Back to Journals » Psychology Research and Behavior Management » Volume 19
MMPI-3 Psychopathological Profiles in Iranian Patients with Somatic Symptom and Related Disorders: A Cross-Sectional Study
Authors Naderi Rajeh Y, Kameli P, Norouzi A, Rezapour M
Received 25 February 2026
Accepted for publication 25 June 2026
Published 3 July 2026 Volume 2026:19 604186
DOI https://doi.org/10.2147/PRBM.S604186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mei-Chun Cheung
Yazdan Naderi Rajeh,1 Parisa Kameli,2 Asghar Norouzi,3 Maryam Rezapour,1
1Psychiatry and Behavioral Sciences Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran; 2Faculty of Psychology and Educational Sciences, Islamic Azad University, Roudehen, Iran; 3Department of Psychology, Sari Branch, Islamic Azad University, Sari, Iran
Correspondence: Parisa Kameli, Faculty of Psychology and Educational Sciences, Islamic Azad University, Roudehen, Iran, Email [email protected]
Background: Somatic symptom and related disorders are characterized by persistent physical symptoms accompanied by psychological distress, functional impairment, and complex patterns of emotional and cognitive vulnerability. Although these disorders are clinically important, multidimensional psychopathological profiling with contemporary instruments remains limited in Middle Eastern populations. This study aimed to characterize the MMPI-3 psychopathological profile of Iranian patients with somatic symptom and related disorders.
Methods: Using convenience sampling, this cross-sectional study included 120 patients diagnosed with somatic symptom and related disorders according to DSM-5 criteria at Imam Khomeini Hospital, Sari, Iran, between May and September 2024. Participants completed the Minnesota Multiphasic Personality Inventory-3. MMPI-3 T-scores were compared with the normative mean of 50 using one-sample t-tests. Cohen’s d effect sizes were calculated, and domain-wise Bonferroni correction was applied.
Results: Patients showed the largest elevations in Anxiety (mean T-score = 62.71, d = 0.99), Anger Proneness (mean T-score = 58.63, d = 0.96), Low Positive Emotions (mean T-score = 59.26, d = 0.87), Somatic Complaints (mean T-score = 61.03, d = 0.86), Fearfulness (mean T-score = 63.66, d = 0.85), Dysfunctional Negative Emotions (mean T-score = 59.48, d = 0.84), and Negative Emotionality/Neuroticism (mean T-score = 58.94, d = 0.82). In contrast, Juvenile Conduct Problems, Antisocial Behavior, Aggressiveness, and Disconstraint were lower than normative values. The overall profile indicated a predominantly internalizing pattern rather than an externalizing behavioral profile.
Conclusion: Iranian patients with somatic symptom and related disorders showed a distinctive MMPI-3 profile marked by internalized emotional distress, somatic-cognitive preoccupation, and reduced externalizing pathology. These findings support the clinical value of structured psychological assessment in this population and highlight treatment-relevant targets, including anxiety, hopelessness, body-focused preoccupation, emotion regulation difficulties, and suicide-risk monitoring.
Keywords: somatic symptom disorder, psychosomatic disorders, MMPI-3, psychopathology, internalizing spectrum, suicide ideation, behavior management
Background
Somatic symptom and related disorders are clinically important conditions in which persistent physical symptoms are accompanied by disproportionate psychological distress, excessive health-related thoughts, and functional impairment. These disorders occupy an important position at the interface of psychiatry, psychology, and general medicine because patients frequently present first with bodily complaints rather than overt psychological symptoms. This presentation can complicate diagnosis, increase repeated healthcare use, and delay appropriate psychological or psychiatric intervention.1–3
Mental disorders contribute substantially to the global burden of disease, and their impact has increased over recent decades. This burden is particularly relevant in Middle Eastern populations, where sociocultural, structural, and healthcare-related factors may influence the recognition, expression, and management of psychological distress.4,5 In many clinical contexts, distress may be communicated through physical symptoms, making the assessment of somatic symptom presentations especially important. In Iran, previous studies have reported associations between somatization, anxiety, depression, alexithymia, and psychosomatic complaints, but comprehensive psychometric profiling of patients with somatic symptom and related disorders remains limited.6
A key theoretical construct in this field is alexithymia, which refers to difficulty identifying, describing, and regulating emotions. When emotional distress is poorly recognized or verbally expressed, it may be experienced and communicated through somatic channels. This mechanism is consistent with the broader internalizing model of psychopathology, in which anxiety, depression, helplessness, worry, and stress are expressed inwardly rather than through externalizing behaviors such as aggression, substance misuse, or antisocial conduct. Distinguishing internalizing from externalizing patterns may therefore help clinicians understand the dominant psychological profile of patients with somatic symptom and related disorders and tailor management accordingly.7,8
The Minnesota Multiphasic Personality Inventory-3 (MMPI-3) provides a contemporary, multidimensional assessment of psychopathology and personality functioning. Its scale structure allows simultaneous evaluation of higher-order emotional, thought, and behavioral dysfunction; somatic and cognitive complaints; internalizing and externalizing symptoms; interpersonal functioning; and personality psychopathology. This makes it particularly suitable for identifying broad psychological patterns in patients whose primary presentation is somatic. However, few studies have used the MMPI-3 to characterize somatic symptom and related disorders in Middle Eastern clinical populations.9
A detailed MMPI-3 profile may also have practical treatment implications. If patients with somatic symptom and related disorders show a predominantly internalizing profile, management may need to prioritize anxiety, hopelessness, emotional regulation, body-focused preoccupation, and suicide-risk monitoring rather than approaches directed mainly at externalizing behavior. Such profiling may support more individualized treatment planning and clarify the role of psychological interventions such as cognitive-behavioral therapy, acceptance-based therapy, and emotion-focused approaches.10–12
The present study aimed to characterize the psychopathological profile of Iranian patients with somatic symptom and related disorders using the MMPI-3. Specifically, the study addressed the following research questions:
- Do patients with somatic symptom and related disorders differ from population norms across MMPI-3 higher-order, clinical, somatic/cognitive, internalizing, externalizing, interpersonal, and personality psychopathology scales?
- Is the dominant MMPI-3 profile of this clinical group characterized primarily by internalizing distress and somatic-cognitive preoccupation rather than externalizing pathology?
