Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Mobile Application-Based Interventions to Improve Attention in Stroke Survivors: A Scoping Review
Authors Nugraha A ![]() , Kosasih CE
, Kosasih CE ![]() , Pramukti I
, Pramukti I ![]() , Biben V
, Biben V ![]()
Received 7 October 2025
Accepted for publication 19 January 2026
Published 11 February 2026 Volume 2026:19 571115
DOI https://doi.org/10.2147/JMDH.S571115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Linda Yoder
Andri Nugraha,1,2 Cecep Eli Kosasih,3 Iqbal Pramukti,4 Vitriana Biben5
1Doctoral Program in Medical Sciences, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Nursing, STIKes Karsa Husada Garut, Garut, West Java, Indonesia; 3Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 4Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 5Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Cecep Eli Kosasih, Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Fax +62 02287793411, Email [email protected]
Background: Stroke is a major global cause of disability, and attention deficits are among the most common cognitive impairments in survivors. These deficits limit independence and hinder rehabilitation outcomes. Conventional post-stroke rehabilitation focuses primarily on motor recovery, while targeted cognitive rehabilitation, particularly attention training, remains underrepresented.
Purpose: This scoping review aimed to identify mobile application–based interventions developed to improve attention in stroke survivors. The secondary aim was to describe the implementation settings of these interventions.
Methods: This review followed the PRISMA-ScR Arksey and O’Malley frameworks. Systematic searches were conducted in PubMed, Scopus, EBSCO-host, and Google Scholar up to January 2025. Eligible studies included randomized controlled trials (RCTs), pilot RCTs, and quasi-experimental designs involving post-stroke patients with attentional deficits using mobile applications via smartphones or tablets. Methodological quality was appraised using the Joanna Briggs Institute (JBI) checklist for RCTs and the National Institutes of Health (NIH) tool for pre–post studies without a control group.
Results: Eleven studies were included from 5840 identified records. Two types of mobile applications were identified: cognitive training applications (n = 4) incorporating structured exercises and telehealth support, and game-based rehabilitation applications (n = 7), emphasizing gamification and training tasks. The interventions were implemented in hospital-based and hybrid settings.
Conclusion: Mobile applications show promise in post-stroke attentional rehabilitation, with evidence supporting cognitive training and game-based programs via tablets in hospital or hybrid settings and these interventions improve attention. However, methodological variability and heterogeneous protocols limit study comparability. Future research needs standardized frameworks and large clinical trials, supported by digital literacy among healthcare professionals, to strengthen clinical integration within stroke rehabilitation.
Keywords: attention, cognitive rehabilitation, mHealth, mobile applications, stroke
Introduction
Stroke is an acute neurological event caused by a sudden disruption of cerebral blood flow, leading to neuronal injury and potentially resulting in long-term functional impairments.1 According to the World Health Organization and recent global estimates, the worldwide burden of stroke is projected to increase substantially from 104.2 million cases in 2017 to 113.7 million by 2030, and nearly 150 million by 2045.2 Although survival rates have improved, particularly for ischemic stroke compared to hemorrhagic stroke a considerable proportion of survivors continue to experience persistent complications.3 Cognitive impairments, including attention deficits, are particularly debilitating, affecting approximately 46% to 92% of individuals who have experienced a stroke.4 These impairments hindering recovery, reducing independence, compromising quality of life, and necessitating targeted rehabilitation strategies.5
Attentional deficits are widely acknowledged as the primary cognitive impairment following a stroke.6 Attentional deficits, marked by impairments in sustained, selective, and divided attention, result from disruptions within cortical and subcortical networks that regulate attention.7,8 Sustained attention refers to the ability to maintain focus over prolonged periods, selective attention involves filtering relevant from irrelevant information, and divided attention encompasses managing multiple tasks or stimuli simultaneously.9 Deficits in these areas manifest as significant impairments in daily activities, such as the inability to drive safely, complete household tasks (multitasking), or difficulty in following conversations in noisy environments.10,11 These deficits compromise executive function, memory, language, and daily activities, consistently linked with poorer rehabilitation outcomes and reduced quality of life.12,13 Although the global prevalence of post-stroke cognitive impairment is well documented, attentional difficulties specifically are common yet often underrecognized, particularly in low- and middle-income countries where disparities in acute care and rehabilitation access are more pronounced.14
