Back to Journals » Journal of Pain Research » Volume 14
Minimum Effective Analgesic Concentration of Ropivacaine in Saphenous Block Guided by Ultrasound for Knee Arthroscopic Meniscectomy: Randomized, Double-Blind Study
Authors Rey Moura EC, de Oliveira CMB ![]() , da Cunha Leal P, Kimiko Sakata R
, da Cunha Leal P, Kimiko Sakata R ![]()
Received 29 September 2020
Accepted for publication 16 December 2020
Published 13 January 2021 Volume 2021:14 Pages 53—59
DOI https://doi.org/10.2147/JPR.S282286
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Michael Schatman
Ed Carlos Rey Moura,1 Caio Marcio Barros de Oliveira,2 Plinio da Cunha Leal,2 Rioko Kimiko Sakata1
1Universidade Federal de São Paulo, Department of Anesthesia, São Paulo, Brazil; 2Universidade Federal do Maranhão, Department of Medicine, São Luiz, Maranhão, Brazil
Correspondence: Rioko Kimiko Sakata Email [email protected]
Background: After knee surgery, analgesia should be effective for mobilization and discharge.
Aim of the Study: The primary objective of this study was to achieve the lowest effective analgesic concentration (MEC50 and MEC90) of ropivacaine for saphenous nerve block in arthroscopic meniscectomy. The secondary objective was to determine whether the block causes muscle weakness in the postoperative period.
Methods: The study was randomized, comparative, and double-blind. Fifty-one patients between 18 and 65 years old of both sexes, ASA I or II, who underwent knee arthroscopic meniscectomy at São Domingos Hospital were included. Patients underwent saphenous nerve block with 10 mL of ropivacaine administered by using the up-and-down method. The ropivacaine concentration was determined based on the previous patient’s response (a biased-coin up-down design sequential method). If a patient had a negative response, the concentration of ropivacaine was increased by 0.05% in the next patient; if the response was positive, the next patient was randomized to be administered the same concentration of ropivacaine or a 0.05% lower concentration. Successful block was defined as pain < 4 during 6 h. Patients underwent general anesthesia with 30 μg/kg alfentanil and propofol and maintenance with propofol, and, if necessary, remifentanil was administered. Postoperative analgesia was complemented with dipyrone, and if necessary, tramadol (100 mg) could be used. The following parameters were assessed: the success of the block; pain intensity after 2, 4, and 6 h; the consumption of remifentanil; time to the first analgesic supplementation; percent of patients who needed analgesics during 6h; and muscle strength.
Results: The MEC50 of ropivacaine was 0.36%, and the MEC90 was 0.477%. The block was successful in 45 patients.
Conclusion: Saphenous block with 10 mL of 0.36% ropivacaine provides adequate analgesia for outpatient meniscectomy.
Keywords: saphenous nerve, block, up-and-down, meniscectomy, MEC50, MEC90
Introduction
Preventive analgesia is the use of medications or techniques as nerve blocks before the start of the surgical stimulus.1 Postoperative pain relief speeds up recovery and hospital discharge2,3 and is essential for patients undergoing knee surgery. Nerve blocks can reduce the need for systemic analgesics, lowering their adverse effects.3,4
Knee innervation is performed through the femoral and sciatic nerves, and their block can prevent the transmission of pain. However, there are some constraints, such as patient positioning and the need for a large dose of local anesthetic.5 In addition, isolated femoral nerve block provides adequate analgesia for knee ligament reconstruction.4 In another study, there was adequate postoperative analgesia by blocking the saphenous nerve, a sensory branch of the femoral nerve.6 The saphenous nerve crosses between the sartorius muscle and the vastus medialis in the adductor canal and halfway between the inguinal crease and the patella in the thigh. The saphenous nerve and its branches to the vastus medialis are located lateral to the superficial femoral artery and anterior to the vein and to the vastus medialis muscle.7
Contrast injection went approximately halfway through the adductor canal in cadavers, and a volume of 15 mL was sufficient to spread throughout the adductor canal, from the apex of the femoral triangle to its most distal part and beyond.8
To determine the concentration of local anesthetic needed to block the nerve, Dixon’s modified up-and-down method can be used, where depending on the effectiveness of the block with the previous local anesthetic concentration, the concentration for the next patient is adjusted up or down in 0.05% increments.9
Arthroscopic knee surgery is routinely performed under spinal anesthesia. Among the reasons for hospitalization are motor block, urinary retention, and ineffective analgesia for mobilizing the knee.10 By blocking the saphenous nerve at the lowest effective concentration of local anesthetic, these issues are expected to be eliminated, and the patient could be discharged on the same day with adequate analgesia.