- What treatment-relevant psychological targets can be inferred from the observed MMPI-3 profile?
We hypothesized that, compared with population norms, patients with somatic symptom and related disorders would show higher scores on emotional dysfunction, somatic/cognitive complaints, and internalizing scales, and lower or non-elevated scores on externalizing scales.
Methods
Study Design and Setting
This descriptive cross-sectional study was conducted at the psychosomatic department of Imam Khomeini Hospital, Sari, Iran, between May and September 2024. The study was designed to characterize the MMPI-3 psychopathological profile of patients diagnosed with somatic symptom and related disorders.
Participants and Sampling
Participants were recruited using convenience sampling from patients presenting to the psychosomatic department during the study period. The sampling frame consisted of 700 patients who attended the department between May and September 2024. After applying the inclusion and exclusion criteria and excluding patients with incomplete or invalid questionnaire data, 120 patients were included in the final analysis (Figure 1).
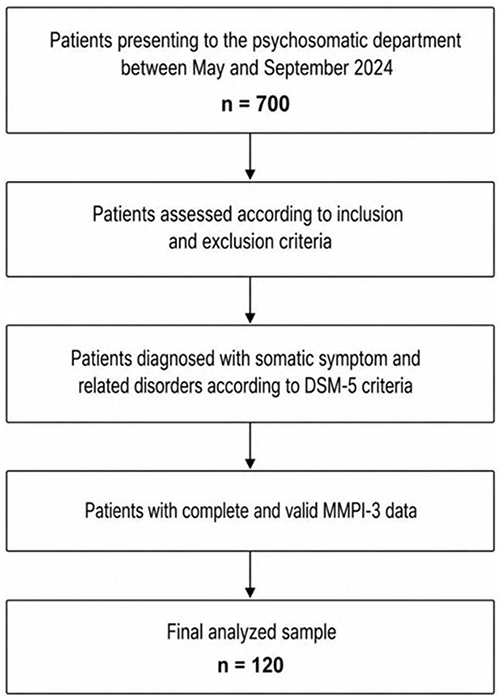 |
Figure 1 Participant selection flow diagram. The diagram shows the selection process for patients included in the final analysis. A total of 700 patients presented to the psychosomatic department during the study period. After applying the inclusion and exclusion criteria and retaining patients with complete and valid MMPI-3 data, 120 patients were included in the final analysis. Abbreviations: DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; MMPI-3, Minnesota Multiphasic Personality Inventory-3. |
Eligible participants were adults aged 18 to 65 years who had at least a middle-school level of education, were diagnosed with a somatic symptom or related disorder according to DSM-5 criteria by a psychiatrist, and provided written informed consent. The diagnostic categories included somatic symptom disorder, illness anxiety disorder, and conversion disorder/functional neurological symptom disorder. Patients were excluded if they had an acute unstable medical condition requiring urgent treatment, a severe psychiatric disorder such as psychotic disorder or bipolar disorder that substantially impaired cooperation with assessment, incomplete MMPI-3 data, invalid response patterns, or unwillingness to continue participation.
The final analyzed sample consisted of 120 patients, including 72 females and 48 males, with a mean age of 42.5 years. The age range was 19 to 65 years. Marital status and diagnostic characteristics are presented in Table 1.
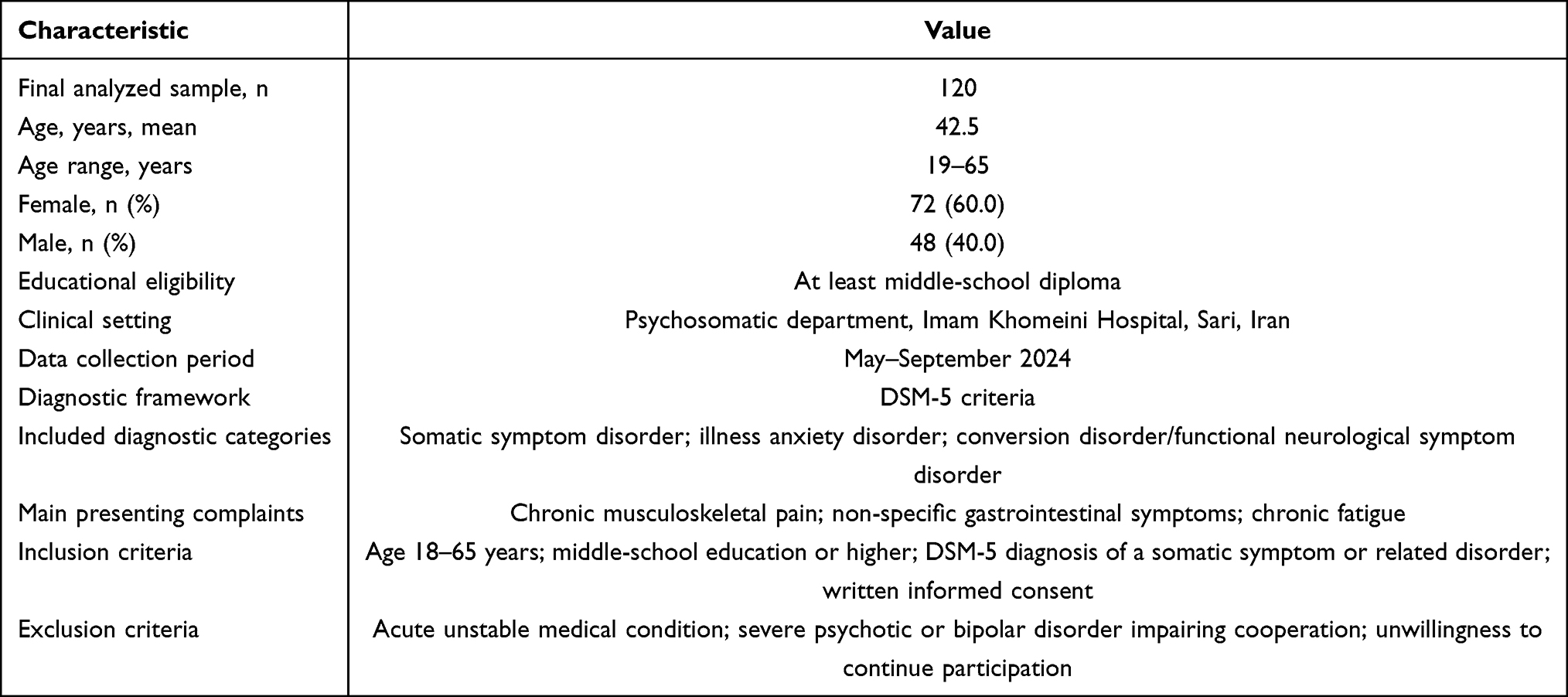 |
Table 1 Demographic and Clinical Characteristics of the Study Sample |
No formal a priori power analysis was performed before data collection. The target sample size was determined pragmatically based on the number of eligible patients with complete and valid MMPI-3 data during the study period. As a sensitivity estimate, a sample size of 120 provides approximately 80% power to detect a small-to-moderate one-sample effect size of Cohen’s d = 0.32 at a two-sided α level of 0.01. The absence of an a priori power analysis is acknowledged as a study limitation.
