Back to Journals » International Journal of General Medicine » Volume 19
Model-Dependent Cardiovascular Risk Stratification in Obese Populations: Multicenter Study in Türkiye
Authors Düzen Oflas N ![]() , Oral A
, Oral A ![]() , Solmaz I, Topaloglu US
, Solmaz I, Topaloglu US ![]() , Demir I, Dundar A, Kirik A, Kama Başcı O, Sen H, Binnetoglu E
, Demir I, Dundar A, Kirik A, Kama Başcı O, Sen H, Binnetoglu E ![]() , Okuroglu N, Aydin A
, Okuroglu N, Aydin A ![]() , Kaya ZI, Yıldız H, Acet A
, Kaya ZI, Yıldız H, Acet A ![]() , Tazegül G, Sozel H, Ozudogru O, Issever K, Yaylacı S, Korkmaz UB
, Tazegül G, Sozel H, Ozudogru O, Issever K, Yaylacı S, Korkmaz UB ![]() , Küçük C, Konur K
, Küçük C, Konur K ![]() , Ayaz T, Isiklar A, Arac E
, Ayaz T, Isiklar A, Arac E ![]() , Sumbul HE
, Sumbul HE ![]() , Öztürk HA, Govez AB, Durmus YÜ, Onmez A, Ocak Serin S, Koca N, Yalcın N, Ertinmaz A, Güven AT
, Öztürk HA, Govez AB, Durmus YÜ, Onmez A, Ocak Serin S, Koca N, Yalcın N, Ertinmaz A, Güven AT ![]() , Kok M
, Kok M ![]() , Alp HH, Sahinturk Y, Uyar S
, Alp HH, Sahinturk Y, Uyar S
Received 22 February 2026
Accepted for publication 14 May 2026
Published 18 June 2026 Volume 2026:19 602816
DOI https://doi.org/10.2147/IJGM.S602816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Nur Düzen Oflas,1 Alihan Oral,2 Ihsan Solmaz,3 Ulas Serkan Topaloglu,4 Ismail Demir,5 Ahmet Dundar,6 Ali Kirik,7 Ozge Kama Başcı,7 Hacer Sen,7 Emine Binnetoglu,8 Nalan Okuroglu,9 Ahmet Aydin,10 Zeynep Irmak Kaya,11 Hamit Yıldız,12 Aycan Acet,13 Gökhan Tazegül,14 Hasan Sozel,15 Osman Ozudogru,16 Kubilay Issever,17 Selcuk Yaylacı,18 Ugur Bayram Korkmaz,19 Celalettin Küçük,20 Kamil Konur,21 Teslime Ayaz,22 Aysun Isiklar,23 Esref Arac,24 Hilmi Erdem Sumbul,25 Hüseyin Ali Öztürk,25 Ali Burak Govez,25 Yusuf Üsame Durmus,25 Attila Onmez,26 Sibel Ocak Serin,27 Nizameddin Koca,28 Nazif Yalcın,28 Aysegul Ertinmaz,28 Alper Tuna Güven,29 Mehmet Kok,30 Hamit Hakan Alp,31 Yasin Sahinturk,30 Seyit Uyar30
1Department of Internal Medicine, Faculty of Medicine, Van Yuzuncu Yil University, Van, Türkiye; 2Department of Internal Medicine, Faculty of Medicine, Biruni University, İstanbul, Türkiye; 3Department of Internal Medicine, Diyarbakir Gazi Yasargil Education Research Hospital, Diyarbakir, Türkiye; 4Department of Internal Medicine, Kayseri City Hospital, Kayseri, Türkiye; 5Department of Internal Medicine, Bozyaka Education Research Hospital, Izmir, Türkiye; 6Department of Internal Medicine, Mardin Savur Prof. Dr. Aziz Sancar State Hospital, Mardin, Türkiye; 7Department of Internal Medicine, Faculty of Medicine, Balikesir University, Balikesir, Türkiye; 8Department of Internal Medicine, Corlu Vatan Hospital, Tekirdag, Türkiye; 9Department of Internal Medicine, Fatih Sultan Mehmet Education Research Hospital, Istanbul, Türkiye; 10Department of Internal Medicine, Faculty of Medicine, Medipol University, Istanbul, Türkiye; 11Department of Internal Medicine, Health Sciences University Eskisehir Health Application and Research Center, Eskisehir City Hospital, Eskisehir, Türkiye; 12Department of Internal Medicine, Faculty of Medicine, Gaziantep University, Gaziantep, Türkiye; 13Department of Internal Medicine, Faculty of Medicine, Kutahya Health Sciences University, Kutahya, Türkiye; 14Department of Internal Medicine, Faculty of Medicine, Marmara University, Istanbul, Türkiye; 15Department of Internal Medicine, Faculty of Medicine, Akdeniz University, Antalya, Türkiye; 16Department of Internal Medicine, Faculty of Medicine, Erzincan Binali Yildirim University, Erzincan, Türkiye; 17Department of Internal Medicine, Giresun University Education Research Hospital, Giresun, Türkiye; 18Department of Internal Medicine, Faculty of Medicine, Sakarya University, Sakarya, Türkiye; 19Department of Internal Medicine, Izmir Katip Celebi Education Research Hospital, Izmir, Türkiye; 20Department of Internal Medicine, Memorial Bahçelievler Hospital, Istanbul, Türkiye; 21Department of Internal Medicine, Faculty of Medicine, Recep Tayyip Erdogan University, Rize, Türkiye; 22Department of Internal Medicine, Bakircay University Cigli Education Research Hospital, Izmir, Türkiye; 23Department of Internal Medicine, Acibadem Atasehir Hospital, Istanbul, Türkiye; 24Department of Internal Medicine, Faculty of Medicine, Dicle University, Diyarbakir, Türkiye; 25Department of Internal Medicine, Health Sciences University Adana Health Application and Research Center, Adana City Hospital, Adana, Türkiye; 26Department of Internal Medicine, Faculty of Medicine, Duzce University, Duzce, Türkiye; 27Department of Internal Medicine, Umraniye Education Research Hospital, Istanbul, Türkiye; 28Department of Internal Medicine, Health Sciences University Bursa Health Application and Research Center, Bursa City Hospital, Bursa, Türkiye; 29Department of Internal Medicine, Faculty of Medicine, Baskent University, Ankara, Türkiye; 30Department of Internal Medicine, Antalya Education Research Hospital, Antalya, Türkiye; 31Department of Basic Medical Sciences, Division of Biochemistry, Faculty of Medicine, Van Yuzuncu Yil University, Van, Türkiye
Correspondence: Osman Ozudogru, Department of Internal Medicine, Faculty of Medicine, Erzincan Binali Yildirim University, Erzincan, Türkiye, Tel +90 505 704 2034, Email [email protected]
Background: Cardiovascular risk prediction models are essential for preventive cardiology; however, most were developed in populations with limited representation of individuals with severe obesity. Given the high prevalence of obesity in Türkiye and its strong association with cardiometabolic disorders, uncertainty exists regarding the applicability and agreement of contemporary cardiovascular risk estimation tools in this population. This study aimed to compare cardiovascular risk estimates derived from SCORE2, SCORE2-DM, and AHA PREVENT models across geographical regions in a large obese cohort from Türkiye, and to formally evaluate inter-model agreement and confounder-adjusted regional differences.
