Back to Journals » Open Access Journal of Contraception » Volume 13
Modern Contraceptive Utilization and Associated Factors Among Married Women in Liberia: Evidence from the 2019 Liberia Demographic and Health Survey
Authors Tsegaw M ![]() , Mulat B, Shitu K
, Mulat B, Shitu K
Received 18 November 2021
Accepted for publication 26 January 2022
Published 15 February 2022 Volume 2022:13 Pages 17—28
DOI https://doi.org/10.2147/OAJC.S350117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Igal Wolman
Menen Tsegaw,1 Bezawit Mulat,2 Kegnie Shitu3
1Department of Public Health, College of Medicine and Health Sciences, Ambo University, Ambo, Ethiopia; 2Department of Human Physiology, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Health Education and Behavioral Sciences, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Menen Tsegaw, Tel +251 934934533, Email [email protected]
Background: Contraceptive methods help individuals control the number, interval, and timing of pregnancies and prevent unwanted pregnancies.
Objective: This study aimed to assess the prevalence of modern contraceptive utilization and associated factors among married reproductive-age women in Liberia.
Methods: This study was based on a large community-based cross-sectional survey, conducted from October 16, 2019, to February 12, 2020, in Liberia. The survey employed a multistage cluster sampling technique to recruit study participants. Binary logistic regression was used to identify associated factors of contraceptive utilization. A p-value of < 0.05 and a 95% confidence interval were used to declare statistical significance.
Results: The overall modern contraceptive utilization among reproductive-age women in Liberia was 23.87% (95% CI: 27.3, 29.9). Women with the age group of 20 and 24 years [AOR = 2.08 (95% CI:1.37, 3.14)], 25– 29 years [AOR = 1.73 (95% CI: 1.13, 2.65)], 45– 49 years [AOR = 0.46, 95% CI: 0.27, 0.76], being Muslim [AOR = 0.52, 95% CI: 0.399, 0.67], residing in South Eastern Regions (B) [AOR = 1.40, 95% CI: 1.11, 1.79], south central [AOR=0.48 95% CI:0.37, 0.61] and North Central region [AOR = 0.48, 95% CI: 0.37, 0.61], being employed [AOR = 1.26, 95% CI:1.06, 1.51], having 1– 2 child/children [AOR = 2.81, 95% CI:1.80, 4.39] 3– 4 children [AOR = 3.87, 95% CI:3.87, 6.24] and 5 and above [AOR = 7.06, 95% CI: 4.27, 11.69], completed primary [AOR = 1.52, 95% CI: 1.22, 1.88] and higher education [AOR = 1.72, 95% CI: 1.01, 2.94], having educated husband [AOR = 1.35, 95% CI: 1.12, 1.63], being from richer households [AOR = 1.41, 95% CI:1.09, 1.82], and had declared infecund [AOR = 0.13, 95% CI: 0.046, 0.36] were independently associated with modern contraceptive utilization among married women in Liberia.
Conclusion: The prevalence of modern contraceptive utilization among reproductive-age women in Liberia was low. Contraceptive utilization was affected by partners’ education and participants’ socio-demographic and obstetric attributes. Thus, public health interventions are urgently required to enhance use of contraceptives among this group of population.
Keywords: modern contraceptive method, married reproductive age women, Liberia
Background
Contraception is defined as the intentional prevention of conception or pregnancy during sexual activity.1 Modern contraceptive utilization is a human right issued under the international human rights law. The use of modern contraception helps couples and individuals realize their basic right to decide freely and responsibly on their family.2–8 Contraceptive methods help individuals control the number, interval, and timing of pregnancies and births. Traditional and modern methods are the two common types of contraceptive methods. Modern contraceptive methods are more effective than traditional methods that include pills, the intrauterine device (IUD), injectable, implants, and condoms. Sub-Saharan Africa has the highest average fertility rate in the world.9–13 It was estimated that 222 million women in developing countries would like to delay or stop childbearing but are not using any contraception.14,15 Contraceptive use prevented 218 million unintended pregnancies in developing countries in 2012, averting 55 million unplanned births, 138 million abortions (of which 40 million are unsafe), and 118,000 maternal deaths.15 The contraceptive prevalence rate among married women in sub-Saharan Africa increased from 14.7% in 2000 to 27.9% in 2019 and 29.6% in 2021.16,17 In the past decades, studies in developing countries have shown that contraceptive use is influenced by various factors; these factors include demographic characteristics, religious beliefs, knowledge of contraception, education of couples, gender preference among children, the quality of the Contraception among women, limited choice of methods, and fear or experience of side-effects.6,11,18–24 The unmet need for modern contraception is high in Liberia.14,24 The 2019 Liberia Demographic and Health Survey (LDHS) reported that 33% of women have an unmet need for family planning (21% for spacing and 13% for limiting). Subsequently, the total fertility rate (TFR) in Liberia was estimated to be approximately 4.2 children per woman. About 24% of married women are currently using a modern method of contraception. Injectable, implants, and pills are the most commonly used methods.25 Condoms reduce the risk of transmission of many Sexually Transmitted Infections (STIs), including Human Immune Virus/Acquired Immune Deficiency Syndrome (HIV/AIDS) when used consistently and correctly.2 To decrease the high burden of maternal mortality and obstetric complication by increasing modern contraceptive utilization Liberia established a five-year costed implementation plan (CIP) (2018–2022). The CIP describes priority interventions to increase the modern contraceptive prevalence rate (mCPR) at the national level from 30.7% in 2016 to 39.7% in 2022.26 Achieving this plan is estimated to avert more than 600,000 unintended pregnancies and nearly 216,000 abortions and will prevent more than 3300 maternal deaths.27 Modern contraceptive is an important and cost-effective public health intervention to reduce maternal mortality and avert unintended pregnancies, especially in developing countries.13,17,28 However, mCPR was low in most of the developing countries, including Liberia.7,27,29 To increase the level of contraceptive use, it is necessary to understand factors that significantly influence contraceptive use. Therefore, assessment of the various socio-demographic and reproductive variables that contribute to contraceptive use is essential to the development of effective family planning programs. This study aimed to examine the factors affecting modern contraceptives utilization among married women aged 15–49 years in Liberia, and the finding will help to assess culturally acceptable interventions to increase modern contraceptive utilization.
