Back to Journals » Open Access Emergency Medicine » Volume 16
Microsurgical Digits Replantation in Resource-Limited Setting: A Retrospective Study
Authors Altam A, Obadiel Y ![]() , Alazaiza RS
, Alazaiza RS ![]() , Alshujaa MA, Alhajami F
, Alshujaa MA, Alhajami F ![]() , Ahmed F
, Ahmed F ![]() , Al-Naggar AM
, Al-Naggar AM ![]() , Albushtra AM
, Albushtra AM ![]() , Badheeb M
, Badheeb M ![]()
Received 26 October 2023
Accepted for publication 26 December 2023
Published 3 January 2024 Volume 2024:16 Pages 1—13
DOI https://doi.org/10.2147/OAEM.S443219
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Abdulfattah Altam,1 Yasser Obadiel,2 Rami Salim Alazaiza,1 Mohamed Ali Alshujaa,3 Faris Alhajami,1 Faisal Ahmed,4 Abdullah Mohammed Al-Naggar,5 Ahmed Mohamed Albushtra,6 Mohamed Badheeb7
1Department of General Surgery, School of Medicine, 21 September University, Sana’a, Yemen; 2Department of General Surgery, School of Medicine, Sana’a University, Sana’a, Yemen; 3Department of General Surgery, School of Medicine, Thamar University, Dhamar, Yemen; 4Department of Urology, School of Medicine, Ibb University, Ibb, Yemen; 5Department of Anesthesiology, Faculty of Medicine, Sana’a University, Sana’a, Yemen; 6Department of Orthopedics, School of Medicine, Ibb University, Ibb, Yemen; 7Department of Internal Medicine, Yale New-Haven Health/Bridgeport Hospital, Bridgeport, CT, USA
Correspondence: Faisal Ahmed, Department of Urology, School of Medicine, Ibb University, Ibb, Yemen, Tel/Fax +967 4428950, Email [email protected]
Background: This article aims to share our experiences with microsurgical finger replantation in a resource-limited setting.
Methods: This multi-institutional, retrospective study included 21 cases of finger amputation that underwent microsurgical replantation, within 7 years period. Patient demographics, preoperative assessments, surgical approaches, and outcomes were documented and analyzed. A univariate analysis was performed to obtain factors associated with digit reimplantation failure.
Results: Out of 21 cases included, 8 (38.1%) had complete amputations and 13 (61.9%) had incomplete amputations. Crush injuries accounted for the majority (71.4%). On average, 2.2 ± 1.1 digits were affected, with the ring finger being the most commonly injured (71.4%). The mean operative time was 121.5 ± 26.8 minutes. The success rate of digit replantation was 76.2%. During a mean follow-up of 14.3 ± 3.7 months, 85.7% of successfully replanted digits considered their replantation results satisfactory. The majority of replanted digits demonstrated active and effective holding and grasping abilities without pain or instability (76.2%). Replantation failure was associated with a higher number of affected digits (p < 0.001), longer operative time (p = 0.004), complete avulsion (p = 0.003), current smoking (p = 0.025), diabetes (p = 0.006), hypertension (p = 0.047), procedure difficulty score (p= 0.004), and occurrence of complications (p < 0.001).
Conclusion: Microsurgical finger replantation can yield favorable outcomes and acceptable survival rates, even within resource-limited settings. However, this procedure requires specialized equipment and personnel that may not be available at all institutions. Influential factors in digit replantation failure, include an increased number of damaged digits, extended operative duration, complete avulsion, current smoking, diabetes, hypertension, procedure difficulty score, and postoperative complications occurrence.
Keywords: microsurgery, digital replantation, amputation, resource-limited setting
Introduction
The first surgically acceptable digit replantation was performed in the mid-1960s.1 Since then, various surgical approaches and techniques have been implemented to improve overall outcomes.2 Indeed, the rapid expansion of surgical interventions, along with advancements in healthcare innovation and accessibility, has made microsurgical replantation a routine procedure in various healthcare centers. However, controversies surrounding digit replantation persist, with significant variability observed among countries and institutions.3 Recently, there has been a noted decline in surgical replantation despite an increase in cases, as stricter patient selection criteria are being applied.4,5 This rationale can be reasonably justified by considering the fundamental objective of replantation, which is to achieve the restoration of both the structure and function of the affected digit. In this context, the potential benefits of replantation must outweigh the associated risks in order to justify the pursuit of this complex surgical intervention.6
Indeed, successful replantation may be an optimal and desirable outcome for every patient; however, achieving this outcome is contingent upon proper patient selection. In a large study conducted by Shaterian et al, the overall survival of replanted digits varied significantly (48–97%) among the included studies.7 Numerous factors have been identified as influential in determining the overall outcome, including intrinsic factors related to the affected digit, injury mechanics, comorbidities, and duration of vascular compromise, as well as extrinsic factors such as surgical experience, techniques, and approaches.8,9
Many studies describe the overall survival rates of digital replantation across different digits and levels, as well as functional results using various categorization systems. However, there is a discrepancy between subjective satisfaction with the procedure and quantitative evaluations of finger range of motion and grip strength. Quantifying the true benefit of replantation for the patient is challenging and may be determined by their ability to cope with the trauma and return to a regular life involving everyday activities, employment, and leisure pursuits.10
Microsurgical replantation is still in its early stages in low-income nations. This is primarily due to inadequate healthcare funding, a lack of skilled personnel, and the absence of an academic curriculum focused on this sophisticated surgical procedure. The present study aims to document our experiences with microsurgical finger replantation in our low-resource setting. Based on our current knowledge, this study represents the initial investigation on microsurgical finger replantation conducted in Yemen.
