Back to Journals » Clinical Ophthalmology » Volume 17
Microbiological Profile of Infectious Keratitis During Covid-19 Pandemic
Authors Lima-Fontes M ![]() , Martinho-Dias D, Leuzinger-Dias M
, Martinho-Dias D, Leuzinger-Dias M ![]() , Cunha AM
, Cunha AM ![]() , Neves Cardoso P
, Neves Cardoso P ![]() , Torrão L
, Torrão L ![]() , Moreira R, Falcão-Reis F, Pinheiro-Costa J
, Moreira R, Falcão-Reis F, Pinheiro-Costa J ![]()
Received 10 November 2022
Accepted for publication 21 December 2022
Published 10 February 2023 Volume 2023:17 Pages 535—543
DOI https://doi.org/10.2147/OPTH.S395877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mário Lima-Fontes,1,2 Daniel Martinho-Dias,3– 5 Mariana Leuzinger-Dias,1 Ana Maria Cunha,1 Pedro Neves Cardoso,1 Luís Torrão,1 Raúl Moreira,1 Fernando Falcão-Reis,1,6 João Pinheiro-Costa1,6
1Department of Ophthalmology, Centro Hospitalar Universitário São João, Porto, 4200-319, Portugal; 2Department of Biomedicine, Faculty of Medicine, University of Porto, Porto, 4050-313, Portugal; 3Department of Community Medicine, Information and Decision in Health, University of Porto Faculty of Medicine, Porto, 4050-313, Portugal; 4CINTESIS – Center for Health Technology and Services Research, University of Porto, Porto, 4050-313, Portugal; 5Family Health Unit Ao encontro da Saúde, ACES Santo Tirso-Trofa, Trofa, 4745-559, Portugal; 6Department of Surgery and Physiology, Faculty of Medicine, University of Porto, Porto, 4050-313, Portugal
Correspondence: Mário Lima-Fontes, Department of Ophthalmology, Centro Hospitalar Universitário São João, Alameda Prof. Hernâni Monteiro, Porto, 4200-319, Portugal, Email [email protected]
Purpose: The Covid-19 pandemic introduced significant changes in our daily life, including the widespread use of face masks. The purpose of this study was to assess if significant changes occurred in the microbiological profile of infectious keratitis.
Patients and Methods: A retrospective study was performed, based on a survey review of the electronic medical records of all patients with presumed infectious keratitis, between March 2020 and October 2021. The microbiological isolates in this sample (pandemic group) were compared with those obtained in our center between 2009 and 2018 (pre-pandemic group).
Results: A total of 194 samples were included in the pandemic group. We obtained a culture-positivity rate of 43.3%, which was significantly higher when compared with the pre-pandemic data (35.15%, p = 0.033). Several further significant differences were found between the pandemic and the pre-pandemic groups: the proportion of bacteria, including gram-positive and gram-negative groups, was higher in our sample (pre-pandemic vs pandemic: 76.78% vs 83.33%, p = 0.010; 53.35% vs 60.71%, p = 0.016; 23.43% vs 34.52%, p = 0.005, respectively); two populations of Gram-positive bacteria found in this study were not isolated in the pre-pandemic sample – Dolosigranulum pigrum and Propionibacterium spp.; and two bacterial isolates were significantly increased in our sample – Corynebacterium spp. (18.41% vs 29.76%, p = 0.003) and Pseudomonas aeruginosa (9.00% vs 16.66%, p = 0.012).
Conclusion: In conclusion, significant changes were found in the microbiological profile of infectious keratitis in our center during the Covid-19 pandemic. While these changes could be related to face mask use, more observational and experimental studies are needed to explore this possible association.
