Back to Journals » Infection and Drug Resistance » Volume 14
Metagenomic Next-Generation Sequencing for Pulmonary Fungal Infection Diagnosis: Lung Biopsy versus Bronchoalveolar Lavage Fluid
Authors Yang L ![]() , Song J, Wang Y
, Song J, Wang Y ![]() , Feng J
, Feng J
Received 17 August 2021
Accepted for publication 30 September 2021
Published 20 October 2021 Volume 2021:14 Pages 4333—4359
DOI https://doi.org/10.2147/IDR.S333818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Lei Yang,1 Junxiu Song,1 Yubao Wang,2 Jing Feng1
1Department of Respiratory and Critical Care Medicine, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China; 2Institute of Infectious Diseases, The Second Hospital of Tianjin Medical University, Tianjin, People’s Republic of China
Correspondence: Yubao Wang
Institute of Infectious Diseases, The Second Hospital of Tianjin Medical University, Pingjiang Road NO. 23, Tianjin, 300211, People’s Republic of China
Email [email protected]
Jing Feng
Department of Respiratory and Critical Care Medicine, Tianjin Medical University General Hospital, Anshan Road No. 154, Heping District, Tianjin, 300052, People’s Republic of China
Email [email protected]
Purpose: Metagenomic next-generation sequencing (mNGS) is widely used for pulmonary infection; nonetheless, the experience from its clinical use in diagnosing pulmonary fungal infections is sparse. This study aimed to compare mNGS results from lung biopsy and bronchoalveolar lavage fluid (BALF) and determine their clinical diagnostic efficacy.
Patients and Methods: A total of 106 patients with suspected pulmonary fungal infection from May 2018 to January 2020 were included in this retrospective study. All patients’ lung biopsy and BALF specimens were collected through bronchoscopy. Overall, 45 (42.5%) patients had pulmonary fungal infection. The performance of lung biopsy and BALF used for mNGS in diagnosing pulmonary fungal infections and identifying pathogens was compared. Additionally, mNGS was compared with conventional tests (pathology, galactomannan test, and cultures) with respect to the diagnosis of pulmonary fungal infections.
Results: Lung biopsy-mNGS and BALF-mNGS exhibited no difference in terms of sensitivity (80.0% vs 84.4%, P=0.754) and specificity (91.8% vs 85.3%, P=0.39). Additionally, there was no difference in specificity between mNGS and conventional tests; however, the sensitivity of mNGS (lung biopsy, BALF) in diagnosing pulmonary fungal infections was significantly higher than that of conventional tests (conventional tests vs biopsy-mNGS: 44.4% vs 80.0%, P< 0.05; conventional tests vs BALF-mNGS: 44.4% vs 84.4%, P< 0.05). Among 32 patients with positive mNGS results for both biopsy and BALF specimens, 23 (71.9%) cases of consistency between the two tests for the detected fungi and nine (28.1%) cases of a partial match were identified. Receiver operating curve analysis revealed that the area under the curve for the combination of biopsy and BALF was significantly higher than that for BALF-mNGS (P=0.018).
Conclusion: We recommend biopsy-based or BALF-based mNGS for diagnosing pulmonary fungal infections because of their diagnostic advantages over conventional tests. The combination of biopsy and BALF for mNGS can be considered when higher diagnostic efficacy is required.
Keywords: mNGS, diagnosis, sensitivity, specificity
Introduction
In recent years, with the increase in high-risk groups requiring immunosuppressant use, the prevalence of pulmonary fungal disease has shown a significant upward trend. The main sources of fungal infections in human lungs are opportunistic fungi: Aspergillus, Cryptococcus, Pneumocystis jirovecii, and endemic fungi. Among them, Aspergillus and Cryptococcus are the main fungal pathogens associated with lung infections.1 Microscopic smears and cultures are conventional microbial methods used for pathogen identification; however, both methods are time consuming and not highly sensitive. The gold standard for the detection of invasive fungal infections is histopathological diagnosis. However, it is time consuming, it cannot identify pathogens, and it has low sensitivity. For Aspergillus infections, the positive predictive value (PPV) of respiratory specimen cultures obtained by sputum induction or bronchoalveolar lavage fluid (BALF) is low (approximately 72%).2 When testing patients with non-hematological diseases or those who have been treated with antifungal drugs, the PPV may be even lower.3 Clinically, BALF’s galactomannan (GM) test results are affected by various factors, which can lower the sensitivity and increase the false positivity rate.4–7
Since the conventional tests for the diagnosis of pulmonary fungal infections have a low sensitivity and are influenced by various factors, there is an urgent need for new technology with a higher sensitivity for the diagnosis of pulmonary fungal infections. Currently, metagenomic next-generation sequencing (mNGS) is a widely used method for the clinical detection of pathogens and has obvious advantages in pathogen detection.8 One study showed that mNGS can improve the sensitivity of pathogen detection and that it is less affected by antibiotic exposure before detection.9 In the studies that used mNGS for the detection of lung infections,10–13 there have been advantages identified over traditional detection methods, indicating that mNGS can be used to detect lung infections. However, there is limited experience from the clinical use of mNGS in the diagnosis of pulmonary fungal infections.
