")
Back to Journals » Clinical Optometry » Volume 13
Mini-Scleral Contact Lens for Asian Eyes Post-Penetrating Keratoplasty with Smaller Palpebral Aperture: Case Reports
Authors Kim H , Yanase Park T, Joo CK
Received 9 January 2021
Accepted for publication 4 May 2021
Published 20 May 2021 Volume 2021:13 Pages 161—166
DOI https://doi.org/10.2147/OPTO.S295238
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Mr Simon Berry
Video abstract presented by Tiffany Yanase Park.
Views: 292
Hyojin Kim,1 Tiffany Yanase Park,2 Choun-Ki Joo3
1Department of Optometry, Baekseok University, Cheonan, Republic of Korea; 2Department of Ophthalmology, Loma Linda University, Loma Linda, CA, USA; 3CK St.Mary’s Eye Center, Seoul, Republic of Korea
Correspondence: Choun-Ki Joo
CK St. Mary’s Eye Center, Kangnamdae-ro 91-5, Seoul, 06530, Korea
Tel +82-2-516-3434
Fax +82-41-550-2829
Email [email protected]
Purpose: To report the use of miniscleral contact lenses (MSCLs) with diameter of 14.7 mm for Asian eyes to improve vision in patients after penetrating keratoplasty (PKP) surgery.
Methods: Two patients with high corneal astigmatism post-PKP were evaluated for a contact lens fitting. Visual acuity, slit lamp, and anterior segment OCT findings before and after fitted the lens of 14.7 mm diameter were recorded.
Results: A Kmax of case 1 and 2 were 52.8 D and 76.9 D, respectively at the first visit. Both patients were successfully fit with MSCLs, showing adequate corneal clearance of over 250 μm with no corneal touch on OCT and sufficient limbal clearance and edge alignment. MSCLs use resulted in improved comfort and visual acuity of 20/30 or better.
Conclusion: MSCLs with diameter of 14.7 mm can be considered a safe and effective option for patients with highly steep corneas post-PKP surgery in Asian eyes.
Keywords: scleral lenses, miniscleral lenses, irregular cornea, penetrating keratoplasty
Introduction
Miniscleral contact lenses (MSCLs) are especially beneficial for patients with corneas incompatible with other lens designs. The lenses land on conjunctiva while vaulting over the cornea with a fluid reservoir, simultaneously providing corneal hydration and optical correction.1 Another advantage is the ability to precisely tailor every aspect of the fit. A MSCLs has an overall diameter up to 6 mm larger than the horizontal visible iris diameter (HVID).1
Numerous reports have shown the promising therapeutic potential of scleral lenses in keratoconus,2 irregular corneas,2,3 corneal ectasias,4 and corneas post-PKP.5 This study reports the use of a Onefit A 14.7 mm diameter MSCLs (Blanchard Contact Lenses, CooperVision, Lake Forest, California, USA) to improve vision in two patients with high corneal astigmatism after PKP. Both patients were treated at CK St. Mary’s Eye Center in Seoul, South Korea from 2019 September to 2020 June. The study protocol was approved by the CK Ethical Committee of the CK Mary’s Eye Clinic (Seoul, South Korea) (No. CK_IRB_2020002). Informed consent was obtained from both patients to publish their case details and associated images.
Case 1
A 53-year-old man presented to our clinic for post-PKP follow-up. He had a history of phacoemulsification with IOL implantation in the left eye in July 2015 and unilateral PKP of the left eye in October 2015. The PKP was required due a penetrating knife injury to the eye.
He complained of reduced vision in the left eye and severe asthenopia due to significant anisometropia. He also reported moderate eye pain, redness, and a foreign body sensation in the left eye that had been worsening for more than two weeks. UCVA (uncorrected visual acuity) in the left eye was 4/200 and BCVA (best corrected visual acuity) in the right eye was 20/20 with SMR (subjective manifest refraction) of Plano −0.50 x 015. The suture was removed at the slit lamp without complications, and BCVA in the left eye was 8/200 with SMR of plano –12.00 x 085.
Figure 1A shows the corneal topography of his left eye using Pentacam HR (Oculus Inc., Wetzlar, Germany). Simulated keratometry (simK in D) was assessed at the flattest (Flat) and steepest (Steep) meridians. His simK values were 40.6D @ 005/50.7D @ 175, resulting in a notable 10 D of astigmatism between Flat and Steep. The anterior corneal curvatures using an auto-keratometer (ARK-1; Nidek Co., Ltd, Gamagori, Japan) were 38.5D @ 005/49.75D @ 175. The thinnest corneal pachymetry and posterior elevation showed 547 μm and 76 μm, respectively. His white-to-white by Pentacam HR, which is the horizontal distance between the corneal limbal borders, was 11.1 mm. His vertical palpebral aperture (PA) was 10.08 mm.