Methods: This multicenter retrospective analysis included 6,378 obese individuals recruited from seven geographical regions of Türkiye. Demographic characteristics, comorbidities, anthropometric measurements, and laboratory data were obtained from standardized electronic medical records. Ten-year cardiovascular risk was estimated, rather than prospectively predicted, using SCORE2, SCORE2-DM, and AHA PREVENT equations. Regional comparisons were performed using the Kruskal–Wallis test and chi-square analysis. Inter-model agreement was assessed using Spearman correlation, intraclass correlation coefficients (ICC), Bland–Altman analysis, and linear-weighted Cohen’s kappa for guideline-based risk strata. Multivariable linear regression was used to evaluate regional differences after adjustment for age, sex, smoking, diabetes, hypertension, dyslipidemia, statin use, and body mass index. Statistical significance was set at p< 0.05.
Results: Substantial regional heterogeneity was observed in smoking prevalence, cardiometabolic comorbidities, and medication use. Cardiovascular risk estimates differed according to the selected prediction model: SCORE2 identified the highest median risk in Mediterranean and Southeastern Anatolia, SCORE2-DM demonstrated relatively homogeneous risk estimates across regions, and PREVENT showed greater regional discrimination, identifying the highest risk in the Aegean region and the lowest risk in Eastern and Central Anatolia. SCORE2 and PREVENT showed strong rank-order agreement (Spearman ρ=0.95) but only modest categorical agreement (weighted κ=0.31). SCORE2-DM systematically estimated 10-year risk approximately 6 percentage points higher than PREVENT (mean difference 6.37%, 95% LoA 5.70 to 7.04). Regional differences in risk estimates remained statistically significant after multivariable adjustment for all three models (all p≤ 0.009).
Conclusion: Cardiovascular risk estimation in obese individuals is highly sensitive to the choice of prediction model and regional population characteristics. Although the three contemporary models rank patients similarly, their absolute risk estimates and categorical risk classifications can diverge substantially, particularly in obese patients with diabetes. Because this analysis is based on model-derived estimates rather than observed cardiovascular outcomes, our findings should be interpreted as descriptive risk estimation rather than validated risk prediction. These findings highlight the importance of cautious interpretation of risk scores and emphasize the need for outcome-based, population-specific validation of cardiovascular risk prediction tools in high-risk obese populations.
Keywords: obesity, cardiovascular risk prediction, SCORE2, AHA PREVENT, Türkiye, multicenter study, risk stratification, SCORE2-DM
Introduction
Despite the widespread use of cardiovascular risk scores in clinical practice, most prediction models were derived from cohorts with limited representation of individuals with severe obesity. This creates uncertainty regarding their calibration and clinical applicability in countries such as Türkiye, where obesity prevalence is among the highest in Europe.
Obesity has emerged as one of the most important global public health challenges of the twenty-first century and is strongly associated with cardiovascular disease (CVD), type 2 diabetes mellitus, hypertension, dyslipidemia, and increased all-cause mortality.1 Beyond its epidemiological impact, obesity represents a complex multisystem disease characterized by excessive adiposity, metabolic dysregulation, and chronic low-grade inflammation.2 According to the Global Burden of Disease study, obesity and overweight have become major contributors to preventable morbidity and mortality worldwide, with a steadily increasing burden over recent decades.3
Excess adipose tissue, particularly visceral fat accumulation, promotes insulin resistance, endothelial dysfunction, and proatherogenic inflammatory pathways, thereby accelerating cardiovascular disease development.4 These mechanisms form the biological basis linking obesity to cardiometabolic disorders such as diabetes, hypertension, and atherosclerotic cardiovascular disease.5 Importantly, obesity is increasingly recognized not merely as a risk factor, but as a disease entity that amplifies cardiometabolic risk across the lifespan, even in the absence of overt metabolic abnormalities.6
The burden of obesity is particularly pronounced in Türkiye. According to the World Health Organization, Türkiye has one of the highest prevalences of overweight and obesity among European countries, with approximately two-thirds of adults affected.7 This high prevalence translates into a substantial national cardiometabolic disease burden. In this context, the multicenter OBREDI-TR study, which included more than 10,000 obese individuals from seven geographical regions of Türkiye, demonstrated strikingly high prevalences of hypertension, diabetes mellitus, dyslipidemia, coronary artery disease, and fatty liver disease, underscoring the scale of obesity-related health problems at a population level.8
Accurate estimation of cardiovascular risk is a cornerstone of preventive cardiology, as it guides both lifestyle interventions and pharmacological treatment decisions. The SCORE2 algorithm, introduced by the European Society of Cardiology, estimates the 10-year risk of fatal and non-fatal cardiovascular events and incorporates regional recalibration to account for differences in baseline cardiovascular risk across European populations.9 The SCORE2-DM model was subsequently developed to provide diabetes-specific cardiovascular risk estimation within the SCORE2 framework.10 More recently, the American Heart Association introduced the PREVENT risk equations, designed to predict total cardiovascular disease risk using contemporary, multiethnic cohorts and broader cardiovascular endpoints.11
Recent external validation studies have provided important insight into the real-world performance of these contemporary tools. Large evaluations in ethnically and socioeconomically diverse populations have shown that SCORE2 generally retains acceptable discrimination but exhibits substantial calibration variability across regions and patient subgroups,12 and contemporary European cohorts have similarly reported divergent calibration performance when SCORE2 is applied outside its derivation population.13 Comparative analyses of SCORE2 with other contemporary risk tools have further suggested that, even among Europeans, agreement between these scores can be only moderate, supporting the need for population-specific evaluation.14 These observations are particularly relevant to high-prevalence obesity populations such as Türkiye, where regional cardiometabolic heterogeneity may amplify calibration differences across risk tools.
A central limitation of these contemporary models is that obesity itself is not directly incorporated as an independent predictor variable. Body mass index, waist circumference, and adiposity-related metabolic abnormalities are absent from the input variables of SCORE2, SCORE2-DM, and PREVENT, despite robust evidence linking these factors to cardiovascular risk. This omission raises specific concerns about potential misclassification or underestimation of cardiovascular risk in obese individuals, particularly in populations with high concomitant burdens of diabetes, hypertension, and dyslipidemia.12 Furthermore, regional differences in lifestyle, socioeconomic status, and healthcare access may influence the calibration and applicability of these tools across geographical settings.15
Despite the high prevalence of obesity and the substantial cardiometabolic burden in Türkiye, no large-scale, nationwide comparison has yet evaluated how contemporary cardiovascular risk estimation tools perform, or how their estimates differ, across this geographically and ethnically heterogeneous population. Therefore, the present study aimed to compare 10-year cardiovascular risk estimates derived from SCORE2, SCORE2-DM, and AHA PREVENT in a large multicenter cohort of obese individuals from seven geographical regions of Türkiye, with three specific objectives: (i) to characterize regional differences in model-derived risk estimates, (ii) to formally quantify inter-model agreement using complementary statistical approaches, and (iii) to evaluate whether observed regional differences persist after multivariable adjustment for demographic and cardiometabolic confounders.
