Back to Journals » International Journal of Women's Health » Volume 15
Misconceptions About Female Cancers Contributing to Late Presentation to Health Facilities in Ethiopia: A Qualitative Study
Authors Solomon K, Tamire M, Solomon N ![]() , Bililign N
, Bililign N ![]() , Kaba M
, Kaba M ![]()
Received 2 November 2022
Accepted for publication 3 February 2023
Published 15 February 2023 Volume 2023:15 Pages 299—309
DOI https://doi.org/10.2147/IJWH.S395824
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Kalkidan Solomon,1 Mulugeta Tamire,1 Nahom Solomon,2 Nigus Bililign,3 Mirgissa Kaba1
1Department of Preventive Medicine, School of Public Health, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Public Health, School of Public Health, College of Medicine and Health Sciences, Mizan Tepi University, Mizan-Aman, Ethiopia; 3Department of Midwifery, School of Midwifery, College of Health Sciences, Woldia University, Woldia, Ethiopia
Correspondence: Kalkidan Solomon, Email [email protected]
Introduction: Morbidity and mortality from female cancers is a major public health problem in low- and middle-income countries, including Ethiopia. More than three quarters of women visiting health facilities are diagnosed with late-stage cervical and breast cancer. Evidence reveals that misconception affects timely health seeking behavior which could have averted expensive treatment and poor survival. This study aimed to explore misconceptions about female cancers that may have contributed to late presentation of the problem to health facilities in Sidama region, Ethiopia.
Methods: A descriptive qualitative study was carried out in June 2021. Nine focus group discussions (six with women and three with men) and 14 key informants were conducted. Data were collected using interview guide until all information get saturated. Data were inductively coded and qualitative content analysis was applied.
Results: A total of 63 (24 men and 39 women) people participated in this study. Nearly all (12) key informant interviewees have awareness about cervical and breast cancer, yet reported that their community members clearly lack awareness and they are working to improve misconceptions regarding cervical and breast cancer. The focus group discussion participants (15 men and 36 women) reported lack of detailed information related to cervical and breast cancer. Women believe that cervical and breast cancer mainly resulted from poor hygiene, trauma, having multiple sexual partners, early marriage, breast exposure to heat, not breast feeding, birth complication, urinating in the sun, hereditary, devil’s intrusion and God’s punishment.
Conclusion: There were misconceptions among the community on what cervical and breast cancer mean, how they could happen, what the symptoms are, why and when to screen, when to seek health care and how to use modern treatment options. Therefore, we recommended the design of social and behavioral change strategies to address the misconceptions among different population groups.
Keywords: female cancer, breast cancer, cervical cancer, misconception
Introduction
Female cancer (FC) morbidity and mortality is a major public health problem in most developing countries. Cervical and breast cancer are the most frequent cancers in women, globally.1 About 9 in 10 deaths from them occurred in low- and middle-income countries.2,3 The high mortality rate from it globally could be due to lack of a comprehensive approach on prevention, early diagnosis, screening and treatment programs.4 Globally, more than three quarters of patients are presented and diagnosed at a late-stage (stages III and IV) of cervical and breast cancer.2,5
According to the estimate of GLOBOCAN, 7% of the incidence and 9% of the mortality globally occurs in Africa and breast cancer is the leading cause of death followed by cervix uteri cancer in Ethiopia.6 In the presence of this problem, cancer programs were not strong in Ethiopia until recently and early diagnosis and treatment was probably an exception. The first ever strategy to control cancer in Ethiopia was developed in 2016 and focused on early detection, diagnosis and treatment, palliative care, cancer surveillance and research.7 The strategy gives prominence to public awareness creation to early detection,treatment and prevent the disease.
Misconception is one of the barrier for early detection and treatment.8 Evidence reveals that there are misconceptions on the causes and means of prevention of female cancers that affect early presentation to health facilities.8 The most common myths and misconceptions among women include the fear of being considered as a prostitute if found positive for screening, the instruments used for screening were painful and that cancer results from a satanic curse.8–10 A study in south western (Jimma) and central Ethiopia (Addis Ababa) showed very low levels of awareness among people on cervical and breast cancer.11 Studies reveal that a community’s awareness on cancer, by explaining the symptoms, risk, treatment and preventive procedure of female cancers, could help to avoid misconceptions.11–14
Through this study, we have explored the common misconceptions about cervical and breast cancer that might have contributed to late presentation of the cases to health facilities in Sidama region, Ethiopia. Hence, we believed that, the generated evidence could support interventions for this severe public health issue.
