")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Mimicking Rosacea? Jessner’s Lymphocytic Infiltration of the Skin: A Case Report
Received 15 December 2023
Accepted for publication 29 February 2024
Published 13 April 2024 Volume 2024:17 Pages 847—851
DOI https://doi.org/10.2147/CCID.S452008
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jeffrey Weinberg
Lingjia Li,1 Yulan Wang,2 Hua Gu2
1Department of Dermatology, Jiangnan University Medical Center, Jiangnan University, Wuxi, People’s Republic of China; 2Department of Dermatology, The First Affiliated Hospital of Kunming Medical University Kunming, Kunming, People’s Republic of China
Correspondence: Hua Gu, Department of Dermatology, The first Affiliated Hospital of Kunming Medical University Kunming, Kunming, People’s Republic of China, Tel +86-18762675765, Email [email protected]
Abstract: We report a case of rash in a 35-year-old female presenting with erythematous papules and infiltrative plaques on the nose and upper jaw resembling rosacea. The patient had been experiencing these symptoms for one year. A pathological biopsy revealed an inflammatory infiltrate consisting of dense perivascular lymphocytes surrounding hair follicles and sweat glands in the dermis. Immunohistochemistry demonstrated a predominance of CD4+ T cells compared to CD8+ T cells. Based on the clinical manifestations, histopathology, and immunohistochemistry, the patient was diagnosed with Jessner’s Lymphocytic infiltration of the skin (JLIS). The patient was treated with oral Minocycline, 100mg twice daily. After 4 weeks, the dosage was reduced by half and the treatment continued for 2 months, resulting in complete resolution of the rash. The clinical presentation resembled rosacea, and this particular manifestation of JLIS has not been previously reported. Treatment with minocycline yielded satisfactory efficacy, and no recurrence has been observed for 5 year.
Keywords: lymphocytic infiltration, skin, rosacea, minocycline
Introduction
JLIS, first described by Jessner and Kanof in 1953,1 is a rare chronic condition that mimics a pseudo-T-cell lymphoma. It lacks clonality and has a benign nature, although less commonly seen. JLIS is characterized by a CD8+ polyclonal reactive skin condition.2 However, in our patient, the main feature was infiltration of the dermis with a predominance of CD4+ T cells. It has been proposed that CD4+ T cells are predominant in the acute phase, while CD8+ T cells are predominant in the chronic phase and may be involved in JLIS recurrence.3 Clinically, JLIS presents as asymptomatic single or multiple scar-free erythematous papules or plaques, typically occurring on the face, neck, upper back, and trunk. Involvement of the entire nose and upper jaw is rare, making this case report the first of its kind.
Case Presentation
On March 7, 2018, a 35-year-old Chinese female patient presented with a one-year history of persistent erythematous papules and infiltrative plaques on the nose without any obvious triggers. Initially, a hard nodule the size of rice grains appeared on the right alar part of the nose, which was painless and itchy. Over time, the skin lesions gradually increased in size, became thick, and diffused across the entire nose. Infiltrating plaques also developed on the upper jaw. Initially, the patient was diagnosed with rosacea. However, the discovery of infiltrating plaques in the upper jaw indicated a more complex condition that required closer attention.