Conventional rehabilitation approaches frequently fall short of addressing cognitive recovery, particularly attentional impairments.15 These interventions primarily emphasize physical restoration and often provide limited individualized or engaging cognitive stimulation.16,17 Challenges such as low patient engagement, restricted accessibility, and limited personalization further reduce their long-term effectiveness and the generalization of cognitive gains to everyday activities.18 Consequently, targeted and domain-specific attentional rehabilitation is essential for optimizing post-stroke recovery and improving overall quality of life.9
Recent advancements in digital health have introduced mobile application–based cognitive interventions as promising alternatives to traditional rehabilitation.17 Mobile health tools offer enhanced accessibility, affordability, and scalability, allowing patients to engage in structured cognitive exercises at home with real-time feedback.19 Gamification features and personalized training modules have been shown to improve adherence and user engagement, supporting their potential role as supplementary digital therapeutics.20,21 While digital interventions for other cognitive domains, such as memory and executive function, are increasingly available, evidence specifically targeting attentional rehabilitation through mobile applications remains limited.22
Previous reviews and meta-analyses have confirmed the general efficacy of digital cognitive rehabilitation for stroke survivors, showing significant improvements in global cognitive function, memory, and executive functions however, the specific impact on attentional domains remains insufficiently defined.23,24 This uncertainty frequently occurs because current reviews merge broad cognitive outcomes, which hides the effects on specific attentional components, and because they examine diverse digital rehabilitation technologies collectively, which makes it difficult to isolate the benefits of mobile applications alone.25 Although mobile application-based interventions offer advantages such as accessibility, personalization, and home-based usability, there is limited knowledge on whether these tools specifically target attentional domains that are critical for functional independence.26 To address this gap, the present scoping review aims to identify mobile applications that target attention in individuals with stroke and to describe their implementation settings, with implications for health service delivery and digital health strategies.
Materials and Methods
Design
This study used a scoping review following the PRISMA Extension for Scoping Reviews (PRISMA-ScR) as proposed by Arksey and O’Malley (2005).27 The broad review question was, What mobile application-based interventions have been explored to improve attention in stroke patients within rehabilitation settings (hospital, home, or community)?. The narrow question of this review was which mobile application-based cognitive interventions have been identified, and in which rehabilitation settings (hospital, home, or community) have they been implemented to enhance attention among stroke patients, with implications for clinical practice and digital health strategies?.
Eligibility Criteria
The search approach adhered to the PRISMA-ScR guidelines. Articles were selected based on the inclusion and exclusion criteria. In this study, the Population, Concept, Context (PCC) framework was used as a guide.
Population: Stroke patients with attention deficits.
Concept: Mobile application-based interventions to improve attention.
Context: Rehabilitation settings (hospital, home, and community).
Additionally, we included primary studies, such as randomized controlled trials and quasi-experiments, which evaluated mobile application-based (smartphone and tablet) interventions, either as the primary delivery or as an adjunct (eg, monitoring, feedback) alongside other platforms, such as virtual reality interventions aimed at improving attention in stroke. Only studies published in English, with publication years up to January 2025, and conducted in various rehabilitation settings were considered. The exclusion criteria were studies focusing exclusively on motor or language rehabilitation, those employing non-mobile technologies such as robotics or personal computers, protocols, reviews, meta-analyses, editorials, commentaries, and studies lacking primary data or available only as abstracts.
Search Strategy and Study Selection
In this scoping review, articles were obtained from PubMed, Scopus, EBSCO-host, and Google Scholar databases. A keyword-adjusted MeSH term was used, focusing on mobile application-based interventions designed to improve attention in stroke patients with attention deficits (Table 1). Two authors from the research team (C.E. and A.N). independently screened the titles and abstracts, followed by a full-text review and data extraction by the same team. In cases of disagreement, discussions were conducted to reach a consensus.