Method
Study Area and Period
The study was conducted in three districts of the Sidama region (Loka Abaya, Dale and Yirgalaem) in June 2021. The three districts were operational sites of the Ethiopian Female Cancer Initiative implemented by Beza for Generation, a local non profit organization with financial support from Catholic Organization for Relief and Development Aid (Cordaid) and technical support from the School of Public Health, Addis Ababa, Ethiopia.
Study Approach
A qualitative study was carried out in June 2021 in Sidama, Ethiopia and an explorative approach was followed to identify prevailing and hidden misconceptions about female cancers among the community members and draw the inherent meaning.
Study Participants
For the focus group discussions (FGDs) the study participants were of both sexes, above 18 years and purposively selected. Key informant interviews (KIIs) were conducted with the regional non communicable disease (NCD) unit, maternal and child health (MCH) unit, gynecologist, trained health professional, community leaders, and religious leaders.
Data Collection Tool and Procedures
A total of 63 people (24 men and 39 women) participated in this study Nine focus group discussions (FGDs); six FGDs with women, and three FGDs with men and 14 key informant interviews (KIIs) were conducted. Each FGD comprised of six to eight participants. KIIs were conducted with the regional non communicable disease (NCD) unit, maternal and child health (MCH) unit, gynecologist, trained health professional, community leaders, religious leaders, and community based structure (“Idir”) chairpersons. The village facilitators and supervisors helped to identify the study participants in the study area who met the eligibility criteria and those who had an opinion on the topic that they were willing to share. An interview (discussion) guide that had all the important issues related to breast and cervical cancer misconceptions in the form of open-ended questions was used to fully explore the gaps. Study participants had the discussion and interview in a separate room in order to be more neutral and to make the participants more comfortable.
The interview (discussion) guide was prepared in English and translated to Amharic and Sidamic language by a professional translator. Following the right procedures, data were collected until information redundancy was seen relative to prior data. The interviews were tape-recorded with the participants’ permission and field notes were taken by the interviewer (moderator) during the interview and discussion not to miss any information, facial cues and emotion during the interviews. The interviews and discussions were carried out by six experienced and trained data collectors and carried out in places where it was convenient and secure for study participants. The principal investigator and supervisors closely followed the data collection.
Trustworthiness
In order to ensure the credibility of the findings, experienced qualitative researchers led the team and appropriate discussions and debriefings were undertaken. Researchers’ knowledge and experience on female cancers, application of appropriate procedures such as; creating trust, thick description, audit trial, proper documentation and comments from qualitative study experts helped to ensure the credibility, dependability, confirmability and transferability of this study. Furthermore, data were gathered from different types of participants at different times. The researcher's (KS) initial coding and reliability check was done by another team member (MT and NS).
Data Analysis
Information in the audio recorders and field notes were stored in a separate file on a daily basis. Field notes were expanded and records were transcribed verbatim. After transcription was complete, the researchers independently read sample transcripts to ascertain consistency. Whenever differences were noted discussions were made to clarify. The researchers re-examined the whole and parts of the text to gain deeper comprehension of the emerging themes, codes and categories. Themes and sub-themes were developed to categorize the raw data and eventually interpretations and meanings were developed within the rubric of the original data (Table 1). Data were inductively coded and qualitative content analysis was applied to analyze and interpret the findings. ATLAS.ti version 9 software was used for both data reduction and analysis and the study was reported following the Standards for Reporting Qualitative Research (SRQR) guideline.