Materials and Methods
Study design: In this retrospective study, we evaluated 21 cases of amputated digits that underwent microsurgical replantation in 21 academic hospitals over a period of seven years (Jun, 2015-May 2022). Ethical approval for the study was obtained from the ethics committees of 21 September University, Sana´a, Yemen, (ID: S-98-H-02-F22), and we conducted the study in accordance with the Helsinki Declaration. We obtained informed consent from the patients and/or their families to participate in the study. All eligible participants or legal guardian of patients under 18 years of age provided informed consent for participation and publication of the case details and images.
Inclusion criteria: The research comprised all patients who had traumatic finger amputations (complete or partial) and underwent microsurgical replantation.
Exclusion criteria: Patients with prior attempted replantation(s), extensive multi-level injuries, and crush injuries, as well as those with mental or physical instability, were excluded.
Surgical procedure: Upon the initial encounter, patients with an amputated digit(s) underwent assessment and evaluation for possible replantation. Factors considered included injury mechanics, duration of vascular compromise (vascular compromise lasting ≥12 hours was considered vascularly unviable), as well as the presence of concomitant life-threatening or distracting injuries that rendered patients ineligible for replantation. All cases were performed under general anesthesia, allowing for thorough debridement of the affected digits and precise identification of vascular and nerve supplies, as well as tendons and digit stumps. Then, intramedullary Kirschner wires were used to remove an estimated 1–2 cm of bone from both ends of the digit, which were then repaired. Intraosseous cerclages or two crossed Kirschner wires were employed for stabilization. To minimize tendon adhesion and prevent subsequent post-operative stiffness, the intrasynovial superficial flexor tendons were dissected between the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS). Two approaches described by Kaplan et al and Verdan et al were used for the repair of the deep flexor and extensor tendons.11,12 The vascular restoration was achieved through meticulous tension-free anastomoses, with careful assessment for any intimal injuries or vascular tortuosity that could potentially lead to thrombotic events. In cases where microvascular anastomoses were under strain, vein transplants utilizing veins of similar diameter were utilized. Nerve bundles were meticulously aligned, and if necessary, trimmed, followed by meticulous end-to-end coaptation. A microsurgical technique employing Nylon 9/0 sutures was employed in our cases. Thereafter, the skin was closed loosely and drained, and the involved limb was placed on pronation while elevated and wrapped in a non-compressive plaster splint for a period of 10–15 days.
Postoperative Evaluation
Patients were initially evaluated on an hourly basis, with close monitoring of the involved digits for any color or temperature alterations. Additionally, frequent assessments of pulses and dressings were performed. Oral intake was withheld on the first post-operative day, and patients were administered broad-spectrum antibiotics, typically Cefotaxime at a dosage of 3 g daily for a duration of 7 days unless an alternative regimen was recommended. Pain control was achieved through the administration of Paracetamol and Opioids, with careful consideration to avoid any vasoconstrictive effects of pain management. Moreover, a low-dose aspirin (81 mg daily for 10 days) and low-molecular-weight heparin (3000 IU daily for 5 days) were prescribed. Additional therapeutic interventions were tailored to each patient’s specific needs, in consultation with the medical team. On the ninth postoperative day, a structured physical rehabilitation program was initiated and continued daily until the third or fourth postoperative month.
Data Gathering and Study Outcome
Data regarding age, gender, cause of injuries, operative findings, procedure difficulty score, postoperative complications, total active range of motion, and disabilities were gathered and analyzed. The primary outcome was digit survival, postoperative complications, active range of motion, and disabilities while the secondary outcome was factors associated with digit replantation failure.
Definition
Amputations were classified as complete when the proximal stump was completely separated. In contrast, incomplete amputations were identified by the presence of distal digit attachment to a musculoskeletal structure (such as a tendon), nerve, or cutaneous remnant. The viability of incomplete amputations was assessed based on the presence of vascular compromise that necessitated microsurgical vascular anastomoses (Figure 1).
 |
Figure 1 Index and middle fingers amputation and devascularization (A). Bone fixation by K-wires (B). Microvascular anastomosis, two digital arteries, one dorsal vein, and two digital nerves for each finger (C). Post-operative finger appearance (D), on the third postoperative day (E). Showing accepted finger grasp function (F). |
Digit replantation referred to the restoration of served digit musculoskeletal and neurovascular attachments. The replanted or revascularized digit deemed viable on the basis of the functional outcome and vascular patency through a 1-month period following the procedure.
Procedure Difficulty Score
We integrated a scoring system by Yoon et al13 to predict digit replantation difficulty. This score included the type of amputation (complete or partial), injury nature (avulsion or crush), the number of involved digits, active smoking, and whether the procedures involved replantation or revascularization.
To define the functional outcomes, patient satisfaction, digit mobility (motor functions), and digit sensitivity (sensory functions) were assessed. The total active motion (TAM) of the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints were compared to the uninjured counterpart (TAM = flexion [MCP + PIP + DIP] - extension deficit [MCP + PIP + DIP]), while sensitivity recovery was assessed using the two-point discrimination test.
