Back to Journals » Journal of Pain Research » Volume 14
Mind-Body Activity Program for Chronic Pain: Exploring Mechanisms of Improvement in Patient-Reported, Performance-Based and Ambulatory Physical Function
Authors Greenberg J ![]() , Mace RA
, Mace RA ![]() , Bannon SM, Kulich RJ
, Bannon SM, Kulich RJ ![]() , Vranceanu AM
, Vranceanu AM ![]()
Received 24 December 2020
Accepted for publication 20 January 2021
Published 5 February 2021 Volume 2021:14 Pages 359—368
DOI https://doi.org/10.2147/JPR.S298212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Michael Schatman
Jonathan Greenberg,1,2 Ryan A Mace,1,2 Sarah M Bannon,1,2 Ronald J Kulich,2,3 Ana-Maria Vranceanu2
1Integrated Brain Health Clinical and Research Program, Department of Psychiatry, Massachusetts General Hospital, Boston, MA, USA; 2Harvard Medical School, Boston, MA, USA; 3Center for Pain Medicine, Massachusetts General Hospital, Boston, MA, USA
Correspondence: Ana-Maria Vranceanu
Integrated Brain Health Clinical and Research Program, Department of Psychiatry, Massachusetts General Hospital/Harvard Medical School, One Bowdoin Square, 1st Floor, Suite 100, Boston, MA, 02114, USA
Tel +1 617 724 4977
Email [email protected]
Background: Improving physical function among patients with chronic pain is critical for reducing disability and healthcare costs. However, mechanisms underlying improvement in patient-reported, performance-based, and ambulatory physical function in chronic pain remain poorly understood.
Purpose: To explore psychosocial mediators of improvement in patient-reported, performance-based, and objective/accelerometer-measured physical function among participants in a mind-body activity program.
Methods: Individuals with chronic pain were randomized to one of two identical 10-week mind-body activity interventions aimed at improving physical function with (GetActive-Fitbit; N=41) or without (GetActive; N=41) a Fitbit device. They completed self-reported (WHODAS 2.0), performance-based (6-minute walk test), and objective (accelerometer-measured step-count) measures of physical function, as well as measures of kinesiophobia (Tampa Kinesiophobia Scale), mindfulness (CAMS-R), and pain resilience (Pain Resilience Scale) before and after the intervention. We conducted secondary data analyses to test mediation via mixed-effects modeline.
Results: Improvements in patient-reported physical function were fully and uniquely mediated by kinesiophobia (Completely Standardized Indirect Effect (CSIE)=.18; CI=0.08, 0.30; medium-large effect size), mindfulness (CSIE=− .14; CI=− 25, − .05; medium effect size) and pain resilience (CSIE=− .07; CI=− .16, − .005; small-medium effect size). Improvements in performance-based physical function were mediated only by kinesiophobia (CSIE=− .11; CI=− 23, − .008; medium effect size). No measures mediated improvements in objective (accelerometer measured) physical function.
Conclusion: Interventions aiming to improve patient-reported physical function in patients with chronic pain may benefit from skills that target kinesiophobia, mindfulness, and pain resilience, while those focused on improving performance-based physical function should target primarily kinesiophobia. More research is needed to understand mechanisms of improvement in objective, accelerometer-measured physical function.
Trial Registration: ClinicalTrials.gov NCT03412916.
Keywords: chronic pain, disability, mind-body, physical function, mediation, psychosocial variables
Introduction
Improving physical function among patients with chronic musculoskeletal pain is key to reducing disability and healthcare costs.1,2 Non-pharmacological interventions for chronic pain can help improve physical function among patients with chronic pain.3,4 While identifying mechanisms contributing to improvement in physical function is a high priority for the treatment of this patient population, such mechanisms currently remain poorly understood.
Much of what is currently known about increasing physical function among patients with chronic pain is limited to patient-reported measures.1,5 While patient-reported measures provide important information about patients’ experiences and perceptions, relying solely on such measures neglects additional important facets of function, such as an individual’s functional capacity (eg, performance during a time-limited standard test) and ambulatory activity (eg, daily step-count measured across a specified time period with accelerometers).6 A comprehensive, multidimensional assessment of physical function in chronic pain trials is consistent with guidelines from the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT)7 and the International Classification of Functioning, Disability and Health (ICF).8 However, to date, no prior intervention studies to our knowledge have complied.
In a recent randomized controlled trial (RCT) of patients with heterogeneous chronic pain, we have shown that participation in two identical mind-body activity programs without (GetActive) or with a Fitbit (GetActive-Fitbit) was associated with statistically and clinically significant improvements in patient-reported and performance-based physical function,9,10 with effect sizes that are similar or greater to those reported following other multidisciplinary and mind-body programs for chronic pain.1,11 Changes in accelerometer-measured step-count were not significant. Here, we conducted secondary data analyses with mixed-effects modeling to explore mechanisms of change in each of the three aspects of physical function. Identification of such process variables is important, as it can inform which constructs to target in order to maximize improvement in physical function. We specifically focus on three psychosocial variables that are theoretically and empirically relevant to physical function: kinesiophobia, which refers to fear of pain due to movement and is highly prevalent among patients with chronic pain;12 mindfulness, which refers to the ability paying attention, on purpose, in the present moment and in a non-judgmental manner and can increase tolerance of physical discomfort;13 and pain resilience, which pertains to the ability to restore and sustain living a fulfilling life in the presence of pain.14 While evidence linking these psychosocial variables to increased patient-reported physical function has been mostly consistent,12,15–17 evidence linking them to performance and accelerometer-based physical function is sparse and weak.1,18,19 Further, we have recently demonstrated that psychosocial variables, including kinesiophobia, mindfulness, and pain-resilience, correlate with patient-reported, but not performance or accelerometer-based physical function among patients with chronic pain.20 However, given that no intervention studies of chronic pain have included all three types of physical function measures, little is known about their unique contribution and specific role in increasing physical function among these patients, and whether this role differs between various types of physical function measurement.