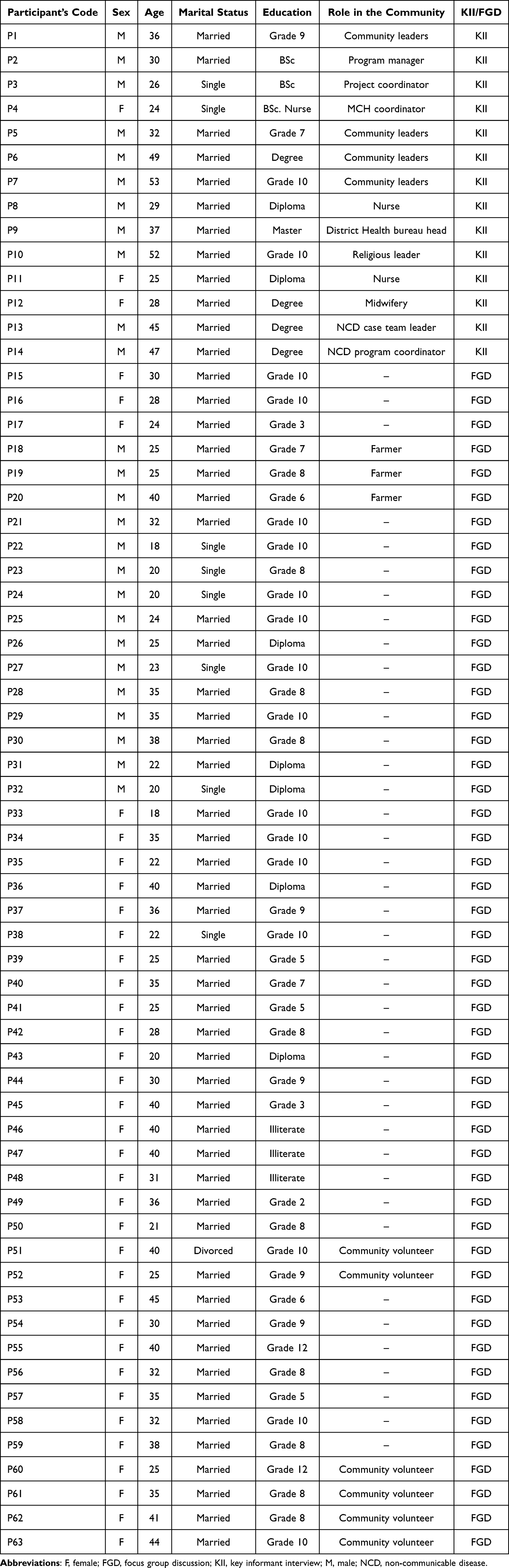 |
Table 1 Socio-Demographic Characteristics of Study Participants |
Results
The majority of men were married, illiterate and farmers. Almost all FGD women participants were married, most of them were housewives and some of them had completed at least elementary school (Table 1). The findings are presented in six categories; awareness about female cancers, causes of female cancers, symptoms of female cancers, misconceptions around screening, misconceptions which affect modern treatment seeking behavior and suggested action.
Awareness about Female Cancers
The KII participants have experiences of different training and working on female cancers, and they explained what female cancer means and mentioned some kinds of female cancers. On the other hand, FGD participants (both sexes) responded that they lack detailed information about female cancers and described female cancers as serious cases which are mostly fatal unless they get treated in a timely fashion. All participants reported breast cancer and cervical cancer to be the most commonly known cancers for females.
Cancer is not something that can be seen rather that can be known by getting screened. It’s not transmitted for person to person rather it’s known by only getting screened. (30-year-old female FGD participant)
Mothers when their breast swells, they visit traditional healers. Once it takes its root in the body, it won’t come out completely. I knew three people who were following their cervical cancer treatment who eventually died. This disease is fatal and merciless. (28-year-old female FGD participant)
More than half of the study participants reported that they heard about female cancers from friends, neighbors, health professionals and media but lack clear information on its mode of transmission.
We hear it on TV on news when the kids open it, since on TV it is mentioned about cervical cancer. (42-year-old female FGD participant)
Causes of Female Cancers
Most of the participants reported early marriage, failing to breast feed after giving birth, and trauma as causes of breast cancer. There was also a reflection as breast cancer might result from the exposure of the breast to heat, perfumes and oils. The following quotes are parts of the responses from participants.