In this study, we used bronchoscopy to obtain lung biopsy and BALF for mNGS from 106 patients with suspected pulmonary fungal infection to identify pathogens. We compared the mNGS results from lung biopsy and BALF to specifically determine the difference between the two mNGS results and the clinical diagnostic efficacy. Additionally, mNGS (BALF) was compared with conventional tests (pathology, GM test, and cultures).
Patients and Methods
Specimen Collection and Processing
The present study is a retrospective cohort study. Patients admitted to the Respiratory Department at Tianjin Medical University General Hospital for suspected pulmonary fungal infection from May 2018 to January 2020 provided informed consent to undergo bronchoscopy and mNGS. Experienced physicians collected the patient’s lung biopsy and BALF specimens through bronchoscopy based on canonical operational procedures.14 During bronchoscopy, the operating physician recorded complications such as bleeding, fatal hemoptysis, arrhythmia, and death. Six to ten lung biopsy specimens collected from the enrolled patients were used for pathology, rapid on-site evaluation (ROSE), and mNGS. Within 2 hours, the lung biopsy specimens were sent to the histopathology laboratory and then processed using standard procedures.15 The remaining lung biopsy specimens were stored at −80°C for mNGS. Part of the BALF was used for fungal and bacterial culture. Another part of the BALF was used for Xpert MTB, GM test, and smear. The remaining BALF specimens were stored at −80°C for mNGS.
mNGS and Analyses
The TIANamp Micro DNA Kit (DP316, TIANGEN BIOTECH) was used to extract the DNA from the BALF and lung biopsy homogenates based on the company’s recommendation. DNA libraries were constructed based on the Beijing Genomics Institute sequencer-100. By removing low-quality and shorter (<35 bp) readings, high-quality sequencing data were generated. Burrows-Wheeler Aligner software was applied to map to a human reference (hg19) to identify human sequence data. Microbial genome databases were used to classify the remaining data.9,16,17 The classification reference databases were downloaded from NCBI (ftp://ftp.ncbi.nlm.nih.gov/genomes/).
Criteria of Diagnosis of Pulmonary Fungal Infection
Pulmonary fungal infection was defined based on the European Organization for Research and Treatment of Cancer (EORTC)/Mycoses Study Group (MSG) criteria.18 In our study, for proven Invasive Fungal Disease (IFDs), histopathological findings of hyphae on lung biopsy were considered an IFI diagnosis, and this criterion was adapted for any patient. For probable IFDs, experts in the respiratory department of our hospital reviewed the chest CT images of pulmonary fungal infection, which was one of the clinical diagnostic criteria, and evaluated possible mycological evidence such as the GM antigen test. Patients with no proven or probable IFDs throughout the study period were categorized as exclude IFDs.
The pathogen responsible for the fungal infections was diagnosed if it met any of the following thresholds. First, culture and/or histopathological examination positive for fungi; it is strongly recommended to use BALF GM to diagnose invasive pulmonary aspergillosis in immunosuppressed patients.4 Second, at least 50 unique reads from a single species of fungi; for pathogens with unique reads less than 50, the diagnosis of pulmonary fungal infection can still be made based on the clinical situation.13
Statistical Analysis
In order to determine the sensitivity, specificity, PPV, and negative predictive value (NPV), 2×2 contingency tables were derived. All data are reported as the absolute value of their 95% confidence intervals (CI). Diagnostic accuracy of pulmonary fungal infections based on the fungal reads from mNGS and area under the curve (AUC) was calculated after conducting the corresponding receiver operating characteristic (ROC) curve analysis. Data were analyzed using SPSS 26.0 (IBM Corp., Armonk, NY, USA) and MedCalc 19 (MedCalc Software Ltd., Ostend, Belgium). P-values <0.05 were considered statistically significant.
Ethics
The study was approved by the Ethics Committee of Tianjin Medical University General Hospital. The need for informed consent was waived due to the retrospective nature of the study and because the data were anonymously analyzed.
Results
Patient Characteristics and mNGS Results
Overall, 106 patients were included in the study; 76 (71.7%) were males, and the average age was 43.2±18.5 years. Eighty-four (79.3%) patients had immunocompromised function, and 79 of them suffered from hematological diseases (Table 1). In total, 45 (42.5%) patients were diagnosed with pulmonary fungal infections (Table 2 and Figure 1).
