Back to Journals » Journal of Pain Research » Volume 18
Modelling Pain Perception Using Fuzzy Cognitive Maps
Authors Farahani H ![]() , Kovač N
, Kovač N ![]() , Fardi H, Watson PC
, Fardi H, Watson PC ![]()
Received 19 March 2025
Accepted for publication 29 July 2025
Published 3 October 2025 Volume 2025:18 Pages 5153—5174
DOI https://doi.org/10.2147/JPR.S525200
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Twillman
Hojjatollah Farahani,1 Nataša Kovač,2 Helal Fardi,3 Peter Charles Watson4
1Department of Psychology, Faculty of Humanities, Tarbiat Modares University, Tehran, Iran; 2Faculty of Applied Sciences, University of Donja Gorica, Podgorica, Montenegro; 3Department of Psychology, Faculty of Education and Psychology, University of Tehran, Tehran, Iran; 4MRC Cognition and Brain Sciences Unit, University of Cambridge, Cambridge, UK
Correspondence: Hojjatollah Farahani, Tarbiat Modares University, Jalal AleAhmed, Tehran, Nasr, 14115-111, Iran, Email [email protected] Peter Charles Watson, Cambridge University, 15 Chaucer Road, Cambridge, CB2 7EF, United Kingdom, Email [email protected]
Purpose: Perception of pain is a multifactorial mechanism involving physiological, psychological and social factors; only by understanding the interplays of these factors can we hope to develop effective management strategies for pain. To that effect, we developed a computational model using Fuzzy Cognitive Maps (FCMs) to simulate and predict individual pain experiences, based on expert input across multiple disciplines. This framework has potential application in individualized pain management, drug development and pain research.
Patients and Methods: The Method of the study is an FCM model based on expert-sourced data for pain perception. A total of 20 experts were recruited using a snowball sampling technique, divided into five specialist groups: neurologists, pain specialists, psychologists, sociologists, and geneticists, with four experts in each group. The experts contributed input in CSV file format specifying concept associations and linguistic terms. Therefore, three types of data collection were used: questionnaires for capturing inter-factor interactions, fuzzy matrices measuring strengths of influences and interviewing in order to validate relationships. The data was then analyzed by summing up expert-defined causal relationships based on fuzzy logic rules, allowing for the construction of the initial weight matrix that reflects both the strength and direction of influence between concepts.
Results: The built FCM model integrates six significant concepts that influence pain perception: brain and neural basis of pain, psychological factors, social factors, individual differences, type of tissue damage and general pain perception. The model structure indicates strong reinforcing influences between psychological and neural factors, while social influences tend to inhibit perceived pain. Centrality analysis highlighted individual differences as a critical mediating node in the system. The model stabilized to an internally consistent fixed point under a variety of initial conditions, providing internal stability.
Conclusion: The findings indicate that the FCM model provides a useful framework for representing interactions between pain and its influencing factors. The model was validated through expert consensus and scenario-based simulations. Future work will include empirical validation using standardized psychological instruments to compare FCM outcomes with real-world psychological profiles.
Keywords: pain perception, fuzzy cognitive maps, pain management, elements of pain perception, medical decision support systems
Introduction
Pain is conventionally defined as an uncomfortable sensation or feeling with actual or potential tissue damage, and it is recognized as a complex multidimensional phenomenon affected by a variety of changes such as neurophysiological, immunological, cognitive, psychological, social and cultural factors. This understanding is vital for forming appropriate pain treatment plans.1–3
Pain perception is not a straightforward, linear process; It varies widely among individuals and cultures, influenced by both subjective interpretation and environmental context.4 These factors interact to shape pain experience, and a structured medical decision-making model is essential for integrating these variables into effective clinical responses and, at the same time infer a decision. To address this need, computational tools capable of handling complexity, subjectivity, and interdependence are required.5
Among such tools, FCMs offer an interpretable and flexible framework for modeling Medical Decision Support Systems (MDSS). FCM is a fuzzy modeling technique that employs the building blocks of fuzzy logic, neural networks, and cognitive maps. FCMs are a robust form of modeling knowledge in systems where there is uncertainty, causality, and complex interactions. In this case, each concept is a definite state or property of the system, and concepts affect each other to describe the dynamic process of the system. These models can incorporate expert knowledge and dynamically update system states via feedback.5,6
FCM is a powerful modeling approach that consists of a range of nodes or concepts (variables) and shows causal relationships through weighted connections between them.7 When multiple experts contribute their perspectives, individual FCMs are synthesized into a comprehensive, consensus-based model.8,9
Pain perception is highly individualized, influenced by an interplay of biological, psychological, socio-cultural, and genetic factors. Neurobiologically, pain signals originating from nociceptors in peripheral tissues travel through the spinal cord to brain regions such as the somatosensory cortex, thalamus, and anterior cingulate cortex. Pain processing involves neurotransmitters including excitatory substances like substance P and glutamate, and inhibitory agents like serotonin, norepinephrine, and endorphins. Central modulation of these signals through neuroplasticity enables adaptations in neural responses, often leading to increased sensitivity and chronic pain conditions.1,2,10–12
Psychologically, pain experience is shaped by cognitive, emotional, and behavioral factors. Protective psychological traits such as optimism and self-efficacy mitigate pain, while vulnerability factors, including fear, anxiety, and pain catastrophizing, enhance pain perception and chronicity. Negative emotions, notably anxiety and anger, significantly contribute to increased pain sensitivity by activating hormonal and neurotransmitter pathways.13–16 Sociocultural context further modulates pain perception. Cultural norms influence the expression and interpretation of pain, with some societies encouraging open emotional displays and others promoting restraint. Strong social support generally correlates with lower pain perception, whereas isolation and lack of support are associated with heightened sensitivity.17–21
Individual differences in pain perception are rooted in both genetic and environmental factors. Genetic variations, evidenced by twin studies, contribute significantly to individual variability in pain sensitivity. Moreover, gender differences exist in pain processing mechanisms, partly due to sex-specific quantitative trait loci (QTLs), hormones, and neurobiological differences. Aging is another critical determinant, affecting pain thresholds and tolerance levels due to progressive sensory system changes. Personality traits, notably neuroticism, extraversion, openness, agreeableness, and conscientiousness, significantly impact how pain is experienced and managed. Higher neuroticism levels correlate with increased pain sensitivity and reduced tolerance, while secure attachment styles and positive personality traits are generally protective against intense pain perception.22–31 Pain classifications (acute vs chronic and nociceptive vs neuropathic) differ primarily by their underlying tissue or nerve damage mechanisms, influencing treatment approaches and prognosis.32–34
Despite the extensive body of literature on the biological, psychological, and social dimensions of pain, a significant research gap remains in modeling how these domains dynamically interact to shape individual pain experiences. Existing clinical and computational models tend to either isolate these factors or lack the interpretability necessary for integration into medical decision-making. For instance, while machine learning algorithms may provide predictive power, they often operate as opaque systems that do not offer causal insight into the mechanisms of pain perception. Conversely, traditional psychometric and clinical approaches may be interpretable but fall short in capturing feedback loops and contextual modulation among factors. To bridge this gap, we propose an FCM framework that synthesizes expert knowledge to construct a transparent, simulation-ready model. The FCM structure enables the encoding of causal, often uncertain, relationships using linguistic variables, while maintaining a level of interpretability conducive to clinical use. This approach offers a novel perspective by embedding domain knowledge directly into the model and facilitating scenario testing, ultimately aiming to support personalized pain assessment and management. The next section describes the development of the FCM model, including expert elicitation methods, data integration, and the rationale for selecting key pain-related concepts.
Material and Methods
FCM model, first introduced by Kosko in 1986, was described as a recurrent neural network that mimics human reasoning and decision-making processes.35 With FCMs, it is feasible to simulate complicated systems, such as the human organism, and also examine patient data, such as symptoms, history and laboratory test results and graphically depict the correlation between different clinical and medical conditions variables.36,37 By encoding causal relationships as perceived by experts, FCMs simulate human-like reasoning through iterative state updates that mirror real-world feedback processes, supporting intuitive decision-making under complex, interrelated conditions.38 FCM consists of different nodes where each node represents a concept, and the arrow between any two linked concepts indicates the presence of a cause-and-effect relationship. Each arrow is weighted, with the value lying anywhere on the scale from 1 to −1. A negative weight implies an inverse relationship, where an increase in one concept leads to a decrease in the other. A positive weight denotes a direct relationship, where an increase in one concept increases the other. The absence of an edge between two nodes signifies their independence within the FCM model. Different FCMs are derived from the knowledge of various experts, where the resulting FCM is the fusion of all these individual FCMs.36,37
The current paper presents a novel medical decision support system utilizing FCMs to enhance pain perception assessment in individuals experiencing acute or chronic pain. This study aims to facilitate early and accurate identification of diverse pain types, enabling more timely and precise diagnoses by focusing on the fundamental factors influencing pain perception. Initially, a literature review was conducted to identify relevant factors, resulting in the selection of 6 key concepts (5 inputs and 1 output), as shown in Table 1.
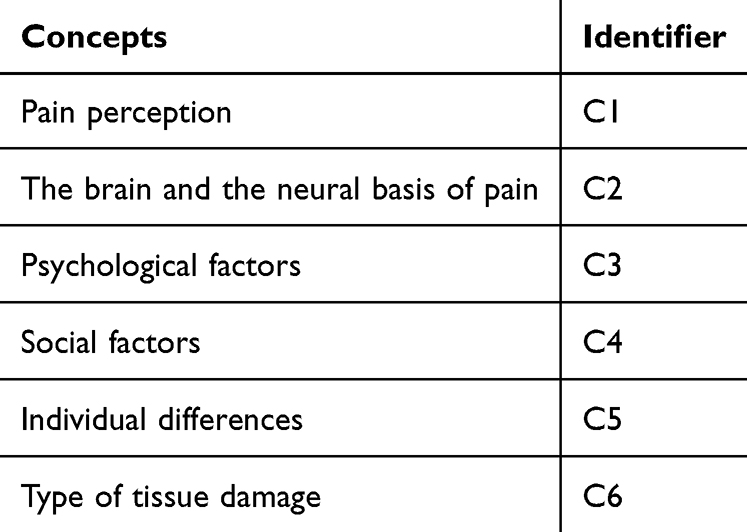 |
Table 1 Core Conceptual Constructs in Pain Modelling and Their Identifiers |
In constructing the FCM model, expert input was gathered to capture relationships and dynamics among the identified concepts. A total of 20 experts participated in the study, organized into five domain-specific groups (neurologists, pain specialists, psychologists, sociologists, and geneticists), with four participants in each. Experts were identified using a snowball sampling technique, which is commonly used in qualitative modeling where domain-specific expertise is required and the expert population is limited or specialized. These individuals were selected for their established contributions in their respective fields and were then asked to recommend peers who could offer complementary insights. While snowball sampling carries a risk of introducing selection bias and homogeneity of viewpoints, since participants tend to nominate individuals with similar perspectives, these limitations were actively mitigated by ensuring that the initial expert pool was intentionally diverse in both discipline and professional background. Experts were interviewed independently to minimize peer influence and groupthink. This sampling method was deemed appropriate given the exploratory and interdisciplinary nature of the FCM construction, where the richness of domain-specific knowledge outweighed the need for randomization. Nevertheless, the potential for sampling bias is acknowledged as a limitation, particularly in how it may influence the weighting of concept relationships in the model.
