Back to Journals » Clinical Ophthalmology » Volume 18
Microbiology and Antimicrobial Susceptibility in Adult Dacryocystitis
Authors Chi YC ![]() , Lin CC, Chiu TY
, Lin CC, Chiu TY
Received 16 December 2023
Accepted for publication 9 February 2024
Published 23 February 2024 Volume 2024:18 Pages 575—582
DOI https://doi.org/10.2147/OPTH.S452707
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yi-Chun Chi,1,2 Chia-Ching Lin,1,2 Tzu-Yu Chiu1,2
1Department of Ophthalmology, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan; 2Kaohsiung Medical University, Kaohsiung, Taiwan
Correspondence: Tzu-Yu Chiu, Department of Ophthalmology, Kaohsiung Medical University Hospital, Number 100, Tzyou 1st Road, Sanmin District, Kaohsiung City, 807, Taiwan, Tel +886-7-3121101 ext. 6531, Email [email protected]
Purpose: To investigate the microbiology and antimicrobial susceptibility of dacryocystitis in adults and identify the changing trends over time in Taiwan.
Methods: This is a single-centered, retrospective study. We retrospectively reviewed adult patients with dacryocystitis from January 2012 to December 2021 in a tertiary medical center in Taiwan. The pathogens and in vitro antimicrobial susceptibility of the pus cultures from the lacrimal sac were collected.
Results: Thirty-five cultures in acute and 211 cultures in chronic dacryocystitis were collected. Of the 220 isolates, a similar proportion of gram-positive (44%) and gram-negative (43%) aerobes were demonstrated in chronic dacryocystitis and more gram-negative aerobes (50%) than gram-positive aereobes (41%) in acute dacryocystitis. The most common pathogens were methicillin-resistant Staphylococcus aureus (MRSA; 28.1%) and Pseudomonas aeruginosa (28.1%) in acute dacryocystitis, while coagulase-negative Staphylococci was the most common micro-organism in chronic dacryocystitis. The effective antibiotics for gram-positive aerobes were vancomycin (100%), moxifloxacin (88%) and trimethoprim/sulfamethoxazole (78%). Meropenem (95%), amikacin (93%), and levofloxacin (91%) were sensitive to more than 90% of gram-negative aerobes in current study. High resistant species were also isolated in our cohort.
Conclusion: More gram-negative pathogens and more resistant species are rising in adult dacryocystitis. Understanding the bacteriology and antimicrobial susceptibility of the region is crucial for the empirical antibiotic selection in clinical practice.
Keywords: dacryocystitis, antibiotic, microbiology
Introduction
Dacryocystitis is an inflammation of the lacrimal sac, usually results from nasolacrimal duct obstruction (NLDO). The obstruction of lacrimal system may lead to stasis of tears and accumulation of desquamated cells as well as mucoid secretions, consequently, create a fertile environment for secondary bacterial infection or chronic inflammation.
Dacryocystitis is typically categorized into acute or chronic forms. Acute dacryocystitis, an acute inflammation of the lacrimal sac, is usually presenting with erythematous, swelling and tenderness of the overlying tissue of lacrimal sac area. Chronic dacryocystitis is a more common and indolent form of the lacrimal sac inflammation with presentation of epiphora, mucoid discharge and chronic conjunctivitis. A few studies had attempted to analyze and conclude the different microbiology spectrum between acute and chronic dacryocystitis, and yet various outcomes demonstrated,1–3 which may result from the different geographic distribution of microbials and the distinct antibiotic culture of the medical systems. Besides, the more accessible medical resources and the application of broad-spectrum antibiotic may change the microbiology and its drug susceptibility.1 In the late 20th century, more gram-positive bacteria were isolated in both acute and chronic dacryocystitis, with over 60% pathogens being gram-positive pathogens.4–6 However, more gram-negative organisms and methicillin-resistant Staphylococcus aureus (MRSA) have been isolated in lacrimal sac infections in recent years.2,7
This study aims to investigate the microbiology and antimicrobial susceptibility of dacryocystitis in adults from 2012 to 2021 in southern Taiwan, and to identify the changing trends in bacteriology and drug resistance over time.