Procedure
Potential participants were identified through clinical referral and medical record review. Eligibility was determined according to the predefined inclusion and exclusion criteria. Patients who met the criteria were approached in the clinic, informed about the study aims, assured of confidentiality, and asked to provide written informed consent. Participants then completed the Minnesota Multiphasic Personality Inventory-3 under the supervision of trained research personnel.
Measure
The Minnesota Multiphasic Personality Inventory-3 is a 335-item self-report psychological assessment instrument designed to evaluate broad dimensions of psychopathology and personality functioning. Items are answered in a true/false format. The MMPI-3 includes validity scales and substantive scales assessing higher-order dysfunction, restructured clinical domains, somatic/cognitive complaints, internalizing symptoms, externalizing symptoms, interpersonal functioning, and personality psychopathology.
The MMPI-3 normative reference is based on adult population data and uses standardized T-scores with a normative mean of 50. In the present study, participants’ MMPI-3 scale scores were compared with the normative T-score mean of 50.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics, version 21. Descriptive statistics were calculated for demographic variables and MMPI-3 scale scores. Normality was assessed using the Kolmogorov–Smirnov test, skewness, and kurtosis values. Because the distributions were acceptable for parametric analysis, one-sample t-tests were used to compare MMPI-3 T-scores with the normative T-score mean of 50.
The primary unadjusted significance threshold was set at α = 0.01. Exact p-values were reported where possible, and values smaller than 0.001 were reported as p < 0.001. To improve interpretability beyond statistical significance, Cohen’s d effect sizes were calculated for each one-sample comparison using the formula d = t/√n, where n = 120. Positive values indicated scores above the normative mean, whereas negative values indicated scores below the normative mean.
To address multiple testing, Bonferroni correction was applied within each predefined MMPI-3 domain using the prespecified α = 0.01 threshold divided by the number of scales in that domain. The domain-specific Bonferroni thresholds were p < 0.0033 for higher-order scales, p < 0.00125 for restructured clinical scales, p < 0.0025 for somatic/cognitive complaint scales, p < 0.0010 for internalizing scales, p < 0.0014 for externalizing scales, p < 0.0020 for interpersonal functioning scales, and p < 0.0020 for personality psychopathology scales. The revised tables report Cohen’s d and indicate whether each finding remained significant after domain-wise Bonferroni correction. To avoid overloading the primary domain tables, Cohen’s d values and domain-wise Bonferroni-corrected interpretations are presented separately in Table 2.
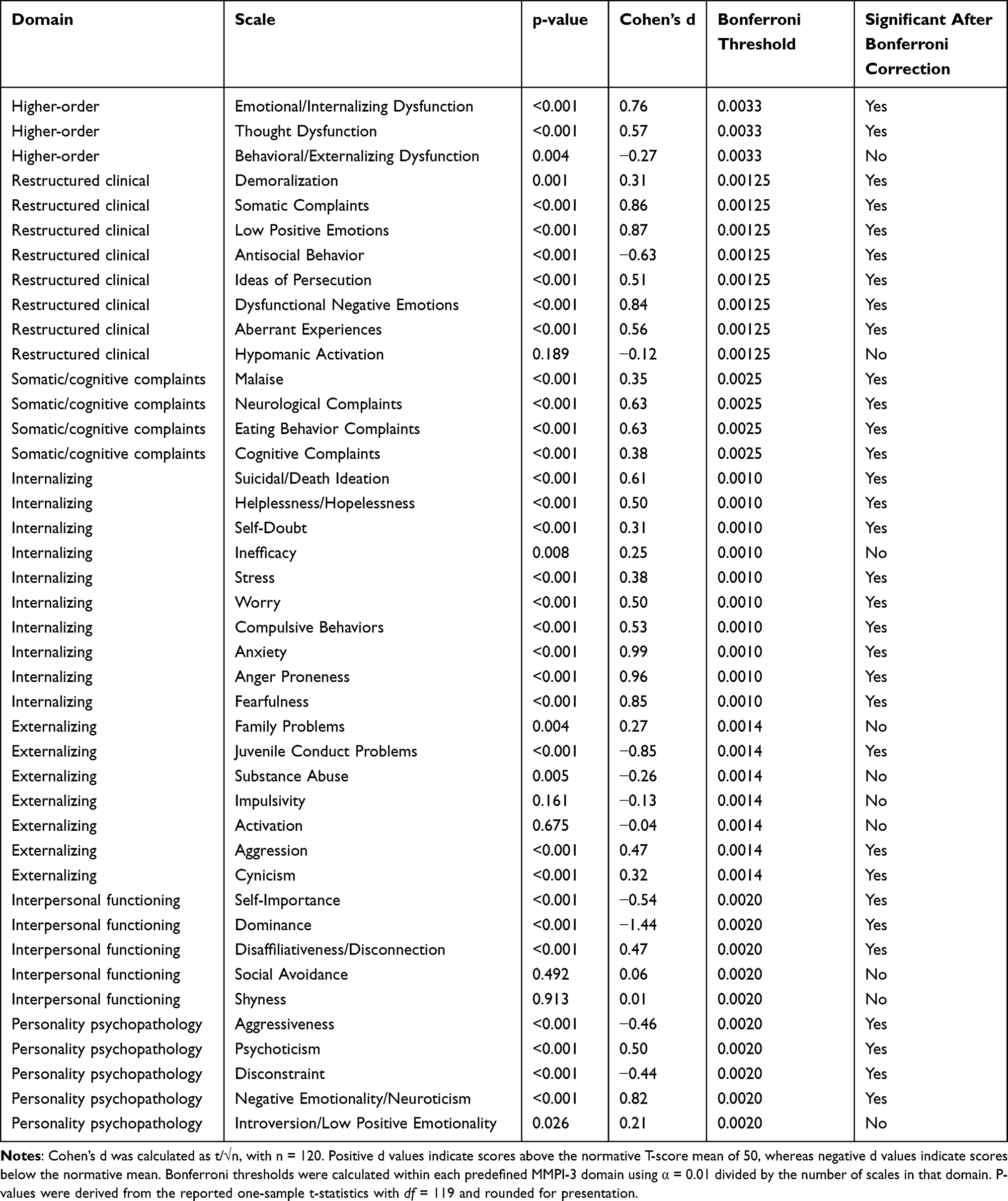 |
Table 2 Effect Sizes and Bonferroni-Corrected Interpretation of MMPI-3 Scale Comparisons |
Results
The final analyzed sample included 120 patients with somatic symptom and related disorders. Demographic and clinical characteristics of the sample are summarized in Table 1.