Data collection employed three methods: questionnaires, fuzzy matrices and interviews. Questionnaires were designed based on the literature review to capture the nature and extent of relationships between factors. In the fuzzy matrix approach, experts quantified the influence of factors using a matrix format. Lastly, in the interview-based method, participants sketched relationships between factors and described their strengths and polarity. Responses were consolidated into a matrix, where rows represented relationships and columns reflected expert opinions. Negative or positive relationships were assigned values based on their intensity, while neutral interactions received a value of zero.39
Building upon the conceptual foundation outlined in the Introduction, the methodology of this study centers on translating the multifactorial understanding of pain perception into a structured, computational model using FCMs. The six primary constructs identified, pain perception (C1), brain and neural basis of pain (C2), psychological factors (C3), social factors (C4), individual differences (C5), and type of tissue damage (C6), were derived through an extensive literature review and selected to represent the most influential and interdependent domains within the biopsychosocial framework of pain. These constructs were not only theoretically grounded but also validated through expert consultation, ensuring their relevance across both clinical and theoretical dimensions.
FCMs are particularly well-suited to this domain because they allow for the representation of causal relationships in systems characterized by uncertainty, complexity, and non-linearity. Each concept (or node) in the FCM corresponds to one of the six identified constructs, and the directed edges between nodes reflect the perceived causal influences among them, quantified by weights ranging from –1 to +1. These weights indicate both the direction and the strength of influence, capturing inhibitory and reinforcing effects. Unlike black-box models, FCMs enable both visualization and interpretability of the relationships, allowing researchers and clinicians to examine how shifts in one domain (eg, psychological distress) may propagate through the network to influence others (eg, pain intensity or social response).
The modeling process was carried out in three stages: expert selection and data elicitation, fuzzy linguistic quantification of concept relationships, and integration of responses into a unified weight matrix. Experts were recruited using a snowball sampling approach and represented five disciplinary perspectives, neurology, psychology, sociology, genetics, and pain medicine. Each expert independently evaluated the relationships among the six constructs using questionnaires, fuzzy matrices, and structured interviews. Their inputs included directional associations, intensity assessments, and qualitative justifications, all of which were encoded in linguistic variables. These linguistic assessments were then translated into numerical weights using predefined membership functions, ensuring consistency in interpretation and mathematical treatment. The resulting model forms the basis for simulation, sensitivity, and policy analysis detailed in the following sections.
The universe of discourse was defined as a range from −1 to 1 with a step size of 0.001, allowing for a fine-grained representation of connection strengths. Each expert was asked to evaluate the pairwise causal relationships between predefined concepts using a 7-point linguistic scale: Very Low Negative (−VL), Low Negative (−L), Medium Negative (−M), High Negative (−H), No Association (NA), Low Positive (+L), Medium Positive (+M), High Positive (+H), and Very High Positive (+VH), as shown in Table 2.
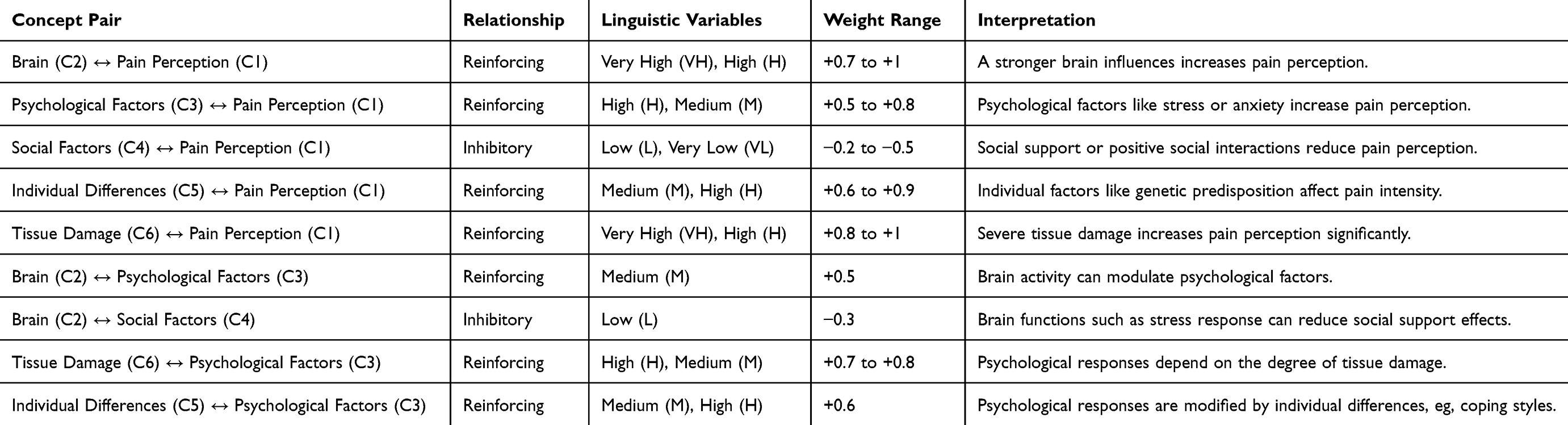 |
Table 2 Fuzzy Linguistic Descriptions and Weight Ranges of Conceptual Relationships in the Pain Model |
To translate expert linguistic assessments into quantitative form suitable for FCM modeling, we defined a structured mapping from real-world qualitative judgments to a numerical interval within [−1,1]. This interval captures the full range of causal influence from strong inhibition to strong stimulation. Linguistic terms (eg, very low, medium, high) were each associated with triangular membership functions defined over this universe of discourse. For example, the linguistic label “+M” (positive medium) corresponds to the fuzzy interval [0.25,0.5,0.75], while “-VH” (very high negative) maps to [−1,−1,−0.75]. These membership functions were defined via standard fuzzy logic conventions and applied uniformly across expert judgments.
Defuzzification was conducted using the centroid method, and the resulting crisp weights inherently fell within [−1,1]. All weights were then aggregated from multiple expert sources using a fuzzy max operator (fMax) and optional entropy-based filtering. We apply the hyperbolic tangent (tanh) as the activation function, which is commonly used in FCMs to model gradual saturation behavior. The outputs of this function lie within (−1,1), and no further transformation was applied. This preserves interpretability in the bipolar space, where negative and positive values denote opposing polarities of concept activation.
The simulation of the FCM dynamics was conducted using Kosko’s reasoning rule,35 which updates the activation level of each concept based on the weighted sum of incoming causal signals. This algorithm can be represented by the following pseudocode:
Input:
- W: Weighted adjacency matrix
- A0: Initial concept activation vector
- f: Activation function (sigmoid)
- T: Maximum number of iterations
- ε: Convergence threshold
Procedure:
1. Set A ← A0
2. For t in 1 to T:
a. Compute A′ ← f(A + A × W)
b. If ||A′ - A|| < ε, break
c. A ← A′
3. Return A (Final Activation Levels)
All modeling and inference processes were implemented using ExpertFCM, a Python-based tool built on top of the fcmpy package.40 ExpertFCM extends the base package with additional functionality, including expert aggregation, entropy visualization, linguistic-weight mapping, and simulation analysis (eg, policy interventions, community detection, node centrality, and sensitivity testing). Visualization and matrix analysis were carried out using matplotlib, seaborn, and pandas.
Results
Before analyzing centrality, sensitivity, and dynamic scenarios, we assessed the global stability characteristics of our FCM model to confirm its suitability for dynamic scenario analysis. Following the spectral analysis methodology,41 we computed the spectral radius (ρ) of the weight matrix. For our FCM model, the spectral radius was 3.25, clearly exceeding the critical threshold of 1 required for global asymptotic stability (ρ(W)<1). This result indicates that our model does not converge to a unique global attractor but rather exhibits potential for multiple equilibria or attractors, depending on initial states or external perturbations. This finding explicitly confirms the dynamic diversity of our model, validating its practical usability in simulating various pain-related scenarios and interventions. With this foundational validation established, we proceed to examine the model’s structural and dynamic properties through centrality analysis, sensitivity testing, and scenario simulations.
Figure 1 showcases a spectrum of influence strengths, with blue shades denoting strong negative influences and red shades indicating strong positive influences. Pain perception (C1) strongly inhibits psychological factors (C3, −0.91) and social factors (C4, −0.78), suggesting a robust regulatory role in emotional and social pain responses. Conversely, brain and neural mechanisms (C2) have dual roles: reinforcing psychological (C3, 0.91) and social factors (C4, 0.70), yet strongly inhibiting tissue damage (C6, −0.71). This duality suggests the brain’s central role as both a mediator and regulator of pain dynamics. Individual differences (C5) notably act as a consistent facilitator, positively influencing nearly all other concepts, underscoring its pivotal role in modulating pain experiences. Tissue damage (C6) emerges primarily as an inhibitor, notably reducing activations in psychological and brain-based nodes, implying its stabilizing or balancing role.
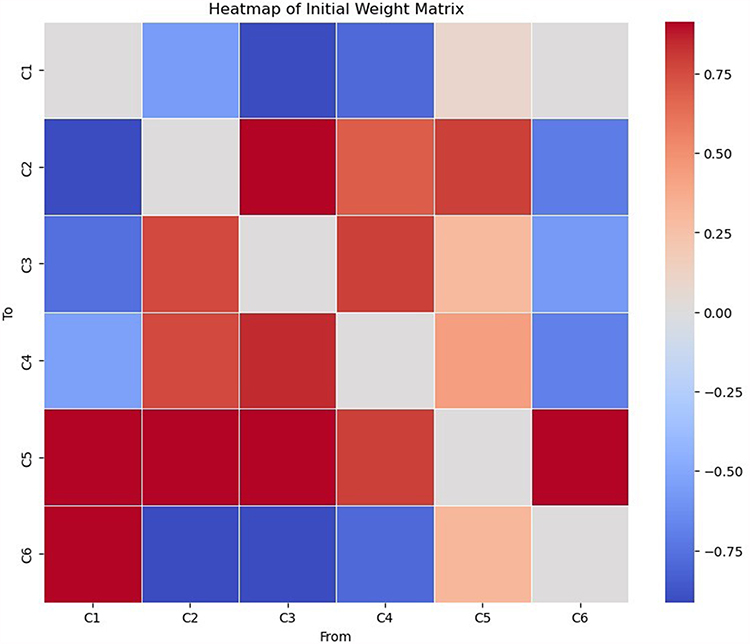 |
Figure 1 Heatmap of the initial weight matrix, displaying the signed connection strengths between all concept pairs in the FCM. Darker colours indicate stronger influence (positive or negative), revealing asymmetries and highlighting dominant pathways such as the strong effects from Psychological Factors (C3) and Social Factors (C4) to Pain Perception (C1). |
Figure 2 shows the summed incoming weights onto each node to evaluate their cumulative receptivity to influence. The node C5 (Individual differences), receiving the most robust combined positive inputs, stands out as a central network reinforcement hub, while C6 (Tissue damage) shows its critical countering role, receiving varied inputs of contrasting strengths.