I think it’s mostly due to fire (the heat) most woman who prepare injera are expose to the fire (the heat) and I think that is the cause. When they are preparing injera the fire (the heat) rest on their chest and then their breast so I think this is how it happens. (25-year-old female FGD participant)
I think breast cancer can cause by getting married early, which we couldn’t handle it but this results breast cancer. (21-year-old female FGD participant)
Most reported early marriage, having multiple sexual partners, lack of hygiene, blood contact, birth related complications, abnormal uterine bleeding or heavy menses, hereditary, alcohol, and cigarette smoking, history of female genital mutilation, the devil’s intrusion, exposure to the sun’s rays, urinating on stone when it was sunny, and sitting on a seat heated by the sun as causes of cervical cancer. Most discussants believed that if a woman gets married at an early age, like in her 12th year, she may face damage to her genitalia and that could lead to cervical cancer. Explaining the reason how a woman may develop the cancer, they have reported that it is because a very young girl’s organ is not well developed and may be traumatized during sexual intercourse and delivery, and that may result in occurrence of cervical cancer.
When the young women deliver their cervix could be injured because the body at young is not yet fully developed to handle the pain of the cervix which could be injured leading to cancer. (25-year-old female FGD participant)
I heard that if a woman sits to urinate during sunny time and also if she sit on a rock which was exposed to the sunlight the uterus will be inflamed and if she rubs it it will be a lesion to change into cervical cancer, I even know the person who has it. (25-year-old male FGD participant)
A few participants thought that cervical cancer was due to trauma to the female genitalia from friction during coitus. They believed that a large penis size causes more trauma and therefore increases the female sexual partner’s risk of developing cervical cancer.
I believe the cause of cervical cancer is having multiple sexual partner and also having sex with men with large penus this may result in tear on the genitalia and later on changed to cancer. (31-year-old female FGD participant)
Symptoms of Female Cancers
More than half of the study participants stated that itching, pussy discharge and swelling as common symptoms for breast cancer. A few mentioned only breast swelling as a symptom of breast cancer.
My sister had the case, you know what it is solid largely swelled on her breast and it is very itchy. (22-year-old male FGD participant)
Vaginal bleeding, foul smelling vaginal discharge, itching of genitalia and back pain were reported as symptoms of cervical cancer. Secondary infertility, leg pain, and repeated abortions were also perceived as the manifestations of cervical cancer by most of the study participants.
Cervical cancer results from small wound around the genital area and that wound will grow and it is itching and has smelly discharge becomes cervical cancer gradually. She may have back pain in addition. (19-year-old female FGD participant)
…I heard that one of the manifestations of cervical cancer is unable to give birth after developing the disease. (33-year-old female FGD participant)
Female Cancer Screening
The majority of the respondents were aware of existing screening services for cervical cancer and examinations for breast cancer. Most of the participants, including those who had been screened for cervical cancer or breast cancer or both, had no detailed information on how frequently screening should be done, the recommended age, and target group. Also they had a misunderstanding on the adverse impact over the benefit. They explained their views as below.
I heard about cervical cancer screening service during community education but I did not screen. Because, I am afraid that when a screener does screening I may develop infertility. (22-year-old female FGD participant)
…As I heard it from my friend there is large metal inserted to uterus and it is very painful, cold and results infection and sexual dysfunction. My friend’s wife got screened for cervical cancer and as he told me she stops sexual contact onwards from that. (55-year-old male FGD participant)
With regard to why women in the community may not be screened for female cancers; lack of awareness about the screening service, low family support, and myths were mentioned by some of the participants.
In our community it is believed that those who are not virgin are eligible for the cervical cancer screening so I want to screen but I am afraid of that my friends and also my families may consider me as I have multiple sexual partners which is a taboo here…. I do not know about breast cancer screening. (31-year-old female FGD participant)
Female Cancer Treatment
Modern treatment is believed to be helpful by most of the screened women, treated patients, their husbands and key informants. They have expressed their willingness to promote it and women also report that they would utilize the service as needed.
From my experience cervical cancer is very devastating disease, that I had a lot of smelly vaginal discharge, back pain, and abdominal pain. But when I got screened, fortunately I got screened after it became cancer then they referred me to Black Lion Hospital, Addis Ababa and I got treated with chemotherapy and radiotherapy since years before and now even. I got cured of the symptoms and able to live my usual life. Those who deny the treatment and stayed home unknowingly might die. I know it’s fatal. (57-year-old female FGD participant)
Although women believe that getting medical support is beneficial, they did not deny that service utilization is not at the expected level. The reason behind underutilization among community members was related to fear of side effects and fear of talking about genital issues as preferring to keep the disease a secret as it was a personal issue and a very few associating it with the devil's intrusion and God’s punishment for having multiple sexual partners.