 |
Table 1 Patient Demographic Characteristics |
 | 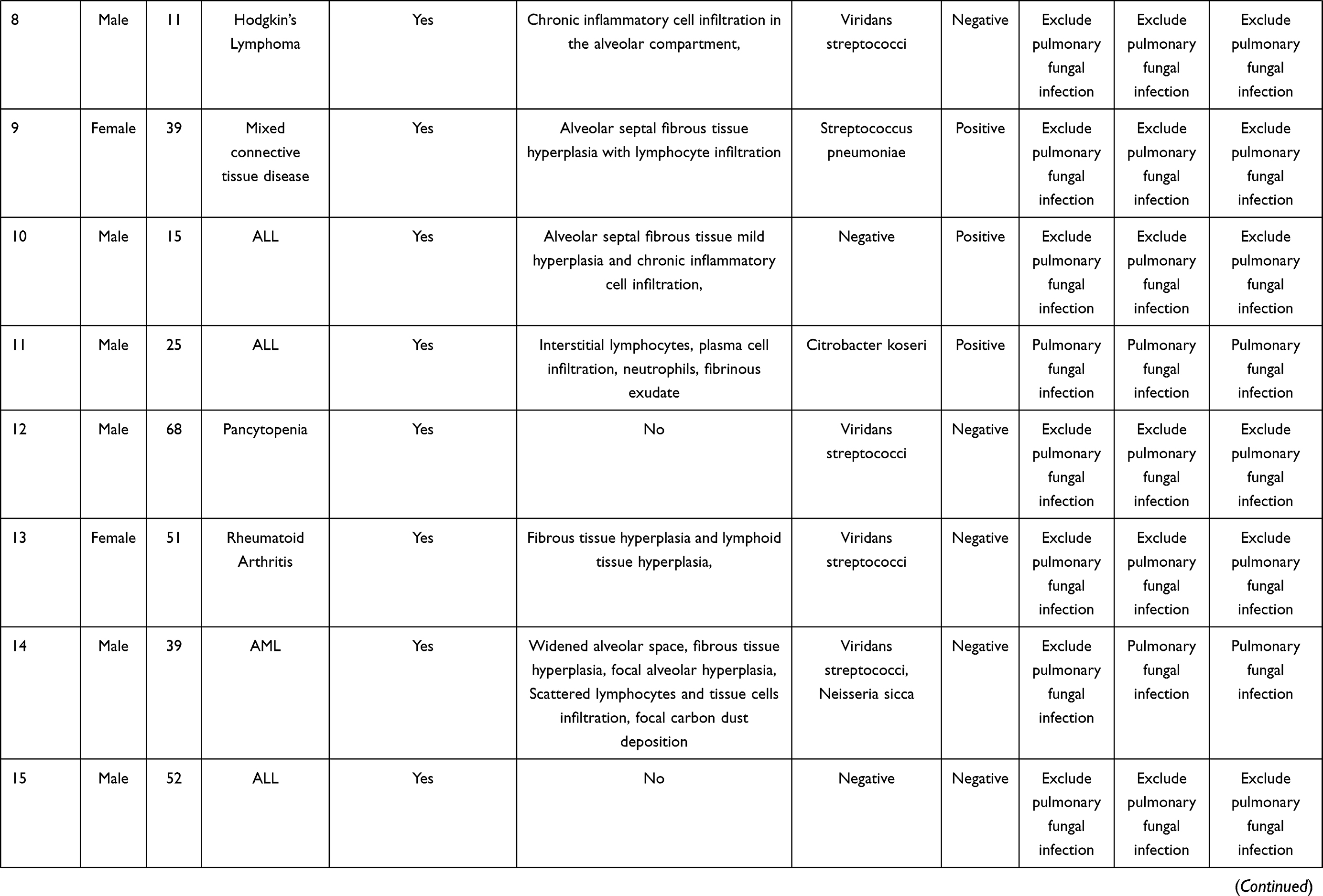 |  |  |  |  | 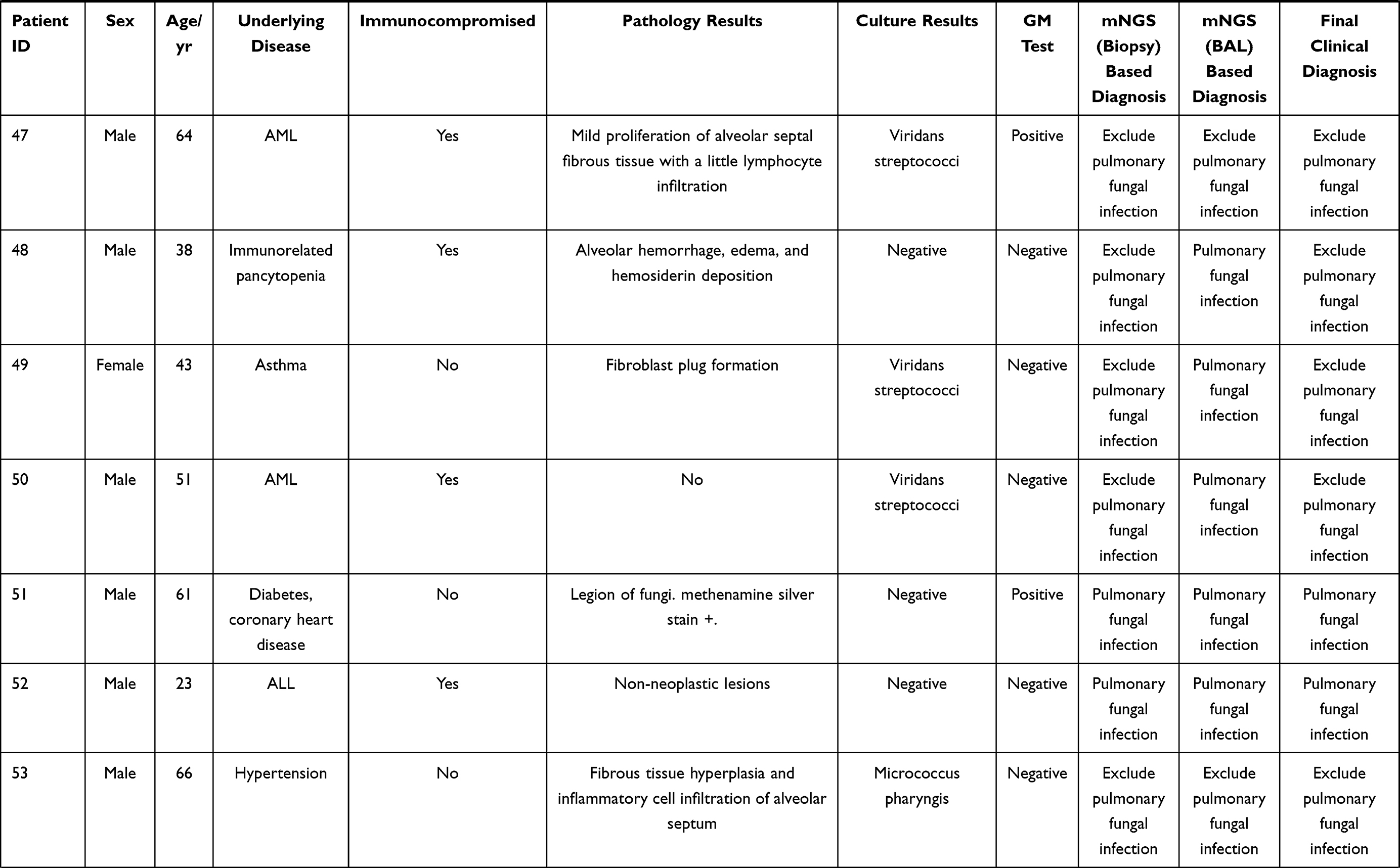 |  |  |  |  |  |  |
Table 2 |
 |
Figure 1 Methods used to diagnose pulmonary fungal infections. |
Comparison Between mNGS and Conventional Tests
Among the 106 patients with suspected pulmonary fungal infection, the diagnostic efficacy of mNGS for lung biopsy and BALF is shown in Table 3. The sensitivity and specificity of lung biopsy-mNGS for the diagnosis of pulmonary fungal infections were 80.0% (95% CI, 65.0–89.9%) and 91.8% (95% CI, 81.2–96.9%), and the PPV and NPV were 87.8% (95% CI, 73.0–95.4%) and 86.2% (95% CI, 74.8–93.1%), respectively. The sensitivity and specificity of BALF-mNGS for the diagnosis of pulmonary fungal infections were 84.4% (95% CI, 69.9–93.0%) and 85.3% (95% CI, 73.3–92.6%), and the PPV and NPV were 80.9% (95% CI, 66.3–90.4%) and 88.1% (95% CI, 76.5–94.7%), respectively.
 |
Table 3 Performance of mNGS and the Conventional Test in the Diagnosis of Pulmonary Fungal Infections |
The sensitivity and specificity of conventional tests in diagnosing pulmonary fungal infections were 44.4% (95% CI, 30.0–59.9%) and 88.5% (95% CI, 77.2–94.9%), whereas the PPV and NPV were 74.1% (95% CI, 53.4–88.1%) and 68.4% (95% CI, 56.8–78.1%), respectively. There was no significant difference in the specificity between mNGS and conventional tests; however, the sensitivity of mNGS (lung biopsy, BALF) in diagnosing pulmonary fungal infections was significantly higher than that of conventional tests (conventional tests vs biopsy-mNGS: 44.4% vs 