Back to Journals » Infection and Drug Resistance » Volume 15
Missed Tuberculosis Investigations and Associated Factors in Patients with Symptoms Indicative of Tuberculosis at Public Health Institutions in Northwest Ethiopia: The Application of a Negative Binomial Model
Authors Asemahagn MA ![]()
Received 1 January 2022
Accepted for publication 26 March 2022
Published 19 April 2022 Volume 2022:15 Pages 1947—1956
DOI https://doi.org/10.2147/IDR.S355247
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Mulusew Andualem Asemahagn
School of Public Health, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Mulusew Andualem Asemahagn, Email [email protected]
Background: Tuberculosis (TB) remains one of the top health problems in Ethiopia, and over one-third of estimated TB cases remain undetected. This study examined the magnitude and factors of missed opportunities for TB investigation at public health facilities in Northwest Ethiopia.
Methods: A facility-based cross-sectional study was conducted among 412 adult patients with TB symptoms from 34 randomly selected public health facilities. Data on socio-demographics, TB symptoms, and clinical status were collected by an exit interview. A patient was considered missed for TB investigation if he/she had at least one symptom suggestive of TB but did not receive a sputum smear and/or x-ray evaluation to rule out TB. We computed descriptive and analytical statistics using SPSS version 26. A negative binomial regression analysis was used to identify factors associated with missed opportunities for TB investigation. Statistical significance was determined at a p-value less than 0.05.
Results: A total of 412 presumptive TB patients, 235 (57%) females and 247 (60%) rural dwellers were interviewed. The mean age of respondents was 35 ± 8 years and 228 (55.3%) were from health centers. Over two-thirds, 284 (69%) were new patients, 62 (15%) were HIV positive and 78 (19%) had diabetes mellitus (DM). Fifty patients with symptoms suggestive of TB did not receive sputum evaluation services. Inability to read and write, having DM, having normal body mass index and facility type they visited were significant factors to missing opportunities to get TB investigations.
Conclusion: A significant number of patients with symptoms suggestive of TB were missed for sputum evaluation to rule out TB. Education level, comorbidity, nutritional status and type of facility patients attended were factors of missing opportunities for TB investigation. Thus, improving quality of TB diagnosis, screening TB among all types of patients, and paying attention to screen illiterate people are crucial to avoid missing potential TB cases.
Keywords: TB, missed investigation, factors, patients, public health facilities, Ethiopia
Introduction
Tuberculosis (TB) is the second leading cause of death from a single infectious agent next to COVID-19.1 In 2020, there were about 9.9 million estimated new TB cases and 1.514 million TB deaths globally.1 About 4.1 million estimated new TB cases were missed in 2020.1 Poor and low socioeconomic countries accounted for the greatest burden of TB cases, where African countries accounted for 25% of the global TB incidence, which could be attributed to high comorbidities (HIV and diabetes mellitus),2–4 limited access and poor quality of healthcare services,1,5–8 poverty and population crowdedness.9–11
One of the key strategies for global TB prevention and control programs is the timely detection and treatment of detected TB cases.11,12 However, the global and national TB case detection performances fall short of the expected TB case detection target.1,13,14 Because of this and other factors, one-third of global estimated TB cases are missed.11,12 This is possibly related to low TB case notification performance due to (poor accessibility and quality of TB services, limited health worker skills, patient delay and limited TB program budget),2,6,11–13 and under-reporting of detected TB cases.11,14,15 Missed TB cases result in having long infectious period, high TB disease complications, delayed treatment, death and high catastrophic costs for families.11–16 As a result, improving the performance of low TB case notification becomes one of the primary gears of the End TB Strategy, which aims to eliminate TB burdens by 2030/5.1,11,15
Ethiopia’s TB situation is similar to that of other developing countries. Despite several anti-TB interventions, Ethiopia is one of the 14 countries with high TB, TB-HIV and multi-drug resistant TB countries.12 The leading contributor to this burden is poor TB case notification performance,2 which results in missing over a third of estimated new infectious TB cases.2,17 Previous studies have reported the presence of more undetected TB cases for a variety of reasons, including poor TB service quality,2,15,17 limited access to TB diagnostic services,2,13 patient and facility delays for TB services,9,13 impaired active TB case finding practices, 2 missing potential TB cases at health facilities (at different departments and laboratory).15,17
For example, a study from Southern Ethiopia discovered that 334 (41.6%) of patients with TB symptoms did not receive sputum microscopic service to rule out Active TB infection.17 Another Ethiopian study also reported a high number of missed TB cases among admitted patients with other diseases.15
The Amhara region is one of the highest TB burden regions in Ethiopia with 61% TB case detection performance,17 falling short of the national TB case detection target of 75%2 and the 2030/5 targets of the end-TB program.18 The burden and the effectiveness of TB control program vary by zone and district. For example, East Gojjam Zone, one of the 15 zones in the Amhara Region, accounted for 13% of the regional TB burden and had the lowest TB case detection performance of any zone in the region (46%).19 Although there have been recent studies on the magnitude and geographic distribution of TB cases, as well as the barriers to TB case detection in the East Gojjam Zone, little is known about the contribution of missing opportunities for TB investigation.