There might be restriction for having sexual intercourse with the appointment….it could be two month or a year after treating for cervical cancer, so It’s going to make things worse by adding another burden on my marriage life thus I am not willing to take the treatment. (36-year-old female FGD participant)
Even in breast cancer having one breast and trying to raise a baby, being disabled and it might even pass to the other one that is also a side effect. (18-year-old female FGD participant)
A very few participants also reported that community members prefer traditional remedies and religious actions would be more effective treatment for cancer than the modern medical journey.
The community believed that traditional treatments are more effective than modern ones. The trend here is they visit traditional healers and they spit the traditional medicine to the swelled breast and eventually they got cured. (50-year-old male Idir leader KII participant)
Suggested action to mend misconceptions about Female Cancers
More than half of the participants and almost all key informants suggested a new attractive and persuasive awareness creation program, strengthening and expanding existing community conversation sessions, counseling services before screening, advertisement about the availability and benefit of screening through mass media platforms, addressing the issues through religious and community leaders during events like holidays, (social event) and market to address misconceptions in the community and to raise the community's awareness about female cancers.
Faith based organizations, social structures, and other educational institutions should work on raising awareness starting from lower level like in schools. It’s essential to address why, how and where it comes from. (30-year-old male KII participant)
Adequate and right information should be provided on community conversation session, TV and radio. Community and religious leaders should pay due attention to the problem and work on prevention, creating awareness. (29-year-old female woreda health office head KII participant)
Discussion
Our findings showed limited awareness about female cancers among the study participants despite the fact that both cervical and breast cancer were found to prevail in the area. Participants generally considered both cancer as serious and fatal. This is not unique as a previous study conducted in Ethiopia also reported a lack of awareness about breast cancer at community level.15 Another community based study has also reported poor comprehensive knowledge about cervical cancer among reproductive age group in northwest Ethiopia16 which is reported in other countries as well.8,17–20
The prevailing misconceptions regarding the causes of cervical and breast cancer are not surprising when awareness about female cancers remains poor. In this study using perfumes was reported to be a risk factor for breast canceryet, another study indicated the use of perfumes or deodorants to not to be a risk for breast cancer.21 Lack of personal hygiene, early marriage and early cessation of breast feeding were reported to be risk factors of breast cancer, likewise in other studies lack of personal hygiene or not taking a bath properly were listed as risk factors for breast cancer.6 Though null parity was identified as a risk factor for the breast cancer development,22 a dominant view about early cessation of breast feeding as a risk factor among the participants of this study should be treated based on the context. Firstly, the Ethiopia Demographic and Health Survey 2016 reported that over 90% of mothers in Ethiopia breast feed their children up to 17 months and 76% until 24 months.23 Secondly, for a rural woman, who has not been employed and usually stays at home with their children, over emphasizing on this risk factor could undermine the understanding of real risk factors of the problem.
Regarding cervical cancer, the common misconceptions were the devil’s intrusion, exposure to the sun’s rays, urinating on stone when it was sunny, and sitting on a stone heated by the sun. Some of these misconceptions around cervical cancer were also consistent with findings from previous studies, which reported the societal beliefs and understandings about the cancer.24,25 For instance, in line with the devil’s intrusion as a cause for cervical cancer in this study, a study from Nigeria reported that cervical cancer could result from wizardry.8
While the discussants were reflecting on their understandings on how early marriage is linked with cervical cancer, for example, they repeatedly stated that trauma during sexual intercourse and delivery will lead to the disease as they are not well developed. However, it is not the wound or other forms of the trauma that are associated with early sexual exposure and cervical cancer, but rather by early events in a woman’s sexually active life that modify the cancer causing potential of human papilloma virus (HPV) infections.26 In the same way, they link the exposure to having multiple sexual partners as the supernatural punishment instead of exposure to the HPV virus, which has been implicated to 99.7% of cervical squamous cell cancer cases worldwide.27 Consistently, a study conducted among educated women in Togo found misconceptions about cervical cancer and its risk factors were similar with what was explained from this study's participants.17 This might indicate that misunderstandings or limited knowledge could exist among women and even among well-educated people unless the misconceptions are targeted and solved. Hence, there is a need to address the myths and misconceptions around female cancers with evidence based social and behavioral change communication interventions to counter them.