The primary objective of this study was to achieve the minimum effective analgesic concentration (MEC50 and MEC90) of ropivacaine for saphenous nerve block via arthroscopic meniscectomy. The secondary objective was to determine whether the block causes muscle weakness in the postoperative period.
Materials and Methods
This study was approved by the Research Ethics Committee of University (CAEE 65396017.3.1001.5505), and written informed consent was obtained from all participants. The clinical trial was registered on April 26, 2017, in the Brazilian Registry of Clinical Trials (REBEC) (Registration URL: http://www.ensaiosclinicos.gov.br) as Trial Register Number RBR-5JSZXW, and the patient enrollment occurred between August 01, 2017, and June 04, 2019. It was performed in accordance with the ethical principles for medical research involving human subjects of the Declaration of Helsinki. The full protocol can be assessed at the University Ethics Committee. The study was randomized, comparative, and double-blind. This method assumes that the previous patient is the control of the current patient, and therefore, the study had one arm.
The distribution of patients in the groups was determined by using Dixon’s modified up-and-down method (1991).11 If a patient had a negative response, the ropivacaine concentration was increased by 0.05% in the next patient, with a probability of 1. If a patient had a positive response (awoke with pain <4), the next patient would be randomized to be administered the same concentration of ropivacaine (probability of 0, 89) or to be administered a 0.05% lower concentration (0.11 probability). Randomization was conducted by drawing a number, for which a table was prepared for guidance. The solution was prepared by another anesthetist, and the patient and the researcher who performed the block did not know the concentration of local anesthetic administered.
There were 51 patients of both sexes, ASA I or II by the American Society of Anesthesiologists, between 18 and 65 years who underwent knee arthroscopic meniscectomy at São Domingos Hospital. Patients with coagulopathy, using anticoagulants, infection at the puncture site, cognitive impairment, allergies to medications, and who were pregnant were excluded. They were not taking any pain medication prior to surgery.
Patients were administered midazolam (0.01 mg/kg) intravenously 5 minutes before the block and were monitored with cardioscopy, pulse oximetry, and noninvasive blood pressure monitoring.
Ultrasound-guided saphenous nerve block (SonoSite M-Turbo®) with ropivacaine was performed with the patient in the supine position and lower limbs in a neutral position using a linear transducer with a frequency between 6 and 18 MHz (depending on the depth of the structures). After preparing the skin, saphenous block was performed by using the technique of Hanson et al7 on the thigh, midway between the inguinal crease and the patella. The nerve was localized between the sartorius muscle and vastus medialis in the adductor canal. The femoral artery was identified dorsal to the sartorius muscle. At this level, the hyperechogenic structure containing the saphenous nerve and the branches to the vastus medialis are located lateral to the artery and anterior to the vein and vastus medialis muscle.
Local anesthetic was injected around the nerve. The biased-coin up-down design sequential method was used to determine the minimum effective dose (MED90). The first patient was administered 10 mL of 0.5% ropivacaine; the second patient was administered 0.55% ropivacaine if the first patient’s pain intensity was ≥4 after awakening from anesthesia; if the first patient awoke with pain <4, the second patient was administered 0.45% ropivacaine or the same concentration would be maintained with a probability of 0.89.
After the block, all participants underwent general anesthesia with 30 µg/kg alfentanil, 2 mg/kg propofol, and an infusion of 3.5 mg/mL propofol. If necessary, remifentanil was used as complementary intraoperative analgesia. The parameter for the use of remifentanil was an increase of more than 20% in the heart rate and blood pressure compared to before anesthesia. Postoperative complementary analgesia was with 2 g of intravenous dipyrone; if necessary, 100 mg of intravenous tramadol was used after 30 minutes of dipyrone use up to 400 mg/day.