As a result, the purpose of this study was to determine the magnitude of missing TB diagnostic tests in patients with suggestive TB symptoms and associated factors at public health facilities in the East Gojjam Zone of Northwest Ethiopia. The study is essential for improving decision-making among TB control programmers in order to improve the quality and performance of TB services. It can also be important literature in TB prevention and control.
Methods
Study Design and Settings
From January to April 2020, a multicenter facility-based cross-sectional study was conducted on 412 adults aged 18 and up who presented with symptoms suggestive of TB according to WHO criteria.19 The research was carried out in the East Gojjam Zone, one of the 15 zones that comprise the Amhara Regional State in Northwest Ethiopia. In 2019, the zone’s estimated population is 2,740,625 people, with approximately 85% of them living in rural areas. The zone spans 14,010 km2 and is divided into 19 administrative woredas (a third-level administrative hierarchy in Ethiopia). At the time of data collection, it had 517 public health facilities (406 health posts, 102 health centers, and nine hospitals). TB prevention and control activities are carried out in accordance with the national and WHO TB diagnosis and treatment manuals.19 Sputum smear microscopy is the primary TB diagnostic tool in all health facilities, and X-ray service is only available in hospitals as a backup TB diagnostic tool. All patients receive free TB diagnosis and treatment.16 Because health posts only provide TB prevention and treatment follow-up,19 only health centers (HCs) and hospitals are included in this study (Figure 1).
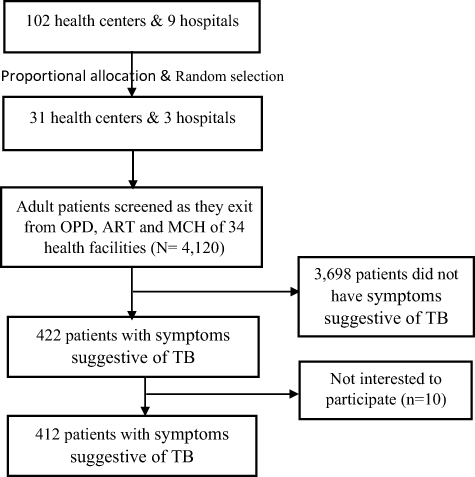 |
Figure 1 Diagram of sampling flow for missed opportunities of PTB cases in East Gojjam Zone, 2020. |
Source and Study Population
The source population for this study was all patients visiting 34 randomly selected public health facilities to seek healthcare services. The study population consisted of all patients aged 18 and up who visited the outpatient (OPD), anti-retroviral treatment (ART), and maternal and child health (MCH) units of those health facilities. Patients who had at least one symptom suggestive of TB according to WHO18 and Ethiopian national TB diagnosis and treatment criteria16 (cough for 2 weeks or more, night sweats, unexplained weight loss, fever for more than 2 weeks, fatigue, loss of appetite, and bloody sputum) were included in the study. Furthermore, for people on ART, we included patients with any duration of cough because HIV is a risk factor for Active TB infection due to a decline in human immune status.12 Patients who already gave sputum/chest X-ray for TB examination were excluded from the study. Accordingly, a patient who had at least one symptom suggestive of TB but did not receive sputum and/or x-ray evaluation to rule out TB was considered a missed opportunity for TB investigation.
Sample Size Determination and Sampling Procedure
The sample size (412) was calculated by Epi Info version 7 using a 95% confidence interval (CI), a 5% margin of error, a 42% proportion of patients with symptoms suggestive of TB, but not ruled out for TB17 and a 10% non-response rate. Due to time and resource constraints, we only used 30% of the 102 health centers and nine hospitals as study sites. As a result, we used a lottery to select 31 health centers and three hospitals. Then, all patients over the age of 18 from 34 health facilities with symptoms suggestive of TB were included in the study (Figure 1).