Materials and Methods
We retrospectively reviewed medical records of patients with acute or chronic dacryocystitis from January 2012 to December 2021 at a single tertiary medical center, Kaohsiung Medical University Hospital. Patients were diagnosed with acute or chronic dacryocystitis according to the clinical signs and symptoms. Acute dacryocystitis was diagnosed when patients presented with acute swelling, pain, and erythematous change of the lacrimal sac area. Chronic dacryocystitis was diagnosed as persistent epiphora and purulent regurgitation from the lacrimal drainage system during nasolacrimal duct irrigation. Patients with pus culture from the lacrimal system were enrolled. We excluded pediatric or infantile patients who were under 18 years of age, dacryocystitis or NLDO secondary to trauma, neoplasm, or foreign body occlusion and patients without a lacrimal pus culture.
All samples were collected from the lacrimal system under sterile conditions. In acute dacryocystitis, the lacrimal sac pus was obtained with pus aspiration through overlying skin from the lacrimal sac with a 19-gauze needle and a 5-cc sterile syringe. In chronic dacryocystitis, pus was collected from the punctum with irrigation of the lacrimal system or from the surgically excised lacrimal sac. The samples were cultured with the aerobic and anaerobic Copan swab transport system or culture media. Clinically significant growth of the pathogens and their antibiotic susceptibility tests were reported within 5–7 days of culture. The antibiotic susceptibility tests were presented as sensitive, resistant, and intermediate according to the Clinical and Laboratory Standards Institute standards.
If the pus culture showed no pathogens or if there were entirely different pathogens isolated with an interval of at least one month between the two cultures, it is considered a new infection despite involving the same participant.
This study was approved by the institutional review board of Kaohsiung Medical University Hospital (KMUHIRB-E(I)-20220219) and in accordance with the ethical standards of the Declaration of Helsinki. Due to the retrospective manner, the informed consents from individual participants were waived. Nevertheless, the database was kept anonymized during data collection, and the analyses were conducted using the same encrypted computer.
Results
One hundred ninety-five dacryocystitis patients with lacrimal pus cultures were involved in current study. We excluded five patients under 18 years old, five trauma-related dacryocystitis, one dacryocystitis secondary to neoplasm, and one with foreign body in the lacrimal system. Thus, the final enrolled cases were 183 patients. There were 134 females (74%) and 49 males (26%). Thirty-five patients (19.1%) with 35 pus cultures had acute dacryocystitis, while 148 patients (80.9%) with a total of 211 pus cultures were diagnosed with chronic dacryocystitis. Five cultures in acute dacryocystitis and 45 cultures in chronic dacryocystitis yielded no growth of pathogen, resulting the total positive culture rate of 80.8%. Polymicrobial infections were observed in one pus culture (2.9%) in acute dacryocystitis, and 21 pus cultures (10%) in chronic dacryocystitis.
Of the 35 cultures in acute dacryocystitis, 13 (40.6%) gram-positive aerobes, 16 (50%) gram-negative aerobes and three (9.4%) anaerobic pathogens were isolated. Of 211 cultures in chronic dacryocystitis, 188 pathogens were isolated, including 84 (44.2%) gram-positive aerobes, 80 (42.6%) gram-negative aerobes, and 25 (12.8%) anaerobic pathogens. The isolated micro-organisms were demonstrated in Table 1. There were similar proportion of gram-positive and gram-negative aerobes in chronic dacryocystitis, and slightly more gram-negative isolates in acute dacryocystitis. More anaerobic pathogens were isolated in chronic dacryocystitis than in acute dacryocystitis (13.30% vs. 9.38%). MRSA (28.1%) and Pseudomonas aeruginosa (28.1%) were the most isolated pathogens followed by Citrobacter koseri (9.4%), methicillin-sensitive MSSA (6.3%), Escherichia coli (6.3%) and coagulase-negative staphylococci (CoNS) (6.3%) in acute dacryocystitis. In chronic dacryocystitis, CoNS (19.2%) was the most isolated micro-organisms, followed by Pseudomonas aeruginosa (13.3%), MRSA (8.5%), and α-hemolytic Streptococcus (5.9%).
 |
Table 1 Microbiology of Acute and Chronic Dacryocystitis |
The susceptibilities of antibiotics commonly used in our practice were shown in Tables 2–4. The most sensitive antibiotics to gram-positive aerobes were vancomycin (100%), moxifloxacin (88%) and trimethoprim/sulfamethoxazole (78%). Cefazolin (31%), oxacillin (31%), erythromycin (29%) and ampicillin/sulbactam (amp/sul) (33%) only yielded an around 30% sensitive rate to gram-positive isolates. Meropenem (95%), amikacin (93%), and levofloxacin (91%) were sensitive to more than 90% of gram-negative aerobes, while amp/sul (37%) and piperacillin (50%) had less sensitivity to the gram-negative micro-organisms. In anaerobes, meropenem (100%) was the most sensitive antimicrobial agent, while metronidazole (59%) seemed to be the most resistant drug.