Level I (excellent and good) indicated patients’ high satisfaction with the replanted digits, achieving a 60% TAM compared to healthy counterparts, along with a 1 cm two-point discrimination. These patients reported no discomfort or paraesthesia. Level II (fair) denoted patients’ contentment with the replanted fingers, achieving a TAM of 30–60% and two-point discrimination of 2 cm. They also experienced no discomfort or paraesthesia. Level III (poor) represented patient dissatisfaction due to ankylosis or loss of function, with a 30% lower TAM and a 2 cm lower two-point discrimination than healthy comparisons.14
Statistical Analysis
Descriptive statistics, including mean and standard deviation, were used to summarize the quantitative data, while frequencies and percentages were employed for qualitative variables. The normality of the data was assessed using the Smirnov-Kolmogorov test. To compare quantitative variables, an independent samples T-test or Mann–Whitney test was applied, depending on the normality assumption. For qualitative variables, Chi-square or Fisher’s exact test was used. The threshold for statistical significance was set at p < 0.05. All statistical analyses were performed using IBM SPSS version 22 software (IBM Corp., Armonk, New York).
Results
In Table 1, we summarized the baseline demographics of patients with finger microsurgical replantation. The main age of patients was 24.2 ±13.3 years (Range 3–50 years) and most of them were male (71.4%). Eight (38.1%) cases had complete amputations and 13 (61.9%) cases had incomplete amputations. Crush injuries were the main mechanism for amputations (71.4%). The comorbidities were smoking, hypertension, and diabetes in 7 (33.3%), 8 (38.1%), and 9 (42.9%) cases respectively. The time to hospital presentation was 6.6 ±1.8 hours (Range 4.0–10.0 hours). The right hand was predominantly affected by 14 (66.7%) cases. The ring finger was most commonly injured 15 (71.4%), followed by the middle finger 14 (66.7%), the index finger 12 (57.1%), the thumb finger 7 (33.3%) (Figures 2 and 3), and the little finger 3 (14.3%). The mean number of affected digits was 2.2 ±1.1 (Range 1.0–5.0) and (38%) of patients had two affected digits. Cold storage of amputated digits was performed in only 9 (42.9%) cases. The levels of amputation included 6 (28.6) digits at the MCP joint, 3 (14.3%) at the shaft of the proximal phalanx, 3 (14.3%) at the PIP joint, 4 (19.0%) between the distal insertion of the FDS and the DIP joint 5 (23.8%) proximal interphalangeal joints (Figure 4).
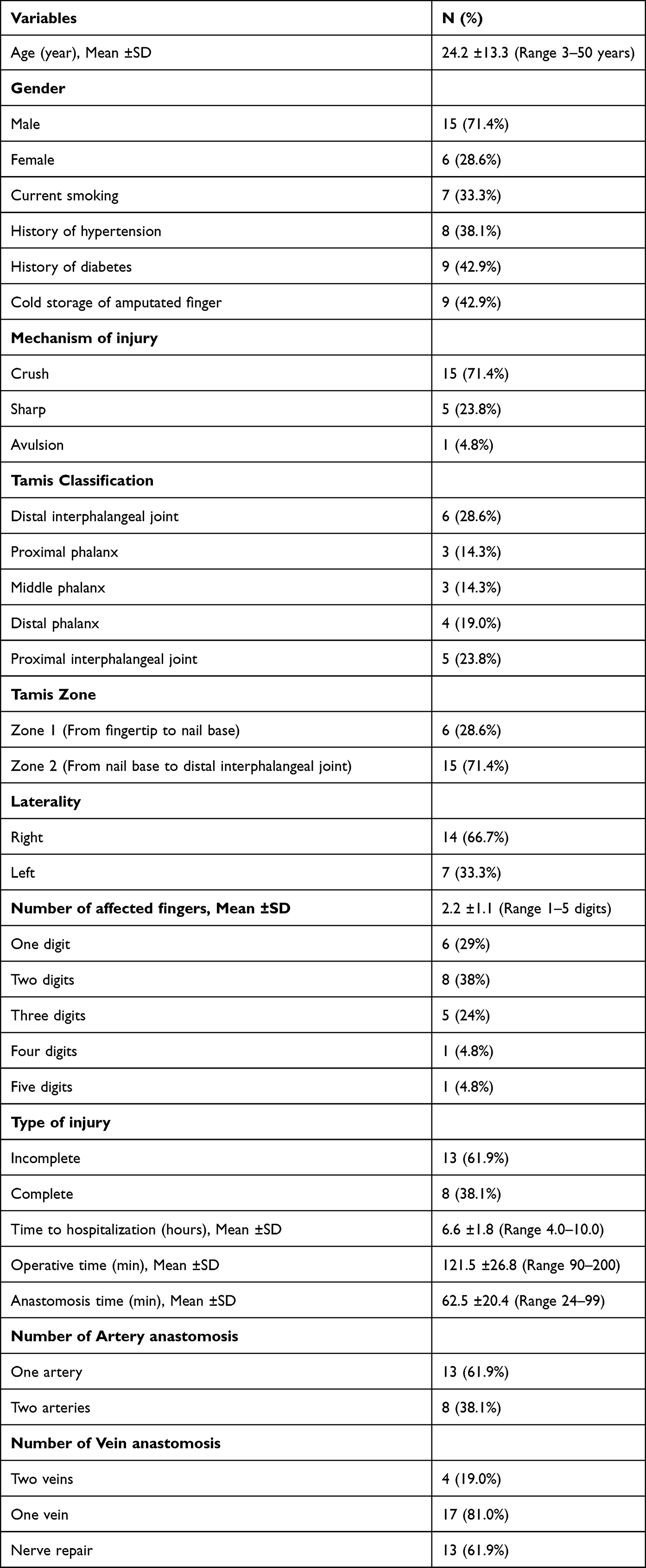 |
Table 1 Baseline Characteristics of Patients with Finger Replantation Surgery |
 |
Figure 2 Thumb fingertip amputation beyond the Distal interphalangeal joint (A). Amputated tip (B). Reattached the fingertip (C). Postoperative appearance (D). 5th-week postoperative appearance [Palmar view (E) and Dorsal view (F)]. |
 |
Figure 3 Thumb fingertip amputation beyond the Middle phalanx joint (A). Amputated finger (B). Reattached the finger using one vein repair and one vein graft (C). Postoperative finger appearance (D). 5th-week postoperative appearance (E). |
 |
Figure 4 Severe injured proximal right hand with multiple fingers amputation and devascularization (A and B). Replantation and bone fixation by K-wires (C). Postoperative appearance with good color, warm, normal capillary refilling (D and E). 5th-week postoperative appearance (F). |
All microsurgical finger re-plantations in this series were performed by a single experienced surgeon (Prof A Altam). The main operative time was 121.5 ±26.8 min (range 90–200 min). The mean anastomosis time (min) was 62.5 ±20.4 min (Range 24–99 min). Vein and artery grafts were performed with two veins and arteries on 4 (19.0%) and 8 (38.1%) cases, respectively. Nerve repairs were needed on 13 (61.9%) cases. Three patients required multiple replantations, including one patient with five digits, and two with three digits.
