Back to Journals » Clinical Interventions in Aging » Volume 18
Minimally Invasive Spinal Fusion Using Percutaneous Pedicle Screw Instrumentation Can Provide a Better Health-Related QOL in Early Stage Than Conventional Methods in the Treatment of Single-Level Degenerative Lumbar Spinal Diseases
Authors Iwabuchi M ![]() , Tominaga R, Komatsu J, Shirado O
, Tominaga R, Komatsu J, Shirado O
Received 17 August 2022
Accepted for publication 3 January 2023
Published 31 January 2023 Volume 2023:18 Pages 131—139
DOI https://doi.org/10.2147/CIA.S385317
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Masumi Iwabuchi,1 Ryoji Tominaga,1 Jun Komatsu,1,2 Osamu Shirado1
1Department of Orthopaedic and Spinal Surgery, Aizu Medical Center at Fukushima Medical University, Aizuwakamatsu, Fukushima, Japan; 2Department of Medicine for Motor Organs, Juntendo University Graduate School of Medicine, Tokyo, Japan
Correspondence: Masumi Iwabuchi, Department of Orthopaedic and Spinal Surgery, Aizu Medical Center at Fukushima Medical University, Aizuwakamatsu, Fukushima, 969-3492, Japan, Tel +81-242-75-2100, Fax +81-242-75-2568, Email [email protected]
Purpose: To investigate whether the minimally invasive spinal fusion can provide the better outcome than conventional fusion surgery in the treatment of degenerative lumbar spinal diseases.
Patients and Methods: One hundred and thirteen patients who had undergone single-level fusion surgery for degenerative lumbar spinal diseases were examined with a minimum of one-year follow-up. There were 56 men and 57 women with a median age of 70s ranging 47– 88. The following three-types of fusion surgery were performed; minimally invasive transforaminal interbody fusion after microscopic decompression through a unilateral approach with percutaneous pedicle screwing (MTLIF), transforaminal interbody fusion after microscopic decompression through a unilateral approach (TLIF), and posterior lumbar interbody fusion with posterolateral fusion after open decompression through a bilateral approach (PLIF). The purpose for limiting on single level degenerative spinal disease was that it would be easy to compare the surgical outcomes among the three groups.
Results: There were no statistically significant differences among three groups in terms of VAS scores, RDQ scores, and all of the domains in the JOABPEQ scores at the baseline. The JOABPEQ score for pain-related disorders at 6 months after surgery was statistically significantly higher in MTLIF group than the other two groups (P = 0.023). There were no statistically significant differences in the scores of the other outcome measures among three groups in whole follow-up period.
Conclusion: The current study demonstrated that the JOABPEQ score for pain-related disorders at 6 months postoperatively was significantly better in MTLIF group than in the other groups. Since lumbar degenerative diseases mostly consisted in elderly patients, less invasive surgeries are desirable. MTLIF resulted in a better health-related QOL at 6 months after surgery, and its outcomes at the final follow-up were non-numerical inferiority. The results strongly indicate that MTLIF is desirable surgery especially for elderly patients with degenerative spinal diseases.
Keywords: minimally invasive spinal fusion surgery, transforaminal lumbar interbody fusion, posterior lumbar interbody fusion, posterolateral fusion, health-related QOL, surgical outcome, percutaneous pedicle screwing, CT-based navigation system
Introduction
Posterior lumbar interbody fusion (PLIF) was developed to provide three-column stabilization through a posterior approach.1 It can also provide indirect decompression of the neural tissue by increasing disc height.1 Furthermore, PLIF combined with posterolateral fusion (PLF) was reported to achieve a greater reduction in spondylolisthesis, lower complication rate, and more excellent results than PLF alone.2 TLIF was developed to be an alternative to PLIF, which implements a unilateral approach to the disc space through resection of a facet joint and minimized retraction of the neural tissue.3 Minimally invasive TLIF using percutaneous posterior fixation has been reported to reduce iatrogenic injury to soft tissue due to retraction of the paraspinal muscles through the conventional spinal approach.4–7
There are representative reports of comparative studies between minimally invasive transforaminal interbody fusion and open transforaminal interbody fusion/posterior interbody fusion.8–22 The long-term outcomes are almost the same among them. However, the effectiveness of minimally invasive spinal fusion (MISF) surgery has not been adequately clarified for the treatment of degenerative lumbar spinal diseases, especially under the same perioperative conditions and the same postoperative treatments including the rehabilitation program for each group. The purpose of this study was to investigate whether MISF can yield better outcomes than conventional fusion surgery in the treatment of degenerative lumbar spinal diseases. Available clinical data are insufficient for comparing minimally invasive transforaminal interbody fusion. To date, a paucity of literature exists directly investigating adequately the effectiveness of MISF surgery for the treatment of degenerative lumbar spinal diseases. Therefore, we developed a working hypothesis that fills out the research gap and clarifies whether MISF can provide a better clinical outcome than conventional fusion surgery in the treatment of degenerative lumbar spinal diseases.
