Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Microtubule-Associated Protein 4 Overexpression Correlates with Early Recurrence in Hepatitis B Virus-Associated Hepatocellular Carcinoma Patients Following Curative Hepatic Resection
Authors Su YA ![]() , Li YT, Wu HL, Kao JH, Chen PJ, Liu CJ
, Li YT, Wu HL, Kao JH, Chen PJ, Liu CJ
Received 28 November 2025
Accepted for publication 17 February 2026
Published 12 March 2026 Volume 2026:13 578725
DOI https://doi.org/10.2147/JHC.S578725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Yu-An Su,1,2 Yung-Tsung Li,1,2 Hui-Lin Wu,1– 3 Jia-Horng Kao,1,2,4 Pei-Jer Chen,1– 4 Chun-Jen Liu1,2,4
1Hepatitis Research Center, National Taiwan University Hospital, Taipei, Taiwan; 2Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan; 3Graduate Institute of Microbiology, College of Medicine, National Taiwan University, Taipei, Taiwan; 4Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
Correspondence: Hui-Lin Wu, Hepatitis Research Center, National Taiwan University Hospital, Room 634, Changde St. No. 1, Zhongzheng District, Taipei, 10002, Taiwan, Tel +886 23123456-267506, Email [email protected] Chun-Jen Liu, Hepatitis Research Center, National Taiwan University Hospital, Room 630, Changde St. No. 1, Zhongzheng Dist, Taipei, 10002, Taiwan, Tel +886 23123456-267503, Email [email protected]
Purpose: This study aimed to investigate the clinical significance of MAP4 in hepatocellular carcinoma (HCC), particularly its association with metastasis-related early recurrence after curative hepatic resection.
Patients and Methods: We enrolled 172 patients with hepatitis B virus-associated HCC (HBV-HCC) who underwent curative resection in our cohort. After excluding potential confounders such as vascular invasion and portal vein thrombosis, 101 patients were selected for MAP4 gene expression analysis by qRT-PCR. Kaplan-Meier and Cox regression analyses were conducted to evaluate its association with early recurrence and prognostic factors. Our findings were further validated in an independent cohort.
Results: MAP4 expression was upregulated in HCC cell lines and tumor tissues, compared to their corresponding non-tumorous controls. The clinical analysis showed that high MAP4 overexpression in liver tumor tissues was positively correlated with early (p = 0.042) rather than late recurrence (p = 0.221) in our cohort. Moreover, it was linked to shorter recurrence-free survival (p = 0.023) and reduced overall survival (p = 0.015). The expression level of serum alpha-fetoprotein (p = 0.001), tumor size (p = 0.012), tumor number (p = 0.018), satellite tumor (p = 0.001), and MAP4 expression (p = 0.042) were correlated with HCC early recurrence by univariate analysis. Consistent clinical findings were observed in the validation cohort.
Conclusion: This study demonstrated that MAP4 overexpression in liver tumor tissue was positively correlated with early recurrence in HBV-HCC patients following curative hepatic resection, providing insights into its clinical significance and potential involvement in underlying molecular mechanisms, particularly in metastasis-related early recurrence.
Keywords: curative hepatic resection, early recurrence, hepatitis B virus-associated hepatocellular carcinoma, HBV-HCC, metastasis, microtubule-associated protein 4, MAP4
Introduction
Hepatocellular carcinoma (HCC) is the fourth leading cause of cancer-related death worldwide.1 Currently, curative hepatectomy is commonly used to treat HCC patients.2 Although the postoperative mortality rate of HCC patients has improved, the overall mortality rate remains significantly high owing to the sustained risk of tumor recurrence.3 The cumulative recurrence rate was up to 50% in HCC patients after surgery within 2 years, and up to 70% of cases 5 years after treatment.4 Generally, early recurrence is defined as recurrence within 2 years. It is primarily attributed to intrahepatic metastasis, whereas late recurrence occurs after 2 years and is mostly caused by de novo tumor formation.5 A more stringent criterion defines early recurrence as occurring within 1 year after surgery. It showed that recurrence within the first postoperative year had more significant effects on overall mortality than recurrence in the second year. Moreover, the recurrence pattern was changed after 1 year.6
Early recurrence accounts for up to 70% of HCC recurrences and is one of the main causes of high mortality rates.3,7 Tumor heterogeneity is a crucial factor contributing to recurrent manifestations and underlies the multifaceted clinical features and variable therapeutic responses observed in HCC.8,9 Such heterogeneity substantially complicates therapeutic strategies and poses a major challenge in the clinical management of HCC. Therefore, assessing the clinical significance of specific molecules in tumors is critical for identifying potential therapeutic targets and elucidating the mechanisms driving tumor recurrence.
We previously identified the major splice variant of metastatic tumor antigen 1 (MTA1), termed MTA1dE4 (lacking exon 4), as a better biomarker for early recurrence than the full-length MTA1 (MTA1-FL) in HBV-HCC patients following curative hepatic resection.10 To explore the underlying mechanisms of MTA1dE4-associated early recurrence, we employed an immunoprecipitation-mass spectrometry (IP-MS) approach and identified microtubule-associated protein 4 (MAP4) as a specific interacting partner of MTA1dE4, but not MTA1-FL (data not shown). MAP4 primarily functions to stabilize microtubules11,12 and is essential for proper spindle assembly during mitosis and for coordinating cytoskeletal remodeling during cell migration,13,14 a key feature of metastatic tumor cells.15,16 Dysregulation of MAP4 expression has been documented in several malignancies. For instance, overexpression of MAP4 has been shown to contribute to cell invasion in esophageal squamous cell carcinoma and promote radioresistance through epithelial–mesenchymal transition (EMT) in lung adenocarcinoma.17,18 Notably, one study demonstrated that MAP4 is overexpressed in highly migratory metastatic cancer cells and is associated with poor survival in patients with HCC.19 However, the clinicopathological significance of MAP4 in HBV-HCC patients undergoing curative hepatic resection remains poorly understood. Therefore, the present study aims to clarify the clinical relevance of MAP4 in this patient population.
Our clinical findings provide a novel insight into the significance of MAP4, especially its association with early recurrence in HBV-HCC patients. These results provide a foundation for future research on its clinical application and underlying molecular mechanisms.
Materials and Methods
Study Cohorts, Patient Enrollment, and HCC Specimens
In this retrospective study, we analyzed two independent cohorts of HBV-related hepatocellular carcinoma (HBV-HCC) patients who underwent curative hepatic resection: the NTUH and the Fudan University cohorts. (I) NTUH cohort: This cohort consisted of 172 HBV-HCC patients who underwent hepatectomy at National Taiwan University Hospital (NTUH, Taipei, Taiwan) between 1997 and 2000. Patients were excluded if they had portal vein thrombosis, vascular or lymphatic invasion, residual intrahepatic or extrahepatic tumors, deaths from non-HCC-related causes, or a postoperative follow-up period of less than 1 year. Curative hepatic resection was defined as complete tumor removal with a tumor-free margin of ≥1 cm in the resected hepatic specimen. Additionally, patients with evidence of residual intrahepatic tumors on contrast-enhanced imaging within 3 months postoperatively were excluded. After applying these criteria, a total of 101 HBV-HCC patients with available clinical liver specimens were included in the analysis. The patient selection process for the NTUH cohort is summarized in Figure 1.