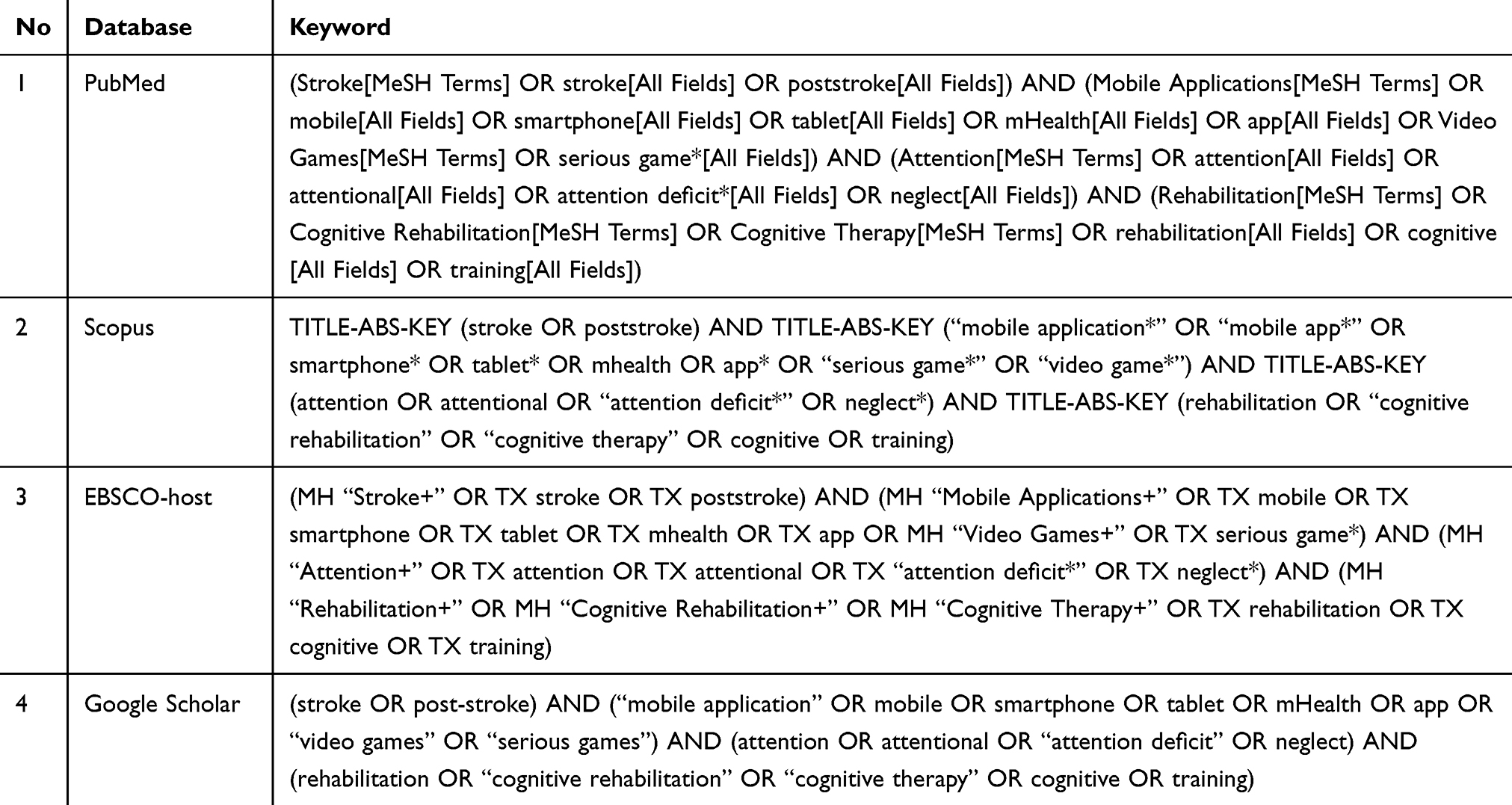 |
Table 1 Searching Strategy |
The study assessment was performed by two independent reviewers, with additional consultation from another author (I.P and V.B). The Joanna Briggs Institute (JBI) critical appraisal tool was used for quality assessment. The quality of the articles was evaluated using the JBI Critical Appraisal Tool for randomized controlled trials (RCTs) and the National Institutes of Health (NIH) quality assessment tool for before–after (pre-post) studies without a control group.28,29 Articles were considered to meet the quality criteria if they achieved a minimum score of ≥75%, calculated based on the proportion of items rated “yes” across all statements. Further details of this study are presented in Table 2.
 |
Table 2 Quality Appraisal |
Data Extraction and Analysis
Data extraction was conducted by the first author (A.N) and subsequently verified by other authors (C.E. and I.P). Essential information was gathered from the articles reviewed in the subsequent sections. The outcomes of this review are shown in Table 3, including the author, year of publication, country, study design, sample size and characteristics (age), application type, platform, key features, outcomes, setting, and main findings. All discrepancies were resolved through discussion until a consensus was reached.
 |
Table 3 Extraction Data |
A descriptive analysis was conducted to summarize the characteristics of the included studies. Study attributes, such as intervention type, delivery platform, features, and outcome categories, were organized into tables and synthesized narratively. Frequency counts and categorical mapping were used to identify patterns in the study designs, implementation settings, and intervention components. To complement the descriptive summaries, the research team performed a qualitative thematic analysis to identify recurring themes related to the intervention features, implementation contexts, and reported outcomes. This integrated approach allowed the findings to be synthesized comprehensively and presented under structured thematic categories.
