Back to Journals » Drug Design, Development and Therapy » Volume 20
Mivacurium Infusion ED50/ED95 for Maintaining Motor Evoked Potentials During Adolescent Scoliosis Surgery Under TIVA: A Modified Dixon Up-and-Down Sequential Dose-Finding Study
Authors Zhang Y, Zhang S, Wei H ![]() , Li Z, Qin H, Yuan H, Jiang X
, Li Z, Qin H, Yuan H, Jiang X ![]()
Received 21 November 2025
Accepted for publication 29 April 2026
Published 8 June 2026 Volume 2026:20 581844
DOI https://doi.org/10.2147/DDDT.S581844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tamer Ibrahim
Yixuan Zhang,1,* Shuhan Zhang,1,* Huawei Wei,1,* Zhenjie Li,1 Hong Qin,2 Hongbin Yuan,1 Xin Jiang1
1Department of Anesthesiology, Second Affiliated Hospital of Naval Medical University, Shanghai, People’s Republic of China; 2Department of Orthopedics, Second Affiliated Hospital of Naval Medical University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongbin Yuan, Department of Anesthesiology, Second Affiliated Hospital of Naval Medical University, Shanghai, 200003, People’s Republic of China, Tel +86 21 81885822, Email [email protected] Xin Jiang, Department of Anesthesiology, Second Affiliated Hospital of Naval Medical University, Shanghai, 200003, People’s Republic of China, Tel +86 21 81885826, Email [email protected]
Purpose: This study aimed to determine the median effective dose (ED50) and 95% effective dose (ED95) of mivacurium for maintaining elicitable motor evoked potentials (MEP) under total intravenous anesthesia (TIVA) during adolescent scoliosis surgery, while fulfilling both muscle relaxation and intraoperative neurophysiological monitoring (IONM) requirements.
Patients and Methods: 26 adolescents scheduled for primary elective scoliosis surgery with MEP monitoring were enrolled. Anesthesia was maintained with TCI propofol to achieve BIS of 40– 60. Infusing mivacurium to maintain train-of-four count 1– 3 until surgical exposure was completed. After train-of-four ratio recovered to 75% and MEP waveforms were elicitable, modified Dixon up-and-down sequential method was employed, with an initial mivacurium infusion dose of 10 μg·kg− 1·min− 1, adjusted by 0.5 μg·kg− 1·min− 1 based on the presence or absence of reproducible MEP at predefined stimulation settings. Positive was defined as reproducible MEP waveform elicitable at a stimulus intensity of 100 V. Dose-finding proceeded until seven crossover pairs were obtained. Excluding cases prior to the first crossover, 21 patients contributed to ED estimation. Hemodynamic parameters, adverse reactions, vasoactive agents use, and L-SRS scores were recorded.
Results: The ED50 was 7.24 μg·kg− 1·min− 1 (95% CI: 6.87– 7.54). The probability of MEP waveform presence demonstrated a negative correlation with mivacurium infusion dose, with an ED95 of 6.70 μg·kg− 1·min− 1 (95% CI: 4.79– 6.99). No patients experienced unintended body movements, spontaneous respiration recovery, or bronchospasm. No significant hemodynamic changes were observed after mivacurium administration. Transient skin flushing occurred in 6 patients, and low-dose ephedrine was required in 7 patients. L-SRS scores were higher during mivacurium infusion compared to post-discontinuation.
Conclusion: Under this TIVA/IONM protocol, the ED50 and ED95 for continuous mivacurium infusion that preserves MEP are 7.24 μg·kg− 1·min− 1 and 6.70 μg·kg− 1·min− 1, respectively. These doses effectively achieve muscle relaxation while maintaining MEP signals without serious adverse events observed.
Plain Language Summary: While adolescent scoliosis surgery requires adequate muscle relaxation for surgical conditions, excessive neuromuscular blockade may compromise intraoperative neurophysiological monitoring (IONM), particularly motor evoked potentials (MEP). This study investigated the appropriate infusion dose of mivacurium that maintains both sufficient muscle relaxation and elicitable MEP signals in adolescent patients undergoing scoliosis surgery. Using the modified Dixon up-and-down sequential method and Probit analysis, researchers estimated the median effective dose (ED50) and 95% effective dose (ED95) of continuous mivacurium infusion. The results demonstrate that an ED50 of 7.24 μg·kg− 1·min− 1 effectively balances surgical requirements with MEP monitoring, with 95% of patients achieving maintainable MEP waveforms at 6.70 μg·kg− 1·min− 1. No serious adverse events were observed, and hemodynamic parameters remained stable throughout the procedure.
Keywords: mivacurium, intraoperative neurophysiological monitoring, motor evoked potentials, adolescent scoliosis surgery, total intravenous anesthesia
Introduction
Scoliosis is characterized by an abnormal three-dimensional configuration and/or developmental irregularity of the spine. Compared with conventional spinal surgical procedures, scoliosis surgeries, which involve techniques such as pedicle screw placement, osteotomy, and spinal correction, present a higher risk of perioperative nerve injury. Such injuries significantly affect patient prognosis and are considered among the most critical perioperative complications.1 Intraoperative neurophysiological monitoring (IONM) is essential for safeguarding nerve function during scoliosis surgery.2 Motor evoked potentials (MEP) waveforms are highly sensitive to nerve injury. Even minor nerve injury can cause a sharp decline in amplitude, typically manifested as disappearance of MEP waveforms at the same stimulation intensity (setting range: 100–500 V), which serves as the primary indicator.3 Therefore, the disappearance of MEP waveforms due to surgical manipulation can provide timely warning of functional impairment in the spinal motor pathways, facilitating the identification and mitigation of factors contributing to nerve injury, and reducing the risk of postoperative motor dysfunction.4
Neuromuscular blocking agents (NMBAs) selectively inhibit neuromuscular transmission to induce muscle relaxation, however, they may also reduce MEP amplitude. Excessive neuromuscular blockade can result in disappearance of the MEP waveform, despite the absence of any nerve function abnormalities, thereby compromising neuromonitoring.5 Consequently, neurophysiological monitoring physicians often prefer to avoid the administration of additional NMBAs during surgery.6 Nonetheless, limiting the use of NMBAs can increase the risk of adverse events, such as muscle tremors, restricted surgical field visibility, increased blood loss, and potential injury to important neural or vascular structures due to unexpected patient movement, which contradicts the original purpose of neuroprotection through IONM.7 Previous studies have demonstrated that the continuous infusion of specific NMBA doses can facilitate the normal implementation of IONM, mitigate adverse reactions associated with muscle tension, and stabilize monitoring signals during IONM-assisted surgeries.8 However, the optimal depth of neuromuscular blockade and the appropriate dosage of NMBAs remain controversial. Existing findings vary across studies, including maintenance of train-of-four ratio (TOFr) at 26–50%, T1/TC at 10–15%, T2/TC at 50%, rocuronium infusion at 5 μg·kg−1·min−1, and rocuronium infusion at 9 μg·kg−1·min−1.9–13 These discrepancies may be related to differences in MEP criteria, surgical types, anesthesia management, and patient populations. Currently, there is insufficient research on the optimal NMBA dosage for adolescent scoliosis patients undergoing routine IONM-assisted surgery.
