Back to Journals » Journal of Pain Research » Volume 15
Modified Acupotomy versus Percutaneous Release for Trigger Thumb: A Retrospective Study
Authors Li SM, Chen P, Yan MZ, Du WS, Guo R, Luo T
Received 27 September 2021
Accepted for publication 5 February 2022
Published 19 April 2022 Volume 2022:15 Pages 1141—1148
DOI https://doi.org/10.2147/JPR.S339710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erika Petersen
Shu-Ming Li, Ping Chen, Ming-Zhe Yan, Wei-Shuai Du, Ren Guo, Tao Luo
Department of Pain Medicine, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing, 100010, People’s Republic of China
Correspondence: Ren Guo; Tao Luo, Department of Pain Medicine, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, No. 23 Backstreet Gallery, Dongcheng District, Beijing, 100010, People’s Republic of China, Email [email protected]; [email protected]
Background: Acupotomy is now increasingly used for trigger thumb, while recent evidence showed it increased the risk of nerve injury. Based on the close proximity of the neurovascular bundles and the A1 pulley, we designed a modified acupotomy. Given that percutaneous release is the common surgical treatment, this retrospective study aimed to compare the effect and safety of modified acupotomy versus percutaneous release for trigger thumb.
Methods: This is a retrospective study. All patients with trigger thumb were retrieved in the electronic records of the Department of Pain Medicine at the Beijing Hospital of Traditional Chinese Medicine from January 2016 to September 2018. Both short-term (3 months) and long-term (2 years) outcomes were evaluated using the criteria established through Gilberts et al.’s questionnaire, including triggering, residual pain, stiffness, digital nerve injury, scar, infection and satisfaction. Chi-square test or Fisher’s exact test was used to compare differences between two groups.
Results: A total of 305 patients with 334 trigger thumbs treated with either modified acupotomy (n = 194 thumbs) or percutaneous release (n = 140 thumbs) were included. Of them, 221 (72.5%) were female, and the mean age was 56.2 ± 10.0 years. The mean duration of trigger thumb lasted for 7.5 ± 3.6 months. At 3 months, all triggering were alleviated by both therapies. Although more digital nerve injury occurred in the percutaneous release (0 [0%] thumbs vs 5 [3.6%] thumbs, P = 0.012), more residual pain (30 [15.5%] thumbs vs 6 [4.3%] thumbs; rate ratio, 3.61; 95% confidence interval [CI]: 1.54– 8.43; P = 0.001) and less satisfaction occurred in the modified acupotomy group. At 2 years, more recurrent triggering, residual pain and digital nerve injury occurred in the percutaneous release group (2 [1.0%] thumbs vs 12 [8.6%] thumbs; rate ratio, 0.12; 95% CI: 0.03– 0.53; P = 0.001; 9 [4.6%] thumbs vs 22 [15.7%] thumbs; rate ratio, 0.30; 95% CI: 0.14– 0.62 P < 0.001; 0 [0%] thumbs vs 4 [2.9%] thumbs, P = 0.030, respectively). Moreover, satisfaction was significantly better in the modified acupotomy group.
Conclusion: The modified acupotomy had better long-term outcomes and satisfaction than the percutaneous release for trigger thumb, although percutaneous release has less residual pain and better satisfaction in the short term. The modified acupotomy is a treatment option for trigger thumb.
Keywords: modified acupotomy, percutaneous release, trigger thumb, retrospective study
Background
Trigger thumb is a common cause of pain and disability of the hand in adults. Trigger thumb is caused by a size mismatch between the flexor tendon and the first annular (A1) pulley and may bring painless clicking with thumb movement, or even painful triggering. The flexor tendon usually locks or clicks at the level of the A1 pulley, and the thumb may be locked in a flexed position.1
The common surgical treatments for trigger thumb include open release and percutaneous release. Compared with the open release, the percutaneous release is more rapid, less invasive, and less costly.2–6 However, the potential disadvantages of the percutaneous release are incomplete release and injury to either the tendon or nerve.7–9 Acupotomy, also called miniscalpel-needle or small needle knife, is now increasingly used for a variety of pain conditions, including trigger thumb.10–13 However, a few studies have indicated that acupotomy for trigger thumb also increased the risk of nerve or tendon injury.14
Based on the close proximity of the neurovascular bundles and the A1 pulley in the thumb, we designed the modified acupotomy, which is already a granted patent (Patent No. CN202859181U, State Intellectual Property Office of the People’s Republic of China). The modified acupotomy is bent to 30° to enable it to be positioned parallel to the tendon (Figure 1). One end of the modified acupotomy is the handle, and the other end is sharpened into a “J” shape with a sharp edge to cut the thickened A1 pulley. The design of the blunt J-shaped tip has two main functions. One is to keep the A1 pulley and the flexor tendon apart and guide the direction of the release; the other is to avoid the potential damage to the nerve by pushing the nerve out of the way. In addition, the extended lower edge is blunt, which aims to avoid the injury to the flexor tendon. Although the modified acupotomy has been used in our department for many years, data with regard to the effectiveness and safety of the modified acupotomy are insufficient. The purpose of this retrospective study was to evaluate the long-term effectiveness and safety of modified acupotomy in the treatment of trigger thumb compared with percutaneous release.
