Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Metabolic Syndrome and Associated Risk Factors in Norwegian Trauma-Exposed Inpatients: A Cross-Sectional Comparison with Blood Donors
Authors Roer GE ![]() , Bolstad I
, Bolstad I ![]() , Abebe DS, Aaseth J
, Abebe DS, Aaseth J ![]() , Haugen M
, Haugen M ![]() , Lien L
, Lien L
Received 23 May 2025
Accepted for publication 24 July 2025
Published 4 August 2025 Volume 2025:18 Pages 2667—2680
DOI https://doi.org/10.2147/DMSO.S536015
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Grethe Emilie Roer,1,2 Ingeborg Bolstad,3 Dawit Shawel Abebe,1,2 Jan Aaseth,3,4 Morten Haugen,5,6 Lars Lien1,3
1Research Center for Substance Use Disorders and Mental Illness, Innlandet Hospital Trust, Brumunddal, NO-2381, Norway; 2Department of Nursing and Health Promotion, Oslo Metropolitan University, Oslo, NO-0130, Norway; 3Faculty of Social and Health Sciences, University of Inland Norway, Elverum, NO-2418, Norway; 4Research Department, Innlandet Hospital Trust, Brumunddal, NO-2381, Norway; 5Department of Blood Centre and Laboratory Medicine, Innlandet Hospital Trust, Brumunddal, NO-2381, Norway; 6Faculty of Medicine, University of Oslo, Blindern, Oslo, NO-0316, Norway
Correspondence: Grethe Emilie Roer, Research Center for Substance Use Disorders and Mental Illness, Innlandet Hospital Trust, P. O. Box 104, Brumunddal, N-2381, Norway, Email [email protected]
Purpose: The incidence of metabolic syndrome (MetS) is increasing, and research indicates a further increased risk of MetS in trauma-exposed individuals, which is yet to be fully understood. Therefore, this study aimed to investigate the risk of MetS in trauma-exposed inpatients compared to blood donors and the influence of putative associated psychological, biological, and behavioral risk factors for MetS.
Patients and Methods: A cross-sectional study of trauma-exposed inpatients (n = 134) compared to blood donors (n = 68) was conducted. Clinical data, blood biomarkers, and self-administered questionnaires were collected. Descriptive statistics and multivariable logistic regression, including interaction analyses, were performed to explore the odds ratio (OR) of MetS among trauma-exposed inpatients compared to blood donors as well as the interaction effects of putative risk factors.
Results: A significantly higher age- and gender adjusted OR (OR = 2.51, 95% CI 1.18– 5.34) of MetS was found among trauma-exposed inpatients compared to the blood donors. Adjusted for education, cigarette smoking, symptoms of disordered eating and consumption of selected nutrients, the higher OR of MetS remained significant in the inpatients compared to the blood donors, ranging from OR = 2.27 95% CI 1.00– 5.14 for symptoms of “dieting” to OR = 3.06 95% CI 1.16– 8.10 for adult trauma. A significant interaction effect was documented only between group and age (OR = 1.07, 95% CI 1.01– 1.13).
Conclusion: The trauma-exposed inpatients in this study had significantly higher age- and gender adjusted risk of MetS compared to the blood donors, and psychological and behavioral lifestyle factors appeared to increase the risk of MetS.