Our primary hypothesis was that changes in kinesiophobia, mindfulness, and pain resilience would have a unique and significant mediating effect in patient-reported physical function improvements from baseline to post-intervention. We also explored whether kinesiophobia, mindfulness, and pain resilience mediate improvements in performance and accelerometer-based physical function.
Materials and Methods
Participants
We recruited participants (N=82) with heterogeneous musculoskeletal chronic pain via direct referrals from the Massachusetts General Hospital Pain Clinic and hospital-wide email lists between July 2018 and September 2019. We targeted heterogeneous pain due to the prevalence of multisite pain in patients from these recruitment sources (>60%),20 in order for the interventions to be easily implementable once efficacy is established and since our theoretical framework supports improvement in outcomes regardless of the type or location of pain. Table 1 summarizes sample characteristics.
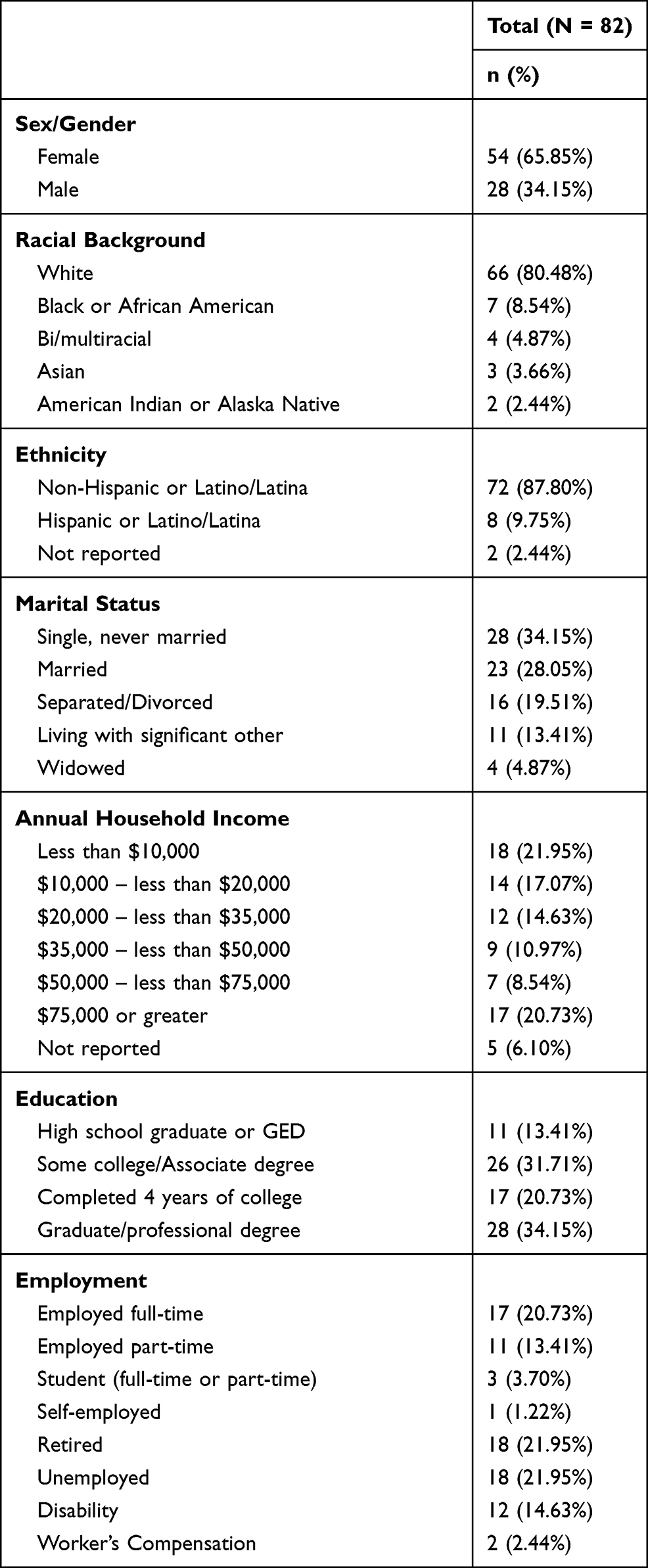 |
Table 1 Participant Socio-Demographics Variables |
The sample consisted of participants who were predominantly white (80%), non-Hispanic (88%), female (66%), and college-educated (55%). To be included in the study, participants had to: (1) be at least 18 years old; (2) report nonmalignant chronic pain lasting over three months; (3) be capable of walking for at least 6 minutes; (4) have access to a Bluetooth-capable device version 4.0; (5) if on psychotropic or pain medications, remaining on a stable dose for past 3 months; and (6) be cleared for participation by a physician. Exclusion criteria were (1) having a medical illness that is expected to worsen in the following six months; (2) having a serious untreated psychiatric condition, including active suicidality; (3) currently having a substance abuse disorder that is untreated; (4) having practiced relaxation or meditation-based skills in the past six months for more than 45 min/week; (5) having used a Fitbit device in past six months; and (6) engaging in physical exercise on a regular basis for over 30 min/day. Further details about this sample are available in our prior work.9
Procedure
Participants were randomized using a 1:1 ratio to one of two 10-week mind-body physical activity intervention programs, GetActive or GetActive-Fitbit. The programs were identical with the exception that the GetActive-Fitbit group additionally received a Fitbit digital monitoring device. Information on program development and descriptions of program sessions is provided in our prior work.9,10 Participants completed baseline assessments and started their first 90-minute group session the following week. Participants completed a post-intervention assessment one week after the last group session. Baseline and post-intervention assessment measures were identical, and participants were compensated $30 for each assessment. The study was approved by the Massachusetts General Hospital Institutional Review Board and all procedures were conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent prior to participation.