Data Collection
An exit interview was conducted by six trained data collectors (nurses and health officers) and three master-holder public health practitioners (supervisors). A structured questionnaire administered by an interviewer was used to collect data on demographics, TB symptoms, and other clinical data relevant to TB. Participants in the study were also asked if they had requested sputum and/or x-ray examination by healthcare workers for TB diagnosis during that visit. If sputum microscopy and/or x-ray were not requested, they were referred back to OPD for appropriate TB investigations. Because there was no access to culture and GeneXpert services during data collection, patients with suggestive TB symptoms were evaluated by sputum smear microscopy and chest X-ray. The diagnostic test procedures were carried out based on the Ethiopian National TB Diagnosis Guidelines adapted from the WHO TB Diagnosis Guidelines19,20 (Figure 2).
 |
Figure 2 Ethiopian national diagnostic algorithms for patients with presumptive TB, 2020. |
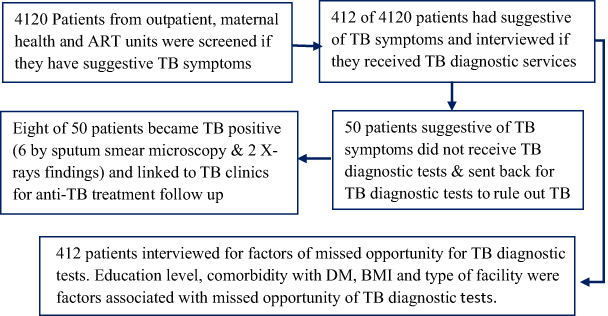 |
Figure 3 Graphic abstract of missed opportunity for TB diagnostic Tests in Ethiopia, 2020. |
Quality Control
The questionnaire was pretested in public health facilities with similar settings but not on study sites. Following two days of training, data collectors and supervisors participated in data collection. The data collector was closely supervised and supported by the principal investigator and supervisors. Data completeness and consistency were checked daily, with possible feedback to data collectors.
Data Analysis
Statistical Analysis for Social Sciences (SPSS) version 26 was used to enter, clean, and analyze the data. Various descriptive statistics, such as means and medians for continuous variables and frequencies and percentages for categorical variables, were computed. The proportion of missed opportunities for TB investigation was calculated by dividing the number of patients with TB symptoms who did not receive sputum and/or x-ray evaluations to rule out TB by the total number of patients with TB symptoms. Since the outcome variable was the number of missed opportunities for TB investigation (count data), we first proposed a Poisson regression analysis. The assumption checking step, on the other hand, revealed that the data were over-dispersed, with a deviation to the degree of freedom ratio of greater than one. As a result, we used bivariate and