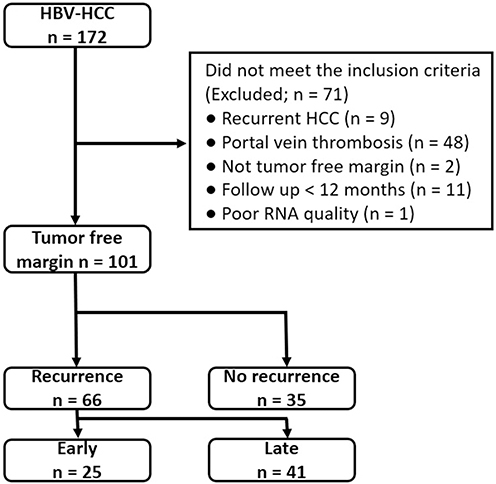 |
Figure 1 Flowchart of patient enrollment in the NTUH cohort. Abbreviations: HBV-HCC, Hepatitis B virus-associated hepatocellular carcinoma; HCC, hepatocellular carcinoma; n, number of patients. |
Following hepatic resection, patients were routinely monitored at outpatient clinics every 3 months, or more frequently if clinically indicated. Among the 101 patients in the cohort, only one had received lamivudine therapy for chronic HBV infection, and none received adjuvant therapy for HCC. All patients underwent liver ultrasonography at 3-month intervals. During each imaging visit, blood biochemical profiles, liver function tests, and serum alpha-fetoprotein (AFP) levels were assessed. When tumor recurrence was suspected during follow-up, additional diagnostic imaging with computed tomography (CT) or magnetic resonance imaging (MRI) was performed to confirm the presence and characteristics of the recurrent tumor. Tumor recurrence was defined based on one of the following criteria: (1) histological confirmation via tumor biopsy or resected specimens from repeat hepatic resection, or (2) concordant findings from at least two non-invasive imaging modalities (eg., CT and MRI) accompanied by elevated serum AFP levels (>400 ng/mL). The recurrence-free interval was defined as the time from the date of primary hepatic resection to the date of confirmed tumor recurrence. The follow-up period was defined as the interval from surgery to the earliest occurrence of tumor recurrence, death, or the last clinical visit. Written informed consent was obtained from all patients, and the study protocol was approved by the Institutional Review Board of National Taiwan University Hospital.
(II) The Fudan University cohort: This cohort served as an independent validation group in this study. Gene expression profiles and corresponding clinical data were retrieved from the NCBI Gene Expression Omnibus (accession number: GSE14520). It included 221 patients with HBV-HCC. All liver specimens were histologically confirmed as HCC and graded according to Edmondson’s grading system.
Cell Line and Cell Culture
Human hepatoma cell lines Hep3B and SNU-387 were purchased from the American Type Culture Collection (ATCC, Manassas, VA, USA), and the HepG2 and HA22T cell lines were obtained from the Bioresource Collection and Research Center (BCRC, Hsinchu, Taiwan). The HuH-7 cell line, originally established in the 1980s,20 was kindly provided by Dr. Jiro Sato (Japan). As the HuH-7 cells were not obtained from a commercial vendor, their experimental use, along with that of other cell lines used in this study, was reviewed and approved by the Committee of Biological Safety at National Taiwan University Hospital. The identity of HepG2, Hep3B, HuH-7, Tong, SNU-387, Mahlavu, and HA22T has been authenticated by Short Tandem Repeat (STR) profiling. The HuS-E/S cell line was verified by assessing the expression patterns of selected key marker genes reported in the original publication describing this cell line,21 as no reference STR profile is available for this cell line.
Human liver cancer cell lines HepG2, HuH-7, Hep3B, and HA22T were cultured in Dulbecco’s modified Eagle’s medium (DMEM; Corning, USA). SNU-387 was cultured in Roswell Park Memorial Institute (RPMI; Corning, USA) medium and incubated at 37°C with 5% CO2. Both DMEM and RPMI media contained 10% fetal bovine serum (Hyclone, Cytiva, USA), MEM Non-essential Amino Acids, HEPES Buffer, and glutagroTM Supplement (Corning, USA). The use of these cell lines was approved by the Committee of Biological Safety of the National Taiwan University Hospital.
Conventional Reverse Transcription-Polymerase Chain Reaction (RT-PCR) and Quantitative RT-PCR (RT-qPCR)
Total RNA was extracted from cells using TRIzol (Invitrogen; CA, USA), and 0.5 μg of total RNA was reverse transcribed into cDNA using the HiScript® III All-in-one RT SuperMix (Vazyme; China). Human normal liver tissue RNA was purchased from OriGene Technologies (Rockville, MD, USA). Conventional RT-PCR was used to amplify MAP4, using the following primers: “Forward: 5”-ggtgcagaatggctgacctcag-3’ and “Reverse: 5”-gctctaagggaactgccgttg-3”. In addition, cDNA derived from the HuS-E/2, Tong, Mahlavu, and HCC36 cell lines was provided by other researchers. Quantitative real-time RT-PCR was conducted on a Rotor-Gene Q qRT-PCR system (QIAGEN, Germany) to assess MAP4 mRNA expression levels in liver tissues using the following primers: “Forward: 5’-caaggataaagcactacc-3’ and “Reverse: 5’-tttctgtttctgggagtt-3’. The thermal cycling conditions consisted of 40 cycles of denaturation at 95°C for 10 seconds, annealing at 60°C for 10 seconds, and extension at 72°C for 10 seconds. Gene expression levels were quantified by interpolation from a standard curve generated using plasmids containing the target sequence. Expression of Dead-box helicase 5 (DDX5) was used as the internal control.
Statistical Analysis
Graphs were generated using GraphPad Prism 5, and all statistical analyses were performed using SPSS (version 24.0; IBM, Chicago, IL). The normal distribution of data was assessed using the Shapiro–Wilk test. In the NTUH cohort, MAP4 expression levels did not follow a normal distribution (p < 0.05); therefore, the Wilcoxon signed-rank test was used for comparisons between tumor and paired non-tumor tissues. Conversely, the validation cohort met the criteria for normal distribution (p > 0.05), and a paired t-test was employed. Associations between categorical variables were evaluated using the chi-square test with a 2×2 contingency table Survival differences were assessed using the Kaplan-Meier survival analysis with the log-rank (Mantel-Cox) test. Multivariate analysis was conducted using the Cox proportional hazards regression model to identify independent factors significantly associated with early recurrence. Post hoc power analysis was performed using G*Power (version 3.1) with an alpha level of 0.05. A P value < 0.05 was considered statistically significant.
Use of AI Tools
During the preparation of this manuscript, the authors drafted the original text independently. Artificial intelligence tools (such as OpenAI’s ChatGPT) were used to improve grammar and clarity. All content was carefully reviewed and verified by the authors to ensure accuracy and originality.