 |
Figure 1 Photograph of a modified acupotomy. |
Methods
Patients
All patients with trigger thumb were retrieved in the electronic records of the Department of Pain Medicine at the Beijing Hospital of Traditional Chinese Medicine from January 2016 to September 2018. This retrospective observational study was approved by the Ethics Committee of Beijing Hospital of Traditional Chinese Medicine (Permit No. 2018BL-080-02) and complied with the Declaration of Helsinki. The acquisition of written informed consent for the modified acupotomy or the percutaneous release treatment was noted in the medical records of all patients. All patient records and data were anonymized and de-identified prior to analysis.
The diagnosis of trigger thumb was established by the attending physicians based on the patient’s symptoms and physical examination. Patients exhibiting symptoms greater than Grade 2 (according to the Quinnell classification) with a history of triggering for at least 3 months were included.15 The Quinnell classification system includes five distinct grades: Grade 0, normal movement; Grade I, uneven movement; Grade II, actively correctable; Grade III, passively correctable; and Grade IV, fixed deformity. Patients were excluded if they had any of the following: previous surgical release of triggering, rheumatoid disease, severe neurologic deficit of the involved upper extremity, loss of follow-up, or diabetes.
Intervention
The modified acupotomy treatment was performed in the outpatient operating room by an experienced hand surgeon. At the beginning, the location of A1 pulley was marked on the skin of the affected thumb according to a previous study.16 After skin sterilization, local anesthesia was established by administration of 2 mL of 2% lidocaine. Next, a longitudinal incision of 3 mm was made with a No. 11 scalpel at approximately 1 cm proximal to the A1 pulley when the thumb was held in extension (Figure 2A). The modified acupotomy was then inserted into the same track to reach the proximal edge of the A1 pulley (Figure 2B). The blunt tip and extended edge helped the surgeon to confirm the proximal edge of the A1 pulley, and slipped the device into the space between the A1 pulley and the underlying flexor tendon minimizing the damage of the flexor tendon. The whole A1 pulley was incised along the direction of the flexor tendon with the sharp J-shaped edge of the modified acupotomy, proximally to distally (Figure 2C). A distinct sense of resistance was felt during the process of incising the A1 pulley, and the operation was completed when the resistance feeling disappeared (Figure 2D). The modified acupotomy was then withdrawn, and the patients were asked to flex and extend the thumb to confirm if there was any residual triggering. After the modified acupotomy treatment, a compressive bandage was applied to the surgical wound. Finally, patients were encouraged to return to normal daily activities as soon as possible. For patients with two trigger thumbs, the modified acupotomy treatments were performed at different times.