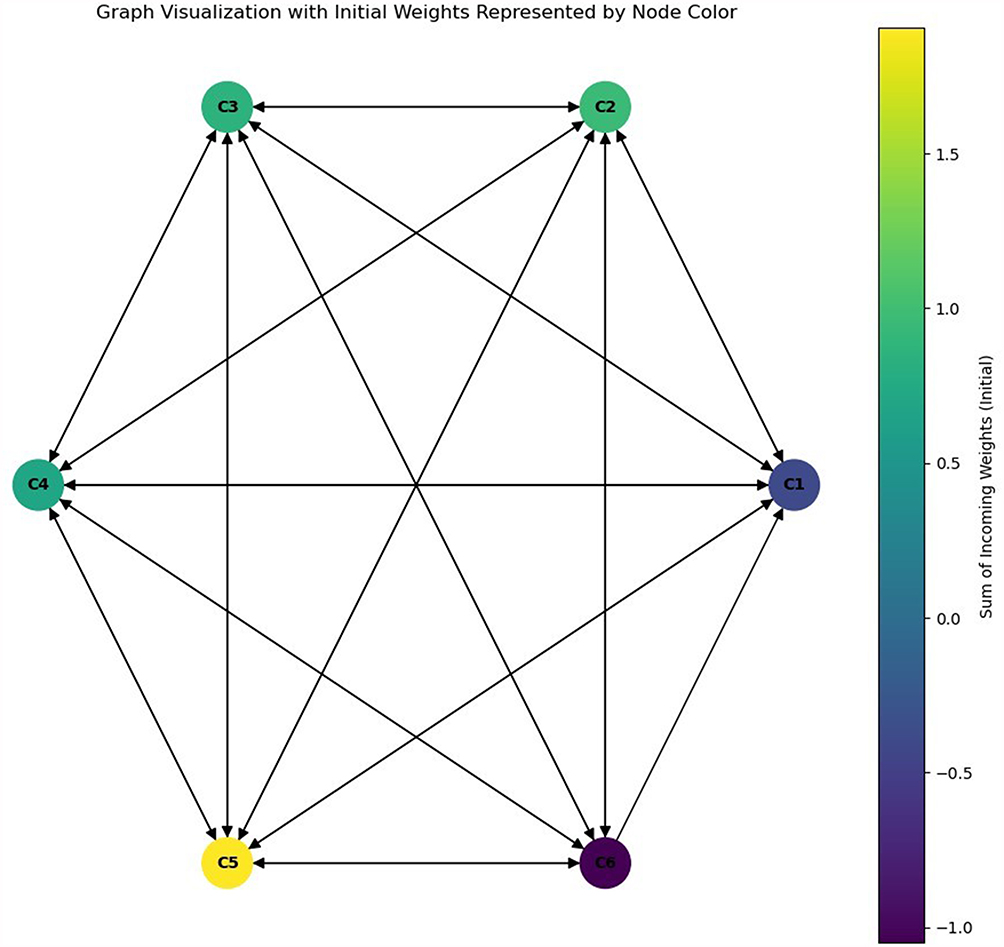 |
Figure 2 Graph visualisation of the FCM with initial weights, where node colour represents total influence strength (in-degree plus out-degree). This topological overview emphasises the network’s most influential nodes and the structure of causal loops within the pain-related system. |
Figure 3 provides a detailed view of the interactions among nodes in the conceptual model, revealing each node’s directional influence on others. The weights, ranging from strong positive to negative values, illustrate the complexity of the relationships and their potential implications for the system’s dynamics.
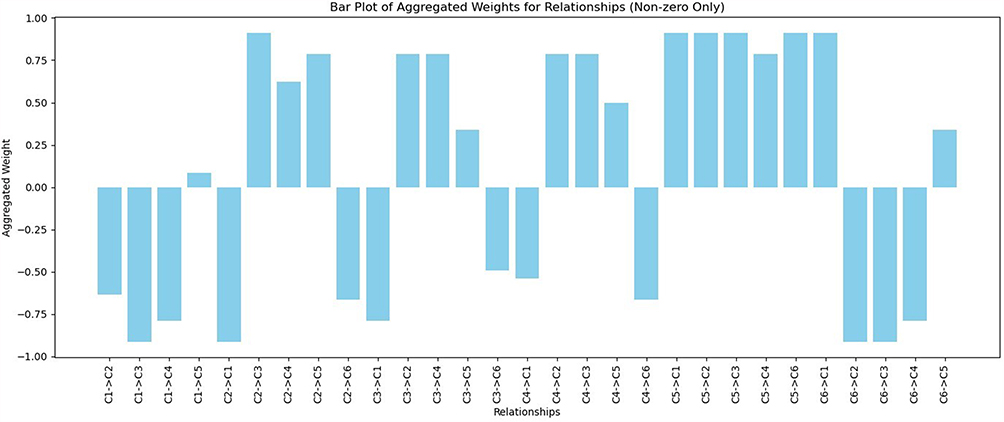 |
Figure 3 Bar plot of all non-zero aggregated weights across concept pairs. The plot emphasises asymmetries in influence, showing that certain concept relationships, especially those involving Psychological Factors (C3) and Social Factors (C4), dominate the causal architecture of the model. |
Negative weights, such as −0.91 for C1 (Pain perception) → C3 (Psychological factors) and −0.91 for C6 (Tissue damage) → C2 (Brain and neural basis of pain) (Brain and neural basis of pain), suggest inhibitory effects where the source node diminishes the target node’s activation level. C1 (Pain perception) → C3 (Psychological factors), for instance, C1 (Pain perception) significant role in dampening C3 (Psychological factors) influence, aligning with its broader balancing function within the network. Similarly, C6 (Tissue damage) negative impact on C2 (Brain and neural basis of pain) and C3 (Psychological factors) highlights its counteractive position, emphasizing its potential to stabilize or disrupt the network depending on its state. Positive weights underscore supportive or reinforcing relationships. C5 (Individual differences), as a central hub, displays strong positive connections, such as C5 (Individual differences) → C3 (Psychological factors) (0.91) and C5 (Individual differences) → C6 (Tissue damage) (0.91), positioning it as a node that amplifies the activation of others. Its uniformly high positive interactions reveal its pivotal role in driving overall system behaviour, potentially enabling cascading effects. Moderate weights, such as C2 (Brain and neural basis of pain) → C4 (Social factors) (0.62) and C4 (Social factors) → C5 (Individual differences) (0.5), highlight interactions that balance reinforcement and inhibition. These relationships suggest nuanced dependencies, where changes in one node moderately influence another without overwhelming the network dynamics. The symmetry and asymmetry of weights between specific nodes, such as C2 (Brain and neural basis of pain) → C3 (Psychological factors) (0.91) versus C3 (Psychological factors) → C2 (Brain and neural basis of pain) (0.78), also reveal the unequal reciprocal influences in certain relationships. Such patterns provide insights into which nodes may disproportionately affect the network’s equilibrium.
Individual differences (C5) appear as a central reinforcing node, while tissue damage (C6) displays complex balancing influences, indicating both stimulatory and inhibitory impacts depending on context.
The centrality analysis (Figure 4) reveals essential insights into each node’s structural and functional roles in the network. The degree centrality values indicate the direct connections a node has with others. Nodes C2 (Brain and neural basis of pain), C3 (Psychological factors), C4 (Social factors), and C5 (Individual differences) exhibit the highest degree of centrality, each with a score of 2.0, suggesting their critical roles as hubs with maximal direct connections. In contrast, nodes C1 (Pain perception) and C6 (Tissue damage), with slightly lower scores of 1.8, have fewer connections but remain integral to the network’s structure.
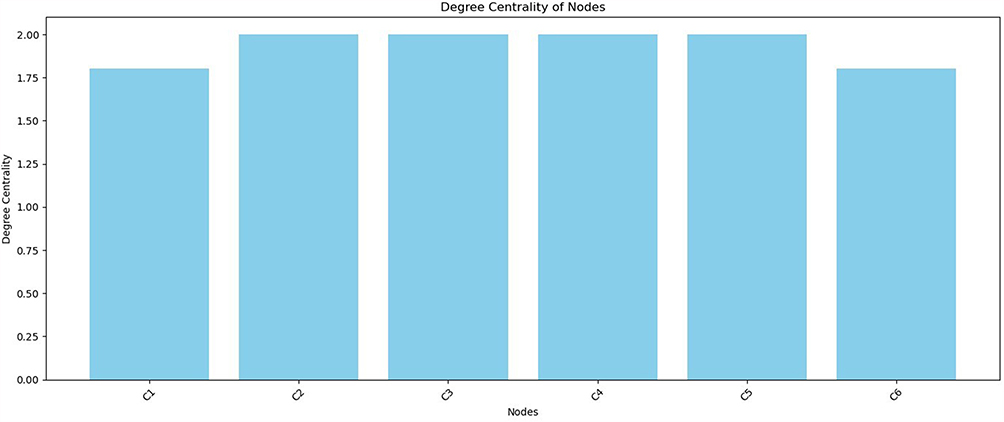 |
Figure 4 Degree centrality of each concept, indicating the number of direct influences received and exerted. Individual Differences (C5) and Psychological Factors (C3) emerge as one of the most connected nodes, confirming their central role in the network and their potential as leverage points in interventions. |
Betweenness centrality (Figure 5) quantifies the degree to which a node acts as a bridge within the network. Nodes C2 (Brain and neural basis of pain), C3 (Psychological factors), C4 (Social factors) and C5 (Individual differences) exhibit moderate betweenness centrality scores of 0.0125, indicating a moderate level of involvement in facilitating communication pathways within the network. Nodes C1 (Pain perception) and C6 (Tissue damage) show zero betweenness centrality, implying they act primarily as endpoints rather than intermediaries.
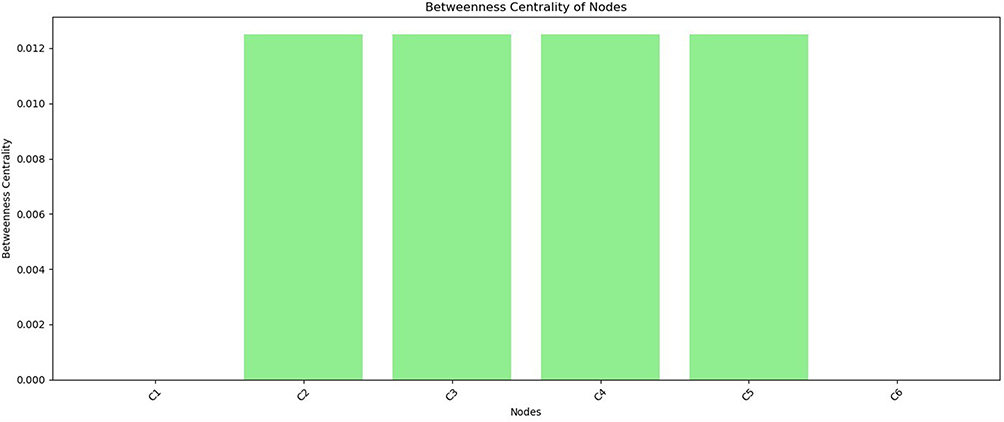 |
Figure 5 Betweenness centrality scores across all nodes, quantifying the extent to which each concept acts as a bridge connecting other nodes in the network. The concepts Brain and neural basis of pain (C2), Psychological factors (C3), Social factors (C4), and Individual differences (C5) share equally high centrality, indicating their collective role as key conduits in facilitating interactions between biological, psychological, and social components of pain perception. |
The closeness centrality (Figure 6) emphasizes how efficiently a node can access others within the network. Nodes C1 (Pain perception), C2 (Brain and neural basis of pain), C3 (Psychological factors), C4 (Social factors) and C5 (Individual differences) demonstrate optimal accessibility, each with a perfect score of 1.0. This highlights their central positions, which can quickly interact with all other nodes. Node C6 (Tissue damage) exhibits a lower closeness centrality of 0.833, suggesting its position is slightly more peripheral than the others.