Past and family history revealed no similar diseases within the family. Since the onset of the illness, the patient’s urine, stool, and weight remained normal. Skin examination revealed diffuse erythematous papules, infiltrations, and hypertrophic plaques on the entire nose and upper jaw, with a smooth surface (Figure 1A–C). Dermoscopy showed a bright red background with diffuse telangiectasia, but no obvious keratinized hair follicle structures (Figure 2A). Laboratory examinations, including antinuclear antibody, anti-dsDNA antibody, anti-Ro, anti-La, and Borrelia, as well as direct immunofluorescence serology, yielded negative results. Blood and urine routine tests, liver and kidney function tests, chest X-ray, and ECG all showed no obvious abnormalities. Maxillary CT plain scan with enhancement revealed several findings: (1) a soft tissue nodule in the right soft palate, with multiple enlarged lymph nodes in both necks, and thickening and enhancement of nasal soft tissue; (2) right frontal sinus and ethmoid sinusitis. Histopathological examination of the biopsy sample showed a normal epidermis and an inflammatory infiltrate consisting of dense perivascular lymphocytes, as well as lymphocytes surrounding hair follicles and sweat glands in the dermis. Immunohistochemistry demonstrated a predominance of CD4+ T cells compared to CD8+ T cells (Figure 2B and C). The immunohistochemical panel further revealed positive staining for CD3, CD4, CD8, CD20, CD43, CD68, CD1a, and Ki-67 (10%), while staining for CD123, CD56, GB, PAS, and acid-fast organisms was negative (Figure 3A–K). TCR gene rearrangement analysis did not show any clonal amplification peaks in the target fragment. Differential diagnosis included rosacea and lymphoma. Based on the clinical and histological characteristics observed, and the absence of evidence supporting cutaneous lymphoma in the immunohistochemical studies, the definitive diagnosis of JLIS was established.