Intervention Conditions
The structure and content of the GetActive and GetActive-Fitbit programs is detailed elsewhere.9 Briefly, both conditions had 10 weekly group sessions (90 minutes each) administered by a clinical psychologist with expertise in mind-body interventions for chronic pain. The programs taught mind-body skills (eg, mindfulness, deep breathing) to reduce stress and promote acceptance, cognitive behavioral skills that are pain-specific (eg, cognitive restructuring of negative reactions to pain, behavioral activation, goal setting), and physical restoration skills (eg, pacing activity based on a given quota derived from participants’ individual activity levels rather than on pain levels). Both programs also included education on the “disability spiral” (eg, how low levels of activity perpetuate pain and disability), debunking common myths about chronic pain and involuntary pain-related thoughts.
Measures
Physical Function
Consistent with IMMPACT criteria7,21 and International Classification of Functioning, Disability and Health (ICF) guidelines,8 we assessed physical function comprehensively, including patient-reported, performance-based, and objective/accelerometry-based measures. We assessed patient-reported physical function using the World Health Organization Disability Assessment Schedule (WHODAS 2.0),22 a 36-item questionnaire assessing difficulties in six main areas of function. Internal reliability was excellent for the WHODAS 2.0 (Chronbach’s α=0.97). We used participants’ walking distances on standardized flat track during a 6-minute walk test (6MWT),23 as a measure of performance-based physical function. Finally, we used average daily step-counts calculated via a wGT3X-BT ActiGraph accelerometer device worn for one week at baseline and post-intervention, as a measure of objective physical function.24
Proposed Mediators
We selected kinesiophobia, pain resilience, and mindfulness as mediators in our model. The Tampa Kinesiophobia Scale (TSK)12 is a measure of fear of pain due to movement. Internal reliability was good for the TSK (α=0.87). The Pain Resilience Scale (PRS)25 is a measure of one’s ability to regulate emotions and engage in activities in spite of pain. Internal reliability was good for the PRS (α=0.89). The Cognitive and Affective Mindfulness Scale-Revised (CAMS-R)26 is a measure of one’s ability to pay attention to the present moment in a nonjudgmental way. Internal reliability was good for the CAMS-R (α=0.85).
While our RCT9 also found improvements in measures such as pain catastrophizing (pain catastrophizing scale)27 and adaptive coping (measure of current status)28 that have theoretical support as potential mediators, we did not include them in the models due to statistical and conceptual overlap with other mediators. Kinesiophobia and pain catastrophizing (r=0.67) as well as mindfulness and adaptive coping (r=0.68) were highly correlated, which would violate multicollinearity if all variables were modeled simultaneously. We selected kinesiophobia over pain catastrophizing because it specifically involves attitudes towards movement, and is reported to be more highly related to physical function outcomes in chronic pain populations.29 We selected mindfulness over adaptive coping due to the strong emphasis on mindfulness and meditation-based skills in the programs.
Analysis Plan
We conducted multilevel linear modeling (MLM) using linear mixed-effects models (MIXED) in SPSS, version 24.0 (IBM, 2018). This approach to mediation allowed us to accommodate participant differences in baseline levels of study measures (ie, random intercepts) and retain all available data, thereby maximizing the power of analyses.30 Prior to modeling, we conducted descriptive analyses and examined assumptions for mediation analyses (eg, outliers, normality) using raw scores for each study variable. We then entered mean-centered and standardized z-scores for the study variables to calculate both unstandardized and unstandardized coefficients, respectively. The multiple mediation models described below used restricted maximum likelihood estimation and contained two levels: one for repeated assessments (Level 1: time, hypothesized mediators) and another of participants (Level 2).
We tested the three physical function outcomes in a separate multiple mediation models and entered all three mediators simultaneously. In each multiple mediation model, we entered Time as a predictor and the three treatment targets (kinesiophobia, pain resilience, and mindfulness) as mediators, physical function (step-count, 6-minute walk test, or WHODAS) as the outcome and participants as random effects. We adjusted for treatment group as a fixed effect in all models to quantify study-wide mediation by the treatment targets. The inclusion of all 3 mediators in the same model simultaneously enables identification of their unique influence on physical function outcomes.