Mivacurium is the sole short-acting non-depolarizing NMBA currently utilized in clinical practice, while rocuronium has a specific antagonist (sugammadex). Both agents can restore muscle strength in a short time when needed during surgery.14,15 The probability of MEP waveform presence is negatively correlated with NMBA infusion dose and positively correlated with stimulation intensity. Therefore, in previous studies, we determined that under total intravenous anesthesia (TIVA) with 100 V stimulation intensity, the median effective dose (ED50) and 95% effective dose (ED95) of rocuronium for maintaining MEP waveforms were 8.69 μg·kg−1·min−1 and 7.51 μg·kg−1·min−1, respectively, which is also applicable to higher stimulation intensities.16 The second part of the trial also employed the modified Dixon up-and-down sequential method to precisely determine the appropriate infusion dose of mivacurium for IONM and to evaluate its intraoperative application. The determination of appropriate infusion doses for both rocuronium and mivacurium offers expanded therapeutic options for neuromuscular blockade management in adolescent scoliosis surgery, thereby optimizing perioperative care.
Materials and Methods
Ethics and Registration
This trial was approved by the Ethics Committee of the Second Affiliated Hospital of Naval Medical University with the ethics approval number 2023SL048. It was registered in the Chinese Clinical Trial Registry under the registration number ChiCTR2400082163. Conducted between January 2025 and August 2025, the study included a total of 26 adolescent patients, aged 12 to 18 years, scheduled for elective scoliosis surgery. Informed consent was obtained from both the subjects and their guardians. The research team affirms that the study adhered strictly to ethical standards and the principles outlined in the Declaration of Helsinki.
Protocol Deviations/Amendments
This trial was progressively implemented after successful registration with the Chinese Clinical Trial Registry on March 22, 2024. The study was delayed due to several factors: adolescent scoliosis surgery in China is predominantly performed during school vacation periods (December to February and June to August annually), and there was a temporary shortage of mivacurium in China due to the international trade environment. During this period, we took the opportunity to optimize the trial, including modifying the predefined execution and recruitment period ending from March 2025 to August 2025, as well as revising the broadly described primary outcome to a more precise statement: “the dosage of rocuronium or mivacurium and the corresponding changes in MEP waveforms”. These modifications did not affect the final research results. After obtaining Ethics Committee approval for the trial update on May 2, 2024, the appropriate infusion dose of rocuronium for this type of surgery was determined from May to December 2024 (with the results published in the Chinese top-tier anesthesiology journal, Journal of Clinical Anesthesiology), and the appropriate infusion dose of mivacurium was determined from January to August 2025. Following trial completion, the trial status and related content have been updated in the Chinese Clinical Trial Registry.
Participants and Inclusion Criteria
Inclusion criteria for the study are as follows: (1) Participants aged between 12 and 18 years; (2) Individuals classified as American Society of Anesthesiologists (ASA) status I–II; (3) Participants scheduled to undergo elective surgery for scoliosis with IONM; (4) Participants and their legal guardians have provided informed consent.
Exclusion criteria include: (1) Presence of severe cardiovascular and cerebrovascular diseases; (2) Severe pulmonary diseases or a history of asthma; (3) Severe hepatic or renal dysfunction; (4) Neuromuscular disorders; (5) Limb muscle strength graded at 2 or below; (6) Allergy to mivacurium; (7) Abnormal butyrylcholinesterase (BChE) levels; (8) Skin breakage at the neuromuscular monitoring or IONM site within 3 months; (9) Body Mass Index (BMI) greater than 28 kg/m2 or less than 18.5 kg/m2; (10) Contraindications for MEP monitoring, including conditions such as epilepsy, presence of pacemakers, cochlear implants, etc.
Cases may be eliminated if: (1) The mivacurium dosage is not administered according to the intraoperative sequential method; (2) Participants or their legal guardians request withdrawal from the study.
Study Procedure
Upon admission to the operating room, monitoring of the electrocardiogram (ECG), oxygen saturation (SpO2), and bispectral index (BIS) was initiated. Neuromuscular monitoring was facilitated using the Mindray plug-in neuromuscular monitoring module. Two intravenous lines were established: one dedicated to the administration of lactated Ringer’s solution and mivacurium, and the other allocated for additional fluids and anesthetic agents. Radial artery catheterization was performed under local anesthesia to enable the monitoring of invasive blood pressure (IBP).
Induction period: All patients received pure oxygen via mask. Subsequently, an intravenous injection of dexamethasone (5 mg) and lidocaine (40 mg) was administered, followed by a target-controlled infusion (TCI) of propofol at a concentration of 4 μg/mL. Train-of-four (TOF) stimulation monitoring was initiated once the BIS was below 60, with parameters set at a frequency of 2 Hz, a pulse width of 200 μs, a current intensity of 50 mA, and an interval of 1 minute. Sufentanil was administered intravenously at a dose of 0.5 μg/kg, and mivacurium was injected slowly at a dose of 0.2 mg/kg over approximately 30 seconds. Endotracheal intubation and controlled ventilation were performed when TOF reached 0. Following patient positioning, the neurophysiological monitoring physician commenced combined somatosensory evoked potentials (SEP) and MEP monitoring. MEP stimulation electrodes were positioned at the standard electrode sites C3 and C4, as per the 10–20 system of electroencephalography. Stimulation parameters included five trains of square wave pulses, with a stimulation duration of 0.5 ms, a pulse interval of 2 ms, and an initial voltage of 100 V. It was necessary to determine whether the voltage could be appropriately increased in the event of nerve injury, with a maximum stimulation voltage of 500 V. Recording electrodes were placed on the adductor hallucis of the lower limbs to capture the peripheral compound muscle action potentials.
Maintenance period: The TCI of propofol was maintained at a concentration of 2 to 6 μg/mL to achieve a BIS of 40 to 60. If the BIS exceeded 60 or fell below 40 for more than one minute, the infusion rate was adjusted by increasing or decreasing the dose by 0.5 μg/mL, respectively. TCI remifentanil was administered at a concentration of 2 to 4 ng/mL, with dosages of remifentanil and sufentanil adjusted based on changes in mean arterial pressure (MAP) and heart rate (HR) to ensure adequate analgesia. Following intubation, mivacurium was infused to sustain moderate neuromuscular blockade, indicated by a train-of-four count (TOFc) of 1 to 3, until the surgical exposure was completed. Once TOFr recovered to 75% and MEP waveform could be elicited, mivacurium was administered according to the sequential method, and MEP monitoring was conducted every 20 minutes until the incision closure began. During MEP monitoring, if surgery renders monitoring unsuitable, the monitoring interval may be appropriately postponed. If nerve injury was suspected, the monitoring frequency may be increased as needed. Throughout the operation, MAP and HR were maintained within a 20% range of baseline values, and body temperature was kept between 36.0 and 36.9 °C. The infusion of mivacurium and propofol continued until the subcutaneous superficial fascia was sutured. Ropivacaine infiltration at the incision site was performed for postoperative analgesia.
Awakening period: The endotracheal tube may be removed once patients meet the following criteria: a BIS greater than 90, a TOFr exceeding 90%, recovery of consciousness and muscle strength, ability to follow commands, restoration of pharyngeal, cough, and swallowing reflexes, stable respiratory function characterized by normal tidal volume, minute ventilation, and regular rhythm, as well as stable circulatory status.