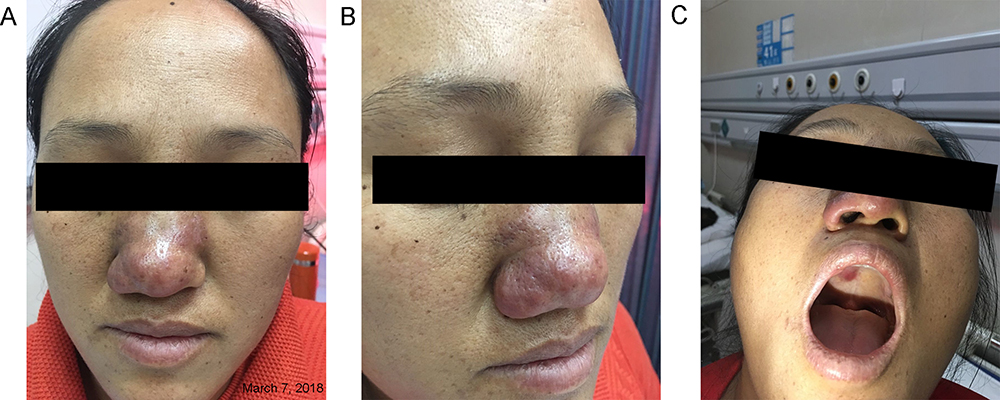 |
Figure 1 (A-C) Erythematous, infiltrating plaques on the patient’s nose and upper jaw. |
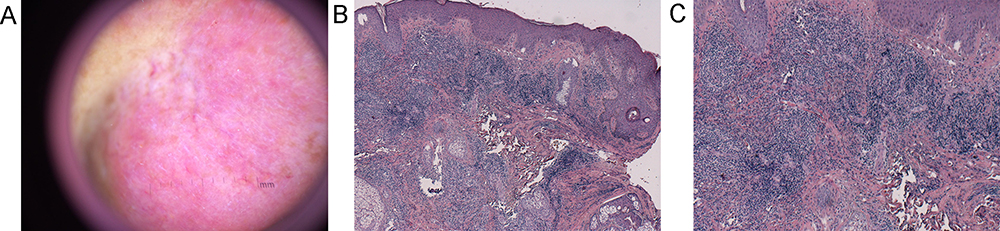 |
Figure 2 (A) Dermoscopy shows bright red background with diffuse telangiectasia but no obvious keratinized hair follicle structure. (B) Biopsy from nose. The epidermis is normal and there are dense perivascular, hair follicles and sweat glands lymphocytic infiltrates. (C) Periadnexial mature lymphocytes was observed in the dermis, mostly of CD4+ T cells. |
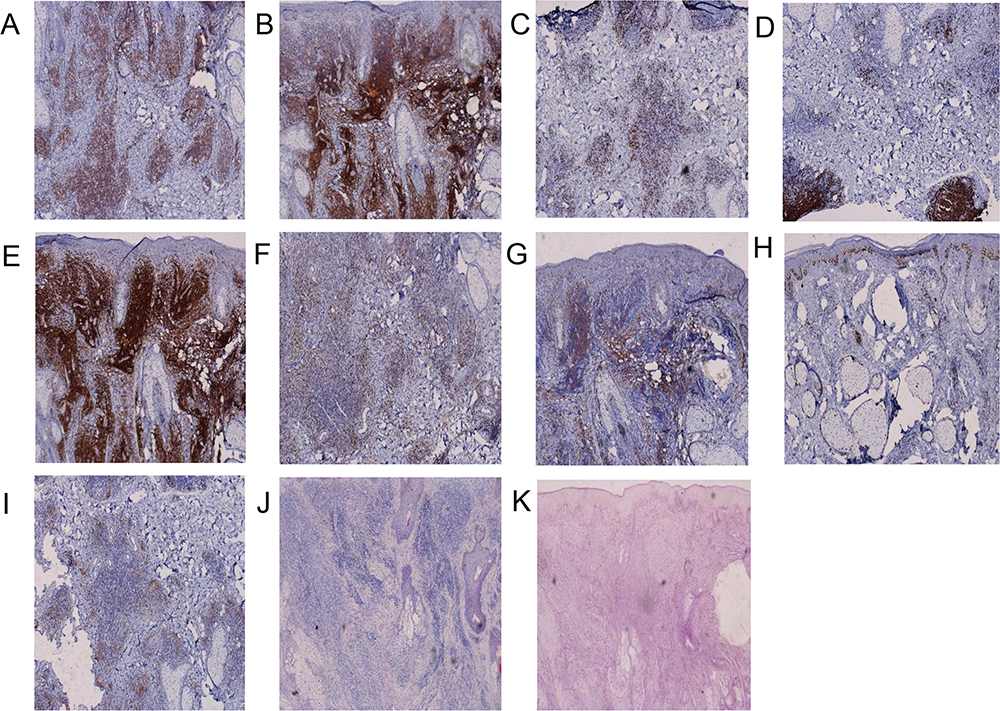 |
Figure 3 (A–K) CD3 (+), CD4 (+++), CD8 (+), CD20 (+), CD1a (+), CD43 (+), CD68 (+), Ki-67 10% (+), CD123 (-), acid-fast dyeing (-), PAS (-). |
Minocycline, known for its anti-neutrophil differentiation and lymphocyte proliferation effects, is commonly used in clinical practice due to its minimal side effects. In this case, the patient was prescribed oral Minocycline at a dose of 100mg twice a day. After 4 weeks of treatment, a significant improvement was observed with an 80% regression of infiltrative erythema, prompting a reduction in Minocycline dosage. During the outpatient follow-up conducted 2 months later, complete clearance of the skin changes on the nose and upper jaw was observed, leading to the discontinuation of Minocycline treatment (Figure 4A–C). No adverse reactions were observed, and there was no recurrence during the 5-year observation period. The patient is currently still under follow-up.