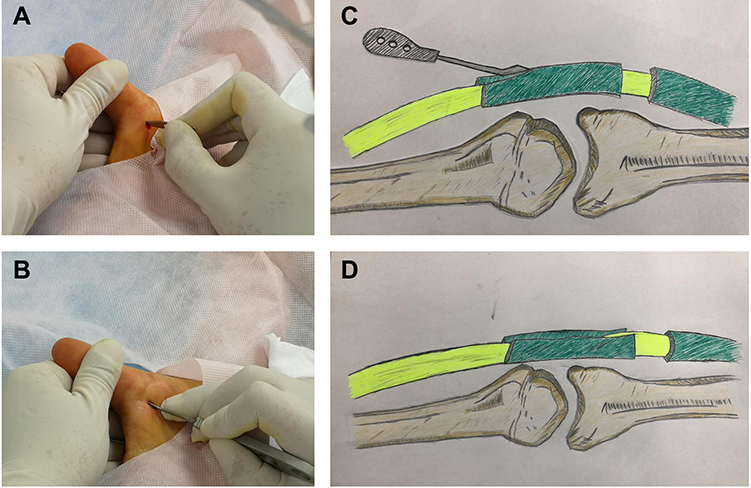 |
Figure 2 The process of modified acupotomy release. (A) After skin sterilization and local anesthesia, a 3-mm longitudinal stab incision was then made. (B) The modified acupotomy was inserted into the same track to reach the proximal edge of the A1 pulley, then slipped into the space between the pulley and the flexor tendon. (C) The modified acupotomy was gently pushed distally to release the A1 pulley with the sharp J-shaped edge. (D) The A1 pulley was completely released by the modified acupotomy. |
Percutaneous release, which was the technique as described in previous studies,17,18 was also performed in the outpatient operating room. The surface landmark was marked on the palm.16 After skin sterilization, local anesthesia was administered with 2 mL 2% lidocaine. Then the affected thumb was held in a hyperextended position. An 18-gauge needle tip was inserted through the skin at the proximal extent of the A1 pulley and into the flexor tendon parallel to the longitudinal axis of the flexor tendon. Needle tip position was checked by passively flexing and extending the patient’s thumb. The needle was slightly withdrawn until no paradoxical swing was observed. The A1 pulley was divided from proximally to distally through a sweeping motion of the sharp needle tip. The surgeon would feel a characteristic gritting sensation during the procedure, and complete release of the A1 pulley was confirmed by the disappearance of the grating sensation and full active thumb motion without triggering. A compressive bandage was applied at the puncture site for 2 days postoperatively, and the patients were allowed to return to normal activity as tolerated.
Postoperative Assessment
The patients in both groups were asked to return to the outpatient clinic for a re-examination at 1 week after treatment. They were then contacted at 3 months and 2 years after treatment and were reassessed at our outpatient clinic or by telephone. All patients were evaluated by two doctors who were not involved in the treatments. The evaluation at 3 months was recorded as short-term follow-up, and the evaluation at 2 years was recorded as long-term follow-up. Functional outcomes were evaluated with the validated questionnaire of Gilberts and Wereldsma administered in the previous studies.19–21 The following questions were asked: Do you have triggering? Do you have pain? Do you have stiffness? Do you feel numbness? Do you have a scar? Are you dissatisfied, satisfied, or very satisfied with the result of the treatment? We also recorded any complications.
Statistical Analysis
SPSS 26.0 was used to perform the statistical analysis. Enumeration data were expressed as absolute numbers and percentage and chi-square test was used to compare differences between two groups. Continuous variables of normal distribution were expressed as means and standard deviations and were assessed with Student’s t-test. Continuous variables of skewness distribution were expressed as means (minimum to maximum), and non-parametric test was used. A P value <0.05 was considered statistically significant.
Results
Through reviewing our patient database, we retrieved 339 patients with trigger thumb who met the inclusion criteria from January 2016 to September 2018. Among them, 34 patients were excluded due to being unreachable, incomplete follow-up information, diabetes or other reasons. Finally, this study included 305 patients with 334 treated thumbs (176 patients with 194 treated thumbs in the modified acupotomy group and 129 patients with 140 treated thumbs in the percutaneous release group). Of the them, 221 (72.5%) were female, and the mean age was 56.2 ± 10.0 years. The mean duration of trigger thumb lasted for 7.5 ± 3.6 months. The two groups were similar regarding age, sex, hand side involvement, and triggering grade prior to release (Table 1). However, the duration of symptoms was longer in the modified acupotomy group (P <0.001) (Table 1).