The following parameters were assessed: the success of the block; pain intensity based on a numerical scale after 2, 4, and 6 h; consumption of remifentanil; time to first analgesic supplementation; and percent of patients who needed analgesics over 6 h. A successful block was defined as pain <4 6 h after the block and before they asked for rescue analgesics; if pain was ≥4, the block was regarded as a failure. A dynamometer was used to measure strength prior to the surgery and at T0.
The sample calculation was based on the concept of sample stabilization proposed by Pace and Stylianou12 for this method (biased-coin up-and-down design sequential method). As for the method for calculating the effective concentration (EC)50, the sample stabilized at approximately 40 patients. The calculation of the EC90 was based on the calculation by George et al,13 who recommended a minimum sample size greater than 40 and a multiple of 9, with 45 patients (hits) for this study. From the estimated successful probabilities with 51 patients, 1000 bootstrap experiments were generated. Each of the 1000 experiments had their success probabilities isotonized with the aid of the Isoreg function (R software 3.1.2). After the experiments were isotonized, EC50 and EC90 doses were estimated using the μ3 isotonic regression estimator proposed by Pace and Stylianou,12 which showed more favorable properties than other estimators. After calculating the EC50 and EC90, the 95% confidence intervals were estimated. This process was repeated with the generation of 2500, 5000, and 10,000 bootstrap samples.
The following tests were used: isotonic regression achieved by bootstrapping to identify the EC50 and 90; the Kruskal–Wallis test for different ropivacaine concentrations with successful block, pain intensity, and analgesic consumption; analysis of variance (ANOVA) to compare the time until the first supplementation; and the Wilcoxon test for muscle strength. The significance level was p ≤ 0.05. Statistical analysis was performed using R 3.1.2 software for Windows and SPSS 15 software.
Results
All participants completed the study according to the CONSORT flowchart (Figure 1). Patient data and duration are shown in Table 1.
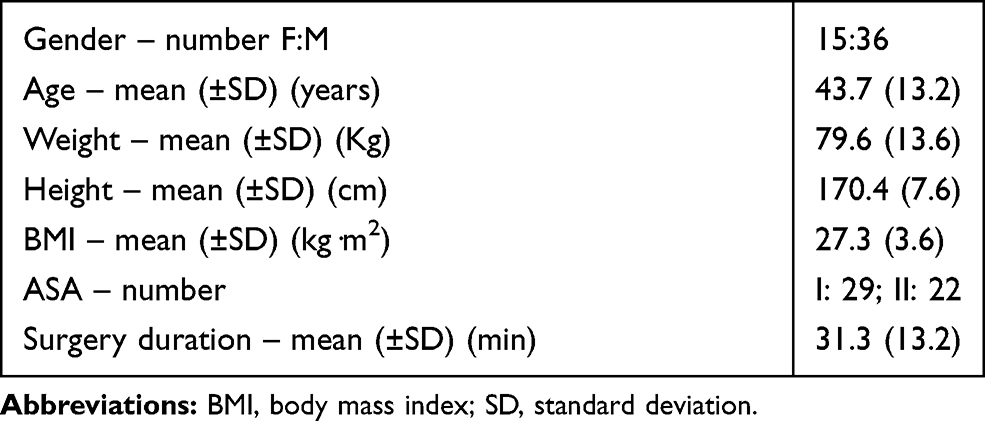 |
Table 1 Data of Participants |
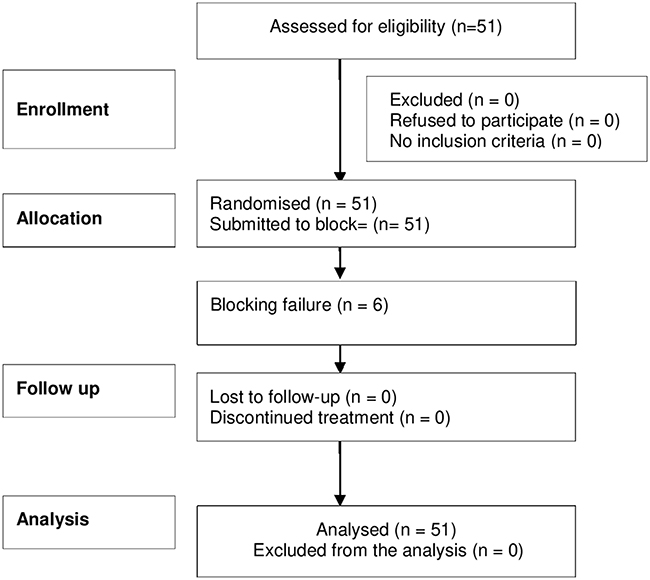 |
Figure 1 CONSORT flowchart. There were assessed for eligibility 51 participants, and no one was excluded. All of them were randomized and submitted to block, with blocking failure in 6 participants. All participants completed the study. |
The concentrations of ropivacaine used were 0.35% (2 patients= 3.9%), 0.40% (13 patients= 25.4%), 0.45% (19 patients= 37.2%), 0.50% (14 patients= 27.4%), 0.55% (2 patients= 3.9%), and 0.60% (1 patient= 1.96%). The MEC50 was 0.360 (95% CI: 0.350–0.386), and the MEC90 was 0.477 (95% CI: 0.395–0.579). The sequential response of patients is shown in Figure 2.