The survival rate of digit replantations in our series was 16 (76.2%), and one infection was occurred and treated with the proper antibiotic. The failure rate was 5 (23.8%). During a mean follow-up duration of 14.3 ± 3.7 months (range 7–21 months), an overall satisfaction rate of 85.7% was reported among patients with successfully replanted digits. However, one case necessitated subsequent amputation due to persistent paraesthesia and loss of function. Although most replanted digits exhibited effective performance in holding and grasping motions without pain or instability, the TAM score was 54.5 ± 28.1 (range 30–90%) compared to their uninjured counterparts. Ankyloses of the MCP joint, PIP joint, and DIP joint were present in 9 (42.9%) of the surviving digits. Overall functional evaluations yielded Level I (excellent and good) outcomes in 12 (57.1%) replants, Level II (fair) in 4 (19.0%) replants, and Level III (poor) in 5 (23.8%) replants within our series (Table 2).
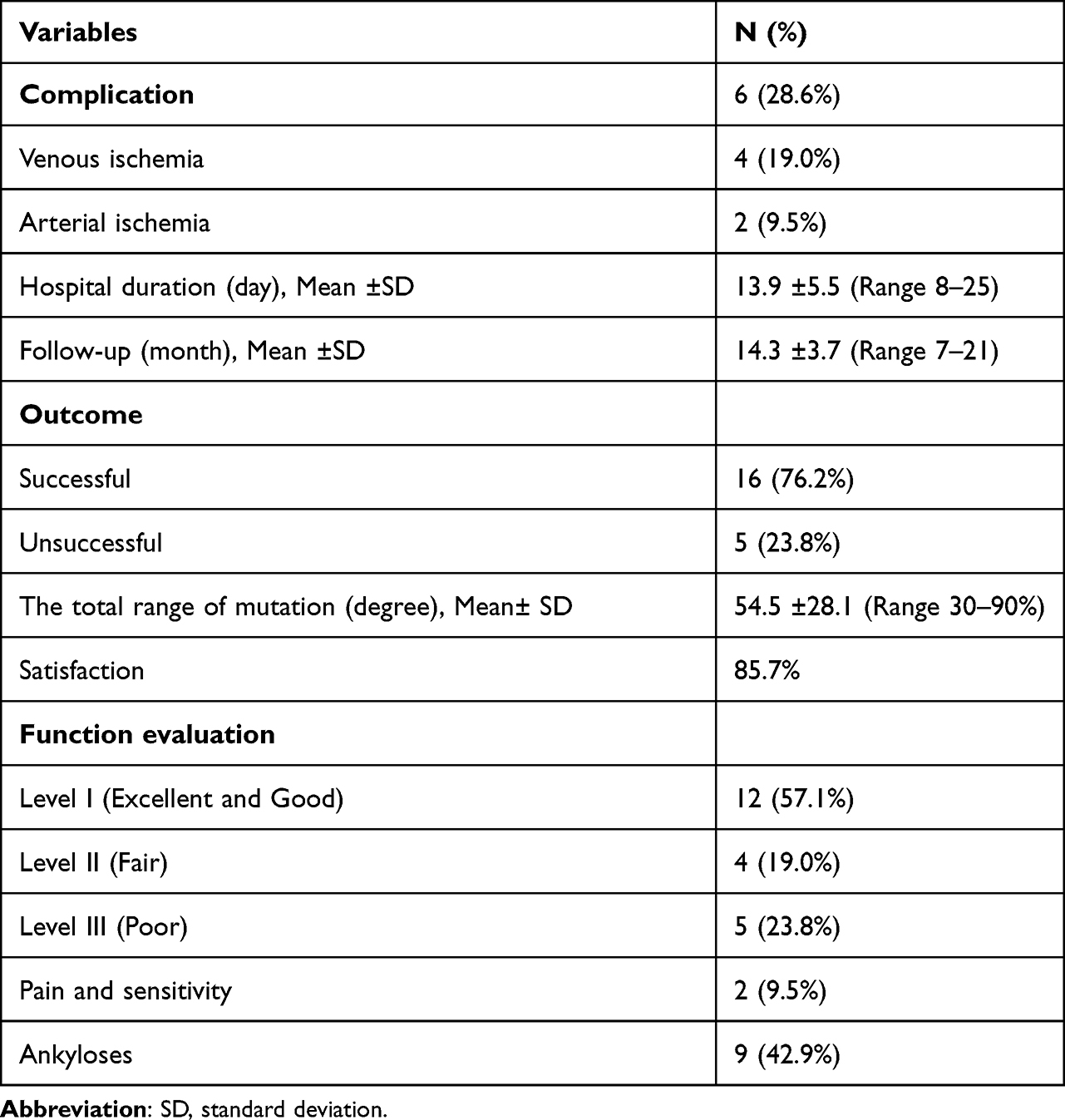 |
Table 2 Postoperative Complication and Outcome Characteristics of Patients with Finger Replantation Surgery |
Factors Associated with Digit Replantation Failure
Increase the number of affected fingers (p < 0.001), complication occurrence (p< 0.001), complete avulsion (p= 0.003), longer operative time (p=0.004), diabetes (p=0.006), hypertension (p= 0.047), procedure difficulty score (p= 0.004), and smoking (p= 0.025), were statistically significant and associated with digit replantation failure (Table 3).