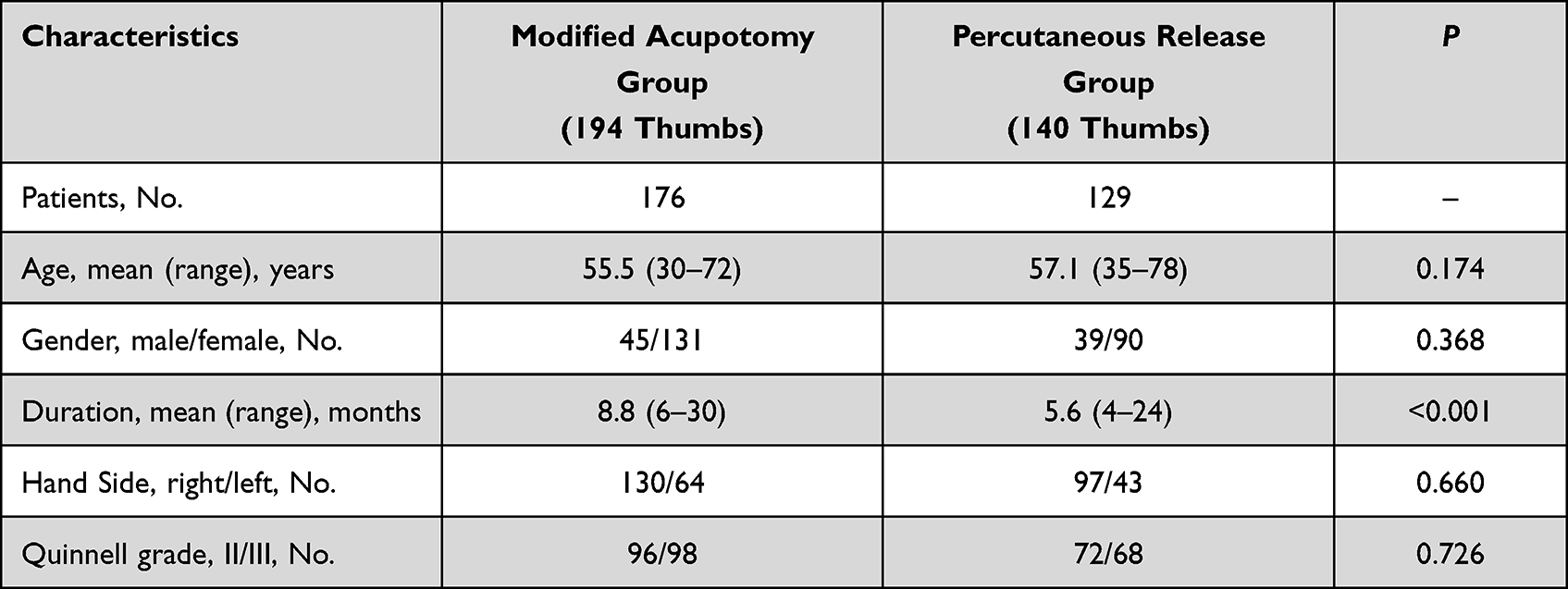 |
Table 1 Patients’ Baseline Characteristics |
For the short-term outcomes, there was no recurrent triggering in both groups. Residual pain occurred in 30 digits (15.5%) in the modified acupotomy group and in 6 digits (4.3%) in the percutaneous release group, with a significant difference (rate ratio [RR], 3.61; 95% confidence interval [CI]: 1.54–8.43; P = 0.001). No stiffness or scar occurred in any groups, which may owe to the immediate exercise requested by doctors. Five digits (3.6%) in the percutaneous release group had digital nerve injury, but none in the modified acupotomy group (P = 0.012). There were 2 digits (1.4%) in which the wound became infected in the percutaneous release group and 4 digits (2.1%) in the modified acupotomy group (RR, 1.44; 95% CI: 0.27–7.77; P > 0.999), and they were all cured with oral antibiotics. Short-term patient satisfaction was significantly better in the percutaneous release group (P < 0.001). All results regarding short-term outcomes are summarized in Table 2.