Results
Baseline Characteristics of Patients
We analyzed patient cohorts from NTUH and Fudan University to investigate the clinical significance of MAP4 in HBV-HCC. The Fudan cohort was used as an independent validation group in this study. Demographic and baseline clinicopathological characteristics of the NTUH cohort are summarized in Table 1. The median follow-up duration was 48.2 months (range, 16.6–150.4), during which 66 patients (65.3%) experienced tumor recurrence. Details regarding the patient recruitment criteria, demographics, and clinicopathological features of the validation cohort can be found in the reference.22 The NTUH and Fudan University cohorts included 25 and 60 early recurrence HBV-HCC patients, respectively (37.8% and 27.1%). In this study, early recurrence was defined as recurrence occurring within 1 year after surgery, as it represents a more stringent criterion.6
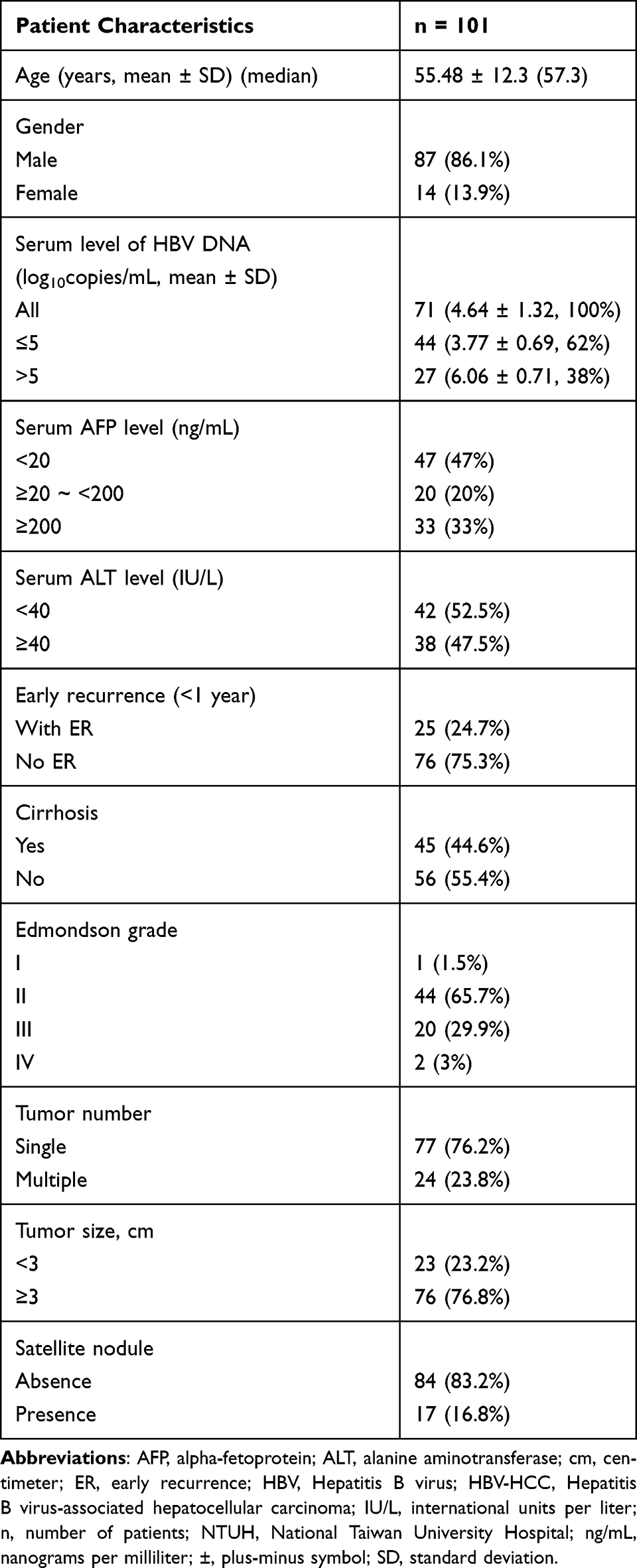 |
Table 1 Clinical Characteristics of 101 HBV-HCC Patients in the NTUH Cohort at the Time of Surgery |
MAP4 Gene Expression Is Upregulated in HCC Cell Lines and Tumor Tissues
Our previous study revealed an interaction between MAP4 and the major MTA1 splice variant MTA1dE4. Given the role of MTA1dE4 in the early recurrence of HCC,10 we hypothesized that MAP4 might also contribute to HCC progression. To investigate the hypothesis, we first analyzed the clinical significance of MAP4 in patients with HBV-HCC. We examined the expression levels of MAP4 in HCC cell lines and human liver tumor tissues, respectively. The gene expression levels of MAP4 were upregulated in various types of HCC cell lines compared to human normal liver tissues (Figure 2A). In addition, MAP4 expression was significantly upregulated in human liver tumor tissues compared to their matched adjacent non-tumor liver tissues in HBV-HCC patients in the NTUH cohort (Figure 2B and C). Notably, 91.1% of samples in the NTUH cohort exhibited MAP4 expression levels in tumor tissues that were more than twice those in adjacent non-tumor tissues. These findings suggest that MAP4 overexpression in human liver tumors may contribute to HCC progression.
