Back to Journals » Clinical Ophthalmology » Volume 17
Modified Four-Point Scleral Fixated Sutured Posterior Chamber Intraocular Lens Implantation Using 2 Eyelets Polymethyl Methacrylate Lens and 8-0 Polypropylene Suture
Authors Angsana NC, Wardhana FS, Supanji ![]() , Prayogo ME, Sasongko MB
, Prayogo ME, Sasongko MB ![]()
Received 17 June 2023
Accepted for publication 13 November 2023
Published 29 November 2023 Volume 2023:17 Pages 3657—3662
DOI https://doi.org/10.2147/OPTH.S426443
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Modified 4-point scleral fixation technique" [ID 426443].
Views: 397
Natalia Christina Angsana,1 Firman Setya Wardhana,1 Supanji,1 Mohammad Eko Prayogo,2 Muhammad Bayu Sasongko1
1Department of Ophthalmology, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada – Sardjito Eye Center, Dr. Sardjito General Hospital, Yogyakarta, Indonesia; 2Department of Ophthalmology, Universitas Gadjah Mada Academic Hospital, Yogyakarta, Indonesia
Correspondence: Muhammad Bayu Sasongko, Department of Ophthalmology, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada – Sardjito Eye Center, Dr. Sardjito General Hospital, Jalan Farmako Sekip Utara, Yogyakarta, Indonesia, Tel/Fax +62 274 552850, Email [email protected]
Purpose: To present a modified technique of 4-point scleral fixation using polymethyl methacrylate (PMMA) 2 eyelets intraocular lens (IOL) with 8-0 polypropylene sutures.
Methods: A 270-degree conjunctival peritomy is done, and 4 sclerotomies (2 nasal and 2 temporal) are created. Lamellar scleral or clear corneal incision is made at superior site (6 mm wide for sclera or 5.5– 6 mm for corneal). A short segment of 8-0 polypropylene is inserted into each eyelet, each thread of the suture is externalized through the sclerotomy site, and the lens is inserted. The suture is tightened evenly, and the knot is rotated and internalized. Scleral incision and conjunctival peritomy are sutured with 8-0 vicryl.
Results: We have performed this technique in 6 patients with excellent visual outcomes and no reported complications over 1 year of follow-up. This technique has practical advantages including rigid and stable PMMA IOL, high tensile, and slim 8-0 polypropylene suture which is easily internalized and less irritated, and affordable and widely available overall consumables.
Conclusion: We present a modified 4-point scleral fixation technique for posterior chamber IOL placement using PMMA IOL with 2 eyelets and 8-0 polypropylene as compared to previous studies that used foldable IOL with 4 eyelets and 10-0 polypropylene or Gore-Tex sutures. This procedure has moderate technical complexity, comparable to previously reported techniques with good overall clinical outcomes and several practical advantages, particularly related to the affordability and availability of the consumables.
Plain Language Summary: This paper presents a modification of currently existing 4-point sutured scleral fixation technique for posterior chamber intraocular lens implantation using PMMA IOL with 2 eyelets using 8-0 polypropylene. This technique has some practical advantages compared to previously reported techniques with potential applicability in low-resource setting.
Keywords: sutured scleral fixation, four-point, polymethyl methacrylate, 2-eyelets, secondary intraocular lens implantation
Introduction
Scleral-fixated posterior chamber IOL (SF-IOL), both sutured and sutureless, is often preferred in cases without capsular support and unfavourable anterior chamber milieu (eg less corneal endothelial cell count [<1000–2000 cells/mm2], shallow dimension, anatomical iris dystrophy) when aiming to achieve better anterior chamber profile.1,2 Whilst sutured SF-IOL has been associated with suture erosion, knot exposure, and suture breakage after some time,1,2 sutureless SF-IOL using three-piece IOL was more recently developed and originated to avoid such complications.3 However, sutureless SF-IOL was related to some intra-operative failure such as broken or tilted haptic of the IOL.3 Importantly, some studies have already reported some complications such as IOL haptic exposure in the subconjunctiva, tilted IOL and IOL dislocation, and pupil capture over a relatively short follow-up period.3–5 To avoid such complications, a novel sutureless scleral fixation technique using the Carlevale IOL was introduced.6 Carlevale IOL is a single-piece foldable acrylic IOL with flexible sclero-corneal plugs at the ends of the two haptics. The technique of sutureless scleral fixation IOL with Carlevale IOL was able to preserve conjunctiva and reduce suture-related complications and surgery time. Nevertheless, there were still some problems including malpositioning and subluxed IOL, hypotony, corneal edema, cystoid macular edema, vitreous hemorrhage, and retinal tears.6 Therefore, sutured SF-IOL remains an effective alternative procedure for secondary IOL implantation.