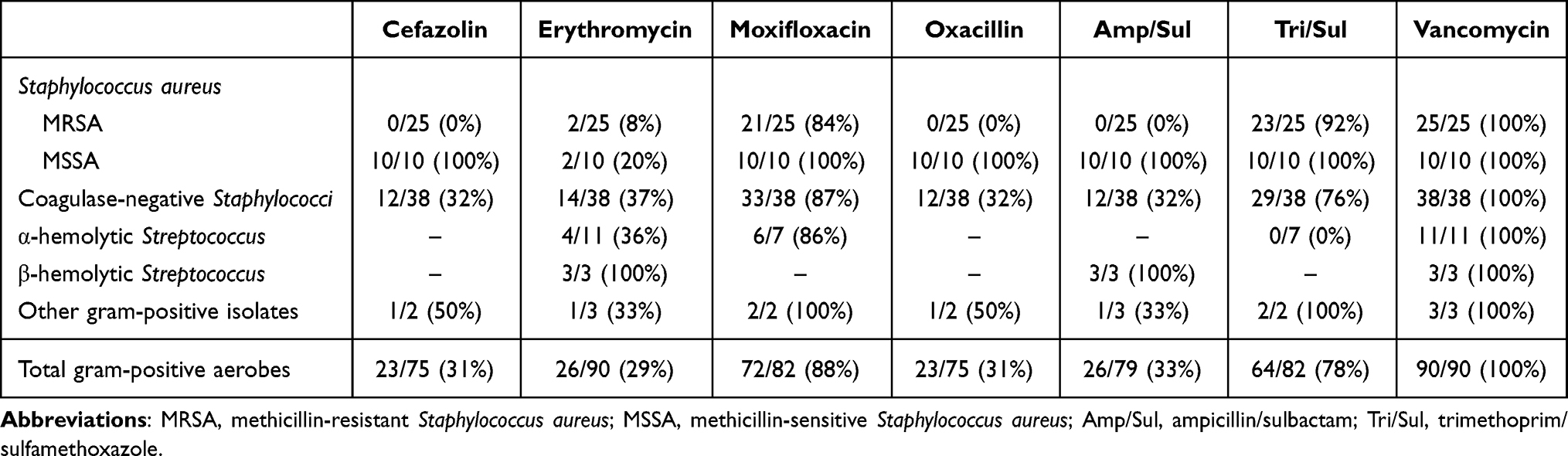 |
Table 2 Antimicrobial Susceptibility of the Gram-Positive Aerobes |
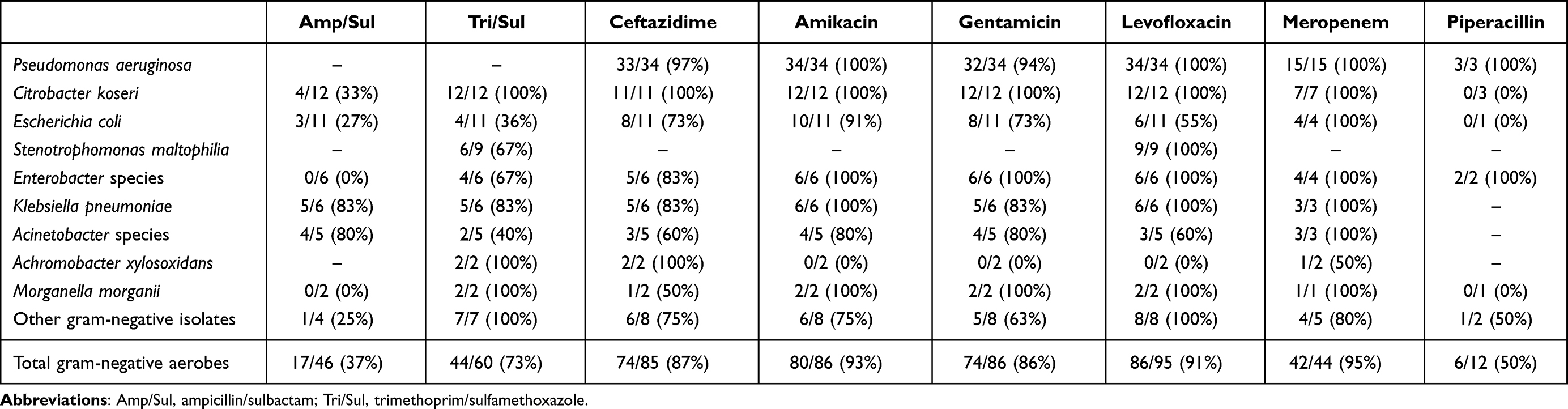 |
Table 3 Antimicrobial Susceptibility of the Gram-Negative Aerobes |
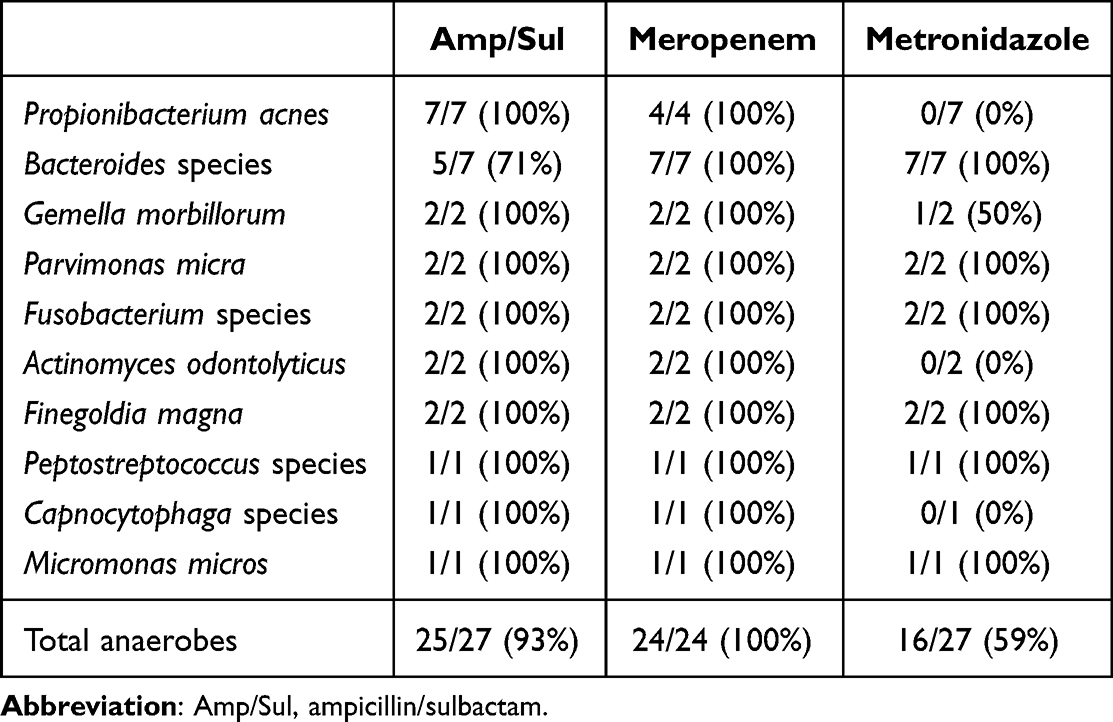 |
Table 4 Antimicrobial Susceptibility of the Anaerobes |
Discussion
Dacryocystitis is the most common infection of the lacrimal system mainly secondary to NLDO. In this study, there was a trend of female predominance (72%) in dacryocystitis, which is compatible to previous studies,1, 8, 9 and in concordance with the female preponderance in NLDO.10 It might be a result of smaller diameter of nasolacrimal duct in women,11 or the hormonal change in postmenopausal females.12 More chronic dacryocystitis was presented than the clinically acute one, which may imply the chronic structural change in the lacrimal system as its main pathophysiology.8, 13
The common causative pathogens of dacryocystitis are changing over time. Streptococcus pneumoniae was once the most common species in the 1930s, but gradually replaced by Staphylococci (Staphylococcus epidermidis and Staphylococcus aureus) in the late 20th century.4, 5 The gram-positive pathogens remained to be the leading pathogens then, which was responsible for around 60% of the isolates in the 1980–1990s.4–6 However, recent bacteriologic analysis in dacryocystitis revealed an increasing incidence of gram-negative bacteria, especially the Pseudomonas species.1, 3, 7, 14 In the current study, there were similar proportion of gram-positive and gram-negative isolates in dacryocystitis, which supported the observation of an increasing number of gram-negative pathogens infection in recent studies.3, 7
Stenotrophomonas maltophilia was a rare causative pathogen in dacryocystitis.15 It is mostly seen in immunocompromised patients, and highly resistant to majority of β-lactam antibiotics; as a result, it presented mostly as a nosocomial infection. This pathogen was reported in chronic dacryocystitis in one case (2.5%) in Briscoe’s study and four cases (<1%) in Chaudhry et al16, 17 Further case reports demonstrated Stenotrophomonas maltophilia as a responsible micro-organism in chronic dacryocystitis in different age and various immune status around the 2010s.18, 19 In our study, we reported nine cases (4.79%) of Stenotrophomonas, all isolated from chronic dacryocystitis, which was the highest incidence among present literatures. The relatively high incidence of Stenotrophomonas highlights the emerging change that the rare, highly resistant gram-negative pathogens are rising recently.