Discussants could not explain the signs and symptoms of cervical cancer correctly other than mentioning some of them, like vaginal discharge and bleeding. This aligns with a quantitative study conducted in Zimbabwe, where a majority of the study participants were not familiar with the signs and symptoms of cervical cancer.18 Lack of adequate awareness about the signs and symptoms of female cancers could also result in delayed screening as the women might assume that they had no health problem as identified by previous studies.28,29 Very few also correctly stated that itching, pussy discharge and swelling as common signs and symptoms for breast cancer.
In addition to the misconceptions, the lack of detailed information about the screening services, including the duration, proper age group and even the benefits of being screened were reported in our study. This might directly affect the utilization of the screening service even though it is available for free for females in the community. Researchers in Jamaica also found that women who were reported to have poor knowledge about the Pap smear test were 85% less likely to have ever had the test.30 This could be worse in rural areas where the women might have limited exposure to mass media and not frequently travel to the health facilities, which could result in a lack of awareness and low health literacy. However, the awareness about the availability of screening service and the number of participants with their or their spouse’s screening practice was found to be more widely reported for cervical cancer in this study. Similarly, findings from a survey involving three different regions in Ethiopia also reported that the number of women who had heard about cervical cancer screening were nearly double compared to the breast cancer screening.19
The misconceptions are not limited to the risk factors and screening utilization of the women in the community but are also linked with the modern treatment seeking behavior, though there were living witnesses of healed patients in the localities, as mentioned during the discussions. Obviously, the initial misconceptions about the causes of the diseases and considering it as supernatural punishments for the socially unacceptable and wrong sexual engagements could end upmisconceiving that traditional or spiritual remedies are more effective options of treatment. One of the previous studies in Ethiopia also revealed similar findings and identified that viewing cancer as a deadly and incurable disease lead the patients to either perform spiritual acts or search for other non-medical managements.15 Fear of treatments’ adverse effect was also linked with the unwillingness to seek the modern treatment options in our study. In line with this, another qualitative study among Malaysian women identified that cancer cases even misunderstood chemotherapy treatment as a cause of death, which indicated the need to include creating awareness even about treatment options including their side effects at a community level.31
Given the existence of the misconceptions and the low utilization of the screening services in the health facilities of the area, the study participants were asked to indicate the best strategies to address the misconceptions going forward. They suggested advertising about availability and benefit of screening through mass media, religious and other traditional social systems and social events like holidays and market places to increase the knowledge of the community regarding female cancers in the future. Incorporation of the locally available information centers, which include the use of churches and other social gatherings including schools were recommended as approaches to increase the level of knowledge in the community.20 This in turn could debunk the existing myths and misconception around female cancers if properly designed and implemented using social and behavioral change communication. Likewise, raising awareness about self-sampling devices for the collection of samples directly by women at home would increase the coverage of screening services as evidenced by previous studies in Ethiopia and a review of randomized control trails (RCTs) and other observational studies.32
Limitations of the Study
Although the findings here share commonalities with studies on cervical and breast cancer as evidenced in this study, as a limitation, we fear social desirability bias and lack of participants who had experience of cancer might have limited us from getting more information.
Conclusion
The findings have revealed that the public in rural settings, where the majority live in this study, with limited access to information and services, exhibited widespread misconceptions about the causes, risk factors, transmission and consequences of both cervical and breast cancers. Such widespread misconceptions are attributed to a lack of and/or inconsistent availability of locally sound information about the diseases and how to prevent and manage them. Despite measures the government is taking and the focuses of its strategic plan, prevention intervention in the study area is largely invisible and people maintain their misconceptions with their consequences of stigma, infertility and fear of death.
Local authorities may use the outcomes from here to improve their interventions while the ministry of health in Ethiopia may consider organized and locally sound cervical and breast cancer prevention and control interventions.
Abbreviations
BC, breast cancer; CC, cervical cancer; FC, female cancer; FGD, focus group discussion; HPV, human papilloma virus; KII, key informant interview; LMICs, low- and middle-income countries; RCT, randomized control trial.