Materials and Methods
Ethics Statements
We conducted this study in compliance with the principles of the Declaration of Helsinki. This study protocol has been reviewed and approved by Fukushima Medical University Certified Review Board (Approval number: 2019-131). Informed consent was obtained in the form of opt-out on the website.
Study Design, Population, and Setting
This cohort study was performed at a single center and included patients who had undergone single-level fusion surgery for degenerative lumbar spinal diseases. The purpose for limiting on single level degenerative spinal disease was that it would be easy to compare the surgical outcomes among following three groups. Patients with a history of spinal surgery, severe kidney dysfunction (estimated glomerular filtration rate <30 mL/min/1.73 m2), liver cirrhosis, and systemic diseases were excluded.
The following three types of fusion surgeries that have different invasiveness from each other were compared for the treatment of unstable degenerative spondylolisthesis and foraminal stenosis: minimally invasive transforaminal interbody fusion after microscopic bilateral decompression through a unilateral approach (MTLIF) (Figure 1), transforaminal interbody fusion after microscopic bilateral decompression through a unilateral approach (TLIF) (Figure 1), and posterior lumbar interbody fusion combined with posterolateral fusion after open decompression through a bilateral approach (PLIF). MTLIF was performed using percutaneous pedicle screwing with the guidance of a X-ray computed tomography (CT)-based navigation system following insertion of local bone and a cage filled with local bone into an intervertebral space after microscopic bilateral decompression through a unilateral approach in the MTLIF group (Figure 2A–C). In the TLIF group, pedicle screws were inserted through the open method for the approach side and the subcutaneous transfascial method for the opposite side under X-ray fluoroscopic control following insertion of local bone and a cage filled with local bone into an intervertebral space after microscopic bilateral decompression through a unilateral approach (Figure 3). PLIF was performed by posterior lumbar interbody fusion combined with posterolateral fusion after open decompression through a bilateral approach in the PLIF group. The screws were inserted using a freehand method following insertion of local bone and a cage filled with local bone into an intervertebral space in the PLIF group.
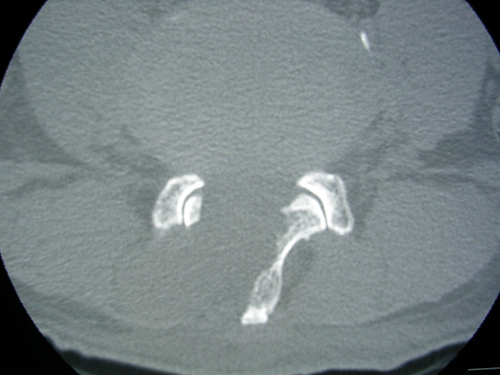 |
Figure 1 An X-ray computed tomography image after microscopic bilateral decompression through a unilateral approach. |
 |
Figure 2 Minimally invasive transforaminal interbody fusion after microscopic decompression through a unilateral approach is performed using percutaneous pedicle screwing with the guidance of a X-ray computed tomography (CT)-based navigation system in the MTLIF group. (A) shows image scanning for target lumbar vertebrae by CT. (B and C) show percutaneous pedicle screwing with the guidance of a CT-based navigation system. |
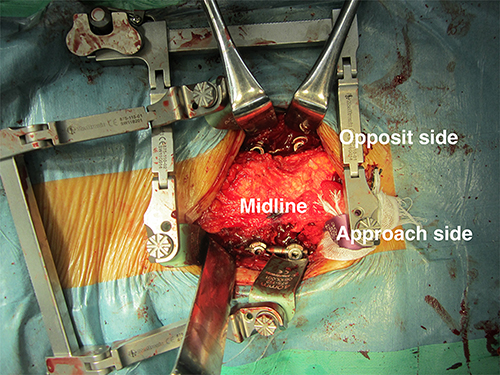 |
Figure 3 Pedicle screws were inserted through the open method for the approach side and the subcutaneous transfascial method for the opposite side under X-ray fluoroscopic control in the TLIF group. |
Unstable degenerative spondylolisthesis was defined to be ≥5 mm of anterior slip of the cranial vertebra on the lateral radiograph in the neutral position or an increase of 5 mm of anterior slip on the lateral radiograph in the flexion position compared to that in the neutral position, and an increase of ≥10 degrees of posteriorly intervertebral angulation on the lateral radiograph in the flexion position compared to that in the neutral position. Two board-certified spine surgeons approved by the Japanese Society for Spine and Related Research conducted all operations. One junior surgeon performed MTLIF and TLIF for the patients on their first visit to the outpatient on every Monday when the junior surgeon took charge. TLIF was performed from 2010 to 2014, and MTLIF was performed after the CT-based navigation system was introduced in 2014. The other senior surgeon performed PLIF for the patients on their first visit to the outpatient on every Tuesday when the senior surgeon took charge. PLIF was performed from 2010 to 2014. The patients were followed up for a minimum of 1 year.