Materials and Methods
Study Design and Population
Although the data were derived from the OBREDI-TR registry, the present analysis represents an independent and purpose-built dataset with distinct inclusion criteria, variable selection, and statistical objectives, designed specifically to evaluate contemporary cardiovascular risk estimation models rather than obesity-related comorbidity prevalence. Accordingly, no overlapping analyses or duplicated outcomes exist with previously published OBREDI-TR studies. The three estimation models—SCORE2, SCORE2-DM, and AHA PREVENT—were deliberately selected because they represent the most up-to-date European and American frameworks for cardiovascular risk estimation, allowing a comprehensive and internationally relevant comparison within a high-risk obese population.
Data were retrospectively extracted from electronic medical records covering the period 15 December 2023 to 31 December 2024. Inclusion required adult age (≥18 years) and a documented body mass index ≥30 kg/m2. Patients with active malignancy, established cardiovascular disease at the time of recruitment, pregnancy, or incomplete records that prevented calculation of any of the three risk scores in their respective subpopulations were excluded from the corresponding analyses.
Ethics Approval
The OBREDI-TR registry was approved by the Non-Interventional Clinical Research Ethics Committee of Biruni University (Approval date: 03 November 2023; Approval No: 2023/84-01). In addition, this retrospective analysis was approved by the Non-Interventional Clinical Research Ethics Committee of Van Yüzüncü Yıl University Faculty of Medicine Hospital (Approval date: 16 January 2026; Approval No: 2026/01-32).
Data Collection and Definitions
Demographic characteristics, anthropometric measurements, smoking status, laboratory parameters, comorbidities, and medication use were extracted from standardized electronic medical records. Continuous variables were summarized as median and interquartile range (IQR), while categorical variables were expressed as counts and percentages.
Variables required for each prediction model—including age, sex, smoking status, systolic blood pressure, total and HDL cholesterol, glycated hemoglobin (HbA1c) for SCORE2-DM, and additional variables required by AHA PREVENT (estimated glomerular filtration rate, body mass index, and diabetes status)—were verified for completeness in each record. No imputation of missing values was performed for any variable. Instead, a complete-case approach was applied separately for each prediction model: for a given model, only participants who simultaneously (i) met the model’s eligibility criteria as defined in its original derivation study and (ii) had complete data for every variable required by that model were included in the corresponding risk-score calculation. Cases not meeting eligibility criteria, or with any missing required variable for a given model, were excluded from that model’s analysis only and could still contribute to analyses of the other models if eligibility and completeness were satisfied for those models. Eligibility criteria were as follows: SCORE2 was applied only to non-diabetic individuals aged 40–69 years; SCORE2-DM was applied only to individuals with established diabetes mellitus aged 40–69 years; and AHA PREVENT was applied to individuals aged 30–79 years. Of the 6,378 obese individuals enrolled, the resulting model-specific analysis populations comprised 2,430 (38.1%) participants for SCORE2, 1,348 (21.1%) participants for SCORE2-DM, and 5,431 (85.2%) participants for AHA PREVENT. Because SCORE2 and SCORE2-DM target mutually exclusive populations (non-diabetic versus diabetic), the lower numbers for these two scores primarily reflect model-specific eligibility criteria—particularly the diabetes-status requirement and the narrower 40–69 year age range—rather than loss of laboratory data; AHA PREVENT, with its broader 30–79 year age range and applicability to both diabetic and non-diabetic individuals, retained substantially more participants.
Diabetes mellitus, hypertension, dyslipidemia, coronary artery disease, chronic obstructive pulmonary disease, and obstructive sleep apnea syndrome were defined according to contemporary international guidelines.7,9
Cardiovascular Risk Assessment
Cardiovascular risk was estimated using three contemporary risk prediction models: SCORE2, which estimates 10-year risk of fatal and non-fatal cardiovascular disease in the general population9; SCORE2-DM, applied to individuals with diabetes mellitus to account for diabetes-specific cardiovascular risk10; and AHA PREVENT, which estimates total 10-year cardiovascular disease risk using updated, multiethnic cohorts.11
All risk scores were computed using the official, internationally standardized equations published in the original derivation studies of SCORE2, SCORE2-DM, and AHA PREVENT. To ensure standardization across centers, calculations were performed centrally using a single validated computational script, and inputs were verified against source records before computation. For each model, both 10-year cardiovascular risk (%) and corresponding estimated survival probabilities (%) were calculated. Because risk estimates were derived from model equations rather than from observed cardiovascular events, the present analysis evaluates risk estimation rather than predictive accuracy or outcome-based validation.
Statistical Analysis
Comparisons across geographical regions were conducted using the Kruskal–Wallis test for continuous variables and the chi-square test for categorical variables. Post-hoc multiple comparisons were adjusted using appropriate correction methods. Inter-model agreement was assessed using four complementary approaches: (i) Spearman rank correlation and Pearson correlation for monotonic and linear relationships between continuous risk estimates; (ii) Bland–Altman analysis to quantify the systematic mean difference and the 95% limits of agreement (LoA, calculated as mean difference ± 1.96·SD); (iii) intraclass correlation coefficients (ICC, two-way mixed model, single rater, absolute agreement); and (iv) linear-weighted Cohen’s kappa for agreement on standard categorical risk strata (low: <5%; moderate: 5–<10%; high: ≥10%). To evaluate whether observed regional differences in cardiovascular risk estimates persisted after accounting for individual-level cardiometabolic and demographic factors, multivariable linear regression was performed for each of the three risk score outcomes, with the dependent variable being the model-derived risk and the independent variables comprising age, sex, smoking status, diabetes mellitus, hypertension, dyslipidemia, statin use, and body mass index. Adjusted regional means were obtained by predicting risk at the cohort-mean covariate values, and the overall significance of the regional effect was assessed using Type-II analysis of variance. A two-sided p-value <0.05 was considered statistically significant. All analyses were performed using SPSS software (version 26.0, IBM Corp., Armonk, NY, USA) and verified with Python 3 (statsmodels, scikit-learn, and SciPy libraries) for the agreement and multivariable analyses.
With a final sample of 6,378 obese individuals distributed across seven geographical regions, the study provides greater than 95% statistical power (α = 0.05, two-sided) to detect small-to-moderate between-region differences (Cohen’s d ≥ 0.2) in continuous risk score values, and adequate power to detect clinically relevant differences in categorical risk classification across models. The sample size therefore exceeds conventional thresholds for descriptive comparative analyses of cardiovascular risk estimates.