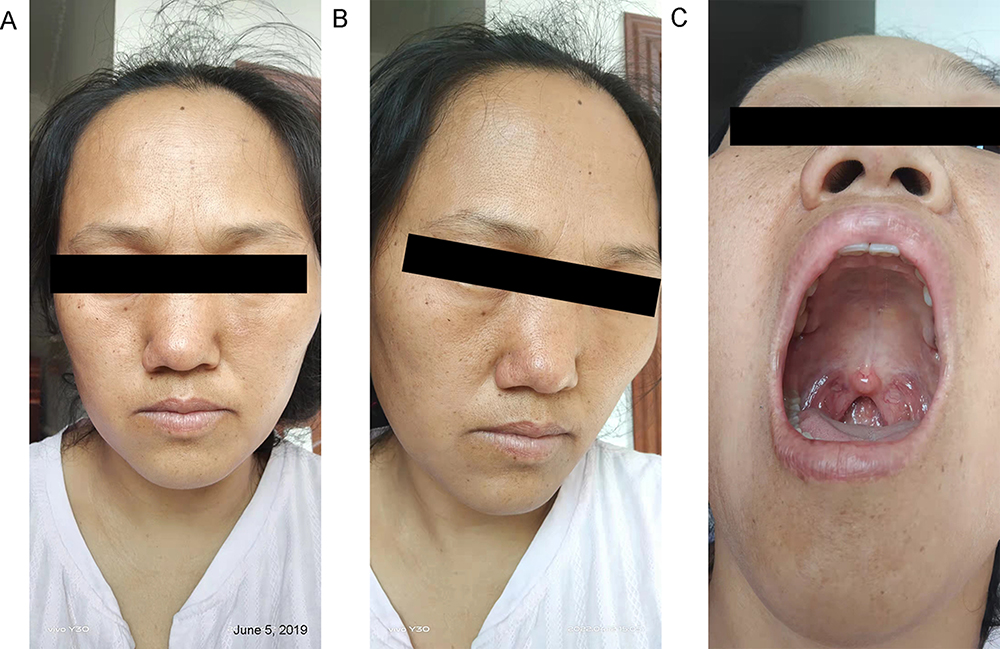 |
Figure 4 (A–C) Erythematous, infiltrating plaques changes had cleared completely. |
Discussion
JLIS is characterized by erythematous papules and plaques primarily located on the face, neck, and trunk. Differential diagnosis of JLIS includes conditions such as lupus erythematosus, gyrate erythema, polymorphous light eruption, lymphocytoma cutis, and lymphocytic leukemia. There is ongoing debate regarding whether JLIS is a distinct entity on its own4 or part of the disease spectrum that includes cutaneous lupus erythematosus, polymorphous light eruption, cutaneous lymphoid hyperplasia, and reticular erythematous mucinosis. Here, we present a case of JLIS with atypical clinical features suggestive of rosacea.
Rosacea predominantly affects individuals in middle age, specifically those aged 30 to 50 years, with a higher incidence observed in females than in males. It is characterised as a chronic inflammatory condition manifesting in the nose and perinasal areas. The subject of this case is a middle-aged female presenting with a rash on the nose, necessitating differentiation from the rhinophymatous stage of rosacea. Severe nasal hypertrophy is more frequently observed in males over the age of 40, featuring enlarged and distorted nasal tips that resemble tumorous growths. Notably, the surfaces of these nasal enlargements exhibit markedly dilated sebaceous gland openings from which streaks of white, viscous sebum exude upon compression. Given the absence of these characteristics in the present case, a diagnosis of rosacea can be confidently excluded.
JLIS is a rare disorder with an unclear etiology. Genetic factors may play a role, as evidenced by a reported familial case of the disease.3 Another potential etiology is autoimmune. It has been hypothesized that JLIS could be an early cutaneous manifestation of systemic lupus erythematosus (SLE) or even a progression of lupus erythematosus tumidus. Photosensitivity has also been suggested as a trigger for this condition, along with a few reported cases related to contact allergy.5 Additionally, JLIS has been associated with certain medications, particularly angiotensin-converting enzyme inhibitors, as well as immunosuppressive therapies such as etanercept, ustekinumab, and leflunomide.6 In rare instances, infections like HIV and Borrelia burgdorferi have been implicated.7,8
Current treatment primarily involves topical options such as glucocorticoid ointment and calcineurin inhibitors. Systemic therapies including proquazone, hydroxychloroquine, etretinate, thalidomide, auranofin, and methotrexate have been used.9,10 Less common treatment approaches encompass laser therapy and photodynamic therapy. Minocycline, known for its multiple anti-inflammatory mechanisms, including the inhibition of proinflammatory cytokines and modulation of immune cell function, has shown promise in the treatment of JLIS. In this case, minocycline was successfully utilized, leading to satisfactory outcomes. However, further clinical validation is necessary to determine whether the complete resolution of the patient’s rash was due to the natural healing process of JLIS or the beneficial effects of minocycline. Clinicians should remain vigilant and conduct long-term follow-up with these patients.