The prevalence of pathogens responsible for acute or chronic dacryocystitis differed. The predominant micro-organisms in acute dacryocystitis were Staphylococcus aureus (34.38%) and Pseudomonas aeruginosa (28.13%) in acute dacryocystitis, whereas CoNS (19.15%) was the most common pathogen in chronic dacryocystitis. The results were similar to that of reported in Bharathi et al,1 since infections of highly virulent pathogens (Staphylococcus aureus and Pseudomonas) are more likely to present acutely, while a less virulent pathogen (CoNS) usually cause an indolent form of dacryocystitis. Higher frequency of MRSA was observed within the acute group, as reported in Mills et al,20 may result from the more fulminant characteristic and antimicrobial resistance to first-line antibiotics.
The overall polymicrobial infection rate was 10.43% which was within the range of previous reported incident rates in adults with dacryocystitis (5–23%).3, 21 More polymicrobial micro-organisms were cultured from chronic dacryocystitis. Moreover, more anaerobes were isolated from chronic dacryocystitis. The most common anaerobes in current study were Propionibacterium acne and anaerobic gram-negative bacilli (Bacteroides species and Fusobacterium species). These micro-organisms constituted the normal floral in oral and skin flora.22
More antimicrobial-resistant isolates were taking place nowadays. MRSA accounted for more than half of the Staphylococcus aureus in either acute or chronic dacryocystitis in current study. The increased frequency of MRSA was reported not only in dacryocystitis but all infectious diseases.20, 23, 24 Furthermore, all Streptococcal pneumoniae were resistant to erythromycin in our study, which was consistent with the increasing trend of erythromycin-resistant pneumococci in Asian countries over these years, and nearly total resistance (96.4%) in Zhou’s study in 2010.25 We reported a proportion of Stenotrophomonas maltophilia, which was strongly resistant to multiple broad-spectrum antibiotics due to its β-lactamases, efflux pumps for quinolone agents, and aminoglycoside acetyl transferases.18, 19
Vancomycin (100%) remained to be the most effective antibiotic for gram-positive pathogens as previously reported.26, 27 The third generation quinolones such as moxifloxacin or gatifloxacin also possessed a high sensitivity to gram-positive aerobes.27 Trimethoprim/sulfamethoxazole may be a reasonable choice for gram-positive and gram-negative aerobes with over 70% sensitivity rate in our study. Additionally, it was relatively sensitive to Stenotrophomonas, which is resistant to a broad spectrum of antibiotics.19 Of gram-negative aerobes, more antimicrobials yielded an over 90% sensitivity rate other than some resistance to piperacillin (50%). Cefazolin, oxacillin, erythromycin and amp/sul had a low sensitivity rate.26, 27
Chen et al reported a significantly decreased sensitivity of erythromycin in gram-positive pathogens over time. They also reported no significant decreased in sensitivity of cefazolin (68.3%), sulfamethoxazole (79.3%), gatifloxacin (86.5%), and the same as our result, 100% sensitivity to vancomycin. In the susceptibility tests for gram-negative pathogens, they reported 74.6% sensitivity to gentamicin, 85% to ciprofloxacin, 92% to tobramycin, 92% to ceftazidime and 99.5% to gatifloxacin.27 In our investigation, we observed a higher resistance to cefazolin and erythromycin among gram-positive pathogens than that shown in Chen’s results. A small-scaled microbiology study for dacryocystitis in the same center in Taiwan was conducted from April 1995 to June 1998.28 There were 50% sensitivity to erythromycin, 75% to ampicillin/sulbactam and 100% to vancomycin in gram-positive micro-organisms. Additionally, sensitivity rates were 50% for ampicillin/sulbactam, 77.8% for gentamicin, 100% for amikacin and piperacillin in gram-negative pathogens. Longitudinally, the sensitivities of erythromycin, ampicillin/sulbactam and piperacillin exhibited a decline when comparing to the results of the present study.