Outcome Measures
Outcome measures were as follows: surgical time, amount of bleeding during surgery, visual analogue scale (VAS) for low back pain, lower limb pain, and lower limb numbness; Roland-Morris Disability Questionnaire (RDQ);23 Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ);24–26 and graft bone union rate. The status of graft bone union was evaluated using X-ray CT. An independent radiologist without knowledge about the patients evaluated graft bone union. Graft bone union was evaluated by the continuity of the bone trabeculae between upper and lower vertebral body through a graft bone (Figure 4A and B). Outcome measures were evaluated at 3 months, 6 months, and 1 year postoperatively. After 1 year postoperatively, outcomes were measured once every year.
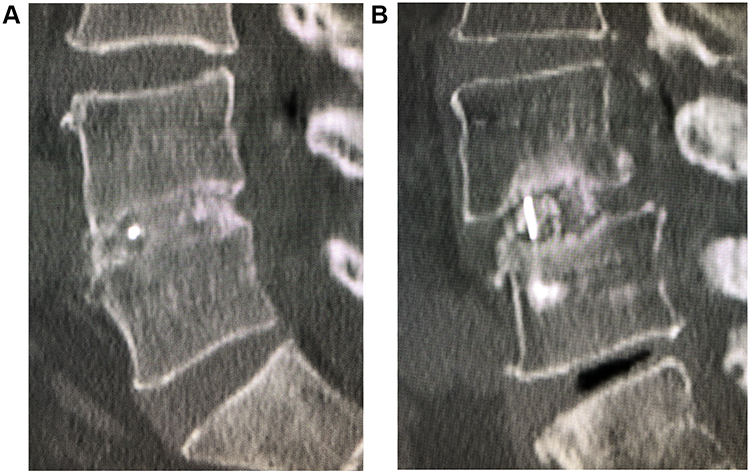 |
Figure 4 The status of graft bone union was evaluated using X-ray computed tomography. An independent radiologist without knowledge about the patients evaluated graft bone union. Graft bone union was evaluated by the continuity of the bone trabeculae between upper and lower vertebral body through a graft bone. (A) shows the presence of union. (B) shows the absence of union. |
Statistical Analyses
Baseline characteristics are described using appropriate summary statistics. The Kolmogorov–Smirnov test was used for the evaluation of normality in baseline characteristics. The one-way ANOVA would be used for the data of the baseline characteristics which had normal distribution. The Kruskal–Wallis test would be used for the data of the baseline characteristics which had non-normal distribution. The Kruskal Wallis test was also used to analyze the outcome data. Statistical analyses were performed using SPSS for Windows, version 17.0 (IBM Japan Ltd., Tokyo, Japan). A two-sided p-value <0.05 was considered statistically significant.
Results
Patients’ Characteristics
One hundred and thirteen patients were examined with a mean follow-up period of 28 months. There were 56 men and 57 women with a median age of 70s (range, 47–88 years). The main pathologies were unstable degenerative spondylolisthesis in 84 patients and foraminal stenosis in 29. The MTLIF group had 45 patients with a follow-up rate of 98%, TLIF group had 27 patients with a follow-up rate of 93%, and PLIF group had 41 patients with a follow-up rate of 85% (Table 1). The Kruskal Wallis test was used for all of the data in patients’ characteristics because of their non-normal distributions. There were no statistically significant differences among the three groups in terms of age, sex, disease, body mass index, smoking history, surgical site, follow-up period, VAS scores, RDQ scores and all of the domains of the JOABPEQ scores at baseline (Table 2).