In other circumstances, if patient movement occurred due to an insufficient dose of mivacurium, an immediate rescue was performed by administering an additional mivacurium dose of 0.07 mg/kg, and the infusion rate was increased by 0.5 μg·kg−1·min−1 for subsequent patients. In cases where the HR fell below 50 beats per minute, an intravenous injection of atropine 0.5 mg was administered. If the MAP decreased by more than 20% from baseline or if the systolic blood pressure (SBP) dropped below 90 mmHg, the following interventions were applied: for HR ≤ 80 beats/min, 6 mg of ephedrine was administered intravenously, whereas for HR > 80 beats/min, 10 μg of phenylephrine was injected intravenously. In instances where SBP exceeded 180 mmHg, and inadequate anesthetic depth was ruled out, an intravenous injection of urapidil 5 mg was administered.
Modified Dixon Up-and-Down Sequential Method
The initial mivacurium infusion dose was set at 10 μg·kg−1·min−1, with subsequent dose adjustments made in increments of 0.5 μg·kg−1·min−1. At a stimulation voltage of 100 V, the absence of the MEP waveform after excluding nerve injury was classified as a negative outcome. In such cases, the mivacurium dose was decreased by 0.5 μg·kg−1·min−1 for the subsequent patient to maintain muscle relaxation. Conversely, if the MEP waveform was consistently elicited throughout the surgical procedure, the outcome was deemed positive, and the mivacurium dose was increased by 0.5 μg·kg−1·min−1 for the next patient. Dose-finding proceeded until seven crossover pairs were obtained. To ensure blinding implementation, the neurophysiological monitoring physician assessed the MEP waveform without knowledge of the mivacurium infusion rate.
Outcomes
The primary outcome is the mivacurium infusion dose and corresponding changes in MEP waveforms, based on which the ED50, ED95, and the 95% confidence interval (95% CI) of mivacurium that does not interfere with IONM in adolescent scoliosis surgery were determined.
The secondary outcomes encompass: (1) the preoperative baseline characteristics of the patients; (2) intraoperative conditions, including the surgery time (defined as the time from the initial skin incision to the closure of the incision), the awakening time (defined as the interval from the conclusion of surgery to when the patient regains consciousness), and the extubation time (defined as the interval from the conclusion of surgery to the removal of the endotracheal tube); (3) the incidence of complications, such as unexpected body movements and anaphylactoid reactions, characterized by symptoms including erythema of the chest and facial skin, asthma, or hemodynamic instability; (4) measurement of MBP and HR at three time points both prior to and following the administration of mivacurium: immediately (T1) and five minutes (T2) after intravenous injection of mivacurium during induction; immediately (T3) and five minutes (T4) after infusion of mivacurium post-intubation; and immediately (T5) and five minutes (T6) after infusion of mivacurium following the induction of MEP waveforms; (5) The application of vasoactive agents; (6) the surgeon’s evaluation of surgical conditions using the Leiden-Surgical Rating Scale (L-SRS), which is based on the surgical field, muscle contraction, and the progress of the surgery at four time points: the start of incision exposure (TL1), the end of incision exposure (TL2), immediately after infusion of mivacurium following the induction of MEP waveforms (TL3), and upon discontinuation of mivacurium infusion (TL4).
Statistical Analysis
Statistical analyses were conducted using SPSS version 27.0, with a significance threshold set at p < 0.05. Employing the modified Dixon up-and-down sequential methodology, the study identified seven pairs demonstrating negative-to-positive transitions, with a cohort size exceeding 20 patients to ensure statistical robustness.10 The ED50, ED95, and 95% CI for mivacurium during continuous infusion, which did not interfere with IONM in adolescent scoliosis surgery, were calculated using Probit regression analysis. Data following a normal distribution were reported as mean ± standard deviation (x ± s). Intergroup comparisons were conducted using the independent samples t-test, while comparisons across multiple groups were performed using repeated measures ANOVA. Data not following a normal distribution were presented as median and interquartile range [M (25th percentile, 75th percentile)], with intergroup comparisons conducted using the Mann–Whitney U-test, and comparisons across multiple groups were performed using non-parametric tests. Categorical variables were expressed as frequency (percentage), and intergroup comparisons were conducted using the chi-square (χ2) test.
Results
The initial infusion dose of mivacurium was 10 μg·kg−1·min−1, with adjacent dose increments of 0.5 μg·kg−1·min−1. To ensure adequate statistical power, patients were recruited until 7 crossover points were reached and the sample exceeded 20 participants.14,17 A total of 26 patients participated in the study (the individual sequential dosing data is provided in the Supplementary Figure). All of them maintained BIS between 40–60 throughout the surgical procedure, with no instances of BIS exceeding 60 or falling below 40 for more than one minute. Neuromuscular monitoring confirmed that all patients received mivacurium infusion to maintain TOFc1-3 until surgical exposure was completed, avoiding significant surgical impairment due to myoclonus. After TOFr recovered to 75% and MEP waveforms could be evoked, mivacurium infusion was resumed according to the sequential dose-setting method. According to the requirements of the modified Dixon up-and-down sequential method, cases before the first crossover (ie., the first through fifth patients) were excluded.18 Consequently, 21 patients were included in the final statistical analysis (Figure 1), comprising 3 males and 18 females.
 |
Figure 1 Flowchart of this trial. Notes: According to the requirements of the modified Dixon up-and-down sequential method, cases before the first crossover (i.e., the first through fifth patients) were excluded. 21 patients were included in the final statistical analysis. |
Comparisons Between the Positive and Negative Cases
Statistical analysis was ultimately performed on 21 patients, including 10 positive cases and 11 negative cases. There were no statistically significant differences between the two groups (p > 0.05) concerning demographic variables (gender, age, height, weight, ASA status), preoperative baseline conditions (Cobb angle, preoperative liver and kidney function indicators, electrolytes, BChE activity), and surgical parameters (surgery time, awakening time, extubation time). Detailed information is provided in Tables 1–3.