80.0%, P<0.05; conventional tests vs BALF-mNGS: 44.4% vs 84.4%, P<0.05) (Table 3). There were no fungi detected based on the mNGS results for specimens obtained from three patients (patient nos. 91, 101, and 105); nevertheless, the presence of fungi was confirmed in the pathology or culture results. Both mNGS (BALF) and traditional detection methods were positive for pulmonary fungal infections in 19 patients. The pathology of the lung biopsy for 11 patients revealed fungal hyphae. Among all fungal cultures, the fungal culture results for six patients suggested the growth of mold. Of the 10 positive results using BALF from the GM test, six were false positives.
Lung Biopsy and BALF for mNGS
ROC analysis of biopsy-mNGS and BALF-mNGS for the diagnosis of pulmonary fungal infections yielded an AUC of 0.8663 (95% CI, 0.8122–0.9605) and 0.8632 (95% CI, 0.7879–0.9385), respectively (Table 4). Additionally, ROC analysis of mNGS (combination of biopsy and BALF) for the diagnosis of pulmonary fungal infections yielded an AUC of 0.929 (95% CI, 0.862–0.970) (Table 4). When the threshold was greater than 0.3022, the sensitivity and specificity of mNGS (combination of biopsy and BALF) were 77.8% (95% CI, 62.9–88.8%) and 95.1% (95% CI, 86.3–99%), respectively. Pairwise ROC curves are shown in Figure 2 and Table 5. The difference in AUC of the two mNGS was only 0.0231 (P=0.5748). The difference in the AUC between mNGS (combination of biopsy and BALF) and lung biopsy-mNGS was 0.0423 (P=0.0509). Finally, the difference in AUC between mNGS (combination of biopsy and BALF) and BALF-mNGS was 0.0654 (P=0.018).