Results
Study Selection Results
A total of 5840 records were initially identified from Scopus (n = 572), PubMed (n = 981), EBSCO-host (n = 1117), and Google Scholar (n = 3170) databases. After removing 378 duplicates, 5462 records were screened by title and abstract based on predetermined inclusion and exclusion criteria. This process yielded 30 full-text articles for eligibility assessment. Following a detailed evaluation, 19 articles were excluded (eg, not related to digital health interventions, not randomized controlled trials, or not stroke populations), resulting in the inclusion of 11 studies in the final review. The details of the selection process are presented in Figure 1 and Table 1, respectively.
 |
Figure 1 PRISMA Flowchart of Study Selection Process. Adapted from the study by Page et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews.41. |
Characteristic of Included Studies
Eleven studies were included in this review. The study designs included randomized controlled trials (n = 4),22,34,36,38 pilot randomized controlled trials (n = 4),31,32,35,39 and quasi-experimental studies (n = 3).30,33,37 Across all studies, the combined sample size was 412 post-stroke participants. The studies were geographically diverse, with contributions from the United States (n = 1),30 Italy (n = 3),22,31 South Korea (n = 2),32,38 Thailand (n = 1),33 Egypt (n = 2),34,37 China (n = 1),35 and Germany (n = 1).39 Regarding patient characteristics, the reported mean age of participants ranged from 18 to approximately 75 years, with the majority of the studies involving participants in the 60–70 year age group. The detailed characteristics of the included studies are summarized in Table 3.
Mobile Applications Identified
This review identified 11 mobile application–based interventions targeting post-stroke attentional rehabilitation (Table 3, Figures 2 and 3). Two primary categories of applications were used: cognitive training applications (n = 4)30,31,36,38 and game-based rehabilitation applications (n = 7).22,32–35,37,39 As illustrated in Figures 2 and 3, cognitive training interventions typically incorporated multiple functional components, including monitoring, assessment, and telehealth support. In contrast, game-based interventions were characterized primarily by training-intensive tasks and robust gamification features, with limited use of monitoring or clinician-facing capabilities. Overall, Figures 2 and 3 show that training and gamification were the most frequently reported components, followed by monitoring, telehealth, and assessment. Cognitive training applications were predominantly tablet-based and featured structured attention-focused exercises supported by clinician monitoring and feedback. Game-based applications emphasized engagement through gamification mechanics combined with cognitive training tasks to support attentional rehabilitation. A synthesis of application types and intervention characteristics is presented in Table 3, with methodological quality summarized in Table 2.
 |
Figure 2 Key features of mobile application–based interventions for post-stroke attentional rehabilitation, categorized by cognitive training and game-based applications. |
 |
Figure 3 Distribution of key features in mobile application–based interventions for post-stroke attentional rehabilitation, showing training, gamification, monitoring, assessment, and telehealth support. |
Cognitive Training Applications
The cognitive training applications identified in this review were consistently designed for tablet-based delivery and emphasized structured training protocols tailored to attentional rehabilitation (Table 3, Figures 2 and 3).30,31,36,38 As reflected in Figures 2 and 3, cognitive training applications demonstrate a broader range of functional components than game-based applications, particularly through the inclusion of assessment and telehealth features. This functional diversity highlights the emphasis on structured therapeutic delivery and clinician-guided monitoring. These applications incorporated multiple functionalities, including task-based cognitive exercises, continuous monitoring of user performance, integrated assessment tools, and telehealth support features to facilitate remote clinician supervision.36 Despite similarities in platform and core functions, the studies demonstrated heterogeneous outcomes. A quasi-experiment study30 and a pilot RCT31 both reported significant improvements in attention, particularly in sustained and selective domains, highlighting their potential efficacy in clinical and home-based settings.30,31 In contrast, two randomized controlled trials found no measurable benefits, indicating variability in the intervention protocols, dosage, and study design.36,38 Across the included trials, outcome measures differed considerably in terms of the attentional domains assessed, the instruments used, and the scoring criteria applied. This variability likely influenced the comparability of the findings across studies and contributed to the differences in the reported effectiveness.
Game-Based Rehabilitation Applications
Game-based rehabilitation applications represent the most frequently reported category of intervention for post-stroke attentional rehabilitation (Table 3, Figures 2 and 3).22,32–35,37,39 Consistent with the distribution patterns shown in Figures 2 and 3, game-based interventions relied heavily on training and gamification features, with minimal integration of monitoring, assessment, or telehealth capabilities. This concentration of features reflects a design approach focused on engagement and task repetition rather than on comprehensive clinical oversight. These applications were primarily delivered via tablets or smartphones and consistently incorporated gamification elements such as levels, scoring systems, and feedback mechanisms, along with structured training tasks to sustain user motivation and engagement. Six studies reported significant improvements in various domains of attention, including sustained, selective, and visual–spatial attention.22,32–35,37 In contrast, one pilot randomized controlled trial found no significant effects, underscoring the methodological variability in study designs, intervention protocols, and sample characteristics.39 These mixed findings underscore the variability in study design, intervention intensity, and sample characteristics. A summary of the outcomes of game-based applications is presented in Table 3.