Methods
Study Design, Data Source, and Population
This study was based on a large community-based cross-sectional survey, Liberia Demographic Health Survey (LDHS), conducted From October 16, 2019, to February 12, 2020, in Liberia. The 2019–20 LDHS used a stratified two-stage cluster design, the first stage involved clusters and the second stage involved systematic sampling of households. 4654 reproductive-age women were included, of those 4216 were married women. Liberia is a West African country bounded by Sierra Leone to the Northwest, Guinea to the North, Côte d’Ivoire to the east, and the Atlantic Ocean to the South and west. The current total population of Liberia is 5,214,517. The country has designed a strategic plan named Family planning costed implementation plan (CIP/2018–2022) to increase contraceptive utilization among reproductive-age women and to ensure the realization of the human right to use modern family planning method declared under the international human rights law. The country is also making an effort to achieve its plan by reducing the occurrences of unwanted pregnancy and its complications.
Population
All married reproductive-age women were included in the study. The current study used data extracted from 2019 LDHS from individual records of 4216 married women who were in the reproductive age group. The authors selected only married women for the analysis because Married women are already exposed to sexual intercourse and are supposed to use modern contraceptive methods to limit the number of their children and spacing of their birth intervals. We left out unmarried women because they may not be engaged in frequent sexual activity. Pregnant and unmarried women were excluded from the current study.
Variables of the Study
Dependent Variable
Modern Contraceptive Utilization
In the current study, a woman was considered as a modern contraceptive method user if she reported to use at least one of the modern contraceptives (female sterilization, male sterilization, IUCD, injectable, implants, pills, male condom, female condom, emergency contraception) during DHS data collection period.20
Independent Variables
Independent variables included socio-demographic characteristics (age, religion, region, educational status, wealth index, residence, occupation), respondents’ media exposure (reading newspaper or magazine, listening to the radio, and watching TV), obstetric characteristics (fertility preference, number of living children and visit to health facility) and husbands’ socio-demographic characteristics (educational status, occupation and desire to have a child).4,14,18,20,21,24,30–32
Data Analysis
Stata version 14.0 was used for statistical analysis. Descriptive studies like measures of central tendency and measures of dispersion for continuous data, and frequency count and proportion for categorical data were used to summarize the data descriptively. Bivariable logistic regression was used to select candidate variables for multivariable logistic regression, by which variables with a p-value of less than 0.2 were passed to the multivariable regression. Multivariable logistic regression was used to identify independent predictors of modern contraceptive method utilization among married women in Liberia and to control confounders. Adjusted odds ratio was used to measure the association between modern contraceptive utilization and predictor variables. A p-value of less than 0.05 and 95% confidence interval were used to declare statistical significance
Results
Socio-Demographic Characteristics
The mean age of respondents was 32.66 (±8.36) years with the age range of 15–49 years. From the total 4216 respondents interviewed, 204 (4.85%) were within the age group of 15–19 years. Out of the total participants of this study, 788 (18.69%) and 819 (19.43%) were found in the age groups of 25–29 and 30–34 years, respectively. From the total of respondents, 400 (9.49%), 1801 (42.74%), and 1464 (34.73%) were from northwest, south-central, and north-central regions. Regarding the religion of the participants, 3482 (82.59%) were Christians and 658 (15.62%) were Muslims. Concerning, the residence of respondents 1948 (46.2%) women were rural and 2268 (53.8%) urban residents. Concerning educational status, 1814 (43.02%) were not educated and 1101 (26.13%) women had uneducated husbands. Regarding the economic status of the women, 931 (22.07%) women were from the poorest, and 792 (18.78%) were from the richest family. Regarding occupational status 1013 (24.07%) of women had no work (Table 1).
