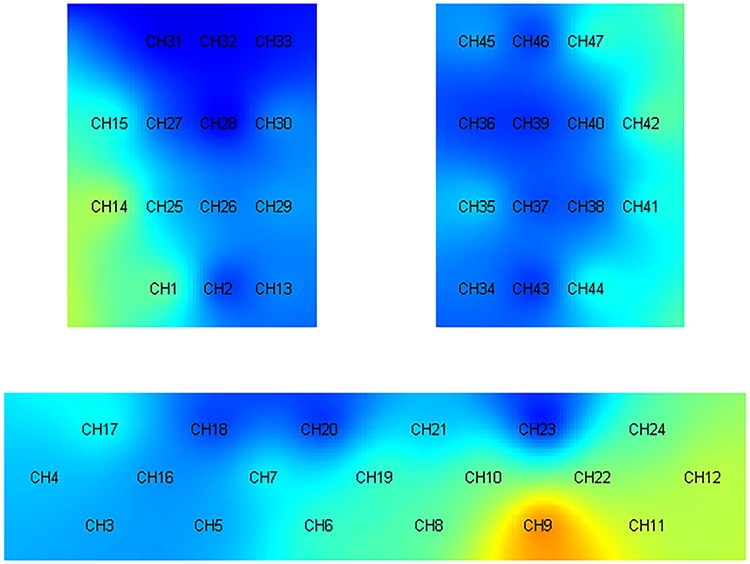 |
Figure 14 T value diagram of ΔHbO2 concentration in each channel after treatment. |
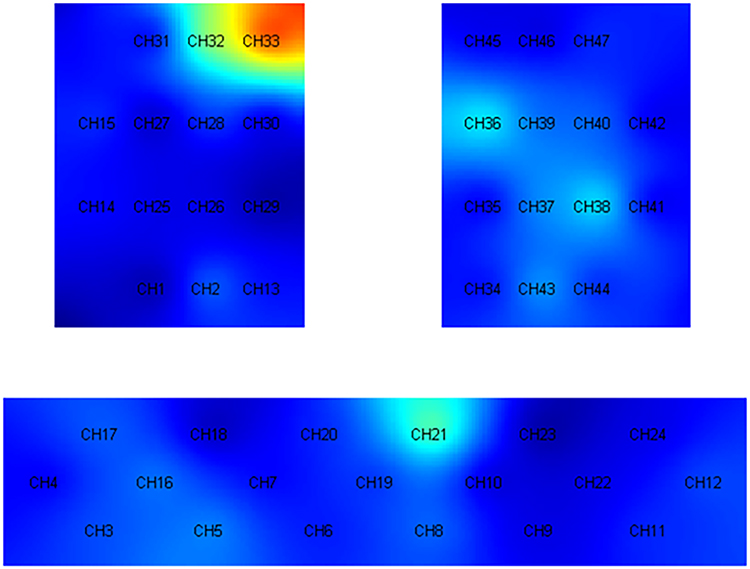 |
Figure 15 T value diagram of ΔHbO2 concentration difference in each channel before and after treatment. |
Correlation Between Clinical Data and ΔHbO2 Concentration
The WTG was found to reduce the ΔHbO2 concentration in CH33 during the pressing task and also increase the pressing pain threshold. To quantify these effects, we calculated the ΔHbO2 concentration for CH33 and the change in pressure pain threshold before and after treatment. To reveal the correlation between the difference in pain threshold and the change in HbO2 concentration, Spearman correlation analysis was conducted. The results showed that there was a significant negative correlation between the change in ΔHbO2 concentration and pressure pain threshold (P=0.045, r= −0.587), as shown in Figure 16.
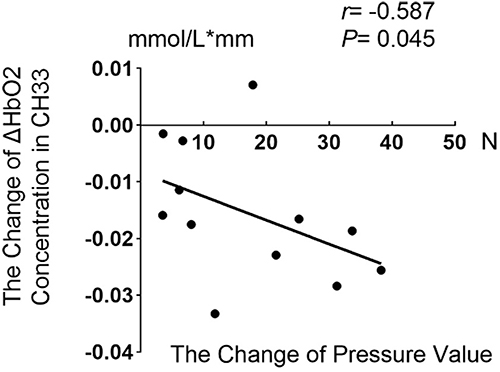 |
Figure 16 Correlation analysis between ΔHbO2 Concentration and Pressure Value. |
Discussion
To the best of our knowledge, this study is the first to use fNIRS to investigate the effects of WTG on brain function in ANSLBP patients. We examined the analgesic effect of WTG therapy, changes in ΔHbO2 concentration, and impacts on functional connectivity in 12 ANSLBP patients using a pre-post treatment design. Data analysis revealed a significant decrease in ΔHbO2 concentration in SAC (CH33) following WTG treatment. Additionally, the analysis of VAS score and pressure value of the patients showed significant pain relief for these patients. All these changes indicate that WTG has a significant effect on analgesics in ANSLBP patients. Moreover, we also found that the DLPFC (CH17), a brain region that exhibited significantly increased activity in response to pressure before treatment, did not show a significant response after treatment. This suggests that the DLPFC, along with the SAC, may be key brain regions involved in the pain modulation mechanism of WTG therapy in ANSLBP patients.