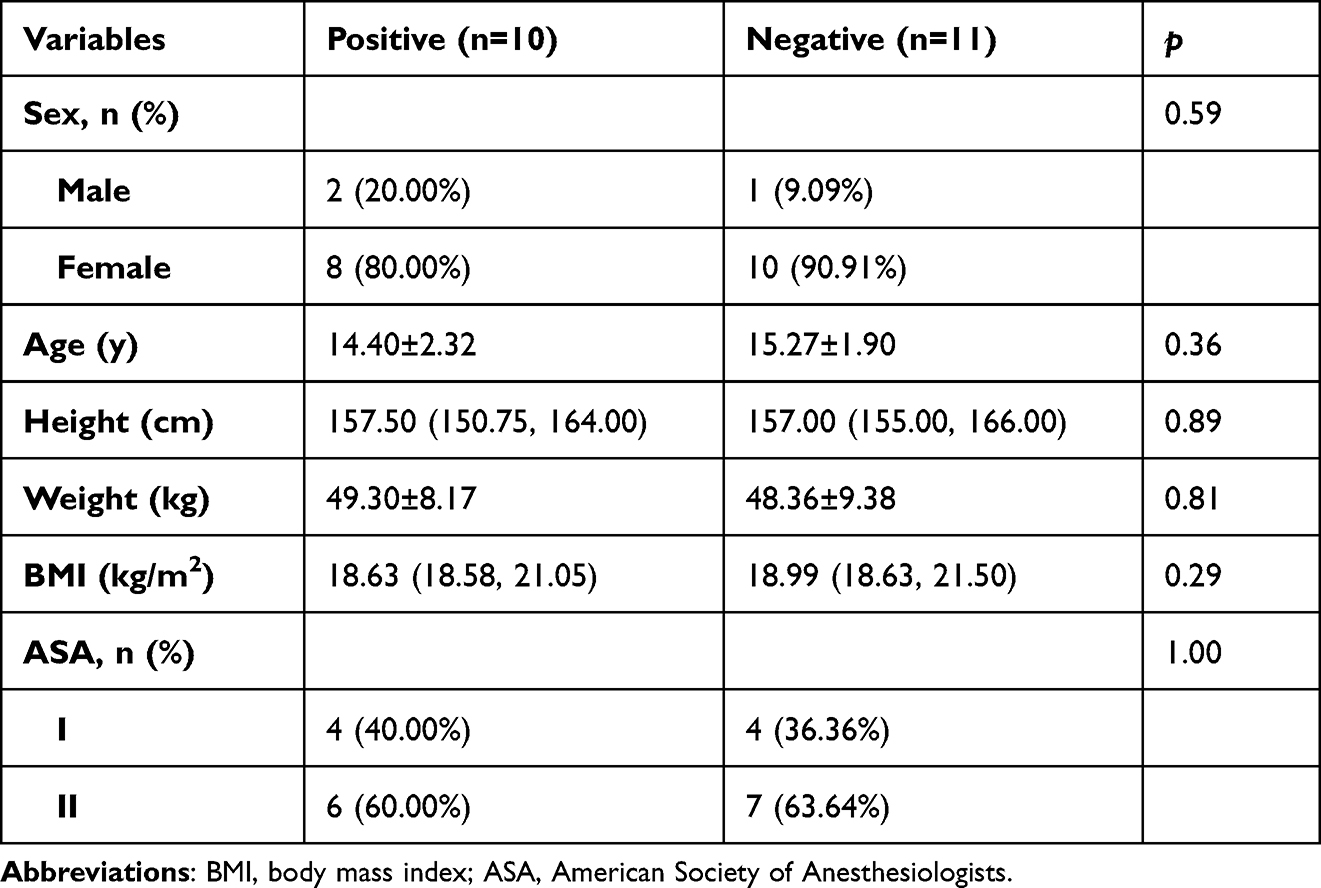 |
Table 1 Demographic Data of Patients |
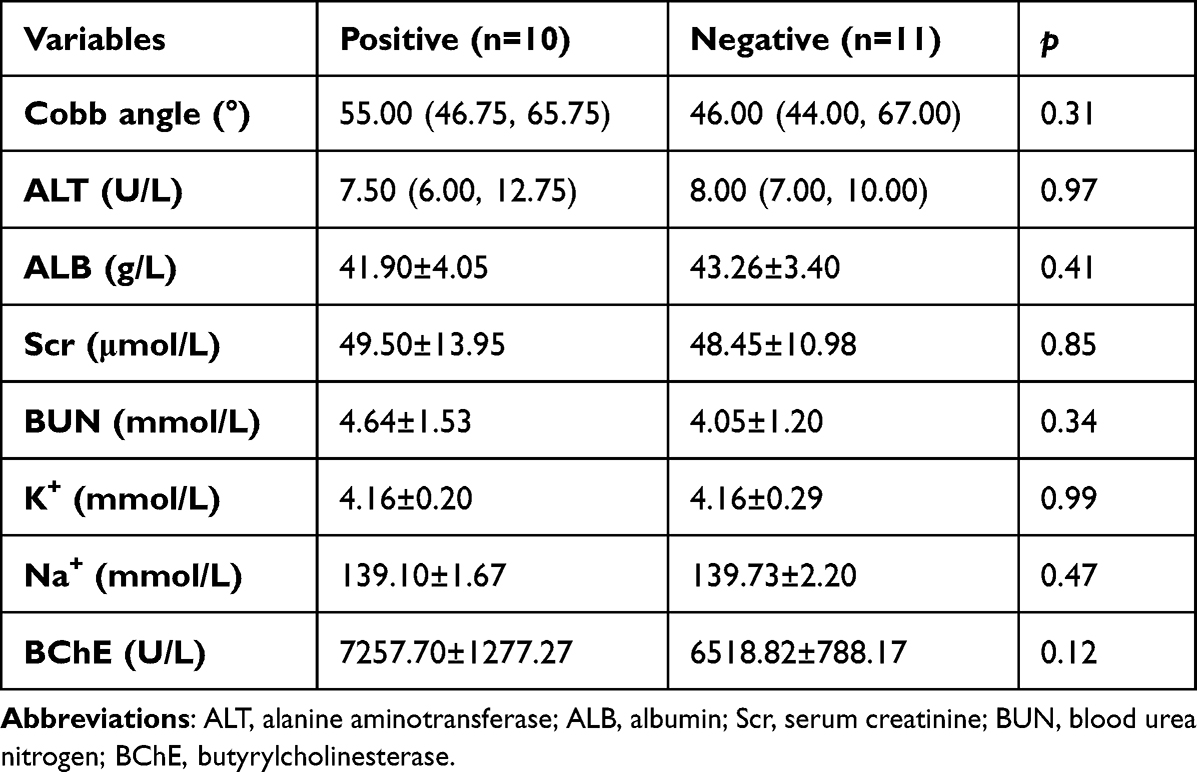 |
Table 2 Preoperative Basic Conditions of Patients |
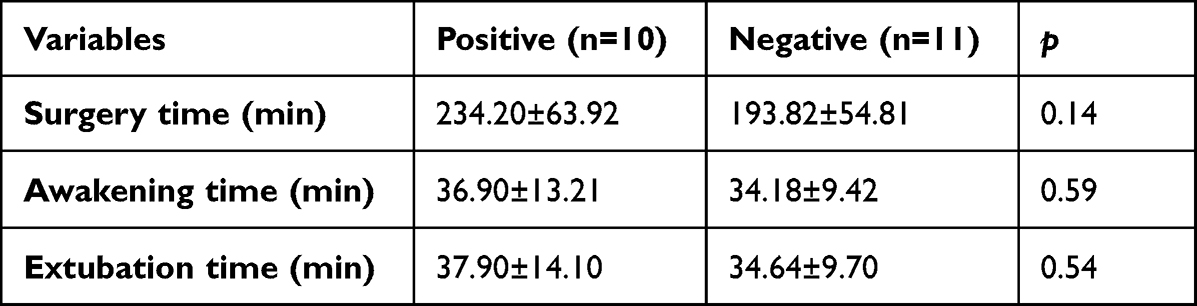 |
Table 3 Intraoperative Information |
ED50 and ED95 of Mivacurium
The sequence diagram illustrating the continuous infusion dosing of mivacurium for monitoring MEP during adolescent scoliosis surgery is presented in Figure 2. The initial dose formally incorporated into the statistical analysis was 7.5 μg·kg−1·min−1. A total of 21 cases were enrolled by the conclusion of seven crossover events, comprising 10 cases with positive reactions and 11 cases with negative reactions. Utilizing SPSS Probit analysis, the model equation was determined to be: Probit (p) = 22.008–3.041x. The Pearson’s chi-squared goodness-of-fit test yielded a result of χ2=0.061, p=0.97, indicating a satisfactory model fit. In adolescent scoliosis surgery, under TIVA maintenance with BIS 40–60, the estimated ED50 of continuously infused mivacurium that does not interfere with MEP waveform induction at a low stimulation voltage of 100 V was 7.24 μg·kg−1·min−1 (95% CI: 6.87 μg·kg−1·min−1 to 7.54 μg·kg−1·min−1), while the ED95 was 6.70 μg·kg−1·min−1 (95% CI: 4.79 μg·kg−1·min−1 to 6.99 μg·kg−1·min−1). The dose-response curve is depicted in Figure 3.