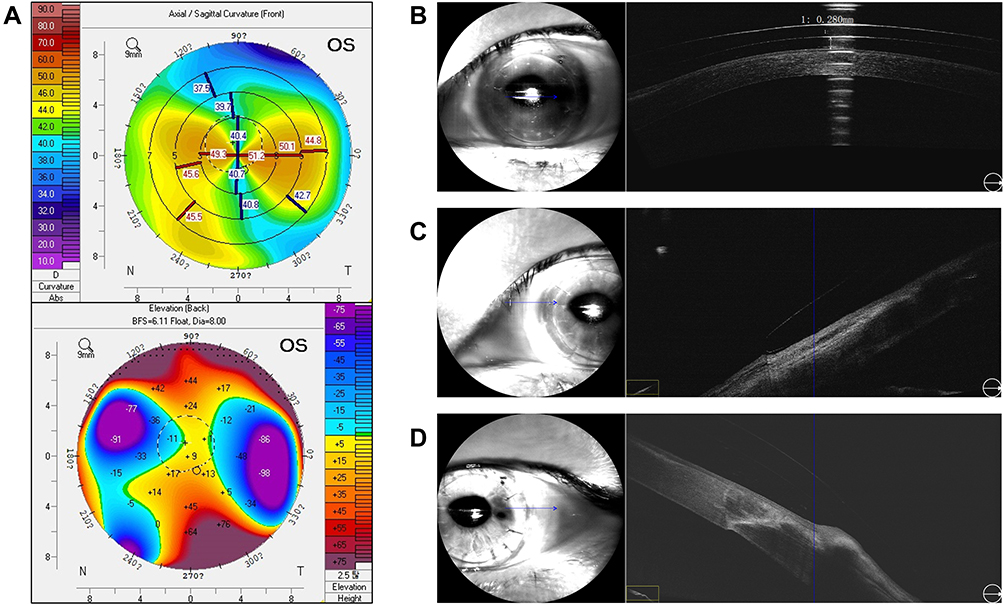 |
Figure 1 Corneal topography before wearing scleral lenses as measured with Pentacam (A) and OCT illustrating good central clearance (B), edge assessment of nasal (C) and temporal location (D) in case 1. The blue arrow corresponds to the directionality of the scan in relation to adjacent OCT cross section. |
The patient’s left eye was fit with a Onefit A MSCL (Blanchard Contact Lenses, CooperVision, Lake Forest, California, USA). The lens is made with 100 Dk material of hexafocon A (Acuity Polymers, Inc. Rochester, NY). The lens made with 100 Dk material of hexafocon A (Acuity Polymers, Inc. Rochester, NY) was first introduced in April 2016. Its oxygen permeability and water content were 111 [10−11 mL O2 cm/(cm2·s·mmHg) @ 35°C], and <1%, respectively. As well as, it was transformed into the following form than the original model which is Onefit 2.0 to fit better for Asian; smaller diameter and prolate shape, in other words lower sagittal height (Figure 2). It is a geometry design with anterior aspheric surface that is specified to made to Asian, reducing only central clearance while maintaining the peripheral limbal clearance and edge alignment as shown in Figure 2. The Onefit A scleral design is smaller, with a different para central to edge geometry than fond with scleral lenses designed for Caucasian eyes. Therefore, it can provide Asian with more prolate cornea enough vaults even with a small diameter than Onefit 2.0 scleral lenses for Caucasian. An 8.30 mm base curve lens was selected based on the flat K value (8.31 mm). A lens diameter of 14.7 mm, large enough to vault over her white-to-white without corneal apical or limbal touch, was selected.