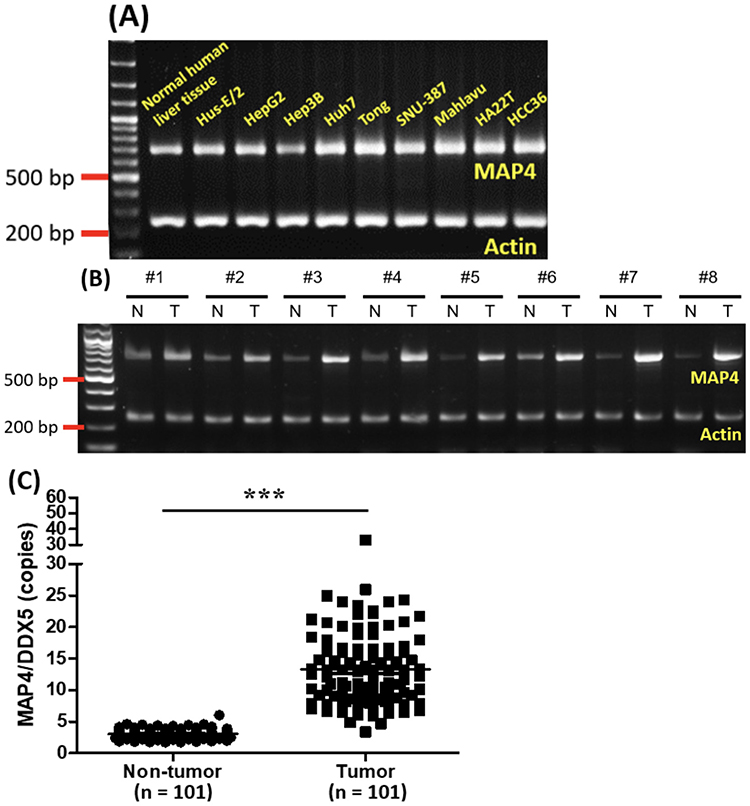 |
Figure 2 MAP4 gene expression in HCC cell lines and human liver tissues. (A) MAP4 gene expression in human normal liver tissue, immortalized hepatic cell line, and HCC cell lines. (B) Comparison of the expression levels of MAP4 in 8 randomly selected pairs of tumor and adjacent non-tumor tissues from HBV-HCC patients in the NTUH cohort. (C) Comparison of the gene expression levels of MAP4 in 101 paired liver tumor and adjacent non-tumor tissues from HBV-HCC patients using qRT-PCR. The expression level of MAP4 was normalized to the internal control DDX5. Results are presented as mean ±SD. Statistical significance was determined using the Wilcoxon signed-rank test (***p < 0.0001). Abbreviations: bp, base pairs; DDX5, DEAD-box helicase 5; HBV-HCC, Hepatitis B virus-associated hepatocellular carcinoma; HCC, hepatocellular carcinoma; MAP4, microtubule-associated protein 4; NTUH, National Taiwan University Hospital; n, number of patients; N, adjacent non-tumor liver tissues; ±, plus-minus symbol; qRT-PCR, quantitative reverse transcription polymerase chain reaction; SD, standard deviation; T, tumor liver tissues. |
MAP4 Overexpression in Liver Tumor Tissues Correlates with Early Recurrence in Patients with HBV-HCC
To focus on whether MAP4 overexpression in tumor tissues correlates with early recurrence in patients with HBV-HCC after hepatic resection, we sought to determine the MAP4 expression threshold in liver tumor tissues that best predicts early recurrence in the NTUH cohort. Receiver Operating Characteristic (ROC) curve analysis was employed to evaluate the predictive ability of MAP4 expression levels based on the data from the entire NTUH discovery cohort (n = 101). The optimal threshold was calculated using the maximum Youden’s index, yielding a cut-off value of 16.1 MAP4 copies per DDX5 copy. Based on this cut-off, patients were categorized into high- and low-expression groups for further clinical association analysis. High MAP4 expression in liver tumor tissues showed a significant positive association with the presence of multiple tumors (p = 0.042), and a trend toward association with satellite nodules (p = 0.082), and early recurrence (p = 0.074), although the latter two did not reach statistical significance likely due to limited sample size (Table 2). We further examined the impact of MAP4 expression on recurrence timing. In the NTUH cohort, the cumulative early recurrence rate in the high-expression group was nearly 40% within the first year after liver resection, compared to approximately 20% in the low-expression group, indicating a statistically significant difference (HR = 2.53, 95% CI = 1.04–6.19, p = 0.042) (Figure 3A). Furthermore, high MAP4 expression was significantly negatively correlated with recurrence-free survival (HR = 2.38, 95% CI = 1.12–5.06, p = 0.023) and overall survival (HR = 3.42, 95% CI = 1.27–9.21, p = 0.0152) of patients with HBV-HCC (Figure 3B and C).