Descriptive assessment of the MMPI-3 scale distributions showed acceptable normality for parametric analysis. Across the higher-order, restructured clinical, somatic/cognitive, internalizing, externalizing, interpersonal, and personality psychopathology domains, skewness and kurtosis values were within acceptable limits. Therefore, one-sample t-tests were used to compare patient MMPI-3 T-scores with the normative population mean of 50 (Figure 2).
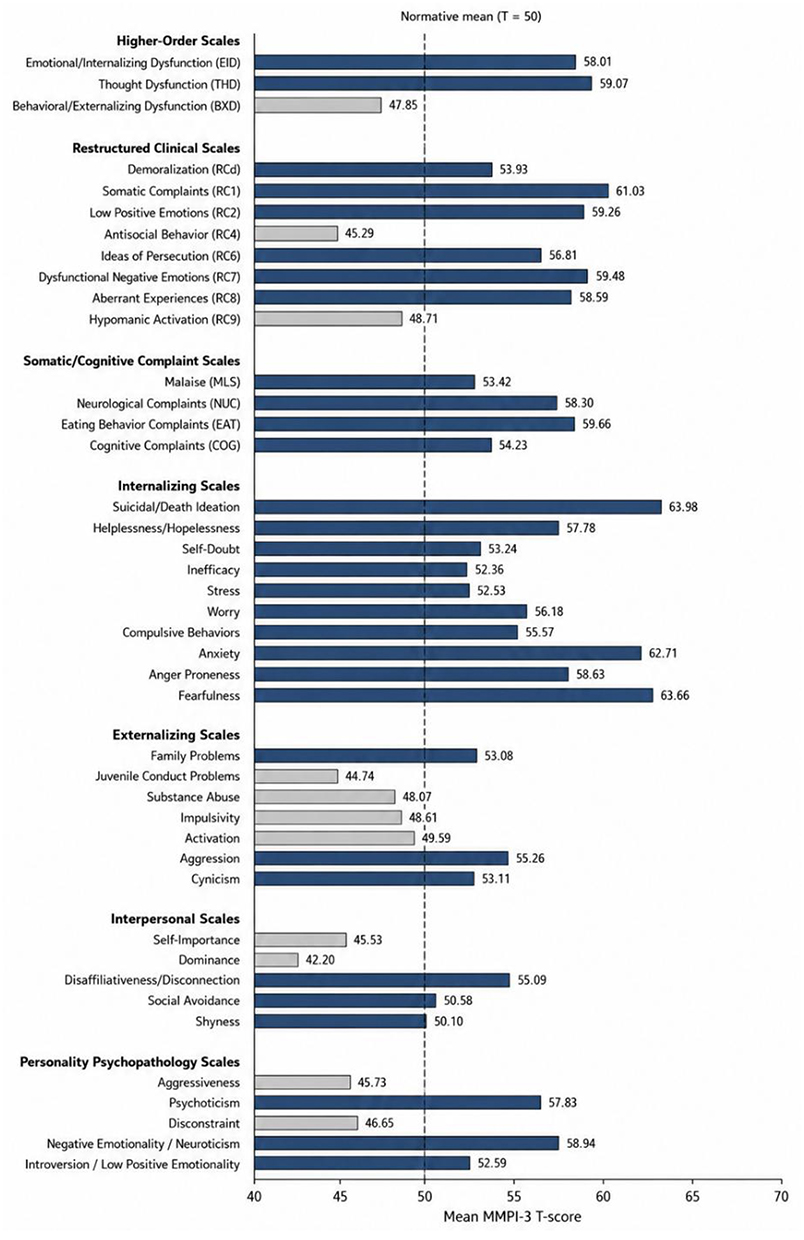 |
Figure 2 MMPI-3 profile of patients with somatic symptom and related disorders. The figure displays mean MMPI-3 T-scores across the analyzed clinical scales. The dashed reference line represents the normative T-score mean of 50. Scores above 50 indicate elevations relative to the normative mean, whereas scores below 50 indicate lower scores relative to the normative mean. |
On the higher-order scales, patients scored significantly above the normative mean on Emotional/Internalizing Dysfunction and Thought Dysfunction, indicating greater emotional distress and thought-related dysfunction. Behavioral/Externalizing Dysfunction was lower than the normative mean at the unadjusted α = 0.01 threshold, although this finding did not remain significant after domain-wise Bonferroni correction (Table 3).
 |
Table 3 Comparison of Higher-Order Deficiency Scale Scores Between Patients with Psychosomatic Disorders and Population Norms |
On the restructured clinical scales, significant elevations were observed for Demoralization, Somatic Complaints, Low Positive Emotions, Ideas of Persecution, Dysfunctional Negative Emotions, and Aberrant Experiences. Antisocial Behavior was significantly lower than the normative mean, whereas Hypomanic Activation did not differ significantly from the normative mean. These findings indicate a profile marked by demoralization, somatic preoccupation, negative affect, and unusual perceptual or thought experiences, rather than antisocial or hypomanic features (Table 4).