Results
Baseline Demographic and Clinical Characteristics
A total of 6,378 obese individuals were included in the analysis. Participants were recruited from seven geographical regions of Türkiye, with the highest proportion from the Marmara region (n = 1,385) and the lowest from Eastern Anatolia (n = 451). Sex distribution was comparable across regions (p = 0.067). In contrast, smoking status differed significantly between regions (p = 0.001), with the highest prevalence of active smoking observed in the Southeastern Anatolia (32%) and Marmara (23%) regions, and the lowest prevalence in Eastern Anatolia (6%).
Marked regional heterogeneity was observed in cardiometabolic comorbidities and medication use (all p = 0.001). The prevalence of diabetes mellitus and hypertension was highest in the Marmara and Aegean regions, whereas Eastern and Central Anatolia showed substantially lower rates. Dyslipidemia and hyperlipidemia were also more prevalent in the Marmara and Aegean regions. Coronary artery disease prevalence peaked in the Marmara region (28%), while chronic obstructive pulmonary disease was most frequent in the Aegean region (27%). Obstructive sleep apnea syndrome was most prevalent in Southeastern Anatolia (35%) and least prevalent in Eastern Anatolia and the Black Sea region (3% each). Parallel regional patterns were observed for statin and antihypertensive drug use, with the highest utilization rates in the Marmara region.
These demographic characteristics, smoking status, comorbidity distributions, and medication use patterns are summarized in Table 1.
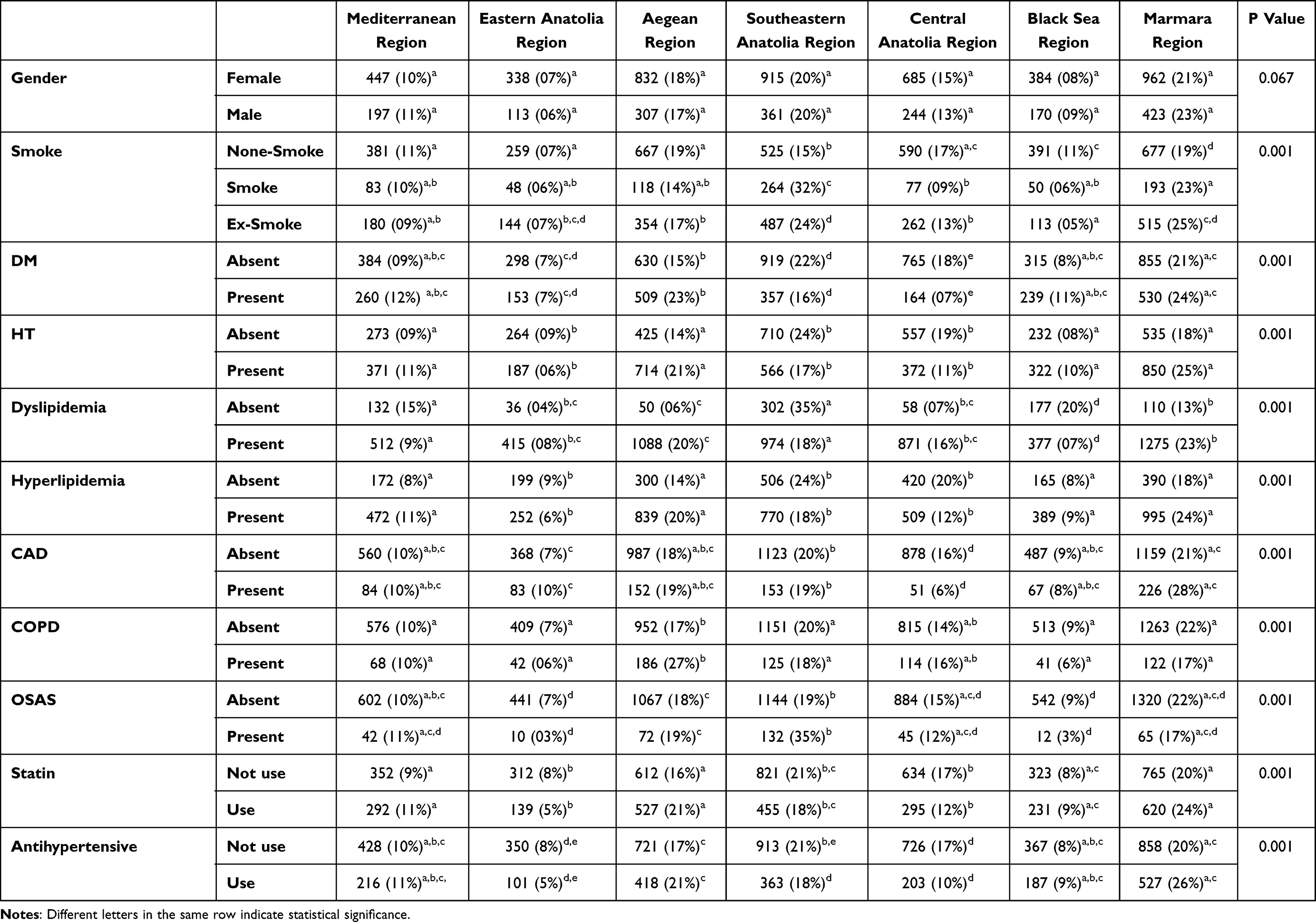 |
Table 1 Demographic Characteristics, Smoking Status, Comorbidity Distribution, and Medication Use of Participants by Geographical Regions of Türkiye |
Anthropometric, Hemodynamic, and Biochemical Parameters
Anthropometric measurements were relatively homogeneous across regions. Median body mass index ranged between 35.2 and 36.6 kg/m2, and median waist circumference was consistently approximately 110–111 cm in all geographical regions. Blood pressure measurements also showed limited variability, with a median systolic blood pressure of 140 mmHg and a median diastolic blood pressure of 80 mmHg across regions.
In contrast, several biochemical parameters exhibited significant regional variation. Fasting plasma glucose and HbA1c levels were highest in the Black Sea and Marmara regions, whereas Central Anatolia demonstrated the lowest glycemic indices. Lipid profile analysis revealed higher triglyceride and LDL-cholesterol levels in the Mediterranean and Black Sea regions, while HDL-cholesterol levels were lowest in Southeastern Anatolia.
Regional distributions of anthropometric measurements, blood pressure values, and biochemical parameters are presented in Table 2.