Data Sharing Statement
The original raw data used in this study is available from the corresponding author and can be presented upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Research Ethical Committee, School of Public Health, College of Health Sciences, Addis Ababa University and registered with number prv/154/10. An official letter of permission was provided to the administrative office of each of the selected health facilities. Written informed consent was obtained from the study participants. They were informed about the purpose of the study, and publication of anonymized responses.
The study has followed the international principles of research ethics Declared at Helsinki.
Acknowledgments
The authors would like to pass their gratitude for all study participants, data collectors and supervisors without whom this research would have not been realized. We also want to send our appreciation to Cordaid Ethiopia for the financial support to conduct this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation. All authors took part in drafting, revising or critically reviewing the article and gave final approval of the version to be published, have agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work.
Disclosure
The authors declare they have no competing interests.
References
1. Cancer facts & figures 2016 [internet]; 2016. Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2016/cancer-facts-and-figures-2016.pdf.
2. Global burden of cancer in women. Current status, trends, and interventions [Internet]. Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/global-cancer-facts-and-figures/global-burden-of-cancer-in-women.pdf.
3. Fitzmaurice C, Allen C, Barber RM, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol. 2017;3(4):524–548. doi:10.1001/jamaoncol.2016.5688
4. Ibekwe CM. Factors Influencing Cervical Cancer Screening Uptake Among Women Attending Mahalapye District Hospital in Botswana-Use of the Health Belief Model. University of LIMPOPO; 2009.
5. African Cancer Registry Network. Addis Ababa City cancer registry; 2014. Available from: http://afcrn.org/membership/membership-list/100-addisababa.
6. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
7. Ethiopian Ministry of Health, National cancer control plan; 2015. Available from: https://www.iccpportal.org/sites/default/files/plans/NCCP%20Ethiopia%20Final%20261015.pdf.
8. Isa Modibbo F, Dareng E, Bamisaye P, et al. Qualitative study of barriers to cervical cancer screening among Nigerian women. BMJ Open. 2016;6(1):e008533. doi:10.1136/bmjopen-2015-008533
9. Karnaki P. Attitudes, practices and knowledge regarding cervical cancer screening among Greek women in the area of Perth; 2000.
10. Teng FF, Mitchell SM, Sekikubo M, et al. Understanding the role of embarrassment in gynaecological screening: a qualitative study from the ASPIRE cervical cancer screening project in Uganda. BMJ Open. 2014;4(4):e004783. doi:10.1136/bmjopen-2014-004783
11. Birhanu Z, Abdissa A, Belachew T, et al. Health seeking behavior for cervical cancer in Ethiopia: a qualitative study. Int J Equity Health. 2012;11(1):83. doi:10.1186/1475-9276-11-83
12. Fylan F. Screening for cervical cancer: a review of women’s attitudes, knowledge, and behaviour. Br J Gen Pract. 1998;48(433):1509–1514.
13. Ashagrie A, Seme A, Assegid M. Knowledge and screening practice on cervical cancer among HIV positive women and associated factors in Adama, Ethiopia MPH thesis. In press; 2017.
14. Aweke YH, Ayanto SY, Ersado TL. Knowledge, attitude and practice for cervical cancer prevention and control among women of childbearing age in Hossana Town, Hadiya zone, Southern Ethiopia: community-based cross-sectional study. PLoS One. 2017;12(7):e0181415. doi:10.1371/journal.pone.0181415
15. Gebremariam A, Addissie A, Worku A, Assefa M, Kantelhardt EJ, Jemal A. Perspectives of patients, family members, and health care providers on late diagnosis of breast cancer in Ethiopia: a qualitative study. PLoS One. 2019;14(8):e0220769. doi:10.1371/journal.pone.0220769
16. Getahun F, Mazengia F, Abuhay M, Birhanu Z. Comprehensive knowledge about cervical cancer is low among women in Northwest Ethiopia. BMC Cancer. 2013;13:2. doi:10.1186/1471-2407-13-2
17. Moore AR, Driver N. Knowledge of cervical cancer risk factors among educated women in lomé, togo: half-truths and misconceptions. SAGE Open. 2014;4(4):2158244014557041. doi:10.1177/2158244014557041
18. Makurirofa L, Mangwiro P, James V, et al. Women’s knowledge, attitudes and practices (KAP) relating to breast and cervical cancers in rural Zimbabwe: a cross sectional study in Mudzi District, Mashonaland East Province. BMC Public Health. 2019;19(1):109. doi:10.1186/s12889-018-6333-5
19. Chaka B, Sayed A-R, Goeieman B, Rayne S. A survey of knowledge and attitudes relating to cervical and breast cancer among women in Ethiopia. BMC Public Health. 2018;18(1):1072. doi:10.1186/s12889-018-5958-8
20. Gatune JW, Nyamongo IK. An ethnographic study of cervical cancer among women in rural Kenya: is there a folk causal model? Int J Gynecol Cancer. 2005;15(6):1049–1059. doi:10.1111/j.1525-1438.2005.00261.x
21. Fakri S, Azzawi AA, Tawil NA. Antiperspirant use as a risk factor for breast cancer in Iraq. EMHJ. 2006;12(3–4):478–482.