Techniques for sutured SF-IOL have evolved significantly over the last 2 decades owing to the advancement of surgical instruments and consumables. Four-point sutured SF-IOL was first introduced by Bergren, using one-piece polymethyl methacrylate (PMMA) with one eyelet in each haptic and tied with 10-0 polypropylene sutures.7 Several more recent modifications of this technique, using foldable IOL with 4 eyelets and polytetrafluoroethylene (Gore-Tex) suture, were reported to simplify the complexity and avoid the limitations of 10-0 polypropylene.1,2,8 This technique has gained increased popularity; however, there were few practical limitations noted. First, the availability of foldable IOL with 4 eyelets is very limited and relatively expensive because there are very finite companies in the world that produce this type of IOL. Second, despite its resistance to degradation, Gore-Tex suture is bulky, floppy, and also expensive.9 Importantly, the off-label use of Gore-Tex for intraocular surgery has raised some legal concerns in the US.9,10 Therefore, the combination of 4 eyelets foldable IOL and Gore-Tex has apparent practical limitations, particularly in some settings where the resource constraint is an issue. In this paper, we described a modification of the 4-point sutured SF-IOL technique using 2 eyelets polymethyl methacrylate (PMMA) IOL and 8-0 polypropylene sutures.
Surgical Technique
The patient is under sub-tenon or retrobulbar block. Temporal, superior, and nasal conjunctival peritomy (270 degrees) is done. An infusion cannula is inserted at infero-temporal, then 4 scleral markings are made, 2 at temporal and 2 at nasal side adjacent to 3 and 9 o’clock position, 2 mm from limbus and 4 mm apart between each marking (2 mm superior and 2 mm inferior to 3 and 9 o’clock points). Sclerotomies are made using trocar, without angulation. Following sclerotomies, a 6 mm scleral tunnel is created at superior sclera using a crescent blade. The external scleral incision is 2–3 mm away from limbus, continued by lamellar sclerocorneal tunnel and internal corneal incision connecting the tunnel and anterior chamber. The shape of the scleral incision can be U-shape, straight, or inverse U-shape. The IOL insertion can also be done via corneal incision with 5.5–6 mm wide, depending on surgeon’s preference.
Complete vitrectomy and vitreous shaving are performed as per routine and IOL and the suture are prepared. Polypropylene 8-0 needles are removed, and the suture is cut into 4 segments to reduce the length. Only 2 segments are used. Each segment is inserted into each lens eyelet, IOL is positioned in a correct intraocular position at the entrance of the tunnel, and each thread is pulled and externalized from each sclerotomy using micro-forceps. IOL is then inserted, and the suture is tightened evenly until the IOL is central. The sutures are tied, and the knots are rotated and internalized through the sclerotomy sites. The scleral tunnel and conjunctiva are sutured with 8-0 vicryl. The complete surgery procedures are illustrated in Figures 1, 2, and Supplementary Video.