Keywords: infectious keratitis, Covid-19, face mask, microbiology
Introduction
The Covid-19 pandemic caused significant changes in our daily habits, including maintaining physical distance, practicing hand hygiene, and wearing protective face masks.1 Particularly after the generalized use of face masks, numerous reports from around the world pointed to a perceived increase in dry eye symptoms, such as irritation, blurred vision, foreign body sensation, pain, and itching.2–5 The raised awareness for this possible association boosted investigation about this topic and multiple studies were published in 2021 and 2022, reporting significant changes in Ocular Surface Disease Index (OSDI) score and ocular surface parameters, including tear meniscus height, tear film break up time, corneal fluorescein staining, and Schirmer-I test.6–8 These findings led to the consolidation of a new clinical entity called “mask-associated dry eye” (MADE).9,10
Since most of the commonly used face masks are not air-tight superiorly, this configuration results in an unnatural airflow towards the eyelids and ocular surface during expiration, which could explain the above mentioned findings.11 In fact, it has been reported that taping the upper mask edge improves ocular surface stability and reduces dry eye symptoms.12
Due to this interesting and proven mechanism, we wondered if it could also have resulted in a change in the microbiological profile of infectious keratitis. Aside from a reported increase in the incidence of chalazion associated with face mask use, a case of infectious keratitis in a patient with an initial corneal abrasion from mask use who later developed recurrent corneal erosion syndrome complicated by microbial keratitis was published.13,14 Furthermore, an increase in the rate of infectious keratitis after PRK during the COVID-19 pandemic was reported by Soleimani et al.15
Kapelushnik et al reported an increase in ocular surface temperature when wearing a face mask, which may affect the local microbiota.11 Angaramo et al attempted to assess differences in oral flora dispersion by evaluating colony formation during exhalation in 3 distinct face mask scenarios: no face mask, surgical face mask and surgical face mask with superior edge tape secured. However, no statistically significant differences were found between the groups.16
One study published in 2022, assessed the impact of the COVID-19 pandemic on the incidence and characteristics of culture-positive microbial keratitis at a tertiary eye hospital in the United Kingdom. No significant differences were found in the incidence of culture-positive microbial keratitis and organism subtypes - fungi, acanthamoeba, Gram-positive bacteria, or Gram negative bacteria.17
In this sense, the goal of this study was to analyze the microbiological results of corneal scrapes from patients with suspected infectious keratitis, in our tertiary center, since March 2020, when the first cases of Covid-19 were identified in Portugal, and to compare them with data published by our group regarding the period of 2009 to 2018.
Materials and Methods
This retrospective study was conducted in a Portuguese tertiary center between March 1, 2020, and October 31, 2021 (20 months), and was based on a survey review of electronic medical records of all patients with presumed infectious keratitis.
The study was carried out in accordance with the tenets of the Declaration of Helsinki the study adhered to the tenets of the Declaration of Helsinki and was approved by the local Ethics Committee of Centro Hospitalar Universitário de São João / Faculty of Medicine, University of Porto (CHUSJ/FMUP, project n° 228/22). Informed consent was waived due to the retrospective nature of the study and the absence of reported data that can identify single patients.
Presumed infectious keratitis was defined by the presence of a corneal infiltrate >1mm2 in size with or without epithelial defect.
All samples were collected in the emergency room, under topical anesthesia. Scrapes were taken from the ulcer base and inoculated onto Amies Agar Gel each time (Copan, Brescia, Italy). Finally, they were sent to the Microbiology Department for culture and antibiotic sensitivity testing. Selective media and stains for aerobic and anaerobic bacteria, Mycobacterium and Acanthamoeba, were used in clinically suspicious or nonresponsive cases.
Patients were treated hourly with an empiric topical third- or fourth-generation fluoroquinolone and an aminoglycoside, according to an internal protocol. Topical clotrimazole was added to the treatment regimen if a fungi etiology was suspected (soil contamination or trauma with vegetable matter).
Patients’ age, gender, presence of risk factors (contact lens use, ocular trauma, ocular surface diseases, or systemic diseases), and sample results were all evaluated.
Microbiological isolates in this sample (pandemic group) were compared with the ones obtained in our center between January 1, 2009, and December 31, 2018, and published by Oliveira-Ferreira et al in 2019 (pre-pandemic group).18
SPSS software, version 28 (IBM, Chicago, IL), was used for statistical analysis. To compare differences between groups, the independent-samples t-test and the fisher exact test were used. P<0.05 was deemed significant.
Results
A total of 194 samples from the same number of patients were included in the pandemic period, which were compared with 1360 scrapes from the pre-pandemic period. In the pandemic group, the patients’ mean age was 49.39 ± 19.87 years (range 18–91), with 54.12% (n=105) being female. No significant differences were found regarding age and gender distribution between this sample and the pre-pandemic data, as portrayed in Table 1.