Implementation Settings
This scoping review identified two primary implementation settings for mobile application–based interventions in post-stroke attentional rehabilitation: clinical settings and hybrid hospital-based approaches (Table 3). Clinical settings (n = 7)22,32–35,37,39 were the most frequently reported, with studies conducted exclusively in hospitals. These interventions often demonstrate improvements in attentional performance. However, some randomized controlled trials (RCTs) have yielded non-significant results, underscoring the variability in study design, intervention protocols, and dosage.22,32–35,37,39 While some studies have reported significant improvements in attention, others have found no measurable benefits, highlighting the heterogeneity of intervention delivery and outcome measures in this field.22,32–35,37,39 Summaries of implementation contexts and associated outcomes are presented in Table 3.
Discussion
Compared with previously published reviews on technology-assisted or digital cognitive rehabilitation after stroke, this review provides a more focused and methodologically distinct contribution by examining mobile application–based interventions specifically targeting attentional rehabilitation. Prior reviews have generally encompassed broad cognitive domains, computer-based training, virtual reality systems, or generalized telerehabilitation models without isolating mobile platforms as an independent modality.23 No previous synthesis has evaluated evidence exclusively on mobile-delivered attentional interventions or investigated how clinical contexts, such as hospital-based, hybrid hospital-to-home, or remotely supervised models, influence therapeutic outcomes.24 It also identifies critical evidence gaps that earlier studies did not address, including the complete absence of community-based programs and the lack of personalized or AI-driven adaptive mechanisms within current mobile interventions.
Although many studies reported statistically significant improvements in attentional outcomes,22,30–35,37 several did not show measurable benefits.36,38,39 These mixed findings extend the variability highlighted earlier and illustrate the heterogeneity of outcomes across studies and can be linked to methodological variability, including differences in intervention duration, frequency, therapeutic intensity, targeted attentional domains such as sustained (the ability to maintain focus over time), selective (the ability to focus on relevant stimuli while ignoring distractions), or visuospatial attention (the ability to direct attention to specific locations in the visual field), and the sensitivity of outcome measures.31,35 Cognitive training applications typically focused on structured tasks designed to enhance specific attentional processes,30,31,36,38 whereas game-based applications emphasized motivation and engagement through reward systems and adaptive difficulty.22,32–35,37,39 Studies with higher therapeutic dosages, clearer alignment between app tasks and attentional domains, and structured supervision tended to report more positive outcomes,22,31,37 while shorter or nonspecific interventions more frequently showed null results.36,38,39 Collectively, these findings underscore the need for standardized intervention protocols and theoretically grounded task designs to reduce heterogeneity.
Mobile applications were consistently designed to deliver structured cognitive training, often incorporating gamified elements to enhance user engagement as seen in several trials of tablet- and smartphone-based interventions.22,32–35,37,39 In some studies, remote monitoring or telehealth support was also included to extend care beyond the clinic.30,31,36,38 These studies were conducted across diverse regions, including the United States, Italy, South Korea, China, Egypt, Thailand, and Germany, indicating that mobile-based interventions are adaptable across various healthcare contexts.22,30–39 However, descriptions of personalization, adaptive feedback, or AI-driven mechanisms were notably absent, and none of the included studies detailed cultural tailoring or local development, limiting conclusions about contextual fit or cultural relevance. This gap mirrors the broader inconsistencies in intervention design and highlights the need for clearer reporting standards.
The crucial role of healthcare professionals further shapes the effectiveness of mobile-based attention rehabilitation. Evidence shows that mobile applications, serious games, and telerehabilitation can support improvements in attention, but their success depends on clinicians’ ability to tailor tasks, monitor progress, and adapt interventions to individual needs as demonstrated in studies that incorporated clinician-supported features such as monitoring, assessment, and telehealth support.30,31,36,38 Occupational therapists adjust tablet-based tasks for motor limitations, while nurses help maintain motivation and adherence in subacute settings, reflecting the supervised nature of most interventions, particularly those conducted in hospital-based environments.22,32–35 As remote rehabilitation models expand and digital platforms incorporate more advanced features, clinicians require stronger competencies in digital literacy, ethical considerations, and technology-enabled care consistent with the hybrid hospital to home designs reported in multiple trials.30,31,36,38 These demands underscore the importance of interprofessional training that integrates digital health skills with evidence-based rehabilitation strategies.