multivariable negative binomial regression analysis to find factors linked to the missed TB research opportunity, and control confounding effects, respectively. Steps with the lowest Akaike’s Information Criteria and Bayesian Information Criteria values were followed throughout the data analysis. As a result, a negative binomial regression analysis was carried out by selecting a “custom tab” from the model window type. We utilized a negative binomial model from the “Distribution” options, log from the connection function, and the “Estimate values” button in this stage. The statistical significance was determined at p-values <0.05, and the association was described using an adjusted incidence rate ratio (AIRR) at a 95% confidence interval (CI) (Table 1).
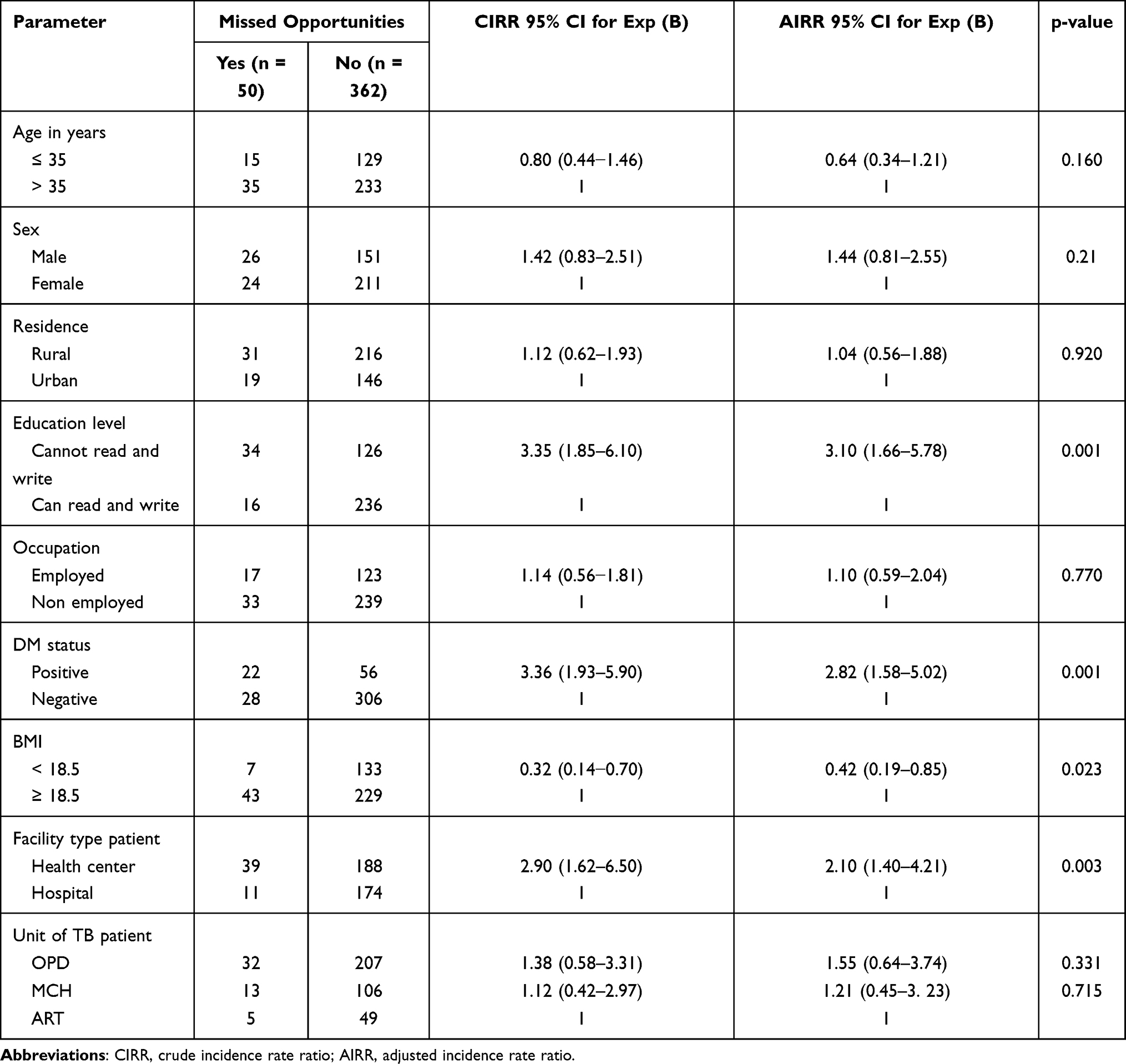 |
Table 1 Factors Associated with Missing to Get TB Diagnostics in East Gojjam Zone, Northwest Ethiopia, 2020 (N = 412) |
Ethical Considerations
The study was conducted according to the principles of the Declaration of Helsinki and fulfilled the Ethiopian National Health Research and Ethics Guideline. The ethical review committee of Bahir Dar University’s College of Medicine and Health Sciences approved the study protocol and gave ethical clearance (Protocol No: 091/18-04). The Amhara Regional Health Bureau and the East Gojjam Zone Health Department both sent letters of support. Prior to data collection, managers of district health offices and health facilities were contacted and informed. All study participants provided informed consent, and participation was entirely voluntary. Data confidentiality was ensured by removing personal identifiers from the data and restricting it with a password. All patients who tested positive for TB were referred to TB clinics for anti-TB treatment monitoring and HIV screening. Families of TB positive cases were advised to visit health facilities to check their TB status.
Results
Characteristics of the Respondents
From a total of 4120 screened adult patients who visited 33 public health facilities, 412 (10%) had symptoms suggestive of TB and were included in the analysis with a 100% response rate (Figure 1). The average age was 35 ± 8 SD years, and 235 (57%) were females. Over half of the patients, 239 (58%) were from the outpatient department. Significant number of patients interviewed; 247 (60%), 252 (61%), and 272 (66%) were from rural areas, not able to read and write and unemployed, respectively (Table 2).