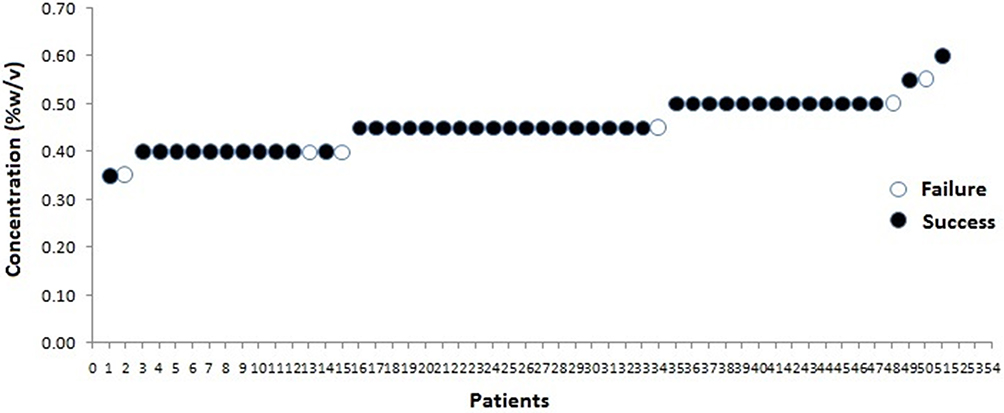 |
Figure 2 Ropivacaine concentration and successful or failure of the saphenous block for up-and-down sequence of patients. |
The block was effective in 45 patients and failed in 6 (1 with a concentration of 0.35%, 2 with 0.4%, 1 with 0.45%, 1 with 0.5% and 1 with 0.55%) (Figure 2). The use of remifentanil was not required. Local anesthetic was not injected into the surgical site, and the patients did not use an immobilizer and were encouraged to walk early. There was no significant difference in muscle strength between the operated and nonoperated limbs before or after surgery. Before surgery, the mean strength of the operated limb was 60.49±15.7 mmHg, and in the nonoperated limb, it was 64.8±13.1; after surgery, the strength of the operated limb was 51.1±15.2, and in the nonoperated limb, it was 53.8±14.9 mmHg. There were no side effects or complications related to local anesthetic or saphenous block. There were no differences in the use of complementary analgesics (Table 2).