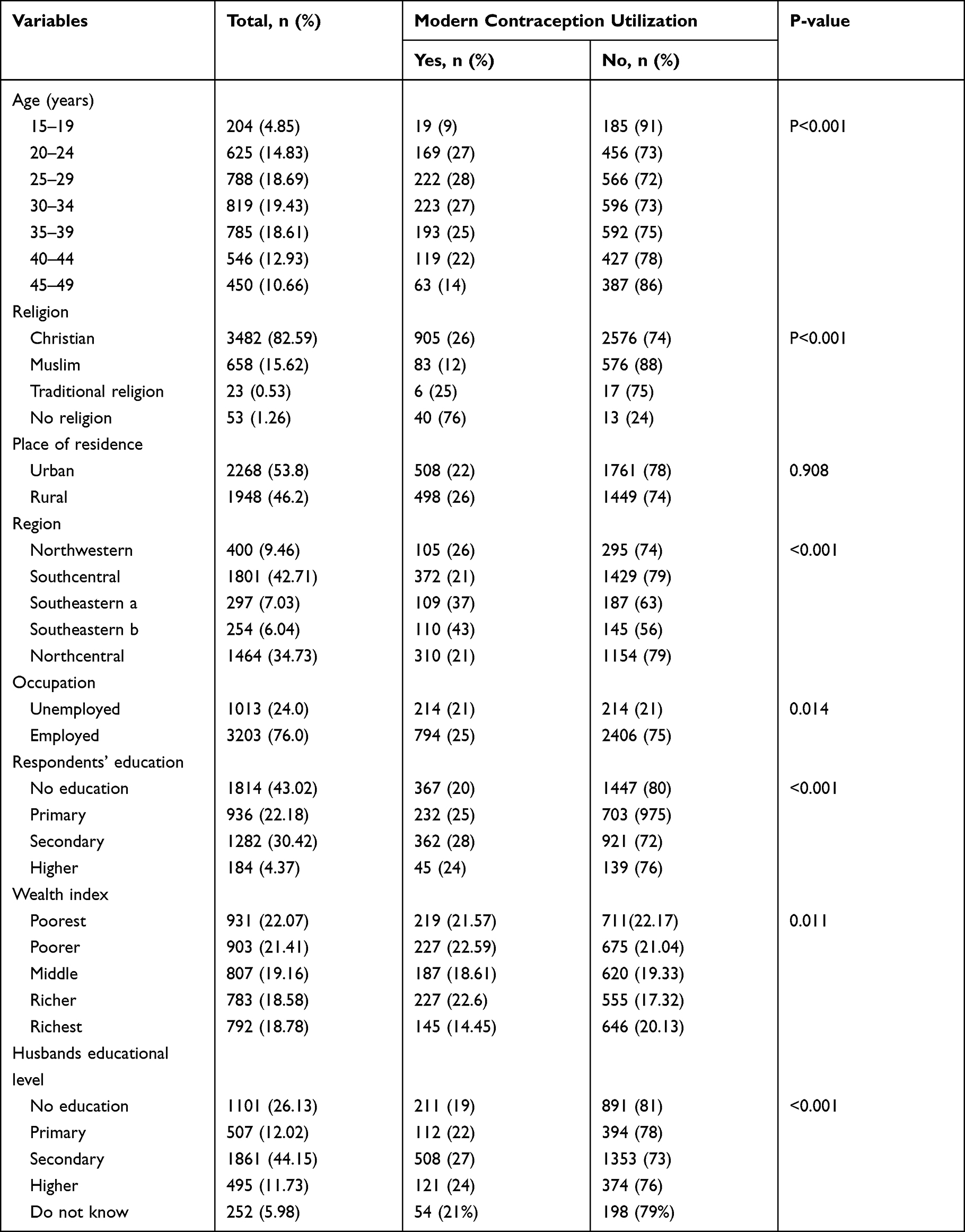 |
Table 1 Socio-Demographic Characteristics of the Respondents (n = 4216) |
Obstetric and Media Exposure Related Characteristics of Respondents
Regarding knowledge of contraceptive methods, 4161 (98.72%) of married reproductive women know modern contraceptive methods 189 (4.5%). 249 (5.9%) of the participants never give birth, whereas 1094 (25.96%) of the participants had five and an above number of children. 3796 (90.05%), 1768 (41.94%) and 2867 (68.02%) did not read the newspaper, listen to the radio and watch television. Concerning decision-making on contraceptive use, 508 (48.35%) reproductive age women jointly decided with their husbands and 400 (38.1%) of married women decided on their own. Concerning fertility preference, 2268 (53.82%) want to have another child (Table 2).
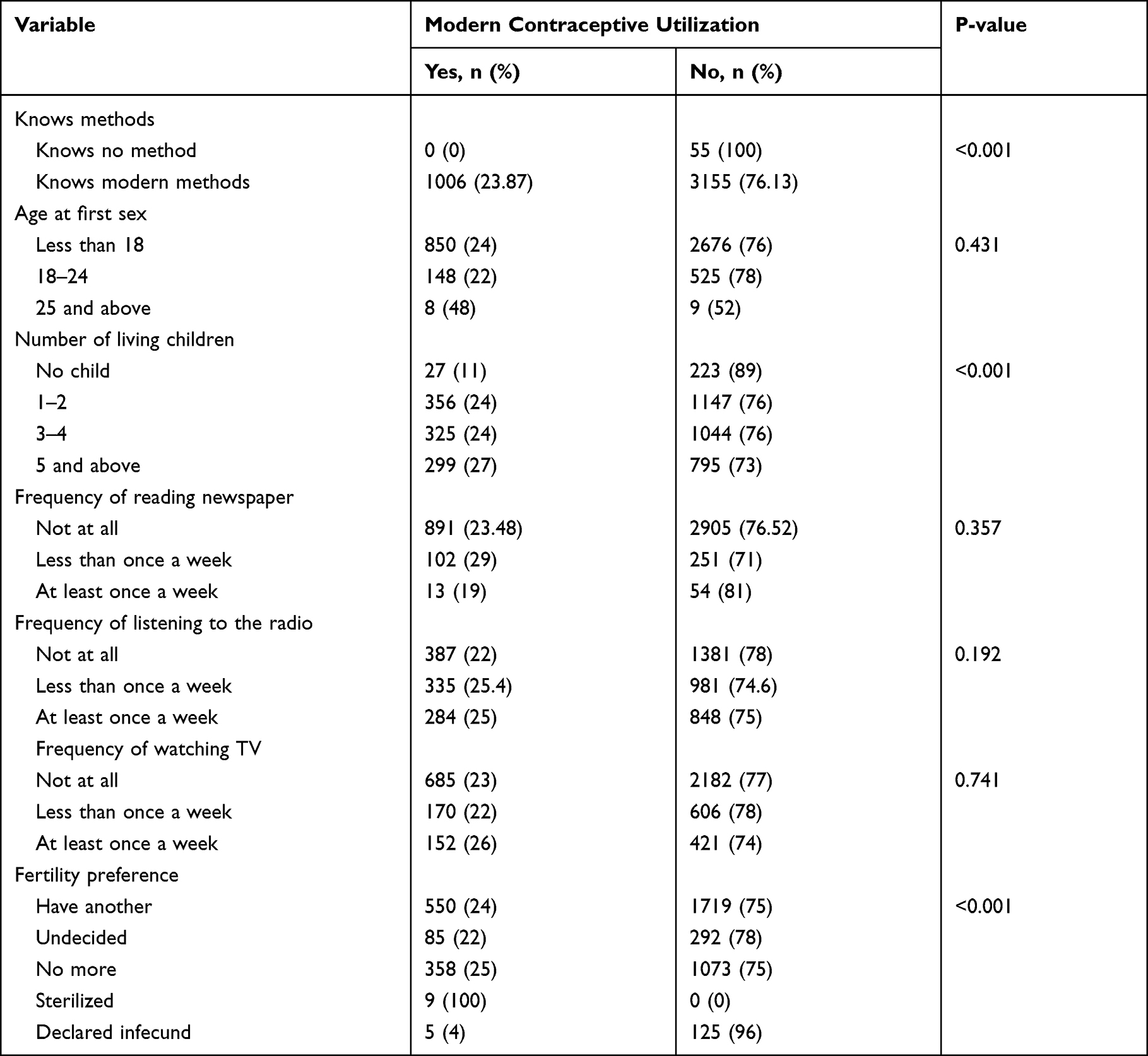 |
Table 2 Obstetric and Media Exposure Among Reproductive-Age Women in Liberia |
Prevalence of Modern Contraceptive Use
The overall prevalence of modern contraceptive utilization was 1006 (23.87%, 95% CI:27.3, 29.9). The injectable contraceptive method was the most, 579 (13.74%) commonly used modern contraceptive method followed by implant/Norplant, 195 (4.63%) (Table 3).
 |
Table 3 Prevalence of Modern Contraceptive Among Married Reproductive Age Women in Liberia |
Factors Associated with Modern Contraceptive Use
Bivariable logistic regression was fitted to identify candidate variables for multivariable logistic regression. Accordingly, age of the respondents, religion, region, educational level, occupation, number of living children, husband’s educational level, and husband’s desire for a child, women’s fertility preference, wealth index, frequency of listening to the radio, and frequency of reading newspaper or magazine were a candidate for multivariable logistic regression. Consequently, age of the participants, region of residence, occupation, number of living children, Husband’s education, educational status, religion, women’s fertility preference, and wealth index were independently associated with modern contraceptive utilization (Table 4).
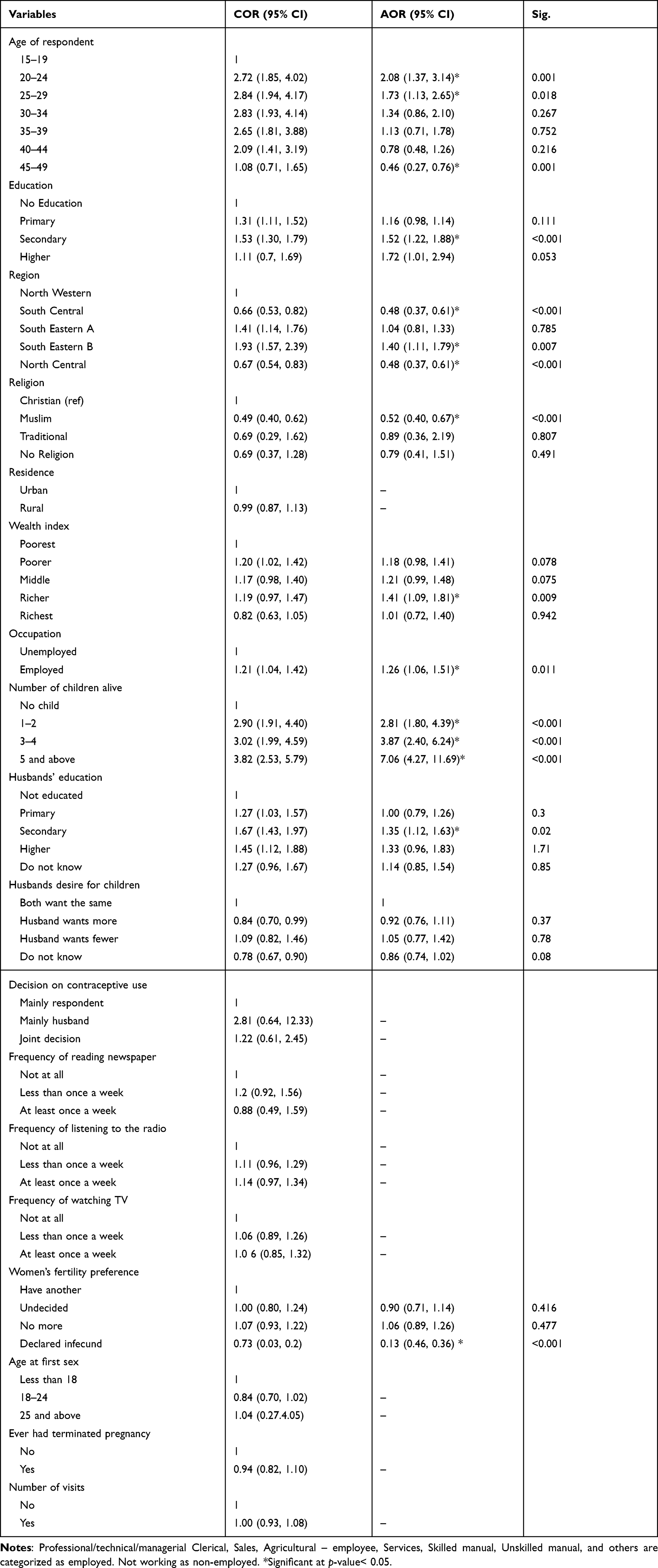 |
Table 4 Factors Associated with Modern Contraceptive Utilization Among Reproductive-Age Women in Liberia, 2019 |
Women with the age group of 20–24 and 25–29 years, was nearly 2.08 [AOR = 2.08 (1.37, 3.14)], and 1.73 [1.73 (1.13, 2.65)] times more likely to utilize modern contraceptive methods as compared to women with the age group of 15 and 19 years. The odds of contraceptive utilization were 54% lower among participants with the group of 45–49 years as compared to participants with the age group of 15–19 years [AOR = 0.46, 95% CI: 0.27, 0.76]. The odds of modern contraceptive