To test the a path (change in the hypothesized mediators following the intervention; see Figure 1), we separately regressed changes in the three treatment targets (kinesiophobia, pain resilience, and mindfulness) on Time. To test the b path (relationship between changes in the hypothesized mediators and physical function), we separately regressed changes in the physical function outcomes (step-count, 6-minute walk test, or WHODAS) on changes in the treatment targets (kinesiophobia, pain resilience, and mindfulness) entered simultaneously as fixed effects to account for their shared variance. We regressed changes in the physical function outcomes on Time (c path) and the attenuation of these direct effects after including the mediators (c’ path). Finally, we tested the a*b path with Monte-Carlo resampling using the RMediation package31 in R 3.6.132 to calculate the 95% confidence interval (CI) of the indirect effects for each mediator. The indirect effect was deemed significant if the 95% CI did not include zero.33 The indirect effect of Time on the physical function variables through the mediators was the only requirement necessary to show mediation.34,35 Following guidelines for mediation in intervention research,36–38 we tested the indirect effects for all three outcomes regardless of whether the c path (changes in physical function over time) was statistically significant (p < 0.05). The effect size for the indirect effect was calculated via the Completely Standardized Indirect Effect (CSIE). Effect sizes of small, medium, and large magnitude correspond with standardized coefficients or approximately 0.01, 0.09, and 0.25, respectively.39
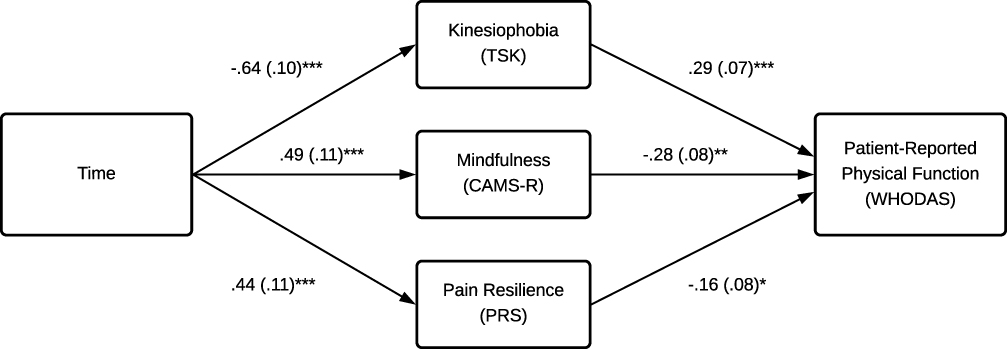 |
Figure 1 Multiple mediation model testing the effect of hypothesized mechanisms of change on patient-reported physical function. Notes: Paths specify level-1 mixed linear modeling (MLM) equations with standardized values, *p < 0.05; **p <0.01; ***p <0.001, path c’ ß = −.07 (0.10). |
Results
We summarize descriptive statistics in Table 2. Compared to patients with chronic pain in other trials, participants at baseline were generally sedentary (M daily step-count=~5400 steps),40 though variability was relatively wide (SD=~3000). Patients had relatively lower performance on the 6-minute walk test (M=~340 meters)41 and reported high disability scores on the WHODAS 2.0 (~32).5,42 Overall, mindfulness (M=31.21), kinesiophobia (M=39.09), and pain resilience (M=35.09) scores at baseline were comparable to previously reported values.12,26,43
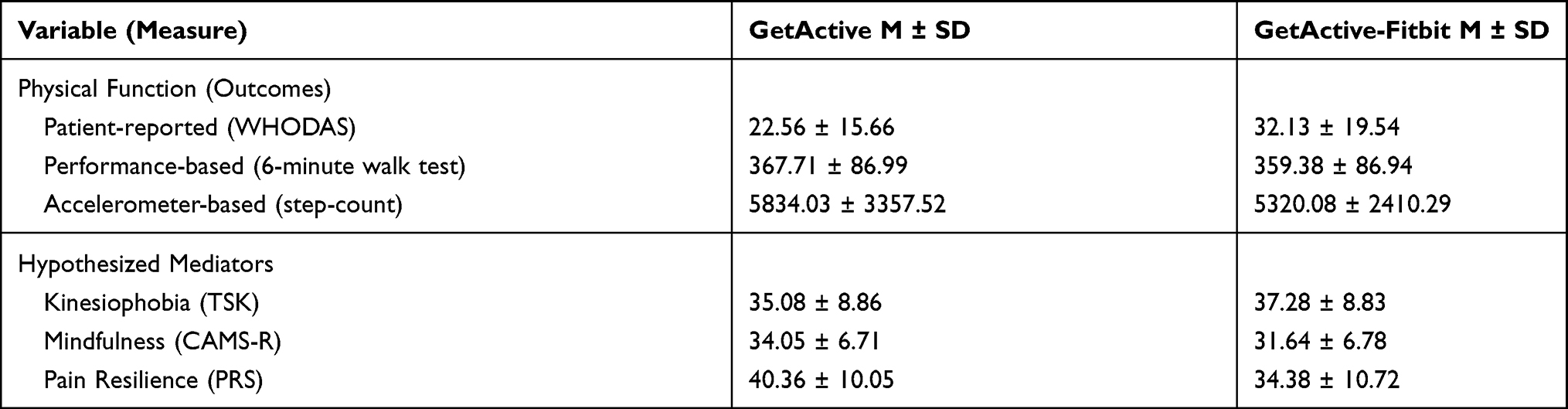 |
Table 2 Total Raw Scores for Primary Variables by Group |
Mediators of Improvement in Physical Function
Mixed-effects models for patient-reported, performance-based, and accelerometer-based physical function are summarized in Table 3. Mixed-effects modeling of a path indicated that all treatment targets improved following the programs. Pain resilience (b=4.73; CI=2.28, 7.18; p<0.001) and mindfulness (b=3.35; CI=1.89, 4.80; p<0.001) significantly increased, while kinesiophobia (b=−5.69; CI=−7.53, −3.85; p<0.001) significantly decreased from baseline to post-intervention (Figure 1). The a paths are identical across physical function outcomes; therefore, we report the remaining paths for step-count, 6-minute walk test, and WHODAS separately below.