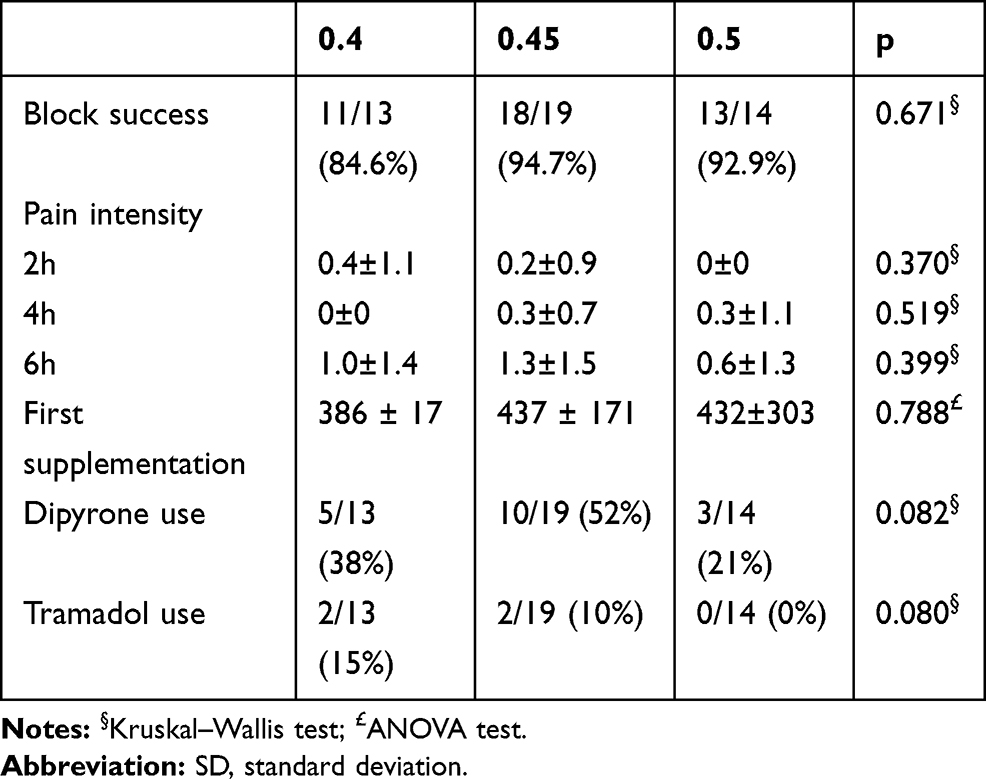 |
Table 2 Ropivacaine Concentration and Successful Block – Number (%) of Patients, Pain Intensity – Mean (±SD), Time Till First Supplementation (Min), and Need for Dipyrone and Tramadol Supplementation – Number (%) |
Discussion
The modified up-and-down method was used successfully to determine effective doses of drugs and is a technique with recognized validity. This study had 45 successes and 6 failures, as in a previous study that used this technique.8
The effective concentration in 90% of patients was similar to that found by Bonet et al,6 although they used another research method.
Compared with other nerve blocks used for analgesia, such as femoral block, saphenous block is unique, providing a similar analgesic effect with minimal motor block. Depending on the surgical technique and other knee surgical procedures, the block may not be effective, mainly because the surgical stimulus may cover areas innervated by other nerves, such as the sciatic nerve.5
The study aimed to assess postoperative analgesia during the first 6 h for early hospital discharge after release from anesthetic recovery. All patients were discharged without requiring hospitalization.
Although the primary objective aimed to assess postoperative analgesia, if there was an increase in the heart rate or blood pressure during surgery, indicating a sympathetic stimulus from the surgical stimulus, remifentanil would have been added as a venous infusion, but this was not needed in any patients.
The concomitant use of ultrasound with a peripheral nerve stimulator improves the quality of block results,14 enabling the volume and total dose of the local anesthetic to be lowered and reducing the possibility of toxic effects15 and complications.16
Saphenous nerve blocks can be considered safe for knee analgesia in relation to motor loss.3 In healthy volunteers, adductor canal block reduced quadricep strength by only 8%, which suggests that the risk of weakness, as well as the risk of patient fall, is low.17 This is essential for both patient discharge and early mobilization.
In this study, with 10 mL of ropivacaine, as recommended by Tao et al,18 it was found that an MEC90% of 0.477% was the minimum effective concentration for saphenous block in arthroscopic meniscectomy.
Akkaya et al19 recommend 10 mL of 0.5% ropivacaine for saphenous block. However, other authors, such as Bonet et al,6 used 10 mL of 0.475% ropivacaine and achieved good analgesia for knee arthroscopy. Elkassabany et al20 used 20 mL at 0.5% for knee arthroplasty, and Hanson et al7 used 15 mL of 0.5% ropivacaine. The minimum effective dose for saphenous nerve analgesia also varies with the local anesthetic used.
One of the major concerns of the study was the possibility of motor weakness after analgesic block. Therefore, patients were assessed prior to the block, in the preanesthetic room, and after surgery in the anesthetic recovery room.