Keywords: insulin resistance, metabolism, type 2 diabetes mellitus, mental disorders, posttraumatic stress, disordered eating
Introduction
Metabolic syndrome (MetS), defined as a cluster of metabolic risk factors (ie, abdominal obesity; hyperglycemia; hypertriglyceridemia; hypertension; and low high-density lipoprotein (HDL) cholesterol levels),1 is a growing public health concern with increased prevalence in the last decades.2 The incidence of MetS is often parallel with obesity and type 2 diabetes mellitus (T2DM), which have increased worryingly in the last decades, especially in urban areas.2 MetS increases the risk of T2DM, cardiovascular diseases (CVD) and early death.3 During the past decades, the impact of trauma exposure on physical health has received more attention, and there is a growing body of evidence that trauma exposure and posttraumatic stress disorder (PTSD) are associated with an increased risk of MetS.4–8 A recent 9-year longitudinal study found that childhood trauma was associated with poorer metabolic health outcome.9
The association between trauma exposure and risk of MetS, however, consists of a complex interaction between biological, psychological, and behavioral risk factors, which are not yet fully understood.10,11 Lifestyle factors (eg, nutrition; physical activity; alcohol use; and cigarette smoking) are widely known to impact the risk of MetS.12–15 With studies documenting health risk behaviors after traumatic experiences,16,17 such as poorer diet, and unhealthy consumption of alcohol, physical inactivity, and cigarette smoking,16–19 it is reasonable to assume that these behaviors contribute to the increased risk of MetS, and thus T2DM, and CVD in trauma-exposed individuals. However, the effect of dietary intake in the relationship between trauma and metabolic health outcomes is less consistent.19 Trauma-exposure can disrupt stress regulation and promote maladaptive coping behaviors, such as disordered eating behavior. A recent qualitative study20 by our group documented trauma-exposed inpatients experiences with the impact of traumatic stress on eating behavior, which over time may increase the risk of metabolic dysfunction. Although some research has linked trauma-exposure to increased risk of MetS, few studies have focused specifically on trauma-exposed inpatients, a population likely to have severe and/or complex trauma histories. Moreover, less is known about how psychological (eg, symptoms of disordered eating) and behavioral (eg, smoking, diet, physical activity) risk factors interact with trauma-exposure to influence MetS risk. Therefore, this study aimed to explore the risk of MetS in trauma-exposed inpatients compared with blood donors and the interaction effect of putative risk factors for MetS.
Materials and Methods
Study Design
A cross-sectional study, based on self-reported surveys as well as clinical and biological measures, was performed. The present study is part of a research project exploring the association between traumatic experiences and risk of MetS and T2DM.
Participants, Recruitment and Study Setting
Figure 1 illustrates the flow of the study sample. Trauma-exposed adult (≥18 years) inpatients, both male and female, were recruited from a psychiatric clinic in South-Eastern Norway from November 3rd, 2020, to February 22nd, 2023. All patients in the study had a history of traumatic experiences and had received treatment for severe trauma-related disorders in the specialist health service for many years. According to the criteria for receiving treatment at the clinic, the inpatients had no current severe symptoms of psychosis, severe eating disorders, and/or self-harm, acute suicidality, substance use, or violent behaviors. Additional exclusion criteria for the inpatients were lack of trauma history, pregnancy, type 1 diabetes mellitus, age ≥70 years, lack of consent competence, language barriers, and substantial amount of missing data. All inpatients admitted during the inclusion period were offered the opportunity to participate in the study, if not excluded due to the exclusion criteria. The total number of unique admissions to the clinic during the study inclusion period was 200 of which 142 consented to participate, four withdrawn their consent to participate and four were excluded after inclusion due to the exclusion criteria. The clinic offers inpatient treatment to adults (≥18 years) with severe mental disorders such as PTSD, anxiety, and depression. The clinic has 26 beds where patients receive intensive psychological treatment for a period of three months.