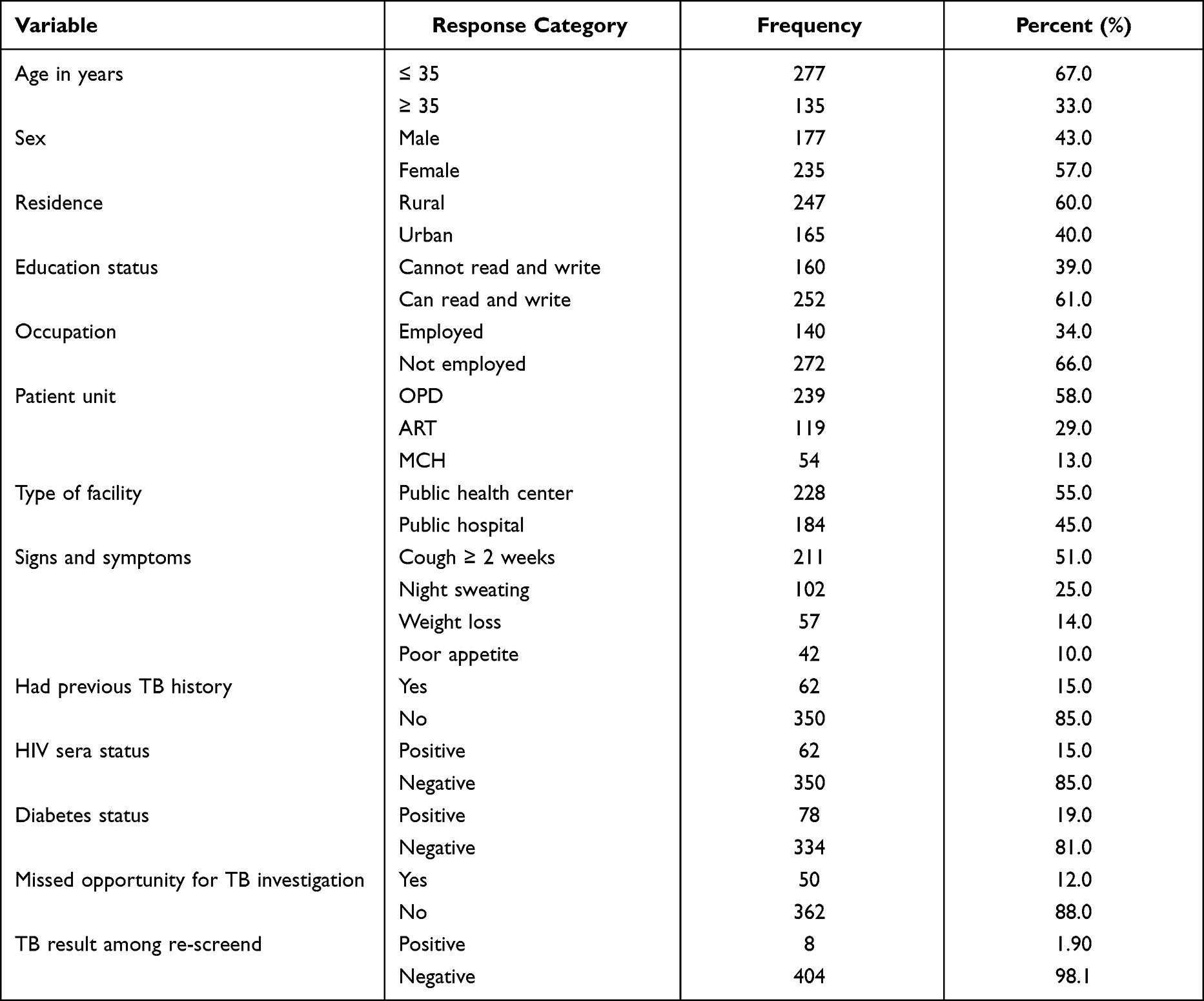 |
Table 2 Socio-Demographic Characteristics of Patients with Symptoms Suggestive of PTB in East Gojjam Zone, Northwest Ethiopia, 2020 |
Missed Opportunities for TB Investigation
Out of the 412 patients interviewed, 50 (12%) did not have a sputum and/or x-ray evaluation to rule out TB. Over half, 211 (51%), of the interviewed patients had coughing that lasted for more than two weeks. The proportion of missed TB cases among re-screened patients was 8 (1.90%); six TB cases were detected by sputum smear microscopy and two by chest x-ray (Table 2).
Factors Associated with Missed Opportunities for TB Investigation
According to a multivariable negative binomial regression analysis, patients who cannot read and write were three times more likely to be missed for TB diagnostic tests than patients who can read and write; AIRR = 3.10, 95% CI = 1.66–5.78. Diabetes mellitus (DM) patients were more than twice as likely as control patients to miss TB diagnostic tests; AIRR = 2.82, 95% CI = 1.58–5.02. Similarly, patients who visited health centers were twice as likely as patients who visited hospitals to be missed for TB diagnostic tests; AIRR = 2.10, 95% CI = 1.40–4.21. Patients with less than 18.5 BMI were 58% less likely to miss TB diagnostic tests than patients with greater than or equal to 18.5 BMI; AIRR = 0.42, 95% CI = 0.19–0.85 (Table 1).