Over the years, the American College of Physicians has recommended non-drug therapies such as massage and spinal manipulation for the treatment of ANSLBP.40,41 Several systematic reviews have also confirmed the positive effects of massage on pain relief and functional improvement in LBP patients.12,42–45 In essence, the brain effect mechanisms of non-drug therapies are gradually being applied. Research has also established that Chinese massage therapy affects brain activity, mainly in the DLPFC, inferior frontal gyrus, posterior cingulate gyrus, and postcentral gyrus of patients with LBP.32,46
Markowski47 investigated the effects of cupping therapy on subacute LBP, and the results demonstrated that cupping can reduce muscle tenderness and improve joint range of motion. Also, a systematic review involving 10 randomized controlled trials with a total of 627 patients,48 confirmed scrapping therapy significantly reduces pain in LBP patients and continuously improve lumbar function both at the end of treatment and during follow-up. Lee et al49 obtained similar findings. Currently, several systematic reviews that have validated the efficacy and safety of moxibustion for LBP.9,50,51 Utilizing technologies such as fNIRS, and EEG, researchers have found that moxibustion treatment can significantly increase cerebral cortical blood flow, increase blood oxygen concentration, with widespread EEG responses observed in areas such as the prefrontal lobe, Primary somatosensory cortex (S1), secondary somatosensory cortex, and cingulate cortex.52–54 Studies by Lee et al found that acupuncture can reduce the functional connectivity between the medial prefrontal cortex and the posterior cingulate cortex, thereby alleviating low back extension pain.55 Kim’s research revealed that acupuncture can improve somatosensory processing and relieve low back pain.56 Li et al discovered that the mechanism by which acupuncture relieves sciatica may be related to the reduced activity of the DLPFC and the anterior cingulate cortex, which is similar to the results of this study.57
These studies support the effectiveness of complementary and alternative medicine methods including spinal manipulation, massage, acupuncture, and moxibustion in the treatment of LBP.40 ANSLBP is the interaction between physical dysfunction and psychological and social factors.58 Consequently, the multidisciplinary rehabilitation approach for ANSLBP is increasingly being adopted. Among these therapies being adopted is the WTG which is a combination of treatment with better efficacy than single therapy.13–16 In this study, WTG demonstrated significant analgesic effects. Neuroimaging studies have found that low back pain changes the spatiotemporal dynamics of blood oxygen level-dependent (BOLD) signals in response to sustained noxious stimulation, involving sensory, emotional, cognitive, and other functional networks.24,59 The mechanisms by which complementary and alternative therapies such as Chinese massage and moxibustion treat LBP have been revealed through neurofunctional imaging, highlighting the adaptation of the central nervous system to regulate and maintain LBP pain processing.32,60 However, the mechanisms underlying the efficacy of WTG remain unclear. Existing research is primarily based on patient self-reports, physical examinations, and some serological studies.21,23 The regulatory mechanisms of WTG on the brain in ANSLBP patients are yet to be fully understood.
Pain is not solely the result of sensory input directly caused by injury, inflammation, or other pathologies.61 Instead, it is caused by the activation of cognitive, emotional, and motor networks after injury, and is the output of widely distributed neural networks in the brain.62,63 Therefore, pain is an experience related to actual or potential tissue damage, which includes multiple components such as sensation, emotion, cognition, and movement.64 Our study observed a statistically significant difference in the decrease in ΔHbO2 concentration in SAC (CH33) during pressure application before and after WTG treatment. This area is generally considered to integrate and interpret somatosensory information from S1 and is involved in the comprehensive processing of somatosensory information, including pain perception.65–67 This finding is consistent with Matsuo et al’s study68 which found that LBP patients showed deactivation in large areas of the bilateral parietal lobes (including the upper part) under pressure stimulation. Previous fMRI studies have shown that BOLD signal inactivation reflects the inhibition of neuronal activity.69,70 Given that BOLD signal is related to changes in hemoglobin concentration,71 the observed reduction in ΔHbO2 response in this study may indicate potential inhibition of neural activity. A study involving lumbar compressions in healthy volunteers72 observed significant changes in HbO2 concentrations in S1 and SMA. Another study involving LBP patients showed73 that hemodynamic activity in the somatosensory area was significantly reduced when pain was alleviated. These findings suggest that pain relief in ANSLBP patients may be related to the inhibition of neural activity in the somatosensory association cortex. This inhibition could represent the brain mechanism underlying the efficacy of WTG in treating low back pain.
The prefrontal cortex is important in human cognition, emotion, and executive function, and is also plays a significant role in pain processing.74–76 Kobayashi’s study showed77 that pressing stimulation activates the contralateral prefrontal cortex, with stronger activation in LBP patients compared to healthy volunteers. DLPFC is involved in higher-order cognitive functions related to attention, working memory, response inhibition, and information processing.78 It plays a key role in the top-down regulation of pain perception and is also an important brain region involved in pain regulation in patients with LBP.79,80 In this study, significant results in ΔHbO2 concentration were observed in CH17 (DLPFC) before treatment, whereas post-treatment compression did not elicit a significant response in this region. This suggests that the DLPFC is engaged in responding to pressure pain, requiring increased neural resource recruitment. During the acute phase of pain, the DLPFC utilizes more cognitive resources to manage pain, resulting in a significant response.81 Previous studies have shown82,83 that reduced activation in the DLPFC, orbitofrontal cortex, anterior cingulate cortex, and other regions may be associated with pain relief. In this study, the patients’ pain was relieved after treatment, and the ΔHbO2 concentration of DLPFC caused by pressing decreased compared to that before treatment, which suggest that WTG inhibited the activation of DLPFC and reduced the unpleasant emotional experience caused by pain.84 This diminishes the ability of DLPFC to sense pain and produce an analgesic effect. However, the post-treatment ΔHbO2 concentration changes in the DLPFC did not remain significant after FDR correction, likely due to the small sample size of this study.