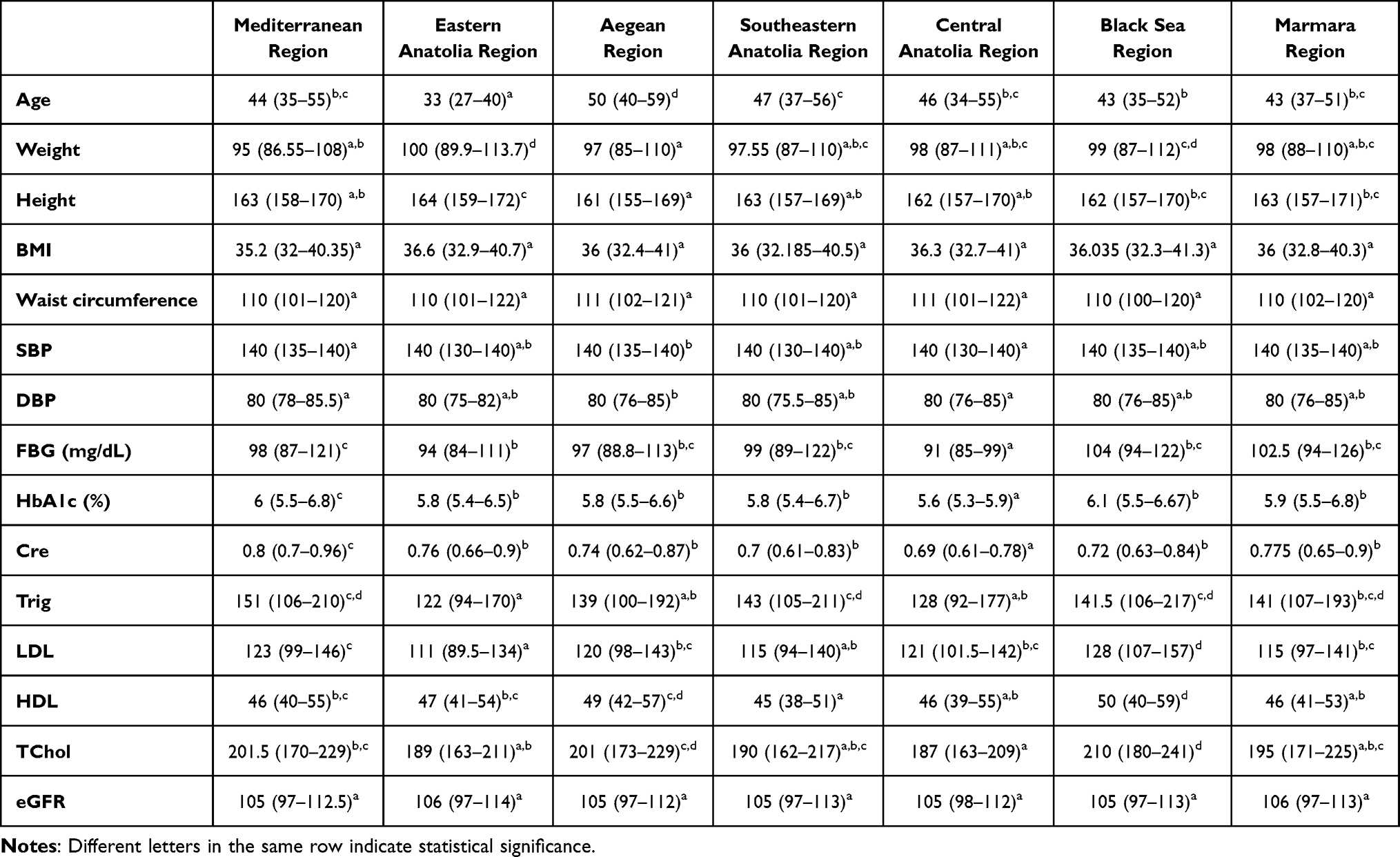 |
Table 2 Distribution of Anthropometric Measurements, Blood Pressure, and Biochemical Parameters by Geographical Regions of Türkiye (Median [IQR]) |
Cardiovascular Risk Estimates by Prediction Model
Comparison of cardiovascular risk estimates across geographical regions demonstrated model-dependent differences. According to the SCORE2 model, the highest median 10-year cardiovascular risk was observed in the Mediterranean and Southeastern Anatolia regions, whereas Central Anatolia exhibited the lowest median risk. Correspondingly, SCORE2-based 10-year cardiovascular survival estimates were highest in Central Anatolia and lowest in the Mediterranean region.
Regional variations and model-dependent differences in 10-year cardiovascular risk estimates across geographical regions are visually summarized in Figure 1.
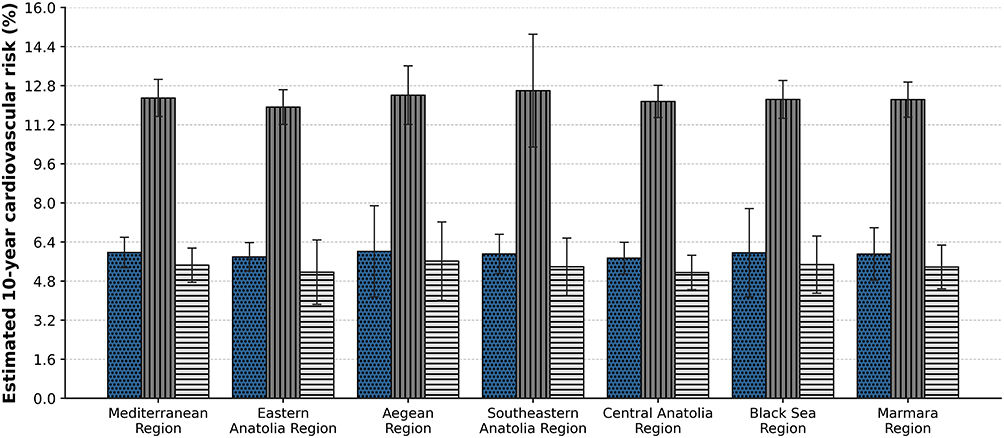 |
Figure 1 Model-dependent variability in 10-year cardiovascular risk across Turkish regions. |
SCORE2-DM estimates were comparatively more homogeneous across regions, with median 10-year cardiovascular risk values clustering around 12% and minimal variation in estimated survival probabilities. In contrast, the PREVENT model demonstrated greater regional discrimination, identifying the highest median 10-year cardiovascular risk in the Aegean region and the lowest risk in Eastern and Central Anatolia. PREVENT-derived survival estimates mirrored this pattern, with the lowest survival probabilities observed in the Aegean region. Corresponding differences in estimated 10-year cardiovascular survival probabilities according to SCORE2, SCORE2-DM, and PREVENT models are illustrated in Figure 2.
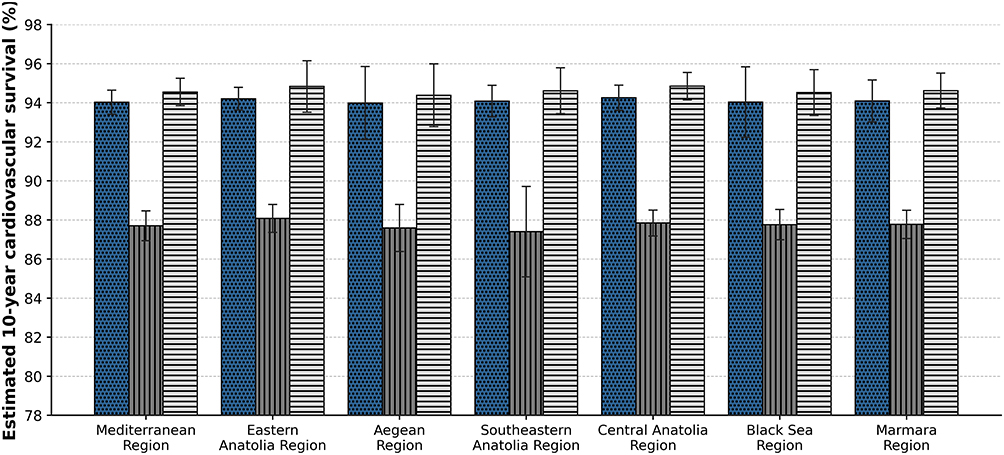 |
Figure 2 Model-dependent variability in 10-year cardiovascular survival across Turkish regions. Bar chart comparing model-derived 10-year cardiovascular survival estimates across seven geographical regions of Türkiye. Survival estimates are presented for SCORE2, SCORE2-Diabetes, and PREVENT models, demonstrating regional variation and differences according to the cardiovascular risk prediction model used. |
Detailed comparisons of 10-year cardiovascular risk and survival estimates derived from SCORE2, SCORE2-DM, and PREVENT models are shown in Table 3.