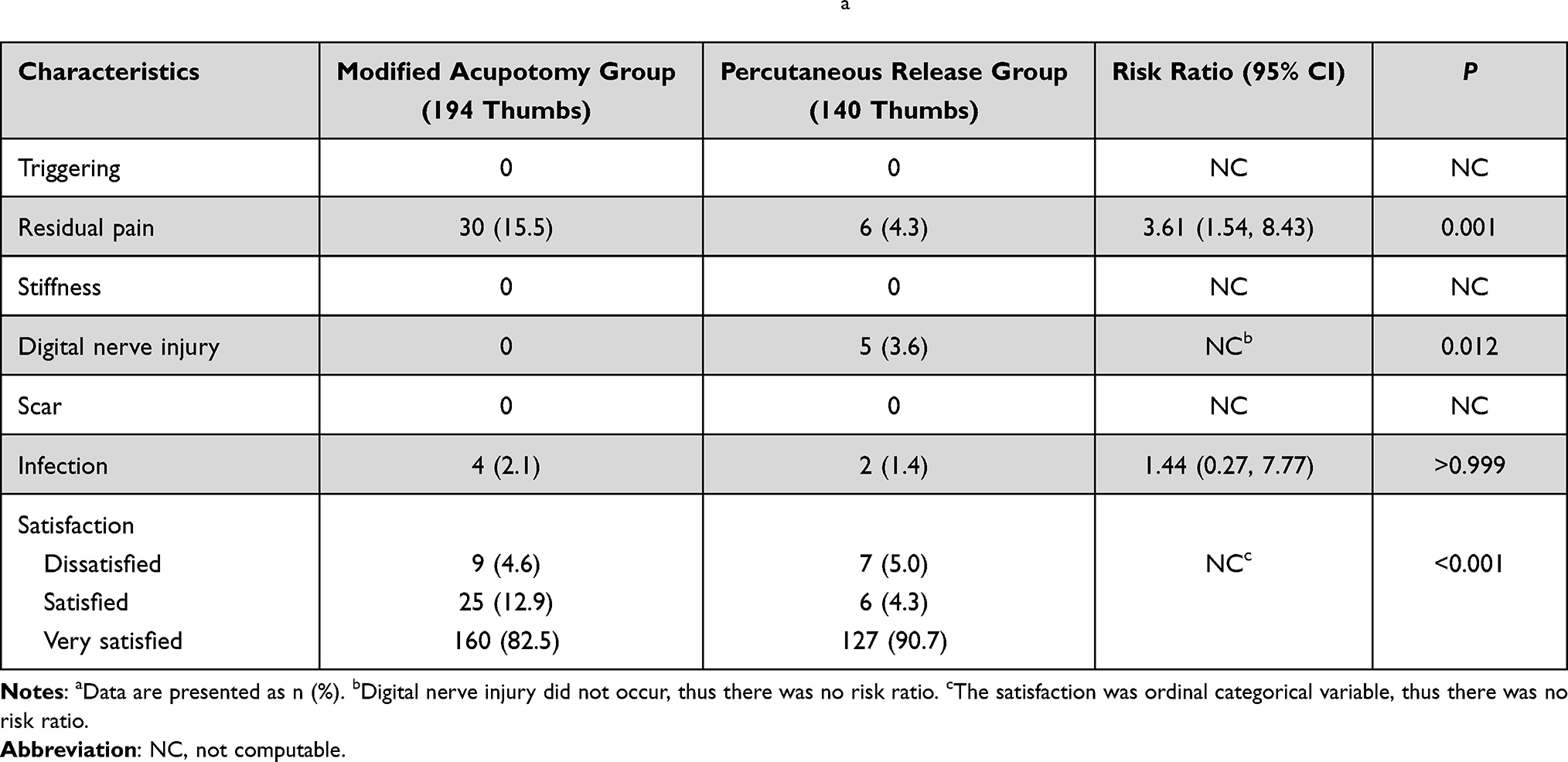 |
Table 2 Summary of Results at the Short-Term Follow-Up (3 Months)a |
For the long-term outcomes, recurrent triggering occurred in 2 digits (1.0%) in the modified acupotomy group and in 12 digits (8.6%) in the percutaneous release group, and the difference was statistically significant (RR, 0.12; 95% CI: 0.03–0.53; P = 0.001). Residual pain occurred in 9 digits (4.6%) in the modified acupotomy group and in 22 digits (15.7%) in the percutaneous release group (RR, 0.30; 95% CI: 0.14 to 0.62; P < 0.001). No patients had stiffness, scar or infection in any groups. Four patients (2.9%) had continuing digital nerve injury in the percutaneous release group (P = 0.030). Long-term patient satisfaction was significantly better in the modified acupotomy group (P <0.001). All results regarding long-term outcomes are summarized in Table 3.