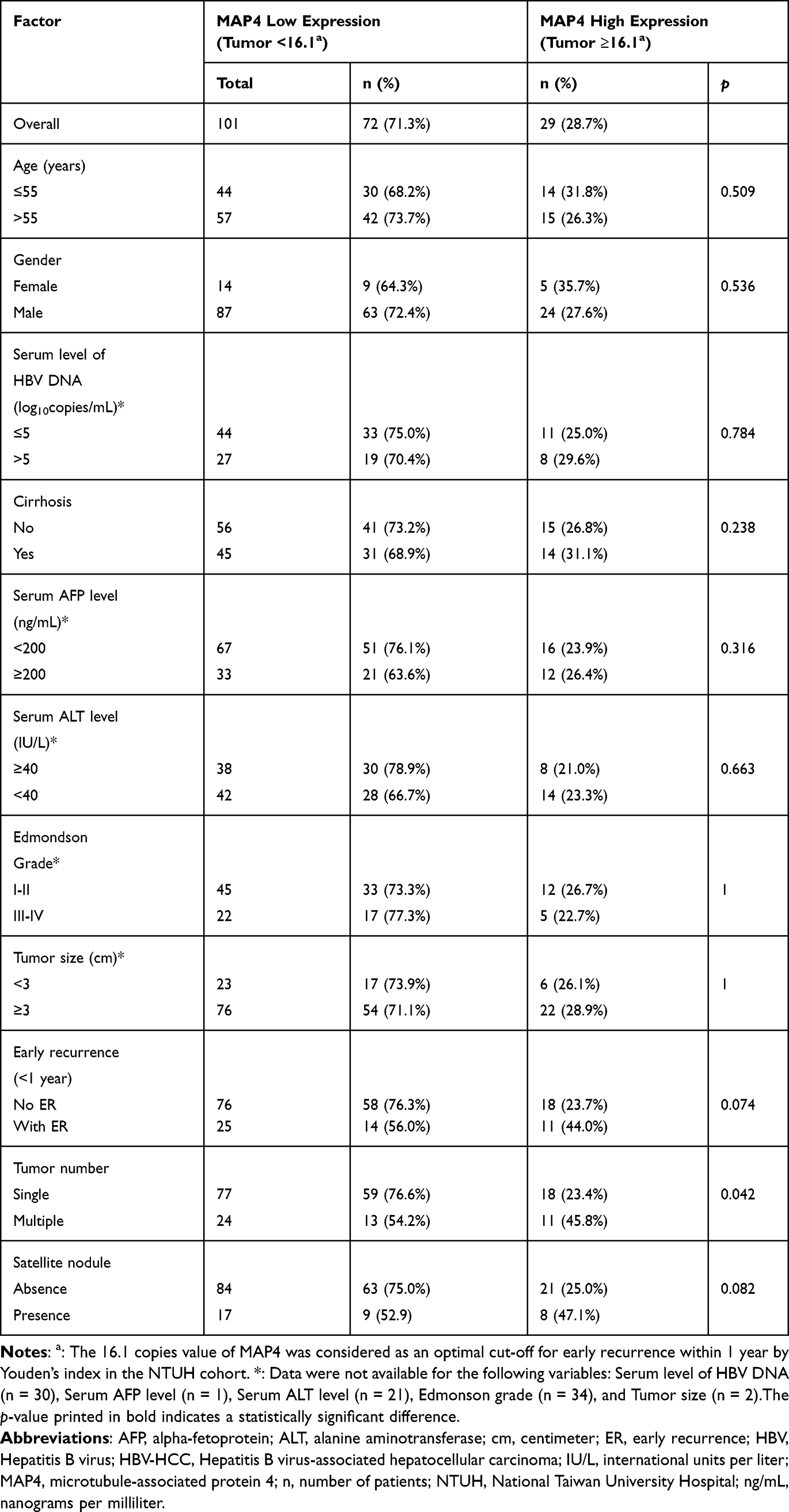 |
Table 2 Association Between MAP4 Overexpression and Clinicopathological Parameters of 101 Patients with HBV-HCC |
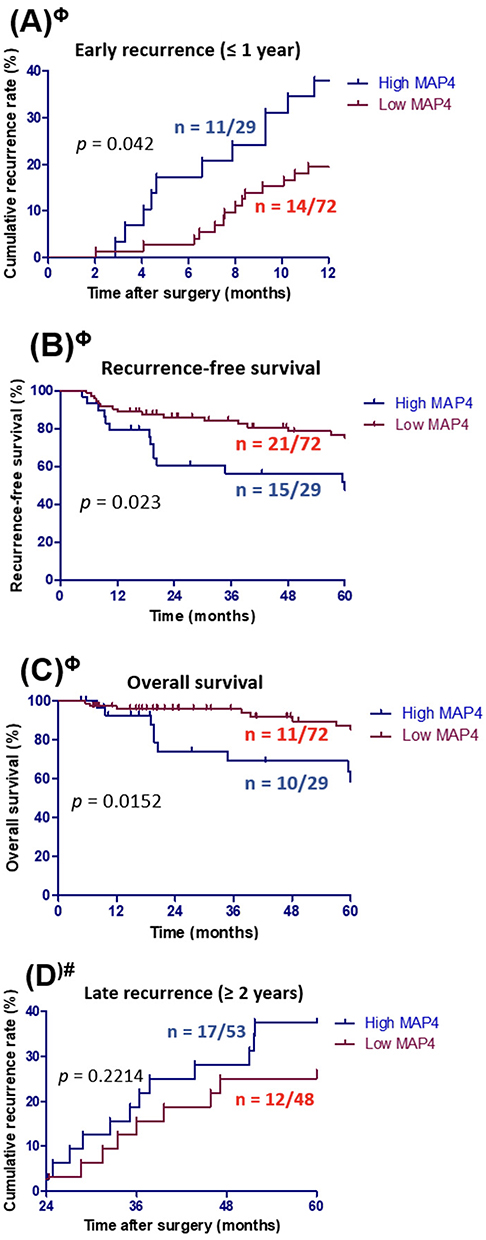 |
Figure 3 The correlation between MAP4 expression in liver tumor tissues and (A) cumulative early recurrence, (B) recurrence-free survival, (C) overall survival, and (D) late recurrence of HBV-HCC following curative hepatic resection in the NTUH cohort. The optimal MAP4 cut-off values for dividing high and low expression groups were determined separately for predicting early recurrence (Φ) and late recurrence (#) using Youden’s index in the NTUH cohort. The Log rank test was performed to calculate the p-value. Abbreviations: HBV-HCC, Hepatitis B virus-associated hepatocellular carcinoma; MAP4, microtubule-associated protein 4; NTUH, National Taiwan University Hospital; n, number of patients. |
To assess whether MAP4 is also associated with late recurrence (occurring after 2 years), we applied the same ROC-based approach to identify an optimal threshold for predicting late recurrence, which was determined to be 11.6 MAP4 copies per DDX5 copy. However, when applying this threshold, no significant association was found between high MAP4 expression and late recurrence in the NTUH cohort, although a slight trend toward increased risk was observed (HR = 1.57, 95% CI = 0.76–3.27, p = 0.221) (Figure 3D).
Taken together, these findings suggest that high MAP4 expression in liver tumor tissues is more closely associated with metastasis-related early recurrence rather than late recurrence of HCC. Furthermore, elevated MAP4 expression is correlated with poorer recurrence-free survival and overall survival, indicating its potential prognostic value for the patient population.
Clinical Factors Associated with Early Recurrence in HBV-HCC Patients After Curative Hepatic Resection
The Log rank test was used to identify clinicopathological factors significantly associated with tumor early recurrence within 1 year, including MAP4 expression in liver tumor tissues. Univariate analysis showed that elevated AFP, large tumor size, multiple tumor numbers, presence of satellite nodules, and high expression of MAP4 in the tumor (≥16.1 MAP4 copies per DDX5 copy) were significantly associated with early recurrence (p = 0.001, 0.012, 0.018, 0.001, and 0.042, respectively; Table 3). While subsequently multivariate analysis incorporating these five factors identified high serum AFP levels (HR = 2.924, 95% CI = 1.27–6.75, p = 0.012) and larger tumor size (HR = 9.404, 95% CI = 1.27–69.77, p = 0.028) as independent risk factors for early recurrence, high MAP4 expression did not reach statistical significance in this analysis, possibly due to the small sample size. However, the observed trend suggests that MAP4 may play a role in early recurrence and warrants further investigation, particularly in larger cohorts.