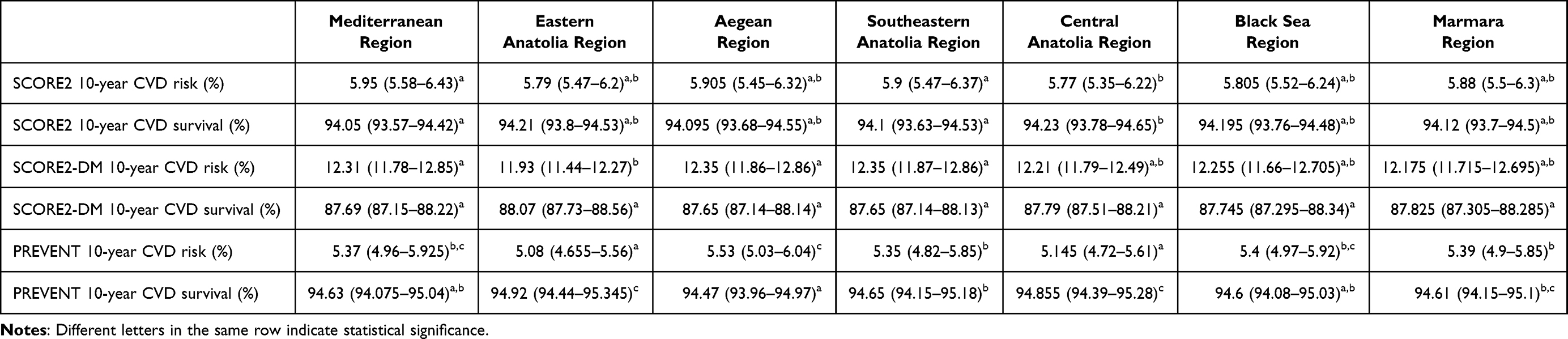 |
Table 3 Comparison of 10-Year Cardiovascular Disease (CVD) Risk and Survival Estimates Derived from SCORE2, SCORE2-DM, and PREVENT Models Across Geographical Regions of Türkiye (Median [IQR]) |
Inter-Model Agreement
Inter-model agreement was substantial in terms of rank ordering but varied considerably in absolute risk classification. Among the 2,430 participants with both SCORE2 and PREVENT estimates, the two models showed very high rank correlation (Spearman ρ = 0.95, p < 0.001) and excellent intraclass agreement (ICC = 0.83). However, Bland–Altman analysis revealed a small but consistent systematic difference: SCORE2 estimates exceeded PREVENT estimates by a mean of 0.68 percentage points (95% LoA: 0.28 to 1.09). Categorical agreement using guideline-based risk strata (<5%, 5–<10%, ≥10%) was modest, with linear-weighted Cohen’s κ = 0.31 and 72.6% raw concordance.
In contrast, agreement between SCORE2-DM and PREVENT was substantially weaker in absolute terms, despite high rank correlation. In the 1,348 individuals with diabetes mellitus, SCORE2-DM and PREVENT estimates were highly correlated (Spearman ρ = 0.95, p < 0.001) but exhibited a large systematic difference, with SCORE2-DM exceeding PREVENT by an average of 6.37 percentage points (95% LoA: 5.70 to 7.04). The corresponding ICC was poor (0.06), and categorical agreement was negligible (weighted κ < 0.01); 94% of patients were classified as high risk (≥10%) by SCORE2-DM but as moderate risk (5–<10%) by PREVENT. These findings indicate that, although the two models rank patients similarly, their absolute risk estimates and resulting categorical classifications diverge markedly in obese patients with diabetes. Detailed inter-model agreement statistics are summarized in Table 4.
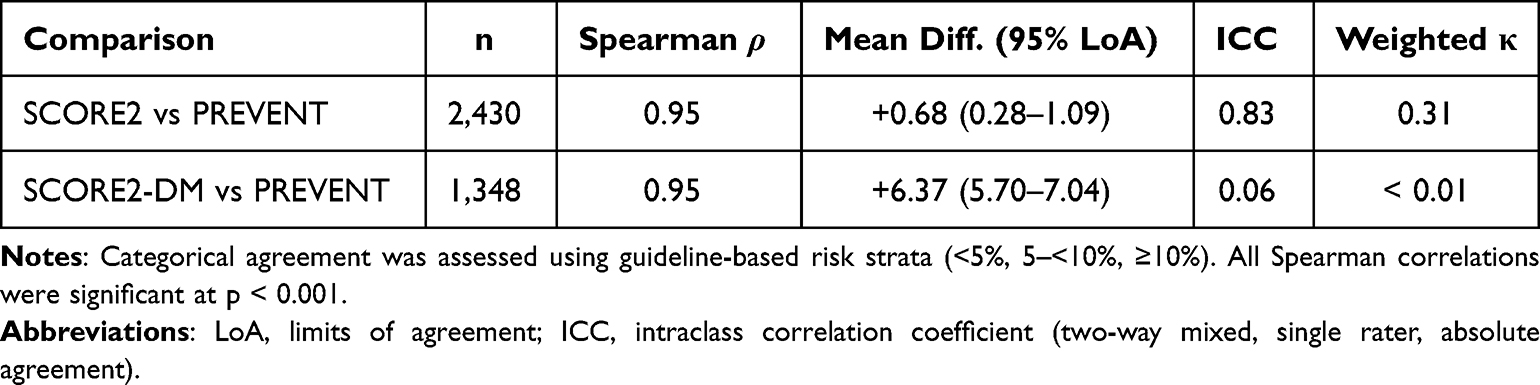 |
Table 4 Between-Model Agreement of 10-Year Cardiovascular Risk Estimates |
Multivariable-Adjusted Regional Differences
After adjustment for age, sex, smoking status, diabetes mellitus, hypertension, dyslipidemia, statin use, and body mass index, regional differences in cardiovascular risk estimates remained statistically significant for all three models (SCORE2: F = 2.94, p = 0.007; SCORE2-DM: F = 2.88, p = 0.009; PREVENT: F = 11.90, p < 0.001). Adjusted regional means showed a similar pattern to the unadjusted analyses but with attenuated magnitude. For SCORE2, the highest adjusted mean was observed in the Black Sea region (6.01%) and the lowest in Central Anatolia (5.71%); for PREVENT, adjusted means ranged from 5.11% in Central Anatolia to 5.51% in the Aegean region. The persistence of regional differences after multivariable adjustment indicates that the geographic heterogeneity in risk estimates is not entirely explained by between-region differences in measured cardiometabolic and demographic confounders, and that additional unmeasured factors—such as healthcare access, socioeconomic disparities, dietary patterns, or biological-environmental interactions—may also contribute to the observed variation.
