Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Mindfulness-Based Spiritual Interventions for Patients with Advanced Cancer Receiving Palliative Care: A Systematic Review of Randomized Controlled Trials
Authors Sinaga F, Komariah M ![]() , Haroen H, Agustina HR
, Haroen H, Agustina HR ![]()
Received 14 April 2026
Accepted for publication 4 July 2026
Published 10 July 2026 Volume 2026:19 616728
DOI https://doi.org/10.2147/JMDH.S616728
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Friska Sinaga,1 Maria Komariah,2 Hartiah Haroen,3 Hana Rizmadewi Agustina2
1Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Department of Fundamental Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia; 3Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia
Correspondence: Friska Sinaga, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia, Email [email protected]
Background: Psychological and spiritual distress are highly prevalent in patients with advanced cancer, yet conventional interventions often fail to address their interconnected nature. While mindfulness-based interventions (MBIs) are widely used in oncology, their integration with spiritual or meaning-centered components remains insufficiently synthesized in high-level evidence.
Objective: This review aimed to evaluate the effectiveness and characteristics of mindfulness-based spiritual interventions on psychological and spiritual outcomes in patients with advanced and palliative cancer.
Methods: A PRISMA-guided systematic review of randomized controlled trials (RCTs) was conducted using PubMed, Scopus, and CINAHL databases (2015– 2025). Eligible studies included adult patients with cancer receiving mindfulness-based interventions incorporating explicit spiritual, religious, or existential components. Methodological quality was appraised using the Joanna Briggs Institute checklist, and findings were synthesized using qualitative descriptive and narrative synthesis.
Results: Thirteen RCTs were included. The interventions were categorized into (1) hospital-based interventions and (2) remotely delivered interventions. Across these categories, five outcome domains were identified: psychological well-being (anxiety, depression, distress, quality of life), spiritual well-being (meaning, peace, faith, existential acceptance), attrition and treatment engagement, intervention acceptability, and mixed or inconsistent findings.
Conclusion: Mindfulness-based interventions that explicitly integrate spiritual or meaning-centered elements offer a comprehensive approach to addressing multidimensional distress in advanced cancer. These findings suggest that integrative psycho-spiritual care models may be beneficial in oncology and palliative care. Future research should prioritize standardized intervention frameworks and mechanism-driven evaluation across diverse populations.
Keywords: mindfulness-based interventions, spiritual well-being, psychological outcome, advanced cancer, palliative care
Introduction
Cancer remains a major global public health challenge, with an estimated 20 million new cases and 9.7 million cancer-related deaths worldwide in 2022.1 The global cancer burden is projected to increase by approximately 77% by 2050, with the most pronounced rise expected in low- and middle-income countries.2 In many low- and middle-income countries (LMICs), cancer is frequently diagnosed at advanced stages, leading to substantial symptom burden and an increased demand for palliative and supportive care.1,2 This trend highlights persistent disparities in early detection and access to comprehensive oncology services across diverse health care systems.
Beyond its physical consequences, cancer is widely recognized as a condition that profoundly affects psychological and existential well-being across the disease trajectory, particularly in advanced and life-limiting stages.3,4 Patients with cancer frequently experience anxiety, depression, emotional distress, fear of disease progression, and existential concerns related to loss of meaning and control.5,6 Evidence indicates that up to 60–70% of individuals with cancer report clinically significant psychological distress, which may adversely influence symptom perception, treatment adherence, and overall quality of life.7,8
In advanced cancer and palliative care contexts, psychological distress is often closely intertwined with spiritual distress.9,10 Spiritual distress is increasingly recognized as a multidimensional form of suffering that may involve existential concerns related to meaning, purpose, hope, and spiritual needs. In patients with advanced cancer, spiritual distress may arise when serious illness challenges an individual’s sense of meaning, personal beliefs, sources of hope, and connectedness. These concerns frequently coexist with physical symptom burden and psychological distress, contributing to profound suffering among patients with advanced illness.9,10 Spiritual well-being, commonly conceptualized as a sense of meaning, purpose, inner peace, and connectedness to self, others, and transcendence, has been identified as a critical dimension of quality of life in patients facing life-limiting illness.4,11 Higher levels of spiritual well-being have been associated with reduced anxiety and depression, improved coping capacity, and greater acceptance of illness and mortality, whereas unmet spiritual needs are linked to demoralization, hopelessness, and poorer psychosocial outcomes.12,13 Spiritual needs may also vary according to individuals’ beliefs, values, and personal sources of meaning, highlighting the importance of considering diverse patient perspectives when evaluating spiritually oriented interventions.
Palliative care aims to alleviate suffering and improve quality of life through the holistic management of physical symptoms, psychological distress, social challenges, and spiritual concerns.14,15 While pharmacological treatments play a central role in symptom control, they are insufficient to address the complex emotional and existential dimensions of suffering commonly experienced by patients with advanced cancer.16,17 Consequently, there is growing interest in integrative non-pharmacological interventions that simultaneously target psychological and spiritual well-being within palliative care frameworks.18
Mindfulness-based interventions (MBIs) have emerged as promising psychosocial approaches in oncology and palliative care settings.3,19 Mindfulness is generally defined as purposeful, non-judgmental awareness of present-moment experiences that has been shown to enhance emotional regulation, reduce stress, and foster psychological resilience among individuals with chronic and life-threatening illness.20,21 Randomized controlled trials suggest that MBIs, including Mindfulness-Based Stress Reduction (MBSR), Mindfulness-Based Cognitive Therapy (MBCT), and Mindfulness-Based Cancer Recovery (MBCR), are effective in reducing anxiety, depression, and cancer-related distress and improving quality of life in patients with cancer.3,22,23 Although conventional mindfulness-based interventions primarily focus on emotional regulation and psychological adaptation, increasing attention has been directed toward integrating spiritual and existential dimensions to address the deeper concerns frequently experienced by patients with advanced cancer and those receiving palliative care.24,25
Importantly, an increasing body of literature highlights the conceptual and therapeutic overlap between mindfulness and spirituality, particularly in the context of serious illness and end-of-life care.24,25 Mindfulness practices may facilitate acceptance, compassion, existential reflection, and meaning-making, which are core elements of spiritual well-being.26 From a theoretical perspective, mindfulness and spirituality share overlapping processes, including self-awareness, acceptance, meaning-making, and connectedness, which may contribute to enhanced spiritual well-being in individuals facing serious illness.24–26 Several studies indicate that spiritual well-being may mediate the relationship between mindfulness practice and psychological outcomes, suggesting that interventions integrating mindfulness with spiritual components may exert synergistic effects on psychological and existential distress.13,27
In the context of this review, mindfulness-based spiritual interventions refer to structured interventions that combine mindfulness practices with explicit spiritual, religious, existential, or meaning-centered components aimed at enhancing both psychological and spiritual well-being. A growing number of randomized controlled trials have examined mindfulness-based spiritual interventions in cancer care, including Couple-Based Meditation, Religious Prayer Therapy, Individual Meaning-Centered Psychotherapy, and compassion-focused mindfulness programs.12,28,29 These interventions have demonstrated beneficial effects on psychological and spiritual well-being; however, findings remain heterogeneous regarding intervention content, delivery format, outcome measures, and patient populations.