Focusing specifically on attentional rehabilitation, trials of mobile-based cognitive training and serious-game interventions have frequently reported improvements in attentional performance, as shown in multiple quasi-experimental and randomized controlled studies.22,30–35,37 These gains were demonstrated across tablet and smartphone platforms employing multimodal digital features designed to structure training, enhance engagement, and support remote clinician oversight when available.30,31,36,38 However, several studies reported no significant improvements, indicating variability in effectiveness.36,38,39 The convergence of findings from earlier paragraphs suggests that these inconsistencies arise not only from study design and intervention intensity but also from supervision levels, application features, adherence, and accessibility, all of which varied considerably across the included trials. To maximize therapeutic benefits, mobile-based interventions should incorporate clinically meaningful tasks, user-centered designs, and structured oversight and standardized outcome measures, rigorous methodologies, and clear reporting are essential for strengthening the evidence base.40 While mobile applications provide valuable opportunities for home-based practice, current evidence suggests that they complement rather than replace clinician-guided therapy.41 Consistent with trends in the broader rehabilitation literature, focused evidence on attentional outcomes remains limited, indicating the need for higher-quality studies with clearer intervention frameworks.42
Implications for Clinical Practice
Mobile applications have the potential to improve attention in stroke survivors through gamification and telehealth cognitive training. Most interventions occurred in hospitals or hybrid hospital-to-home settings, extending rehabilitation beyond supervision. These tools can complement conventional rehabilitation by supporting continuity and enhancing patient engagement. However, multidisciplinary oversight remains essential to ensure safety. The findings were mixed, with varying results across different designs and protocols. The success of digital health depends on cultural adaptation, accessibility, and patient adherence. Policymakers should consider integrating validated mobile applications into rehabilitation pathways while supporting additional trials to strengthen the evidence.
Strengths and Limitations
This review demonstrates the value of a comprehensive search across diverse settings to provide an overview of mobile applications for post-stroke attentional rehabilitation in adults. The methodological quality of the included studies was acceptable, enhancing the reliability of the findings. However, this study has several limitations. Variations in protocols and outcome measures complicate comparisons and limit their generalizability. The findings were heterogeneous, with mixed effectiveness, suggesting that study design, patient characteristics, and intervention features may influence outcomes. The evidence base is limited by small-scale, short-term studies, and few telehealth approaches are compared with hospital-based programs. Moreover, no studies were identified in community-based settings, which restricts generalizability and highlights an important research gap. Addressing these limitations through standardized methods, larger samples, and extended follow-up will be critical to strengthen the evidence and guide future practice and policy.
Conclusion
Mobile application interventions show promise in post-stroke attentional rehabilitation. The strongest and most consistent evidence emerged from structured cognitive training applications and game-based attentional training programs, particularly when delivered via tablets or smartphones in hospital or hybrid hospital-to-home settings. These interventions reliably improved attention performance and added value through increased engagement and remote monitoring capabilities. However, methodological variability and heterogeneous intervention protocols continue to limit the comparability of studies. Future progress will require standardized frameworks and large-scale clinical trials supported by adequate digital literacy and training among healthcare professionals. Overall, mobile applications can effectively complement conventional rehabilitation methods. These findings advance current practice by identifying the most evidence-supported app-based approaches and clarifying future research priorities centered on standardization, scalability, and clinical integration.
Acknowledgments
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science, and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6.RKT/HK.07.00/2025). The authors would also like to express their sincere gratitude to STIKes Karsa Husada Garut for their institutional support during this study. The authors also acknowledge the use of Paperpal (2025 version) for language editing. All the scientific content, analyses, interpretations, and conclusions are the sole responsibility of the authors.