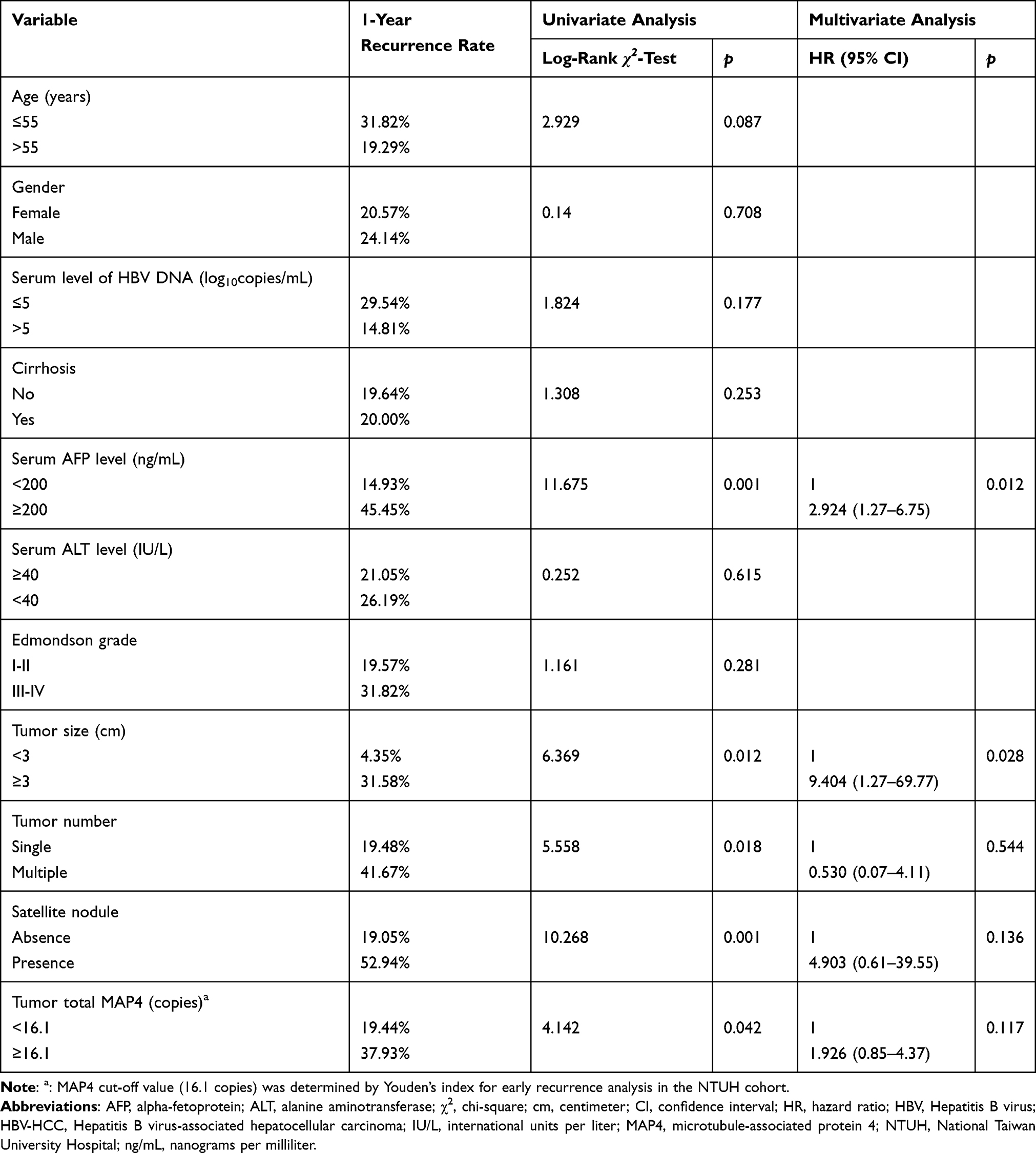 |
Table 3 Univariate and Multivariate Analysis of Factors Possibly Associated with Early Recurrence in Patients with HBV-HCC After Tumor Resection |
Independent Cohort Confirms MAP4-Associated Clinical Outcomes Observed in the NTUH Cohort
To support the generalization of the MAP4 clinical findings observed in the NTUH cohort, we utilized an independent study cohort as an external validation dataset. We obtained the gene expression profile of liver tissues (NCBI GEO accession number: GSE14520) and clinical data from HBV-HCC patients who underwent hepatic resection were obtained from Fudan University, Shanghai. The same analytical strategy used for the NTUH cohort was applied to this dataset. Consistent with the NTUH findings, MAP4 expression was significantly upregulated in liver tumor tissues compared to paired adjacent non-tumor tissues in the validation cohort (Figure 4A). Patients were stratified into high- and low-MAP4 expression groups based on an optimal cut-off value for early recurrence determined using Youden’s index. This threshold differed from that of the NTUH cohort due to the use of different quantification platforms, RT-qPCR in the NTUH cohort and microarray analysis in the Fudan cohort. In alignment with the NTUH results, high expression of MAP4 in tumor tissues was significantly correlated with a higher cumulative rate of early recurrence within 1 year (HR = 2.88, 95% CI = 1.69–4.89, p < 0.0001) (Figure 4B), as well as with reduced recurrence-free survival (HR = 1.70, 95% CI = 1.13–2.55, p = 0.0105) and overall survival (HR = 1.66, 95% CI = 1.06–2.59, p = 0.0273) (Figure 4C and D). Moreover, similar to the NTUH cohort, high MAP4 expression did not show a significant association with late recurrence (HR = 1.84, 95% CI = 0.77–4.38, p = 0.1667) (Figure 4E).
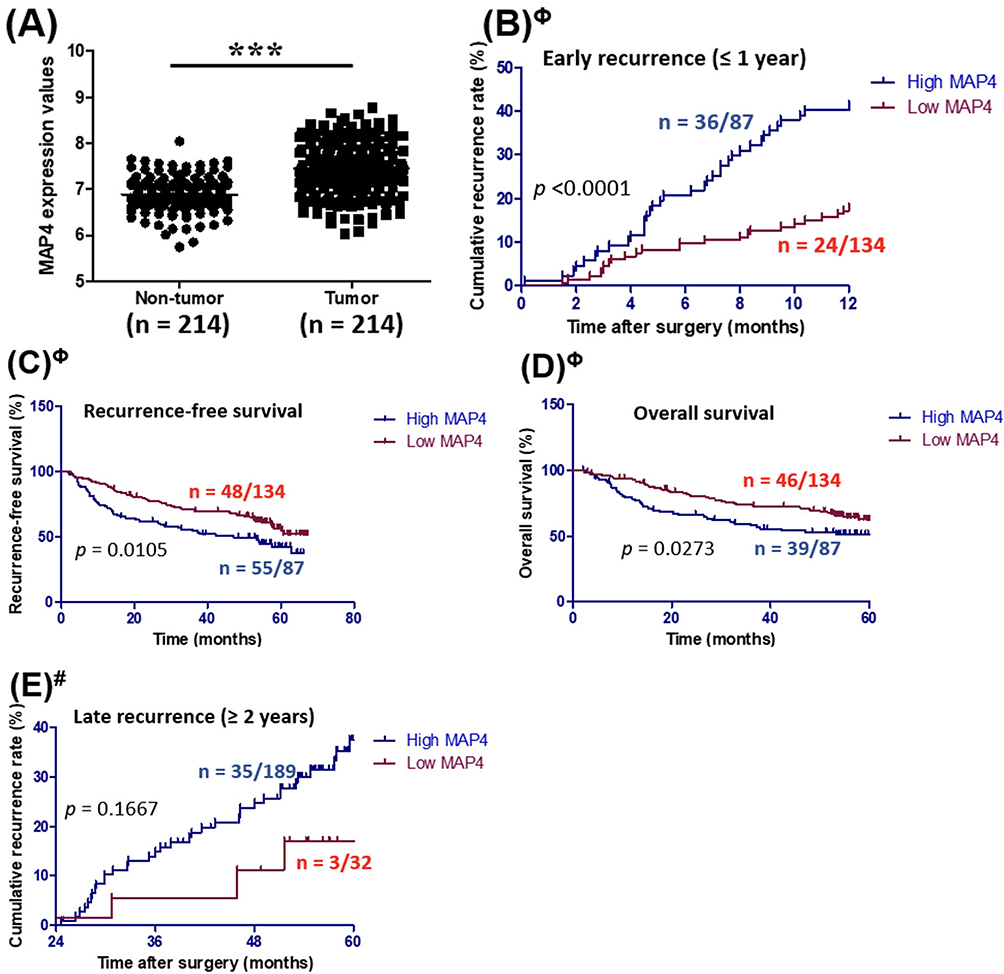 |
Figure 4 (A) MAP4 gene expression in liver tumor tissues and its correlation with (B) cumulative early recurrence, (C) recurrence-free survival, (D) overall survival, and (E) late recurrence in the validation cohort of HBV-HCC patients from Fudan University, Shanghai. The optimal MAP4 cut-off values for classifying high and low expression groups were determined separately for predicting early recurrence (Φ) and late recurrence (#) using Youden’s index in the Fudan University cohort. Abbreviations: HBV-HCC, Hepatitis B virus-associated hepatocellular carcinoma; MAP4, microtubule-associated protein 4; n, number of patients. |
Collectively, these results independently validate the association between elevated MAP4 expression with early, but not late, recurrence and poor survival outcomes in HBV-HCC patients following curative hepatic resection.