Despite this expanding evidence base, there is currently a lack of systematic synthesis focusing specifically on randomized controlled trials evaluating mindfulness-based spiritual interventions for psychological and spiritual well-being in palliative and advanced cancer care. Existing systematic reviews have primarily focused on the psychological benefits of mindfulness-based interventions, such as reductions in anxiety, depression, and distress, as well as improvements in quality of life among general cancer populations.3,30 However, these reviews rarely examined spiritual well-being as a primary outcome. They did not specifically target patients with advanced or palliative cancer, limiting the applicability of their conclusions to populations facing profound existential and spiritual challenges. Consequently, the effectiveness of mindfulness-based interventions that explicitly incorporate spiritual or meaning-centered elements for improving both psychological and spiritual outcomes in advanced cancer populations remains insufficiently understood. Given the heterogeneity of psychosocial and spiritual interventions in oncology and palliative care, evidence derived from randomized controlled trials provides the most rigorous basis for evaluating intervention effectiveness and minimizing potential sources of bias.
Therefore, this systematic review aimed to synthesize and evaluate evidence from randomized controlled trials on mindfulness-based spiritual interventions among patients with advanced cancer receiving palliative care, with a particular focus on psychological and spiritual outcomes. By clarifying the effectiveness of these interventions, this review may help support the development of holistic care strategies, provide evidence-based recommendations for clinical practice, and facilitate the integration of spiritual care within palliative care settings.
Methods
Study Design
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and was prospectively registered in PROSPERO (CRD420261352990).
Eligibility Criteria
Eligibility criteria were defined a priori using the PICOS framework.
- Population: Adults (≥18 years) diagnosed with advanced-stage or palliative cancer, regardless of cancer type or treatment status.
- Intervention: Mindfulness-based spiritual interventions including mindfulness practices with explicit spiritual, religious, existential, or meaning-centered components.
- Comparison: Usual care, waitlist, or active control without structured mindfulness or spiritual components.
- Outcomes: Psychological well-being (eg, anxiety, depression, distress, quality of life) and spiritual well-being (eg, meaning, inner peace, existential well-being).
- Study Design: Randomized controlled trials.
Studies published in English between January 2015 and December 2025 were included in this systematic review. The restriction to English-language publications was applied to ensure methodological consistency and accuracy in data extraction and critical appraisal, given the absence of resources for professional translation. Moreover, the majority of high-quality randomized controlled trials evaluating mindfulness-based and spiritual interventions in oncology and palliative care are published in English-language peer-reviewed journals. This approach is consistent with established methodological guidance for systematic reviews and is unlikely to compromise the completeness of the evidence base substantially.
The primary outcomes of interest were psychological well-being and spiritual well-being. Psychological well-being included indicators such as anxiety, depression, psychological distress, mood disturbance, fatigue, and quality of life, as assessed using validated instruments reported in the included studies. Spiritual well-being referred to dimensions such as meaning, peace, faith, existential well-being, spiritual coping, and connectedness, typically measured using validated spiritual well-being instruments. Secondary outcomes included intervention acceptability, treatment engagement, attrition, and feasibility, which were extracted when reported.
The publication period was restricted to studies published from 2015 onward to capture contemporary evidence reflecting current theoretical frameworks, standardized intervention protocols, and validated outcome measures in mindfulness-based and spiritual interventions. Earlier studies frequently employed heterogeneous or non-standardized intervention designs and outcome instruments, which may limit comparability and synthesis. This time restriction was applied to enhance methodological homogeneity, clinical relevance, and interpretability of pooled findings, rather than to limit comprehensiveness. In addition, conference abstracts, study protocols, dissertations, theses, and other forms of grey literature were not eligible for inclusion because they generally provide insufficient methodological detail and incomplete outcome data for critical appraisal and evidence synthesis.
Data Collection
Search Strategy
A comprehensive literature search was conducted on January 30, 2026, using electronic databases, including Scopus, CINAHL, and PubMed, to retrieve relevant studies published between 2015 and 2025. The search strategy employed combinations of keywords related to mindfulness, spirituality, cancer, and psychological well-being. The search terms included: “mindfulness-based” OR “mindfulness meditation” OR MBSR AND spiritual OR faith-based OR religious OR spirituality AND cancer OR oncology OR “advanced cancer” OR palliative AND “psychological well-being” OR “mental health” OR anxiety OR depression OR hope OR “inner peace” OR meaning AND intervention OR therapy OR program. More details are provided in Supplementary Table S1.
Study Selection and Quality Appraisal
Study selection was conducted in accordance with the PRISMA guidelines. The selection process consisted of two sequential stages. First, two reviewers independently screened the titles and abstracts to identify potentially eligible articles. Second, the full texts of the selected articles were independently assessed against the predefined inclusion and exclusion criteria.
Following the study selection process, the methodological quality of the included articles was critically appraised using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Randomized Controlled Trials. The JBI checklist was used to identify methodological strengths and potential sources of bias and to support interpretation of the review findings. The appraisal was conducted independently by two reviewers (F.S. and M.K). Each study was evaluated across key JBI domains, including randomization procedures, allocation concealment, baseline comparability, blinding, completeness of follow-up, reliability of outcome measurement, and appropriateness of statistical analysis. No studies were excluded based on quality appraisal results. Any discrepancies between reviewers were resolved through discussion until consensus was reached.
Data Extraction and Analysis
In the data extraction and analysis stage, all included studies were systematically extracted using a structured data extraction form. Key study information was summarized in Table 1 (Characteristics of Studies), which includes sample size, country, intervention characteristics, follow-up (including loss to follow-up), outcomes assessed, and a brief synthesis of the main findings. This table was used to provide an overview of the included evidence and to facilitate comparison across studies in terms of context, intervention type, and outcome patterns.