utilization was decreased by 48% among Muslim married women as compared with Christian women [AOR = 0.52, 95% CI: 0.399, 0.67]. A woman who resides in regions South Eastern Regions (B) of Liberia was nearly 1.40 [AOR = 1.40, 95% CI: 1.11, 1.79] times more likely to utilize modern contraceptive methods as compared to a woman who resides in the northwestern region. Living in south central [AOR=0.48 95% CI:0.37, 0.61] and North Central region [AOR = 0.48, 95% CI: 0.37, 0.61] of Liberia has a reduced likelihood of using contraception by 52% as compared with northwestern. A woman who has been employed was 1.26 [AOR = 1.26, 95% CI: 1.06, 1.51], times more likely to utilize modern contraceptive methods as compared to a woman who had not been employed. Women who had 1–2, 3–4, and 5 or more living children were 2.81 [AOR = 2.81, 95% CI: 1.80, 4.39], 3.87 [AOR = 3.87, 95% CI: 3.87, 6.24] and 7.06[AOR = 7.06, 95% CI: 4.27, 11.69] times more likely to utilize modern contraceptive methods as compared to women who had no children, respectively. Women who had completed primary and higher education were 1.52 [AOR = 1.52, 95% CI: 1.22, 1.88], and 1.72 [AOR = 1.72, 95% CI: 1.01, 2.94] times more likely to utilize modern contraceptive methods as compared to those who was not educated, respectively. A woman whose husband had completed secondary education was nearly 1.35 [AOR = 1.35, 95% CI: 1.12, 1.63] times more likely to utilize modern contraceptive methods as compared to a woman whose husband was not educated. A woman who was from a richer was 1.41 [AOR = 1.41, 95% CI: 1.09, 1.82] times more likely to utilize modern contraceptive methods as compared to a married woman from the poorest household. The odds of modern contraceptive utilization were decreased by 87% [AOR = 0.13, 95% CI: 0.046, 0.36] among women who declared infecund as compared with married women who want another child (Table 4).
Discussions
This study was conducted to assess the magnitude of modern contraceptive use and associated factors among reproductive age groups in Liberia. In the present study, the overall prevalence of modern contraceptive utilization among married women was 23.87%. The finding is almost consistent with the result of secondary data analysis of Burkina Faso demographic health survey and cross-sectional study done in Hadiya Ethiopia where the prevalence of modern contraceptive utilization was 23.6% and 23.9% respectively.29,33 However, the current prevalence is higher than the results of secondary data analysis of Liberia (22%) and Nigeria (10.3%), Ethiopia (20.42%), Mali (15.3%), and Afghanistan (11.3%) Demographic and Health Surveys.9,20,24,29 The results of the current study are also higher than cross-sectional studies done in Benishangul Gumz