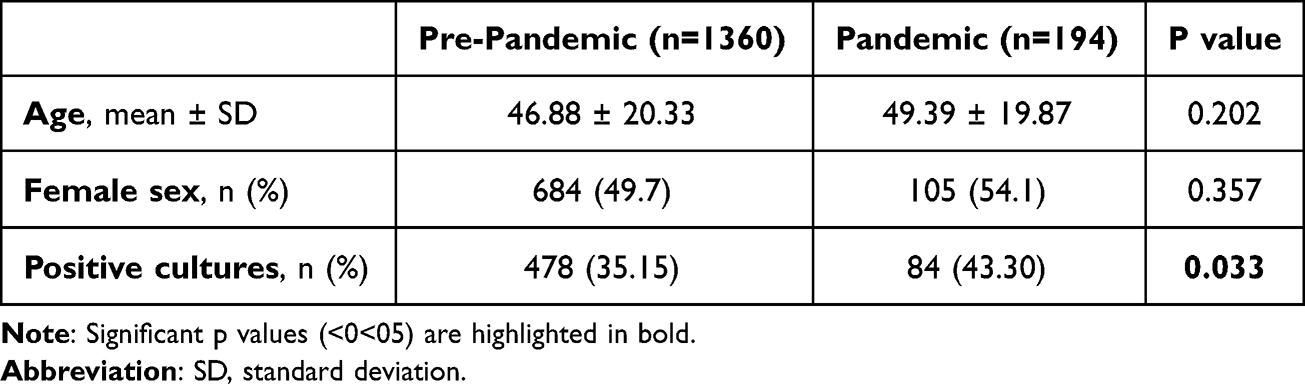 |
Table 1 Age and Gender Distribution, and Proportion of Positive Cultures in the Pre-Pandemic and Pandemic Samples |
We obtained a 43.30% (n=84) culture-positive rate, which was significantly higher than in the pre-pandemic sample (35.15%, n=478, p=0.033). Bacteria accounted for 83.33% (n=70) of all positive scrapes, with Gram-positive and Gram-negative bacteria being isolated in 60.71% (n=51) and 34.52% (n=29) of the positive cultures, respectively. Positive fungi isolates were found in 11.90% (n=10) of the cases, and Acanthamoeba was found in 3.57% (n=3) of the cases. Figure 1 depicts the distribution of the microbiological profile in our sample.
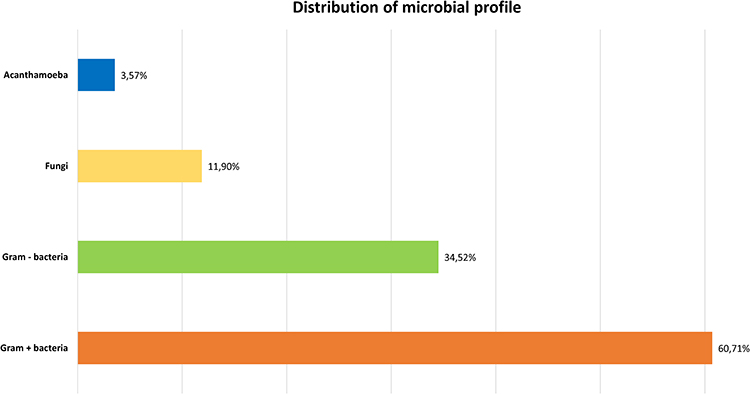 |
Figure 1 Distribution of microbial profile in corneal scrapes in the pandemic sample. |
The most frequent Gram-positive bacteria isolated were Corynebacterium macginleyi (22.62%, n=19), Staphylococcus Aureus (16.67%, n=14), and Streptococcus pneumoniae (8.33%, n=7). Pseudomonas Aeruginosa was the most common Gram-negative bacteria isolate (16.67%, n=14). Candida species were the most commonly isolated fungi (7.14%, n=6). Table 2 shows the distribution of all microbiological isolates.