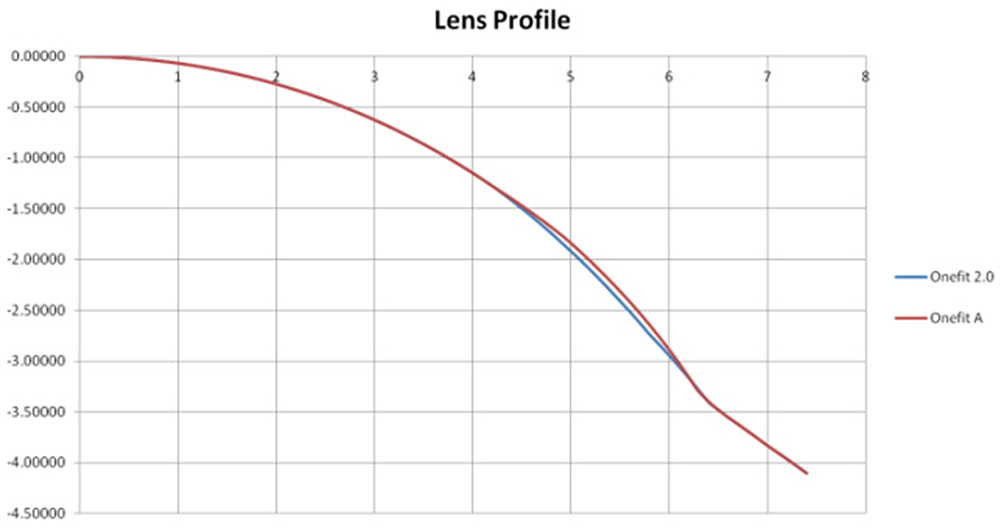 |
Figure 2 Comparison of lens design between onefit 2.0 and onefit A. |
The corneal apical clearance was judged 30 minutes after insertion by noting the space between the anterior and posterior surface of the lens on slit-lamp with fluorescein. The lens should move slightly on pushed up by slightly pressing conjunctiva with a finger on the first insertion (about 0.5 mm). Then the desired clearance after lens settling was confirmed using AS-OCT (Mocean 4000, Moptim Inc, Shenzhen, China) again (Figure 1B). Initially, the 8.30 mm base curve lens did not provide ample apical clearance, so multiple steeper lenses were trialed until an apt vault of 280 μm using a ruler of the picture over the steepest part of the cornea was achieved. Appropriate apical clearance with an 8.00 mm base curve, 14.7 mm diameter lens is showed with an AS-OCT in Figure 1B.
Good limbal clearance was judged by the visible presence of fluorescein extending beyond the limbus with diffuse white light and also with optic section from slit-lamp Scleral landing zones were assessed subjectively at the slit lamp, by diffuse white light for impingement of blood vessels and by a broad parallelepiped beam for edge lift. Shortly after insertion of the lens, there was moderate edge lift along the horizontal meridian. After the lens settled for four hours, alignment improved as seen on slit lamp and AS-OCT (Figure 1C and D). The patient was asymptomatic for lens awareness and no evidence of excessive tear exchange. Therefore, no toric periphery was used.
The trial lens ordered using over-refraction data and the fitting findings was 8.00 mm base curve, 14.7 mm diameter lens with −3.00 power. On the first day, it was recommended to wear for 4 hours, and wearing time was asked. If there were no symptoms of redness or any discomfort, it was recommended to wear it for up to 8 hours a day. At the 1-week follow-up, the patient was very satisfied with his vision and comfort. His final visual acuity was 20/20 with adequate central clearance, limbal clearance and edge alignment. At the 1-month visit, he had no pain, redness, and foreign body sensation and no corneal complications. After 1 month, it was continuously recommended to wear it for 8 hours a day, and it was allowed to wear it all day except when sleeping. At the 4-month visit, he still had improved vision of 20/20 in left eye.
Case 2
A 41-year-old woman presented to us with complaints of poor vision and conjunctival redness. She had a history of unilateral PKP of the right eye in 1994 due to a corneal ulcer. Her UCVA of the right eye was 20/200 and her SMR was −3.75 −10.50 x 088 with no visual improvement. BCVA in the left eye was 20/20 with a SMR of −0.25 −0.75 x 172.
Her corneal topography of the right eye showed significant astigmatism and a superiorly displaced corneal apex (Figure 3A). Her sim KS were 45.9D @ 087/49.6D @ 177 and Kmax was a remarkable 76.9 D. Her the flat K value was 7.61 mm and the anterior corneal curvatures based on autokeratometer were 42.5D @ 088/49.75D @ 178. The thinnest corneal pachymetry was 521 μm. Her white-to-white and PA were 11.5 mm and 10.46 mm, respectively. Her posterior elevation was 96.5 μm.