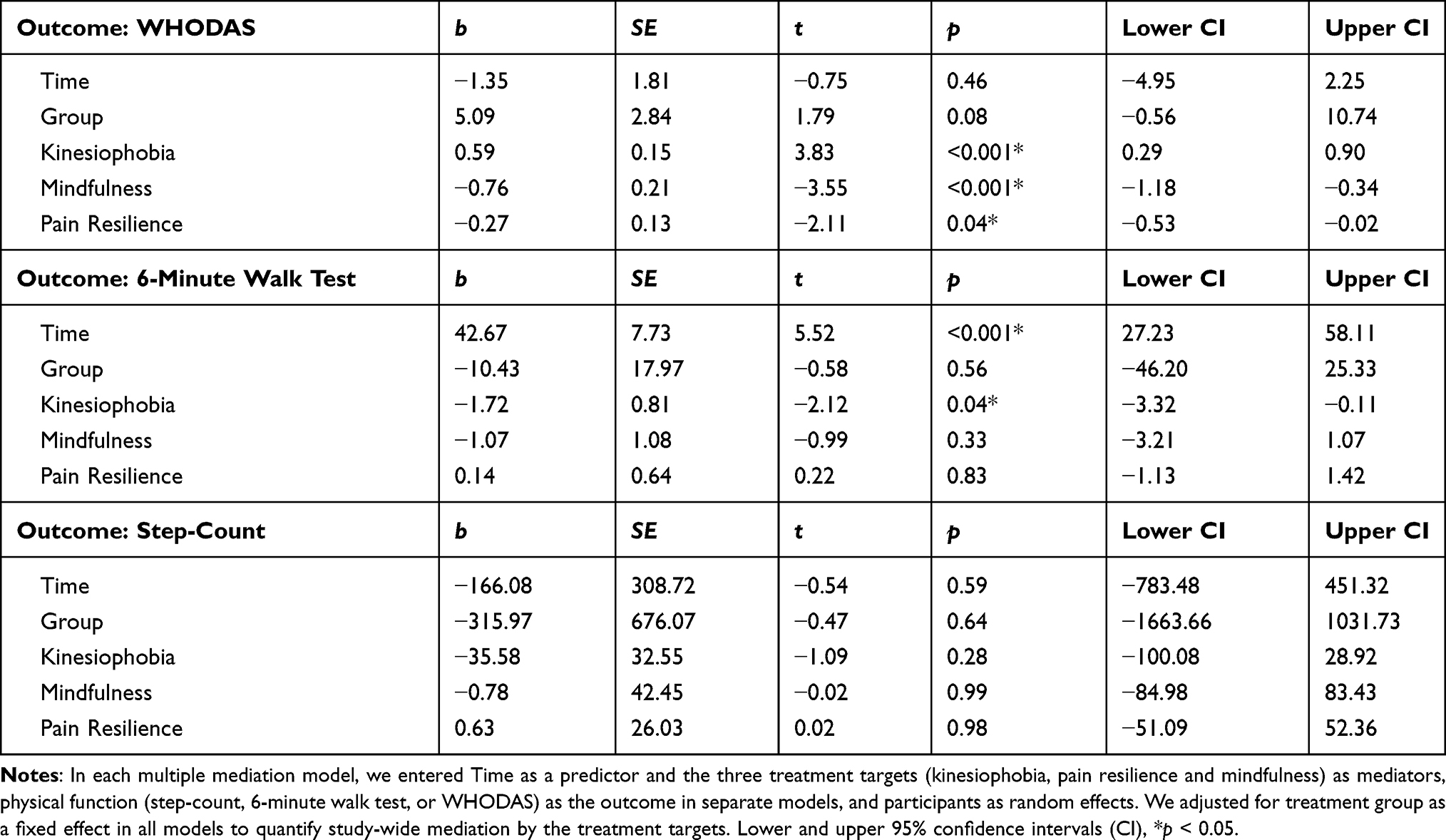 |
Table 3 Mixed-Effects Models for Patient-Reported, Performance-Based, and Accelerometer-Based Physical Function |
WHODAS
The b path was significant for mindfulness (b=−.76; CI=−1.18, −.34; p=0.001), pain resilience (b=−.27; CI=−.53, −.02; p=0.037), and kinesiophobia (b=0.59; CI=0.29–90; p<0.001), indicating that changes in each mediator uniquely explained changes in patient-reported disability from baseline to post-intervention (Figure 1). The c path indicated that WHODAS scores significantly decreased (ie, improved patient-reported physical function) from baseline to post-intervention (b=−8.42; CI=−12.23, −4.62; p<0.001). After including the mediators into the model (c’ path), the direct effect of Time on WHODAS was no longer significant (b=−1.35; CI=−4.95, 2.25; p=0.46), indicating full mediation. All indirect (path a*b) effects were significant, suggesting that decreases in kinesiophobia (CSIE=0.18; CI=0.08, 0.30; medium-large effect size), followed by increases in mindfulness (CSIE=−.14; CI=−25, −.05; medium effect size) and pain resilience (CSIE=−.07; CI=−.16, −.005; small-medium effect size), uniquely mediated improvements in disability from baseline to post-intervention.
6-Minute Walk Test
The b path indicated that, when the mediators were entered simultaneously, only changes from baseline to post-intervention in kinesiophobia accounted for unique variance in change in the 6-minute walk test (b=−1.72; CI=−3.32, −.11; p=0.036) from baseline to post-intervention (Figure 2). The b path for mindfulness (b=−1.07; CI=−3.21–1.07; p=0.32) and pain resilience (b=0.14; CI=−1.13, 1.41; p=0.83) was not significant. The c path indicated that the 6-minute walk test significantly increased (ie, greater performance-based physical function) from baseline to post-intervention (b=47.81; CI=34.74, 60.87; p<0.001). After including the mediators into the model (path c’), improvements on the 6-minute walk test remained significant (b=42.67; CI=27.23, 58.11; p<0.001). The indirect effect (path a*b) of Time on the 6-minute walk test through kinesiophobia was significant (CSIE=−.11; CI=−23, −.008; medium effect size), indicating that decreases in kinesiophobia partially mediated increases in the 6-minute walk test. The indirect effect of Time on 6-minute walk test through pain resilience (CSIE=0.008; CI=−.07–0.09) and through mindfulness (CSIE=−.04; CI=−.13–0.40) were each non-significant.