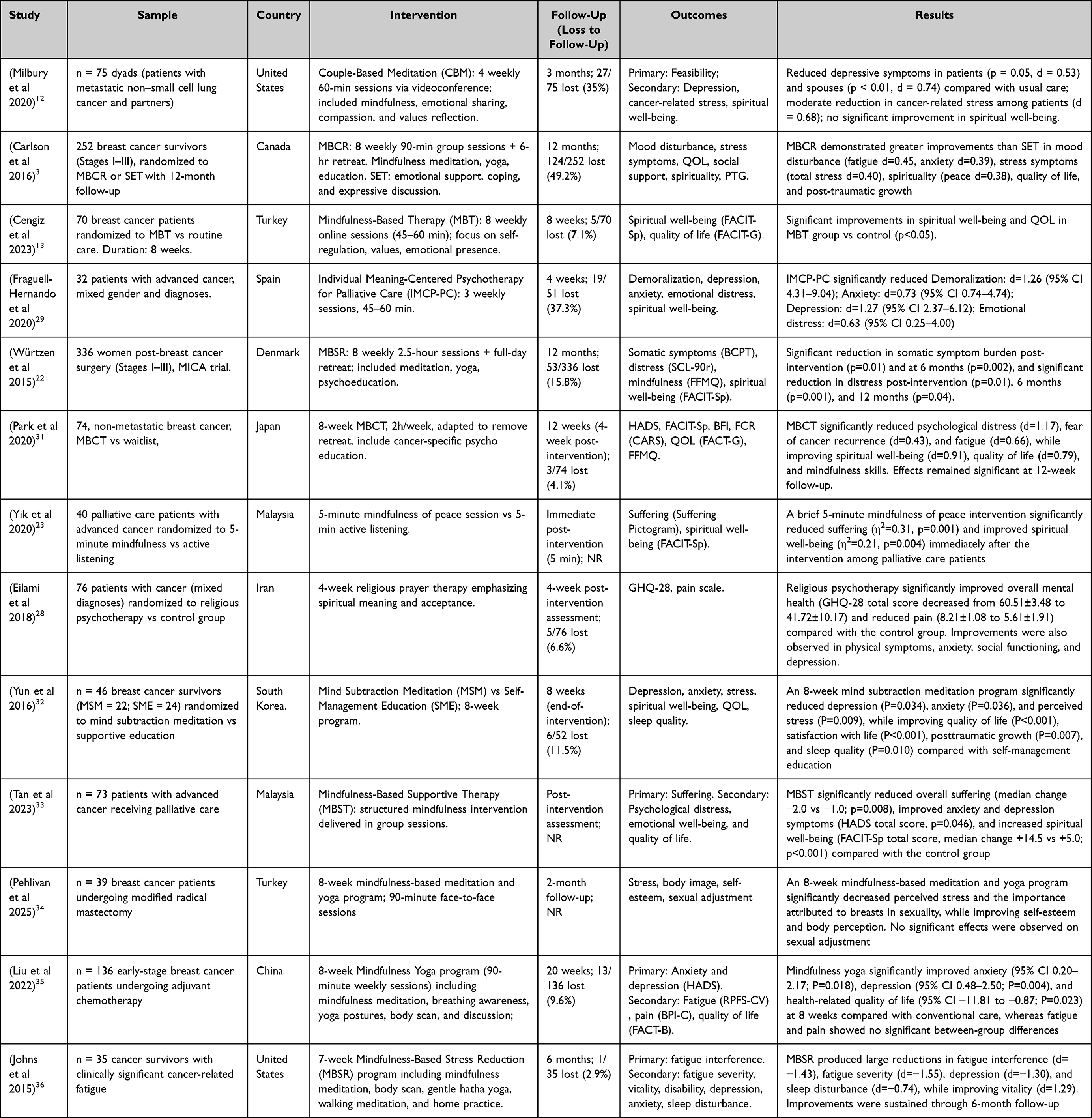 |
Table 1 Characteristics of Studies |
To ensure that intervention reporting was comprehensive and replicable, intervention details were additionally extracted and assessed using the Template for Intervention Description and Replication (TIDieR) checklist, as presented in Table 2. Each article was evaluated according to the TIDieR domains, including the intervention name, rationale for delivery, intervention content and materials, the individuals delivering the intervention, mode of delivery, setting, dose and duration, tailoring, modifications, intervention fidelity (how well it was delivered), and other relevant implementation details. This process strengthened the transparency of intervention reporting and supported the interpretation of how the interventions were implemented across studies.
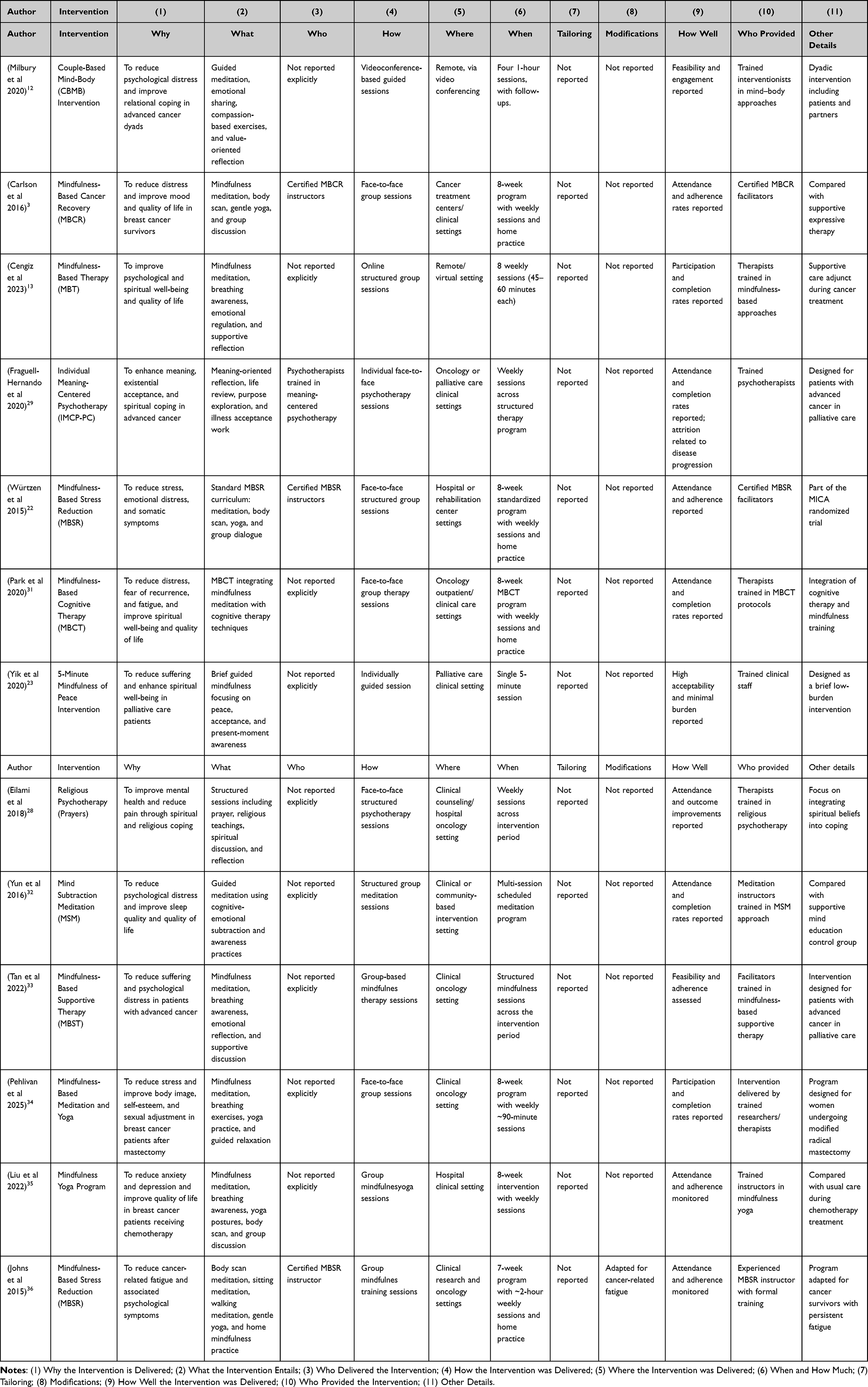 |
Table 2 Intervention Description and Replication (TIDieR) Checklist Evaluation |
Data analysis was conducted using a qualitative descriptive approach and narrative synthesis, summarizing and comparing study characteristics, intervention components, and reported outcomes. In addition, a thematic analysis was applied to identify recurring patterns and similarities across interventions. Through iterative coding and theme development, interventions were grouped into categories based on shared characteristics, such as similarity in core components, delivery method (eg, face-to-face vs technology-assisted), intervention intensity and duration, and the psychological–spiritual targets addressed. The themes generated from this analysis formed the basis for developing intervention categories with comparable features and for describing variations in approaches used to enhance psychological and spiritual well-being in patients receiving palliative and advanced cancer care.