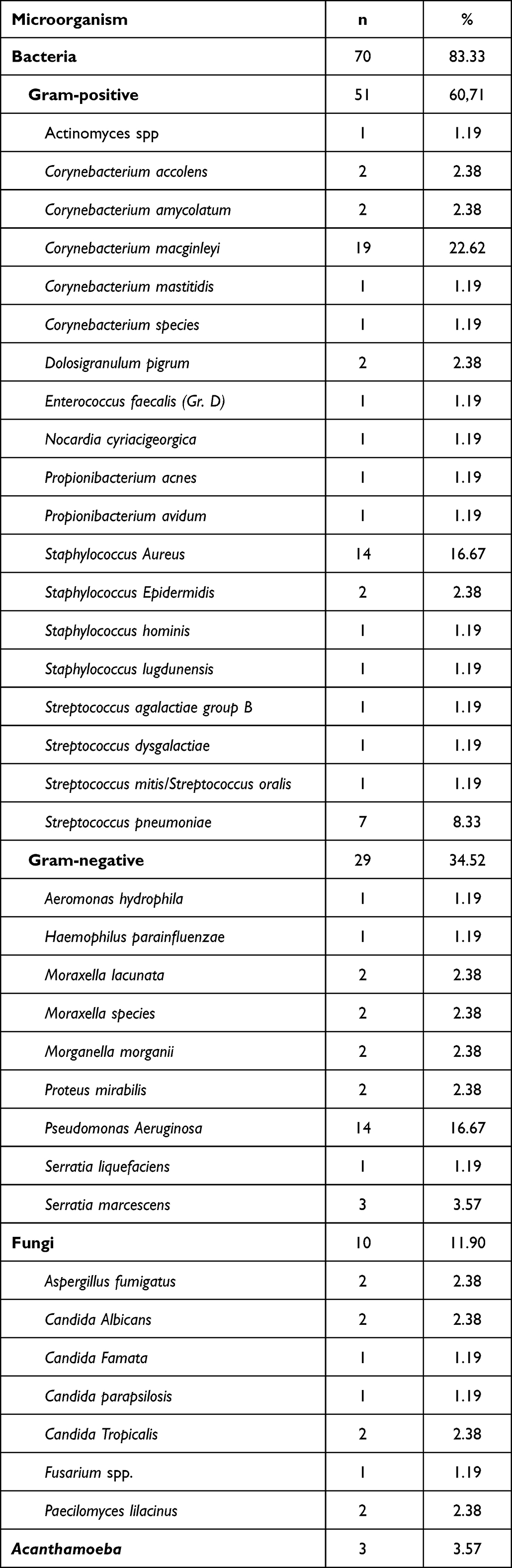 |
Table 2 Microbial Isolates Proportions in the Pandemic Sample |
In 80.95% of the patients (n=68), we found at least one ophthalmologic risk factor. Additionally, 23.81% (n=20) had relevant systemic disorders. The most common local risk factors found were contact lens wear and ocular trauma, accounting for 36.90% (n=31) and 17.86% (n=15) of cases, respectively. Diabetes mellitus was the most common systemic risk factor, accounting for 13.10% (n=11). Table 3 depicts the distribution of the risk factors in the pre-pandemic and pandemic samples. No significant differences were found between groups, except for ocular trauma which was more frequent in the pre-pandemic group (34.94% vs 17.86%, p=0.003).
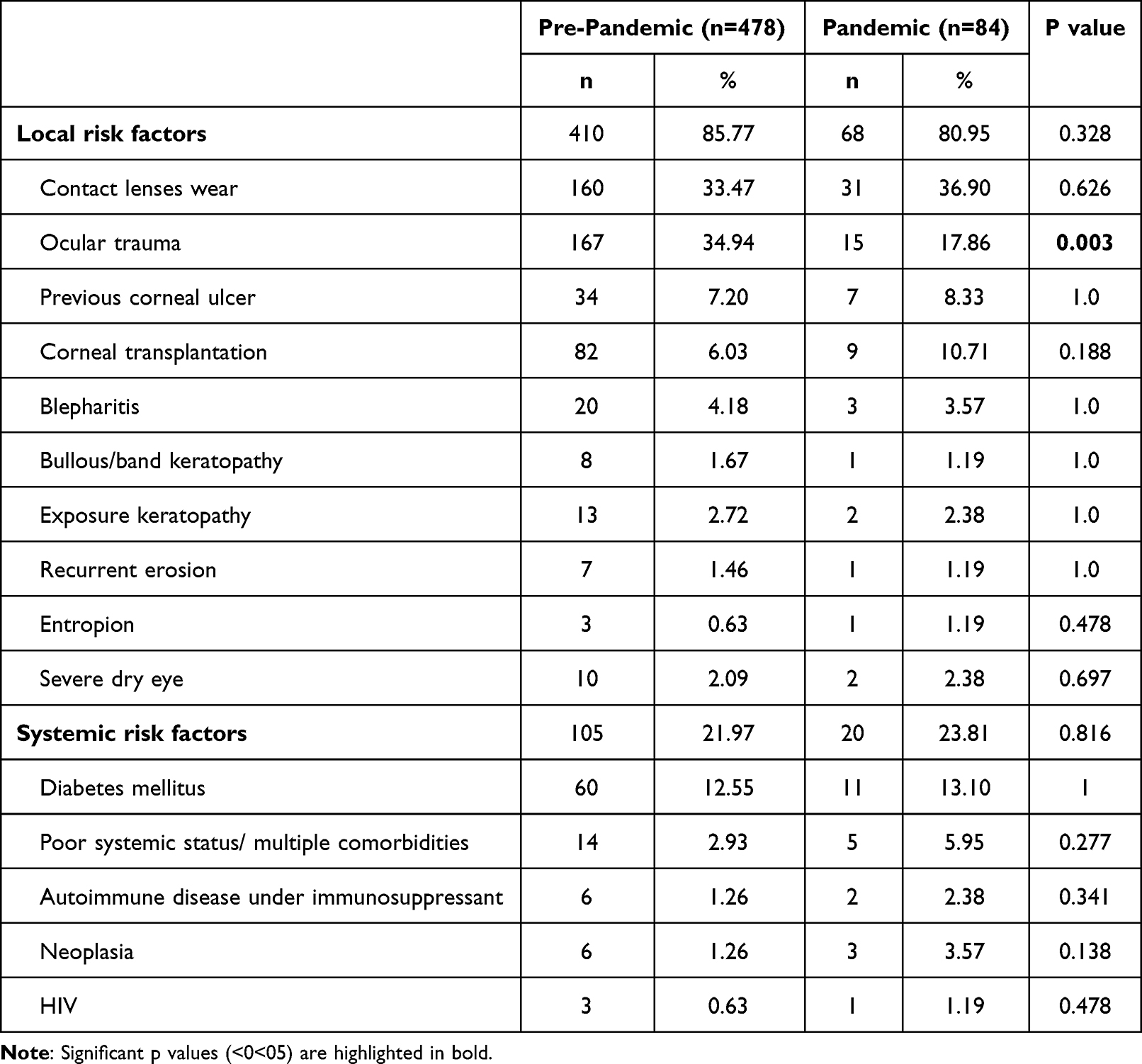 |
Table 3 Local and Systemic Risk Factors in the Pre-Pandemic and Pandemic Samples |
When the microbial isolates from this sample were compared to those published by Oliveira-Ferreira et al18 several significant differences were found. The proportion of