Resting-state brain networks differ between LBP patients and healthy volunteers.85 One study had shown,86 that when the default mode network (DMN) connection is frequent, then a person becomes more sensitive to pain. This study found that before and after WTG, the functional connection strength between channels and ROI demonstrated an overall downward trend, but the results do not apply for multiple comparisons. We suggest that the immediate effect of a single WTG treatment does not cause significant brain network changes. However, cumulative effects can occur after long-term and multiple WTG treatments resulting in significant changes in the brain network.32,46 Additionally, SAC and DLPFC may be key brain network nodes in WTG analgesia.
Current pain assessment methods are limited to self-reporting, mainly including VAS scores and McGill Pain Questionnaire (MPQ), which may lead to objective pain assessment.87 This study implemented an innovative approach to pain assessment using a mechanical testing glove (SK-HTA-01). The glove objectively measures pain by recording three force values. Averaging these values minimizes measurement error and enhances the reliability of the data. In previous studies, the use of real-time compression as a mechanical stimulus to determine the pain threshold of the subject was reported.32,88 Another study77 found that under pressure stimulation, the pain threshold of LBP patients was lower than that of healthy subjects, that is, when experiencing the same degree of pain, the pressure used to press on LBP patients is less. Matsuo et al68 used a fixed pressure value to stimulate the low back to induce pain. In this study, we employed a similar method to apply pressure as Tan,32 in which fixed pressure value was not used, but used the same pain sensation subjectively felt by the subjects (ie., VAS = 5). However, we believe that the same pressure may produce different subjective pain perceptions in different subjects, especially in subjects with different pain perceptions and genders.89,90 This may introduce confounding variables that affect the findings from brain function research.
This study demonstrates that the ΔHbO2 concentration in CH33 (SAC) during the compression task changes significantly before and after treatment. Therefore, the correlation between the ΔHbO2 concentration change on CH33 and the pressure pain value was calculated to explore the correlation between pain perception and brain activity. We found that the Δ HbO2 concentration was negatively correlated with the pressure change value. As the pressure change value increased, the spontaneous neural activity of SAC in patients decreased significantly. This suggests that clinicians can objectively predict the pain level of ANSLBP patients based on the changes in ΔHbO2 concentration in this area. As a relatively newer neuroimaging technology, ΔHbO2 concentration detected by fNIRS offers an important brain biomarker for objective assessment of acute pain and prediction of pain relief. However, such potential biomarkers need to be validated before they can be applied in clinical practice.
Limitation
This study has some potential limitations. Firstly, the longitudinal effect of WTG treatment on brain pain processing over time cannot be studied after only one treatment. Secondly, the sample size of our study was small, and hence complex statistical analyses and subgroup analyses could not be performed. In future, researchers should observe the activity of brain function of ANSLBP patients treated with WTG by expanding the sample size, long-term intervention longitudinal study, and setting up the sham WTG and healthy volunteer groups. In addition, we employed the Pearson correlation coefficient to calculate functional connectivity, which may not reveal the causal relationship between brain area activities. In the future, Granger causality analysis should be adopted to further quantify the strength of effective connectivity between brain regions, as this will be more helpful in revealing the brain mechanism of WTG efficacy.
Conclusion
This study found that WTG can relieve the pain symptoms of ANSLBP patients. Although WTG is a commonly employed TCM for the treatment of pain, the potential mechanism neuromodulatory effect of WTG on the human brain need to be further clarified. In this study, multi-channel fNIRS recordings were performed before and after WTG treatment, and the results showed that WTG decreased Δ HBO2 concentration in the contralateral SAC during compression. We speculate that the mechanism of the analgesic effect of WTG may be related to the inhibition of neuronal activity in the SAC of the brain. By examining the relationship between pressure changes and ΔHbO2 concentration, we discovered that a decreased ΔHbO2 concentration could serve as a potential biomarker for the analgesic effect of WTG. Our research offers objective neuroimaging evidence to elucidate WTG’s neuromodulatory impact on the human brain and provides a methodological reference for studying the brain mechanisms underlying the efficacy of Complementary and Alternative Medicine.
Based on the regulatory effects of WTG on pain-related brain regions and the subjective analgesic effects observed in patients with acute non-specific low back pain ANSLBP in this study, it is initially confirmed that WTG has the potential to serve as a non-pharmacological pain intervention method. It can alleviate pain through the “warming and unblocking” effect, providing a more diverse non-pharmacological option for clinical pain management.