Result
Study Selection
The study selection process is illustrated in Figure 1. A total of 369 records were identified through database searching, of which 114 duplicate records were removed. The remaining 255 records were screened based on titles and abstracts, of which 194 were excluded for not meeting the inclusion criteria. The full texts of the remaining 61 articles were assessed for eligibility. Of these, 48 studies were excluded due to reasons such as non-randomized study design, inappropriate population, or lack of relevant psychological or spiritual outcomes. Ultimately, 13 randomized controlled trials were included in the final synthesis.
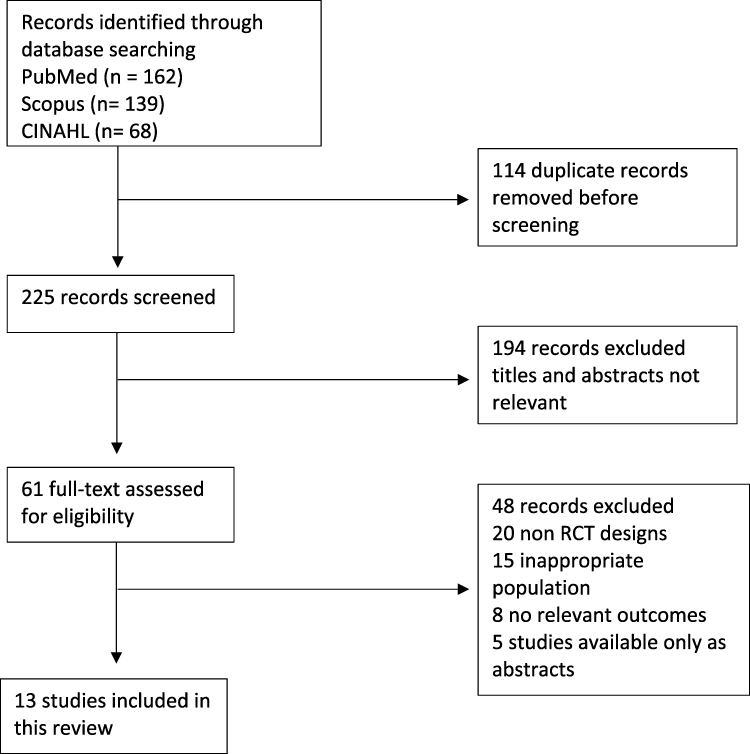 |
Figure 1 PRISMA Flowchart. |
Quality Appraisal Results
The methodological quality of the included studies was assessed using the JBI Critical Appraisal Checklist for RCT. The checklist consists of 13 items evaluating key methodological domains, including randomization procedures, allocation concealment, blinding, completeness of follow-up, and appropriateness of statistical analysis.
The quality appraisal was conducted independently by two reviewers (F.S. and M.K)., and any discrepancies were resolved through discussion and consensus. Overall, the included studies demonstrated generally acceptable methodological quality according to the JBI Critical Appraisal Checklist. All studies adequately reported appropriate randomization procedures, allocation concealment, baseline comparability, complete follow-up, intention-to-treat analysis, and the use of valid and reliable outcome measures (n = 13 for each domain). However, consistent limitations were observed in blinding procedures. None of the included studies reported blinding of participants or intervention providers (n = 13), which is likely due to the behavioral nature of mindfulness-based interventions. In addition, blinding of outcome assessors was unclear across all studies (n = 13). Despite these limitations, all studies met the majority of JBI criteria, indicating generally robust methodological quality.
In addition to the JBI appraisal, methodological characteristics related to trial registration, randomization procedures, and blinding were reviewed where reported. Several studies reported prospective registration in recognized clinical trial registries, although registration information was not consistently available across all trials. All included studies employed individual randomized controlled trial designs, and no cluster-randomized trials were identified. Reporting of outcome assessor blinding and data analyst blinding was limited across studies, restricting further evaluation of these domains. Detailed results of the quality appraisal are presented in Supplementary Table S2.
Characteristic of Studies
The characteristics of the included studies are summarized in Table 1. A total of 13 randomized controlled trials (RCTs) were included in this review. The included studies were conducted between 2015 and 2025 and represented a wide range of geographical settings, including the United States, Canada, Denmark, Spain, Turkey, Japan, South Korea, Malaysia, Iran, and China.3,12,13,22,23,28,29,31–33,35–37
The United States contributed several trials, particularly those evaluating mindfulness-based interventions such as Mindfulness-Based Stress Reduction (MBSR), Mindfulness-Based Cancer Recovery (MBCR), Couple-Based Meditation (CBM), and interventions targeting cancer-related fatigue.3,12,36 Studies conducted in Europe, including Denmark and Spain, examined structured mindfulness programs and meaning-centered psychotherapy in oncology and palliative care contexts.22,29 Several trials were conducted in Asian and Middle Eastern countries, including Turkey, Japan, South Korea, Malaysia, Iran, and China, reflecting increasing interest in culturally adapted mindfulness-based and spiritually integrated interventions in cancer care.13,23,28,31–35
Most studies employed parallel-group RCT designs, with sample sizes ranging from 32 to 336 participants. Interventions included both individual-based and dyadic approaches, particularly in studies involving patients with advanced cancer and their partners.12 The majority of trials were conducted in hospital-based or clinical oncology settings, including cancer treatment centers and palliative care services.3,22,29,35 In addition to traditional face-to-face programs, several studies employed technology-assisted or remotely delivered interventions, such as videoconferencing-based mindfulness programs and brief guided mindfulness sessions designed for patients with advanced illness or limited mobility.12,13,23 Overall, the included trials demonstrate substantial diversity in intervention models, delivery formats, and clinical contexts while sharing a common focus on enhancing psychological and spiritual well-being among individuals with cancer.
Characteristic of Participants
Across the 13 included RCTs, participant sample sizes ranged from 32 to 336 individuals, with several studies also including patient–caregiver dyads, particularly in trials involving patients with advanced cancer.3,12,13 Participants were predominantly adults diagnosed with cancer, with most studies enrolling individuals in middle adulthood to older age, reflecting the typical demographic profile of oncology and palliative care populations.3,22,31
The majority of included studies involved female participants, largely due to the high proportion of trials focusing on breast cancer patients and survivors.3,22,31,32,34,35 Several studies included women exclusively, particularly those examining survivorship or post-surgical populations. Other trials enrolled both male and female participants, particularly studies involving patients with advanced or metastatic cancer, such as metastatic non–small cell lung cancer or mixed advanced cancer populations.12,29,33
Regarding cancer diagnosis, breast cancer was the most frequently represented condition across the included studies.3,22,31,32,35 Other diagnoses included metastatic non–small cell lung cancer, mixed advanced cancer types, and patients receiving palliative care for life-limiting malignancies.12,23,29,33 Some studies focused specifically on patients with advanced or terminal disease, whereas others enrolled cancer survivors or patients undergoing active treatments such as chemotherapy or surgery.35–37
Participants were primarily recruited from oncology clinics, hospitals, rehabilitation programs, and palliative care services, with eligibility criteria commonly defined by cancer diagnosis, treatment status, and the ability to participate in mindfulness-based or spiritually oriented interventions.3,12,29,35 Overall, participant characteristics reflected a heterogeneous cancer population, encompassing individuals across the cancer trajectory, including patients undergoing treatment, survivors, and those receiving palliative or advanced cancer care.