There were some limitations in current study. First, relatively small sample size was included in our study. This may result from the less culture performed clinically especially in acute dacryocystitis, since some clinicians might avoid immediate aspiration of the pus from lacrimal sac to avoid further fistula formation. Moreover, we did not exclude patients with previous antibiotic treatment since most patients had been treated before referral to our hospital, a tertiary medical center. There may be a bias that more resistant pathogens than those in the community might be presented in current study. Furthermore, the limitation of the retrospective manner should be recognized. Inevitably, there were missing data, and the initial treatment of each patient was barely identified if it was from other medical institutions and not recorded in the chart.
Conclusion
This study echoes to a trend that more gram-negative pathogens and more resistant species are rising in adult dacryocystitis. CoNS remains to be the leading pathogen in chronic dacryocystitis, but more Pseudomonas species perceived. More virulent species such as Pseudomonas and Staphylococcus aureus are more common in acute dacryocystitis. We identified MRSA more than MSSA, as well as a proportion of Stenotrophomonas suggest the high resistant micro-organisms are emerging. This study disclosed the causative pathogens and the drug susceptibility in dacryocystitis and provide a reference for empirical antibiotics selection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bharathi MJ, Ramakrishnan R, Maneksha V, Shivakumar C, Nithya V, Mittal S. Comparative bacteriology of acute and chronic dacryocystitis. Eye. 2008;22(7):953–960. doi:10.1038/sj.eye.6702918
2. Eshraghi B, Abdi P, Akbari M, Fard MA. Microbiologic spectrum of acute and chronic dacryocystitis. Int J Ophthalmol. 2014;7(5):864–867. doi:10.3980/j.issn.2222-3959.2014.05.23
3. Luo B, Li M, Xiang N, Hu W, Liu R, Yan X. The microbiologic spectrum of dacryocystitis. BMC Ophthalmol. 2021;21(1):29. doi:10.1186/s12886-020-01792-4
4. Coden DJ, Hornblass A, Haas BD. Clinical bacteriology of dacryocystitis in adults. Ophthalmic Plast Reconstr Surg. 1993;9(2):125–131. doi:10.1097/00002341-199306000-00008
5. Hartikainen J, Lehtonen OP, Saari KM. Bacteriology of lacrimal duct obstruction in adults. Br J Ophthalmol. 1997;81(1):37–40. doi:10.1136/bjo.81.1.37
6. Huber-Spitzy V, Steinkogler FJ, Huber E, Arocker-Mettinger E, Schiffbänker M. Acquired dacryocystitis: microbiology and conservative therapy. Acta Ophthalmol. 1992;70(6):745–749. doi:10.1111/j.1755-3768.1992.tb04880.x
7. Chung SY, Rafailov L, Turbin RE, Langer PD. The microbiologic profile of dacryocystitis. Orbit. 2019;38(1):72–78. doi:10.1080/01676830.2018.1466901
8. Eslami F, Ghasemi Basir HR, Moradi A, Heidari Farah S. Microbiological study of dacryocystitis in northwest of Iran. Clin Ophthalmol. 2018;12:1859–1864. doi:10.2147/opth.S175463
9. Khatoon J, Rizvi SAR, Gupta Y, Alam MS. A prospective study on epidemiology of dacryocystitis at a tertiary eye care center in Northern India. Oman J Ophthalmol. 2021;14(3):169–172. doi:10.4103/ojo.ojo_80_21
10. Mills DM, Meyer DR. Acquired nasolacrimal duct obstruction. Otolaryngol Clin North Am. 2006;39(5):979–99, vii. doi:10.1016/j.otc.2006.07.002
11. Janssen AG, Mansour K, Bos JJ, Castelijns JA. Diameter of the bony lacrimal canal: normal values and values related to nasolacrimal duct obstruction: assessment with CT. AJNR Am J Neuroradiol. 2001;22(5):845–850.