Ethiopia, (18.6%), Cameroon (13%), and somewhere else in Ethiopia (20.8%).18,34,35 The results of the present study are lower than the results of secondary data analysis of Tanzania (34.3%) and Bangladesh (62.4%) Demographic and Health Surveys, which were conducted in 2016 and 2014, respectively.36,37 This is also lower than cross-sectional studies done in Ghana (64.4%), Gondar, Ethiopia (41.2%) and Dembia, Ethiopia (31.7%).4,8,21 The possible reason for the discrepancies might be due to a difference in knowledge and awareness of modern contraceptive methods. The difference might also be due to the socio-cultural difference between the different countries that might have a great impact on contraceptive utilization. This lower contraceptive utilization rate implies that there is lower maternal health care utilization in the country that in turn shows that there will be higher fertility and infant mortality rates.
The current study revealed that the injectable contraceptive method was the most commonly used contraceptive method which was consistent with the results of different studies done in Ethiopia and Liberia.20,24,33,35,38
In the current study, age was an independent predictor of modern contraceptive method utilization among married reproductive-age women in Liberia. Women with the age group of 20–24 and 25–29 years, were more likely to utilize modern contraceptive methods as compared to those within the age group of 15 and 19 years. This finding is in line with a study done in Sierra Leone.32 This might be due to the fact that women at younger age are less likely to engage in income generating activities and therefore they may not be able to buy contraceeptives unlike older women. Women with the age of 45 and 49 years were less likely to use contraceptives as compared with those aged between 15 and 19. Results from secondary data analysis of Liberia, Ethiopia, Indonesia and Senegal Demographic and Health Surveys also showed that a woman whose age was from 45 to 49 years less likely to use modern contraceptive, which is consistent with the current study.20,24,39–41 The possible reason might be that women with older reproductive age group may experience peri-menopausal symptoms that may reduce their likelihood of using modern contraceptive methods. In addition, such women may have medical conditions that make some contraceptive methods inappropriate. Older women of reproductive age might have reduced desire to use contraceptive methods than younger women because of lower fecundity (probability of achieving a live birth per menstrual cycle) and less frequent sexual intercourse. Even if women become financially strong as they get older, these conditions hinder the utilization of modern contraceptive methods among women aged 45–49 years.