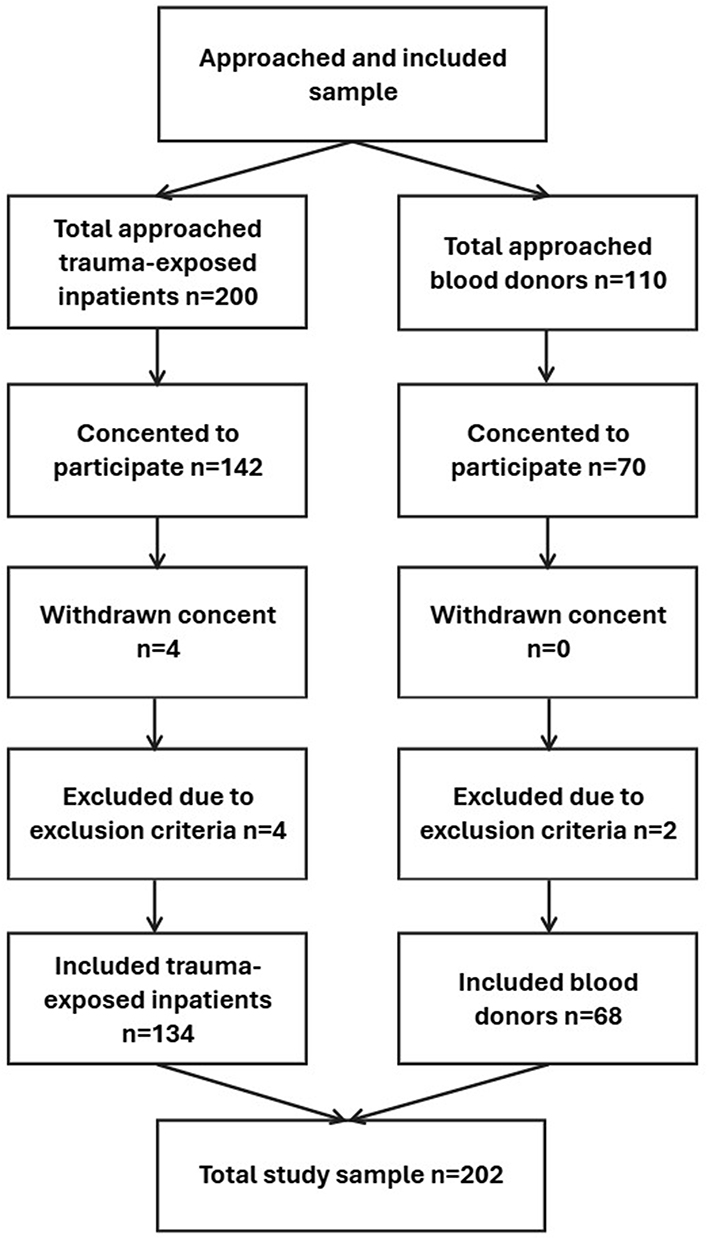 |
Figure 1 Study sample flow chart. |
Adult (≥18 years) blood donors, both male and female, were recruited as a comparison group from the Blood Center at Innlandet Hospital Trust in the period August 2022–October 2022. During this period, a total of six days were allocated to recruit blood donors. The exclusion criteria for the blood donors were pregnancy, type 1 diabetes mellitus, age ≥70 years, lack of consent competence, language barriers, and substantial amount of missing data. All blood donors scheduled to donate blood on these specific days were invited to participate in the study, if not excluded due to the exclusion criteria. The total number of blood donors donating blood these days was 110 and 70 consented to participate. Afterwards, two blood donors were excluded due to the exclusion criteria. In general, active blood donors represent a healthy population that is easily accessible, making it simpler, more efficient, and more cost-effective to collect data or biological material from them compared to a randomly selected group.
Data Collection
Of practical reasons, self-administered questionnaires were completed by trauma-exposed inpatients either on paper or in digital form. The blood donors answered all questionnaires in paper form. A nurse at the clinic instructed the participants (inpatients and blood donors) in completing the questionnaires and dietary record. The inpatients and blood donors returned their answers over a period of approximately two to three weeks.
For the inpatients, clinical measurements (height (cm); weight (kg); waist circumference (cm); blood pressure; fasting blood samples) were collected by a nurse at the clinic between 07.00 and 08.00 am during the first 14 days of their stay. The blood samples were centrifuged directly and sent to the laboratory for analysis on the same day. For blood donors, clinical measurements (ie, weight (kg); waist circumference (cm); and blood pressure) were collected by the same nurse immediately before donating blood at varying times throughout the day. The height (cm) was self-reported. Blood pressure was measured after sitting down for 5–10 minutes. The participants were instructed not to speak during blood pressure measurement. Weight was measured in the absence of a jacket/large jumper, belt, shoe, and contents of pockets. Waist circumference was measured by placing the measuring tape in a horizontal plane midway between the lower rib and upper part of the iliac crest. Blood donors were advised to eat before donating blood. Non-fasting blood samples from the blood donors were collected by technicians at the blood bank and sent directly for centrifugation and analysis at the hospital laboratory.
The blood samples were analyzed at the same health-care institution. However, although at two different laboratory departments, both laboratory departments used similar procedures and instruments. The same blood pressure device, scale, and waist measurement tape were used for both inpatients and blood donors.