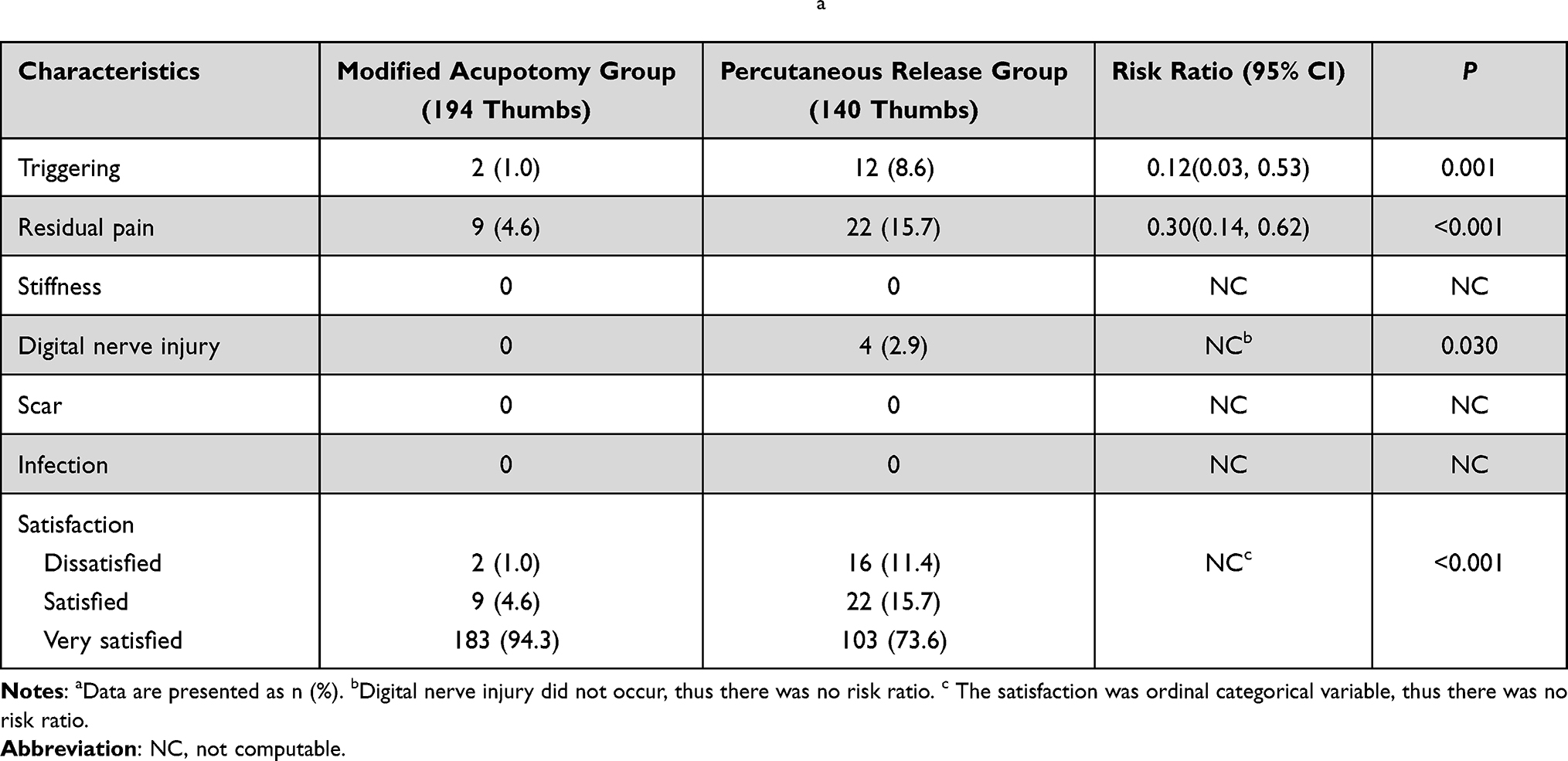 |
Table 3 Summary of Results at the Long-Term Follow-Up (2 Years) a |
Discussion
This study aimed to investigate the effect of modified acupotomy compared with percutaneous release for the treatment of trigger thumb. In the short-term follow-up, there was no recurrent triggering in both groups. There were more patients with residual pain in the modified acupotomy group than in the percutaneous release group, and patient satisfaction was significantly better in the percutaneous release group, while there were more patients who suffered from digital nerve injury. Moreover, in the long-term follow-up, there were fewer patients with recurrent triggering, residual pain, digital nerve injury or dissatisfaction in the modified acupotomy group compared with the percutaneous release group. The RR values for recurrent triggering and residual pain at 2 years were 0.12 and 0.30, respectively, indicating a robust correlation. The modified acupotomy is a treatment option for trigger thumb.
This study found that both two techniques relieved triggering at short-term follow-up. It means that the modified acupotomy is as effective as percutaneous release. Most of the previous trials also found that no triggering occurred at short-term follow-up after percutaneous release. However, more recurrences (8.6%) were found in the percutaneous release group at long-term follow-up. Other studies observed similar recurrences (3.9–8.8%) in the percutaneous release group at long-term follow-up.20,21 However, open surgery had fewer long-term recurrences (1.3–3.4%),20,21 which was numerically as small as modified acupotomy (1.0%) in current study.