Discussion
Early identification and treatment of infectious TB cases is a primary strategy for TB control programs worldwide.2,11,14 As a result, improving the performance of TB case detection (both active and passive) is critical for reducing TB transmission and burdens.11,14,21 Taking this concept into consideration, this study attempted to assess the quality of facility-based TB case detection activity by estimating the number of patients who had suggestive of TB symptoms but were missed for TB diagnostic tests to rule out TB infection. According to the findings of this study, 50 (12.14%) of patients with at least one TB symptom did not receive TB diagnostic services. This implies that health facilities are missing a significant number of potential TB casesas a result of weak TB case finding processes. This could be attributed to low healthcare worker knowledge and skills in TB investigation,2,15,21 no or limited TB diagnostic services,5,9,17,21 low patient knowledge of TB symptoms,2,17,22 limited refreshment training for healthcare workers2,6,16 and patient load in each working unit.2,21,22 Moreover, giving more emphasis to COVID-19 that has nearly similar symptoms to TB, particularly coughing, might have contributed to missing to offer TB diagnostic tests for patients coming with coughing for a certain duration.23,24
This finding was found to be lower than evidence from the Southern7,17 and Eastern10 parts of Ethiopia, where 41.6%, 39% and 35.2% of patients with suggestive of TB symptoms did not receive TB diagnostic tests to rule out TB infection, respectively. Similarly, this finding was lower than study findings from other countries, which reported 56%,14 16%, 33.5%25 and 75%26 missed opportunities for TB diagnostic tests. This disparity may be due to differences in study periods that are directly related to TB control program interventions. The most important point to note here is that, despite being smaller in size than previous studies, there are still significant gaps in these health facilities’ TB case-finding practices that require timely action to improve the performance of TB case-finding activities there.
Based on our rescreening process, eight patients tested positive for TB in their sputum evaluation due to gaps in the current TB case finding strategy. This occasion increased the transmission and burdens of TB. This figure is slightly lower than findings from the previous Ethiopian studies, which included 11 TB cases from the Kaffa zone,17 10 TB cases from Oromiya region hospitals,15 and 11 TB cases from systematic and meta-analysis studies.27 Similarly, it is lower than findings from Ghana28 that reported 27 missed TB cases from 410 TB suspects and 95 TB cases among 543 TB suspected patients in South Africa.29 The difference in sputum sample evaluation could be due to the fact that previous studies used GeneXpert, which has higher sensitivity to detect TB cases than sputum smear evaluation.
According to the negative binomial regression analysis, variables such as being unable to read and write, being a DM patient, and attending a health center had positive associations with failing to obtain TB investigation tests. Having a lower BMI, on the other hand, was inversely related to the likelihood of missing TB investigation tests.
Patients with no education were three times more likely to be missed for sputum smear and/or chest X-ray services to rule out active TB infection than patients who could read and write. This could be due to patients’ lack of understanding and inability to describe TB symptoms they experienced. This is due to the fact that illiterate patients are unable to easily search for the literature and understand the messages.
Similarly, the type of health facility was found to be statistically significant in terms of missed opportunities for TB diagnostic tests. The likelihood of being missed for Active TB infection investigation was twice as high among patients who went to health centers as it was among patients who went to hospitals. This is also supported by findings from previous studies.2,21,25,28 This is due to the availability of relatively better TB diagnostic tests, experienced staff (physicians and laboratory technologies), and less interrupted electric power in hospitals than in health centers in developing countries, including Ethiopia.2,17,21,26 According to previous studies, a better facility has a direct relationship with better TB case finding performance.5,6,26
Moreover, comorbidity infection was associated with a missed opportunity to obtain TB diagnostic tests. In contrast to previous study findings that reported a positive association between diabetes and active TB infection,3,30 the likelihood of missing TB diagnostic tests was three times higher in DM patients compared to counterpart patients. This is not to say that there is no scientific link between TB and DM,2,3,9,22 but our goal is to examine healthcare workers’ practices in offering TB diagnostic tests to patients with symptoms suggestive of TB infection. The reason for this association could be related to healthcare workers paying less attention to comorbidity investigations among patients. They may simply accept symptoms and investigations of DM that mask symptoms of TB, resulting in less attention to TB.
Furthermore, patients with a BMI of less than 18.5 were 58% less likely to miss TB diagnostic tests than patients with a BMI greater than or equal to 18.5. Previous research15,31 found an inverse relationship between BMI and TB infection. Low BMI may result in active TB infection due to immune declination, and TB may result in poor dietary intake and thus low BMI.31 Additionally, weight loss and loss of appetite are two suggestive symptoms of Active TB infection.14 Hence, health workers working at OPD, MCH and ART rooms might suspect patients with lower BMI for TB since they are most susceptible to acquiring TB infection.
Despite its strengths and best efforts to maintain its quality, this study has some limitations that may have a minor impact on the quantity and quality of research findings. This was a cross-sectional study that did not demonstrate causality. Because the study was conducted among patients visiting health facilities, it may not accurately represent the magnitude at the community level (difficulty of generalizing). In addition, when compared to GeneXpert and culture, using only sputum smear microscopy and X-ray diagnostics to rule out Active TB infection has low sensitivity, resulting in missed detection of potential TB cases. Moreover, recall bias among patients on identifying types of TB symptoms might increase the chance of missing TB cases at OPD and during our re-screening process.