Funding
This research was financially supported by the Indonesian Education Scholarship, Center for Higher Education Funding and Assessment, and Indonesian Endowment Fund for Education under grant number: 00565/BPPT/BPI.06/9/2024.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Uysal S. Stroke and Vascular Cognitive Impairment. In: Functional Neuroanatomy and Clinical Neuroscience. Oxford University PressNew York; 2023:226–12. doi:10.1093/oso/9780190943608.003.0018
2. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: A report from the American Heart Association. Circulation. 2020;141(9). doi:10.1161/CIR.0000000000000757
3. Waziry R, Heshmatollah A, Bos D, et al. Time trends in survival following first hemorrhagic or ischemic stroke between 1991 and 2015 in the rotterdam study. Stroke. 2020;51(3):824–829. doi:10.1161/STROKEAHA.119.027198
4. Wang W, You M, Ma W, Yang Y. Effect of eye-tracking-based attention training for patients with poststroke cognitive impairment: a study protocol for a prospective, single-blinded, single-centre, randomised controlled trial in China. BMJ Open. 2024;14(2):e079917. doi:10.1136/bmjopen-2023-079917
5. Mancuso M, Iosa M, Aabbruzesse L, et al. The impact of cognitive function deficits and their recovery on functional outcome in subjects affected by ischemic subacute stroke: results from the Italian multicenter longitudinal study CogniReMo. Eur J Phys Rehabil Med. 2023;59(3). doi:10.23736/S1973-9087.23.07716-X
6. Ebaid D, Bird LJ, McCambridge LJE, et al. Mood and cognitive trajectories over the first year after mild ischemic stroke. J Stroke Cerebrovascular Dis. 2022;31(4):106323. doi:10.1016/j.jstrokecerebrovasdis.2022.106323
7. Sakai K, Miyauchi T, Tanabe J. Assessment tools for attention deficits in patients with stroke: a scoping review across components and recovery phases. PeerJ. 2025;13:e19163. doi:10.7717/peerj.19163
8. Liu J, Wang C, Zhang Y, Guo J, Miao P, Wei Y. Cortical structure reorganization and correlation with attention deficit in subcortical stroke: an underlying pattern analysis. Neuroimage Clin. 2024;42:103612. doi:10.1016/j.nicl.2024.103612
9. Loetscher T, Potter KJ, Wong D, Das Nair R. Cognitive rehabilitation for attention deficits following stroke. Cochrane Database Syst Rev. 2019. doi:10.1002/14651858.CD002842.pub3
10. Milani G, Baroni A, Galluccio M, et al. Action observation training for upper limb stroke rehabilitation: a pilot study on the role of attention. J Clin Med. 2025;14(18):6618. doi:10.3390/jcm14186618
11. Fitzhugh MC, LaCroix AN, Rogalsky C. Distinct contributions of working memory and attentional control to sentence comprehension in noise in persons with stroke. J Speech Lang Hear Res. 2021;64(8):3230–3241. doi:10.1044/2021_JSLHR-20-00694
12. Schumacher R, Halai AD, Lambon Ralph MA. Assessing and mapping language, attention and executive multidimensional deficits in stroke aphasia. Brain. 2019;142(10):3202–3216. doi:10.1093/brain/awz258
13. Milosevich E, Kusec A, Pendlebury ST, Demeyere N. Domain-specific cognitive impairments, mood and quality of life 6 months after stroke. Disabil Rehabil. 2025;47(2):435–444. doi:10.1080/09638288.2024.2340121
14. Mtambo ML, Ragunathan T, Mohan D, Warren N, Su TT, Quek KF. Post-stroke cognitive impairment and dementia research in Southeast Asia: a scoping review. Asian J Psychiatr. 2025;107:104460. doi:10.1016/j.ajp.2025.104460
15. D’Imperio D, Romeo Z, Maistrello L, et al. Sensorimotor, attentional, and neuroanatomical predictors of upper limb motor deficits and rehabilitation outcome after stroke. Neural Plast. 2021;2021:1–12. doi:10.1155/2021/8845685
16. Jin L, Zhao Y, Ye T, He Y, Yao L. Cognitive and emotional impairment in stroke survivors: insights from a multi-center study on inpatient rehabilitation therapy. Brain Inj. 2024;38(8):630–636. doi:10.1080/02699052.2024.2333398
17. Kulshrestha S, Agrawal M, Singh AK, Ved A. Comparison of changes in cognitive functions of post-stroke patients with the computer-based cognitive intervention (PABLO System) and conventional cognitive intervention (Paper-pencil Method). Current Psychiatry Res Rev. 2021;17(1):47–56. doi:10.2174/2666082217666210408122228
18. Silva GS, Rocha E. Developing systems of care for stroke in resource-limited settings. Semin Neurol. 2024;44(02):119–129. doi:10.1055/s-0044-1782617
19. Kumar A, Khurana D, Pattanaik S, et al. A mobile application-based post-stroke care strategy for survivors and their caregivers for prevention and management of post-stroke complications – “Stroke Home Care:” Development and feasibility. J Neurosci Rural Pract. 2023;15:217. doi:10.25259/JNRP_411_2023
20. Sánchez-Gil JJ, Sáez-Manzano A, López-Luque R, Ochoa-Sepúlveda JJ, Cañete-Carmona E. Gamified devices for stroke rehabilitation: a systematic review. Comput Methods Programs Biomed. 2025;258:108476. doi:10.1016/j.cmpb.2024.108476
21. Nugraha A, Kosasih C, Pramukti I, Biben V. Gamification strategies in digital health interventions for attention rehabilitation in stroke survivors: a systematic review. J Multidiscip Healthc. 2025;18:8169–8184. doi:10.2147/JMDH.S566115
22. Oliveri M, Bagnato S, Rizzo S, et al. A novel digital approach for post-stroke cognitive deficits: a pilot study. Restor Neurol Neurosci. 2023;41(3–4):103–113. doi:10.3233/RNN-231305
23. Wang C, Liu M. Digital interventions for cognitive dysfunction in patients with stroke: systematic review and meta-analysis. J Med Internet Res. 2025;27:e73687. doi:10.2196/73687
24. Liu S, Li M, Ding J, et al. Effectiveness, feasibility, acceptability, and safety of digital interventions in post-stroke rehabilitation: a systematic review and meta-analysis of randomized controlled trials. Arch Phys Med Rehabil. 2025. doi:10.1016/j.apmr.2025.07.004
25. Szeto SG, Wan H, Alavinia M, Dukelow S, MacNeill H. Effect of mobile application types on stroke rehabilitation: a systematic review. J Neuroeng Rehabil. 2023;20(1):12. doi:10.1186/s12984-023-01124-9
26. Kheirollahzadeh M, Sarvghadi P, Bani Hani J, Azizkhani S, Monnin C, Choukou MA. Digital health technologies to support at-home recovery of people with stroke: a scoping review. Appl Sci. 2025;15(10):5335. doi:10.3390/app15105335
27. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
28. Joanna Briggs Institute (JBI). JBI’s critical appraisal tools [internet]. Available from: https://jbi.global/critical-appraisal-tools. 2022.