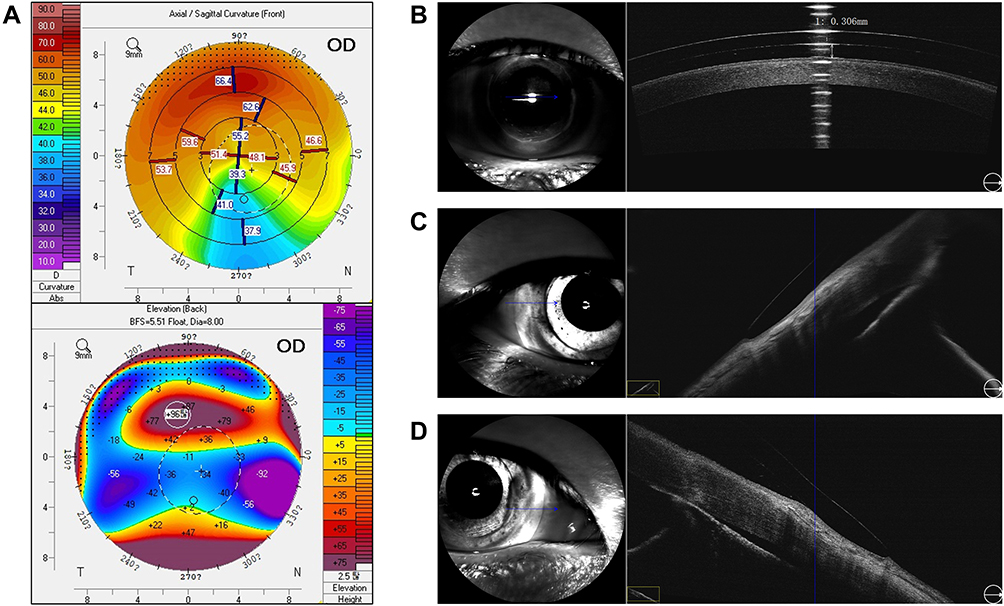 |
Figure 3 Corneal topography before wearing scleral lenses as measured with Pentacam (A) and OCT illustrating good central clearance (B), edge assessment of nasal (C) and temporal location (D) in case 2. The blue arrow on the left means the central blue line of OCT cross section in the right photo. |
A MSCL Onefit A diagnostic lens with 14.7 mm diameter and 7.10 mm base curve was trialed based on Pentacam data. As this initial lens did not provide acceptable apical corneal clearance, the base curve was adjusted to an eventual radius of 6.90 mm of base curve. The subsequent fitting process was done similar to that of case 1, evaluating the fit after insertion and after four hours of lens settling. The apical cornea and landing zone relationships were assessed with AS-OCT, as seen in Figure 3B–D). Given the great fit and reliable over-refraction findings, a trial lens of 6.90 mm base curve, 14.7 mm diameter lens, −10.50 power was ordered.
She was comfortably wearing the lenses for 12 hours per day with no signs of redness or vision complaints at the 1-week follow-up. Her final visual acuity was 20/30 with adequate central clearance, limbal clearance and edge alignment. At the 1-month, she still reported good vision and subjectively described the lenses to be comfortable Also, no contact lens related complications were observed.
Discussion
PKP is a frequently used treatment option for advanced keratoconus when refractive management is no longer satisfactory. Though some patients achieve successful visual improvement after PKP, many studies account for challenging visual sequalae. Corneal scarring, reduced BCVA, as well as pronounced corneal steepening have been documented.6 Aside from limited evidence in support of astigmatic keratotomy,7 contact lenses are often the option of choice to mitigate these consequential visual problems.8
Effective post-operative care is a critical consideration, as the average amount of resultant astigmatism after PKP was 5.22 D in post-operative 1 year.9 Favorable visual outcomes have been demonstrated recently using MSCLs for astigmatism after PKP. Alipour et al10 showed more than 5 lines of improvement from BCVA with spectacle by fitting eyes post-PKP with a 15.8 mm diameter MSCLs. In another study, Barnett et al1 showed success fitting eyes post-PKP with lenses ranging in diameters of 15.6 to 18.4 mm, with nearly 92% of eyes achieving functional visual acuity of 20/40 or better. A majority of other studies using scleral lenses ranging from 15 mm to 24 mm in diameter effectively improved vision for irregular astigmatism.9 In addition, recently vision-related quality of life has also improved after wearing MSCL in keratoconus and irregular corneas.3,9
Despite these advantages the most common reason for discontinuing scleral lens wear was due to insertion and removal difficulties.1 This may be more pronounced in the Asian population, as anatomical differences for East Asian eyes include significantly smaller HVID, smaller palpebral apertures, and smaller corneas than white eyes.11 A better understanding of ethnic variations of the eye and ocular adnexa will optimize development of contact lenses for the Asian market. In the present study, we used the Onefit A lens with a smaller diameter than previous lenses. It is specifically designed to benefit patients with smaller interpalpebral fissures and maintain all of the benefits of a larger diameter scleral lens. This is the first known case series to use the Onefit A lens, and should be considered as a viable option for patients having difficulty handling or inserting larger diameter lenses. Since large diameter scleral lenses are not widely distributed in South Korea, the OneFit A miniscleral lens is well designed to be a viable option for this population. The most significant barrier to wear is the cost of the lens, as the miniscleral lenses are not covered under government health insurance in Korea. It is approximately twice as expensive as standard rigid gas permeable lenses. Corneal specialists in Korea can consider this case series and the established evidence of efficacy to include mini scleral lenses as a treatment option for complications after PKP.