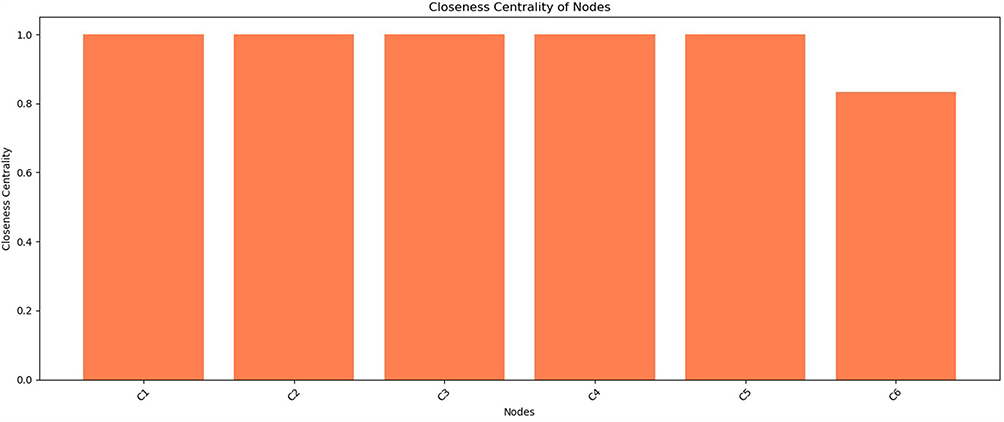 |
Figure 6 Closeness centrality values for each concept, indicating how efficiently a node can influence or be influenced by others in the network. The results reinforce the integrative role of nodes like Individual Differences (C5) and Psychological Factors (C3) in modulating the broader system. |
The node importance analysis (Figure 7) provides a deeper understanding of each node’s roles and influences within the network by considering the sum of incoming and outgoing connections. Node C5 (Individual differences) emerges as the most influential node, exhibiting a notably high importance score of 6.35. This indicates its centrality in propagating influence to other nodes, underscoring its role as a primary driver within the system. Nodes C1 (Pain perception) and C6 (Tissue damage) exhibit negative importance scores of −2.55 and −2.44, respectively. These values highlight their limited or counteracting influence within the network dynamics. They may serve as sinks that absorb influence or as nodes with weaker outgoing interactions. The remaining nodes C2 (Brain and neural basis of pain), C3 (Psychological factors) and C4 (Social factors) show moderate importance scores of 1.73, 1.36 and 1.50, respectively. This suggests balanced roles in which they contribute to and receive influence from other nodes. This balanced positioning may indicate their roles as intermediaries, supporting the influence flow between more dominant and less impactful nodes.
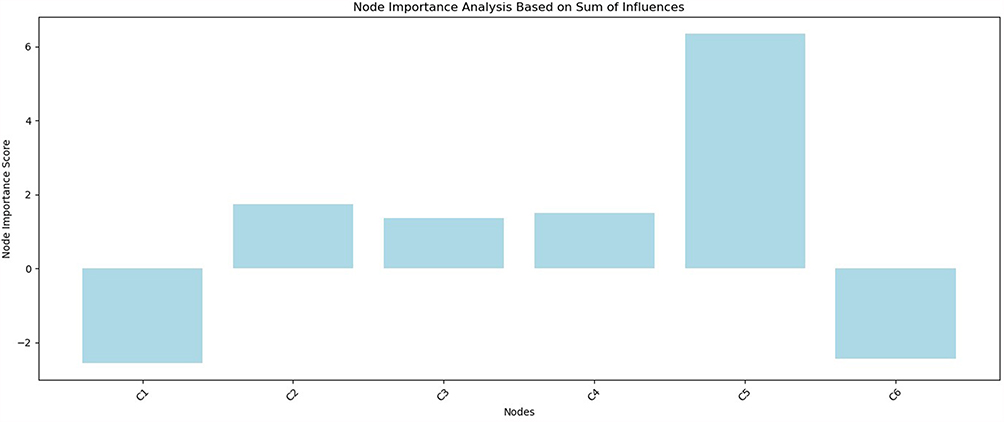 |
Figure 7 Node importance analysis based on total influences (sum of outgoing weights). This analysis identifies nodes exerting the greatest control within the network. Individual Differences (C5) exhibits the strongest positive influence, while Pain perception (C1) shows significant negative influence. These results highlight Individual Differences as a primary candidate for targeted interventions, given its prominent regulatory role within the model dynamics. |
Nodes representing the brain (C2), psychological factors (C3), social factors (C4), and individual differences (C5) emerge as critical hubs, consistently central across different measures (degree, betweenness, closeness, importance). In contrast, pain perception (C1) and tissue damage (C6), although slightly less connected, remain significant endpoints or regulators in the system.
The FCM’s community detection analysis (Figure 8) reveals two distinct groups within the network. The first community is represented solely by concept C1 (Pain perception), indicating its isolated influence and unique role within the system. This suggests that C1 (Pain perception) might have specific characteristics or connections that set it apart from the remaining nodes. The second community encompasses a tightly interconnected group of concepts C2 (Brain and neural basis of pain), C3 (Psychological factors), C4 (Social factors), C5 (Individual differences) and C6 (Tissue damage). This clustering highlights their collective dynamics and mutual influence, forming a cohesive sub-network. These nodes share strong relationships, which could indicate their collaborative roles in driving specific outcomes or maintaining the stability of the overall network. The separation of C1 (Pain perception) into its community underscores its distinctive role compared to the remaining nodes, which exhibit interdependencies within their community. This distinction might reflect structural or functional differences in how C1 (Pain perception) interacts with other elements, suggesting potential areas for further exploration in its impact on the system’s behavior.
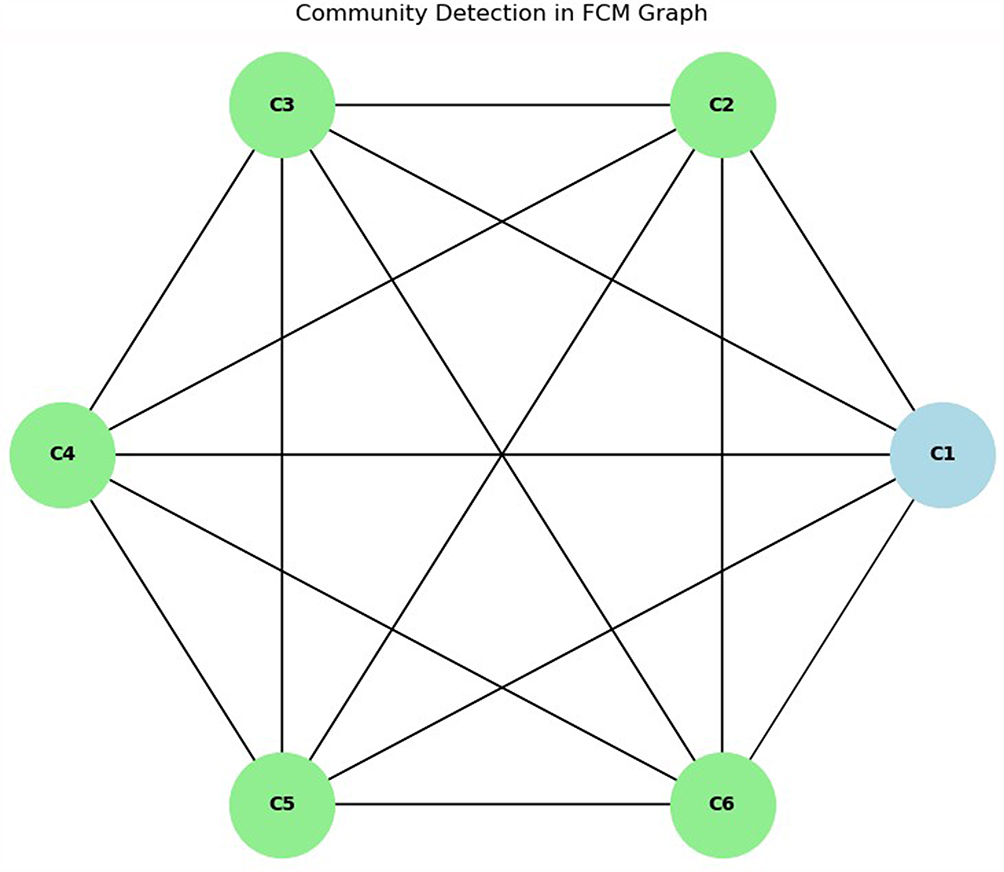 |
Figure 8 Community detection within the FCM graph using a modularity-based algorithm. Two distinct clusters emerge: one comprising solely the perceptual concept (C1, Pain perception), and the other cluster integrating neural (C2), psychosocial (C3–C5), and biological (C6) concepts. This division highlights the central integration of neural and psychosocial factors within pain dynamics, while distinctly positioning pain perception (C1) as a separate cluster, underscoring its unique role in the system. |
Figure 9 provides a concise summary of linguistic labels and weights. Here, individual differences (C5) consistently display strong positive effects, reinforcing their position as a primary modulator. This finding underscores the critical importance of personal traits, coping strategies, and genetic predispositions in shaping the experience of pain. Clinically, it suggests that interventions targeting individual characteristics, such as personalized psychological or behavioral therapies, may significantly influence broader pain outcomes and therapeutic effectiveness.
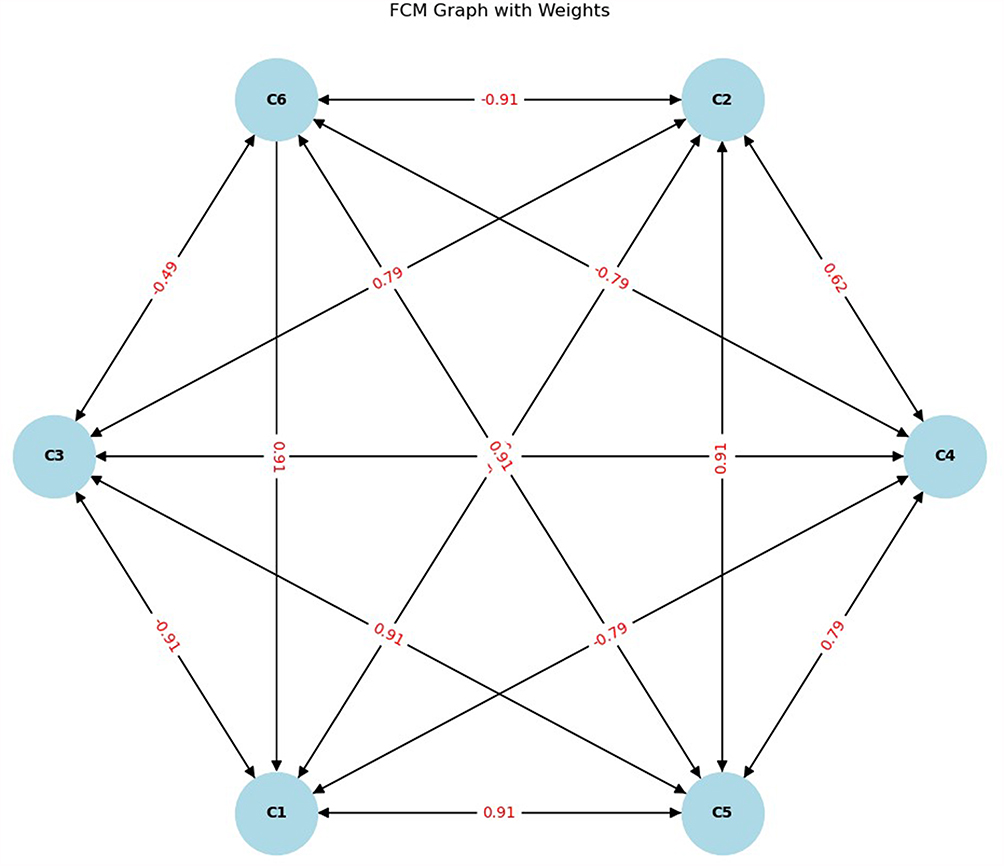 |
Figure 9 Updated FCM graph with all weights labelled. This visualisation shows the strength and polarity of each connection, enabling an intuitive overview of feedback loops and highlighting competing effects (eg, tissue damage both reinforcing and inhibiting certain constructs). |
Conversely, tissue damage (C6) again reveals mixed influences, further emphasizing its dual role as both a reinforcing and inhibiting node depending on the target context. This dual nature may reflect the complex interplay between actual physical injury and perceived pain severity, where tissue damage serves not only as an origin of nociceptive signals but also triggers central regulatory mechanisms. Practically, it highlights that clinical pain assessments and treatments should not solely focus on the extent of physical damage but also consider its broader modulatory effects across biological and psychological domains.