 |
Table 4 Comparison of the ROC for mNGS and the Conventional Tests |
 |
Table 5 Comparison of the Difference in the AUC |
 |
Figure 2 Pairwise comparison of the ROC curves. Abbreviation: ROC, receiver operating characteristic. |
The mNGS provided specific sequencing reads of all microorganisms and valid data that can be detected in the sample. Based on the definition for the pathogens responsible for fungal infections, in combination with the patient’s clinical data to exclude some fungi considered for colonization, this study detected pulmonary fungal infections caused by Rhizopus microsporus, Aspergillus flavus, Aspergillus oryzae, Aspergillus fumigatus, Rhizomucor pusillus, and Pneumocystis jirovecii. In lung biopsy-mNGS, most of the fungi detected were Aspergillus oryzae, Aspergillus flavus, Pneumocystis jirovecii, Rhizomucor pusillus, and Aspergillus fumigatus (Figure 3A). In mNGS (BALF), most of the fungi detected were Pneumocystis jirovecii, Aspergillus fumigatus, Aspergillus oryzae, Aspergillus flavus, and Rhizomucor pusillus (Figure 3B). The sequencing reads for fungi produced by each sample ranged from 2 to 522,197.
 |
Figure 3 (A) Fungi detected using lung biopsy-mNGS. (B) Fungi detected using BALF-mNGS. Abbreviations: BALF, bronchoalveolar lavage fluid; mNGS, metagenomic next-generation sequencing. |
The lung biopsy and BALF results for mNGS were positive for the diagnosis of lung fungal infection in 33 cases. The lung biopsy and BALF from patient no. 54 were used for mNGS to detect Aspergillus and Mycobacterium; however, the final clinical diagnosis was tuberculosis. Both tests were negative for the diagnosis of pulmonary fungal infection in 51 patients. Eight cases were positive for pulmonary fungal infections using mNGS (biopsy) only, and 14 cases were positive for pulmonary fungal infections using mNGS (BALF) only. In 14 cases, we found that Pneumocystis jiroveci was detected by mNGS (BALF) in patient no. 58; however, the final diagnosis was cryptococcal infection. Among the 32 patients whose final diagnoses were pulmonary fungal infections and mNGS results were positive, 23 (71.88%) cases of consistency between the two detected fungi and nine (28.13%) cases of a partial match were identified (Figure 4). With respect to the partially matched results, the mNGS results of the two specimens did not appear to be completely different; nevertheless, they were partially contained.
 |
Figure 4 Consistency of the two specimens for mNGS in diagnosing pulmonary fungal infections. The pie chart shows the positive distribution of 106 cases investigated for pulmonary fungal infections using lung biopsy and BALF for mNGS. Among the patients whose mNGS results matched for both specimens, the mNGS results of nine patients showed partial matches, 24 patients showed complete matches, but 54 patients had false-positive results. Abbreviations: BALF, bronchoalveolar lavage fluid; mNGS, metagenomic next-generation sequencing. |
Among 45 patients with a final diagnosis of pulmonary fungal infection, the results from lung biopsy and BALF for mNGS were positive in 32 (75%) patients (Table 6). When multiple types of fungi were detected by mNGS for the two specimens, the fungi with the largest reads were recorded and compared. Among 32 patients with positive mNGS results for both specimens, 27 (84.38%) had more reads of fungi detected by lung biopsy-mNGS than by BALF-mNGS (Figures 5 and 6). In 17 (53.13%) patients, fungal reads detected by lung biopsy-mNGS were more than 10 times greater than those by BALF-mNGS. In 10 patients, the fungal reads detected by lung biopsy-mNGS were between 1 and 10 times greater than those detected by BALF-mNGS. In patient no. 16, the fungal reads detected by BALF-mNGS were significantly greater than those by lung biopsy-mNGS. The fungal reads detected by BALF-mNGS were approximately the same as those by lung biopsy in five patients.