29. National Institutes of Health. Quality assessment tool for before-after (pre-post) studies with No control group [internet]. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. 2022.
30. Des Roches CA, Balachandran I, Ascenso EM, Tripodis Y, Kiran S. Effectiveness of an impairment-based individualized rehabilitation program using an iPad-based software platform. Front Hum Neurosci. 2015;8. doi:10.3389/fnhum.2014.01015
31. Torrisi M, Maresca G, De Cola MC, et al. Using telerehabilitation to improve cognitive function in post-stroke survivors: is this the time for the continuity of care? Int J Rehabil Res. 2019;42(4):344–351. doi:10.1097/MRR.0000000000000369
32. Jung HT, Daneault JF, Nanglo T, et al. Effectiveness of a serious game for cognitive training in chronic stroke survivors with mild-to-moderate cognitive impairment: a pilot randomized controlled trial. Appl Sci. 2020;10(19):6703. doi:10.3390/app10196703
33. Thaivon T, Munkhetvit P. Effects of applications on computer tablet for cognitive training in stroke patients. ASEAN J Rehabil Med. 2020;30(2):47–53.
34. Abou-Shady NAE, Omara T, Soliman KMAEH, Abdelhakiem NM. Influence of mobile application based brain training program on cognitive function and quality of life in patients post stroke. J Adv Zool. 2023;44(S–3):204–210. doi:10.17762/jaz.v44iS-3.568
35. Liu Z, He Z, Yuan J, et al. Application of immersive virtual-reality-based puzzle games in elderly patients with post-stroke cognitive impairment: a pilot study. Brain Sci. 2022;13(1):79. doi:10.3390/brainsci13010079
36. Contrada M, Arabia G, Vatrano M, et al. Multidomain cognitive tele-neurorehabilitation training in long-term post-stroke patients: an RCT study. Brain Sci. 2025;15(2):145. doi:10.3390/brainsci15020145
37. Abdou FA, Abd Elbaky MM, Ahmed NA. Effect of using mobile games on patients with acute stroke during cognitive rehabilitation at the intensive care unit. Alexandria Scient Nurs J. 2023;25(3):13–25.
38. Kim S, Park SW, Jeong T, Kang MS, Kim DY. AI-driven cognitive telerehabilitation for stroke: a randomized controlled trial. Front Neurol. 2025;16. doi:10.3389/fneur.2025.1636017
39. Specht J, Stegmann B, Gross H, Krakow K. Cognitive training with head-mounted display virtual reality in neurorehabilitation: pilot randomized controlled trial. JMIR Serious Games. 2023;11:e45816. doi:10.2196/45816
40. Chien SY. A usability evaluation framework for a mobile application in supporting home-based rehabilitation for stroke patients: a qualitative study. Digit Health. 2025;11. doi:10.1177/20552076251340183
41. Cao W, Kadir AA, Tang W, Wang J, Yuan J, Hassan II. Effectiveness of mobile application interventions for stroke survivors: systematic review and meta-analysis. BMC Med Inform Decis Mak. 2024;24(1). doi:10.1186/S12911-023-02391-1
42. Zhou X, Du M, Zhou L. Use of mobile applications in post-stroke rehabilitation: a systematic review. Top Stroke Rehabil. 2018;25(7):489–499. doi:10.1080/10749357.2018.1482446
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.