 |
Figure 2 Multiple mediation model testing the effect of hypothesized mechanisms of change on performance-based physical function. Notes: Paths specify level-1 mixed linear modeling (MLM) equations with standardized values, *p < 0.05; ***p <0.001, path c’ ß = 0.49 (0.09). Solid lines represent significant pathways and dashed lines represent non-significant pathway. |
Step-Count
The b path indicated that mindfulness (b =−.78; CI=−84.98, 83.42; p=0.98), pain resilience (b=0.63; CI=−51.09, 52.36; p=0.98) and kinesiophobia (b=−35.58; CI=−100.08, 28.92; p=0.28) did not significantly account for variance in step-count from baseline to post-intervention. Further, the c path revealed there were no significant increases in step-count from baseline to post-intervention (step-count b=7.31; CI=−529.99, 544.61; p=0.98). The c’ path, reflecting the direct effect of Time on step-count while taking the mediators into account, was non-significant (b=−166.08, CI=−783.48–451.31, p=0.59). The indirect effect (path a*b) of Time on step-count through mindfulness (CSIE=−.001; CI=−.10–0.10), pain resilience (CSIE=0.001; CI=−.09–0.09) and kinesiophobia (CSIE=−.07; CI=−.21–0.06) was non-significant.
Discussion
Improving physical function in patients with chronic pain is critical for reducing disability and healthcare costs. While psychosocial variables such as kinesiophobia, mindfulness, and pain resilience are associated with physical function, their specific role in improvements in physical function, and their potential differential impact on various facets of physical function measures remain unclear. The current study tested whether changes in kinesiophobia, mindfulness, and pain resilience – three theoretically informed constructs targeted in a mind-body activity program with (GetActive-Fitbit) or without (GetActive) a Fitbit device mediate changes in patient-reported (WHODAS), performance-based (6MWT), and objective/accelerometer-based (step-count) physical function.
In support of our primary hypothesis, kinesiophobia, mindfulness, and pain resilience all uniquely and fully mediated improvements in patient-reported physical function from baseline to post-intervention. In other words, increases in mindfulness and pain-resilience as well as decreases in kinesiophobia during the mind-body activity programs fully explained improvements in patient-reported physical function. This finding supports previous evidence linking these psychosocial variables to patient-reported physical function,12,16,17 and adds a mechanistic component, indicating that this relationship is one of mediation over time. This suggests that targeting kinesiophobia, mindfulness, and pain-resilience in interventions for chronic pain holds promise for increasing patients’ perceptions of their physical function. Of the three psychosocial variables, reduction in kinesiophobia had the largest mediation effect, followed by increases in mindfulness. While all three psychosocial variables hold unique contribution to increases in patient-reported physical function, there may be particular benefit to prioritizing fear of movement-related pain, given the degree to which it can limit patient-reported physical function.
We found mixed support for our exploratory hypothesis that the psychosocial variables would also mediate improvements in performance-based physical function. Kinesiophobia was the only psychosocial variable to significantly mediate improvements in performance-based psychical function. The more participants decreased their fear of movement-related pain following the intervention, the greater their improvements were in the distance walked for the 6-minute walk test. While improvements in mindfulness and pain-resilience contributed to participants’ perceptions and experiences of their own physical function, only improvements in kinesiophobia additionally contributed to improvement in functional capacity during a standard and time-limited performance test, further supporting the centrality of this variable in improving physical function. This centrality may also relate to the fact that of the three coping strategies, kinesiophobia is the only psychosocial variable that emphasizes movement, which directly relates to the distance-based nature of the 6-minute walk test.
None of the three psychosocial variables mediated changes in step-count from baseline to post-intervention. This finding, taken together with the discrepancy between the patient-reported and performance-based physical function reported previously,20 highlights the differentiation between each type of physical function measurement, and supports the notion that each of these measures captures unique and distinct dimensions of physical function.20,44 Further, it supports the importance of comprehensive and multidimensional assessment of physical function, in accord with IMMPACT7 and ICF8 guidelines.
Several strengths of this study are worth highlighting. The data in this study is from an RCT that utilized valid, reliable, and established measures, thus minimizing the risk of confounding factors. The analytical approach further supports the study’s rigor by simultaneously testing multiple mediators, controlling for other potentially contributing factors (eg, baseline individual differences, effect of Group) in a single model, and increasing statistical power by including all available RCT data. This study is the first, to our knowledge, to simultaneously test the mediating effects of multiple psychosocial variables on physical function and is one of very few trials complying with IMMPACT and ICF criteria for comprehensive assessment of physical function.
Study Limitations
Due to the fact that the study was primarily aimed at informing a future efficacy trial,9 the sample size is small and the study lacks a control group. Therefore, we are unable to attribute improvements specifically to either the GetActive and GetActive-Fitbit interventions. Additionally, the mediation analysis was limited to two time points. While this is preferable to mediation studies that use cross-sectional data,45,46 having only two timepoints limits causal inference. Future research with an active control group, larger sample size, a follow-up assessment and testing multiple sites to minimize selection bias may strengthen the findings of this study and the ability to infer causality.