 |
Figure 2 Sequential infusion dose diagram of mivacurium for continuous infusion during MEP monitoring in adolescent scoliosis surgery. The black dot represents “positive”, referring to MEP waveforms induced reproducibly at the current dose. The white square represents “negative”, referring to MEP waveforms disappeared at the current dose. Notes: A total of 26 patients participated in the study. According to the requirements of the modified Dixon up-and-down sequential method, cases before the first crossover (i.e., the first through fifth patients) were excluded. Consequently, 21 patients contributed to ED estimation. |
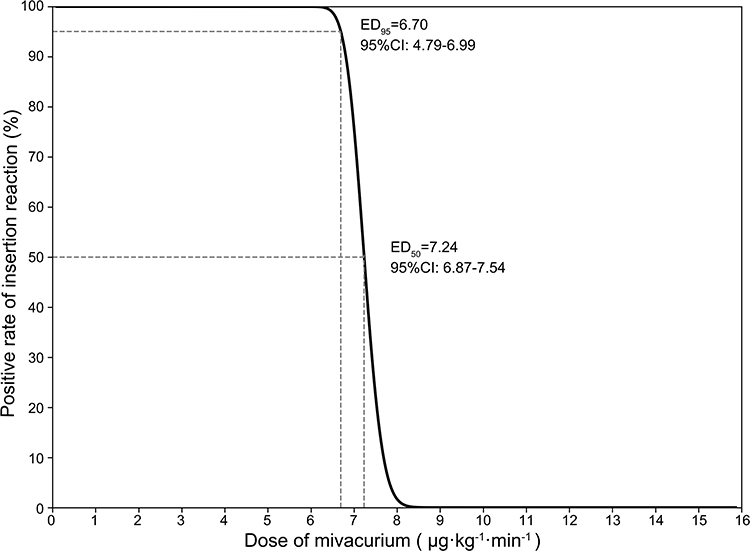 |
Figure 3 Dose-response curve of continuous infusion of mivacurium for MEP monitoring in adolescent scoliosis surgery according to the Probit analysis. Notes: ED95 estimated from small sequential samples exhibits relatively low precision and is primarily intended to serve as a reference dose. |
Safety and Effectiveness
Incidence of adverse reactions: None of the patients exhibited intraoperative unexpected body movement, asthma, or spontaneous recovery of breathing. Six patients (28.57%) developed transient chest skin erythema during induction, however, no significant alterations in MAP or HR were observed. Re-administration of mivacurium during surgery did not result in skin erythema or hemodynamic changes.
Hemodynamic changes before and after drug administration: There was no statistically significant difference in MAP before and after the three administrations of mivacurium (T1 vs T2, T3 vs T4, T5 vs T6) (p > 0.05), as illustrated in Table 4. Similarly, no statistically significant difference was observed in HR (p > 0.05), as shown in Table 5.
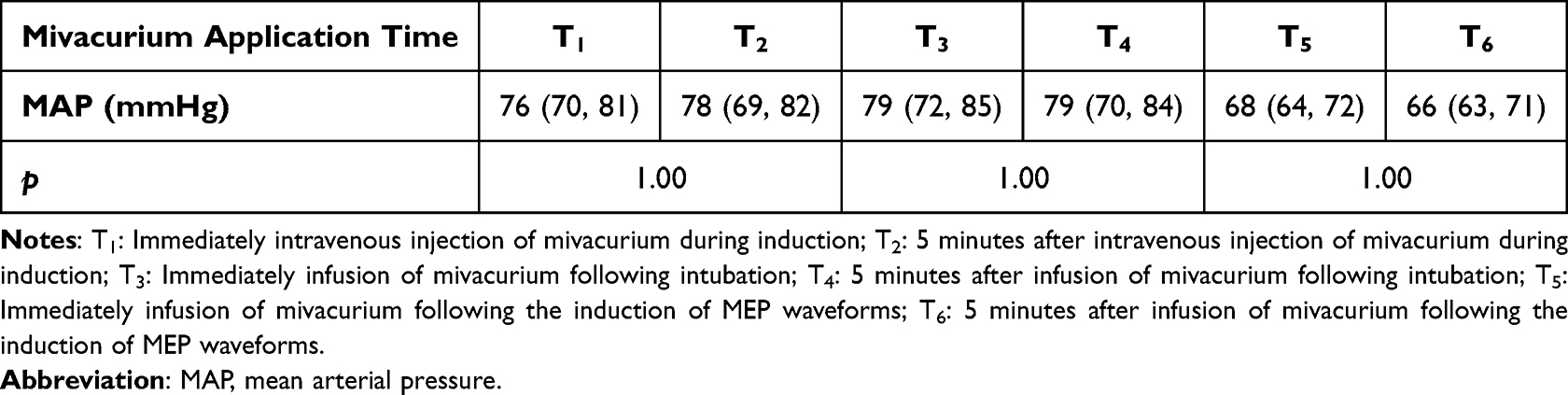 |
Table 4 Changes in MAP of Patients Before and After the Application of Mivacurium |
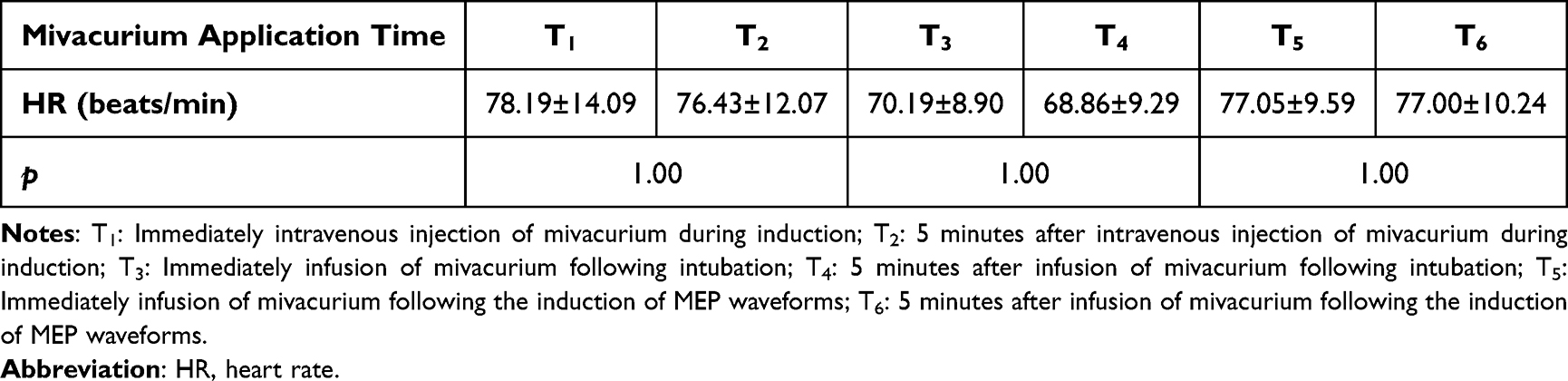 |
Table 5 Changes in HR of Patients Before and After the Application of Mivacurium |
Application of vasoactive agents: Seven patients (33.33%) received small doses of ephedrine intraoperatively, with a dosage of 6 mg. None of the patients received atropine, phenylephrine, or urapidil.