 |
Figure 1 Illustration of step-by-step surgical procedures. (a) Conjunctival peritomy. (b) An infusion cannula is inserted at infero-temporal and 4 scleral markings are made. (c) 6 mm scleral tunnel incision at superior sclera. (d) Internal corneal incision connecting the tunnel and anterior chamber. (e) Polypropylene 8–0 sutures are inserted into each lens eyelet. (f) IOL is positioned in a correct intraocular position at the entrance of the tunnel and each thread is pulled and externalized from each sclerotomy using a micro-forceps. (g) IOL is inserted and the suture is tightened evenly until the IOL is central. (h) The sutures are tied, and the knots are rotated and internalized through the sclerotomy sites. (i) Suture the scleral tunnel. (j) Suture the conjunctiva. |
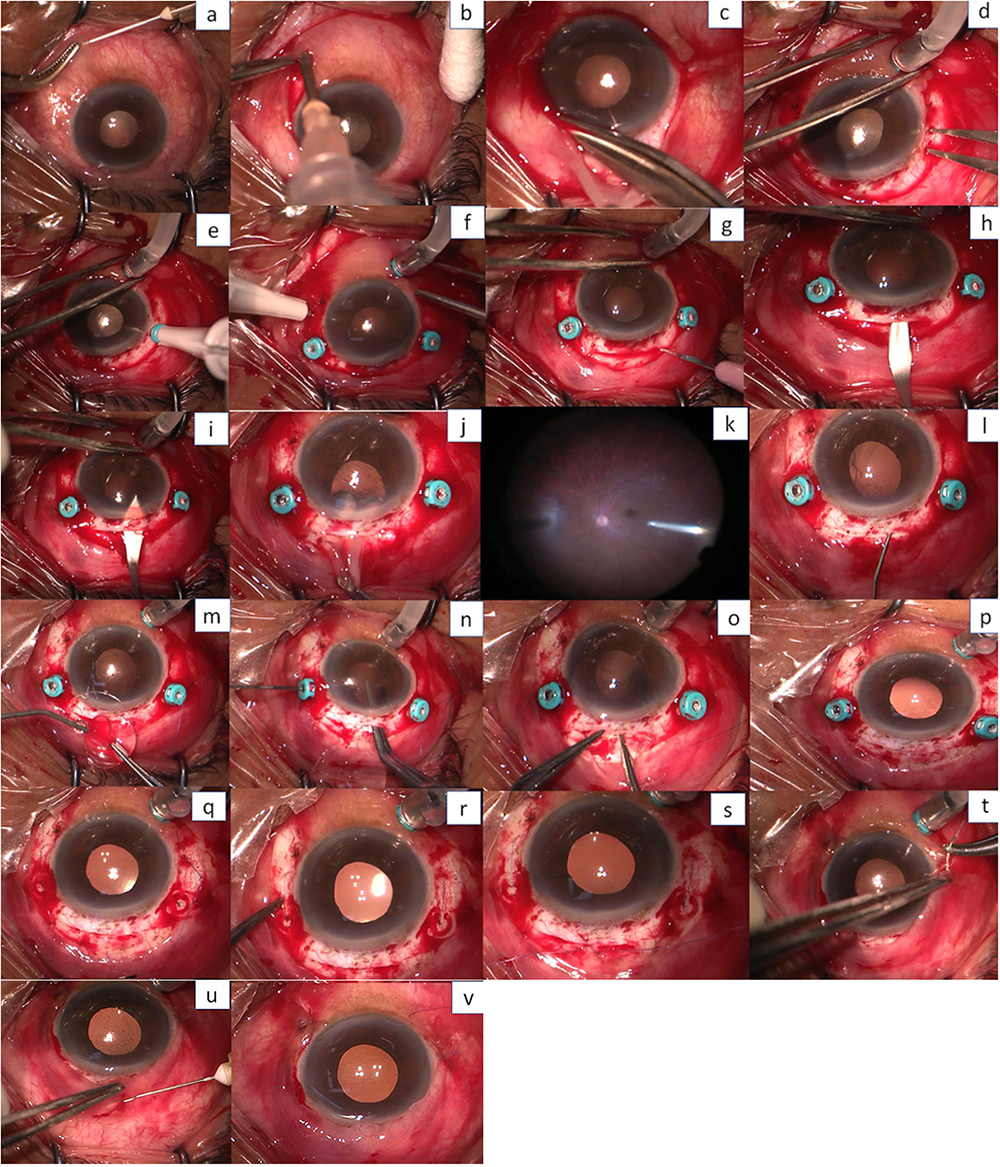 |
Figure 2 Complete surgical procedures. (a) Lidocaine subconjunctival injection. (b) Sub-tenon block. (c) 270-degree conjunctival peritomy. (d) An infusion cannula is inserted at infero-temporal. (e) 2 scleral markings at the temporal side adjacent to the 3 o’clock position. (f) 2 scleral markings at the nasal side adjacent to 9 o’clock position, 2 mm from the limbus and 4 mm apart between each marking (2 mm superior and 2 mm inferior to 3 and 9 o’clock points). (g) 6 mm scleral tunnel incision created at superior sclera using slit knife. (h) The lamellar sclerocorneal tunnel was made using crescent knife. (i) Internal corneal incision connecting the tunnel and anterior chamber. (j) IOL was evacuated. (k) Complete vitrectomy and vitreous shaving are performed. (l) Ophthalmic viscoelastic device (OVD) was injected. (m) Polypropylene 8-0 sutures inserted into each lens eyelet, IOL is positioned in a correct intraocular position at the entrance of the tunnel. (n) Nasal side thread is pulled and externalized from each sclerotomy using micro-forceps. (o) Temporal side thread is also pulled and externalized and IOL is then inserted. (p) Stabilize the IOL. (q) The suture is tightened evenly until the IOL is central. (r) The knots are rotated and internalized through the sclerotomy sites. (s) The scleral tunnel is sutured with 8-0 vicryl. (t) Conjunctiva is sutured using 8-0 426443 vicryl. (u) Antibiotic subconjunctival injection. (v) Surgery procedures are done. |
Discussion
In this paper, we have described a modification of currently existing 4-point scleral fixation technique for posterior chamber IOL placement. We have performed this procedure in 6 eyes that have been followed-up for over a year with excellent visual outcomes (from 1 month post-operative best-corrected visual acuity better than 6/12) and no reported complications. There was one eye with post-operative hyphema on day 1 but resolved spontaneously within 1 week. There was also one patient with elapsing iris capture which spontaneously occurred upon dilation but did not present in normal undilated pupils.