Concept C1 (Pain perception) demonstrates mixed interactions. It has strong negative influences on C2 (Brain and neural basis of pain), C3 (Psychological factors) and C4 (Social factors). This observation suggests that pain perception actively engages regulatory feedback mechanisms, potentially to limit emotional distress, cognitive overload, and social disruption associated with pain. The negative feedback loops identified here highlight the body’s inherent protective mechanisms aimed at maintaining psychological and social homeostasis despite ongoing pain.
Concept C2 (Brain and neural basis of pain) is predominantly positively influential, especially towards C3 (Psychological factors), C4 (Social factors) and C5 (Individual differences). Its negative impact on C6 (Tissue damage) is substantial. This central neural control likely underlies neuroplastic adaptations, allowing the brain to amplify or suppress the relevance of pain signals depending on context, thereby shaping both individual psychological responses and social behaviors. Such central modulation could form the basis for neuro-focused interventions, such as neuromodulation therapies or cognitive-behavioral techniques that harness neural plasticity for pain relief.
Concept C3 (Psychological factors) shows a balanced influence pattern. While it exerts strong positive effects on C4 (Social factors) and C5 (Individual differences), it negatively affects C1 (Pain perception) and C6 (Tissue damage). This complex balance underscores the dual role of psychological states in pain modulation, where positive psychological states can enhance social engagement and resilience, whereas negative states like anxiety or depression might amplify perceived pain intensity and prolong recovery. Therapeutically, this indicates psychological factors are pivotal targets for intervention, aiming to mitigate their adverse impacts while bolstering their protective elements through supportive social environments and targeted psychological therapies.
Concept C6 (Tissue damage) stands out for its dual nature. While positively influencing C1 (Pain perception) and C5 (Individual differences), it strongly negatively impacts C2 (Brain and neural basis of pain), C3 (Psychological factors) and C4 (Social factors). This complex interplay indicates that tissue injury not only directly escalates pain experiences but also potentially reduces cognitive, emotional, and social functioning by impairing central and psychological regulation. This suggests that interventions focused on physical healing should be complemented with strategies aimed at protecting cognitive-emotional resources and social support systems to comprehensively manage the overall pain experience.
When examining the system’s sensitivity analysis, the activation levels for top-ranked nodes (Figure 10) and key nodes (Figure 11) reveal subtle but significant variations in response to changes in their initial values. The two plots offer complementary perspectives on this analysis. For the top-ranked nodes C2 (Brain and neural basis of pain), C3 (Psychological factors) and C4 (Social factors) the analysis focuses on differences in activation levels relative to their baseline states across various initial values ranging from 0.1 to 0.9. This reveals how influential these nodes are in propagating changes throughout the system. The plot shows that while some nodes exhibit pronounced deviations from their baselines, others remain more stable, indicating differing roles in maintaining the system’s equilibrium. For instance, as the initial values increase, nodes like C3 (Psychological factors) display a more pronounced divergence, highlighting their dynamic influence under changing conditions. On the other hand, the sensitivity analysis for key drivers C1 (Pain perception), C2 (Brain and neural basis of pain), C5 (Individual differences) and C6 (Tissue damage) extends this examination by considering even more minor initial variations, such as 0.001 and 0.1, alongside higher values. This detailed approach illustrates that nodes such as C5 (Individual differences) are exceptionally responsive, with significant differences in their activation levels emerging under minimal perturbations. Nodes like C6 (Tissue damage) demonstrate a more muted response, suggesting a stabilizing role in the network. Including finer variations underscores the validity of specific nodes while revealing others’ susceptibility to external changes.
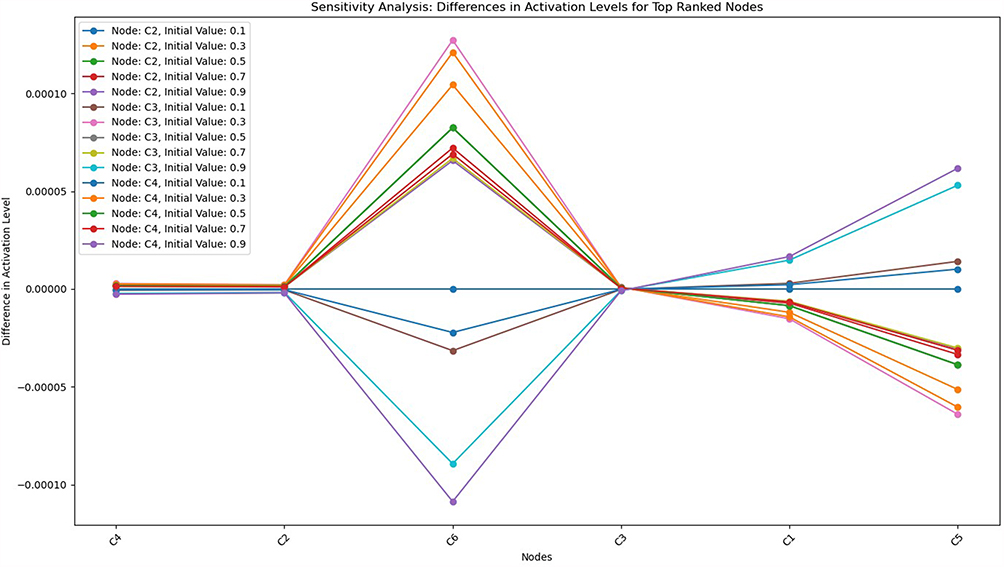 |
Figure 10 Sensitivity analysis illustrating differences in activation values for key nodes following incremental perturbations of top-ranked nodes (C2–C4). The results confirm that Individual Differences (C5) and Psychological Factors (C3) exhibit substantial sensitivity to these perturbations, validating their significant regulatory roles within the modeled pain dynamics. |
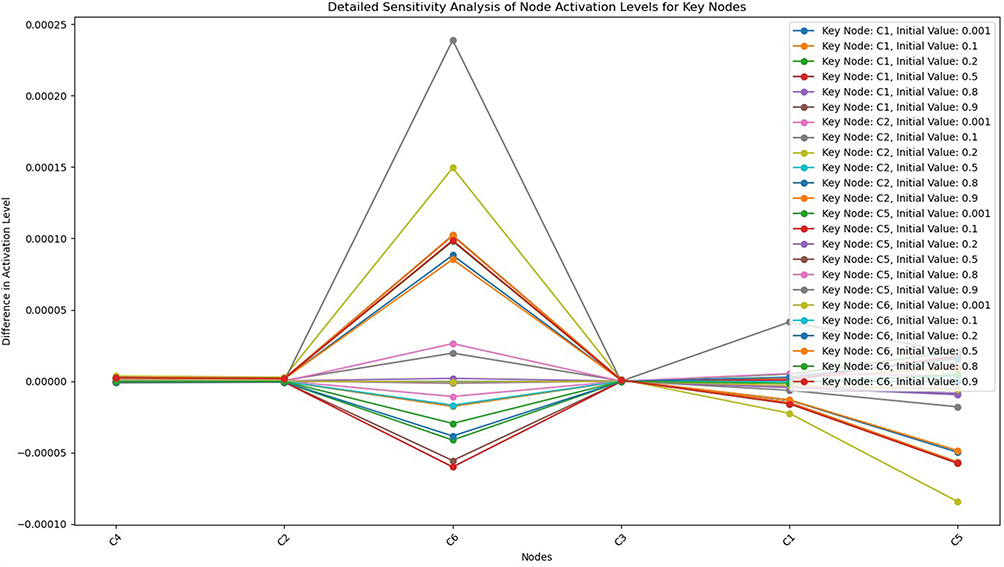 |
Figure 11 Detailed sensitivity analysis of activation patterns in response to small changes in input values for key nodes. The nonlinear propagation of influence is visible, indicating that even minor adjustments in these nodes can substantially reshape the system’s final equilibrium. |
Psychological factors (C3) and individual differences (C5) respond most dynamically to small initial changes, suggesting that these nodes critically mediate pain dynamics. By contrast, tissue damage (C6) remains relatively stable, again reinforcing its role as a stabilizing force within the network.
Figure 12 illustrates the progression of node activations over successive time steps in the simulated system. All nodes initially begin at an equal activation level of 0.5. Subsequent iterations depict dynamic changes as interactions between nodes unfold, governed by the weighted relationships within the network. Node C4 (Social factors) rapidly converges toward equilibrium, stabilizing at approximately 0.998 by the fourth iteration. Similarly, node C2 (Brain and neural basis of pain) consistently increases its activation, aligning closely with C4 (Social factors)’s trajectory. Both nodes exhibit a strong positive influence, as inferred from their steady climb in activation levels. In contrast, node C6 (Tissue damage) reveals a significant negative trend, initially fluctuating but stabilizing at an activation level near −0.775. This downward trajectory indicates that negatively weighted interactions highly influence C6 (Tissue damage) in the network. Node C1 (Pain perception) also declines but stabilizes around −0.974, reflecting a similar but slightly more intense negative influence. Nodes C3 (Psychological factors) and C5 (Individual differences) display more dynamic patterns. Node C3 (Psychological factors) rises quickly, achieving an activation level close to 0.999, indicating its dominance and strong positive relationships with other nodes. Node C5 (Individual differences) exhibits a nonlinear response, oscillating initially before converging to approximately 0.856, signaling moderate positive influence. The temporal evolution of activations underscores the network’s interconnected nature. Some nodes strongly drive the dynamics (eg, psychological factors and social factors), while others, like C6 (Tissue damage), act as suppressors due to their predominantly negative relationships. The stability achieved across all nodes by the eighth time step reflects the balance attained within the system. This balance highlights the system’s capacity to harmonize conflicting influences governed by the interplay of weights and activation functions.