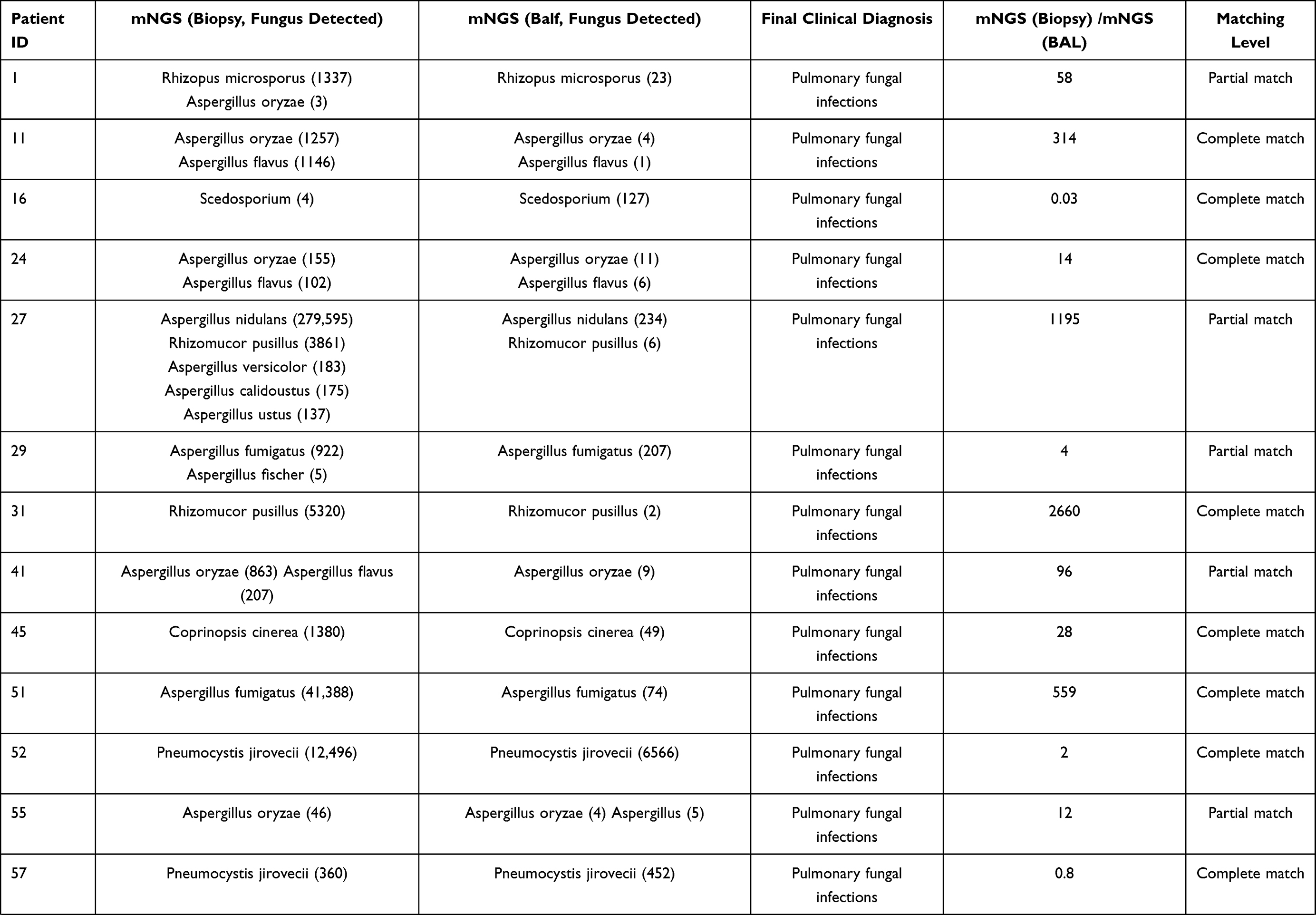 |  |  |
Table 6 Results of the 32 Patients with Matching mNGS Results |
 |
Figure 5 Comparison of the fungal reads detected by lung biopsy and BALF for mNGS. Multiple interval: mNGS (Biopsy) most detected fungal reads/mNGS (BAL) most detected fungal reads. Abbreviations: BALF, bronchoalveolar lavage fluid; mNGS, metagenomic next-generation sequencing. |
 |
Figure 6 Comparison of the fungal reads detected by mNGS with matching results from both specimens in 32 patients. Abbreviation: mNGS, metagenomic next-generation sequencing. |
The information from the 22 patients with inconsistent mNGS results is shown in Table 7. Among the eight and 13 cases with positive lung biopsy-mNGS and positive BALF-mNGS, four and five cases were eventually diagnosed with pulmonary fungal infections, respectively. Among the above mentioned 22 patients, 12 patients had false-positive mNGS results. Only four and eight cases had positive lung biopsy-mNGS and BALF-mNGS results, respectively. Among the false positive cases, Aspergillus, Pneumocystis jejuni, and Candida albicans were most frequently detected, and in 10 (83.33%) patients, the mNGS reads were less than 20. In patients with false positive results, there was a greater frequency of BALF-mNGS cases than lung biopsy-mNGS; however, this difference was not significant (P>0.05).
 |
Table 7 Sequencing Results for 22 Patients with Inconsistent Lung Biopsy-mNGS and BALF-mNGS |
Complications in Bronchoscopy
Among the 106 patients included in this study, lung biopsy and BALF were performed at the same time. During transbronchial lung biopsy, a small amount of bleeding was observed under bronchoscopy in eight patients. After instilling hemocoagulase was injected into the bleeding bronchus through the bronchoscope, no active bleeding was observed under the bronchoscope, and the patient’s safety was not threatened. Among the 106 patients who underwent bronchoscopy, none experienced any complications, including fatal hemoptysis, pneumothorax, arrhythmia, and death.