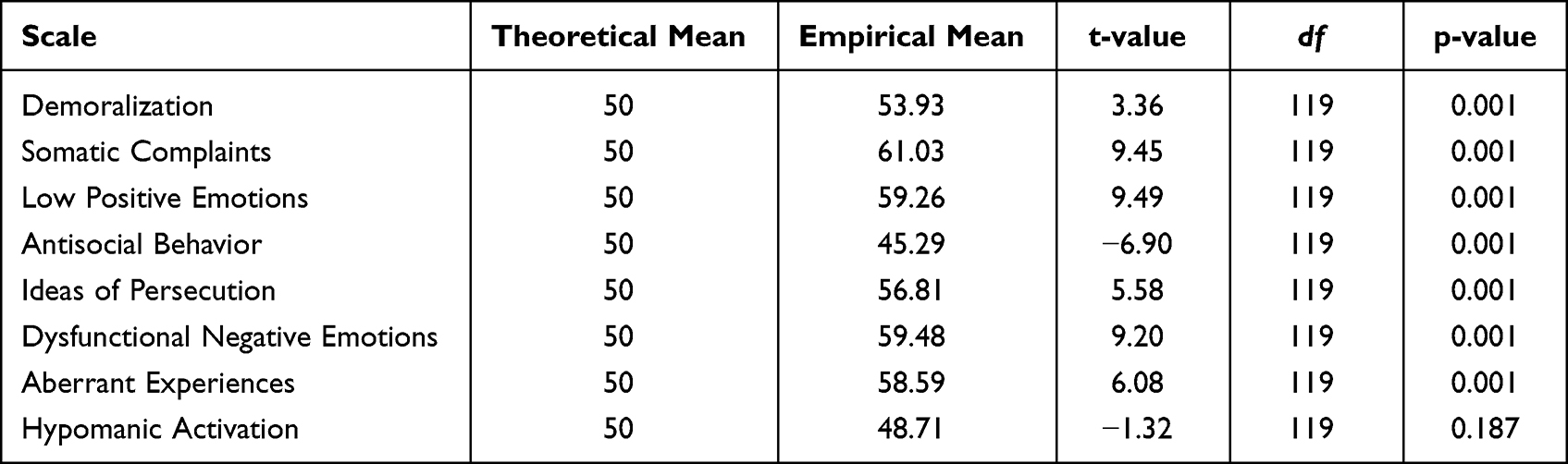 |
Table 4 Scores on Restructured Clinical Scales (MMPI-3) in Patients with Psychosomatic Disorders |
All somatic/cognitive complaint scales were significantly elevated compared with the normative mean. These included Malaise, Neurological Complaints, Eating Behavior Complaints, and Cognitive Complaints. This pattern supports the central role of bodily and cognitive symptom preoccupation in the clinical presentation of this group (Table 5).
 |
Table 5 Somatic and Cognitive Complaint Scale Scores in the Study Sample |
Within the internalizing domain, patients showed significant elevations on Suicidal/Death Ideation, Helplessness/Hopelessness, Self-Doubt, Stress, Worry, Compulsive Behaviors, Anxiety, Anger Proneness, and Fearfulness. Inefficacy showed a smaller elevation and should be interpreted cautiously after correction for multiple comparisons. Overall, the internalizing profile was dominated by anxiety, fearfulness, anger proneness, hopelessness, and suicide-related ideation (Table 6).
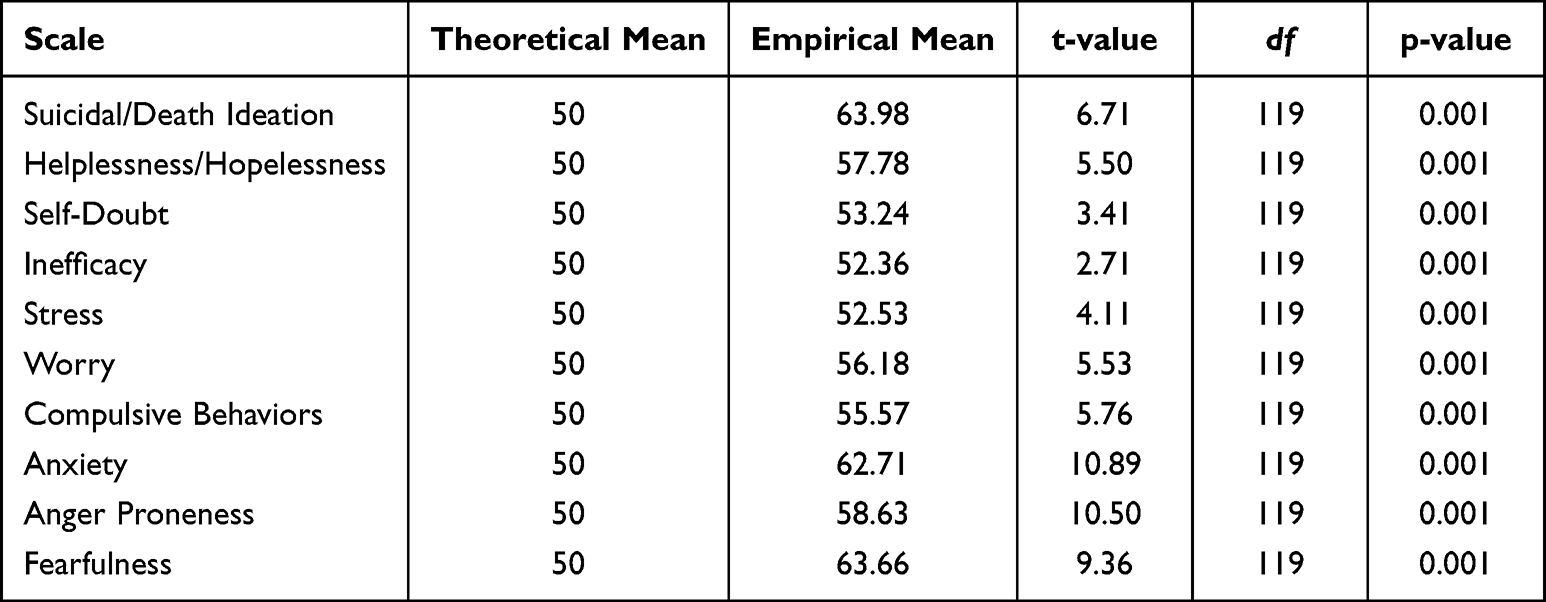 |
Table 6 Internalizing Scale Scores in Patients with Psychosomatic Disorders |
In the externalizing domain, Aggression and Cynicism remained significantly elevated after Bonferroni correction, whereas Family Problems showed only an unadjusted elevation. Juvenile Conduct Problems remained significantly lower than the normative mean after correction, whereas Substance Abuse showed only an unadjusted reduction. Impulsivity and Activation did not differ significantly from normative values. This pattern suggests that although interpersonal conflict, anger, and cynical attitudes were present, broader externalizing behaviors such as substance misuse, conduct problems, and impulsivity were not prominent (Table 7).