Conclusion and Recommendations
This study found a significant number of missed opportunities for TB diagnostic tests as well as significant infectious TB cases during the rescreening process. According to this study, being illiterate, having diabetes, being undernourished, and seeking healthcare services from health centers rather than hospitals were statistically significant factors in missed opportunities for TB diagnostic tests among patients with at least one suggestive of TB symptom recommended by the WHO (Figure 3). Improving healthcare workers’ skills in TB diagnosis and treatment through in-service training and making TB diagnosis and treatment guidelines available in each unit is critical for improving the performance of passive TB case-finding practices. Conducting TB screening among patients with other diseases, such as HIV, diabetes, and malnutrition, as well as paying special attention to illiterate people while conducting a clinical diagnosis, is critical for improving TB case-finding performance. Furthermore, a community-based mixed study is recommended to better estimate missed opportunities for TB diagnosis using advanced diagnostic tests and to investigate barriers that result in the missed of potential TB cases.
Abbreviations
AIRR, adjusted incidence rate ratio; ART, anti-retroviral treatment; BMI, body mass index; CI, confidence interval; DM, diabetes mellitus; HCs, health centers; HIV, human immune deficiency virus; TB, tuberculosis; MCH, maternal and child health; OPD, out-patient department; SD, standard deviation; SPSS, Statistical Package for Social Science; WHO, World Health Organization.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The researcher would like to express his heartfelt gratitude to Bahir Dar University for covering the data collection budget. The author also expressed gratitude to TB program officers, PTB patients, data collectors, and supervisors for their invaluable supports during data collection.
Funding
Bahir Dar University covered the budget for data collection (Grant No: RCS/254/09), but the University has no any technical role in the research processes.
Disclosure
The author reports no conflicts of interest in this work.
References
1. World Health Organization. Global Tuberculosis Report 2021. Geneva: World Health Organization; 2021.
2. Asemahagn MA, Alene GD, Yimer SA. A qualitative insight into barriers to tuberculosis case detection in East Gojjam Zone, Ethiopia. Am J Trop Med Hyg. 2020;103(4):1455–1465. doi:10.4269/ajtmh.20-0050
3. Dousa KM, Hamad A, Albirair M, et al. Impact of diabetes mellitus on the presentation and response to treatment of adults with pulmonary tuberculosis in Qatar. Open Forum Infect Dis. 2019;6(1). doi:10.1093/ofid/ofy335
4. Gelaw YA, Williams G, Soares Magalhaes RJ, Gilks CF, Assefa Y. HIV prevalence among tuberculosis patients in Sub-Saharan Africa: a systematic review and meta-analysis. AIDS Behav. 2019;23(6):1561–1575. doi:10.1007/s10461-018-02386-4
5. Asemahagn MA, Alene GD, Yimer SA. Geographic accessibility, readiness, and barriers of health facilities to offer tuberculosis services in East Gojjam Zone, Ethiopia: a convergent parallel design. Res Rep Trop Med. 2020;11:3–16. doi:10.2147/RRTM.S233052
6. Cazabon D, Alsdurf H, Satyanarayana S, Nathavitharana R, Subbaraman R, Daftary A. Quality of tuberculosis care in high burden countries: the urgent need to address gaps in the care cascade. Int J Infect Dis. 2017;56:111–116. doi:10.1016/j.ijid.2016.10.016
7. Dangisso MH, Datiko DG, Lindtjørn B. Accessibility to tuberculosis control services and tuberculosis programme performance in southern Ethiopia. Global Health Action Dec. 2015;8(1):29443. doi:10.3402/gha.v8.29443
8. Neshati H, Sheybani F, Naderi H, Sarvghad M, Soltani AH, Efterkharpoor E. Diagnostic errors in tuberculosis patients: a multicenter study from a developing country. J Environ Public Health. 2018;2018:11. doi:10.1155/2018/1975931
9. Asres M, Gedefaw M, Kahsay A, Weldu Y. Patients’ delay in seeking health care for tuberculosis diagnosis in East Gojjam Zone, Northwest Ethiopia. Am J Trop Med Hyg. 2017;96(5):1071–1075. doi:10.4269/ajtmh.16-0892
10. Dabaro D. Factors affecting tuberculosis case detection in Kersa woredas, South West Ethiopia. J Clin Tubercu Mycobact Dis. 2017;9:1–4. doi:10.1016/j.jctube.2017.08.003
11. Pande T, Vasquez NA, Cazabon D, et al. Finding the missing millions: lessons from 10 active case finding interventions in high tuberculosis burden countries. BMJ Global Health. 2020;5(12):e003835. doi:10.1136/bmjgh-2020-003835