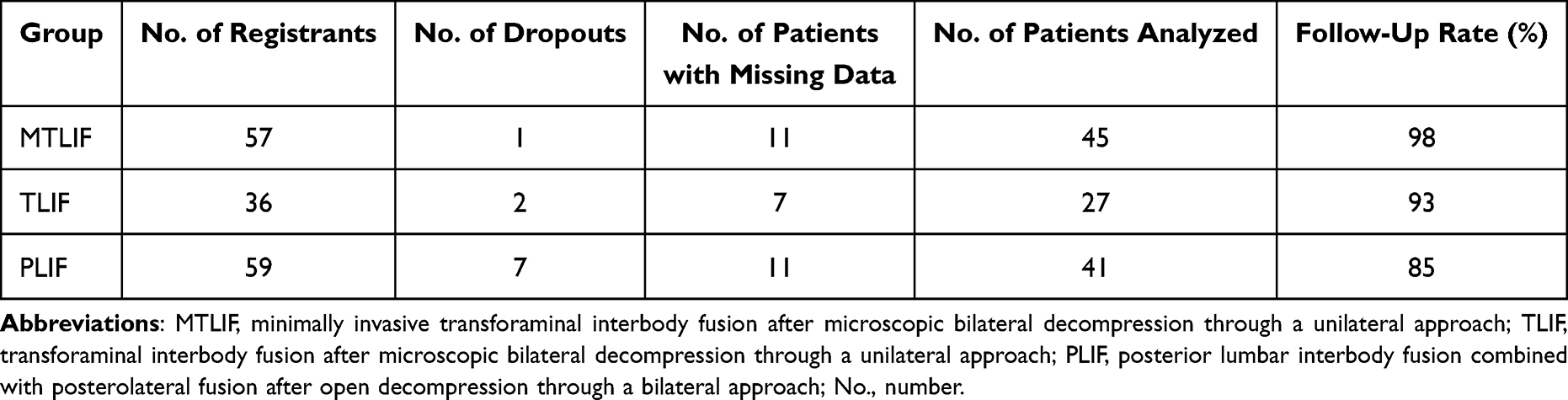 |
Table 1 Patients’ Registry |
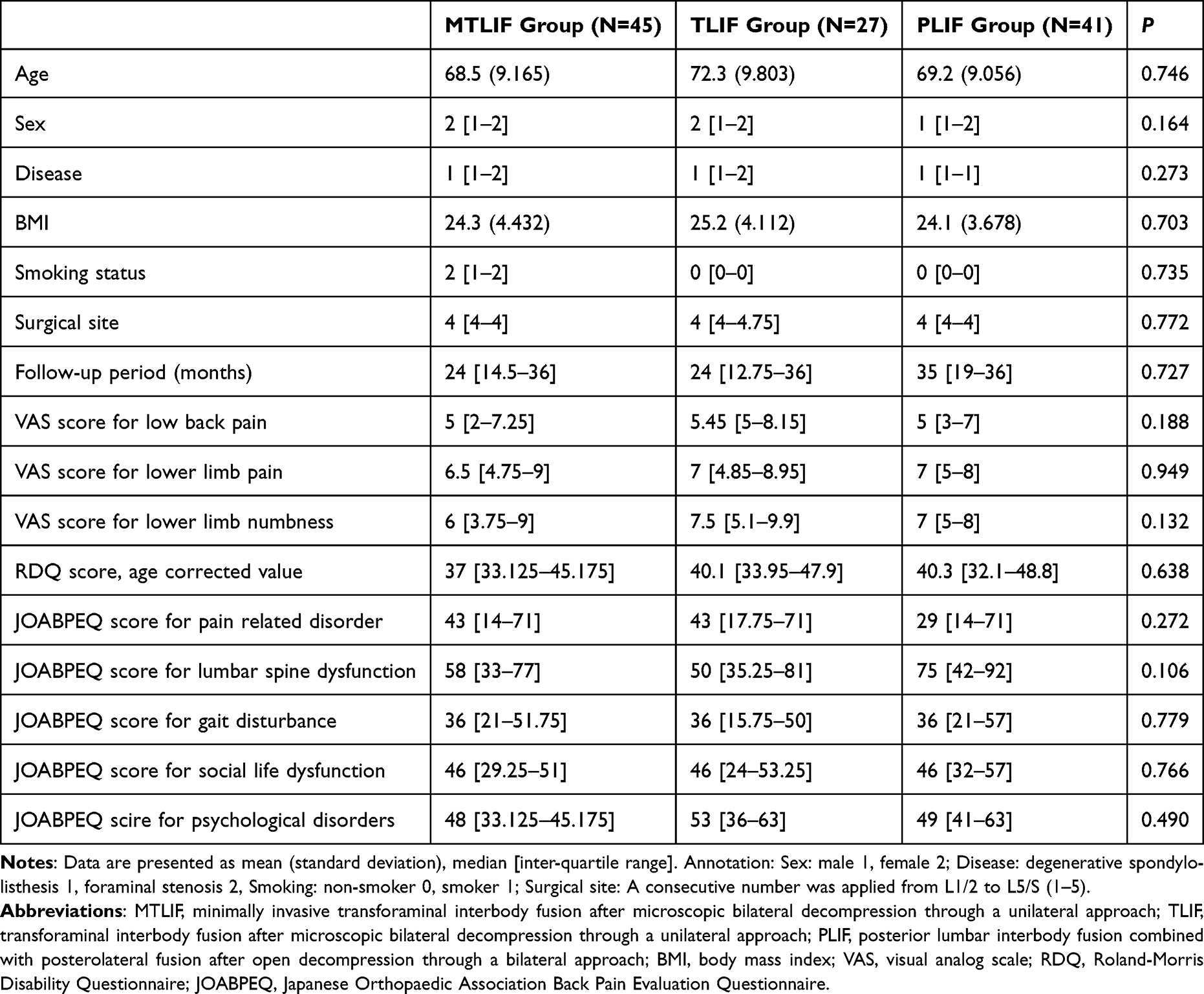 |
Table 2 Baseline Characteristics of the Three Groups |
Main Analyses
The surgical time of the TLIF group was significantly longer than those of the other two groups (P < 0.0001, TLIF group 237±37 min., MTLIF group 202±29 min., PLIF group 209±35 min.; mean±SD) The amount of bleeding during surgery of the TLIF group was also higher than those of the other two groups (P = 0.009, TLIF group 576±213 mL., MTLIF group 433±210 mL., PLIF group 488±199 mL.; mean±SD). There were no significant differences in surgical time and amount of bleeding between MTLIF and PLIF groups.
There were no statistically significant differences in all the scores of outcome measures among the three groups at the final follow-up (Table 3). The JOABPEQ score for pain-related disorders at 6 months postoperatively was statistically significantly higher in the MTLIF group than in the other two groups (P = 0.023, Table 4). There were no statistically significant differences in the scores of the other outcome measures among the three groups during the entire follow-up period. There were also no statistically significant differences in the graft bone union rate among the three groups (Table 5).
 |
Table 3 Outcomes at the Final Follow-Up |
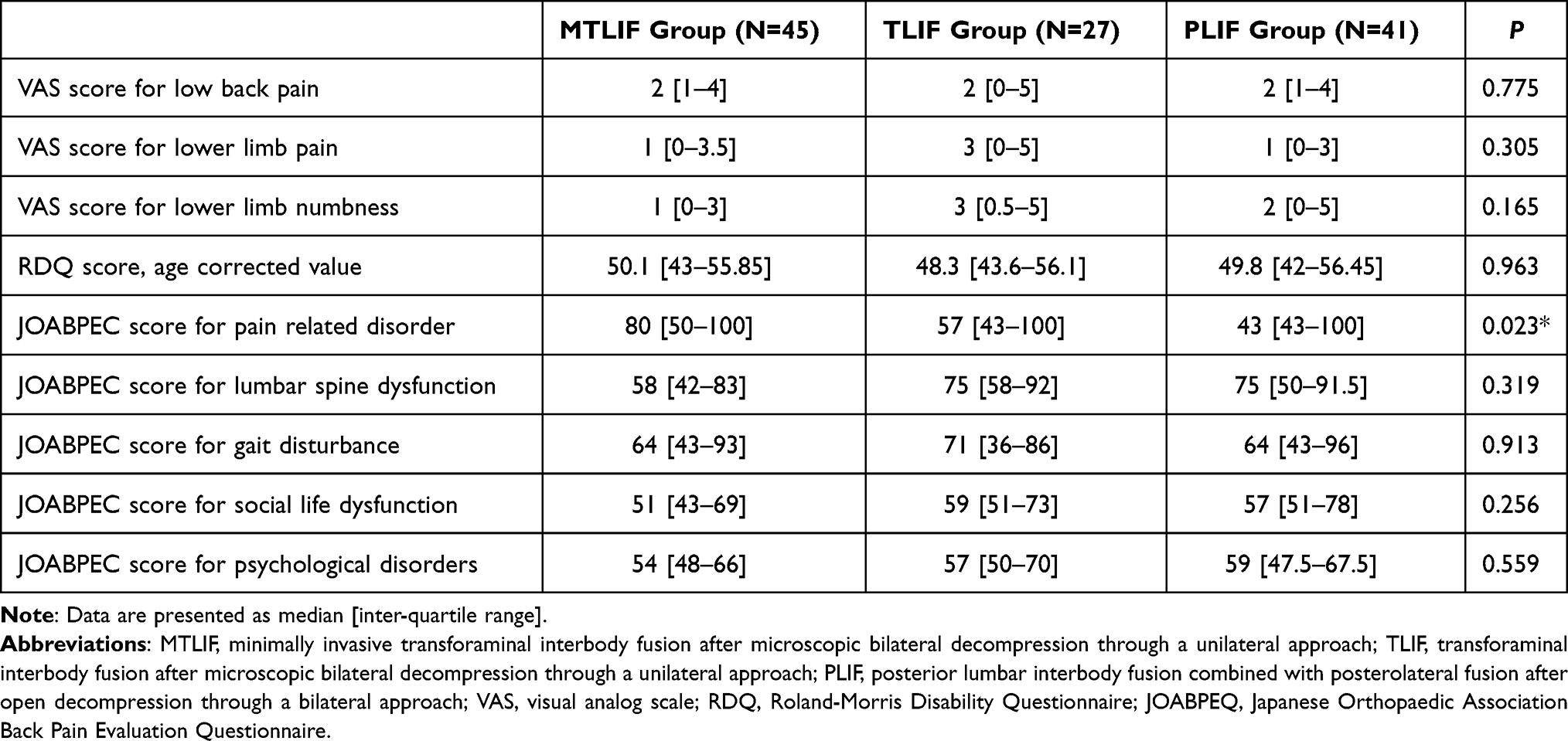 |
Table 4 Outcomes at 6 Months Postoperatively |
 |
Table 5 Union Rate of Intervertebral Graft Bone |
Discussion