Discussion
Among high-risk groups of patients with immunosuppression, empirical antifungal therapy is becoming increasingly common, which makes the diagnosis of pulmonary fungal infections more difficult.19 mNGS has been widely used in infectious diseases, but there is a lack of evidence regarding its use in pulmonary fungal infections. Therefore, this study aimed to address this gap and compare the difference between lung biopsy and BALF for mNGS. A previous study reported that mNGS was better than cultures in diagnosing pulmonary fungal infections (OR, 4.0 [95% CI, 1.6–10.3], P<0.01).9 In the current study, the specificity of conventional tests did not differ compared to mNGS (conventional tests vs biopsy-mNGS: 88.52% vs 91.8%, P>0.05; conventional tests vs BALF-mNGS: 88.52% vs 85.25%, P>0.05), but the sensitivity of mNGS significantly differed (conventional tests vs biopsy-mNGS: 44.44% vs 80.00%, P<0.05; conventional test vs BALF-mNGS: 44.44% vs 84.44%, P<0.05). The PPV and NPV of conventional tests were 74.07% (95% CI, 53.41–88.13%) and 68.35% (95% CI, 56.80–78.11%), respectively. Since patients with immunodeficiencies were treated with antifungal therapy before the test, the positivity rate of the conventional tests was very low. Compared with the conventional tests, it has been previously reported that mNGS is less affected by antibiotic exposure before detection,9 and that mNGS can detect corresponding pathogens, which is beneficial for targeted treatment.
Reviewing the relevant literature, there are many studies on single lung biopsy or BALF for mNGS in pulmonary infections,10,12 but few studies have evaluated simultaneous mNGS using lung biopsy and BALF specimens to diagnose pulmonary fungal infections. In this study involving 106 patients with suspected pulmonary fungal infection, mNGS detected fungi in the lung biopsy and/or BALF of 55 patients. The sensitivity of lung biopsy and BALF for mNGS in diagnosing pulmonary fungal infections was 80.00% (95% CI, 64.95–89.91%) and 84.44% (95% CI, 69.94–93.01%), whereas their specificity was 91.8% (95% CI, 81.17–96.94%) and 85.25% (95% CI, 73.32–92.62%), respectively; however, these values did not show significant difference (P>0.05). The smaller difference between the two samples in terms of sensitivity might be explained by the fungal infection method (filamentous fungi spread on the surface of lung tissue, and it is often difficult to wash pathogens off using lavage) and the scope of the alveolar lavage (bronchoalveolar lavage involves more lobe segments and more distant sub-segment bronchi). The positivity rate of lung biopsy-mNGS mainly depends on the location of the lesion, such as whether the lesion is connected to the bronchus or close to the surrounding area. In this study, with the assistance of virtual navigation and ROSE, the sensitivity of mNGS (lung biopsy and BALF) was relatively high. ROC analysis of lung biopsy-mNGS for the diagnosis of pulmonary fungal infections yielded an AUC of 0.8663 (95% CI, 0.8122–0.9605). ROC analysis of BALF-mNGS for the diagnosis of pulmonary fungal infections yielded an AUC of 0.8632 (95% CI, 0.7879–0.9385). The difference in the AUC of the two samples evaluated using mNGS was only 0.0.231 (P=0.5748). These findings highlight that mNGS (regardless of whether the test specimen was a lung biopsy or BALF) is a better detection method for the diagnosis of pulmonary fungal infections. The difference in the AUC between the mNGS (combination of biopsy and BALF) and the mNGS (lung BALF) was 0.0654 (P=0.018). Thus, we found that mNGS (combination of biopsy and BALF) had a better diagnostic value than BALF-mNGS. The difference in the AUC between the mNGS (combination of biopsy and BALF) and the mNGS (lung biopsy) was 0.0423 (P=0.0509). Thus, the mNGS (combination of biopsy and BALF) was not better than the lung biopsy-mNGS, possibly because the sample size was not large enough to show a significant difference.
The study detected fungal infections of the lungs caused by Rhizopus microsporus, Aspergillus flavus, Aspergillus oryzae, Aspergillus fumigatus, Rhizomucor pusillus, and Pneumocystis jirovecii. These findings are similar to those reported by Li et al,1 but the current study only identified one case of cryptococcal infection. In this study, among 32 patients whose lung biopsy and BALF were both positive on the basis of mNGS and were thus diagnosed with pulmonary fungal infection, 23 (71.88%) cases of a complete match between the two detected fungi and nine (28.13%) cases of a partial match were identified. The results from the two different specimens did not completely differ; however, the mNGS results matched completely or contained each other. The findings of this study indicated that lung biopsy and BALF for mNGS showed specific consistency in fungal detection. Out of 32 patients with positive mNGS results for both specimens, 27 (84.38%) had more reads of fungi detected by lung biopsy-mNGS than by BALF-mNGS. Reads of fungi detected by lung biopsy-mNGS were more than 10 times greater than those detected by BALF-mNGS in 17 (53.13%) patients. These findings suggest that the reads of fungi detected by BALF-mNGS were generally small, which may be related to the fungal infection method (filamentous fungi spread on the surface of lung tissue, and it is often difficult to wash pathogens off using lavage). When lung tissues are obtained from the target site of the lesion and used for mNGS, the fungal reads can be detected several times higher than that with BALF.
In this study, 22 patients had inconsistent results from lung biopsy-mNGS and BALF-mNGS. The mNGS results were positive for lung biopsy and negative for BALF in eight patients; this might be attributed to the fact that the fungi are filamentous and spread on the tissue surface, which is difficult to wash down using bronchoalveolar lavage. Furthermore, the mNGS results were negative for lung biopsy and positive for BALF in 14 patients, which might be explained by the fact that the bronchi are not connected to the lesion site or the lesion tissue is not obtained; however, the alveolar lavage involves a wider range. Since the lavage fluid involves more leaf segments and a more distant sub-segment bronchus, which involves a wider range, we found that BALF-mNGS had more false positive results than lung biopsy. However, this difference was not significant (P>0.05), which may be a result of the small sample size.