12. World Health Organization. Global Tuberculosis Report 2020. Geneva; 2020.
13. Getnet F, Demissie M, Assefa N, Mengistie B, Worku A. Delay in diagnosis of pulmonary tuberculosis in low-and middle-income settings: systematic review and metaanalysis. BMC Pulm Med. 2017;17(1):202. doi:10.1186/s12890-017-0551-y
14. Kakame KT, Namuhani N, Kazibwe A, Bongomin F, Baluku JB, Baine SO. Missed opportunities in tuberculosis investigation and associated factors at public health facilities in Uganda. BMC Health Serv Res. 2021;21(1):359. doi:10.1186/s12913-021-06368-6
15. Assefa D, Belachew F, Wondimagegn G, Klinkenberg E. Missed pulmonary tuberculosis: a cross sectional study in the general medical inpatient wards of a large referral hospital in Ethiopia. BMC Infect Dis. 2019;19(60). doi:10.1186/s12879-019-3716-x
16. Asemahagn MA, Alene GD, Yimer SA. Tuberculosis infectious pool and associated factors in East Gojjam Zone, Northwest Ethiopia. BMC Pulm Med. 2019;19(1):229. doi:10.1186/s12890-019-0995-3
17. Abayneh M, HaileMariam S, Asres A. Low tuberculosis (TB) case detection: a health facility-based study of possible obstacles in Kaffa Zone, Southwest District of Ethiopia. Can J Infect Dis Med Microbiol. 2020;2020:9. doi:10.1155/2020/7029458
18. World Health Organization. The end TB strategy: global strategy and targets for tuberculosis prevention, care and control after 2015. World Health Organization; 2015.
19. Amhara National Regional State Health Bureau. The 2018/19 annual performance report of Amhara National Regional State Health Bureau. Bahir Dar; 2019.
20. Ministry of Health-Ethiopia. Guidelines for Clinical and Programmatic Management of TB, TB/ HIV, DR-TB and Leprosy in Ethiopia.
21. Hanson C, Osberg M, Brown J, Durham G, Chin DP. Finding the missing patients with tuberculosis: lessons learned from patient-pathway analyses in 5 countries. J Infect Dis. 2017;216(S7):S686–95. doi:10.1093/infdis/jix388
22. Asemahagn MA. Are shopkeepers suffering fromTB infection in Bahir Dar City, Northwest Ethiopia. Tuberc Res Treat. 2017;2017(7):2569598. doi:10.1155/2017/2569598
23. Arega B, Negesso A, Taye B, et al. Impact of COVID-19 pandemic on TB prevention and care in Addis Ababa, Ethiopia: a retrospective database study. BMJ Open. 2022;12(2):e053290. doi:10.1136/bmjopen-2021-053290
24. Odume B, Falokun V, Chukwuogo O, et al. Impact of COVID-19 on TB active case finding in Nigeria. international union against tuberculosis and lung disease health solutions for the poor. Public Health Action. 2020;10(4).
25. Miller AC, Polgreen LA, Cavanaugh JE, Hornick DB, Polgreen PM. Missed opportunities to diagnose tuberculosis are common among hospitalized patients and patients seen in emergency departments. InOpen forum infectious diseases 2015. Open Forum Infect Dis. 2015;2(4). doi:10.1093/ofid/ofv171
26. Amenuvegbe GK, Francis A, Fred B. Low tuberculosis case detection: a community and health facility based study of contributory factors in the Nkwanta South district of Ghana. BMC Res Notes. 2016;9(1):330. doi:10.1186/s13104-016-2136-x
27. Arega B, Tilahun K, Minda A, Agunie A, Mengistu G. Prevalence rate of undiagnosed tuberculosis in the community in Ethiopia from 2001 to 2014: systematic review and meta-analysis. Archives Public Health Dec. 2019;77(1):1–7.
28. Der JB, Grint D, Narh CT, Bonsu F, Grant AD. Where are patients missed in the tuberculosis diagnostic cascade? A prospective cohort study in Ghana. PLoS One. 2020;15(3):e0230604. doi:10.1371/journal.pone.0230604
29. Mohr E, Daniels J, Muller O, et al. Missed opportunities for earlier diagnosis of rifampicin-resistant tuberculosis despite access to Xpert® MTB/RIF. Int J Tuberc Lung Dis. 2017;21(10):1100–1105. doi:10.5588/ijtld.17.0372
30. Hermosilla S, You P, Aifah A, et al. Identifying risk factors associated with smear positivity of pulmonary tuberculosis in Kazakhstan. PLoS One. 2017;12(3):e0172942. doi:10.1371/journal.pone.0172942
31. Casha AR, Scarci M. The link between tuberculosis and body mass index. J Thorac Dis. 2017;9((3):E301–E303. doi:10.21037/jtd.2017.03.47)
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.