Characteristic of Intervention
The included studies evaluated a diverse range of mindfulness-based and spiritually integrated interventions, which varied in their theoretical foundations, delivery format, duration, and intensity. Based on the intervention setting and delivery mode, the interventions were categorized into hospital-based and online or remotely delivered.
Category I: Hospital-Based Interventions
Hospital-based interventions were primarily delivered in oncology clinics, cancer centers, and palliative care services through face-to-face individual or group sessions.3,22,29,31,35,37 These interventions varied in duration and structure, ranging from brief single-session formats to structured multi-week programs lasting four to eight weeks.
The interventions included MBCR, MBSR, MBCT, Individual Meaning-Centered Psychotherapy for Palliative Care (IMCP-PC), Mind Subtraction Meditation (MSM), religious or prayer-based psychotherapy, mindfulness-based supportive therapy, and mindfulness yoga programs.3,22,28,29,32,33,35–37
Across studies, intervention sessions were typically conducted on a weekly basis, with session durations ranging from approximately 45 minutes to 2.5 hours, depending on the intervention model. Core intervention components commonly included guided mindfulness meditation, breathing exercises, body awareness practices, gentle yoga, reflective discussion, and psychoeducation aimed at enhancing emotional regulation and present-moment awareness. Several interventions also incorporated existential or meaning-oriented components, such as values clarification, reflection on life purpose, acceptance of illness, and exploration of spiritual beliefs.
In spiritually oriented programs, including religious psychotherapy and meaning-centered psychotherapy, intervention components emphasized spiritual reflection, meaning-making, existential coping, and faith-based support.28,29 Overall, hospital-based interventions were delivered by trained healthcare professionals, including psychologists, psychotherapists, mindfulness instructors, and spiritual care providers.
Category II: Online or Remotely Delivered Interventions
Online or remotely delivered interventions were implemented in several studies to improve accessibility and feasibility, particularly for patients with advanced cancer or high symptom burden.12,13,23 These interventions were delivered via videoconferencing platforms or brief guided mindfulness formats and varied in duration, frequency, and therapeutic focus across studies.
For example, Couple-Based Meditation (CBM) was delivered through videoconferencing in four weekly sessions of approximately 60 minutes, integrating guided mindfulness meditation, structured emotional sharing between patients and their partners, compassion-based practices, and values-oriented reflection to support psychological and relational coping.12
Similarly, online Mindfulness-Based Therapy involved eight weekly virtual sessions lasting approximately 45–60 minutes, focusing on mindfulness meditation, emotional regulation, and values clarification to enhance psychological and spiritual well-being.13 In palliative care settings, a brief mindfulness-of-peace intervention was delivered as a single five-minute guided session, designed to accommodate patients with advanced illness while addressing spiritual distress and subjective suffering.23
Across studies, remotely delivered interventions were facilitated by trained healthcare professionals or mindfulness instructors and were often adapted to patients’ physical condition and treatment burden. Overall, these interventions demonstrated good feasibility and acceptability, particularly for individuals with limited mobility or advanced disease, while preserving the core components of mindfulness practice and spiritual reflection.
Characteristic of Outcomes
Across the included randomized controlled trials, a wide range of psychological, spiritual, and implementation-related outcomes were assessed. In addition to clinical outcomes, several studies also reported feasibility-related indicators, including attrition rates, treatment engagement, and intervention acceptability. Because some studies reported mixed or non-significant findings, outcomes that did not reach statistical significance were also summarized to provide a balanced interpretation of the evidence. Based on this synthesis, the reported outcomes were categorized into five domains: (I) Psychological Well-Being, (II) Spiritual Well-Being, (III) Attrition and Treatment Engagement, (IV) Acceptability, and (V) Mixed or Inconsistent Findings. All outcome measures were assessed using validated instruments that have been previously applied and validated in cancer and/or palliative care populations.
Outcome I: Psychological Well-Being
Psychological well-being was the most frequently reported outcome domain, assessed in the majority of included studies using validated self-report instruments. Commonly evaluated outcomes included anxiety, depression, psychological distress, mood disturbance, fatigue, demoralization, and quality of life. Measurement tools frequently used across studies included the Hospital Anxiety and Depression Scale (HADS), Profile of Mood States (POMS), Symptom Checklist-90 (SCL-90R), Functional Assessment of Cancer Therapy (FACT), and other validated psychological assessment instruments.3,22,31,32,35
Eleven of the 13 included studies reported statistically significant improvements in at least one psychological outcome among participants receiving mindfulness-based or spiritually integrated interventions compared with control conditions. Improvements were observed across depression, anxiety, psychological distress, stress, mood disturbance, and quality of life.3,12,22,28,29,31–33,35–37 Improvements were observed across diverse patient populations, including breast cancer survivors, individuals undergoing chemotherapy or surgery, patients with advanced or metastatic disease, and those receiving palliative care.12,23,29,33
Outcome II: Spiritual Well-Being
Spiritual well-being was assessed in several included studies using validated instruments, most commonly the Functional Assessment of Chronic Illness Therapy–Spiritual Well-Being (FACIT-Sp) scale. This instrument evaluates dimensions such as meaning, peace, faith, and existential well-being.3,13,31
Six of the 13 included studies reported statistically significant improvements in spiritual well-being, particularly among interventions that incorporated explicit spiritual, religious, existential, or meaning-centered components.3,13,23,29,31,32 Spiritual benefits were reported among breast cancer survivors, patients with advanced cancer, and individuals receiving palliative care, depending on the intervention model and study context.
Outcome III: Attrition and Treatment Engagement
Attrition and treatment engagement were reported in several included studies and were particularly relevant among participants with advanced cancer and those receiving palliative care, where disease progression, symptom burden, and treatment demands could affect intervention completion and adherence. Participant withdrawal was most frequently associated with deterioration in health status, particularly among individuals with advanced cancer or those receiving palliative care.3,12,13
Additional factors contributing to attrition included logistical barriers, such as transportation difficulties, scheduling conflicts, and physical fatigue related to ongoing cancer treatment.22,29 Several studies also noted that longer-duration interventions, particularly those lasting eight weeks or more, were associated with slightly higher dropout rates. Despite these challenges, participants who completed the interventions generally demonstrated high levels of session attendance and treatment engagement.
Outcome IV: Acceptability
Intervention acceptability was reported in several included studies and was generally high across both face-to-face and remotely delivered intervention formats. Participants commonly perceived the interventions as manageable, meaningful, and relevant to their psychosocial and spiritual needs. For example, Couple-Based Meditation (CBM) demonstrated strong acceptability among patients with advanced cancer and their partners when delivered via videoconferencing.12 Similarly, Mindfulness-Based Cancer Recovery (MBCR) programs reported high participation rates and sustained engagement among cancer survivors.3
In palliative care settings, brief mindfulness-based interventions were also reported to be acceptable and feasible, with minimal burden on participants despite advanced illness.23 Overall, both hospital-based and remotely delivered interventions were perceived as manageable and meaningful by participants, suggesting that mindfulness-based spiritual interventions can be integrated into oncology and palliative care services.