The current study demonstrated that the JOABPEQ score for pain-related disorders at 6 months postoperatively was significantly better in MTLIF group than in the other groups. Since lumbar degenerative diseases mostly consisted in elderly patients, less invasive surgeries are desirable. MTLIF resulted in a better health-related QOL (HR-QOL) at 6 months postoperatively, and its outcomes at the final follow-up were non-numerical inferiority.
There are many comparative investigations between minimally invasive transforaminal interbody fusion and open transforaminal interbody fusion/posterior interbody fusion.8–22 The results of long-term outcomes are almost the same among them. Especially, a representative study of a meta-analysis showed equivalent long-term outcomes between open and minimally invasive transforaminal interbody fusion surgeries.20 However, the current study demonstrated that MTLIF resulted in a better HR-QOL at 6 months after surgery. Minimally invasive TLIF using percutaneous posterior fixation has been described to reduce iatrogenic injury to the soft tissue caused by retraction of the paraspinal muscles through the conventional spinal approach.4–7 Accordingly, patients who underwent MTLIF are thought to have early improvement of the disorders due to pain because of its less invasiveness to the paraspinal muscles. For this reason, MTLIF is desirable surgery especially for elderly patients with degenerative spinal diseases.
In perioperative outcomes, the surgical time of the TLIF group was significantly longer than those of the other two groups and the amount of bleeding during surgery of the TLIF group was also higher than those of the other two groups. There were no significant differences in surgical time and the amount of bleeding between MTLIF and PLIF groups. The reason for these results was due to the operator’s factor. The junior surgeon who performed the TLIF was not familiar with the TLIF procedure when he started the TLIF. Thus, we think that the operator’s learning curve for the TLIF induced these results.
The current study has several strengths. Firstly, it is clinically meaningful that the three surgical treatments were simultaneously performed by only two surgeons at a single center, and the surgical indication was completely same between the surgeons. Secondly, the results were acquired under the same perioperative conditions and the same postoperative treatments including the rehabilitation program for each group at a single center.
Despite these strengths, the current study has some limitations. Firstly, the patients were not randomly categorized into the three groups. One junior surgeon performed MTLIF and TLIF for the patients on their first visit to the outpatient on every Monday when the junior surgeon took charge. TLIF was performed from 2010 to 2014, and MTLIF was performed after 2014, when the CT-based navigation system was introduced. The other senior surgeon performed PLIF for the patients on their first visit to the outpatient on every Tuesday when the senior surgeon took charge. PLIF was performed from 2010 to 2014. Thus, patients were not randomized, but they were not intentionally categorized into the three groups. Hence, the demographic and clinical data at baseline were not significantly different among the three groups. Secondary, long-term outcomes of >5 years were not determined. Nevertheless, it is clinically meaningful that the current study revealed the superiority of MTLIF in terms of short-term outcomes.