Conclusion
There exists no definitive treatment for JLIS. Despite the scarcity of published evidence and guidelines, this case indicates that oral minocycline may be considered both safe and efficacious in managing JLIS, without any observed recurrence. Significantly, this case documents a rare instance of JLIS, wherein the clinical presentation closely resembles that of rosacea, further complicated by atypical manifestations affecting the upper jaw.
Data Sharing Statement
The data underlying this article are available in the article.
Ethical Approval
This case doesn’t need institutional approval.
Informed Consent
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images.
Author Contributions
Lingjia Li carried out the studies, participated in collecting data, and drafted the manuscript. Yulan Wang performed the statistical analysis and participated in its design. Hua Gu participated in acquisition, analysis, or interpretation of data and draft the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jessner M, Kanof B. Lymphocytic infiltration of the skin. Arch Dermatol. 1953;68:447–449.
2. Poenitz N, Dippel E, Klemke CD, Qadoumi M, Goerdt S. Jessner’s lymphocytic infiltration of the skin: a CD8+ polyclonal reactive skin condition. Dermatology. 2003;207(3):276–284. doi:10.1159/000073090
3. Dippel E, Poenitz N, Klemke CD, Orfanos CE, Goerdt S. Familial lymphocytic infiltration of the skin: histochemical and molecular analysis in three brothers. Dermatology. 2002;204(1):12–16. doi:10.1159/000051803
4. Tzung TY, Wu JC. Topical calcineurin inhibitors in treating Jessner’s lymphocytic infiltration of the skin: report of a case. Br J Dermatol. 2005;152(2):383–384. doi:10.1111/j.1365-2133.2005.06349.x
5. Caroli UM, Berner D, Schlegel C, et al. Lymphocytic infiltration of the skin Jessner-Kanof after treatment with a hydroquinone-containing bleaching cream. Arch Dermatol. 2006;142(12):1655–1656. doi:10.1001/archderm.142.12.1655
6. Abbad N, Lanal T, Brenuchon C, Morel G, Deprez X. Etanercept-induced lymphocytic infiltration of Jessner-Kanof. Arthritis Rheumatol. 2018;70(3):449. doi:10.1002/art.40347
7. Demirbaş A, Çelik ZE. Jessner’s lymphocytic infiltration as a symptom of immune reconstitution inflammatory syndrome in an HIV-infected patient: a case report. Dermatol Ther. 2020;33(4):e13637. doi:10.1111/dth.13637
8. Ziemer M, Eisendle K, Müller H, Zelger B. Lymphocytic infiltration of the skin (Jessner-Kanof) but not reticular erythematous mucinosis occasionally represents clinical manifestations of Borrelia-associated pseudolymphoma. Br J Dermatol. 2009;161(3):583–590. doi:10.1111/j.1365-2133.2009.09279.x
9. Michel JL, Perrin D. Infiltrat lymphocytaire de Jessner et Kanof traité par laser à colorant pulsé [Pulsed dye laser treatment for Jessner’s lymphocytic infiltration of the skin]. Ann Dermatol Venereol. 2010;137(12):803–807. French. doi:10.1016/j.annder.2010.08.010
10. Park KY, Kim HK, Li K, et al. Photodynamic therapy: new treatment for refractory lymphocytic infiltration of the skin. Clin Exp Dermatol. 2012;37(3):235–237. doi:10.1111/j.1365-2230.2011.04189.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.