Discussion
HCC patients often experience recurrence after surgery, which contributes to poor prognosis, with early recurrence being a major factor affecting postoperative survival.23 Understanding tumor molecular characteristics and identifying critical factors contributing to early recurrence enables improved risk stratification, earlier intervention, more frequent surveillance, deeper insight into underlying molecular mechanisms, and enhanced management of HCC.24,25 In this retrospective study, we found that MAP4 is frequently overexpressed in tumor tissues and is significantly associated with early recurrence within 1 year and poor prognosis after surgery in patients with HBV-HCC. In practice, assessing MAP4 expression in resected tumors may help clinicians to identify patients at high risk for early recurrence, who would benefit from more intensive postoperative surveillance during the critical first year. Furthermore, such patients might be prioritized for clinical trials evaluating adjuvant therapies aimed at reducing recurrence risk.26 These clinical management strategies may improve the survival outcomes associated with early recurrence, as MAP4 expression in tumors provides important insights into aggressiveness and recurrence risk.
Previous studies have shown that metastasis-related early recurrence is primarily driven by intrahepatic dissemination of the primary tumor, whereas late recurrence is often the result of de novo tumor formation associated with underlying chronic liver disease.27 In this context, our findings that MAP4 overexpression is significantly associated with early, but not late, recurrence in patients with HBV-HCC suggest a potential mechanistic role in promoting intrahepatic metastasis. Supporting this notion, in vitro experimental studies have demonstrated that MAP4 knockdown suppresses the migratory and invasive capacities of HCC cell lines via the inhibition of the epithelial-mesenchymal transition (EMT) markers.19 In addition, MAP4 mainly regulates microtubule dynamics through its post-transcriptional and post-translational modifications, and further has an impact on cell migration and invasion.18,28–30 Microtubule reorganization facilitates cancer progression by supporting processes like mitosis and migration, which contribute to tumor growth and metastasis, respectively.31,32 Together, these findings provide mechanistic support for the clinical observation that MAP4 overexpression is associated with metastasis-related early recurrence in HBV-HCC patients, likely through its regulatory role in microtubule dynamics and promotion of metastatic potential.
Our previous study demonstrated that expression of the MTA1dE4 splice variant is correlated with more aggressive tumor behavior, including enhanced migratory and invasive abilities, compared to MTA1-FL.10 A specific interaction between MTA1dE4 and MAP4, which may mediate microtubule remodeling, could potentially facilitate to the MTA1dE4-mediated increased aggressiveness by promoting tumor cell motility and invasion. Further mechanistic studies are needed to elucidate the functional relevance of this interaction. In particular, it will be important to determine whether the MTA1dE4- MAP4 interaction plays a crucial role in promoting HCC progression and recurrence, and whether these two proteins reciprocally regulate each other’s expression or activity.
Despite the promising clinical implications, there are several limitations to this study. Firstly, the retrospective design and relatively small sample size. Although our clinical findings were validated using an external independent cohort with robust statistical power (power = 0.967) compared to the NTUH cohort (power = 0.427), a prospective study would provide stronger evidence of the clinical significance of MAP4 in HBV-HCC and its utility in predicting early recurrence. Additionally, while the positive association between MAP4 overexpression and early recurrence was validated in two independent cohorts, the use of different platforms (RT-qPCR vs. microarray) yielded distinct optimal cut-off values for MAP4 expression. As a result, the RT-qPCR-derived cut-off value of 11.6 MAP4 copies per DDX5, identified in the NTUH cohort, may not be universally transferable to other HBV-HCC patient populations for predicting early recurrence following surgery. This limitation is particularly evident when comparing results across different quantification platforms, where varying sensitivities and normalization methods can lead to inconsistent thresholds. To address this, future efforts should focus on translating these mRNA-based findings into a standardized immunohistochemistry (IHC) scoring system. Unlike transcript-based assays, protein-level IHC is more readily integrated into routine pathology workflows and offers better potential for cross-center standardization. Consequently, validating such IHC-based assays in larger, multi-center cohorts will be critical to establishing a broadly applicable clinical threshold for MAP4. Finally, although our data support a mechanistic role of MAP4 in promoting metastasis-related early recurrence, additional research is required to delineate its interactions with other cellular pathways and to fully elucidate its contribution to HCC progression. Beyond its involvement in regulating EMT markers and enhancing cell migration and invasion,19 MAP4 has also been shown to influence endothelial cell migration and proliferation through post-translational modifications,11 suggesting a broader role in cancer metastasis. However, the exact mechanisms by which MAP4 HCC progression remains elusive and represents an important area for future investigation.
Conclusions
In summary, our research demonstrated that MAP4 overexpression in liver tumor tissues is significantly correlated with early recurrence and poorer survival outcomes in patients with HBV-HCC following curative hepatic resection. These findings suggest that assessment of MAP4 expression may serve as a useful biological indicator for risk stratification to identify patients who may benefit from more intensive post-operative surveillance, particularly during the first year after surgery. Further studies are warranted to validate its clinical utility and to elucidate underlying molecular mechanisms.
Abbreviations
AFP, alpha-fetoprotein; CT, computed tomography; DDX5, dead-box helicase 5; EMT, epithelial-mesenchymal transition; HBV-HCC, hepatitis B virus-associated hepatocellular carcinoma; IP-MS, immunoprecipitation-mass spectrometry; MAP4, microtubule-associated protein 4; MTA1, metastatic tumor antigen 1; MRI, magnetic resonance imaging; NTUH, National Taiwan University Hospital; RT-qPCR, quantitative reverse transcription-polymerase chain reaction; ROC, receiver operating characteristic.
Data Sharing Statement
The data that support the findings of this study are available upon reasonable request from the corresponding author, Hui-Lin Wu.
Ethics Statements
The present retrospective study was approved by the Institutional Review Board of National Taiwan University Hospital (IRB No. 202307113RINC). Surgical specimens and clinical data were originally collected under a previous IRB-approved protocol (IRB No. 201512213RINA). Before surgery, all patients provided written informed consent permitting future research use of their resected tissue and associated clinical information (“tissue reuse” consent). In the current study, we used only de-identified data and archived specimens obtained under IRB No. 201512213RINA, in accordance with the Declaration of Helsinki. No additional interventions or contact with patients were required for this analysis.
Acknowledgments
We thank Mr. Chih-Chiang Wang, Dr. Shih-Chi Wang, Mr. Ke-Ji Lin and Ms. Xiang-Qing Lai for their excellent technical assistance. We are grateful to Dr. Cheng Huang for kindly providing the HuS-E/2 cDNA.
Funding
This work was supported by National Taiwan University Hospital (project number: NTUH.113-S0012).
Disclosure
The authors declare that they have no conflicts of interest to disclose.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–14. doi:10.3322/caac.21492
2. Conci S, Cipriani F, Donadon M, et al. Hepatectomy for Metabolic Associated Fatty Liver Disease (MAFLD) related HCC: propensity case-matched analysis with viral- and alcohol-related HCC. Eur J Surg Oncol. 2022;48(1):103–112. doi:10.1016/j.ejso.2021.07.015
3. Nevola R, Ruocco R, Criscuolo L, et al. Predictors of early and late hepatocellular carcinoma recurrence. World J Gastroenterol. 2023;29(8):1243–1260. doi:10.3748/wjg.v29.i8.1243
4. Imamura H, Matsuyama Y, Tanaka E, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003;38(2):200–207. doi:10.1016/s0168-8278(02)00360-4
5. Lu LC, Hsu CH, Hsu C, Cheng AL. Tumor heterogeneity in hepatocellular carcinoma: facing the challenges. Liver Cancer. 2016;5(2):128–138. doi:10.1159/000367754
6. Lee M, Chang Y, Oh S, et al. Assessment of the surveillance interval at 1 year after curative treatment in hepatocellular carcinoma: risk stratification. Gut Liver. 2018;12;5:571–582.