The study also showed that the region of residence was an independent predictor of modern contraceptive method utilization among married reproductive-age women. A woman who resides in regions South Eastern Regions (B) of Liberia was more likely to utilize modern contraceptive methods as compared to a woman who resides in the northwestern region. Living in south central and North Central region of Liberia has a reduced likelihood of using contraception as compared with north western. This is consistent with a study done in Liberia using 2013 demographic survey data.24
In the current study, the occupation was independently associated with modern contraceptive utilization. Reproductive age women who are employed were more likely to utilize modern contraceptive methods as compared to unemployed reproductive-age women. The finding is consistent with studies done in Ethiopia, Indonesia, Rwanda, and Bangladesh using secondary data analysis of demographic health survey data.20,39,40,42 This could be due to the reason that employed women women may have better income, access to media and healthcare services, that could positively influence women's modern contraceptive utilization. The number of children was also independently associated with the utilization of modern contraceptive methods. Women who had 1–2, 3–4, and 5 or more children were more likely to use modern contraceptives as compared to women with no child at all. This is consistent with the study done in Ethiopia, Liberia, and Rwanda.20,24,40 This may be due to the reason that women with a fewer number of children may need to bear more children to attain the desired family size.
The husband’s educational status was significantly associated with modern contraceptives utilization. A woman whose husband had completed secondary education was more likely to utilize the modern contraceptives as compared to a woman whose husband was not educated. The finding is consistent with the study done in Ethiopia, Liberia, and Senegal.20,24,43 This could be due to the reason that educated husbands might have a good understanding of modern contraceptives and compromise unreasonable social norms, beliefs, and attitudes towards modern contraceptive utilization and encourage their wives to utilize them. Besides, educated husbands may better share decision-making autonomy with their wives and approve the utilization of modern contraceptive utilization. Husband’s education is also related to better household income that has a positive impact on modern contraceptive utilization. Educated husbands might have good knowledge about the importance of using contraceptive methods and empower their wives to use modern contraceptive methods.
The current study also revealed that the wealth index was independently associated with current modern contraceptive utilization. Women from a richer households were more likely to utilize modern contraceptives as compared to reproductive-age women from the poorest households. This finding is in line with the secondary data analysis of the Demographic and Health Survey in Indonesia, Senegal, Rwanda, Liberia, Ethiopia, Nigeria, Afghanistan, and Bangladesh.6,9,10,20,24,39,40,43 This might be due to the reason that the richer woman might have more access to media and health facilities and might have a better awareness of modern contraceptive methods than those from a poorest family.
The present study also revealed that women’s educational status was significantly associated with current modern contraceptive use. A woman who had completed primary and higher education was more likely to utilize modern contraceptive methods as compared to a woman who was not educated. Educated women are more likely to utilize modern contraceptive methods than non-educated women are. This is consistent with the secondary analysis of demographic health surveys in Ethiopia, Indonesia, India, Rwanda, Liberia and Nigeria.9,10,20,24,39,40 The possible reason might be because of educated women might have a good knowledge and a positive attitude towards modern contraceptives. Educated women may also have more media exposure and access to health facilities.
In the current study, religion was significantly associated with modern contraceptive use. Muslims are less likely to use modern contraceptive methods as compared with Christians. This finding is inconsistent with the secondary data analysis of Liberia’s Demographic Health Survey (2013) in which traditional religion was significantly associated with modern contraceptive use.24 The possible reason for the discrepancy might be a difference in sample size, study population that is the present study uses only married Liberian women, and the total sample size was smaller than the previous study. The other possible reason might be due to Islam religion that allows polygamy and most the women who follow this religion believed that they can gain much of their husband’s attention when they got pregnant for him.44 Being in a polygamous relationship may reduce the likelihood of using modern contraceptive methods.45
In the current fertility, preferences were significantly associated with modern contraceptive utilization. Those women who have a declared infecund have less likely to use modern contraceptives. Those women who have a desire to have another child have also reduced the odds of using a modern contraceptive. This finding is in line with the study done in Ethiopia.35 The possible reason might be those women who want to have a child in the near future might not intend to utilize contraceptive methods.
Strengths
The study used nationally weighted representative data that better reflects the proportion of married women using the modern contraceptive method and its associated factors at the national level and regional level. Another strength of the current study is the use of a large sample size that can help to increase the statistical power and validity of the study. Utilization of large sample size and nationally representativeness of DHS data helps to generalize to the population of Liberia.
Limitations
Since the study used data from a single-time survey, it is impossible to ascertain the temporal relationship between modern contraceptive use and its predictor variables. Moreover, since this study was solely dependent on the secondary data set, some important variables that would affect modern contraceptive utilization may not be included.
Conclusions
The magnitude of modern contraceptive utilization among married women in Liberia was very low. Age, religion, region, woman’s occupation, number of living children, husband’s education, women’s educational status, wealth index and number of health facility visits and women’s fertility preference were independent predictors of modern contraceptive use among married reproductive-age women in Liberia. Public health intervention such as a behavior change communication is urgently required to enhance contraceptives utilization among this group of population. Furthermore, interventions should give due emphasis to factors that were significantly affecting women’s contraceptive utilization. Qualitative researches are required to explore further the barriers ofcontraceptive utilization in Liberia.
Abbreviations
AOR, Adjusted Odds Ratio; CI, Confidence Interval; CIP, Costed Implementation Plan; COR, Crude Odds Ratio; DHS, Demographic Health Survey; IUCD, intrauterine Contraceptive Device; LDHS, Liberia Demographic Health Survey; MCPR, Modern Contraceptive Prevalence Rate; TFR, Total Fertility Rate.
Data Sharing Statement
The datasets used and/or analyzed during the current study are publicly available at www.dhsmeasure.org.