This study was subject to several limitations which merit mentioning here. To date, the mNGS test used in this study has been delivered to commercial laboratories, but not to the hospital’s microbiology laboratory. This may increase the turnaround time and reduce the storage capacity, thus reducing the sensitivity of the test. Additionally, the sample size included in this study was not large, which caused a slight deviation in the ROC curve drawn.
Conclusion
This study showed that mNGS has obvious advantages when compared with conventional tests in pulmonary fungal infection. Additionally, there is no difference in diagnostic performance between lung-biopsy-mNGS and BALF-mNGS. However, lung-mNGS can generally detect several times the fungal reads when compared to BALF-mNGS. Lung biopsy or BALF for mNGS is recommended for patients with suspected pulmonary fungal infection to identify the pathogen as early as possible. The combination of biopsy and BALF for mNGS may be considered when higher diagnostic efficacy is required.
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li Z, Lu G, Meng G. Pathogenic fungal infection in the lung. Front Immunol. 2019;10. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6616198/.
2. Arvanitis M, Mylonakis E. Diagnosis of invasive aspergillosis: recent developments and ongoing challenges. Eur J Clin Invest. 2015;45(6):646–652. doi:10.1111/eci.12448
3. Perfect JR, Cox GM, Lee JY, et al. The impact of culture isolation of Aspergillus species: a hospital‐based survey of aspergillosis. Clin Infect Dis. 2001;33(11):1824–1833. doi:10.1086/323900
4. Hage CA, Carmona EM, Epelbaum O, et al. Microbiological laboratory testing in the diagnosis of fungal infections in pulmonary and critical care practice. An official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2019;200(5):535–550. doi:10.1164/rccm.201906-1185ST
5. Surmont I, Stockman W. Gluconate-containing intravenous solutions: another cause of false-positive galactomannan assay reactivity. J Clin Microbiol. 2007;45(4):1373. doi:10.1128/JCM.02373-06
6. Hage CA, Reynolds JM, Durkin M, Wheat LJ, Knox KS. Plasmalyte as a cause of false-positive results for Aspergillus galactomannan in bronchoalveolar lavage fluid. J Clin Microbiol. 2007;45(2):676–677. doi:10.1128/JCM.01940-06
7. Racil Z, Kocmanova I, Lengerova M, Winterova J, Mayer J. Intravenous PLASMA-LYTE as a major cause of false-positive results of platelia aspergillus test for galactomannan detection in serum. J Clin Microbiol. 2007;45(9):3141–3142. doi:10.1128/JCM.00974-07
8. Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for pathogen detection. Annu Rev Pathol Mech Dis. 2019;14(1):319–338. doi:10.1146/annurev-pathmechdis-012418-012751
9. Miao Q, Ma Y, Wang Q, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. 2018;67(suppl_2):S231–S240. doi:10.1093/cid/ciy693
10. Li Y, Sun B, Tang X, et al. Application of metagenomic next-generation sequencing for bronchoalveolar lavage diagnostics in critically ill patients. Eur J Clin Microbiol Infect Dis off Publ Eur Soc Clin Microbiol. 2020;39(2):369–374. doi:10.1007/s10096-019-03734-5
11. Zhang H-C, Ai J-W, Cui P, et al. Incremental value of metagenomic next generation sequencing for the diagnosis of suspected focal infection in adults. J Infect. 2019;79(5):419–425. doi:10.1016/j.jinf.2019.08.012
12. Li H, Gao H, Meng H, et al. Detection of pulmonary infectious pathogens from lung biopsy tissues by metagenomic next-generation sequencing. Front Cell Infect Microbiol. 2018;8:205. doi:10.3389/fcimb.2018.00205
13. Wang J, Han Y, Feng J. Metagenomic next-generation sequencing for mixed pulmonary infection diagnosis. BMC Pulm Med. 2019;19(1):252. doi:10.1186/s12890-019-1022-4
14. Meyer KC, Raghu G, Baughman RP, et al. An official American Thoracic Society Clinical Practice Guideline: the clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am J Respir Crit Care Med. 2012;185(9):1004–1014. doi:10.1164/rccm.201202-0320ST
15. Huang J, Jiang E, Yang D, et al. Metagenomic next-generation sequencing versus traditional pathogen detection in the diagnosis of peripheral pulmonary infectious lesions. Infect Drug Resist. 2020;13:567–576. doi:10.2147/IDR.S235182
16. Li H, Durbin R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinforma Oxf Engl. 2009;25(14):1754–1760. doi:10.1093/bioinformatics/btp324
17. Wang J, Xu H, Li Z, et al. Pathogens in patients with granulomatous lobular mastitis. Int J Infect Dis. 2019;81:123–127. doi:10.1016/j.ijid.2019.01.034
18. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the European organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
19. Li N, Cai Q, Miao Q, Song Z, Fang Y, Hu B. High‐throughput metagenomics for identification of pathogens in the clinical settings. Small Methods. 2021;5(1):2000792. doi:10.1002/smtd.202000792
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.