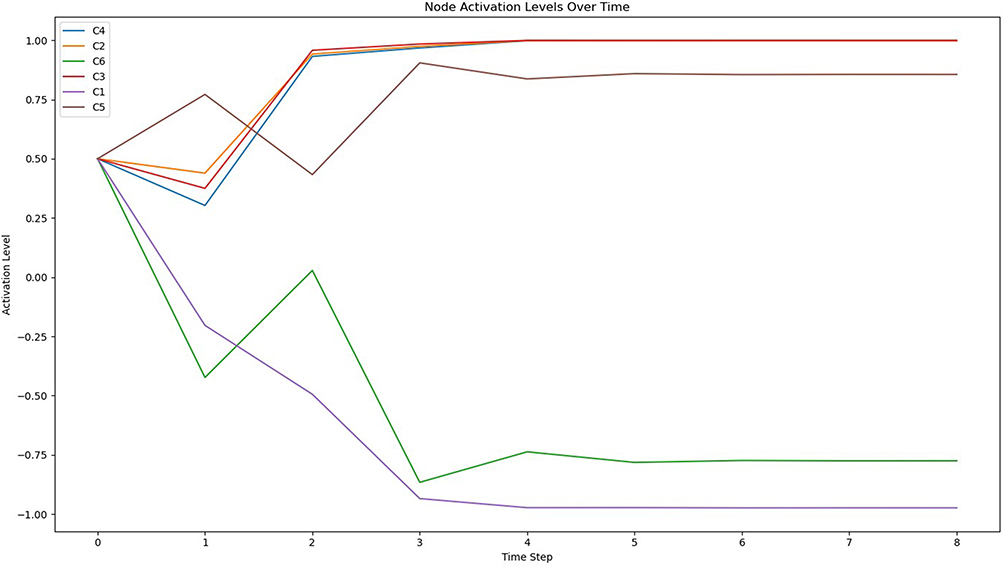 |
Figure 12 Complementary sensitivity analysis showing how target concepts respond to perturbations in controlling nodes. This reverse mapping underscores the directional dependencies and system bottlenecks, with Pain Perception emerging as highly responsive to upstream psychological changes. |
Figure 13 captures the average rate of change for all node activations across successive simulation steps, revealing how rapidly the system adjusts toward equilibrium. Initially, during the first two iterations, the rate of change is high, peaking during the second step. This sharp increase indicates significant adjustments as the nodes react to their initial interactions and weights. Beyond the third iteration, the rate of change begins to decline steadily. This trend signals a progressive stabilization in the activation levels as the influence dynamics between nodes approach balance. By the fourth iteration, the rate of change reduces sharply, and subsequent iterations exhibit minimal changes, indicating that the system is nearing equilibrium. The diminishing fluctuations in later iterations confirm that the network dynamics successfully converge, demonstrating the stability and resilience of the modelled FCM. This behaviour underscores the system’s ability to adapt and stabilize even with varying initial activations and weighted interactions.
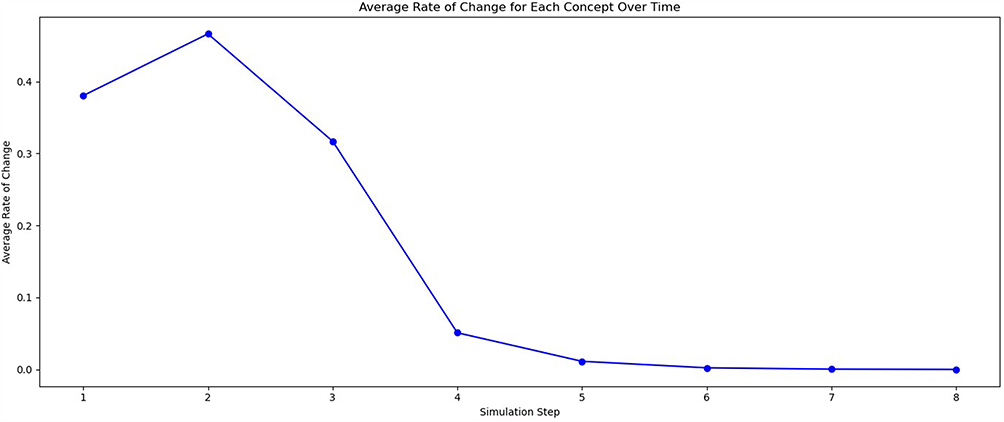 |
Figure 13 The average rate of change in activation across all concepts at each simulation step. The graph illustrates a rapid initial decline in activation rate, indicating quick stabilization of the model dynamics by step 5. The diminishing rate highlights the temporal stability and convergence behavior of the overall system rather than individual concept dynamics or oscillatory behavior. |
Social factors (C4) and psychological factors (C3) rapidly stabilize at high activation levels, reflecting their reinforcing interactions. Conversely, pain perception (C1) and tissue damage (C6) settle at negative levels, indicative of their inhibitory interactions and emphasizing a dynamic equilibrium between stimulatory and inhibitory influences.
The scenario analysis (Figure 14) explores the interplay between various factors influencing pain perception. These factors are represented by the concepts C1 (Pain perception), C2 (Brain and neural basis of pain), C3 (Psychological factors), C4 (Social factors), C5 (Individual differences) and C6 (Tissue damage). The activation dynamics under three distinct scenarios reveal more profound insights into how these factors interact within the model. In scenario 1, the activation levels of C3 (Psychological factors) and C1 (Pain perception) are initially initialized with relatively low values (0.1). This setup reflects a scenario in which psychological attention, emotions and cognitive factors play a minor role, alongside a reduced emphasis on the physical and mental aspects of pain. The downstream effects on other concepts, such as C2 (Brain and neural basis of pain) and C4 (Social factors), remain relatively subdued, highlighting the diminished centrality of C3 (Psychological factors) and C1 (Pain perception) in influencing the network dynamics under these conditions. Scenario 2 centres on a more robust activation of C2 (Brain and neural basis of pain) (0.5), while C1 (Pain perception) maintains its low activation (0.1). Here, the neurological and hormonal functions are moderately stimulated, potentially symbolising the centrality of brain-driven responses to pain. The increased activation of C2 (Brain and neural basis of pain) propagates through the network, exhibiting notable differences in concepts such as C4 (Social factors) and C5 (Individual differences), which are influenced by the neurological underpinnings of pain. This scenario underscores the brain’s vital role in moderating individual and social perceptions of pain. Scenario 3 amplifies the activation of C2 (Brain and neural basis of pain) to a high level (0.9), maintaining a low emphasis on C1 (Pain perception) (0.1). This scenario highlights the dominance of neurological and hormonal processes in shaping pain perception. The heightened activation of C2 (Brain and neural basis of pain) results in significant shifts across the network, particularly influencing C4 (Social factors) and C5 (Individual differences), as these concepts interact dynamically with the brain’s role. The propagation effects underscore how the brain’s role extends beyond direct neurological responses, influencing broader psychosocial and individual dimensions of pain. Comparing the differences in activation levels relative to a baseline reveals how variations in the initial activations of C1 (Pain perception), C2 (Brain and neural basis of pain) and C3 (Psychological factors) drive network-wide changes. The results demonstrate that while C1 (Pain perception) and C3 (Psychological factors) have more localized effects, the brain’s role C2 (Brain and neural basis of pain) is a significant mediator, highlighting its pivotal influence across multiple dimensions of pain perception. These insights can guide further explorations into targeted interventions and scenarios emphasizing specific aspects of pain modulation.
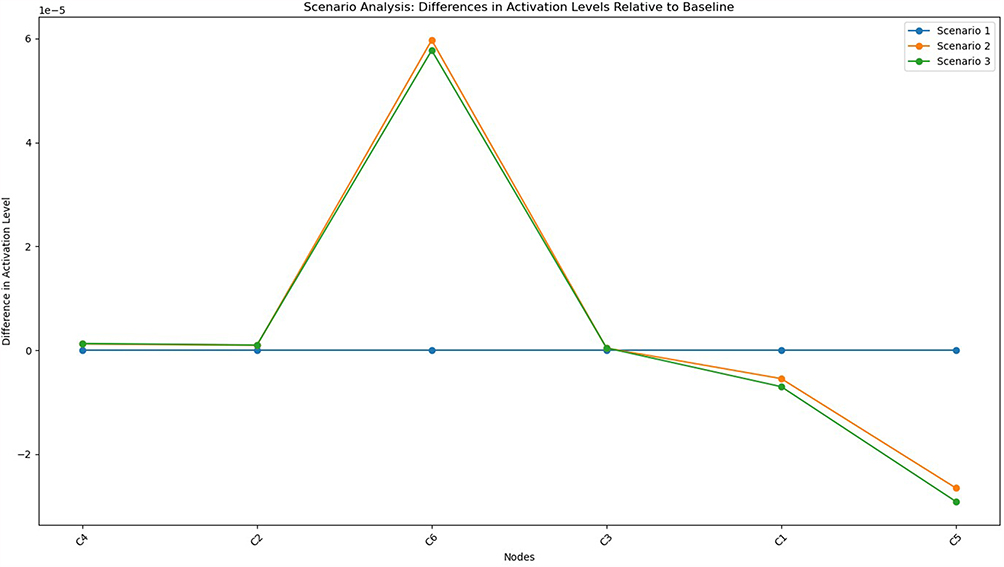 |
Figure 14 Scenario analysis showing differences in activation levels under alternative simulated conditions relative to baseline. The figure highlights the differential impact of modulating psychological versus biological factors, suggesting the dominance of top-down modulation pathways. |
Scenario analyses (Figure 14) reveal how varying the emphasis on psychological, neural, or direct pain inputs impacts the network. Increasing brain-related activation (C2) enhances social and individual factors, underscoring the brain’s central regulatory role. When psychological factors (C3) are less activated, the network shows muted dynamics, confirming the essential role of psychological states in pain perception.
The policy analysis (Figure 15) examines how different initializations of key concepts influence the convergence states of the system and the dynamics between factors related to pain perception, represented by the concepts C1 (Pain perception), C2 (Brain and neural basis of pain), C3 (Psychological factors), C4 (Social factors), C5 (Individual differences) and C6 (Tissue damage). Three distinct policies were evaluated to observe their impact on the final states of the model and the time required for the system to reach stability (error threshold e≤0.001). Under policy 1 (Psychological and Pain-Centric approach), high initial activations for C3 (Psychological factors) (0.9) and C1 (Pain perception) (0.9) emphasize pain’s psychological and direct sensory aspects. This approach resulted in a strong activation of C3 (Psychological factors), which propagated throughout the network, driving substantial influences on C4 (Social factors) and C5 (Individual differences). The system converged in the 9th state, stabilizing slightly slower than the other policies. Final activation levels balance social, individual and brain-centric influences. The negative activation of C6 (Tissue damage) (−0.775242) highlights the diminished role of direct physical damage in this scenario. Policy 2 (Neurological-driven strategy) prioritizes the brain’s role C2 (Brain and neural basis of pain) with an initial activation of 0.8 and a moderate emphasis on C1 (Pain perception) (0.6). The heightened activation of C2 (Brain and neural basis of pain) reinforces the central role of neurological processes in moderating pain perception, leading to significant downstream impacts on C5 (Individual differences) and C4 (Social factors). This configuration converged more rapidly in the 8th state, reflecting the stability introduced by the brain’s centrality in the model. The final states emphasize the importance of neurological modulation, with a slightly higher positive influence on C5 (Individual differences) than policy 1, while C6 (Tissue damage) remains similarly negative (−0.775281). Policy 3 (Balanced psychological and sensory approach) adopts a moderate emphasis on C3 (Psychological factors) (0.7) and a reduced activation of C1 (Pain perception) (0.4). This configuration balances psychological and direct sensory inputs, reflecting scenarios where both factors play significant but not dominant roles. The model converged in the 8th state, similar to policy 2, but with slightly different activation levels. C5 (Individual differences) exhibited the highest final state among all policies (0.855864), indicating a stronger emphasis on individual variability. The reduced negative activation of C1 (Pain perception) (−0.973934) reflects the interplay between psychological and sensory influences in pain modulation. The results indicate that C2 (Brain and neural basis of pain) pain stabilize all policies, contributing to rapid convergence and consistent propagation of influence throughout the network. Policies prioritizing C3 (Psychological factors) result in slower stabilization but higher impacts on social and individual factors, as seen in policy 1. Strategies focusing on C2 (Brain and neural basis of pain) (policy 2) achieve faster convergence and maintain a balanced influence across all concepts. The effects of policy 3 highlight the importance of psychological and sensory integration in driving individual variability.