bacteria, including Gram-positive and Gram-negative groups, was higher in our sample (pre-pandemic vs pandemic: 76.78% vs 83.33%, p=0.010; 53.35% vs 60.71%, p=0.016; 23.43% vs 34.52%, p=0.005, respectively). Two populations of Gram-positive bacteria found in this study were not isolated in the pre-pandemic sample: Dolosigranulum pigrum and Propionibacterium spp. Finally, two bacterial isolates were significantly increased in our sample: Corynebacterium spp. (18.41% vs 29.76%, p=0.003) and Pseudomonas aeruginosa (9.00% vs 16.66%, p=0.012). Table 4 compares the proportion of different microbial isolates between the two groups.
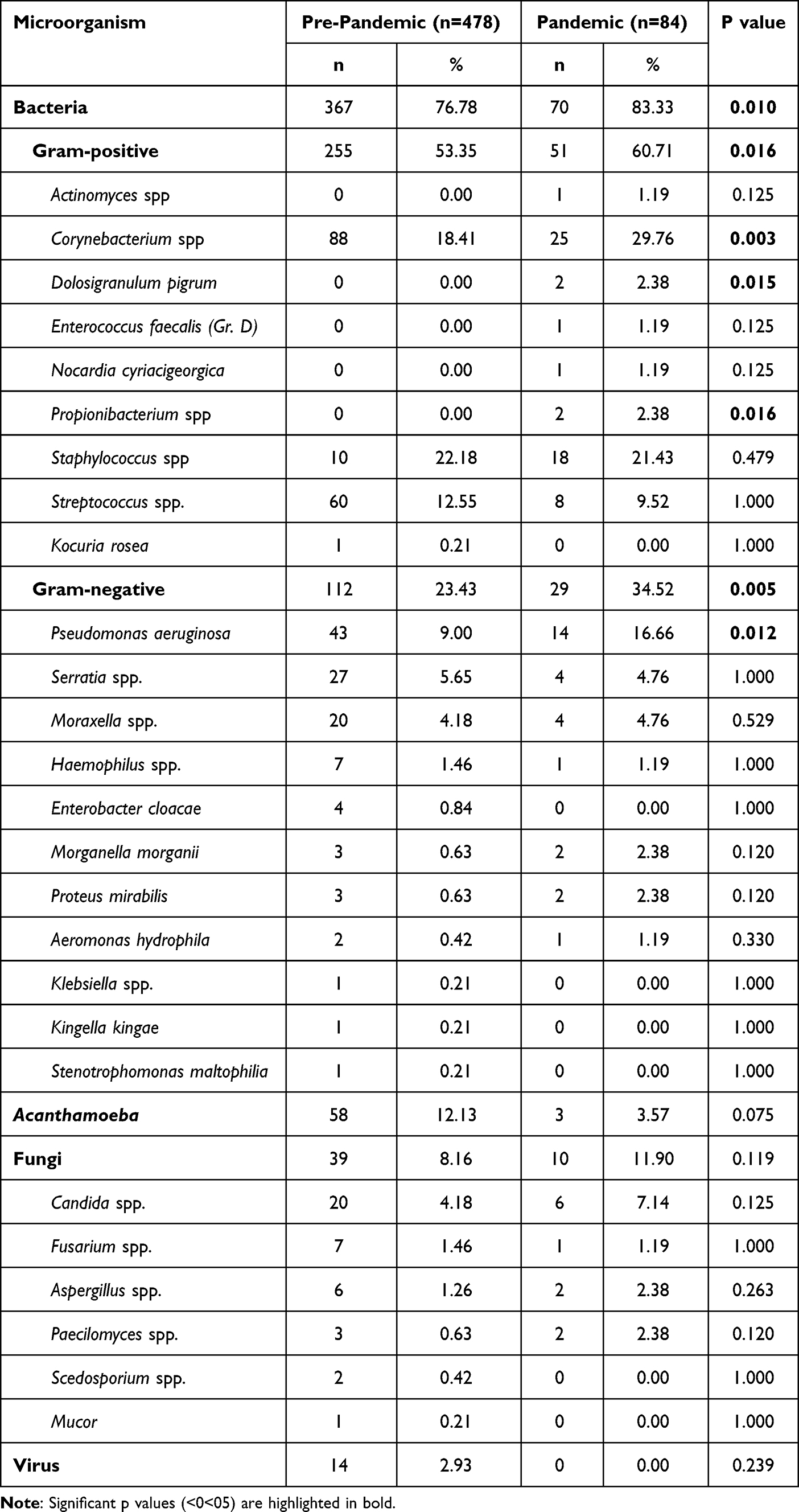 |
Table 4 Microbial Profile Comparison Between the Pandemic and Pre-Pandemic Samples |
Discussion
Constant local updates of microbiological profiles are essential for selecting the best topical treatment for ocular infections.19,20 Since the Covid-19 pandemic caused significant disruptions in our daily lives, including the widespread use of face masks around the world, it is possible that the microbiological profile of infectious keratitis changed significantly.