Ethical Considerations
The DHS program conducted the study after getting ethical approval of the Liberian National Ethics Committee. As it is stated in the 2019–20 LDHS report the DHS obtained informed consent from each participant and anonymized the data set during the analysis.25 Moreover, the data for this study was obtained from the DHS at (http://www.measuredhs.com) after registration and permission had obtained.
Acknowledgment
We would like to express our gratitude to the Demographic Health Survey (DHS) program for giving us 2019 Liberian DHS data.
Author Contributions
MT, KS, and BM contributed to the study conceptualization and provided critical editorial input to the interpretation of the data. MT, KS, and BM conduct the formal analysis and write the draft manuscript. MT, KS, and BM reviewed the drafted manuscript. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval for the version to be published; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Hossain M, Khan M, Ababneh F, Shaw J. Identifying factors influencing contraceptive use in Bangladesh: evidence from BDHS 2014 data. BMC Public Health. 2018;18:1–14. doi:10.1186/s12889-018-5098-1
2. World Health Organization and Johns Hopkins Bloomberg School of Public Health, Knowledge for Health Project. Family planning: a global handbook for providers (2018 update). Baltimore and Geneva: CCP and WHO; 2018. Available from: https://www.fphandbook.org/sites/default/files/global-handbook-2018-full-web.pdf.
3. UNFPA. Research on Factors that Determine Women’s Ability to Make Decisions About Sexual and Reproductive Health and Rights. UNFPA; 2019:9–11.
4. Oumer M, Manaye A, Mengistu Z. Modern contraceptive method utilization and associated factors among women of reproductive age in Gondar City, Northwest Ethiopia. Open Access J Contracept. 2020;11:53–67. doi:10.2147/OAJC.S252970
5. OHCHR. World Contraception day; 2021. Available from: https://www.ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx?NewsID=27517&LangID=E.
6. Osmani AK, Reyer JA, Osmani AR, Hamajima N. Factors influencing contraceptive use among women in Afghanistan: secondary analysis of Afghanistan Health Survey 2012. Nagoya J Med Sci. 2015;77:551–561.
7. Beson P, Appiah R, Adomah-Afari A. Modern contraceptive use among reproductive-aged women in Ghana: prevalence, predictors, and policy implications. BMC Womens Health. 2018;18:1–8. doi:10.1186/s12905-018-0649-2
8. Afriyie P, Tarkang EE. Factors influencing use of modern contraception among married women in Ho west district, Ghana: descriptive cross-sectional study. Pan Afr Med J. 2019;33:1–11. doi:10.11604/pamj.2019.33.15.17500
9. Ofonime JE. Determinants of modern contraceptive uptake among Nigerian women: evidence from the national demographic and health survey. Afr J Reprod Health. 2017;21:89–95. doi:10.29063/ajrh2017/v21i3.8
10. Dey AK. Socio-demographic determinants and modern family planning usage pattern-an analysis of National Family Health Survey-IV data. Int J Commun Med Public Health. 2019;6:738. doi:10.18203/2394-6040.ijcmph20190200
11. Sharan M, Soucat A, May J, Ahmed S. Family planning trends in Sub - Saharan Africa: progress, prospects, and lessons learned. Yes Africa Can. 2011;445:258643–1271798012256.
12. Aviisah PA, Dery S, Atsu BK, et al. Modern contraceptive use among women of reproductive age in Ghana: analysis of the 2003–2014 Ghana Demographic and Health Surveys. BMC Womens Health. 2018;18:1–10. doi:10.1186/s12905-018-0634-9
13. Maria A, Gomes DJ. Exploring women’s knowledge, attitudes and practices about family planning in a rural area of Timor-Leste. 2018.
14. Okigbo CC. Factors associated with unmet need for modern contraception in post-conflict Liberia. Afr J Reprod Health. 2014;18:58–67.
15. World Health Organization. Contraception. Geneva; 2012. Available from: http://apps.who.int/iris/bitstream/handle/10665/112319/WHO_RHR_14.07_eng.pdf?sequence=8.
16. WHO African Region. Sexula and reproductive health fact sheet; 2004. Available from: https://www.afro.who.int/sites/default/files/2020-06/Sexualandreproductivehealth-Factsheet28-05-2020.pdf.
17. Ahinkorah BO, Budu E, Aboagye RG, et al. Factors associated with modern contraceptive use among women with no fertility intention in sub-Saharan Africa: evidence from cross-sectional surveys of 29 countries. Contracept Reprod Med. 2021;6:1–13. doi:10.1186/s40834-021-00165-6
18. Adane AA, Bekele YA, Melese E, Worku GT, Netsere HB. Modern contraceptive utilization and associated factors among married gumuz women in Metekel Zone North West Ethiopia. Biomed Res Int. 2020;2020:1–7. doi:10.1155/2020/8010327
19. Dingeta T, Oljira L, Worku A, Berhane Y, Ortega JA. Low contraceptive utilization among young married women is associated with perceived social norms and belief in contraceptive myths in rural Ethiopia. PLoS One. 2021;16:1–15. doi:10.1371/journal.pone.0247484
20. Gebre MN, Edossa ZK. Modern contraceptive utilization and associated factors among reproductive-age women in Ethiopia: evidence from 2016 Ethiopia demographic and health survey. BMC Womens Health. 2020;20:1–14. doi:10.1186/s12905-020-00923-9
21. Debebe S, Limenih MA, Biadgo B. Modern contraceptive methods utilization and associated factors among reproductive aged women in rural Dembia District, northwest Ethiopia: community based cross-sectional study. Int J Reprod Biomed. 2017;15:367–374.