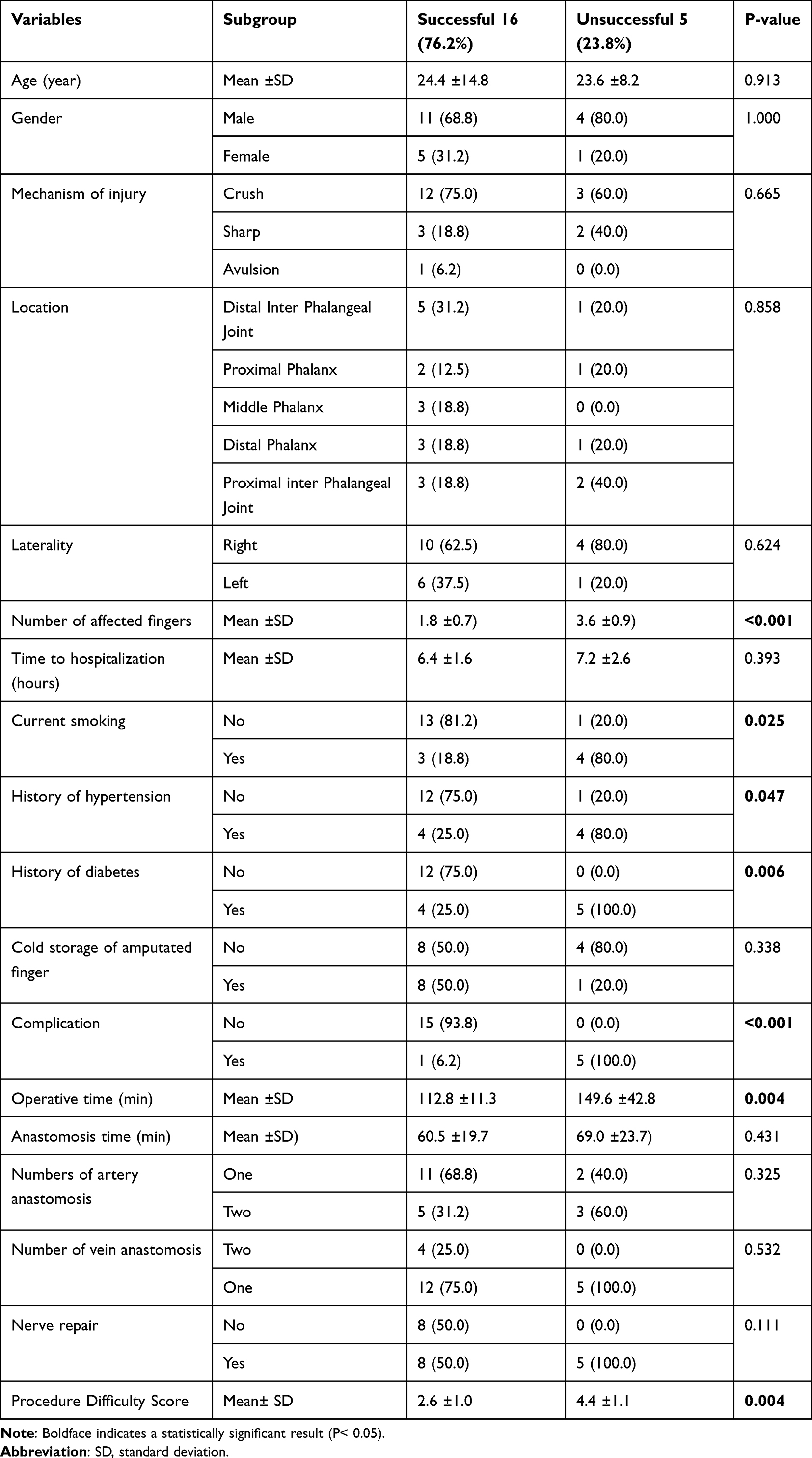 |
Table 3 Factors Associated with Digit Replantation Failure |
Discussion
The success of digit replantation is unequivocally regarded as a highly desirable outcome for patients, particularly those who are younger or heavily reliant on their digits for intricate and complex activities. Thus, the overarching objective of digit replantation is to diligently preserve and restore optimal motor and sensory functionality while also aiming to achieve aesthetically pleasing results.14 The escalating global incidence of amputations has been faced initially with a corresponding surge in microsurgical replantations. Nevertheless, these interventions were recognized to present technical challenges even for the most experienced surgeons. Such challenges included prolonged operative times, intricate vascular structures, concurrent injuries, and the potential for post-operative complications (such as thrombosis, adhesions, scarring, as well as sensory and motor impairments) which collectively limit the scope of this surgical endeavor.9
Hand trauma exhibited notable disproportionality, with a predilection for the right hand, particularly among middle-aged males.15 In a study by Mahajan et al conducted in India, involving an age range of 2 to 55 years, the majority of cases involved males (11 out of 17 cases) and the right hand (16 out of 17 cases).16 Our study cohort, characterized by a mean age of 24.2 ± 13.3 years and spanning from 3 to 50 years, concurred with these findings.