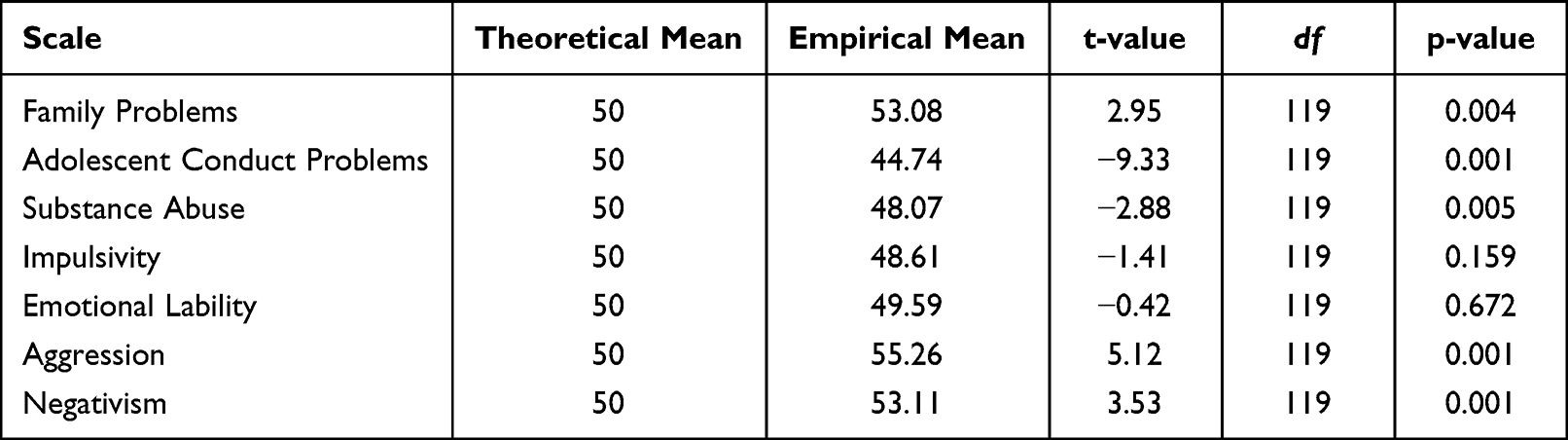 |
Table 7 Externalizing Scale Scores in Patients with Psychosomatic Disorders |
On interpersonal functioning scales, Self-Importance and Dominance were significantly below the normative mean, whereas Disaffiliativeness/Disconnection was significantly elevated. Social Avoidance and Shyness did not differ significantly from normative values. This pattern suggests reduced dominance and interpersonal withdrawal/disconnection without a clear elevation in shyness or social avoidance (Table 8).
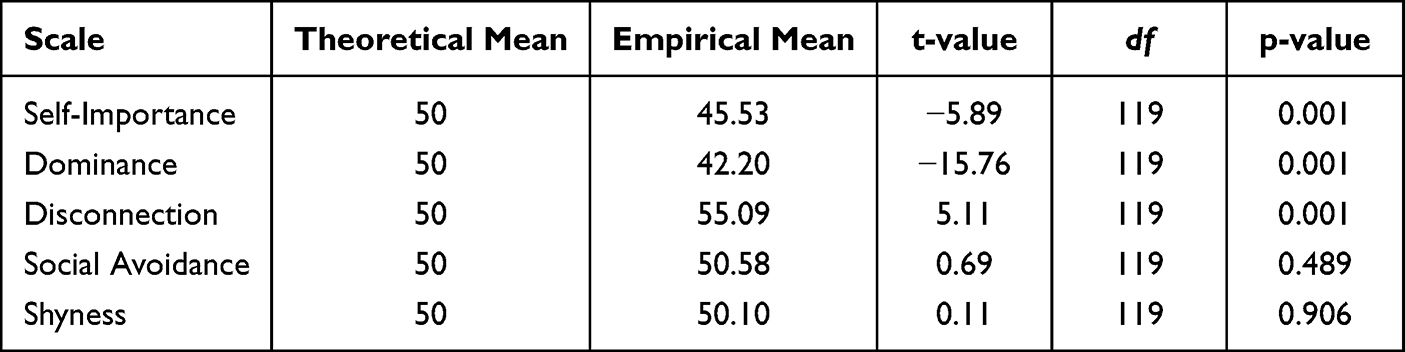 |
Table 8 Interpersonal Functioning Scale Scores in the Clinical Sample |
On personality psychopathology scales, Psychoticism and Negative Emotionality/Neuroticism were significantly elevated, whereas Aggressiveness and Disconstraint were significantly lower than normative values. Introversion/Low Positive Emotionality showed only a small elevation and did not remain significant using the primary α = 0.01 threshold. Taken together, the personality psychopathology profile was characterized by negative emotionality and unusual experiences, with comparatively reduced externalizing personality features (Table 9).