Surgical conditions: There were no statistically significant differences in L-SRS scores at time points TL1, TL2, and TL4 (p > 0.05). The L-SRS scores at time points TL1, TL2, and TL4 were all higher than the L-SRS score at time point TL3 (p < 0.05), as demonstrated in Table 6.
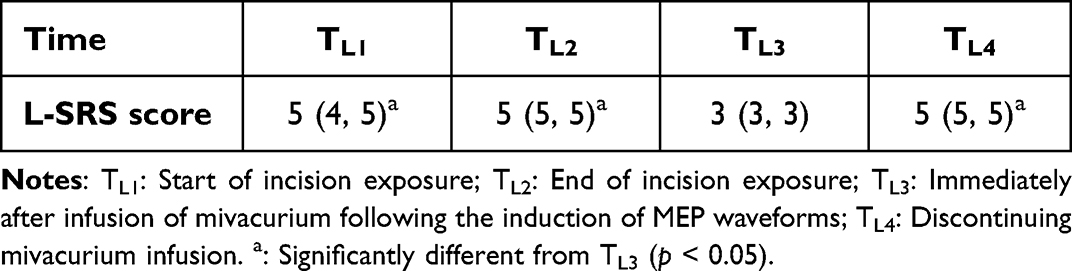 |
Table 6 L-SRS Scores at Different Times |
Discussion
The study employed the modified Dixon up-and-down sequential method to determine the infusion dose of mivacurium that maintains MEP waveform presence in adolescents aged 12–18 years undergoing scoliosis surgery without preoperative neurological impairment under TIVA and a stimulation voltage of 100 V. The ED50 was 7.24 μg·kg−1·min−1 (95% CI: 6.87 μg·kg−1·min−1 to 7.54 μg·kg−1·min−1), and the ED95 was 6.70 μg·kg−1·min−1 (95% CI: 4.79 μg·kg−1·min−1 to 6.99 μg·kg−1·min−1). Additionally, hemodynamic changes, adverse events, and surgical conditions were evaluated, demonstrating that mivacurium could be effectively administered without serious adverse events.
NMBAs selectively inhibit excitation transmission at the neuromuscular junction, thereby facilitating appropriate muscle relaxation for surgical procedures. This mechanism reduces the risk of adverse reactions, such as muscle twitching that may compromise the surgical field, accidental body movement that may damage significant nerves or blood vessels, excessive use of sedatives or analgesics, and blood loss.19,20 Additionally, the stabilization of monitoring signals is enhanced. The L-SRS scores, as evaluated by the surgeon, indicated improved surgical conditions during the medication period compared to the off-medication period, underscoring the importance of utilizing NMBAs. Nonetheless, excessively high doses of NMBAs can lead to the disappearance of MEP waveforms, thereby hindering the application of this critical monitoring technique for safeguarding neural function during scoliosis surgery. Previous research has demonstrated that an appropriate dose of NMBAs can concurrently fulfill the requirements for surgical muscle relaxation and MEP monitoring. This may be attributed to factors such as the distribution of neuromuscular junctions, the frequency of excitation transmission, the receptor density on the postsynaptic membrane, and the concentration of NMBAs in various regions.21,22 The relaxation of paravertebral muscles precedes that of limb muscles, allowing for a balance point within this contradiction. The central challenge lies in determining an appropriate NMBA dosage, yet there is a paucity of research regarding medication dosages in adolescent scoliosis surgery.
Mivacurium is currently the sole short-acting non-depolarizing NMBAs used in clinical practice. Administered at an intubation dosage of 0.2–0.25 mg/kg, it induces a neuromuscular blocking effect lasting approximately 19.7 to 21 minutes. Mivacurium is rapidly metabolized by BChE, which prevents accumulation during prolonged infusion and results in a low incidence of residual neuromuscular blockade postoperatively.23,24 Its favorable controllability enables the provision of necessary neuromuscular blockade for surgical procedures, while allowing for the rapid restoration of muscle strength following the cessation of infusion. This characteristic facilitates prompt IONM when required during surgery. Consequently, mivacurium is particularly suitable for adolescent scoliosis surgeries that necessitate IONM. In two studies by Chen et al,25,26 the sequential method was employed to ascertain that the maximum infusion doses of mivacurium, which do not interfere with recurrent laryngeal nerve monitoring during thyroid surgery under propofol total intravenous anesthesia and sevoflurane inhalation anesthesia, are 18.9 μg·kg−1·min−1 and 8.94 μg·kg−1·min−1, respectively. These findings confirm the feasibility of utilizing appropriate doses of mivacurium to concurrently achieve muscle relaxation and facilitate IONM. Considering the inhibitory effect of inhaled anesthetic agents on IONM and the fact that patients with scoliosis are a high-risk group for malignant hyperthermia,27 this trial measured the infusion dose of mivacurium for IONM under TIVA in scoliosis surgery.
Based on infusion doses of mivacurium established in previous studies, and considering the infusion dose necessary to maintain 90–99% twitch depression under TIVA is 5–15 μg·kg−1·min−1, the initial dose in this trial was set at 10 μg·kg−1·min−1. To ensure precise drug concentration and infusion rate, adjacent doses were adjusted using an arithmetic gradient of 0.5 μg·kg−1·min−1. Given that the disappearance of MEP waveforms serves as the primary warning indicator, suprathreshold stimulation can generate waveforms in the absence of nerve injury.28 This study employed a low stimulation voltage of 100 V as the standard, and the final measured continuous infusion ED50 of mivacurium, which simultaneously satisfies surgical muscle relaxation and MEP monitoring requirements, was determined to be 7.24 μg·kg−1·min−1, with an ED95 of 6.70 μg·kg−1·min−1. This precise dosing is convenient for clinical application and is also applicable to MEP monitoring with higher stimulation voltages. Although this finding significantly differs from the 18.9 μg·kg−1·min−1 reported by Chen et al,26 Liu et al29 showed that an infusion dose of 8 μg·kg−1·min−1 is sufficient to maintain the depth of muscle relaxation required for laryngeal microsurgery The difference in doses may be related to the type of neural monitoring and the response of the target monitored nerves to NMBAs.
Determining the ED50 (7.24 μg·kg−1·min−1) and ED95 (6.70 μg·kg−1·min−1) for continuous mivacurium infusion provides important reference for clinical management in TIVA-based IONM-assisted adolescent scoliosis surgery. ED50 can serve as a reference for the initial infusion dose during the anesthesia maintenance phase, using this dose or slightly lower to balance surgical muscle relaxation and MEP monitoring needs. The range of 6.70–7.24 μg·kg−1·min−1 serves as a practical titration window, within which clinicians can adjust the infusion rate based on individual patient responses, surgical requirements, and MEP waveforms. However, it should be noted that ED95 is derived from small sequential samples, resulting in relatively low precision. Additionally, the narrow adjustment range indicates that small changes can affect MEP waveforms, necessitating careful titration. Our preliminary study also determined ED50 and ED95 for rocuronium, providing a titration window (7.51–8.69 μg·kg−1·min−1) for clinical application. The determination of doses for both agents facilitates evidence-based alternative selection when one agent is contraindicated.