In terms of the injury mechanism, we noticed that the majority of major hand traumas stemmed from crushing and sharp injuries in (71.4%), and (23.8%), respectively. Counterintuitively, despite the divergent nature of these injury mechanisms, our analysis did not identify a statistically significant correlation between a specific mechanism and the failure of digit replantation. These findings deviate from prior studies,9,16 which have emphasized the influence of the injury mechanism on the success of replantation. However, it is important to note that some of these studies had a limited number of cases involving crush injuries, unlike our study. Notably, a case series conducted by Molski et al documented remarkable rates of successful replantation in patients with crush injuries.17 This finding suggests that successful outcomes in replantation can still be achieved in cases of crush injuries, highlighting the potential for favorable results despite the inherent complexities involved.
The time interval from injury to hospital presentation and subsequent operation was determined to be 6.6 ± 1.8 hours in our study, ranging from 4 to 10 hours. Notably, all cases were presented within the recommended viable time frame of less than 12 hours. It is important to highlight those previous reports by Hatchell et al and Oruç et al have emphasized that delayed replantation does not diminish the outcomes compared to immediate intervention.9,18 However, it is essential to acknowledge the need for individualized assessment, considering the specific characteristics of the injury, patients, and operative settings, as several limitations have been identified, and studies have failed to provide a definitive duration range considered suitable for replantation.19 Therefore, the implementation of rigorously designed controlled prospective studies is pivotal to provide stronger evidence regarding the optimal time frame for digit replantation.
The surgical approach to digit replantation may vary, depending on the surgeon’s experience, preference, and common practice. Nevertheless, extensive debridement, with proper visualization, should be followed by an assessment of the osseous structures, stabilizing any concomitant fracture, and trimming the bony stumps. These interventions were noticed to provide better outcomes.20 As bone fixation may require initial fragment amputation, the levels of amputation in our study were as follows; 6 (28.6) digits at the MCP joint, 3 (14.3%) at the shaft of the proximal phalanx, 3 (14.3%) at the PIP joint, 4 (19.0%) between the distal insertion of the FDS and the DIP joint 5 (23.8%) proximal interphalangeal joints. The general rule of thumb in replantation is to preserve tendon insertion, aiming to allow maximum mobility, thus, when replantation is to be sought, it may be optimal for the amputation to be performed distally to the FDS, as recommended by many authors.9,18
In contrast, proximal amputations have been associated with poorer functional outcomes and higher failure rates.21 We performed distal amputation in only 5 (23.8%) cases, while the majority of cases involved proximal amputations. Remarkably, reasonable postoperative recovery and digit functionality were observed in the majority of proximal amputation cases. These findings align with previous reports, indicating more favorable outcomes in replantation cases involving the thumb, hand, distal forearm, and fingers distal to the FDS insertion (Zone 1).14
Traditionally, tendon repair is typically prioritized before any vascular or neurological bundle repair.22 The timing of neurologic versus vascular repair, however, remains a subject of debate. Repairing the nerves earlier may provide better surgical visualization, as vascular repair can lead to blood extravasation that obscures the surgical field.20 In our cases, neurologic repair was performed before vascular repair. Subsequently, the vascular repair was initiated, considering the patency and health of both ends, before proceeding with any anastomosis. Veins were sutured in a similar manner with fewer sutures. It is important to ensure that all anastomoses are tension-free, and that appropriate grafting techniques are employed when defects are present.20,23 Previous studies have highlighted improved outcomes with increased anastomoses, with a 2:1 vein-to-artery ratio being identified as optimal.22 In our study, two artery anastomoses were performed in 8 cases (38.1%), and two vein anastomoses were performed in 4 cases (19.0%). Although these findings did not achieve statistical significance, it is important to acknowledge that this may be attributed to the limited sample size in our study. Additionally, we were unable to perform a detailed analysis to include involved hand zones, which have been demonstrated to have differential outcomes depending on the affected zone in a study by Lee et al.24
The definition of successful replantation remains a subject of controversy. Some institutions define successful replantation based on the initial vascular survival of the transplanted digit. In a comprehensive national study, a success rate of 79% for the thumb and 67% for other digits was reported.25 In our study, the overall survival rate was 76.2%, which is consistent with the findings of Brown et al, who reported a success rate of 70%.26 Nevertheless, it is important to interpret these reports cautiously, as it is unclear whether these numbers include cases of revision replantations or subsequent amputations. Furthermore, as mentioned previously, the primary goal of replantation should be to restore the functional capabilities of the affected digits rather than focusing solely on vascular supply restoration.22 Therefore, patient satisfaction and objective assessments of motor and sensory functions should be considered when evaluating the success of replantation. In our study, functional recovery was evaluated based on patient satisfaction, range of motion, sensibility ratings, and grip strength. The mean total range of motion was 54.5 ± 28.1, ranging from 30% to 90% in the survived digits. Pain and sensitivity were reported in 2 cases (9.5%), and the functional evaluation resulted in Level I (Excellent and Good) in 12 cases (57.1%), Level II (Fair) in 4 cases (19.0%), and Level III (Poor) in 5 cases (23.8%). Kleinert et al proposed a set of functional criteria for assessing replantation outcomes, including sensibility ratings, grip strength, range of motion, absence of cold intolerance, and ability to return to work.27
Our result showed that three patients required multiple replantations, including one patient with five digits, and two with three digits. Our result was in the line with a systematic review that mentioned higher complications and take-back rates in low-income and middle-income countries.5