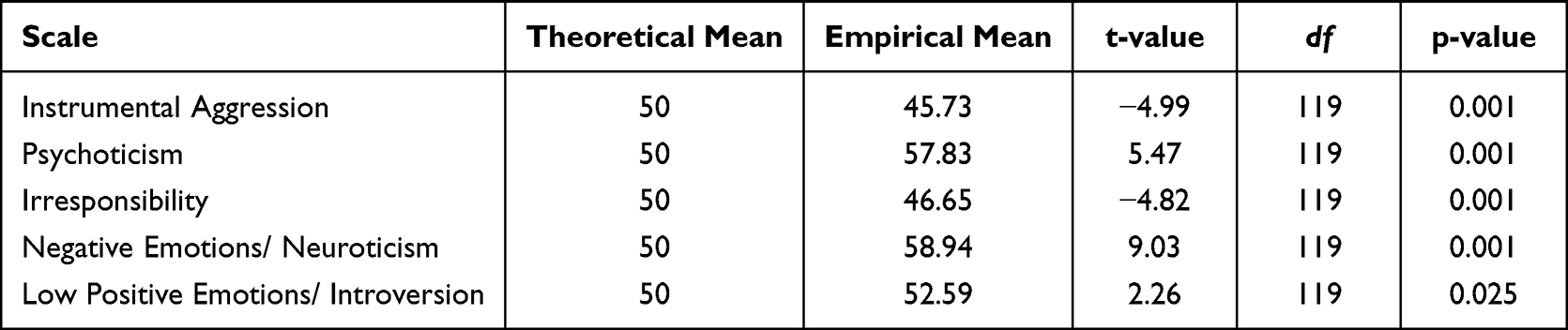 |
Table 9 Personality Psychopathology Scale Profiles of Patients with Psychosomatic Disorders |
Overall, the MMPI-3 profile of patients with somatic symptom and related disorders was characterized by elevated emotional distress, somatic/cognitive complaints, internalizing symptoms, negative emotionality, and reduced externalizing pathology. The strongest elevations were observed in anxiety, anger proneness, fearfulness, somatic complaints, low positive emotions, and dysfunctional negative emotions. These findings support the hypothesis that this clinical group demonstrates a predominantly internalizing psychopathological profile (Tables 1–9).
Discussion
This study characterized the MMPI-3 psychopathological profile of Iranian patients with somatic symptom and related disorders. The main finding was a predominantly internalizing profile, marked by elevations in emotional/internalizing dysfunction, somatic and cognitive complaints, anxiety, fearfulness, anger proneness, helplessness/hopelessness, suicidal/death ideation, psychoticism, and negative emotionality/neuroticism. In contrast, several externalizing dimensions, including behavioral/externalizing dysfunction, antisocial behavior, juvenile conduct problems, substance abuse, aggressiveness, and disconstraint, were below normative values. Taken together, these findings suggest that the psychopathological expression of somatic symptom and related disorders in this sample was driven more by internalized distress, somatic-cognitive preoccupation, and negative affect than by overt externalizing behavior.
The elevated somatic/cognitive complaint scales are consistent with the clinical definition of somatic symptom and related disorders, in which bodily symptoms are accompanied by persistent health-related concern, distress, and functional impairment. The observed elevations in malaise, neurological complaints, eating behavior complaints, and cognitive complaints suggest that symptom burden in this population extends beyond isolated physical discomfort and involves broader cognitive and bodily preoccupation. This pattern supports the need for assessment models that evaluate both physical complaints and the psychological processes that maintain or amplify them.13
The strong internalizing profile is clinically important. Elevations in anxiety, fearfulness, worry, stress, helplessness/hopelessness, and suicidal/death ideation indicate that patients with somatic symptom and related disorders may experience substantial inwardly directed emotional distress. These findings are consistent with models in which unprocessed or poorly regulated emotional distress is expressed through bodily symptoms. They also support the relevance of alexithymia, emotional avoidance, health anxiety, and catastrophic interpretation of bodily sensations as potential mechanisms contributing to symptom persistence. The elevation of suicidal/death ideation is particularly important and suggests that suicide-risk screening should not be overlooked in patients whose primary presentation is somatic.
The contrast between elevated internalizing scales and reduced externalizing scales provides a useful clinical distinction. Patients did not show a broad pattern of antisocial behavior, substance abuse, conduct problems, impulsivity, or hypomanic activation. Instead, their profile suggested emotional constriction, distress, and bodily preoccupation. This distinction may help clinicians avoid misinterpreting these patients as primarily behaviorally dysregulated and instead direct attention toward anxiety, hopelessness, affect regulation, and health-related cognitive patterns.
The personality psychopathology findings further support this interpretation. Elevated negative emotionality/neuroticism suggests a tendency toward distress sensitivity and persistent negative affect. Elevated psychoticism should not be interpreted as evidence of psychotic disorder in this context; rather, it may reflect unusual experiences, detachment, or atypical interpretations of bodily sensations in patients with severe somatic preoccupation. Lower aggressiveness and disconstraint are consistent with the broader finding that externalizing personality features were not dominant in this sample.
The Iranian context may also shape the presentation and reporting of symptoms. In many settings, psychological distress may be more socially acceptable when expressed through physical symptoms than through direct emotional disclosure. Cultural expectations, stigma surrounding psychiatric symptoms, family roles, gender norms, and patterns of healthcare access may all influence how patients describe distress and seek care. Therefore, somatic presentations in Iranian clinical settings should be understood not only as individual psychopathology but also as expressions shaped by sociocultural context. This reinforces the value of culturally informed assessment and management.14–16
From a treatment perspective, the identified profile supports a stepped and integrated approach. Cognitive-behavioral therapy may help patients identify catastrophic health beliefs, reduce reassurance-seeking, and modify maladaptive interpretations of bodily sensations. Acceptance and commitment therapy may be useful for reducing experiential avoidance and improving psychological flexibility. Emotion-focused and dynamic approaches may be beneficial when emotional awareness and expression are limited. Given the elevation in suicidal/death ideation and helplessness/hopelessness, structured suicide-risk monitoring should be included in clinical management, even when patients present primarily with physical complaints.
Several alternative explanations should be considered. First, physical symptom burden itself may increase anxiety, hopelessness, and cognitive complaints, meaning that the observed psychological profile may be both a contributor to and a consequence of chronic somatic symptoms. Second, unmeasured factors such as pain severity, duration of illness, comorbid depression or anxiety disorders, medication use, socioeconomic stress, and previous healthcare experiences may influence MMPI-3 scores. Third, the clinical setting may have selected for patients with more severe or persistent symptoms than those seen in community settings.11,17,18
Limitations
This study has several limitations
- The cross-sectional design prevents causal interpretation. The findings show associations between somatic symptom and related disorders and MMPI-3 profile elevations, but they cannot determine whether psychological distress preceded, followed, or developed alongside somatic symptoms.
- The study used a single clinical site in Sari, Iran. Therefore, the findings may not be fully generalizable to other regions, healthcare settings, or community samples.