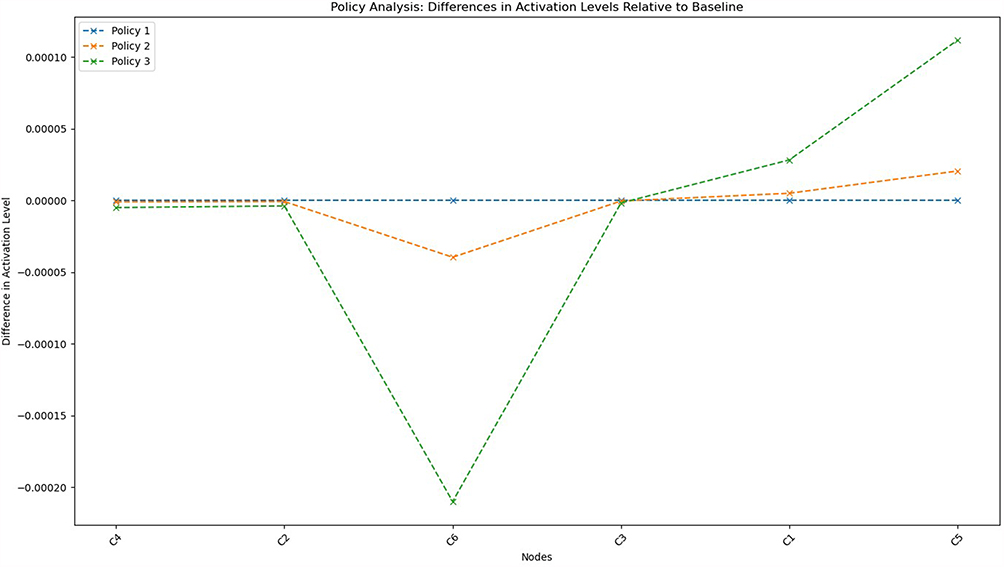 |
Figure 15 A policy simulation analysis comparing differences in activation levels relative to a baseline scenario. The three policies reflect distinct strategies: Policy 1 demonstrates minimal differences across nodes, Policy 2 shows moderate deviations primarily affecting social and individual factors, and Policy 3 exhibits pronounced negative effects on psychological factors (C3) and significant positive effects on individual differences (C5). These results confirm Individual Differences (C5) as a critical leverage point for clinical intervention design due to its substantial responsiveness across interventions. The significant negative deviation observed for Psychological Factors (C3) under Policy 3 highlights its sensitivity to interventions, suggesting that psychological modulation can heavily influence system-wide dynamics. |
Policy analyses (Figure 15) highlight distinct clinical implications. A psychologically driven approach (high C3 activation) stabilizes more slowly but effectively amplifies positive social and individual outcomes. Conversely, neurologically driven policies (high C2 activation) stabilize faster, underscoring neurological factors’ stabilizing effect. A balanced psychological-neurological approach optimally activates individual differences (C5), suggesting it as an effective clinical strategy emphasizing patient-specific factors.
Discussion
Policy and scenario analyses have yielded invaluable insights into the dynamic relationships among pain perception, the brain, the neural basis of pain, psychological factors, social influences, individual differences, and types of tissue damage, as modelled by FCM. The simulated interventions highlighted key leverage points in the conceptual network, offering potential targets for clinical strategies to alleviate chronic pain conditions. Each node within FCM, C1 (Pain perception) to C6 (Tissue damage), represents distinct aspects of the multifaceted nature of pain perception, shaped by the interplay of biological, psychological, social and individual factors. Analysing these nodes under various scenarios highlighted how specific interventions can create cascading effects throughout the network.37,42,43 In contrast to the elderly, pain measurement for younger individuals appears divergent. Research indicates that females exhibit higher pain perception compared to males. From another perspective, culture also significantly impacts pain perception; some define pain as stemming from the mind, while others advocate for an opposing view. Certain individuals possess heightened pain sensitivity and, therefore, experience more pain due to their focus on it. Fatigue, anxiety and pain are interrelated. Pain perception notably increases with fatigue and anxiety.16 Ultimately, pain perception depends fundamentally on the brain and its corresponding neurophysiological processes. For instance, node C2 (the brain and the neural basis of pain) demonstrated high positivity in both psychological and social domains, emphasising the brain’s integrative role as a mediator of pain-related external and internal stimuli.10,12 Baruch’s statements regarding neuroplasticity recognise the brain’s inherent ability to dynamically adjust to incoming pain stimuli and their associated cognitive and emotional modifications.1,2 Psychological factors (C3) have also emerged as a significant influence, with both “protective” and “vulnerability” pathways affecting pain outcomes. Protective elements such as optimism and self-efficacy diminish pain perception, whereas maladaptive factors like catastrophising and pain-related fear amplify it.13,14 These findings justify psychological interventions aimed at enhancing resilience to reduce pain-related distress and disability outcomes. Besides the crucial pathway through which social support systems affect pain perception (C4, Social factors), positive social interactions have been shown to cultivate positive perceptions of pain. Conversely, other social factors impacting the pain experience may include financial hardships, ineffective family functioning and involvement in litigation. For example, the rates of chronic pain tend to be higher, more challenging and create a greater impact in individuals residing in areas of socioeconomic deprivation. Understanding the role of the social environment in human pain perception and its interaction with biological and psychological determinants has significantly advanced the study of pain and furthered efforts to prevent and manage it.35 Concept C5 (individual differences) has played a pivotal role in shaping pain perception, particularly concerning policy 3 (Balanced Psychological and Sensory Approach). This indicates that individual traits related to coping mechanisms and personality have the most substantial impact on pain perception. It suggests a balanced approach that integrates psychological and sensory factors to best represent personal differences in pain experiences. Conversely, C6 (tissue damage) consistently showed negative outcomes across all policies, indicating that the tissue damage itself plays a lesser role in pain perception. This suggests that central modulation mechanisms, rather than peripheral injury, are more influential in shaping pain, highlighting the importance of psychological, neurological and social factors in pain management.
Although our model effectively integrates multidisciplinary perspectives, its methodological limitations deserve attention. The reliance on expert judgment through snowball sampling introduces potential biases stemming from shared professional or theoretical viewpoints.44 Despite our mitigation strategies, initial diversity among experts and independent assessments, this limitation remains significant, potentially influencing relationship weightings and model structure. Thus, the generalizability and reproducibility of our findings necessitate validation through empirical methods, including real-world clinical data or patient-reported outcomes.
While FCMs offer advantages in interpretability and integration of expert knowledge, it is essential to contextualize this approach within the broader landscape of computational medical modeling. Unlike machine learning algorithms such as neural networks, which excel in predictive accuracy but suffer from opacity,5 or Bayesian models known for probabilistic rigor but demanding substantial prior knowledge,8 FCMs uniquely balance transparency, interpretability, and human-like reasoning. Nonetheless, hybrid modeling that combines FCM interpretability with data-driven accuracy (eg, neural network-generated weights) could enhance predictive validity, overcoming inherent expert-judgment limitations.9
Clinically, the translation of our FCM-based model can be significantly advanced by integrating it into decision-support systems within electronic health records (EHRs), providing real-time personalized feedback to clinicians. For example, scenario-based simulations could inform clinicians on potential psychological or social interventions tailored to individual patient profiles, optimizing multidisciplinary treatment approaches. Embedding this model in clinician training programs could enhance diagnostic accuracy and therapeutic decision-making by helping clinicians visualize complex biopsychosocial interactions dynamically.37 Compared to other computational models such as neural networks, Bayesian decision models, or rule-based systems, FCMs have a distinctive balance of transparency, flexibility, and human-like reasoning. However, the integration of FCMs with machine learning approaches can further increase model generalizability and validity. As emphasised in the biopsychosocial model of pain, all variables mentioned in this study are validated, confirming that the biopsychosocial model asserts pain to be a personally experienced phenomenon arising from the dynamic interplay among complex sensory-discriminative, cognitive-evaluative, motivational-affective, behavioural and social dimensions, none of which are mutually exclusive. In light of this data, the EFIC recommends the comprehensive implementation of the biopsychosocial model of pain in clinical care, research, education, including EFIC medicine, physiotherapy, nursing and psychology core curricula and policy.35,45 This model can be best embedded in clinical decision support systems (CDSS) for providing real-time feedback regarding the risk of pain perception for patient profiles that will aid in personalised treatment planning.
Conclusion
Pain, as a multidimensional phenomenon and an across-the-board problem in clinical practice, significantly influences individuals’ physiological, psychological, and social functioning. Knowledge of pain perception, information about pain and coping mechanisms is also relevant for the establishment of effective new therapies.16,18 This study proposed an integrative FCM-based model of pain perception, systematically analysing interrelated neural, psychological, social, and individual determinants of pain. Utilising FCMs, this research contributes a transparent framework that aligns well with contemporary personalised medicine initiatives as well as clinical practices. The idea of this study can be implemented in the proper diagnosis and treatment of other pain disorders. The proposed approach, which is founded on the use of the knowledge and experience of experts in a sophisticated automated medical system, can be used both for the diagnosis of other types of pain disorders and for the recommendation of the appropriate treatments.
Concerning model convergence as a critical aspect of FCM usability, we applied spectral analysis.43 Our computed spectral radius exceeds the threshold of unity, confirming the existence of multiple stable attractors rather than a unique global attractor. This outcome preserves the practical applicability of our model, demonstrating its dynamic versatility and capability to simulate various pain-management scenarios effectively.
Notwithstanding the value of the contributions of this study, there are some limitations. The current study was conducted within the Iranian cultural context, and thus, its generalizability to other cultural settings is limited. Whereas pain perception and its interlinked variables may be highly different across societies, future studies should replicate the present analysis in diverse cultural contexts to examine the validity and extension of these findings. Cross-cultural comparisons may tease apart universal patterns and culture-specific differences in the dynamics of the pain experience and perception among individuals.
Even though the FCM model proved effective for analysing causal relationships, the weight assignments, being based on expert judgment and snowball sampling, may introduce subjective bias. Thus, integrating more recent methodological advancements, such as hybrid neural-fuzzy cognitive approaches9 and interpretability-enhancing techniques,46 could reduce subjectivity and enhance the robustness of the results. Although validated primarily through expert consensus and scenario simulations, empirical validation using standardised clinical instruments remains essential. In future work, validated psychological instruments (eg, Beck Depression Inventory,47 GAD-748) will be administered to representative samples, comparing FCM outcomes against empirical data to ensure accurate reflection of real psychological dynamics.