Given that this study adopts a single-group design without a sham control group, it has limitations in that confounding factors such as the placebo effect and natural recovery cannot be completely ruled out. Future studies can set up a “sham WTG group”, which simulating only cupping/massage operations without actual warming and unblocking effects, to more accurately distinguish the specific efficacy of WTG from non-specific effects. Meanwhile, a multi-session design can better align with the actual clinical treatment process, which helps observe the persistence of WTG’s regulatory effect on brain activity and its long-term analgesic effect, and reduces the potential randomness of results caused by a single intervention.
Abbreviations
ANSLBP, Acute non-specific low back pain; BMI, Body Mass Index; BOLD, blood oxygen level-dependent; CH, Channel; CI, Confidence Interval; DLPFC, Dorsolateral Prefrontal Cortex; DMN, Default mode network; EEG, electroencephalogram; FDR, false discovery rate; fMRI, Functional magnetic resonance imaging; fNIRS, Functional near-infrared spectroscopy; Fp, Frontpolar area; Δ HBO2, The changes in HBO2 concentration; HBO2, oxygenated hemoglobin; HbR, deoxygenated hemoglobin; LBP low back pain; M1, Primary Motor Cortex; MPQ, McGill Pain Questionnaire; NSAIDs, non-steroidal anti-inflammatory drugs; PMC and SMA, Pre-Motor and Supplementary Motor Cortex; ROI, Region of Interest; S1, Primary Somatosensory Cortex; SAC, Somatosensory Association Cortex; TCM, Traditional Chinese medicine; VAS, Visual Analogue Scale; WTG, Wentong Guan Therapy.
Data Sharing Statement
We plan to share de-identified individual participant data, including participants’ demographic information, condition-related indicators, treatment parameters, and brain activity data. Data can be obtained by contacting the corresponding author.
Consent Statement
The study participants gave consent to publish.
Acknowledgments
The authors would like to thank all the reviewers who participated in the review and MJEditor (www.mjeditor.com) for its linguistic assistance during the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Tianjin health industry high-level talent selection and training project (TJSJMYXYC-D2-019).
Disclosure
Shifang Fu and Hao Chen are co-first authors for this study. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Johnson SM, Shah LM. Imaging of Acute Low Back Pain. Radiologic Clin North America. 2019;57(2):397–20. doi:10.1016/j.rcl.2018.10.001
2. Oertel J, Sharif S, Zygourakis C, Sippl C. Acute low back pain: epidemiology, etiology, and prevention: WFNS spine committee recommendations. World Neurosurgery: X. 2024;22:100313. doi:10.1016/j.wnsx.2024.100313
3. Deyo RA, Mirza SK, Solomon CG. CLINICAL PRACTICE. Herniated Lumbar Intervertebral Disk. New Engl J Med. 2016;374(18):1763–1772. doi:10.1056/NEJMcp1512658
4. Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica: summary of NICE guidance. BMJ. 2017;356:i6748. doi:10.1136/bmj.i6748
5. Oliveira CB, Maher CG, Pinto RZ, et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J. 2018;27(11):2791–2803. doi:10.1007/s00586-018-5673-2
6. Chou R, Deyo R, Friedly J, et al. Systemic Pharmacologic Therapies for Low Back Pain: a Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann Internal Med. 2017;166(7):2458. doi:10.7326/m16-2458
7. Added MA, Costa LO, Fukuda TY, et al. Efficacy of adding the Kinesio Taping method to guideline-endorsed conventional physiotherapy in patients with chronic nonspecific low back pain: a randomised controlled trial. BMC Musculoskeletal Disorders. 2013;14:301. doi:10.1186/1471-2474-14-301
8. Patrick N, Emanski E, Knaub MA. Acute and chronic low back pain. Med Clin North Am. 2014;98(4):777–89,xii. doi:10.1016/j.mcna.2014.03.005
9. Yao Y, Zhou L, Chen F-Q, et al. The Effect and Safety of Thunder-Fire Moxibustion for Low Back Pain: a Meta-Analysis of Randomized Controlled Trials. eCAM. 2022;2022:6114417. doi:10.1155/2022/6114417
10. Yuen JWM, Tsang WWN, Tse SHM, et al. The effects of Gua sha on symptoms and inflammatory biomarkers associated with chronic low back pain: a randomized active-controlled crossover pilot study in elderly. Complementary Ther Med. 2017;32:25–32. doi:10.1016/j.ctim.2017.03.010
11. Zhang Z, Pasapula M, Wang Z, Edwards K, Norrish A. The effectiveness of cupping therapy on low back pain: a systematic review and meta-analysis of randomized control trials. Complementary Ther Med. 2024;80:103013. doi:10.1016/j.ctim.2024.103013
12. Yang J, Zhou X, Ma Q, et al. Efficacy and safety of Tuina for chronic nonspecific low back pain: a PRISMA-compliant systematic review and meta-analysis. Medicine. 2023;102(9):e33018. doi:10.1097/md.0000000000033018
13. Zhenhua C, Qikai Z, Shuijin C, Xiang L, Xiaowen L. Warming acupuncture combined with “three steps and seven methods” of tuina for chronicnonspecific low back pain of yang deficiency and cold-dampness blockage: a randomized controlled trial. Chin Acupuncture Moxibustion. 2022;42(05):505–510. doi:10.13703/j.0255-2930.20210622-k0001
14. Yujuan H, Lihong K, Wenting F, Yue Z. Application of Teding Dianci Pu therapeutic apparatus and balance cupping in nursing careof patients with cold-dampness low back pain. Chin Nurs res. 2021;35(23):4305–4307.