It is worth noting that the incidence of iatrogenic digital nerve injury in the percutaneous release group was 3.6% at the short-term follow-up, and 2.9% patients still had this injury after 2 years, while none occurred in the modified acupotomy group at both short-term and long-term follow-up. A previous trial found a similar result in that 5.7% of patients with trigger thumb suffered from digital nerve injury after percutaneous release at mean 22.7 months follow-up.7 Although the rate of digital nerve injury is not high in the percutaneous release group, it is believed that any iatrogenic digital nerve injury was clinically serious. It is not surprising that the digital nerve injury occurred during the percutaneous release, due to the proximity of the radial digital nerve and the A1 pulley midline of the thumb.
The close anatomical relationship between the radial digital nerve of the thumb and the A1 pulley has been investigated in several cadaveric studies. Buldu and Schramm dissected thumbs of cadavers and found the radial digital nerve is 2.7–3.4 mm lateral to the A1 pulley at the proximal margin level of the A1 pulley.22,23 Any sharp dissection proximal to the margin of the A1 pulley may cause digital nerve injury where the radial digital neurovascular bundle crosses the flexor tendon sheath. Bain and colleagues concluded that percutaneous release of trigger thumb is potentially hazardous.24 Pope even recommended that percutaneous release should not be used in the index finger and the thumb.17
To avoid the potential digital nerve injury and the incomplete release encountered during the percutaneous release, we designed the modified acupotomy. First, the blunt tip of the J-shaped structure helps to divide the A1 pulley from the flexor tendon and to guide the direction of the division of A1 pulley. Second, the blunt tip of the J-shaped structure serves to push the nerve out of the pathway, thus avoiding potential damage to the nerve. Third, the extended lower edge of the J-shaped structure is blunt and smooth, which ensures that the J-shaped structure is placed over the flexor tendon without injury to this tendon. Finally, the J-shaped structure can promote the complete release of the thickened A1 pulley under the condition of ensuring safety. In addition, the surgeon’s experience and skill in modified acupotomy release are also the key points in achieving successful treatment effects. It should be noted that the thumb should be fully extended during the release in terms of the specific requirements of the procedure. And before the modified acupotomy release, the doctor should identify the proximal edge of the thickened A1 pulley. To minimize neurovascular damage, the modified acupotomy should be held over the tendon along the midline and be pushed distantly to cut the A1 pulley.
In the current study, both pain and patient satisfaction were better in the percutaneous release group than modified acupotomy group at the short-term assessment, but the results were reversed at the long-term follow-up. One reason may be that the modified acupotomy is thick, which resulted in functional impairment not an organic lesion. Functional impairment gradually recovered with longer follow-up, thus digital nerve injury and recurrent triggering in the percutaneous release group led to less satisfaction at 2 years. Another reason may be that a bigger wound was needed due to the thick acupotomy. Improvement of the thickness of acupotomy will be further studied.
This study had several limitations. Firstly, the retrospective nature of study design might cause bias. A further randomized controlled trial to compare modified acupotomy with percutaneous release may be needed and would provide more convincing data. Secondly, there were differences in the duration of symptoms between the two groups, which might be because doctors may be more inclined to choose modified acupotomy for patients with longer duration of symptoms. It is believed that a patient with longer duration of symptom would be more difficult to cure. However, the modified acupotomy had better long-term outcomes despite longer duration of symptom. Thirdly, only patients with trigger thumb were included in this study. The generalization of conclusions in this study for other fingers is unclear. Fourthly, although the Gilberts et al.’s questionnaire is not enough to prove all postoperative results, it has been commonly administered in previous retrospective studies.19–21 Further trials should include more outcomes to evaluate the postoperative results comprehensively.
Conclusion
The modified acupotomy had better long-term outcomes and satisfaction than the percutaneous release for trigger thumb, although percutaneous release has less residual pain and better satisfaction in the short term. The modified acupotomy is a treatment option for trigger thumb.
Data Sharing Statement
All the processed data were included in the current study. If reviewers or readers have any questions regarding our published data, they can contact the corresponding authors [[email protected]; [email protected]] for access to the original data.
Ethics Approval and Consent to Participate
The protocol was approved by the Ethics Committee of Beijing Hospital of Traditional Chinese Medicine (2018BL-080-02). Written consents were obtained for their inclusion in this study.
Acknowledgments
This study was supported by Capital's Funds for Health Improvement and Research (No. 2020-2-2231).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Patent for a modified acupotomy for releasing the pulley of a tendon sheath (No. CN202859181U) was licensed to Tao Luo. The authors declare that they have no other competing interests in this work.
References
1. Dierks U, Hoffmann R, Meek MF. Open versus percutaneous release of the A1-pulley for stenosing tendovaginitis: a prospective randomized trial. Tech Hand Up Extrem Surg. 2008;12(3):183–187.