Mivacurium is among the NMBAs characterized by relatively low allergenicity. Nonetheless, its potential to induce histamine release can lead to abnormal dermatological, respiratory, and circulatory manifestations, with the severity of these symptoms correlating with plasma histamine levels.30 In this trial, dexamethasone was preemptively administered during induction, and mivacurium was injected slowly over a period exceeding 30 seconds, which effectively mitigated the incidence and severity of adverse reactions.31,32 Consequently, only six patients experienced transient chest skin erythema during induction. Furthermore, all patients were assessed at three distinct time points: during anesthesia induction, during the maintenance of muscle relaxation following induction, and at the initiation of muscle relaxation maintenance with sequentially set doses. No statistically significant differences were observed in MAP and HR immediately following mivacurium infusion and five minutes thereafter at these intervals, which may be related to rapid desensitization to histamine release.33 These findings indicate that no serious adverse reactions occurred with the application of mivacurium.
Mivacurium is predominantly metabolized by BChE, with 95–99% undergoing this process. Various factors, including monoamine oxidase inhibitors, impaired hepatic synthetic function, renal failure, and burns, can lead to a slight reduction in BChE activity, thereby modestly extending the duration of mivacurium’s action.34,35 Patients possessing homozygous atypical BChE genes exhibit significantly reduced BChE activity, and demonstrate extremely high sensitivity to mivacurium, with metabolism times potentially exceeding eight hours, which substantially impacts patient recovery and safety.36,37 In this study, all participants demonstrated BChE activity within the normal range. Individuals with abnormal BChE activity were excluded from participation. The final results indicated no statistically significant difference in BChE activity between the groups with positive and negative outcomes. This approach ensured patient safety during the perioperative period and minimized the influence of atypical patients on the trial results.
This study has certain limitations. Firstly, the infusion dose of mivacurium determined in this trial is specifically applicable to adolescent patients aged 12–18 years undergoing primary scoliosis surgery under TIVA without preoperative neurological impairment. Variations in factors such as age, preoperative neurological impairment, and inhalation anesthesia may affect IONM and metabolism of NMBAs,38 necessitating further research to determine the appropriate infusion dose. Secondly, the warning indicators for MEP monitoring include waveform disappearance, amplitude reduction, and increased stimulation threshold. This trial used only the presence of MEP waveforms throughout at a stimulation voltage of 100 V as the indicator to preliminarily explore the critical range of mivacurium applicable to such surgeries. Further research is needed to determine the NMBAs dose suitable for more detailed MEP monitoring and evaluation. Finally, this trial employed the sequential method to maximize the utilization of clinical data in a preliminary investigation of the appropriate mivacurium infusion dose in IONM for scoliosis surgery, thereby providing a practical dose range. However, the ED95 estimated from small sequential samples exhibits relatively low precision and is primarily intended to serve as a reference dose. Currently, there is a lack of comparative analysis between this infusion dose range and conventional perioperative management approaches. Therefore, future studies should continue to explore the advantages of this dosing regimen for adolescent scoliosis surgery and its impact on postoperative outcomes.
Conclusion
In conclusion, this study evaluated the feasibility of using mivacurium for IONM during adolescent scoliosis surgery. Under TIVA, the ED50 and ED95 for continuous infusion of mivacurium to maintain MEP waveform presence at a stimulation voltage of 100 V in adolescents aged 12 to 18 years undergoing scoliosis surgery without preoperative neurological impairment were 7.24 μg·kg−1·min−1 and 6.70 μg·kg−1·min−1, respectively. However, the ED95 estimated from the small sequential sample exhibited relatively low precision and primarily serves as a reference for clinical application. Future research will further explore the impact of the mivacurium infusion dose determined in this study on postoperative outcomes in adolescent scoliosis surgery. Additionally, using this infusion dose as a reference, we aim to investigate the potential applications of mivacurium in other surgeries requiring IONM, such as conventional spinal or cranial surgery, with the goal of continuously optimizing perioperative muscle relaxation management.
Data Sharing Statement
Data related to this study can be obtained by contacting the corresponding authors, Xin Jiang and Hongbin Yuan, upon reasonable request.
Ethics Approval and Consent to Participate
This study was reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Naval Medical University. All patients and their legal guardians signed their written informed consent before being enrolled in this study, agreeing to the conduct of this trial and the publication of related data and potentially identifiable images or data in this article.
Funding
This study was conducted with self-funded. The Military Clinical Key Specialty (JDLCZDZK to Y.H.B) funded the Open Access-related expenses.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Ali S, Talha M, Qureshi MA, et al. Intraoperative Neurophysiological Monitoring in Corrective Surgery of Scoliosis - Experience at a Tertiary Care Hospital. J Coll Physicians Surg Pak. 2024;34(3):284–13. doi:10.29271/jcpsp.2024.03.284
2. Daroszewski P, Huber J, Kaczmarek K, et al. “Real-Time Neuromonitoring” Increases the Safety and Non-Invasiveness and Shortens the Duration of Idiopathic Scoliosis Surgery. J Clin Med. 2024;13(5):1497. doi:10.3390/jcm13051497
3. MacDonald DB. Overview on Criteria for MEP Monitoring. J Clin Neurophysiol. 2017;34(1):4–11. doi:10.1097/WNP.0000000000000302
4. Ajiboye RM, Park HY, Cohen JR, et al. Demographic Trends in the Use of Intraoperative Neuromonitoring for Scoliosis Surgery in the United States. Int J Spine Surg. 2018;12(3):393–398. doi:10.14444/5046
5. Kawaguchi M, Iida H, Tanaka S, et al. A practical guide for anesthetic management during intraoperative motor evoked potential monitoring. J Anesth. 2020;34(1):5–28. doi:10.1007/s00540-019-02698-2
6. Pajewski TN, Arlet V, Phillips LH. Current approach on spinal cord monitoring: the point of view of the neurologist, the anesthesiologist and the spine surgeon. Eur Spine J. 2007;16(Suppl 2):S115–29. doi:10.1007/s00586-007-0419-6
7. Oh SK, Kwon WK, Park S, et al. Comparison of operating conditions, postoperative pain and recovery, and overall satisfaction of surgeons with deep vs no neuromuscular blockade for spinal surgery under general anesthesia: a prospective randomized controlled trial. J Clin Med. 2019;8(4):498. doi:10.3390/jcm8040498
8. Gehle HM, Allen AJ, Keil LG, et al. Neuromuscular blocking agent use in adolescent idiopathic scoliosis surgery: a safety assessment. Spine Deform. 2025;29. doi:10.1007/s43390-025-01211-y
9. Liu HY, Xia TJ, Zhu ZZ, et al. Effect of neuromuscular blockade on transcranial electric motor evoked potentials during surgical correction for idiopathic scoliosis under total intravenous anesthesia. J Clin Monit Comput. 2019;33(3):471–479. doi:10.1007/s10877-018-0182-8
10. Li CX, Song FH, Wang Y, et al. Effect of the degree of muscle relaxation on motor-evoked potential elicited by transcranial electrical stimulation in spine surgery (in Chinese). Nan Fang Yi Ke Da Xue Xue Bao. 2010;30(12):2686–2688.