- The sample was based on patients who presented to a psychosomatic clinic, which may overrepresent individuals with more persistent, complex, or treatment-seeking symptoms.
- The study compared MMPI-3 scores with normative T-score values rather than with a matched clinical or healthy control group. Future studies should include matched comparison groups to strengthen causal and diagnostic interpretation.
- Potential confounding factors, including symptom duration, pain severity, medication use, psychiatric comorbidity, socioeconomic status, and treatment history, were not fully examined. Future research should include these variables to clarify predictors of MMPI-3 profile variation.
- The study relied on self-report psychometric assessment. Although the MMPI-3 is a comprehensive and standardized instrument, self-report responses may be influenced by insight, response style, distress level, and cultural factors.
Despite these limitations, the study provides one of the first MMPI-3-based profiles of Iranian patients with somatic symptom and related disorders and highlights a clinically meaningful internalizing pattern with direct implications for assessment and treatment planning.
Conclusion
This cross-sectional MMPI-3 study identified a predominantly internalizing psychopathological profile in Iranian patients with somatic symptom and related disorders. The profile was characterized by elevated emotional distress, somatic-cognitive complaints, anxiety, fearfulness, hopelessness, suicidal/death ideation, and negative emotionality, together with reduced externalizing features such as antisocial behavior, substance abuse, aggressiveness, and disconstraint.
These findings suggest that clinical assessment and management of somatic symptom and related disorders should extend beyond physical complaints and include structured evaluation of internalizing distress, body-focused preoccupation, emotional regulation difficulties, and suicide risk. Future studies using longitudinal designs and matched comparison groups are needed to clarify the stability, predictors, and treatment relevance of this MMPI-3 profile.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to participant confidentiality, but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Islamic Azad University, Sari Branch (IR.IAU.SARI.REC.1403.228). Written informed consent was obtained from all individual participants included in the study. The study procedures were conducted in accordance with the ethical principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for conducting this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Löwe B, Toussaint A, Rosmalen JGM, et al. Persistent physical symptoms: definition, genesis, and management. Lancet. 2024;403(10444):2649–12. doi:10.1016/S0140-6736(24)00623-8
2. Henningsen P. Management of somatic symptom disorder. Dialogues Clin. Neurosci. 2018;20(1):23–31. doi:10.31887/DCNS.2018.20.1/phenningsen
3. D’Souza RS, Hooten WM. Somatic Symptom Disorder. StatPearls. Treasure Island (FL): StatPearls Publishing LLC.; 2026. Copyright © 2026.
4. Ferrari AJ, Santomauro DF, Mantilla Herrera AM, et al. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. 2022;9(2):137–150. doi:10.1016/S2215-0366(21)00395-3
5. Fan Y, Fan A, Yang Z, Fan D. Global burden of mental disorders in 204 countries and territories, 1990–2021: results from the global burden of disease study 2021. BMC Psychiatry. 2025;25(1):486. doi:10.1186/s12888-025-06932-y
6. Al Busaidi ZQ. The Concept of Somatisation: a Cross-cultural perspective. Sultan Qaboos Univ Med J. 2010;10(2):180–186. doi:10.18295/2075-0528.1184
7. Taylor GJ, Porcelli P, Bagby RM. Alexithymia: a defense of the original conceptualization of the construct and a critique of the attention-appraisal model. Clin Neuropsychiatry. 2024;21(5):329–357. doi:10.36131/cnfioritieditore20240501
8. Preece DA, Gross JJ. Defining alexithymia: the clinical relevance of cognitive behavioral vs psychoanalytic conceptualizations. Pers Individ Dif. 2024;228:112732. doi:10.1016/j.paid.2024.112732
9. Corey DM, Ben-Porath YS. Minnesota Multiphasic Personality Inventory-3. MMPI-3): user’s guide for the public safety candidate interpretive reports. University of. Minnesota Press; 2022.
10. Liu X, He M, Wang W, et al. Personality profile of the primary blepharospasm (BSP): an investigation using the Minnesota Multiphasic Personality Inventory. Neurosci Lett. 2020;722:134821. doi:10.1016/j.neulet.2020.134821
11. Smakowski A, Hüsing P, Völcker S, et al. Psychological risk factors of somatic symptom disorder: a systematic review and meta-analysis of cross-sectional and longitudinal studies. J Psychosom Res. 2024;181:111608. doi:10.1016/j.jpsychores.2024.111608
12. Hsu JW, Lin WC, Tsai SJ, et al. Somatic symptom disorder, psychiatric comorbidities, and suicide. J Affect Disord. 2025;373:459–464. doi:10.1016/j.jad.2024.12.105
13. Pearson assessments. Minneapolis, MN: Pearson. 2020. MMPI-3 Scales. Available from: https://www.pearsonassessments.com/content/dam/school/global/clinical/us/assets/mmpi-3/mmpi-3scales.pdf.
14. Jafari A, Nejatian M, Momeniyan V, Barsalani FR, Tehrani H. Mental health literacy and quality of life in Iran: a cross-sectional study. BMC Psychiatry. 2021;21(1):499. doi:10.1186/s12888-021-03507-5
15. Elshamy F, Hamadeh A, Billings J, Alyafei A. Mental illness and help-seeking behaviours among Middle Eastern cultures: a systematic review and meta-synthesis of qualitative data. PLoS One. 2023;18(10):e0293525. doi:10.1371/journal.pone.0293525
16. Taghva A, Farsi Z, Javanmard Y, Atashi A, Hajebi A, Khademi M. Stigma barriers of mental health in Iran: a qualitative study by stakeholders of mental health. Iran J Psychiatry. 2017;12(3):163–171.
17. Hybelius J, Kosic A, Salomonsson S, et al. Measurement properties of the patient health questionnaire–15 and somatic symptom scale–8: a systematic review and meta-analysis. JAMA Netw Open. 2024;7(11):e2446603–e. doi:10.1001/jamanetworkopen.2024.46603
18. Lehmann M, Pohontsch NJ, Zimmermann T, Scherer M, Löwe B. Diagnostic and treatment barriers to persistent somatic symptoms in primary care – representative survey with physicians. BMC Fam. Prac. 2021;22(1):60. doi:10.1186/s12875-021-01397-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.