15. Li S-K, Zhao J, Cao X-W, Zhu S, Liu Z-Q, Fan Y-X. Core stability training combined with acupuncture in treatment of chronic nonspecific low back pain: a prospective randomized controlled trial. Acupuncture Res. 2022;47(2):160–164. doi:10.13702/j.1000-0607.201050
16. Yiliang L, Nan X, Sumin T, Zhiwen W, Shengli G, Hui W. Therapeutic effect of Yaotongning Capsules and thunder-fire moxibustion in treatment of 40 cases of lumbar disc herniation with cold and blood-stasis syndrome. Chin Tradit Herbal Drugs. 2020;51(21):5431–5435.
17. Qingqing C, Yeyan L, Shuang B, et al. Fire dragon cupping in prevention and treatment of chemotherapy-induced nausea andvomiting in breast cancer: a randomized controlled trial. Chin Acupuncture Moxibustion. 2024;44(05):526–530. doi:10.13703/j.0255-2930.20230712-k0005
18. Shuling J, Yijin L, Xiaoqi T, Chunmei Z. Case of Huolong cupping therapy for eczema during pregnancy. Chin Acupuncture Moxibustion. 2024;44(01):48–50. doi:10.13703/j.0255-2930.20230722-k0002
19. Juanxia Z, Juanli Z, Bifang H, Haiyan M. Observation on application effect of fire dragon pot in the nursing of qi stagnation andblood stasis type Xiangbi disease. Chin Nurs Res. 2022;36(20):3755–3757.
20. Juanxia Z, Juanli Z, Bifang H, Haiyan M, Xuhui H. Application of fire dragon cupping treatment for patients with lumbar discherniation. Chin Nurs Res. 2020;34(22):4098–4100.
21. Caiqin W, Xiuying F. Observation on the efficacy of warming and unblocking scraping therapy in the treatment of acute discogenic low back pain. J Emerg Tradit Chin Med. 2021;30(04):698–700.
22. Shan X, Ruxiang Z, MingYan Y. Clinical observation on external application of Huolong Cup combined with Huaidu Zhuangyao Pills for the treatment of lower back pain of kidney deficiency type. Hubei J Tradit Chin Med. 2022;44(01):53–55.
23. Shiting L, Chunrong L. Effect of Huolong Cupping and Comprehensive Moxibustion on Lumbar Function and Inflammatory Reaction in Patients with Lumbar Disc Herniation of Qi Stagnation and Blood Stasis Type. J External Ther Tradit Chin Med. 2022;31(06):6–8.
24. Boendermaker B, Buechler R, Michels L, Nijs J, Coppieters I, Hotz-Boendermaker S. Adaptive changes in sensorimotor processing in patients with acute low back pain. Sci Rep. 2022;12(1):21741. doi:10.1038/s41598-022-26174-2
25. Jenkins LC, Chang W-J, Buscemi V, et al. Low Somatosensory Cortex Excitability in the Acute Stage of Low Back Pain Causes Chronic Pain. J Pain. 2022;23(2):289–304. doi:10.1016/j.jpain.2021.08.003
26. Jenkins LC, Chang W-J, Buscemi V, et al. Cortical function and sensorimotor plasticity are prognostic factors associated with future low back pain after an acute episode: the Understanding persistent Pain Where it ResiDes prospective cohort study. Pain. 2023;164(1):14–26. doi:10.1097/j.pain.0000000000002684
27. Chang W-J, Buscemi V, Liston MB, McAuley JH, Hodges PW, Schabrun SM. Sensorimotor Cortical Activity in Acute Low Back Pain: a Cross-Sectional Study. J Pain. 2019;20(7):819–829. doi:10.1016/j.jpain.2019.01.006
28. Feitosa AA, Amaro Junior E, Sanches LG, Borba EF, Jorge LL, Halpern ASR. Chronic low back pain and sick-leave: a functional magnetic resonance study. Adv Rheumatol. 2020;60(1):46. doi:10.1186/s42358-020-00146-4
29. Miguel HO, Lisboa IC, Gonçalves ÓF, Sampaio A. Brain mechanisms for processing discriminative and affective touch in 7-month-old infants. Development Cgnitiv Neurosci. 2019;35:20–27. doi:10.1016/j.dcn.2017.10.008
30. Calvo-Lobo C, Diez-Vega I, Martínez-Pascual B, et al. Tensiomyography, sonoelastography, and mechanosensitivity differences between active, latent, and control low back myofascial trigger points: a cross-sectional study. Medicine. 2017;96(10):e6287. doi:10.1097/md.0000000000006287
31. Kodama K, Takamoto K, Nishimaru H, et al. Analgesic Effects of Compression at Trigger Points Are Associated With Reduction of Frontal Polar Cortical Activity as Well as Functional Connectivity Between the Frontal Polar Area and Insula in Patients With Chronic Low Back Pain: a Randomized Trial. Front Syst Neurosci. 2019;13:68. doi:10.3389/fnsys.2019.00068
32. Tan W, Wang W, Yang Y, et al. Spinal Manipulative Therapy Alters Brain Activity in Patients With Chronic Low Back Pain: a Longitudinal Brain fMRI Study. Fronti Integrat Neurosci. 2020;14:534595. doi:10.3389/fnint.2020.534595
33. Ben C, Xin Z, Jun R, et al. Study on the characteristics of muscle-bone imbalance and inflammatory infiltration inlumbar disc herniation. China J Tradit Chin Med Pharmacy. 2023;38(10):4959–4963.