7. Chan AWH, Zhong J, Berhane S, et al. Development of pre and post-operative models to predict early recurrence of hepatocellular carcinoma after surgical resection. J Hepatol. 2018;69(6):1284–1293. doi:10.1016/j.jhep.2018.08.027
8. Safri F, Nguyen R, Zerehpooshnesfchi S, George J, Qiao L. Heterogeneity of hepatocellular carcinoma: from mechanisms to clinical implications. Cancer Gene Ther. 2024;31(8):1105–1112. doi:10.1038/s41417-024-00764-w
9. Wu WJ, Wang J, Chen F, et al. Exploration of heterogeneity and recurrence signatures in hepatocellular carcinoma. Mol Oncol. 2025; 19;(8):2388–411.
10. Li YT, Wu HL, Kao JH, et al. Expression of metastatic tumor antigen 1 splice variant correlates with early recurrence and aggressive features of hepatitis b virus-associated hepatocellular carcinoma. Hepatology. 2019;70(1):184–197. doi:10.1002/hep.30581
11. Zhang J, Li L, Zhang Q, et al. Phosphorylation of microtubule- associated protein 4 promotes hypoxic endothelial cell migration and proliferation. Front Pharmacol. 2019;10:368. doi:10.3389/fphar.2019.00368
12. Nguyen HL, Gruber D, Bulinski JC. Microtubule-associated protein 4 (MAP4) regulates assembly, protomer-polymer partitioning and synthesis of tubulin in cultured cells. J Cell Sci. 1999;112:1813–1824. doi:10.1242/jcs.112.12.1813
13. Ookata K, Hisanaga S, Bulinski JC, et al. Cyclin B interaction with microtubule-associated protein 4 (MAP4) targets p34cdc2 kinase to microtubules and is a potential regulator of M-phase microtubule dynamics. J Cell Biol. 1995;128(5):849–862. doi:10.1083/jcb.128.5.849
14. Matsushima K, Tokuraku K, Hasan MR, Kotani S. Microtubule-associated protein 4 binds to actin filaments and modulates their properties. J Biochem. 2012;151(1):99–108. doi:10.1093/jb/mvr119
15. Mangaonkar S, Nath S, Chatterji BP. Microtubule dynamics in cancer metastasis: harnessing the underappreciated potential for therapeutic interventions. Pharmacol Ther. 2024;263:108726. doi:10.1016/j.pharmthera.2024.108726
16. Legatova A, Pelantova M, Rosel D, Brabek J, Skarkova A. The emerging role of microtubules in invasion plasticity. Front Oncol. 2023;13:1118171. doi:10.3389/fonc.2023.1118171
17. Jiang YY, Shang L, Shi ZZ, et al. Microtubule-associated protein 4 is an important regulator of cell invasion/migration and a potential therapeutic target in esophageal squamous cell carcinoma. Oncogene. 2016;35(37):4846–4856
18. Xia X, Ge Y, Ge F, et al. MAP4 acts as an oncogene and prognostic marker and affects radioresistance by mediating epithelial-mesenchymal transition in lung adenocarcinoma. J Cancer Res Clin Oncol. 2024;150(2):88. doi:10.1007/s00432-024-05614-8
19. Hu P, Zong B, Chen Q, et al. Microtubule-associated protein 4 promotes epithelial mesenchymal transition in hepatocellular cancer cells via regulating GSK3beta/beta-catenin pathway. Heliyon. 2023;9(3):e14309. doi:10.1016/j.heliyon.2023.e14309
20. Nakabayashi H, Taketa K, Miyano K, Yamane T, Sato J. Growth of human hepatoma cells lines with differentiated functions in chemically defined medium. Cancer Res. 1982;42(9):3858–3863.
21. Aly HH, Watashi K, Hijikata M, et al. Serum-derived hepatitis C virus infectivity in interferon regulatory factor-7-suppressed human primary hepatocytes. J Hepatol. 2007;46(1):26–36. doi:10.1016/j.jhep.2006.08.018
22. Roessler S, Jia HL, Budhu A, et al. A unique metastasis gene signature enables prediction of tumor relapse in early-stage hepatocellular carcinoma patients. Cancer Res. 2010;70;24:10202–10212.
23. Abdelhamed W, El-Kassas M. Hepatocellular carcinoma recurrence: predictors and management. Liver Res. 2023;7(4):321–332. doi:10.1016/j.livres.2023.11.004
24. Liu Z, Zhang S. Tumor characterization and stratification by integrated molecular profiles reveals essential pan-cancer features. BMC Genomics. 2015;16(1):503.
25. Wheeler DA, Takebe N, Hinoue T, et al. Molecular features of cancers exhibiting exceptional responses to treatment. Cancer Cell. 2021;39;1:38–53e7.
26. D’Alessio A, Rimassa L. The long and winding road: adjuvant therapy for early-stage hepatocellular carcinoma. Med. 2024;5(1):7–9.
27. Marasco G, Colecchia A, Colli A, et al. Role of liver and spleen stiffness in predicting the recurrence of hepatocellular carcinoma after resection. J Hepatol. 2019;70(3):440–448. doi:10.1016/j.jhep.2018.10.022
28. Ou Y, Zheng X, Gao Y, et al. Activation of cyclic AMP/PKA pathway inhibits bladder cancer cell invasion by targeting MAP4-dependent microtubule dynamics. Urol Oncol. 2014;32(1):47e21–8. doi:10.1016/j.urolonc.2013.06.017
29. Chapin SJ, Bulinski JC. Non-neuronal 210 x 10(3) Mr microtubule-associated protein (MAP4) contains a domain homologous to the microtubule-binding domains of neuronal MAP2 and tau. J Cell Sci. 1991;98:27–36. doi:10.1242/jcs.98.1.27
30. Nguyen HL, Chari S, Gruber D, Lue CM, Chapin SJ, Bulinski JC. Overexpression of full- or partial-length MAP4 stabilizes microtubules and alters cell growth. J Cell Sci. 1997;110:281–294. doi:10.1242/jcs.110.2.281
31. Hashi Y, Kawai G, Kotani S. Microtubule-associated protein (MAP) 4 interacts with microtubules in an intrinsically disordered manner. Biosci Biotechnol Biochem. 2014;78(11):1864–1870. doi:10.1080/09168451.2014.940836
32. Wattanathamsan O, Pongrakhananon V. Emerging role of microtubule-associated proteins on cancer metastasis. Front Pharmacol. 2022;13:935493. doi:10.3389/fphar.2022.935493
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.