Discussion
Our findings suggest that cardiovascular risk stratification in obese populations is highly sensitive to the choice of prediction model. Clinicians should interpret risk estimates cautiously and consider regional epidemiological context when applying these tools in routine practice. Given the high burden of obesity in Türkiye, locally validated risk prediction tools are essential for effective national prevention strategies.
In this large, multicenter cohort of obese individuals from Türkiye, we compared three contemporary cardiovascular risk prediction models—SCORE2, SCORE2-DM, and AHA PREVENT—and found that estimated 10-year cardiovascular risk varied according to both the selected model and geographic region. These findings raise important considerations regarding external validity, calibration, and clinical applicability of risk prediction tools in obese populations with heterogeneous cardiometabolic profiles.
First, although SCORE2 was designed as a contemporary update with regional recalibration, external validation suggests that its performance may vary substantially across populations with different ethnic and socioeconomic compositions. In a large external validation study in an ethnically and socioeconomically diverse population, Kist et al reported acceptable discrimination but variable calibration, with misestimation of risk in certain subgroups.12 This observation is pertinent to our nationwide obese cohort, where substantial regional heterogeneity in smoking, diabetes, hypertension, dyslipidemia, and medication use may influence baseline risk and the calibration of prediction models.
Second, even when a model is well established, agreement across different risk scores is not guaranteed. In a Turkish study evaluating contemporary risk tools, Ozpelit et al demonstrated only moderate correlation and agreement between SCORE2 and other cardiovascular risk scores, emphasizing the importance of population-specific validation before routine clinical adoption.15 Our formal inter-model agreement analyses extend this observation. While SCORE2 and PREVENT showed near-perfect rank-order concordance (Spearman ρ = 0.95) and excellent ICC (0.83), categorical agreement using guideline thresholds was only modest (weighted κ = 0.31), suggesting that a substantial proportion of obese individuals could be assigned different risk categories, and therefore different prevention recommendations, depending on which tool is used. The discrepancy was much greater for SCORE2-DM versus PREVENT in obese patients with diabetes: although the two models ranked patients similarly, SCORE2-DM systematically estimated 10-year cardiovascular risk to be ~6 percentage points higher than PREVENT, and almost all SCORE2-DM-classified high-risk patients were reclassified as moderate risk by PREVENT. This systematic divergence is consistent with the diabetes-specific recalibration applied in SCORE2-DM, which by design produces a higher baseline risk for individuals with diabetes; however, the magnitude of disagreement underscores the need for outcome-based local validation before either model is adopted for routine clinical decision-making in this population.
Third, practical implementation details can further affect risk categorization. Hageman et al showed that using SCORE2 via risk charts versus an online calculator can shift individuals across clinically relevant risk thresholds, thereby potentially altering preventive treatment decisions.16 Although standardized calculations were applied in our analysis, this finding is clinically important because real-world practice often relies on different tools, and the observed inter-model discrepancies may be amplified by differences in implementation method.
Fourth, PREVENT represents a new-generation approach to cardiovascular risk prediction using contemporary cohorts and broader cardiovascular outcomes. In an external validation analysis, Scheuermann et al demonstrated that PREVENT exhibited good discrimination compared with legacy equations but showed calibration differences across populations, supporting the need for local calibration.17 Similarly, a large real-world evaluation across multiple health systems by Cho et al confirmed that PREVENT generally maintains adequate discrimination, yet calibration can vary by healthcare system and population structure.18 In our cohort, PREVENT tended to show more pronounced regional separation than SCORE2-based estimates, which may reflect differences in endpoint definitions, modeling strategy, and baseline risk distributions captured by the PREVENT framework.
Fifth, for individuals with diabetes, SCORE2-DM was specifically developed to address the well-known underestimation of cardiovascular risk when using general population equations. Evidence suggests that SCORE2-DM may better reflect vascular risk and may align more closely with markers of subclinical atherosclerosis in diabetic individuals. Scilletta et al reported that SCORE2-DM differentiated cardiovascular risk profiles and was associated with indicators of subclinical vascular damage, supporting its potential value for diabetes-specific risk stratification.19 Furthermore, SCORE2-DM-derived estimates have also been shown to change meaningfully under contemporary glucose-lowering therapies; sodium–glucose cotransporter-2 (SGLT2) inhibitors, in particular, can favorably modify metabolic parameters, laboratory profiles, and SCORE2-DM-based cardiovascular risk projections in patients with type 2 diabetes.20 In our study, SCORE2-DM estimates were comparatively more homogeneous across regions than other models, which may indicate that diabetes-specific recalibration reduces variability driven by background population differences; however, this also underscores the importance of validating how well these estimates translate into observed outcomes in local settings.
Sixth, our multivariable-adjusted analyses provide additional insight into the drivers of regional variation. Statistically significant residual regional effects remained for all three models after adjustment for age, sex, smoking, comorbidities, statin use, and body mass index. This suggests that unmeasured factors, such as healthcare access, socioeconomic disparities, dietary patterns, or biological-environmental interactions, may contribute meaningfully to the regional variation observed in our cohort, and that risk-tool calibration may need to account for such factors in heterogeneous populations such as Türkiye.
Finally, attempts to further improve SCORE2-DM by adding vascular indices have yielded mixed results. A methodological study assessing the incremental value of adding cardio-ankle vascular index (CAVI) to SCORE2-DM reported limited improvement in risk prediction, suggesting that additional complexity may not always translate into clinically meaningful gains without robust outcome-based validation.21 Together with our findings, this supports a pragmatic interpretation: while contemporary models provide valuable structured risk estimates, their application in obese and metabolically heterogeneous populations should be accompanied by clinical judgment and, where possible, local calibration and prospective outcome validation.
It must be emphasized that the present analysis is based on model-derived 10-year cardiovascular risk estimates rather than observed cardiovascular events. Therefore, while our findings illustrate model-dependent variability, regional differences, and inter-model agreement patterns, they do not constitute outcome-based validation of these prediction tools in the Turkish obese population. Future prospective studies are needed to compare estimated and observed cardiovascular event rates and to derive locally calibrated risk thresholds suitable for clinical decision-making.