34. Deng X, Jian C, Yang Q, Jiang N, Huang Z, Zhao S. The analgesic effect of different interactive modes of virtual reality: a prospective functional near-infrared spectroscopy (fNIRS) study. Front Neurosci. 2022;16:1033155. doi:10.3389/fnins.2022.1033155
35. Zhuang R, Zhu S, Sui Y, et al. Age-Related Differences in Stepping Reactions to a Balance Perturbation: a Functional Near-Infrared Spectroscopy and Surface Electromyography Study. Brain Sci. 2022;12(11):1479. doi:10.3390/brainsci12111479
36. Shu Z, Wu J, Li H, et al. fNIRS-based functional connectivity signifies recovery in patients with disorders of consciousness after DBS treatment. Clin Neurophysiol. 2023;147:60–68. doi:10.1016/j.clinph.2022.12.011
37. Cope M, Delpy DT. System for long-term measurement of cerebral blood and tissue oxygenation on newborn infants by near infra-red transillumination. Med Biol Eng Comput. 1988;26(3):289–294. doi:10.1007/bf02447083
38. Strangman G, Culver JP, Thompson JH, Boas DA. A quantitative comparison of simultaneous BOLD fMRI and NIRS recordings during functional brain activation. NeuroImage. 2002;17(2):719–731. doi:10.1006/nimg.2002.1227
39. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society Series B: Statistical Methodology. 1995;57(1):289–300. doi:10.1111/j.2517-6161.1995.tb02031.x
40. Chou R, Deyo R, Friedly J, et al. Nonpharmacologic Therapies for Low Back Pain: a Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann Intern Med. 2017;166(7):493–505. doi:10.7326/m16-2459
41. Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: a Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/m16-2367
42. Coulter ID, Crawford C, Hurwitz EL, et al. Manipulation and mobilization for treating chronic low back pain: a systematic review and meta-analysis. Spine J. 2018;18(5):866–879. doi:10.1016/j.spinee.2018.01.013
43. Paige NM, Miake-Lye IM, Booth MS, et al. Association of Spinal Manipulative Therapy With Clinical Benefit and Harm for Acute Low Back Pain: systematic Review and Meta-analysis. JAMA. 2017;317(14):1451–1460. doi:10.1001/jama.2017.3086
44. Rubinstein SM, de Zoete A, van Middelkoop M, Assendelft WJJ, de Boer MR, van Tulder MW. Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain: systematic review and meta-analysis of randomised controlled trials. BMJ. 2019;364:l689. doi:10.1136/bmj.l689
45. Wang X-Q, Wang Y-L, Witchalls J, et al. Physical therapy for acute and sub-acute low back pain: a systematic review and expert consensus. Clin rehabilitat. 2024;38(6):715–731. doi:10.1177/02692155241229398
46. Yang Y-C, Zeng K, Wang W, et al. The Changes of Brain Function After Spinal Manipulation Therapy in Patients with Chronic Low Back Pain: a Rest BOLD fMRI Study. <![CDATA[Neuropsychiatric Disease and Treatment]]>. 2022;18:187–199. doi:10.2147/ndt.S339762
47. Markowski A, Sanford S, Pikowski J, Fauvell D, Cimino D, Caplan S. A pilot study analyzing the effects of Chinese cupping as an adjunct treatment for patients with subacute low back pain on relieving pain, improving range of motion, and improving function. The Journal of Alternative and Complementary Medicine. 2014;20(2):113–117. doi:10.1089/acm.2012.0769
48. Wang XQ, Duan PB, Zheng M, Yang LH, Wang AQ, Zhang M. Effect of Scraping Therapy on Chronic Low Back Pain: a Systematic Review and Meta-analysis of Randomized Controlled Trials. J Manipulative Physiol Therap. 2021;44(3):255–270. doi:10.1016/j.jmpt.2020.08.003
49. Lee MS, Choi T-Y, Kim J-I, Choi S-M. Using Guasha to treat musculoskeletal pain: a systematic review of controlled clinical trials. ChinMed. 2010;5(1):5. doi:10.1186/1749-8546-5-5
50. Chen F-Q, Ge J-F, Leng Y-F, Li C, Chen B, Sun Z-L. Efficacy and safety of moxibustion for chronic low back pain: a systematic review and meta-analysis of randomized controlled trials. Complementary Therap Clinical Pract. 2020;39:101130. doi:10.1016/j.ctcp.2020.101130
51. Zhu S, Xiong J, Chen J, et al. The effectiveness of moxibustion for treating of low back pain: a protocol for systematic review and meta-analysis. Medicine. 2020;99(43):e22522. doi:10.1097/md.0000000000022522
52. Hong L, Zhongwei H, Yulan B, Shizhe G. Effects of electric-moxibustion on brain mantle accessed with near infrared-imaging. Chin Acupunct Moxibust. 2010;30(11):925–927. doi:10.13703/j.0255-2930.2010.11.011
53. Liao F, Zhang C, Bian Z, et al. Characterizing heat-sensitization responses in suspended moxibustion with high-density EEG. Pain Med. 2014;15(8):1272–1281. doi:10.1111/pme.12512
54. Wang J, Yi M, Zhang C, et al. Cortical activities of heat-sensitization responses in suspended moxibustion: an EEG source analysis with sLORETA. Cognitive Neurodynamics. 2015;9(6):581–588. doi:10.1007/s11571-015-9349-x
55. Lee J, Eun S, Kim J, Lee J-H, Park K. Differential Influence of Acupuncture Somatosensory and Cognitive/Affective Components on Functional Brain Connectivity and Pain Reduction During Low Back Pain State. Front Neurosci. 2019;13:1062. doi:10.3389/fnins.2019.01062
56. Kim H, Mawla I, Lee J, et al. Reduced tactile acuity in chronic low back pain is linked with structural neuroplasticity in primary somatosensory cortex and is modulated by acupuncture therapy. NeuroImage. 2020;217:116899. doi:10.1016/j.neuroimage.2020.116899
57. Li J, Dong J-C, Yue -J-J. Effects of acupuncture on default mode network images of chronic sciatica patients in the resting network state. Chin J Integrated Traditional Western Med. 2012;32(12):1624–1627.