Outcome V: Mixed or Inconsistent Findings
Although the majority of included studies reported beneficial effects, several trials demonstrated mixed or inconsistent findings across specific outcome domains, particularly spiritual well-being, quality of life, fatigue, and selected psychological subdomains. For example, Würtzen et al (2015) reported no statistically significant improvement in spiritual well-being among breast cancer survivors participating in Mindfulness-Based Stress Reduction, despite reductions in psychological distress.22
Similarly, Fraguell-Hernando et al (2020) reported non-significant changes in some psychological and spiritual subdomains, while other outcomes showed improvement. These mixed findings highlight the heterogeneity of intervention protocols, outcome measures, and participant characteristics, which may influence the magnitude and consistency of observed intervention effects.29
Discussion
This systematic review synthesized evidence from 13 RCTs examining the effectiveness of mindfulness-based and spiritually integrated interventions in improving psychological and spiritual well-being among patients with cancer. Across the included studies, interventions were broadly categorized into two main delivery formats: hospital-based face-to-face interventions and online or remotely delivered interventions.3,12,13,22,23,31,32
Across these intervention types, outcomes were consistently reported in five domains: anxiety, depression, psychological distress, quality of life, and spiritual well-being. Improvements in psychological outcomes were the most consistently observed findings. Several studies reported significant reductions in anxiety and depression following mindfulness-based interventions.3,22,31–33,35 Reductions in overall psychological distress were also documented across multiple trials.12,13,23 These findings suggest that both face-to-face and remotely delivered interventions are effective in addressing emotional burden in cancer populations.
Quality of life was frequently assessed, with several studies reporting improvements following intervention.3,12,33 However, the findings in this domain were less consistent compared to psychological outcomes, with some studies reporting modest or non-significant changes. This variability may be attributed to differences in intervention duration, disease stage, and measurement instruments used across studies.
Enhancements in spiritual well-being were primarily observed in studies that incorporated explicit spiritual or meaning-centered components. Interventions integrating religious or meaning-focused approaches demonstrated improvements in spiritual outcomes and existential coping.32 These findings suggest that the inclusion of spiritual elements plays an important role in addressing existential distress among patients with advanced cancer.
The qualifications of intervention facilitators varied across the included studies. While several studies reported training or certification in mindfulness-based interventions, psychology, nursing, or oncology care, formal qualifications in theology, divinity, or related religious disciplines were rarely reported. In addition, facilitator qualifications and levels of experience were not consistently described across studies. Consequently, it was not possible to determine whether differences in instructor qualifications contributed to variations in intervention outcomes.
Despite generally positive findings, not all studies demonstrated statistically significant effects across all outcome domains. Some trials reported mixed or non-significant results, particularly on spiritual well-being and quality-of-life outcomes.22,29 These inconsistencies may reflect variations in intervention intensity, delivery format, sample characteristics, and outcome measurement approaches.
Overall, the findings suggest that mindfulness-based and spiritually integrated interventions are promising approaches for improving psychological and spiritual well-being in cancer populations. However, the heterogeneity observed across studies highlights the need for more standardized intervention protocols, clearer reporting of intervention components, and the use of consistent outcome measures in future research.
The findings of the present review are broadly consistent with previous systematic reviews and meta-analyses evaluating mindfulness-based and psychosocial interventions in cancer populations. The study reported that mindfulness-based interventions were associated with improvements in psychological well-being, coping, mindfulness, and quality of life among patients with cancer and cancer survivors.25 Similarly, another study found that psychological interventions produced beneficial effects on cancer-related emotional distress and fear of cancer recurrence, although the magnitude of benefit varied across intervention characteristics and follow-up periods.5 The present review extends this evidence by specifically focusing on randomized controlled trials that incorporated spiritual or meaning-centered components and by examining both psychological and spiritual outcomes among patients with advanced cancer receiving palliative care. These findings suggest that integrating spiritual dimensions within mindfulness-based interventions may offer additional benefits for addressing the complex psychological and existential needs of this patient population.
Variability in Intervention Protocols and Delivery Methods
Across the 13 included RCTs, mindfulness-based and spiritually integrated interventions demonstrated substantial variability in structure, delivery format, and therapeutic components. Hospital-based interventions were most commonly implemented in oncology clinics or palliative care settings and frequently involved structured programs such as Mindfulness-Based Cancer Recovery (MBCR), Mindfulness-Based Stress Reduction (MBSR), and mindfulness-based cognitive or meaning-centered approaches.3,22,29,31 These interventions typically included core components such as guided mindfulness meditation, breathing awareness, body scan exercises, emotional regulation strategies, and reflective or meaning-centered discussions.
Remotely delivered interventions, reported in several studies, included videoconference-based sessions, online mindfulness therapy, and brief guided practices designed to improve accessibility for patients with advanced disease or mobility limitations.12,13,23 Across both delivery formats, the most consistently reported components were guided meditation and breathing awareness exercises, which appeared in the majority of studies. Interventions were most commonly delivered by trained healthcare professionals, including psychologists, psychotherapists, mindfulness instructors, and, in some cases, spiritual care providers or multidisciplinary teams. Facilitator backgrounds also varied across studies, ranging from certified mindfulness instructors and psychotherapists to healthcare professionals and spiritual care providers, which may have contributed to differences in intervention implementation and outcomes.
Challenges in Implementing Mindfulness-Based Spiritual Interventions
Despite the promising benefits reported across studies, several challenges may affect the implementation of mindfulness-based spiritual interventions in oncology and palliative care settings. Patients with advanced cancer often experience high symptom burden, treatment fatigue, and disease progression, which may limit consistent participation in structured programs.3,12 Practical barriers such as scheduling conflicts, transportation difficulties, and competing medical appointments may also reduce attendance in hospital-based interventions.22,36
For remotely delivered interventions, additional challenges may include technological barriers and varying levels of digital literacy, particularly among older adults.13,23 These factors highlight the importance of developing flexible and patient-centered intervention designs that can accommodate the physical and logistical challenges experienced by patients living with advanced cancer.29,31
Feasibility and Acceptability of Interventions
Despite these challenges, the included studies generally reported good feasibility and acceptability of mindfulness-based spiritual interventions among cancer patients. High levels of treatment engagement were observed in both hospital-based and remotely delivered programs, suggesting that these interventions can be successfully integrated into oncology and palliative care settings. Remote delivery formats, in particular, may enhance accessibility for patients who experience physical or logistical barriers to attending in-person sessions.12 Overall, the findings suggest that flexible delivery approaches and tailored intervention designs may improve participation and reduce attrition in this patient population.
Strengths and Limitations
This review has several notable strengths. First, only randomized controlled trials (RCTs) were included, providing a relatively high level of evidence and strengthening the internal validity of the findings. Second, the inclusion of studies conducted across diverse geographical and cultural settings enhances the relevance and potential generalizability of the results to different oncology and palliative care populations.