Conclusion
This study is the first to test mechanisms of longitudinal improvement in physical function using all three types of measurement of physical function (patient-reported, performance-based, and objective/accelerometer-based) recommended by IMMPACT and ICF criteria. Interventions aiming to improve physical function in patients with chronic pain may benefit from emphasizing skills to minimize kinesiophobia (eg, by means of psychoeducation about pain, exposure, acceptance, and adaptive thinking) as well as skills to improve mindfulness and pain resilience to increase participants’ perceptions and experiences of their own physical function. Targeting kinesiophobia may further help improve patients’ functional capacity in a standard time-limited test. Additional components may be needed to facilitate ambulatory activity measured by accelerometer, emphasizing the multidimensionality of physical function and the need for interventions for chronic pain to assess physical function comprehensively via patient-reported, performance-based, and objective means.
Abbreviations
6MWT, 6-Minute Walk Test; CAMS-R, Cognitive and Affective Mindfulness Scale-Revised; ICF, International Classification of Functioning, Disability and Health; IMMPACT, Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials; IRB, Institutional Review Board; PRS, Pain Resilience Scale; RCT, Randomized Controlled Trial; TSK, Tampa Kinesiophobia Scale; WHODAS, World Health Organization Disability Assessment Schedule.
Sharing Data Statement
The datasets are available from the corresponding author upon request.
Acknowledgments
This work was supported by the National Center for Complementary and Integrative Health (IR34AT009356-01A1, 2017 to the senior author; 1K23AT01065301A1, 2020 to the first author). We thank Ms. Anya Ragnhildstveit for her contribution to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jackson W, Zale EL, Berman SJ, et al. Physical functioning and mindfulness skills training in chronic pain: A systematic review. J Pain Res. 2019;12:179–189. doi:10.2147/JPR.S172733
2. Pincus T, Burton AK, Vogel S, Field AP. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine. 2002;27:5. doi:10.1097/00007632-200203010-00017
3. La Cour P, Petersen M. Effects of mindfulness meditation on chronic pain: a randomized controlled trial. Pain Med. 2015;16(4):641–652. doi:10.1111/pme.12605
4. Thorn BE, Eyer JC, Van Dyke BP, et al. Literacy-adapted cognitive behavioral therapy versus education for chronic pain at low-income clinics a randomized controlled trial. Ann Intern Med. 2018;168(7):471–480. doi:10.7326/M17-0972
5. Tarvonen-Schröder S, Kaljonen A, Laimi K. Comparing functioning in spinal cord injury and in chronic spinal pain with two ICF-based instruments: WHODAS 2.0 and the WHO minimal generic data set covering functioning and health. Clin Rehabil. 2019;33(7):1241–1251. doi:10.1177/0269215519839104
6. Goverover Y, Kalmar J, Gaudino-Goering E, et al. The relation between subjective and objective measures of everyday life activities in persons with multiple sclerosis. Arch Phys Med Rehabil. 2005;86(12):2303–2308. doi:10.1016/j.apmr.2005.05.016
7. Taylor AM, Phillips K, Patel KV, et al. Assessment of physical function and participation in chronic pain clinical trials: IMMPACT/OMERACT recommendations. Pain. 2016;157(9):1836–1850. doi:10.1097/j.pain.0000000000000577
8. World Health Organization. International Classification of Functioning, Disability and Health (ICF); 2001.
9. Greenberg J, Popok PJ, Lin A, et al. A mind-body physical activity program for chronic pain with or without a digital monitoring device: proof-of-concept feasibility randomized controlled trial. JMIR Form Res. 2020;4(6):e18703. doi:10.2196/18703
10. Greenberg J, Lin A, Zale EL, et al. Development and early feasibility testing of a mind-body physical activity program for patients with heterogeneous chronic pain; the getactive study. J Pain Res. 2019;12:3279–3297. doi:10.2147/JPR.S222448
11. Fedoroff IC, Blackwell E, Speed B. Evaluation of group and individual change in a multidisciplinary pain management program. Clin J Pain. 2014;30(5):399–408. doi:10.1097/AJP.0b013e31829ea1f7
12. Woby SR, Roach NK, Urmston M, Watson PJ. Psychometric properties of the TSK-11: A shortened version of the Tampa Scale for Kinesiophobia. Pain. 2005;117(1–2):137–144. doi:10.1016/j.pain.2005.05.029
13. Liu X, Wang S, Chang S, Chen W, Si M. Effect of brief mindfulness intervention on tolerance and distress of pain induced by cold-pressor task. Stress Heal. 2013;29(3):199–204. doi:10.1002/smi.2446
14. Goubert L, Trompetter H. Towards a science and practice of resilience in the face of pain. Eur J Pain. 2017;21(8):1301–1315. doi:10.1002/ejp.1062
15. Norte GE, Solaas H, Saliba SA, Goetschius J, Slater LV, Hart JM. The relationships between kinesiophobia and clinical outcomes after ACL reconstruction differ by self-reported physical activity engagement. Phys Ther Sport. 2019;40:1–9. doi:10.1016/j.ptsp.2019.08.002
16. Garland EL, Froeliger B, Howard MO. Effects of mindfulness-oriented recovery enhancement on reward responsiveness and opioid cue-reactivity. Psychopharmacology. 2014;231(16):3229–3238. doi:10.1007/s00213-014-3504-7
17. Alschuler KN, Kratz AL, Ehde DM. Resilience and vulnerability in individuals with chronic pain and physical disability. Rehabil Psychol. 2016;61(1):7–18. doi:10.1037/rep0000055
18. Alschuler KN, Hoodin F, Murphy SL, Geisser ME. Ambulatory monitoring as a measure of disability in chronic low back pain populations. Clin J Pain. 2011;27(8):707–715. doi:10.1097/AJP.0b013e318217b7d0
19. Carvalho FA, Maher CG, Franco MR, et al. Fear of movement is not associated with objective and subjective physical activity levels in chronic nonspecific low back pain. Arch Phys Med Rehabil. 2017;98(1):96–104. doi:10.1016/j.apmr.2016.09.115
20. Greenberg J, Mace RA, Popok PJ, et al. Psychosocial correlates of objective, performance-based, and patient-reported physical function among patients with heterogeneous chronic pain. J Pain Res. 2020;13:2255–2265. doi:10.2147/JPR.S266455
21. Gewandter JS, Dworkin RH, Turk DC, et al. Improving study conduct and data quality in clinical trials of chronic pain treatments: IMMPACT recommendations. J Pain. 2019. doi:10.1016/j.jpain.2019.12.003