Despite the efficacy of venous analgesics, we can use spinal morphine or nerve block for knee surgery analgesia. Depending on the intensity of the nociceptive stimulus, nerve blocks have a great advantage. When analyzed in the context of outpatient surgery, this advantage stands out.21 Peripheral nerve block, if performed correctly and at the lowest effective dose of local anesthetic, stands out in relation to spinal block with morphine, avoiding its side effects.22
The biased-coin up-and-down sequential method is used to assess the dose-response of medications. The total sample is not known beforehand, only the number of successes needed. It proved to be an effective method with reduced samples compared to classic studies of multiple groups with fixed concentrations. It also has the advantage of subjecting fewer patients to inadequate analgesia and adverse effects, increasing the cost-effectiveness.
In this study, as in the literature, saphenous block was followed up by general anesthesia. Muscle strength was assessed after surgery because the duration of the block was 15–20 h.23,24
Limitations
The analgesic effect was assessed in only the first 6 h.
Conclusions
In conclusion, ultrasound-guided saphenous block promotes analgesic effects for knee surgery, with a low risk of muscle weakness and side effects.
Data Sharing Statement
Data are available at link
https://drive.google.com/file/d/13UyMBc7rIhMCIZjb3MOIRm9Ea3qJP4Xc/view?usp=sharing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Byrne K, Smith C. Preemptive analgesia: an unobtainable goal? J Cardiothorac Vasc Anesth. 2019;33(2):460–461. doi:10.1053/j.jvca.2018.08.008
2. Barreveld A, Witte J, Chahal H, Durieux ME, Strichartz G. Preventive analgesia by local anesthetics: the reduction of postoperative pain by peripheral nerve blocks and intravenous drugs. Anesth Analg. 2013;116(5):1141–1161. doi:10.1213/ANE.0b013e318277a270
3. Rahimzadeh P, Faiz HR, Imani F, Hobika GG, Abbasi A, Nader ND. Relieving pain after arthroscopic knee surgery: ultrasound-guided femoral nerve block or adductor canal block? Turk Anest Rean Dern Derg. 2017;45(4):218–224. doi:10.5152/TJAR.2017.00868
4. Tantry TP, Muralishankar BG, Rajesh H. Use of a single injection femoral nerve block in the patients of total knee replacement with concomitant epidural analgesia. J Clin Diagn Res. 2012;6(10):1744–1748. doi:10.7860/JCDR/2012/4920.2620
5. Yao J, Zeng Z, Jiao Z, Wang A, Wang J, Yu A. Optimal effective concentration of ropivacaine for postoperative analgesia by single-shot femoral -sciatic nerve block in outpatient knee arthroscopy. J Intern Med Res. 2013;41(2):395–403. doi:10.1177/0300060513476427
6. Bonet A, Koo M, Sabaté A, Otero I, Bocos J, Pi A. Ultrasound-guided saphenous nerve block is an effective technique for perioperative analgesia in ambulatory arthroscopic surgery of the internal knee compartment. Rev Esp Anestesiol Reanim. 2015;62(8):428–435. doi:10.1016/j.redar.2014.10.009
7. Hanson NA, Derby RE, Auyong DB, et al. Ultrasound-guided adductor canal block for arthroscopic medial meniscectomy: a randomized, double-blind trial. Can J Anaesth. 2013;60(9):874–880. doi:10.1007/s12630-013-9992-9
8. Andersen HL, Andersen SL, Tranum-Jensen J. The spread of injectate during saphenous nerve block at the adductor canal: A cadaver study. Acta Anaesthesiol Scand. 2015;59(2):238–245. doi:10.1111/aas.12451
9. Moura EC, de Oliveira Honda CA, Bringel RC, Leal Pda Filho C, Sakata RK. Minimum effective concentration of bupivacaine in ultrasound-guided femoral nerve block after arthroscopic knee meniscectomy: a randomized, double-blind, controlled trial. Pain Phys. 2016;19(1):E79–E86.