However, several limitations should be noted. First, substantial variability in intervention protocols, including differences in duration, format, and content, limits direct comparability across studies. Second, many studies had relatively small sample sizes or were conducted in single-center settings. In addition, volunteer bias may have occurred, as participants willing to engage in mindfulness-based spiritual interventions may have been more motivated or receptive to these approaches than the broader population of patients with advanced cancer. Third, participant attrition related to disease progression, fatigue, treatment burden, and logistical barriers may have affected intervention adherence. Another limitation is that important clinical outcomes, including mortality, pain, nausea, and medication use, were infrequently reported across the included studies. As a result, the potential impact of mindfulness-based spiritual interventions on these clinically relevant outcomes could not be comprehensively assessed within this review.
At the review level, several methodological limitations should also be considered. Although PubMed, Scopus, and CINAHL provide broad coverage of oncology, nursing, and health sciences literature, additional databases such as Embase, PsycINFO, and the Cochrane Library were not searched, and relevant studies may therefore have been missed. The review was also restricted to English-language publications, which may have introduced language bias. Furthermore, conference abstracts, dissertations, theses, and other forms of grey literature were excluded because they generally provide insufficient methodological detail and incomplete outcome data for rigorous critical appraisal and evidence synthesis. Finally, the integration of spiritual components across different cultural and religious contexts may influence intervention acceptability and effectiveness, potentially limiting the transferability of findings across diverse populations.
Future research should prioritize larger multi-center trials, standardized intervention protocols, consistent outcome measurement, and comprehensive reporting of clinically relevant outcomes to strengthen the evidence base for mindfulness-based spiritual interventions in cancer care.
Conclusion
This systematic review synthesizes evidence from 13 RCTs suggesting that mindfulness-based and spiritually integrated interventions may improve psychological and spiritual outcomes among patients with cancer across multiple domains. Overall, 11 of the 13 included studies reported improvements in at least one psychological outcome, while 6 studies reported significant improvements in spiritual well-being, particularly in domains such as meaning, peace, and existential acceptance. However, several trials also reported mixed or non-significant findings in specific outcome domains, reflecting variability in intervention protocols, delivery formats, outcome measures, and patient clinical characteristics.
The available evidence suggests that both hospital-based and remotely delivered interventions are generally feasible and acceptable to patients, although attrition may occur due to disease burden and treatment-related fatigue. Taken together, these findings indicate that mindfulness-based and spiritually integrated interventions have potential as complementary approaches for addressing the multidimensional needs of patients with cancer. Nevertheless, the observed heterogeneity across studies and the presence of mixed findings warrant cautious interpretation of the evidence. Future research should focus on standardizing intervention protocols, identifying mechanisms of action, and evaluating long-term outcomes across diverse cancer populations. The findings may inform nurses and palliative care professionals seeking to incorporate mindfulness-based spiritual care strategies into supportive care for patients with advanced cancer.
Abbreviations
RCT, Randomized Controlled Trial; MBCR, Mindfulness-Based Cancer Recovery; MBSR, Mindfulness-Based Stress Reduction; MBCT, Mindfulness-Based Cognitive Therapy; MBT, Mindfulness-Based Therapy; MBST, Mindfulness-Based Supportive Therapy; CBM, Couple-Based Meditation; IMCP-PC, Individual Meaning-Centered Psychotherapy for Palliative Care; SET, Supportive-Expressive Therapy; MSM, Mind Subtraction Meditation; SME, Self-Management Education; QOL, Quality of Life; PTG, Post-Traumatic Growth; HADS, Hospital Anxiety and Depression Scale; FACIT-Sp, Functional Assessment of Chronic Illness Therapy–Spiritual Well-being; FACIT-G, Functional Assessment of Cancer Therapy–General; FACT-G, Functional Assessment of Cancer Therapy–General; FFMQ, Five Facet Mindfulness Questionnaire; SCL-90-R, Symptom Checklist-90-Revised; BCPT, Breast Cancer Prevention Trial Symptom Scale; BFI, Brief Fatigue Inventory; FCR, Fear of Cancer Recurrence; CARS, Concerns About Recurrence Scale; GHQ-28, General Health Questionnaire-28; RPFS-CV, Revised Piper Fatigue Scale–Chinese Version; BPI-C, Brief Pain Inventory–Chinese Version; NR, Not Reported.
Acknowledgments
The authors would like to thank Universitas Padjadjaran for facilitating the database and funding for this research.
Funding
The Research and Community Engagement Director at Universitas Padjadjaran, Bandung, Indonesia, funded the Article Processing Charge (APC) and a grant to publish a research article.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clin. 2021;71(3):209–19. doi:10.3322/caac.21660
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
3. Carlson LE, Tamagawa R, Stephen J, Drysdale E, Zhong L, Speca M. Randomized-controlled trial of mindfulness-based cancer recovery versus supportive expressive group therapy among distressed breast cancer survivors (MINDSET): long-term follow-up results. Psycho-Oncol. 2016;25(7):750–759. doi:10.1002/pon.4150
4. Vos J, Vitali D. The effects of psychological meaning-centered therapies on quality of life and psychological stress: a metaanalysis. Pall Supp Care. 2018;16(5):608–632. doi:10.1017/S1478951517000931
5. Tauber NM, O’Toole MS, Dinkel A, et al. Effect of psychological intervention on fear of cancer recurrence: a systematic review and meta-analysis. JCO. 2019;37(31):2899–2915. doi:10.1200/JCO.19.00572
6. Smith SK, MacDermott K, Amarasekara S, Pan W, Mayer D, Hockenberry M. Reimagine: a randomized controlled trial of an online, symptom self-management curriculum among breast cancer survivors. Support Care Cancer. 2019;27(5):1775–1781. doi:10.1007/s00520-018-4431-7
7. Osmani V, Hörner L, Klug SJ, Tanaka LF. Prevalence and risk of psychological distress, anxiety and depression in adolescent and young adult (
8. Ostovar S, Modarresi Chahardehi A, Mohd Hashim IH, Othman A, Kruk J, Griffiths MD. Prevalence of psychological distress among cancer patients in Southeast Asian countries: a systematic review. European J Cancer Care. 2022;31(6):e13669. doi:10.1111/ecc.13669
9. Pérez-Cruz PE, Langer P, Carrasco C, et al. Spiritual pain is associated with decreased quality of life in advanced cancer patients in palliative care: an exploratory study. J Palliative Med. 2019;22(6):663–669. doi:10.1089/jpm.2018.0340