Conclusion
The current study demonstrated that the JOABPEQ score for pain-related disorders at 6 months postoperatively was significantly better in MTLIF group than in the other groups. Since lumbar degenerative diseases mostly consisted in elderly patients, less invasive surgeries are desirable. MTLIF resulted in a better HR-QOL at 6 months postoperatively, and its outcomes at the final follow-up were non-numerical inferiority. The results strongly indicate that MTLIF is desirable surgery especially for elderly patients with degenerative spinal diseases.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cloward BB. The treatment of ruptured lumbar intervertebral discs by vertebral body fusion. I. Indications, operating technique, after care. J Neurosurg. 1953;10:154–168. doi:10.3171/jns.1953.10.2.0154
2. Suk SI, Lee CK, Kim WJ, Lee JH, Cho KJ, Kim HG. Adding posterior lumbar interbody fusion to pedicle screw fixation and posterolateral fusion after decompression in spondylolitic spondylolisthesis. Spine. 1997;22:210–219. doi:10.1097/00007632-199701150-00016
3. Harms J, Rolinger H. Die operative Behandlung der Spondylolisthese durch dorsale Aufrichtung und ventrale Verblockung [A one-stager procedure in operative treatment of spondylolistheses: dorsal traction-reposition and anterior fusion (author’s transl)]. Z Orthop Ihre Grenzgeb. 1982;120:343–347. German. doi:10.1055/s-2008-1051624
4. Tsutsumimoto T, Shimogata M, Ohta H, Misawa H. Mini-open versus conventional open posterior lumbar interbody fusion for the treatment of lumbar degenerative spondylolisthesis: comparison of paraspinal muscle damage and slip reduction. Spine. 2009;34:1923–1928. doi:10.1097/BRS.0b013e3181a9d28e
5. Shunwu F, Xing Z, Fengdong Z, Xianggian F. Minimally invasive transforaminal lumbar interbody fusion for the treatment of degenerative lumbar diseases. Spine. 2010;35:1615–1620. doi:10.1097/BRS.0b013e3181c70fe3
6. Karikari IO, Grossi PM, Nimjee SM, et al. Minimally invasive lumbar interbody fusion in patients older than 70 years of age: analysis of peri- and postoperative complications. Neurosurgery. 2011;68:897–902;discussion 902. doi:10.1227/NEU.0b013e3182098bfa
7. Lee JC, Jang HD, Shin BJ. Learning curve and clinical outcomes of minimally invasive transforaminal lumbar interbody fusion: our experience in 86 consecutive cases. Spine. 2012;37:1548–1557. doi:10.1097/BRS.0b013e318252d44b
8. Wang J, Zhou Y, Feng Zhang Z, Qing LC, Jie Zheng W, Liu J. Comparison of the clinical outcome in overweight or obese patients after minimally invasive versus open transforaminal lumbar interbody fusion. J Spinal Disord Tech. 2014;27:202–206. doi:10.1097/BSD.0b013e31825d68ac
9. Terman SW, Yee TJ, Lau D, Kahn AA, La marca F, Park P. Minimally invasive versus open transforaminal lumbar interbody fusion: comparison of clinical outcomes among obese patients. J Neurosurg Spine. 2014;20:644–652. doi:10.3171/2014.2.SPINE13794
10. Wu WJ, Liang Y, Zhang XK, Cao P, Xheng T. Complications and clinical outcomes of minimally invasive transforaminal lumbar interbody fusion for the treatment of one- or two-level degenerative disc diseases of the lumbar spine in patients older than 65 years. Chin Med J. 2012;125:2505–2510.
11. Rodriguez-Vela J, Lobo-Escolar A, Joven E, Muñoz-Marín J, Herrera A, Velilla J. Clinical outcomes of minimally invasive versus open approach for one-level transforaminal lumbar interbody fusion at the 3- to 4-year follow-up. Eur Spine J. 2013;22:2857–2863. doi:10.1007/s00586-013-2853-y
12. Adogwa O, Parker SL, Bydon A, McGirt MJ, McGirt MJ. Comparative effectiveness of minimally invasive versus open transforaminal lumbar interbody fusion: 2-year assessment of narcotic use, return to work, disability, and quality of life. J Spinal Disord Tech. 2011;24:479–484. doi:10.1097/BSD.0b013e3182055cac
13. Tian NF, Wu YS, Zhang XL, Xu HZ, Chi YL, Mao FM. Minimally invasive versus open transforaminal lumbar interbody fusion: a meta-analysis based on the current evidence. Eur Spine J. 2013;22:1741–1749. doi:10.1007/s00586-013-2747-z
14. Sun ZJ, Li WJ, Zhao Y, Qiu GX. Comparing minimally invasive and open transforaminal lumbar interbody fusion for treatment of degenerative lumbar disease: a meta-analysis. Chin Med J. 2013;126:3962–3971.