Infectious keratitis is a serious condition that can have long-term effects on vision and even result in eyeball loss. Untreated keratitis can cause corneal opacification and/or perforation, as well as other equally dangerous complications like secondary glaucoma, corneal thinning, uveitis, and endophthalmitis. Because of this rapidly progressing and potentially fatal course, prompt treatment with effective empirical topical antibiotics is required.18
Bacteria were isolated as the agent in the vast majority of cases in this sample, and Gram-positive bacteria were identified in 60.71% of the positive cultures. While this proportion is comparable to those reported in other studies,21,22 the literature varies widely, with countries such as the United Kingdom and New Zealand reporting ratios of 38.9% and 83%, respectively.23,24 A Canadian study found a decreasing trend in Gram-positive pathogens, most likely due to the widespread use of contact lenses.25
Corynebacterium macginleyi was the most frequently identified agent (22.62%), followed by Staphylococcus aureus and Pseudomonas aeruginosa (16.67% each), and Streptococcus pneumoniae (8.33%). Some studies in the literature identified Pseudomonas aeruginosa as the most common agent,21,23–25 whereas other studies identified Staphylococcus aureus as the primary causal agent.21,23,25 The microbiological department at our hospital classified Corynebacterium macginleyi as a scrape contaminant. However, this microorganism appears to actively contribute to the pathophysiology of blepharitis, and thus it may play a role in the genesis of infectious keratitis, especially if certain risk factors are present.18 As a result, its significance as a causative agent of infections has been increasingly recognized.26,27
Acanthamoeba accounted for 3.57% of positive scrapes, which falls within the ranges published in the literature (1.6% to 16.9%).28,29
Candida spp. was the most common fungus and the whole kingdom accounted for 11.90% of positive scrapes. Fungi are more common in countries from tropical and subtropical regions than in temperate regions, such as Brazil (30%) or India (23–36%).28,30
We discovered an increase in the proportion of bacteria, whether Gram-positive or Gram-negative, when we compared our isolates to the results published by our group prior to the pandemic. Likewise, the diversity of Gram-positive bacteria found in our sample increased, with two isolates not found in the pre-pandemic study: Dolosigranulum pigrum and Propionibacterium spp. Furthermore, there was a significant increase in two specific bacteria, Corynebacterium spp. and Pseudomonas aeruginosa. Corynebacterium spp. and Propionibacterium spp. are knowns commensal of the oral cavity.31 While these bacteria are commonly found in the conjunctiva of healthy adults and are considered non-pathogenic, they can cause ocular infections in patients with compromised immunity, such as those with diabetes or long-term users of topical steroids, as well as those with corneal epithelial damage from trauma, contact lens wear, lagophthalmos, and trichiasis.32,33 Dolosigranulum pigrum is also part of the oral flora and has recently emerged as the causative agent in a few cases of keratitis.34 Pseudomonas aeruginosa is an opportunistic pathogen that can cause sight-threatening microbial keratitis.35 While it is not the only cause of bacterial keratitis linked with contact lens use, Pseudomonas aeruginosa is responsible for the majority of corneal ulcers associated with lens wear.36
Interestingly, Michael et al performed a similar study in a tertiary eye hospital in the UK and found no differences in culture-positive microbial keratitis and organism subtypes - fungi, acanthamoeba, Gram-positive bacteria, or Gram negative bacteria.17 However, in this study a pandemic sample of 312 cases was compared with pre-pandemic data of almost 6000 scrapes, which may have affected the capacity to detect differences between groups.