11. Kim WH, Lee JJ, Lee SM, et al. Comparison of motor-evoked potentials monitoring in response to transcranial electrical stimulation in subjects undergoing neurosurgery with partial vs no neuromuscular block. Br J Anaesth. 2013;110(4):567–576. doi:10.1093/bja/aes395
12. Ko MJ, Oh B, Jung JW, et al. Comparing the effect between continuous infusion and intermittent bolus of rocuronium for intraoperative neurophysiologic monitoring of neurointervention under general anesthesia. Medicine. 2018;97(51):e13816. doi:10.1097/MD.0000000000013816
13. Zhang X, Hu H, Yan R, et al. Effects of rocuronium dosage on intraoperative neurophysiological monitoring in patients undergoing spinal surgery. J Clin Pharm Ther. 2022;47(3):313–320. doi:10.1111/jcpt.13557
14. Pace NL, Stylianou MP. Advances in and limitations of up-and-down methodology: a précis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
15. Yang W, Zhou R, Zhou X, et al. Effective dose of oliceridine fumarate co-administered with remimazolam in suppressing gastroscope insertion responses for adults. Drug Des Devel Ther. 2025;19:5033–5041. doi:10.2147/DDDT.S527586
16. Zhang YX, Jiang X, Qin H, et al. The median effective dose of rocuronium that does not affect intraoperative neurophysiological monitoring in adolescent patients undergoing scoliosis surgery. J Clin Anesthesiol. 2026;42(3):320–323. (in Chinese). doi:10.12089/jca.2026.03.019
17. Görges M, Zhou G, Brant R, et al. Sequential allocation trial design in anesthesia: an introduction to methods, modeling, and clinical applications. Paediatr Anaesth. 2017;27(3):240–247. doi:10.1111/pan.13088
18. Yang C, Dong W, Luo J, et al. The median effective dose of intrathecal hyperbaric bupivacaine for cesarean section at moderately high-altitude. Drug Des Devel Ther. 2024;18:1313–1319. doi:10.2147/DDDT.S455844
19. Phoowanakulchai S, Kawaguchi M. Updated review on the use of neuromuscular blockade during intraoperative motor-evoked potential monitoring in the modern anesthesia era. J Anesth. 2024;38(1):114–124. doi:10.1007/s00540-023-03265-6
20. Hemmer LB, Zeeni C, Bebawy JF, et al. The incidence of unacceptable movement with motor evoked potentials during craniotomy for aneurysm clipping. World Neurosurg. 2014;81:99–104. doi:10.1016/j.wneu.2012.05.034
21. Alfille PH, Merritt C, Chamberlin NL, et al. Control of perioperative muscle strength during ambulatory surgery. Curr Opin Anaesthesiol. 2009;22(6):730–737. doi:10.1097/ACO.0b013e328331d545
22. Betz M, Aguirre J, Schubert M, et al. Hand or foot train-of-four tests and surgical site muscle relaxation assessed with multiple motor evoked potentials: a prospective observational study. Eur J Anaesthesiol. 2021;38(8):872–879. doi:10.1097/EJA.0000000000001398
23. Ezzine S, Donati F, Varin F. Mivacurium arteriovenous gradient during steady state infusion in anesthetized patients. Anesthesiology. 2002;97(3):622–629. doi:10.1097/00000542-200209000-00016
24. Cammu G, De Witte J, De Veylder J, et al. Postoperative residual paralysis in outpatients versus inpatients. Anesth Analg. 2006;102(2):426–429. doi:10.1213/01.ane.0000195543.61123.1f
25. Chen Y, Huang L, Li Y, et al. Sequential method for determining the maximum dose of mivacurium continuously infused for intraoperative neuromonitoring in thyroid surgery. Nan Fang Yi Ke Da Xue Xue Bao. 2018;38(12):1472–1475. doi:10.12122/j.issn.1673-4254.2018.12.12
26. Chen Y, Wang B, Yao L, et al. Maximum dose of continuous infusion of mivacurium for thyroid surgery under total intravenous anesthesia: a sequential trial of monitoring neurological function in 30 patients. Nan Fang Yi Ke Da Xue Xue Bao. 2021;41(1):64–68. doi:10.12122/j.issn.1673-4254.2021.01.08
27. Reysner M, Reysner T, Janusz P, et al. The influence of anesthesia on neuromonitoring during scoliosis surgery: a systematic review. NeuroSci. 2024;5(4):693–712. doi:10.3390/neurosci5040049
28. Guo D, Fan X, You H, et al. Prediction of postoperative motor deficits using intraoperative motor-evoked potentials in middle cerebral artery aneurysm. Neurosurg Rev. 2021;44(1):495–501. doi:10.1007/s10143-020-01235-0
29. Liu Y, Wang Y, Xie M, et al. Optimal dose of mivacurium for laser-assisted laryngeal microsurgery: a pharmacokinetic study using closed-loop target-controlled infusion. Anaesthesiol Intensive Ther. 2024;56(4):231–240. doi:10.5114/ait.2024.145249
30. Che D, Wang J, Ding Y, et al. Mivacurium induce mast cell activation and pseudo-allergic reactions via MAS-related G protein coupled receptor-X2. Cell Immunol. 2018;332:121–128. doi:10.1016/j.cellimm.2018.08.005
31. Xiang Z, Yan-Liang Q, Xiao-Yang S, et al. Effects of promethazine or dexamethasone pretreatment on mivacurium-induced histamine release in children. Paediatr Anaesth. 2014;24(3):322–326. doi:10.1111/pan.12305
32. Plaud B, Marty J, Debaene B, et al. The cardiovascular effects of mivacurium in hypertensive patients. Anesthesia Analg. 2002;95(2):379–384. doi:10.1097/00000539-200208000-00025
33. Koppert W, Blunk JA, Petersen LJ, et al. Different patterns of mast cell activation by muscle relaxants in human skin. Anesthesiology. 2001;95(3):659–667. doi:10.1097/00000542-200109000-00019
34. Donadon M, Cimino M, Procopio F, et al. Potential role of cholinesterases to predict short-term outcome after hepatic resection for hepatocellular carcinoma. Updates Surg. 2013;65(1):11–18. doi:10.1007/s13304-012-0174-z
35. Kamolz LP, Andel H, Greher M, et al. Serum cholinesterase activity reflects morbidity in burned patients. Burns. 2002;28(2):147–150. doi:10.1016/s0305-4179(01)00091-2
36. Cassel J, Staehr-Rye AK, Nielsen CV, et al. Use of neuromuscular monitoring to detect prolonged effect of succinylcholine or mivacurium: three case reports. Acta Anaesthesiol Scand. 2014;58(8):1040–1043. doi:10.1111/aas.12357
37. Eskildsen KZ, Gätke MR. Danish Cholinesterase Research Unit diagnoses patients with prolonged paralysis after succinylcholine and mivacurium. Ugeskr Laeger. 2014;176(12A):V09130566.
38. Kombos T, Kopetsch O, Suess O, et al. Does preoperative paresis influence intraoperative monitoring of the motor cortex? J Clin Neurophysiol. 2003;20(2):129–134. doi:10.1097/00004691-200304000-00007
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.