22. World Health Organization. Whodas 2.0. Assessment. 2010.
23. Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting small differences in functional status: the six minute walk test in chronic lung disease patients. Am J Respir Crit Care Med. 1997;155(4):1278–1282. doi:10.1164/ajrccm.155.4.9105067
24. Cain KL, Conway TL, Adams MA, Husak LE, Sallis JF. Comparison of older and newer generations of ActiGraph accelerometers with the normal filter and the low frequency extension. Int J Behav Nutr Phys Act. 2013;10. doi:10.1186/1479-5868-10-51
25. Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: assessing the ability to bounce back. Int J Behav Med. 2008;15(3):194–200. doi:10.1080/10705500802222972
26. Feldman G, Hayes A, Kumar S, Greeson J, Laurenceau JP. Mindfulness and emotion regulation: the development and initial validation of the Cognitive and Affective Mindfulness Scale-Revised (CAMS-R). J Psychopathol Behav Assess. 2007;29(3):177–190. doi:10.1007/s10862-006-9035-8
27. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
28. Carver CS. MOCS (Measure of Current Status); Published 2006. Available from: http://www.psy.miami.edu/faculty/ccarver/sclMOCS.html.
29. Odole A, Ekediegwu E, Ekechukwu END, Uchenwoke C. Correlates and predictors of pain intensity and physical function among individuals with chronic knee osteoarthritis in Nigeria. Musculoskelet Sci Pract. 2019;39:150–156. doi:10.1016/j.msksp.2018.11.014
30. Gu H. A mixed model approach for intent-to-treat analysis in longitudinal clinical trials with missing values. Methods Report. doi:10.3768/rtipress.2009.mr.0009.0903
31. Tofighi D, MacKinnon DP. RMediation: an R package for mediation analysis confidence intervals. Behav Res Methods. 2011;43(3):692–700. doi:10.3758/s13428-011-0076-x
32. R Development Core Team. R: A language and environment for statistical computing. R Found Stat Comput. 2019. doi:10.1017/CBO9781107415324.004
33. Preacher KJ, Selig JP. Advantages of monte carlo confidence intervals for indirect effects. Commun Methods Meas. 2012;6(2):77–98. doi:10.1080/19312458.2012.679848
34. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891. doi:10.3758/BRM.40.3.879
35. Zhao X, Lynch JG, Chen Q. Reconsidering Baron and Kenny: myths and truths about mediation analysis. J Consum Res. 2010;37(2):197–206. doi:10.1086/651257
36. O’Rourke HP, Mackinnon DP. Reasons for testing mediation in the absence of an intervention effect: A research imperative in prevention and intervention research. J Stud Alcohol Drugs. 2018;79(2):171–181. doi:10.15288/jsad.2018.79.171
37. O’Rourke HP, MacKinnon DP. When the test of mediation is more powerful than the test of the total effect. Behav Res Methods. 2015;47(2):424–442. doi:10.3758/s13428-014-0481-z
38. MacKinnon D. Introduction to Statistical Mediation Analysis. New York: Erlbaum and Taylor Francis Group; 2008.
39. Preacher KJ, Kelley K. Effect size measures for mediation models: quantitative strategies for communicating indirect effects. Psychol Methods. 2011;16(2):93–115. doi:10.1037/a0022658
40. Tudor-Locke C, Craig CL, Thyfault JP, Spence JC. A step-defined sedentary lifestyle index: <5000 steps/day. Appl Physiol Nutr Metab. 2013;38(2):100–114. doi:10.1139/apnm-2012-0235
41. Pankoff BA, Overend TJ, Lucy SD, White KP. Reliability of the six-minute walk test in people with fibromyalgia. Arthritis Rheum. 2000;13(5):291–295. doi:10.1002/1529-0131(200010)13:5<291::aid-anr8>3.0.co;2-x
42. Silva C, Coleta I, Silva AG, et al. Adaptation and validation of whodas 2.0 in patients with musculoskeletal pain. Rev Saude Publica. 2013;47:4. doi:10.1590/S0034-8910.2013047004374
43. Slepian PM, Ankawi B, Himawan LK, France CR. Development and initial validation of the pain resilience scale. J Pain. 2016;17(4):462–472. doi:10.1016/j.jpain.2015.12.010
44. Conway J, Tomkins CC, Haig AJ. Walking assessment in people with lumbar spinal stenosis: capacity, performance, and self-report measures. Spine J. 2011;11(9):816–823. doi:10.1016/j.spinee.2010.10.019
45. Maxwell SE, Cole DA. Bias in cross-sectional analyses of longitudinal mediation. Psychol Methods. 2007;12(1):23–44. doi:10.1037/1082-989X.12.1.23
46. Goldsmith KA, MacKinnon DP, Chalder T, White PD, Sharpe M, Pickles A. Tutorial: the practical application of longitudinal structural equation mediation models in clinical trials. Psychol Methods. 2018;23(2):191–207. doi:10.1037/met0000154
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.