Since the use of a face mask typically results in an unnatural airflow towards the eyelids and ocular surface during expiration, we hypothesize that this could induce major changes in the ocular surface microbial communities. This factor added to the high prevalence of risk factors for microbial keratitis in our sample (80.95% for local and 23.81% for systemic factors), could favor corneal infection with typical commensal organisms, such as Corynebacterium spp. and Propionibacterium spp. Furthermore, 36.90% of the patients were contact lens wearers. The airflow from the face mask may enhance bacterial biofilm growth on contact lenses, potentially enhancing infections by pathogenic species such as Pseudomonas aeruginosa.
Our work does present some limitations, namely, its retrospective nature, which may have resulted in missing data presented in the medical records. Second, there was an important difference on the size of the two compared samples. While this factor is minimized by the statistical analysis, it may still introduce some errors in the interpretation. Third, while interesting differences were found in the microbiological profile between the two samples, it is important to take into consideration that other factors may contribute to these results, such as the availability of a certain class of antibiotic, changes in clinical practice, or social distancing during the pandemic. Fourth, ocular trauma was particularly less frequent in our sample, which is an important risk factor that can affect the microbial isolates. Fifth, while the use of face masks was generally increased in the pandemic period, no information was collected regarding compliance and duration of use, which may greatly vary across patients.
Conclusion
In conclusion, during the Covid-19 pandemic, significant alterations in the microbiological profile of infectious keratitis were discovered in our center. While these changes could potentially be linked to the use of face masks, more observational and experimental studies are needed to explore and clarify this possible association.
Acknowledgments
The authors would like to thank Dr. Cláudia Oliveira-Ferreira (Department of Ophthalmology, Centro Hospitalar Universitário de São João, Porto, Portugal) for sharing the data regarding the microbiological profile of infectious keratitis in our center between 2009 and 2018, which were compared with the ones obtained in this paper.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395(10223):470–473.
2. Jahanbani-Ardakani H, Hosseini M, Almasi S, Khalili MR. Letter to the editor: face mask-associated dry eye in health care professionals amid the COVID-19 pandemic. Optom Vis Sci. 2021;98(8):995–996.
3. Scalinci SZ, Pacella E, Battagliola ET. Prolonged face mask use might worsen dry eye symptoms. Indian J Ophthalmol. 2021;69(6):1508–1510.
4. Fan Q, Liang M, Kong W, et al. Wearing face masks and possibility for dry eye during the COVID-19 pandemic. Sci Rep. 2022;12(1):6214.
5. Boccardo L. Self-reported symptoms of mask-associated dry eye: a survey study of 3605 people. Cont Lens Anterior Eye. 2022;45(2):101408.
6. Esen Baris M, Guven Yilmaz S, Palamar M. Impact of prolonged face mask wearing on tear break-up time and dry eye symptoms in health care professionals. Int Ophthalmol. 2022;42(7):2141–2144.
7. Giannaccare G, Pellegrini M, Borselli M, Senni C, Bruno A, Scorcia V. Diurnal changes of noninvasive parameters of ocular surface in healthy subjects before and after continuous face mask wearing during the COVID-19 pandemic. Sci Rep. 2022;12(1):12998.
8. Shalaby HS, Eldesouky MEE. Effect of facemasks on the tear film during the COVID-19 pandemic. Eur J Ophthalmol. 2022. doi:10.1177/11206721221110010
9. Moshirfar M, West WB
10. Krolo I, Blazeka M, Merdzo I, Vrtar I, Sabol I, Petric-Vickovic I. Mask-associated dry eye during COVID-19 pandemic-how face masks contribute to dry eye disease symptoms. Med Arch. 2021;75(2):144–148.
11. Kapelushnik N, Benyosef S, Skaat A, et al. The effect of face masks during COVID-19 pandemic on ocular surface temperature-a clinical thermographic analysis. Diagnostics. 2022;12(6):1431.
12. Nair S, Kaur M, Sah R, Titiyal JS. Impact of taping the upper mask edge on ocular surface stability and dry eye symptoms. Am J Ophthalmol. 2022;238:128–133.
13. Silkiss RZ, Paap MK, Ugradar S. Increased incidence of chalazion associated with face mask wear during the COVID-19 pandemic. Am J Ophthalmol Case Rep. 2021;22:101032.
14. Tang YF, Chong EWT. Face mask-associated recurrent corneal erosion syndrome and corneal infection. Eye Contact Lens. 2021;47(10):573–574.
15. Soleimani M, Masoumi A, Farrokhpour H, Keykhaei M, Zeidabadinejad H, Tabatabaei SA. Increased rate of infectious keratitis after PRK in the COVID-19 era: the possible role of face masks. J Refract Surg. 2022;38(2):78–81.