15. Phan K, Rao PJ, Kam AC, Mobbs RJ. Minimally invasive versus open transforaminal lumbar interbody fusion for single-level degenerative disease: a systematic review and meta-analysis of randomized controlled trials. Eur Spine J. 2015;24:1017–1030. doi:10.1007/s00586-015-3903-4
16. Qu J, Tang Y, Wang M, Xu-Dong T, Tian-Jian Z, Guo-Hua S. Comparison of MIS vs. open PLIF/TLIF with regard to clinical improvement, fusion rate, and incidence of major complication: a meta-analysis. Eur Spine J. 2015;24:1058–1065. doi:10.1007/s00586-015-3890-5
17. Khan NR, Clark AJ, Lee SL, Venable GT, Rossi NB, Foley KT. Surgical outcomes for minimally invasive vs open transforaminal lumbar interbody fusion: an updated systemic review and meta-analysis. Neurosurgery. 2015;77:847–874. doi:10.1227/NEU.0000000000000913
18. Putzier M, Hartwig T, Hoff EK, et al. Minimally invasive TLIF leads to increased muscle sparing of the multifidus muscle but not the longissimus muscle compared with conventional PLIF-A prospective randomized clinical trial. Spine J. 2016;16:811–819. doi:10.1016/j.spinee.2015.07.460
19. Miller LE, Bhattacharyya S, Pracyk J. Minimally invasive versus open transforaminal lumbar interbody fusion for single level degenerative disease: a systemic review and meta-analysis of randomized controlled trials. World Neurosurg. 2019;133:358–365. doi:10.1016/j.wneu.2019.08.162
20. Hammad A, Wirries A, Ardeshiri A, Nikiforov O, Geiger F. Open versus minimally invasive TLIF: literature review and meta-analysis. J Orthop Surg Res. 2019;14:229. doi:10.1186/s13018-019-1266-y
21. Schizas C, Tzinieris N, Tsiridis E, Kosmopoulos V. Minimally invasive versus open transforaminal lumbar interbody fusion: evaluating initial experience. Int Orthop. 2009;33:1683–1688. doi:10.1007/s00264-008-0687-8
22. Parker SL, Mendenhall SK, Shau DN, et al. Minimally invasive versus open transforaminal lumbar interbody fusion for degenerative spondylolisthesis: comparative effectiveness and cost-utility analysis. World Neurosurg. 2014;82:230–238. doi:10.1016/j.wneu.2013.01.041
23. Rolland M, Morris R. A study of the natural history of back pain. Part 1: development of a reliable and sensitive measure of disability in low-back-pain. Spine. 1983;8:141–144. doi:10.1097/00007632-198303000-00004
24. Fukui M, Chiba K, Kawakami M, et al. Japanese orthopaedic association back pain evaluation questionnaire. part 2. verification of its reliability: the subcommittee on low back pain and cervical myelopathy evaluation of the clinical outcome committee of the Japanese orthopaedic association. J Orthop Sci. 2007;12(6):526e32.
25. Fukui M, Chiba K, Kawakami M, et al. Japanese orthopaedic association back pain evaluation questionnaire. Part 3 validity study and establishment of the measurement scale: subcommittee on low back pain and cervical myelopathy evaluation of the clinical outcome committee of theJapanese orthopaedic association, Japan. J Orthop Sci. 2008;13(3):173e9.
26. Fukui M, Chiba K, Kawakami M, et al. Subcommittee of the clinical outcome committee of the Japanese orthopaedic association on low back pain and cervical myelopathy evaluation. JOA Back pain evaluation questionnaire (JOABPEQ)/JOA cervical myelopathy evaluation questionnaire (JOACMEQ). The report on the development of revised versions. April 16, 2007. The subcommittee of the clinical outcome committee of the Japanese orthopaedic association on low back pain and cervical myelopathy evaluation. J Orthop Sci. 2009;14(3):348e65.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.