Various factors have been reported as predictors of the overall outcome of digit replantation, many of which have been discussed earlier in this study. However, in the postoperative period, patients may benefit from interventions such as physical therapy, rehabilitation, and psychological support, which contribute to the restoration of limb functionality to the pre-amputation level.28 In our study, several factors were identified as statistically significant predictors of digit failure, including an increased number of affected fingers, longer operative time, complete avulsion, and the presence of comorbidities such as smoking, diabetes, hypertension, and the occurrence of complications. It is important to note that these factors have been studied independently in previous research, with variations in case numbers and outcomes. For instance, Lima et al found that the need for venous anastomosis was the sole factor influencing limb survival.29 Additional factors that have been documented as influential in the outcome of digit replantation include multi-level forearm fractures, the involvement of the median nerve, the inability to return to work, crushed injuries, advanced age, diabetes mellitus, hypertension, end-stage renal disease, and hypertensive chronic kidney disease.18,30 Furthermore, previous studies have consistently shown that smoking significantly increases the risk of replantation failure, with nonsmokers having three times higher odds of successful replantation compared to smokers.10 In our study, a higher procedure difficulty was significantly associated with replantation failure, which align with Yoon et al13 findings. Notably, the mentioned study showed a higher trend of operative failure amongst surgeons with an overall higher volume.
This implies that surgeon volume and operative performance may have synergistic associations with some outcomes but distinct associations with others. It is plausible that some surgeons, despite having high procedural volume, are prone to repeating certain mistakes or improper techniques unless these are identified and corrected.
Study Limitations
This study is limited by its retrospective design, which introduces the potential for selection bias and incomplete data, thereby limiting the generalizability of our findings. Furthermore, despite the advantages of multi-center studies, the heterogeneity in protocols, practices, and quality of care among various institutions may serve as an unrecognized confounding factor in our results. Additionally, the loss to follow-up within our cohort was influenced by the involvement of multiple institutions, as well as the limited financial and logistical resources available for patient tracking. Moreover, our study would benefit from a more detailed stratified analysis, considering specific hand zones and evaluating pre-operative surgical planning. However, these aspects were not feasible due to financial constraints faced by our patients and the lack of preparedness in most hospitals where replantation procedures were performed, as none of them were specialized replantation centers. Lastly, the small sample size prevented the inclusion of control groups for comparing alternative treatment approaches and limited the extent of robust statistical analysis. Nevertheless, this study serves as the first report on the current status of finger replantation in Yemen. Based on our findings, further research is warranted to gain a better understanding of the specific needs and future prospects of replantation in such resource-limited settings.
Conclusion
Microsurgical finger replantation can be performed in a resource-limited setting with acceptable outcomes and survival rates. However, this procedure requires specialized equipment and personnel that may not be available at all institutions. In this study, increased the number of affected digits, longer operative time, complete avulsion, current smoking, diabetes, hypertension, and complication occurrence were associated with digit replantation failure.
Data Sharing Statement
All the data was included in this study.
Ethics Approval and Informed Consent
The college’s research review and ethical committee of 21 September University for Medical and Applied Sciences, Sana’a, Yemen approved this project on 16, Jun 2022 with ID number: H-09-E-16-A10, which was carried out in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patients.
Consent for Publication
Written informed consent was obtained from the patients including the figures. Parent or legal guardian of patients under 18 years of age provided informed consent for participation and publication of the case details and images.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Komatsu S, Tamai S. Successful replantation of a completely cut-off thumb. Plast Reconstr Surg. 1968;42(4):374–377. doi:10.1097/00006534-196810000-00021
2. Hadley SR, Capo JT. Digit replantation the first 50 years. Bull Hosp Jt Dis. 2015;73:148–155.
3. Kwon SH, Lao WW, Hsu AT, et al. The preferred management of a single-digit distal phalanx amputation. J Reconstr Microsurg. 2020;36:301–310. doi:10.1055/s-0039-1701013
4. Merrell JC, Tien NV, Son NT, et al. Introduction of microsurgery in Vietnam by a charitable organization: a 15-year experience. Plast Reconst Surg. 2007;119:1267–1273. doi:10.1097/01.prs.0000254544.65054.95
5. de Berker HT, Čebron U, Bradley D, et al. Outcomes of microsurgical free tissue transfer performed on international surgical collaborations in low-income and middle-income countries: a systematic review and meta-analysis. J Plast Reconstr Aesthet Surg. 2022;75(7):2049–2063. doi:10.1016/j.bjps.2022.04.002
6. Reavey PL, Stranix JT, Muresan H, Soares M, Thanik V. Disappearing digits: analysis of national trends in amputation and replantation in the United States. Plast Reconst Surg. 2018;141(6):857e–867e. doi:10.1097/prs.0000000000004368
7. Shaterian A, Rajaii R, Kanack M, Evans GRD, Leis A. Predictors of digit survival following replantation: quantitative review and meta-analysis. J Hand Microsurg. 2018;10(02):66–73. doi:10.1055/s-0038-1626689
8. Chung KC, Yoon AP, Malay S, Shauver MJ, Wang L, Kaur S. Patient-reported and functional outcomes after revision amputation and replantation of digit amputations: the FRANCHISE multicenter international retrospective cohort study. JAMA Surgery. 2019;154(7):637–646. doi:10.1001/jamasurg.2019.0418
9. Oruç M, Gürsoy K, Özer K, et al. Eight years of clinical experience with digit replantation: demographic characteristics and outcomes. Turk J Trauma Emerg Surg. 2017;23:311–316. doi:10.5505/tjtes.2016.40040
10. Cho HE, Kotsis SV, Chung KC. Outcomes following replantation/revascularization in the hand. Hand Clin. 2019;35(2):207–219. doi:10.1016/j.hcl.2018.12.008
11. Verdan C. Detaillierte Beschreibung einer primären Beugesehnennaht im Digitalkanal [Detailed description of the primary flexor tendon suture in the digital canal]. Handchirurgie. 1981;13(3–4):186–188. German.