16. Angaramo S, Law JC, Maris AS, et al. Potential impact of oral flora dispersal on patients wearing face masks when undergoing ophthalmologic procedures. BMJ Open Ophthalmol. 2021;6(1):e000804.
17. Michaels L, Richardson J, Walkden A, Carley F. Impact of the COVID-19 pandemic on the incidence and characteristics of culture-positive microbial keratitis at a tertiary eye hospital in the UK. Clin Ophthalmol. 2022;16:2513–2519.
18. Oliveira-Ferreira C, Leuzinger-Dias M, Tavares-Ferreira J, Torrão L, Falcão-Reis F. Microbiological profile of infectious keratitis in a Portuguese tertiary centre. J Ophthalmol. 2019;2019:6328058.
19. Ferreira CS, Figueira L, Moreira-Gonçalves N, Moreira R, Torrão L, Falcão-Reis F. Clinical and microbiological profile of bacterial microbial keratitis in a Portuguese tertiary referral center-where are we in 2015? Eye Contact Lens. 2018;44(1):15–20.
20. Cunha AM, Loja JT, Torrão L, et al. A 10-year retrospective clinical analysis of fungal keratitis in a Portuguese tertiary centre. Clin Ophthalmol. 2020;14:3833–3839.
21. Ng AL-K, To KK-W, Choi CC-L, et al. Predisposing factors, microbial characteristics, and clinical outcome of microbial keratitis in a tertiary centre in Hong Kong: a 10-year experience. J Ophthalmol. 2015;2015:769436.
22. Hong J, Xu J, Hua J, Sun X. Bacterial keratitis in Shanghai. Ophthalmology. 2013;120(3):647.
23. Shalchi Z, Gurbaxani A, Baker M, Nash J. Antibiotic resistance in microbial keratitis: ten-year experience of corneal scrapes in the United Kingdom. Ophthalmology. 2011;118(11):2161–2165.
24. Pandita A, Murphy C. Microbial keratitis in Waikato, New Zealand. Clin Exp Ophthalmol. 2011;39(5):393–397.
25. Lichtinger A, Yeung SN, Kim P, et al. Shifting trends in bacterial keratitis in Toronto: an 11-year review. Ophthalmology. 2012;119(9):1785–1790.
26. Ung L, Bispo PJM, Shanbhag SS, Gilmore MS, Chodosh J. The persistent dilemma of microbial keratitis: global burden, diagnosis, and antimicrobial resistance. Surv Ophthalmol. 2019;64(3):255–271.
27. Ruoff KL, Toutain-Kidd CM, Srinivasan M, et al. Corynebacterium macginleyi isolated from a corneal ulcer. Infect Dis Rep. 2010;2(1):e3.
28. Farias R, Pinho L, Santos R. Epidemiological profile of infectious keratitis. Rev Bras Oftalmol. 2017;76(3):116–120.
29. Otri AM, Fares U, Al-Aqaba MA, et al. Profile of sight-threatening infectious keratitis: a prospective study. Acta Ophthalmol. 2013;91(7):643–651.
30. Roy P, Das S, Singh NP, et al. Changing trends in fungal and bacterial profile of infectious keratitis at a tertiary care hospital: a six-year study. Clin Epidemiology Glob Health. 2017;5(1):40–45.
31. Deo PN, Deshmukh R. Oral microbiome: unveiling the fundamentals. J Oral Maxillofac Pathol. 2019;23(1):122–128.
32. Aoki T, Kitazawa K, Deguchi H, Sotozono C. Current evidence for Corynebacterium on the ocular surface. Microorganisms. 2021;9(2):254.
33. Lim SA, Na KS, Joo CK. Clinical features of infectious keratitis caused by Propionibacterium acnes. Eye Contact Lens. 2017;43(5):330–333.
34. Sampo M, Ghazouani O, Cadiou D, Trichet E, Hoffart L, Drancourt M. Dolosigranulum pigrum keratitis: a three-case series. BMC Ophthalmol. 2013;13(1):31.
35. Wu YT, Zhu LS, Tam KP, Evans DJ, Fleiszig SM. Pseudomonas aeruginosa survival at posterior contact lens surfaces after daily wear. Optom Vis Sci. 2015;92(6):659–664.
36. Hilliam Y, Kaye S, Winstanley C. Pseudomonas aeruginosa and microbial keratitis. J Med Microbiol. 2020;69(1):3–13.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of the COVID-19 Pandemic on the Incidence and Characteristics of Culture-Positive Microbial Keratitis at a Tertiary Eye Hospital in the UK
Michaels L, Richardson J, Walkden A, Carley F
Clinical Ophthalmology 2022, 16:2513-2519
Published Date: 10 August 2022