10. Soto-Rubio A, Perez-Marin M, Rudilla D, et al. Responding to the spiritual needs of palliative care patients: a randomized controlled trial to test the effectiveness of the kibo therapeutic interview. Front Psychol. 2020;11:1979. doi:10.3389/fpsyg.2020.01979
11. Almeida M, Ramos C, Maciel L, Basto-Pereira M, Leal I. Meaning in life, meaning-making and posttraumatic growth in cancer patients: systematic review and meta-analysis. Front Psychol. 2022;13:995981. doi:10.3389/fpsyg.2022.995981
12. Milbury K, Weathers SP, Durrani S, et al. Online couple-based meditation intervention for patients with primary or metastatic brain tumors and their partners: results of a pilot randomized controlled trial. J Pain Sympt Manag. 2020;59(6):1260–1267. doi:10.1016/j.jpainsymman.2020.02.004
13. Oner Cengiz H, Bayir B, Sayar S, Demirtas M. Effect of mindfulness-based therapy on spiritual well-being in breast cancer patients: a randomized controlled study. Support Care Cancer. 2023;31(7):438. doi:10.1007/s00520-023-07904-2
14. Cherny NI, Paluch-Shimon S, Berner-Wygoda Y. Palliative care: needs of advanced breast cancer patients. Breast Cancer. 2018;10:231–243. doi:10.2147/BCTT.S160462
15. Vanbutsele G, Van Belle S, Surmont V, et al. The effect of early and systematic integration of palliative care in oncology on quality of life and health care use near the end of life: a randomised controlled trial. Eur J Cancer. 2020;124:186–193. doi:10.1016/j.ejca.2019.11.009
16. Maindet C, Burnod A, Minello C, George B, Allano G, Lemaire A. Strategies of complementary and integrative therapies in cancer-related pain—attaining exhaustive cancer pain management. Support Care Cancer. 2019;27(8):3119–3132. doi:10.1007/s00520-019-04829-7
17. Caruso R, Nanni MG, Rodin G, et al. Effectiveness of a brief manualized intervention, managing cancer and living meaningfully (CALM), adapted to the Italian cancer care setting: study protocol for a single-blinded randomized controlled trial. Contemporary Clin Trials Commun. 2020;20:100661. doi:10.1016/j.conctc.2020.100661
18. Sun Y, Wu J, Tian H, et al. Global research trends in palliative care for breast cancer from 2012 to 2022: a scientometric analysis. Front Oncol. 2023;13:1104531. doi:10.3389/fonc.2023.1104531
19. Park S, Sado M, Fujisawa D, et al. Mindfulness-based cognitive therapy for Japanese breast cancer patients-a feasibility study. Japanese Journal of Clinical Oncology. 2018;48(January):68–74. doi:10.1093/jjco/hyx156
20. Keng SL, Tong EMW. Riding the tide of emotions with mindfulness: mindfulness, affect dynamics, and the mediating role of coping. Emotion. 2016;16(5):706–718. doi:10.1037/emo0000165
21. Evans S, Fernandez S, Olive L, Payne LA, Mikocka-Walus A. Psychological and mind-body interventions for endometriosis: a systematic review. J Psychosomatic Res. 2019;124:109756. doi:10.1016/j.jpsychores.2019.109756
22. Rtzen HWÜ, Dalton SO, Christensen J, et al. Effect of mindfulness-based stress reduction on somatic symptoms, distress, mindfulness and spiritual wellbeing in women with breast cancer: results of a randomized controlled trial. Acta Oncologica. 2015;54(5):712–719. doi:10.3109/0284186X.2014.997371
23. Yik LL, Ling LM, Ai LM, et al. The effect of 5-minute mindfulness of peace on suffering and spiritual well-being among palliative care patients: a randomized controlled study. Am J Hosp Palliat Med. 2021;38(9):1083–1090. doi:10.1177/1049909120965944
24. Cho D, Kim S, Durrani S, Liao Z, Milbury K. Associations between spirituality, mindfulness, and psychological symptoms among advanced lung cancer patients and their spousal caregivers. J Pain Sympt Manag. 2021;61(5):898–908.e1. doi:10.1016/j.jpainsymman.2020.10.001
25. Badaghi N, Buskbjerg C, Kwakkenbos L, Bosman S, Zachariae R, Speckens A. Positive health outcomes of mindfulness-based interventions for cancer patients and survivors: a systematic review and meta-analysis. Clinic Psychol Rev. 2024;114:102505. doi:10.1016/j.cpr.2024.102505
26. Matiz A, Fabbro F, Paschetto A, Cantone D, Paolone AR, Crescentini C. Positive impact of mindfulness meditation on mental health of female teachers during the COVID-19 outbreak in Italy. Int J Environ Res Public Health. 2020;17(18):6450. doi:10.3390/ijerph17186450
27. Dehghannezhad J, Zamanzadeh V, Gilani N, Rahmani A, Dadashzadeh A. Compassion satisfaction and compassion fatigue among emergency medical technicians in Iran. Australasian J Paramed. 2020;17:1–7. doi:10.33151/ajp.17.642
28. Eilami O, Moslemirad M, Naimi E, Babuei A, Rezaei K. The effect of religious psychotherapy emphasizing the importance of prayers on mental health and pain in cancer patients. J Religion Health. 2019;58(2):444–451. doi:10.1007/s10943-018-0696-x
29. Fraguell-Hernando C, Limonero JT, Gil F. Psychological intervention in patients with advanced cancer at home through individual meaning-centered psychotherapy-palliative care: a pilot study. Support Care Cancer. 2020;28(10):4803–4811. doi:10.1007/s00520-020-05322-2
30. Lengacher CA, Reich RR, Paterson CL, et al. Examination of broad symptom improvement resulting from mindfulness-based stress reduction in breast cancer survivors: a randomized controlled trial. J Clin Oncol. 2016;34(24):2827–2834. doi:10.1200/JCO.2015.65.7874
31. Park S, Sato Y, Takita Y, et al. Mindfulness-based cognitive therapy for psychological distress, fear of cancer recurrence, fatigue, spiritual well-being, and quality of life in patients with breast cancer—a randomized controlled trial. J Pain Sympt Manag. 2020;60(2):381–389. doi:10.1016/j.jpainsymman.2020.02.017
32. Yun MR, Song M, Jung KH, Yu BJ, Lee KJ. The effects of mind subtraction meditation on breast cancer survivors’ psychological and spiritual well-being and sleep quality: a randomized controlled trial in South Korea. Cancer Nurs. 2017;40(5):377–385. doi:10.1097/NCC.0000000000000443
33. Tan SB, Chee CH, Ngai CF, et al. Mindfulness-based supportive therapy on reducing suffering in patients with advanced cancer: randomised controlled trial. BMJ Support Palliat Care. 2023;13(e3):e1117–25. doi:10.1136/bmjspcare-2021-003349
34. Pehlivan M, Eyi S. The impact of mindfulness-based meditation and yoga on stress, body image, self-esteem, and sexual adjustment in breast cancer patients undergoing modified radical mastectomy: a randomized controlled trial. Cancer Nurs. 2025;48(3):190–199. doi:10.1097/NCC.0000000000001427
35. Liu W, Liu J, Ma L, Chen J. Effect of mindfulness yoga on anxiety and depression in early breast cancer patients received adjuvant chemotherapy: a randomized clinical trial. J Cancer Res Clin Oncol. 2022;148(9):2549–2560. doi:10.1007/s00432-022-04167-y
36. Johns SA, Brown LF, Beck‐Coon K, Monahan PO, Tong Y, Kroenke K. Randomized controlled pilot study of mindfulness‐based stress reduction for persistently fatigued cancer survivors. Psycho-Oncol. 2015;24(8):885–893. doi:10.1002/pon.3648
37. Saribudak TP, Semerci R, Çalişkan BB, Yildiz G, Altinel N, Kapanci M. The effect of a mindfulness-based stress reduction program on professional quality of life and perceived stress level of the pediatric oncology-hematology nurses: quasi-experimental study. Turkiye Klinikleri J Nurs Sci. 2025;17(3):880–888. doi:10.5336/nurses.2024-106063
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.