12. Kaplan FT, Raskin KB. Indications and surgical techniques for digit replantation. Bulletin. 2001;60:179–188.
13. Yoon AP, Kane RL, Wang L, Wang L, Chung KC. Variation in surgeon proficiency scores and association with digit replantation outcomes. JAMA network open. 2021;4(10):e2128765. doi:10.1001/jamanetworkopen.2021.28765
14. Hoang NT. Microsurgical finger replantation in Hanoi, Vietnam: our first experience. Handchir Mikrochir Plast Chir. 2005;37:337–343. doi:10.1055/s-2005-872848
15. Urbaniak JR, Roth JH, Nunley JA, Goldner RD, Koman LA. The results of replantation after amputation of a single finger. J Bone Joint Surg Am. 1985;67:611–619.
16. Mahajan RK, Mittal S. Functional outcome of patients undergoing replantation of hand at wrist level-7 year experience. Indian J Plast Surg. 2013;46(03):555–560. doi:10.4103/0970-0358.122018
17. Molski M. Replantation of fingers and hands after avulsion and crush injuries. J Plast Reconstr Aesthet Surg. 2007;60(7):748–754. doi:10.1016/j.bjps.2007.03.009
18. Hatchell AC, Sandre AR, McRae M, Farrokhyar F, Avram R. The success of salvage procedures for failing digital replants: a retrospective cohort study. Microsurgery. 2019;39(3):200–206. doi:10.1002/micr.30379
19. Woo SH, Cheon HJ, Kim YW, Kang DH, Nam HJ. Delayed and suspended replantation for complete amputation of digits and hands. J Hand Surg. 2015;40:883–889. doi:10.1016/j.jhsa.2015.01.006
20. Barbary S, Dap F, Dautel G. Finger replantation: surgical technique and indications. Chirurgie de la Main. 2013;32(6):363–372. doi:10.1016/j.main.2013.04.012
21. Matsuzaki H, Kouda H, Maniwa K. Secondary surgeries after digital replantations: a case series. Hand surgery : an international journal devoted to hand and upper limb surgery and related research. J Asia Pac Fed Soc Surg Hand. 2012;17:351–357. doi:10.1142/s021881041250030x
22. Prucz RB, Friedrich JB. Upper extremity replantation: current concepts. Plast Reconstr Surg. 2014;133(2):333–342. doi:10.1097/01.prs.0000437254.93574.a8
23. Ross DC, Manktelow RT, Wells MT, Boyd JB. Tendon function after replantation: prognostic factors and strategies to enhance total active motion. Ann Plast Surg. 2003;51(2):141–146. doi:10.1097/01.Sap.0000058499.74279.D8
24. Lee BI, Chung HY, Kim WK, Kim SW, Dhong ES. The effects of the number and ratio of repaired arteries and veins on the survival rate in digital replantation. Ann Plast Surg. 2000;44:288–294. doi:10.1097/00000637-200044030-00007
25. Hustedt JW, Bohl DD, Champagne L. The detrimental effect of decentralization in digital replantation in the United States: 15 years of evidence from the national inpatient sample. J Hand Surg. 2016;41(5):593–601. doi:10.1016/j.jhsa.2016.02.011
26. Brown M, Lu Y, Chung KC, Mahmoudi E. Annual hospital volume and success of digital replantation. Plast Reconstr Surg. 2017;139(3):672–680. doi:10.1097/prs.0000000000003087
27. Kleinert HE, Jablon M, Tsai TM. An overview of replantation and results of 347 replants in 245 patients. J Trauma. 1980;20:390–398. doi:10.1097/00005373-198005000-00005
28. Maricevich M, Carlsen B, Mardini S, Moran S. Upper extremity and digital replantation. Hand. 2011;6(4):356–363. doi:10.1007/s11552-011-9353-5
29. Lima JQ Jr, Carli AD, Nakamoto HA, Bersani G, Crepaldi BE, de Rezende MR. Prognostic factors on survival rate of fingers replantation. Acta Ortop Bras. 2015;23:16–18. doi:10.1590/1413-78522015230101026
30. Rizzo KR, Eckhoff MD, Gonzalez GA, Diamond S, Nesti L, Dunn JC. Predictors of success following microvascular replantation surgery of the upper extremity in adult patients. Plast Reconstr Surg Glob Open. 2022;10:e4501. doi:10.1097/GOX.0000000000004501
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.