22. Anderson KN, Schwab RB, Martinez ME. Reproductive risk factors and breast cancer subtypes: a review of the literature. Breast Cancer Res Treat. 2014;144(1):1–10. doi:10.1007/s10549-014-2852-7
23. Reid EA, Gudina EK, Ayers N, Tigineh W, Azmera YM. Caring for life-limiting illness in Ethiopia: a mixed-methods assessment of outpatient palliative care needs. J Palliat Med. 2018;21(5):622–630. doi:10.1089/jpm.2017.0419
24. Luque JS, Castañeda H, Tyson DM, Vargas N, Proctor S, Meade CD. HPV awareness among latina immigrants and Anglo American Women in the Southern U.S.: cultural models of cervical cancer risk factors and beliefs. NAPA Bull. 2010;34(1):84–104. doi:10.1111/j.1556-4797.2010.01053.x
25. Luque JS, Tarasenko YN, Maupin JN, et al. Cultural beliefs and understandings of cervical cancer among Mexican immigrant women in Southeast Georgia. J Immigr Minor Health. 2015;17(3):713–721. doi:10.1007/s10903-014-0117-5
26. Franceschi S, Plummer M, Clifford G, et al. Differences in the risk of cervical cancer and human papillomavirus infection by education level. Br J Cancer. 2009;101(5):865–870. doi:10.1038/sj.bjc.6605224
27. Walboomers JM, Jacobs MV, Manos MM, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;189(1):12–19. doi:10.1002/(SICI)1096-9896(199909)189:1<12::AID-PATH431>3.0.CO;2-F
28. Dsouza SM, Vyas N, Narayanan P, Parsekar SS, Gore M, Sharan K. A qualitative study on experiences and needs of breast cancer survivors in Karnataka, India. Clin Epidemiol Glob Health. 2018;6(2):69–74. doi:10.1016/j.cegh.2017.08.001
29. Norsa’adah B, Rahmah MA, Rampal KG, Knight A. Understanding barriers to Malaysian women with breast cancer seeking help. Asian Pac J Cancer Prev. 2012;13(8):3723–3730. doi:10.7314/APJCP.2012.13.8.3723
30. Ncube B, Bey A, Knight J, Bessler P, Jolly PE. Factors associated with the uptake of cervical cancer screening among women in Portland, Jamaica. N Am J Med Sci. 2015;7(3):104–113. doi:10.4103/1947-2714.153922
31. Nies YH, Ali AM, Abdullah N, Islahudin F, Shah NM. A qualitative study among breast cancer patients on chemotherapy: experiences and side-effects. Patient Prefer Adherence. 2018;12:1955–1964. doi:10.2147/PPA.S168638
32. Bogale AL, Teklehaymanot T, Ali JH, et al. Comparison of self-collected versus clinician collected cervicovaginal specimens for detection of high risk human papillomavirus among HIV infected women in Ethiopia. BMC Women’s Health. 2022;22(1):1–7. doi:10.1186/s12905-022-01944-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Scoping Review of Patient Navigation in the Continuity of Cancer Care for Women
Haroen H, Agustina HR, Pahria T, Mambang Sari CW, Adhipurnawan Winarno GN, Bangun AV, Pardosi JF, Akuoko CP
International Journal of Women's Health 2025, 17:4779-4798
Published Date: 25 November 2025