58. Yutong F, Feng G, Jianjun L. Nonsurgical treatment of nonspecific low back pain. Chin J Rehabil Med. 2017;32(02):240–244.
59. Zhang -S-S, Wu W, Yang J-M, Wang C-H. Abnormal Spontaneous Brain Activity in Acute Low-Back Pain Revealed by Resting-State Functional MRI. Am J Phys Med Rehabil. 2017;96(4):253–259. doi:10.1097/phm.0000000000000597
60. Shi Y, Liu Z, Zhang S, et al. Brain Network Response to Acupuncture Stimuli in Experimental Acute Low Back Pain: an fMRI Study. eCAM. 2015;2015:210120. doi:10.1155/2015/210120
61. Melzack R. Pain and the neuromatrix in the brain. J Dental Educ. 2001;65(12):1378–1382. doi:10.1002/j.0022-0337.2001.65.12.tb03497.x
62. Taylor KS, Davis KD. 128Stability of tactile- and pain-related fMRI brain activations: an examination of threshold-dependent and threshold-independent methods. Human Brain Mapp. 2009;30(7):1947–1962. doi:10.1002/hbm.20641
63. Gelnar PA, Krauss BR, Sheehe PR, Szeverenyi NM, Apkarian AV. 131A comparative fMRI study of cortical representations for thermal painful, vibrotactile, and motor performance tasks. NeuroImage. 1999;10(4):460–482. doi:10.1006/nimg.1999.0482
64. Moayedi M, Davis KD. Theories of pain: from specificity to gate control. J Neurophysiol. 2013;109(1):5–12. doi:10.1152/jn.00457.2012
65. Mackenzie TN, Bailey AZ, Mi PY, Tsang P, Jones CB, Nelson AJ. Human area 5 modulates corticospinal output during movement preparation. Neuroreport. 2016;27(14):1056–1060. doi:10.1097/wnr.0000000000000655
66. Anders S, Birbaumer N, Sadowski B, et al. Parietal somatosensory association cortex mediates affective blindsight. Nat Neurosci. 2004;7(4):339–340. doi:10.1038/nn1213
67. Qi J, Chen J, Huang Y, et al. Acupuncture at Waiguan (SJ5) and sham points influences activation of functional brain areas of ischemic stroke patients: a functional magnetic resonance imaging study. Neural Regenerat Res. 2014;9(3):293–300. doi:10.4103/1673-5374.128227
68. Matsuo Y, Kurata J, Sekiguchi M, Yoshida K, Nikaido T, Konno S-I. Attenuation of cortical activity triggering descending pain inhibition in chronic low back pain patients: a functional magnetic resonance imaging study. J Anesthesia. 2017;31(4):523–530. doi:10.1007/s00540-017-2343-1
69. Shmuel A, Yacoub E, Pfeuffer J, et al. Sustained negative BOLD, blood flow and oxygen consumption response and its coupling to the positive response in the human brain. Neuron. 2002;36(6):1195–1210. doi:10.1016/s0896-6273(02)01061-9
70. Stefanovic B, Warnking JM, Pike GB. Hemodynamic and metabolic responses to neuronal inhibition. NeuroImage. 2004;22(2):771–778. doi:10.1016/j.neuroimage.2004.01.036
71. Steinbrink J, Villringer A, Kempf F, Haux D, Boden S, Obrig H. Illuminating the BOLD signal: combined fMRI–fNIRS studies. Magnet Resonance Iimag. 2006;24(4):495–505. doi:10.1016/j.mri.2005.12.034
72. Vrana A, Meier ML, Hotz-Boendermaker S, Humphreys BK, Scholkmann F. Different mechanosensory stimulations of the lower back elicit specific changes in hemodynamics and oxygenation in cortical sensorimotor areas-A fNIRS study. Brain Behav. 2016;6(12):e00575. doi:10.1002/brb3.575
73. Sorkpor SK, Montero-Hernandez S, Miao H, Pollonini L, Ahn H. Assessing the impact of preferred web app-based music-listening on pain processing at the central nervous level in older black adults with low back pain: an fNIRS study. Geriatric Nurs. 2023;54:135–143. doi:10.1016/j.gerinurse.2023.09.005
74. Moriarty O, McGuire BE, Finn DP. The effect of pain on cognitive function: a review of clinical and preclinical research. Prog Neurobiol. 2011;93(3):385–404. doi:10.1016/j.pneurobio.2011.01.002
75. de Oliveira Franco Á, de Oliveira Venturini G, da Silveira Alves CF, et al. Functional connectivity response to acute pain assessed by fNIRS is associated with BDNF genotype in fibromyalgia: an exploratory study. Sci Rep. 2022;12(1):18831. doi:10.1038/s41598-022-23476-3