Clinically, the practical implementation of this model can be significantly enhanced by integrating it within decision-support systems, electronic health records, and clinician training frameworks. Embedding such models could offer clinicians dynamic insights into complex biopsychosocial interactions, thereby improving diagnostic precision and personalised treatment strategies. These applications underscore the relevance of FCM approaches within medical decision-making contexts, positioning them distinctively against other computational tools, such as Bayesian models or traditional machine learning methods.
To determine the system’s reliability for diagnosing particular pain conditions, more simulation results and several case studies are needed. Real model application requires the teamwork of more specialists and experts, along with input from those who suffer from chronic pain. Future research should expand this model to diverse cultural and clinical contexts, applying longitudinal designs to assess its sensitivity to change over time. Complementing FCMs with real-time physiological or neuroimaging data will further validate their predictive and explanatory power, ultimately enhancing their contribution to personalised pain medicine.
Abbreviations
FCM, Fuzzy Cognitive Map; CSV, Comma-Separated Values; MDSS, Medical Decision Support Systems; QTL, Quantitative Trait Locus; VH, Very High; H, High; M, Medium; L, Low; VL, Very Low; C1 (Pain perception), Concept 1; C2 (Brain and neural basis of pain), Concept 2; C3 (Psychological factors), Concept 3; C4 (Social factors), Concept 4; C5, Concept 5; C6, Concept 6; EFIC, European Pain Federation.
Ethical Approval and Consent to Participate
This is an observational study. The University of Tehran Research Ethics Committee have confirmed that no ethical approval is required for observational studies. All participants (experts in this work) gave written informed consent prior to participation.
All procedures in this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Acknowledgments
The authors appreciate all experts contributing to this research.
Disclosure
The authors report that there are no conflicts of interest in this work and there is not any financial support in research.
References
1. Apkarian VA, Hashmi JA, Baliki MN. Pain and the brain: specificity and plasticity of the brain in clinical chronic pain. Pain. 2011;152(3 Suppl):S49–S64. doi:10.1016/j.pain.2010.11.010
2. Hiraga SI, Itokazu T, Nishibe M, Yamashita T. Neuroplasticity related to chronic pain and its modulation by microglia. Inflamm Regen. 2022;42(1):15. doi:10.1186/s41232-022-00199-6
3. Maciejewska-Skrendo A, Pawlak M, Leońska-Duniec A, et al. Can injuries have a lasting effect on the perception of pain in young, healthy women and men? Sports Health. 2021;13(3):278–284. doi:10.1177/1941738120953165
4. Okolo CA, Olorunsogo TO, Babawarun O. Cultural variability in pain perception: a review of cross-cultural studies. Int J Sci Res Arch. 2024;11(1):2550–2556. doi:10.30574/ijsra.2024.11.1.0339
5. Chen ZS, Wang J. Pain, from perception to action: a computational perspective. iScience. 2023;26(1):106907. doi:10.1016/j.isci.2023.106907
6. Schuerkamp R, Giabbanelli PJ. Extensions of fuzzy cognitive maps: a systematic review. ACM Comput Surv. 2023;56(2):1–36. doi:10.1145/3610771
7. Párraga JP, Castellanos A. A manifesto in defense of pain complexity: a critical review of essential insights in pain neuroscience. J Clin Med. 2023;12(22):7080. doi:10.3390/jcm12227080
8. Hagger MS. Psychological determinants of health behavior. Annual Rev Psychol. 2025;76(1):821–850. doi:10.1146/annurev-psych-020124-114222
9. Amirkhani A, Nasiriyan-Rad H, Papageorgiou EI. A novel fuzzy inference approach: neuro-fuzzy cognitive map. Int J Fuzzy Syst. 2020;22(3):859–872.
10. Anninou AP, Groumpos PP, Panagiotis P. Modeling health diseases using competitive fuzzy cognitive maps. In: Papadopoulos H, Andreou AS, Iliadis L, Maglogiannis I, editors. Artificial Intelligence Applications and Innovations. Vol. 412. Springer; 2013.
11. Treede RD. Peripheral acute pain mechanisms. Ann Med. 1995;27(2):213–216. doi:10.3109/07853899509031961
12. Karcz M, Gharibo C. Peripheral nervous system pain modulation. Curr Neuropharmacol. 2024;22(1):65–71. doi:10.2174/1570159X21666230803100400
13. Khera T, Rangasamy V. Cognition and pain: a review. Front Psychol. 2021;12:673962. doi:10.3389/fpsyg.2021.673962
14. Edwards RR, Dworkin RH, Sullivan MD, Turk DC, Wasan AD. The role of psychosocial processes in the development and maintenance of chronic pain. J Pain. 2016;17(9 Suppl):T70–T92. doi:10.1016/j.jpain.2016.01.001
15. Martinez-Calderon J, Flores-Cortes M, Morales-Asencio JM, Luque-Suarez A. Which psychological factors are involved in the onset and/or persistence of musculoskeletal pain? An umbrella review of systematic reviews and meta-analyses of prospective cohort studies. Clin J Pain. 2020;36(8):626–637. doi:10.1097/AJP.0000000000000838
16. Romualdo JM, Borges E, Tavares I, Pozza DH. The interplay of fear of pain, emotional states, and pain perception in medical and nursing students: a cross-sectional study. PLoS One. 2024;19(11):e0314094. doi:10.1371/journal.pone.0314094
17. Afridi B, Khan H, Akkol EK, Aschner M. Pain perception and management: where do we stand? Curr Mol Pharmacol. 2021;14(5):678–688. doi:10.2174/1874467213666200611142438
18. Callister LC. Cultural influences on pain perceptions and behaviors. Home Health Care Manag Pract. 2003;15(3):207–211.
19. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
20. Peacock S, Patel S. Cultural influences on pain. Rev Pain. 2008;1(2):6–9. doi:10.1177/204946370800100203
21. Tanaka Y, Nishi Y, Nishi Y, Osumi M, Morioka S. Uncovering the influence of social skills and psychosociological factors on pain sensitivity using structural equation modeling. J Pain Res. 2017;10:2223–2231. doi:10.2147/JPR.S143342
22. Penn TM, Trost Z, Parker R, et al. Social support buffers the negative influence of perceived injustice on pain interference in people living with HIV and chronic pain. Pain Rep. 2019;4(2):e710. doi:10.1097/PR9.0000000000000710
23. Fillingim RB, Wallace MR, Herbstman DM, Ribeiro-Dasilva M, Staud R. Genetic contributions to pain: a review of findings in humans. Oral Dis. 2008;14(8):673–682. doi:10.1111/j.1601-0825.2008.01458.x
24. Fillingim RB. Individual differences in pain: understanding the mosaic that makes pain personal. Pain. 2017;158(Suppl 1):S11–S18. doi:10.1097/j.pain.0000000000000775
25. James S. Human pain and genetics: some basics. Br J Pain. 2013;7(4):171–178. doi:10.1177/2049463713506408
26. Norbury TA, MacGregor AJ, Urwin J, Spector TD, McMahon SB. Heritability of responses to painful stimuli in women: a classical twin study. Brain. 2007;130(Pt 11):3041–3049. doi:10.1093/brain/awm233
27. Fincke A, Wright C, Jones KD, Carson JW, Shih J. Genetic influences on pain perception and treatment. Practical Pain Management. 2010;10(1):1.
28. Stratton H, Lee G, Dolatyari M, et al. Nociceptors are functionally male or female: from mouse to monkey to man. Brain. 2024;147(12):4280–4291. doi:10.1093/brain/awae179
29. Zhi Y, Zhang Y, Zhang Y, Zhang M, Kong Y. Age-associated changes in multimodal pain perception. Age Ageing. 2024;53(5):afae107. doi:10.1093/ageing/afae107
30. Lautenbacher S, Peters JH, Heesen M, Scheel J, Kunz M. Age changes in pain perception: a systematic review and meta-analysis of age effects on pain and tolerance thresholds. Neurosci Biobehav Rev. 2017;75:104–113. doi:10.1016/j.neubiorev.2017.01.039
31. Grouper H, Eisenberg E, Pud D. More insight on the role of personality traits and sensitivity to experimental pain. J Pain Res. 2021;14:1837–1844. doi:10.2147/JPR.S309729
32. Sambo CF, Howard M, Kopelman M, Williams S, Fotopoulou A. Knowing you care: effects of perceived empathy and attachment style on pain perception. Pain. 2010;151(3):687–693. doi:10.1016/j.pain.2010.08.035
33. Amaya F, Izumi Y, Matsuda M, Sasaki M. Tissue injury and related mediators of pain exacerbation. Curr Neuropharmacol. 2013;11(6):592–597. doi:10.2174/1570159X11311060003
34. Saling J. Pain types and classifications. WebMD. 2023.
35. Kosko B. Fuzzy cognitive maps. Int J Man-Machine Stud. 1986;24(1):65–75.
36. Karatzinis GD, Boutalis YS. A Review Study of Fuzzy Cognitive Maps in Engineering: applications, Insights, and Future Directions. Eng. 2025;6(2):37.
37. Apostolopoulos ID, Papandrianos NI, Papathanasiou ND, Papageorgiou EI. Fuzzy cognitive map applications in medicine over the last two decades: a review study. Bioengineering. 2024;11(2):139. doi:10.3390/bioengineering11020139
38. Paraskevas A, Madas M. Neutrosophic cognitive maps: theoretical and mathematical formulations, literature review, and applications. Soft Computing and Machine Learning. 2025;2025:27–58.
39. Saúl LA, Sanfeliciano A, Botella L, Perea R, Gonzalez-Puerto JA. Fuzzy cognitive maps as a tool for identifying cognitive conflicts that hinder the adoption of healthy habits. Int J Environ Res Public Health. 2022;19(3):1411. doi:10.3390/ijerph19031411
40. Mkhitaryan S, Giabbanelli P, Wozniak MK, Nápoles G, De Vries N, Crutzen R. FCMpy: a python module for constructing and analyzing fuzzy cognitive maps. PeerJ Comput Sci. 2022;8:e1078. doi:10.7717/peerj-cs.1078
41. Harmati IÁ, Hatwágner MF, Kóczy LT. Global stability of fuzzy cognitive maps. Neural Comput Appl. 2023;35(10):7283–7295. doi:10.1007/s00521-021-06742-9
42. Eroğlu Demir S. Classification of pain and pain types. Dr Saliha Eroglu Demir. 2022;2022:1.
43. Gregorio SIF, Montané-Jiménez LG, Morales-Rosales LA. A Fuzzy Cognitive Map to Evaluate a Medical Context. In
44. Marcus B, Weigelt O, Hergert J, Gurt J, Gelléri P. The use of snowball sampling for multi source organizational research: some cause for concern. Personnel Psychol. 2017;70(3):635–673. doi:10.1111/peps.12169
45. Smart KM. The biopsychosocial model of pain in physiotherapy: past, present and future. Phys Ther Rev. 2023;28(2):61–70. doi:10.1080/10833196.2023.2177792
46. Zhang K, Shao T, Sun Y, et al. Interpretable Research of Fuzzy Methods: A Literature Survey. Available at SSRN 5251497. 2025.
47. Hubley AM. Beck Depression Inventory. In Encyclopedia of Quality of Life and Well-Being Research (Pp. 393-403). Cham: Springer; 2023.
48. Mullins PM, Yong RJ, Bhattacharyya N. Associations between chronic pain, anxiety, and depression among adults in the United States. Pain Pract. 2023;23(6):589–594. doi:10.1111/papr.13220
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.