The first scleral fixated sutured IOL was described by Malbran et al11 using polypropylene 10-0 sutures and subsequently improvised by Lewis et al in 1991.12,13 This technique was further modified to 4-point fixation, allowing more stable and minimally tilted IOL.7 Due to the easy-to-degrade nature of 10-0 polypropylene suture, Gore-Tex sutures were used and showed suture durability up to 3 years follow-up.8 However, this suture was expensive and its availability in low-resource settings is very limited. Moreover, many hospitals in the United States have prohibited its off-label use for ophthalmic purposes including scleral fixation IOL.9,10 For this latter reason, John and associates first proposed in 2018 the use of 8-0 polypropylene to substitute Gore-Tex in combination with foldable IOL for 4-point sutured SF-IOL.9 Yet, the availability of 4 eyelets foldable IOL remains an issue in our setting.
The present technique used single piece PMMA IOL with 1 eyelet at each haptic and 8-0 polypropylene suture. There are several practical advantages of this procedure. First, this IOL is a hydrophobic and non-foldable rigid lens that decreases the opacification possibility when in contact with intraocular gas or air. The IOL also has a 13.5 mm overall diameter which is wider than the normal horizontal corneal diameter (WTW) and thus may provide more stability of the IOL in the posterior chamber. In addition, this type of IOL is usually very cheap, a lot cheaper than single-piece foldable IOL with 4 eyelets. Second, from a theoretical point of view, 8-0 polypropylene suture has high tensile strength and better resistance compared to its 10-0 version and is also slimmer and less bulky than Gore-Tex, thus it is easier to rotate and the knot can be conveniently internalized through the sclerotomy site.9 The use of 8-0 polypropylene may thus overcome the limitations of both other sutures. Importantly, this suture is widely available and more affordable than Gore-Tex. Third, the use of scleral tunnel to insert the lens is more watertight than a corneal incision and may induce minimal astigmatism.14 Nevertheless, creating a scleral tunnel can be challenging because it has to be adequately thick. Surgeons with minimal experience sometimes encounter buttonhole flap due to too-thin incision or premature entry to the anterior chamber due to too-thick incision.