76. Sakuma S, Inamoto K, Yamaguchi Y, Takagi S, Higuchi N. Changes in prefrontal cerebral hemodynamics during intermittent pain stimulation to gingiva: preliminary study using functional near infrared spectroscopy. J Dental Sci. 2021;16(3):980–986. doi:10.1016/j.jds.2020.09.013
77. Kobayashi Y, Kurata J, Sekiguchi M, et al. Augmented cerebral activation by lumbar mechanical stimulus in chronic low back pain patients: an FMRI study. Spine. 2009;34(22):2431–2436. doi:10.1097/BRS.0b013e3181b1fb76
78. Bandeira JS, Antunes LDC, Soldatelli MD, Sato JR, Fregni F, Caumo W. Functional Spectroscopy Mapping of Pain Processing Cortical Areas During Non-painful Peripheral Electrical Stimulation of the Accessory Spinal Nerve. Front Human Neurosci. 2019;13:200. doi:10.3389/fnhum.2019.00200
79. Fritz HC, McAuley JH, Wittfeld K, et al. Chronic Back Pain Is Associated With Decreased Prefrontal and Anterior Insular Gray Matter: results From a Population-Based Cohort Study. J Pain. 2016;17(1):111–118. doi:10.1016/j.jpain.2015.10.003
80. Li T, Zhang S, Kurata J. Suppressed descending pain modulatory and enhanced sensorimotor networks in patients with chronic low back pain. J Anesthesia. 2018;32(6):831–843. doi:10.1007/s00540-018-2561-1
81. Sutoh C, Koga Y, Kimura H, et al. Repetitive Transcranial Magnetic Stimulation Changes Cerebral Oxygenation on the Left Dorsolateral Prefrontal Cortex in Bulimia Nervosa: a Near-Infrared Spectroscopy Pilot Study. Eur Eating Disorders Rev. 2016;24(1):83–88. doi:10.1002/erv.2413
82. Reddan MC, Young H, Falkner J, López-Solà M, Wager TD. 135Touch and social support influence interpersonal synchrony and pain. Soc Cognit Affective Neurosci. 2020;15(10):1064–1075. doi:10.1093/scan/nsaa048
83. López-Solà M, Geuter S, Koban L, Coan JA, Wager TD. 130Brain mechanisms of social touch-induced analgesia in females. Pain. 2019;160(9):2072–2085. doi:10.1097/j.pain.0000000000001599
84. Osborne NR, Anastakis DJ, Kim JA, et al. Carpal tunnel surgery dampens thalamocortical and normalizes corticocortical functional connectivity. Brain Comm. 2022;4(5):fcac237. doi:10.1016/j.jpain.2021.08.003
85. Ng SK, Urquhart DM, Fitzgerald PB, Cicuttini FM, Hussain SM, Fitzgibbon BM. The Relationship Between Structural and Functional Brain Changes and Altered Emotion and Cognition in Chronic Low Back Pain Brain Changes: a Systematic Review of MRI and fMRI Studies. Clin J Pain. 2018;34(3):237–261. doi:10.1097/ajp.0000000000000534
86. Yuan Y, Zhang L, Li L, et al. 26Distinct dynamic functional connectivity patterns of pain and touch thresholds: a resting-state fMRI study. Behav Brain Res. 2019;375:112142. doi:10.1016/j.bbr.2019.112142
87. Iliopoulos K, Koufaki P, Tsilikas S, et al. A randomized controlled trial evaluating the short-term efficacy of a single-administration intramuscular injection with the fixed combination of thiocolchicoside-diclofenac versus diclofenac monotherapy in patients with acute moderate-to-severe low back pain. BMC Musculoskeletal Disorders. 2023;24(1):476. doi:10.1186/s12891-023-06599-0
88. Shi P, Liu J, Du J, Yu H, Fang F. Pain modulation induced by electronic wrist-ankle acupuncture: a functional near-infrared spectroscopy study. Pain Pract. 2022;22(2):182–190. doi:10.1111/papr.13076
89. Gupta A, Mayer EA, Fling C, et al. Sex-based differences in brain alterations across chronic pain conditions. J Neurosci Res. 2017;95(1–2):604–616. doi:10.1002/jnr.23856
90. Keogh E. Sex and gender differences in pain: past, present, and future. Pain. 2022;163(Suppl 1):S108–s116. doi:10.1097/j.pain.0000000000002738
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.