10. Teunkens A, Vermeulen K, Van Gerven E, Fieuws S, Van de Velde M, Rex S. Comparison of 2-chloroprocaine, bupivacaine, and lidocaine for spinal anesthesia in patients undergoing knee arthroscopy in an outpatient setting: a double-blind randomized controlled trial. Reg Anesth Pain Med. 2016;41(5):576–583. doi:10.1097/AAP.0000000000000420
11. Dixon WJ. Staircase bioassay: the up-and-down method. Neurosci Bio Rev. 1991;15(1):47–50. doi:10.1016/S0149-7634(05)80090-9
12. Pace NL, Stylianou MP. Advances in and limitations of up-and-down methodology: a précis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
13. George RB, McKeen D, Columb MO, Habib AS. Up-down determination of the 90% effective dose of phenylephrine for the treatment of spinal anesthesia-induced hypotension in parturients undergoing cesarean delivery. Anesth Analg. 2010;110(1):154–158. doi:10.1213/ANE.0b013e3181c30b72
14. Min L, Ting X, Wen-yong H, Xue-dong W, Dong-lin J, Xiang-yang G. Use of ultrasound to facilitate femoral nerve block with stimulating catheter. Chine Med J. 2011;124(4):519–524.
15. Kent ML, Hackworth RJ, Riffenburgh RH, Kaesberg JL, Lujan E, Corey JM. A comparison of ultrasound-guided and landmark-based approaches to saphenous nerve blockade: A prospective, controlled, blinded, crossover trial. Anesth Analg. 2013;117(1):265–270. doi:10.1213/ANE.0b013e3182908d5d
16. Jeng CL, Torrillo TM, Rosenblatt MA. Complications of peripheral nerve blocks. Br J Anaesth. 2010;105(1):i97–i107. doi:10.1093/bja/aeq273
17. Jaeger P, Nielsen ZJ, Henningsen MH, Hilsted KL, Mathiesen O, Dahl JB. Adductor canal block versus femoral nerve block and quadriceps strength: a randomized, double-blind, placebo-controlled, crossover study in healthy volunteers. Anesthesiology. 2013;118(2):409–415. doi:10.1097/ALN.0b013e318279fa0b
18. Tao Y, Zheng SQ, Xu T, et al. Median effective volume of ropivacaine 0.5% for ultrasound-guided adductor canal block. J Int Med Res. 2018;46(10):4207–4213. doi:10.1177/0300060518791685
19. Akkaya T, Ersan O, Ozkan D, et al. Saphenous nerve block is an effective regional technique for post-menisectomy pain. Knee Surg Sports Traumatol Arthros. 2008;16(9):855–858. doi:10.1007/s00167-008-0572-4
20. Elkassabany NM, Antosh S, Ahmed M, et al. The risk of falls after total knee arthroplasty with the use of a femoral nerve block versus an adductor canal block: a double-blinded randomized controlled study. Anesth Analg. 2016;122(5):1696–1703. doi:10.1213/ANE.0000000000001237
21. Davarci I, Tuzcu K, Karcioglu M, et al. Comparison between ultrasound-guided sciatic-femoral nerve block and unilateral spinal anaesthesia for outpatient knee arthroscopy. J Int Med Res. 2013;41(5):1639–1647. doi:10.1177/0300060513498671
22. Sundarathiti P, Thammasakulsiri J, Supboon S, Sakdanuwatwong S, Piangjai M. Comparison of continuous femoral nerve block (CFNB/SA) and continuous femoral nerve block with mini-dose spinal morphine (CFNB/SAMO) for postoperative analgesia after total knee arthroplasty (TKA): a randomized controlled study. BMC Anesthesiol. 2016;16(1):38. doi:10.1186/s12871-016-0205-2
23. Andersen JH, Grevstad U, Siegel H, Dahl JB, Mathiesen O, Jæger P. Does dexmedetomidine have a perineural mechanism of action when used as an adjuvant to ropivacaine?: A paired, blinded, randomized trial in healthy volunteers. Anesthesiology. 2017;126(1):66–73. doi:10.1097/ALN.0000000000001429
24. Chisholm MF, Cheng J, Fields KG, et al. Perineural dexamethasone with subsartorial saphenous nerve blocks in ACL reconstruction. Knee Surg Sports Traumatol Arthros. 2017;25(4):1298–1306. doi:10.1007/s00167-016-4120-3
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.