2. Benson LS, Ptaszek AJ. Injection versus surgery in the treatment of trigger finger. J Hand Surg Am. 1997;22(1):138–144.
3. Cakmak F, Wolf MB, Bruckner T, Hahn P, Unglaub F. Follow-up investigation of open trigger digit release. Arch Orthop Trauma Surg. 2012;132(5):685–691.
4. Ucar BY. Percutaneous surgery: a safe procedure for trigger finger. N Am J Med Sci. 2012;4(9):401–403.
5. Ryzewicz M, Wolf JM. Trigger digits: principles, management, and complications. J Hand Surg Am. 2006;31(1):135–146.
6. Kim J, Rhee SH, Gong HS, Oh S, Baek GH. Biomechanical analyses of the human flexor tendon adhesion models in the hand: a cadaveric study. J Orthop Res. 2015;33(5):717–725.
7. Guler F, Kose O, Ercan EC, Turan A, Canbora K. Open versus percutaneous release for the treatment of trigger thumb. Orthopedics. 2013;36(10):e1290–1294.
8. Cihantimur B, Akin S, Ozcan M. Percutaneous treatment of trigger finger. 34 fingers followed 0.5-2 years. Acta Orthop Scand. 1998;69(2):167–168.
9. Patel MR, Moradia VJ. Percutaneous release of trigger digit with and without cortisone injection. J Hand Surg Am. 1997;22(1):150–155.
10. Wang Z, Zhou X, Xie L, et al. Acupotomy and acupuncture in the treatment of avascular necrosis of femoral head at the early and middle stages: a clinical randomized controlled trial. Zhongguo Zhen Jiu. 2016;36(10):1031–1035.
11. Li S, Shen T, Liang Y, Zhang Y, Bai B. Miniscalpel-Needle versus Steroid Injection for Plantar Fasciitis: a Randomized Controlled Trial with a 12-Month Follow-Up. Evid Based Complement Alternat Med. 2014;2014:164714.
12. Li S, Shen T, Liang Y, Bai B, Zhang Y. Miniscalpel-Needle Treatment Is Effective for Work-Related Neck and Shoulder Musculoskeletal Disorders. Evid Based Complement Alternat Med. 2016;2016:5760240.
13. Chao M, Wu S, Yan T. The effect of miniscalpel-needle versus steroid injection for trigger thumb release. J Hand Surg Eur Vol. 2009;34(4):522–525.
14. Ooyang J, Li Y, Yue Y. Evaluation of the injury on fingers in several operating processes of needle knife treatments on trigger finger. Chin J Rehabilitation Med. 2010;25(6):523–526.
15. Quinnell RC. Conservative management of trigger finger. Practitioner. 1980;224(1340):187–190.
16. Wilhelmi BJ. Trigger finger release with hand surface landmark ratios: an anatomic and clinical study. Plast Reconstr Surg. 2001;108(4):908–915.
17. Pope DF, Wolfe SW. Safety and efficacy of percutaneous trigger finger release. J Hand Surg Am. 1995;20(2):280–283.
18. Slesarenko YA, Mallo G, Hurst LC, Sampson SP, Serra-Hsu F. Percutaneous release of A1 pulley. Tech Hand Up Extrem Surg. 2006;10(1):54–56.
19. Gilberts EC, Wereldsma JC. Long-term results of percutaneous and open surgery for trigger fingers and thumbs. Int Surg. 2002;87(1):48–52.
20. Huang HK, Wang JP, Lin CJ, Huang YC, Huang TF, Chang MC. Short-term Versus Long-term Outcomes After Open or Percutaneous Release for Trigger Thumb. Orthopedics. 2017;40(1):e131–131e135.
21. Lin CJ, Huang HK, Wang ST, Huang YC, Liu CL, Wang JP. Open versus percutaneous release for trigger digits: reversal between short-term and long-term outcomes. J Chin Med Assoc. 2016;79(6):340–344.
22. Buldu H, Cepel S, Ki N, Ağritmiş H. References to avoid complications in releases of the trigger thumb: a cadaveric study. Acta Orthop Traumatol Turc. 2006;40(4):311–314.
23. Schramm JM, Nguyen M, Wongworawat MD. The safety of percutaneous trigger finger release. Hand. 2008;3(1):44–46.
24. Bain GI, Turnbull J, Charles MN, Roth JH, Richards RS. Percutaneous A1 pulley release: a cadaveric study. J Hand Surg Am. 1995;20(5):781–786.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.