12. Ali MJ, Schicht M, Paulsen F. Qualitative hormonal profiling of the lacrimal drainage system: potential insights into the etiopathogenesis of primary acquired nasolacrimal duct obstruction. Ophthalmic Plast Reconstr Surg. 2017;33(5):381–388. doi:10.1097/iop.0000000000000962
13. Avdagic E, Phelps PO. Nasolacrimal duct obstruction as an important cause of epiphora. Dis Mon. 2020;66(10):101043. doi:10.1016/j.disamonth.2020.101043
14. Pornpanich K, Luemsamran P, Leelaporn A, et al. Microbiology of primary acquired nasolacrimal duct obstruction: simple epiphora, acute dacryocystitis, and chronic dacryocystitis. Clin Ophthalmol. 2016;10:337–342. doi:10.2147/opth.S100280
15. Marx DP, Chang PT, Winthrop KL. Strenotrophomonas maltophilia-related chronic dacryocystitis. Orbit. 2012;31(6):433–434. doi:10.3109/01676830.2012.694958
16. Briscoe D, Rubowitz A, Assia EI. Changing bacterial isolates and antibiotic sensitivities of purulent dacryocystitis. Orbit. 2005;24(2):95–98. doi:10.1080/01676830590926585
17. Chaudhry IA, Shamsi FA, Al-Rashed W. Bacteriology of chronic dacryocystitis in a tertiary eye care center. Ophthalmic Plast Reconstr Surg. 2005;21(3):207–210. doi:10.1097/01.iop.0000161718.54275.7d
18. Wladis EJ. Dacryocystitis secondary to Stenotrophomonas maltophilia infection. Ophthalmic Plast Reconstr Surg. 2011;27(5):e116–e117. doi:10.1097/IOP.0b013e318201ca3b
19. Comez AT, Koklu A, Akcali A. Chronic dacryocystitis secondary to Stenotrophomonas maltophilia and Staphylococcus aureus mixed infection. BMJ Case Rep. 2014;2014. doi:10.1136/bcr-2014-203642
20. Mills DM, Bodman MG, Meyer DR, Morton AD. The microbiologic spectrum of dacryocystitis: a national study of acute versus chronic infection. Ophthalmic Plast Reconstr Surg. 2007;23(4):302–306. doi:10.1097/IOP.0b013e318070d237
21. Martins MC, Ricardo JR, Akaishi PM, Velasco e Cruz AA. Orbital abscess secondary to acute dacryocystitis: case report. Arq Bras Oftalmol. 2008;71(4):576–578. doi:10.1590/s0004-27492008000400020
22. Brook I, Frazier EH. Aerobic and anaerobic microbiology of dacryocystitis. Am J Ophthalmol. 1998;125(4):552–554. doi:10.1016/s0002-9394(99)80198-6
23. Kotlus BS, Rodgers IR, Udell IJ. Dacryocystitis caused by community-onset methicillin-resistant Staphylococcus aureus. Ophthalmic Plast Reconstr Surg. 2005;21(5):371–375. doi:10.1097/01.iop.0000175035.22953.71
24. Hiramatsu K, Cui L, Kuroda M, Ito T. The emergence and evolution of methicillin-resistant Staphylococcus aureus. Trends Microbiol. 2001;9(10):486–493. doi:10.1016/S0966-842X(01)02175-8
25. Zhou L, Ma X, Gao W, et al. Molecular characteristics of erythromycin-resistant Streptococcus pneumoniae from pediatric patients younger than five years in Beijing, 2010. BMC Microbiol. 2012;12(1):228. doi:10.1186/1471-2180-12-228
26. Pradeep AV, Patil SS, Koti SV, Arunkumar JS, Garag SS, Hegde JS. Clinico-bacteriological study of chronic dacryocystitis cases in northern Karnataka, India. J Clin Diagn Res. 2013;7(11):2502–2504. doi:10.7860/jcdr/2013/6636.3590
27. Chen L, Fu T, Gu H, et al. Trends in dacryocystitis in China: a STROBE-compliant article. Medicine. 2018;97(26):e11318. doi:10.1097/md.0000000000011318
28. Ding P-C, Chang C-H, M-y S, Peng C-F. Dacryocystitis: microbiology and drug susceptibility. Taiwan J Ophthalmol. 2000;39(4):502–506. doi:10.30048/ACTASOS.200012.0009
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.