22. Sserwanja Q, Musaba MW, Mukunya D. Prevalence and factors associated with modern contraceptives utilization among female adolescents in Uganda. BMC Womens Health. 2021;21:61. doi:10.1186/s12905-021-01206-7
23. Sedgh G, Ashford LS, Hussain R. Unmet Need for Contraception in Developing Countries: Examining Women’s Reasons for not Using a Method. Guttmacher Institute; 2016:65.
24. Rourke T. Association between socio-demographic factors and knowledge of contraceptive methods with contraceptive use among women of reproductive age: a cross-sectional study using the 2013 Liberia DHS. 2015:1–51.
25. Liberia demographic and health survey 2019–20. Monrovia, Liberia and Rockville, Maryland, USA: Liberia Institute of Statistics and Geo-Information Services (LISGIS), Ministry of Health, and ICF. Available from: https://www.dhsprogram.com/pubs/pdf/FR362/FR362.pdf.
26. Family planning resource requirements in Liberia. Available from: https://pdf.usaid.gov/pdf_docs/PA00TC2K.pdf.
27. Government of Liberia. Liberia family planning costed implementation plan (2018–2022). Monrovia: Ministry of Health and Social Welfare; 2018. Available from: https://fp2030.org/sites/default/files/10246-10446_FINALLiberiaCIP.pdf.
28. Sserwanja Q, Musaba MW, Mukunya D. Prevalence and factors associated with modern contraceptives utilization among female adolescents in Uganda. BMC Womens Health. 2021;21:1–7.
29. O’Regan A, Thompson G. Indicators of young women’s modern contraceptive use in Burkina Faso and Mali from Demographic and Health Survey data. Contracept Reprod Med. 2017;2:1–8. doi:10.1186/s40834-017-0053-6
30. Kamuyango A, Hou WH, Li CY. Trends and contributing factors to contraceptive use in Kenya: a large population-based survey 1989 to 2014. Int J Environ Res Public Health. 2020;17:1–12. doi:10.3390/ijerph17197065
31. Yemane TT, Bogale GG, Egata G, Tefera TK, Roy V. Postpartum family planning use and its determinants among women of the reproductive age group in low-income countries of Sub-Saharan Africa: a systematic review and meta-analysis. Int J Reprod Med. 2021;2021:1–14. doi:10.1155/2021/5580490
32. Agbadi P, Eunice TT, Akosua AF, Owusu S, Todd CS. Complex samples logistic regression analysis of predictors of the current use of modern contraceptive among married or in-union women in Sierra Leone: insight from the 2013 demographic and health survey. PLoS One. 2020;15:40–44. doi:10.1371/journal.pone.0231630
33. Hamdalla T, Arega A, Markos T. Prevalence and associated factors of modern contraceptive utilization among married women in reproductive age group in Misha Woreda Hadiya Zone, South Ethiopia. J Womens Health Care. 2017;6:3.
34. Edietah EE, Njotang PN, Ajong AB, Essi MJ, Yakum MN, Mbu ER. Contraceptive use and determinants of unmet need for family planning; a cross sectional survey in the North West Region, Cameroon. BMC Womens Health. 2018;18:1–8.
35. Belda SS, Haile MT, Melku AT, Tololu AK. Modern contraceptive utilization and associated factors among married pastoralist women in Bale eco-region, Bale Zone, South East Ethiopia. BMC Health Serv Res. 2017;17:1–12. doi:10.1186/s12913-017-2115-5
36. Yussuf MH, Elewonibi BR, Rwabilimbo MM, Mboya IB, Mahande MJ. Trends and predictors of changes in modern contraceptive use among women aged 15–49 years in Tanzania from 2004–2016: evidence from Tanzania Demographic and Health Surveys. PLoS One. 2020;15:1–14. doi:10.1371/journal.pone.0234980
37. Apanga PA, Kumbeni MT, Ayamga EA, Ulanja MB, Akparibo R. Prevalence and factors associated with modern contraceptive use among women of reproductive age in 20 African countries: a large population-based study. BMJ Open. 2020;10:e041103. doi:10.1136/bmjopen-2020-041103
38. Worku AG, Tessema GA, Zeleke AA. Trends of modern contraceptive use among young married women based on the 2000, 2005, and 2011 Ethiopian demographic and health surveys: a multivariate decomposition analysis. PLoS One. 2015;10:1–14.
39. Antarini A. Factors influencing the use of modern contraception among reproductive aged women in bangka belitung province, Indonesia. Pan Afr Med J. 2021;39. doi:10.11604/pamj.2021.39.39.28870
40. Habyarimana F, Ramroop S. The analysis of socio-economic and demographic factors associated with contraceptive use among married women of reproductive age in Rwanda. Open Public Health J. 2018;11:348–359. doi:10.2174/1874944501811010348
41. Allen RH, Cwiak CA, Kaunitz AM. Contraception in women over 40 years of age. Cmaj. 2013;185:565–573. doi:10.1503/cmaj.121280
42. Haq I, Sakib S, Talukder A. Sociodemographic factors on contraceptive use among ever-married women of reproductive age: evidence from three demographic and health surveys in Bangladesh. Med Sci. 2017;5:31.
43. Zegeye B, Ahinkorah BO, Idriss-Wheeler D, et al. Modern contraceptive utilization and its associated factors among married women in Senegal: a multilevel analysis. BMC Public Health. 2021;21:1–14. doi:10.1186/s12889-021-10252-7
44. Obasohan PE. Ijma-3-63. Int J Matern Child Health AIDS. 2015;3:63–73.
45. Lakew Y, Reda AA, Tamene H, Benedict S, Deribe K. Geographical variation and factors influencing modern contraceptive use among married women in Ethiopia: evidence from a national population based survey. Reprod Health. 2013;10:1–10. doi:10.1186/1742-4755-10-52
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.