Limitations
Several limitations should be acknowledged. First, the retrospective design may introduce residual confounding and information bias, even after multivariable adjustment for measured covariates. Second, although derived from the OBREDI-TR registry, this analysis represents a separate dataset with a distinct analytical focus; nonetheless, the use of registry-based data may limit the availability of certain lifestyle variables such as physical activity, dietary patterns, and socioeconomic status, which were therefore not included in the multivariable models. Third, cardiovascular risk was estimated using prediction models rather than observed cardiovascular outcomes, precluding direct assessment of predictive accuracy or outcome-based validation. Fourth, model-specific eligibility criteria and complete-case analysis—rather than imputation—reduced the number of participants contributing to each individual model’s analysis (SCORE2 n = 2,430; SCORE2-DM n = 1,348; AHA PREVENT n = 5,431 of 6,378 enrolled), reflecting non-overlapping populations (non-diabetic vs. diabetic for SCORE2 vs. SCORE2-DM) and age-range restrictions; while this approach is appropriate for descriptive comparisons across models, the differing analysis populations for each model should be considered when interpreting between-model contrasts. Fifth, obesity was defined using body mass index alone, which does not account for body fat distribution, visceral adiposity, or ectopic fat depots that are increasingly recognized as important contributors to cardiovascular risk. Sixth, regional differences in healthcare access, screening practices, and laboratory measurement standardization may have introduced unmeasured heterogeneity that cannot be fully accounted for in a multicenter retrospective design. Finally, the SCORE2, SCORE2-DM, and PREVENT models differ in their derivation cohorts, age ranges, eligibility criteria, and outcome definitions, which may partially explain the observed inter-model differences and limit direct head-to-head comparison.
Conclusions
In this large, nationwide cohort of obese individuals from Türkiye, contemporary cardiovascular risk estimation models demonstrated model-dependent and region-specific differences in estimated 10-year cardiovascular risk. While SCORE2 and SCORE2-DM yielded relatively consistent estimates, the AHA PREVENT model showed greater regional differentiation. Although the three models showed strong rank-order agreement, their absolute risk estimates and categorical classifications diverged substantially—particularly between SCORE2-DM and PREVENT in obese patients with diabetes—and regional differences persisted after multivariable adjustment for cardiometabolic and demographic confounders.
These findings highlight that cardiovascular risk stratification in obesity is highly sensitive to the choice of prediction model and regional population characteristics. It must be emphasized that these results reflect estimated rather than validated cardiovascular risk, as model output was not compared with observed cardiovascular events. Clinicians should be aware of these differences when applying risk scores in obese patients and should not interpret estimated risk thresholds as definitive predictors of cardiovascular events without local outcome-based calibration. Future prospective studies incorporating observed cardiovascular outcomes are needed to refine risk stratification strategies tailored to high-risk obese populations and to support population-specific, outcome-validated implementation of contemporary risk tools in clinical practice.
Generative AI Statement
In accordance with the Taylor & Francis AI Policy, the authors disclose the use of a Generative AI tool during the preparation of this manuscript. ChatGPT (OpenAI, GPT-5.2) was used solely to assist with language editing, structural organization, and refinement of academic expression. The tool was not used to generate scientific ideas, analyze data, perform statistical analyses, or draw scientific conclusions. All aspects of study design, data collection, data analysis, interpretation of results, and final conclusions remain entirely the responsibility of the authors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Powell-Wiley TM, Poirier P, Burke LE, et al. Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;143:e984–13. doi:10.1161/CIR.0000000000000973
2. Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019;15:288–298. doi:10.1038/s41574-019-0176-8
3. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019. Lancet. 2020;396:1223–1249. doi:10.1016/S0140-6736(20)30752-2
4. Rohm TV, Meier DT, Olefsky JM. Inflammation in obesity, diabetes, and related disorders. Immunity. 2022;55:31–55. doi:10.1016/j.immuni.2021.12.012
5. Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365:1415–1428. doi:10.1016/S0140-6736(05)66378-7
6. Blüher M. Metabolically healthy obesity. Endocr Rev. 2020;41:bnaa004. doi:10.1210/endrev/bnaa004
7. World Health Organization. WHO European regional obesity report 2022. Geneva, Switzerland: WHO; 2022.
8. Oral A, Solmaz I, Koca N, et al. Obesity-Related Disorders in Turkey: A Multicenter, Retrospective, Cross-Sectional Analysis from the OBREDI-TR Study. J Clin Med. 2025;14(8):2680. doi: 10.3390/jcm14082680
9. SCORE2 Working Group; ESC Cardiovascular Risk Collaboration. SCORE2 risk prediction algorithms. Eur Heart J. 2021;42:2439–2454. doi:10.1093/eurheartj/ehab312
10. SCORE2-Diabetes Working Group. SCORE2-Diabetes cardiovascular risk estimation. Eur Heart J. 2023;44:4043–4140. doi:10.1093/eurheartj/ehad332
11. Khan SS, Matsushita K, Sang Y, et al. Development and validation of the AHA PREVENT equations. Circulation. 2024;149:430–440. doi:10.1161/CIRCULATIONAHA.123.065012
12. Kist JM, Cederberg H, Van der Leeuw J, et al. SCORE2 cardiovascular risk prediction in diverse populations. EClinicalMedicine. 2023;58:101900. doi:10.1016/j.eclinm.2023.101900
13. De Vries OJ, Van der Leeuw J, Cederberg H, et al. External validation of the SCORE2 risk model in a contemporary European population. Eur J Prev Cardiol. 2023;30:1012–1021. doi:10.1093/eurjpc/zwad045
14. Veronesi G, De Bacquer D, De Backer G, et al. Comparison of SCORE2 with other contemporary cardiovascular risk prediction tools in European populations. Eur Heart J Qual Care Clin Outcomes. 2024;10:142–150. doi:10.1093/ehjqcco/qcad062
15. Ozpelit ME, Ertürk M, Korkmaz A, et al. Agreement between SCORE2 and other cardiovascular risk scores. Diagnostics. 2024;14:1123. doi:10.3390/diagnostics14111223
16. Hageman SHJ, van der Leeuw J, De Vries OJ, et al. Using SCORE2 with a risk chart or online calculator: impact on cardiovascular risk classification. Eur Heart J Qual Care Clin Outcomes. 2025;11:45–52.
17. Scheuermann B, Schulte-Sutrum N, Rapp MA, et al. External validation of the AHA PREVENT cardiovascular disease risk equations. medRxiv. 2024. doi:10.1101/2024.01.12.24301234
18. Cho SMJ, DeFilippis AP, Collins BC, et al. AHA PREVENT equations and cardiovascular risk across health systems. J Am Coll Cardiol. 2025;85:123–134. doi:10.1016/j.jacc.2024.10.018
19. Scilletta S, Gigante A, Pizzini C, et al. Cardiovascular risk profile and subclinical vascular damage in subjects with diabetes: implications for SCORE2-Diabetes. Res Square. 2025.
20. Yalçın N, Aktaş S, Uyar S, Koca N . Impact of SGLT2 inhibitors on cardiovascular risk scores, metabolic parameters, and laboratory profiles in type 2 diabetes. Life (Basel). 2025;15(5):722. doi:10.3390/life15050722
21. Zhang Y, Liu X, Wang J, et al. Adding cardio-ankle vascular index to SCORE2-Diabetes: incremental value for cardiovascular risk prediction. J Clin Hypertens. 2024;26:345–353. doi:10.1111/jch.14789
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.