Conclusions
This case reports describes our experience and the results of MSCLs fitting with small HIVD after PKP. Our cases revealed that high corneal astigmatism, even more than 10.0 diopters, associated with PKP can be successfully managed with MSCLs. These results suggest that MSCLs are also an excellent option in the treatment of steep corneas after PKP in Asian eyes.
Acknowledgment
The authors wish to thank Sun-A Park for assisting with patient examination for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Barnett M, Lien V, Li JY, Durbin-Johnson B, Mannis M. Use of scleral lenses and miniscleral lenses after penetrating keratoplasty. Eye Contact Lens. 2016;42(3):185–189. doi:10.1097/ICL.0000000000000163
2. Visser ES, Van der Linden BJ, Otten HM, Van der Lelij A, Visser R. Medical applications and outcomes of bitangential scleral lenses. Optom Vis Sci. 2013;90(10):1078–1085. doi:10.1097/OPX.0000000000000018
3. Abou Samra WA, Badawi AE, Kishk H, Abd El Ghafar A, Elwan MM, Abouelkheir HY. Fitting tips and visual rehabilitation of irregular cornea with a new design of corneoscleral contact lens: objective and subjective evaluation. J Ophthalmol. 2018;2018:3923170. doi:10.1155/2018/3923170
4. Baran I, Bradley JA, Alipour F, Rosenthal P, Le HG, Jacobs DS. PROSE treatment of corneal ectasia. Cont Lens Anterior Eye. 2012;35(5):222–227. doi:10.1016/j.clae.2012.04.003
5. Pecego M, Barnett M, Mannis MJ, Durbin-Johnson B. Jupiter scleral lenses: the UV Davis Eye Center experience. Eye Cont Lens. 2012;38(3):179–182. doi:10.1097/ICL.0b013e31824daa5e
6. Sray WA, Cohen EJ, Rapuano CJ, Laibson PR. Factors associated with the need for penetrating keratoplasty in keratoconus. Cornea. 2002;21(8):784–786. doi:10.1097/00003226-200211000-00011
7. Bohringer D, Dineva N, Maier P, et al. Long-term follow-up of astigmatic keratotomy for corneal astigmatism after penetrating keratoplasty. Acta Ophthalmol. 2016;94(7):e607–e611. doi:10.1111/aos.13061
8. Romero-Jimenez M, Santodomingo-Rubido J, Wolffsohn JS. Keratoconus: a review. Cont Lens Anterior Eye. 2010;33(4):157–166. doi:10.1016/j.clae.2010.04.006
9. Oh BL, Kim MK, Wee WR. Comparison of clinical outcomes of same-size grafting between deep anterior lamellar keratoplasty and penetrating keratoplasty for keratoconus. Korean J Ophthalmol. 2013;27(5):322–330. doi:10.3341/kjo.2013.27.5.322
10. Alipour F, Behrouz MJ, Samet B. Mini-scleral lenses in the visual rehabilitation of patients after penetrating keratoplasty and deep lamellar anterior keratoplasty. Cont Lens Anterior Eye. 2015;38(1):54–58. doi:10.1016/j.clae.2014.10.001
11. Hickson-Curran S, Young G, Brennan N, Graeme Y. Comparative evaluation of Asian and white ocular topography. Optom Vis Sci. 2014;91(12):1396–1405. doi:10.1097/OPX.0000000000000413
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.