Conclusion
In conclusion, we presented a modification of the currently existing 4-point scleral fixation technique for posterior chamber IOL placement using PMMA IOL with 2 eyelets using 8-0 polypropylene as compared to previous studies that used foldable IOL with 4 eyelets and 10-0 polypropylene or Gore-Tex sutures. This procedure has moderate technical complexity, comparable to previously reported techniques with good overall clinical outcomes and several practical advantages, particularly related to the affordability and availability of the consumables.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis,and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jacob S, Kumar DA, Rao NK. Scleral fixation of intraocular lenses. Curr Opin Ophthalmol. 2020;31(1):50–60. doi:10.1097/ICU.0000000000000632
2. Patel LG, Starr MR, Ammar MJ, Yonekawa Y. Scleral fixated secondary intraocular lenses: a review of recent literature. Curr Opin Ophthalmol. 2020;31(3):161–166. doi:10.1097/ICU.0000000000000661
3. Bonnell AC, Mantopoulos D, Wheatley HM, Prenner JL. Surgical technique for sutureless intrascleral fixation of a 3-piece intraocular lens using a 30-gauge needle. Retina. 2019;39(1):S13–S15. doi:10.1097/IAE.0000000000001889
4. Czajka MP, Frajdenberg A, Stopa M, Pabin T, Johansson B, Jakobsson G. Sutureless intrascleral fixation using different three‐piece posterior chamber intraocular lenses: a literature review of surgical techniques in cases of insufficient capsular support and a retrospective multicentre study. Acta Ophthalmologica. 2020;98(3):224–236. doi:10.1111/aos.14307
5. Matsui Y, Matsubara H, Hanemoto T, Kondo M. Exposure of haptic of posterior chamber intraocular lens after sutureless intrascleral fixation. BMC Ophthalmol. 2015;15(1):1–3. doi:10.1186/s12886-015-0102-3
6. Carlà MM, Boselli F, Giannuzzi F, et al. Sutureless scleral fixation Carlevale IOL: a review on the novel designed lens. Int Ophthalmol. 2023;43(6):2129–2138. doi:10.1007/s10792-022-02579-w
7. Bergren RL. Four-point fixation technique for sutured posterior chamber intraocular lenses. Arch Ophthalmol. 1994;112(11):1485–1487. doi:10.1001/archopht.1994.01090230099029
8. Khan MA, Gupta OP, Smith RG, et al. Scleral fixation of intraocular lenses using Gore-Tex suture: clinical outcomes and safety profile. Br J Ophthalmol. 2016;100(5):638–643. doi:10.1136/bjophthalmol-2015-306839
9. John T, Tighe S, Hashem O, Sheha H. New use of 8-0 polypropylene suture for four-point scleral fixation of secondary intraocular lenses. J Cataract Refract Surg. 2018;44(12):1421–1425. doi:10.1016/j.jcrs.2018.08.008
10. Mo B, Li S-F. Novel use of an adjustable single 8–0 polypropylene suture of scleral fixation without conjunctival dissection. BMC Ophthalmol. 2020;20(1):1–8. doi:10.1186/s12886-020-01558-y
11. Malbran ES, Malbran JE, Negri I. Lens guide suture for transport and fixation in secondary IOL implantation after intracapsular extraction. Int Ophthalmol. 1986;9(2–3):151–160. doi:10.1007/BF00159844
12. Cavallini GM, Volante V, De Maria M, et al. Long-term analysis of IOL stability of the Lewis technique for scleral fixation. Eur J Ophthalmol. 2015;25(6):525–528. doi:10.5301/ejo.5000652
13. Stem MS, Todorich B, Woodward MA, Hsu J, Wolfe JD. Scleral-fixated intraocular lenses: past and present. J Vitreoret Dis. 2017;1(2):144–152. doi:10.1177/2474126417690650
14. Olsen T, Dam-Johansen M, Bek T, Hjortdal JØ. Corneal versus scleral tunnel incision in cataract surgery: a randomized study. J Cataract Refract Surg. 1997;23(3):337–341. doi:10.1016/S0886-3350(97)80176-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.