For the inpatients, socio-demographics, health and lifestyle-related information, the dietary record, questions about previous traumatic experiences, the Eating Attitude Test (EAT)21 12-item version (EAT-12) by Lavik, Clausen and Pedersen,22 and the Sleep Condition Indicator (SCI)23 were collected in paper form. The International Physical Activity Questionnaire Short Form (IPAQ-SF),24 Symptom Check List 10 (SCL-10), the short version of the Symptom Check List 90 (SCL-90)25 were collected digitally using CheckWare.26 Information about diagnoses based on the International Classification of Diseases 10th Revision (ICD-10) codes27 and medication were collected from the inpatient records by the first author.
For the blood donors, all questionnaires, including demographics, health and lifestyle-related information, were collected in paper form.
Definitions and Measurements
Socio-demographics (ie, age, gender, ethnicity, civilian status, work status, income and education level) and health related information (medication, previous pregnancy diabetes, diabetes in near family (parent/sibling/child), previously detected high blood glucose, polycystic ovary syndrome (PCOS)), were mapped. No additional data on medication adherence or compliance were collected beyond the patients’ medication lists.
Traumatic experiences, defined by ICD-10 criterion:27
A stressful event or situation - of an extremely threatening or catastrophic nature, which is likely to cause extensive and highly unpleasant reactions to most people.
was measured using a five-item structured self-report form. Question one, two and three ask if the participant in childhood has experienced 1) sexual abuse; 2) physical abuse; 3) other traumatic experiences that have subsequently caused significant problems. The last two questions ask if the participant, in adulthood, has experienced 4) sexual or physical abuse; 5) other traumatic experiences that have subsequently caused significant problems. The answer options are No (0); Yes, once (1); Yes, several times (2). A trauma score denoting the extent of trauma experienced was constructed by calculating the total scores for questions dealing with the history of trauma in childhood and adulthood. The maximum severity scores are six for childhood trauma and four for adult trauma. These questions have previously been used in two studies on Norwegian psychiatric inpatients,28,29 although not formally validated.
MetS was identified on the basis of a collection of risk factors; abdominal obesity (waist circumference in males >94 cm, females ≥80 cm), and two or more of the following conditions: hypertension (blood pressure ≥130 mmHg systolic or ≥85 mmHg diastolic or specific treatment for hypertension); fasting triglycerides ≥1.7 mmol/L (non-fasting triglycerides ≥2.0 mmol/L30) or specific treatment for high triglycerides; HDL cholesterol (≤1.03 mmol/L in males, ≤1.29 mmol/L in females or specific treatment for low HDL); and HbA1c ≥5.7% = 39 mmol/mol.1,30
T2DM was identified based on the HbA1c value (limit 6.5% = 48 mmol/mol31), or if the inpatients used medication for T2DM.
Body mass index (BMI) was calculated using the following formula: weight (kg)/height (cm)2 = BMI.
Dietary record: A scannable self-administered paper-based food frequency questionnaire (FFQ) constructed by the University of Oslo was used to collect data on dietary consumption over the last 12 months. The questionnaire consists of 256 questions on food and beverages, including portion sizes. The FFQ has been validated in various groups of Norwegian adults.32,33 The answers were scanned by using Teleform program, version 6.0 (Datascan, Oslo, Norway). Nutrient intake was computed using the Food and Nutrient Calculation System AE22 developed by the Department of Nutrition, University of Oslo. The food database is updated regularly.
Physical activity level was assessed using the International Physical Activity Questionnaire Short Form (IPAQ-SF),24 developed to measure physical activity and inactivity in adults (18–65 years). The instrument is a seven-question self-administered questionnaire that maps the time spent on low, middle, and intense activities, including sitting still. Physical activity level was processed according to the IPAQ processing guidelines,34 using a scoring spreadsheet developed by Cheng.35 Physical activity level was explored both as a three-level variable of weekly physical activity (low; moderate; high) and as a continuous variable using metabolic equivalent of task (MET). IPAQ-SF is evaluated to have acceptable reliability and validity for sitting and vigorous physical activity, and fair validity of walking, in a Norwegian sample of males.36
Tobacco use was assessed by asking, “Do you smoke/use Swedish snus?” with yes/no/sometimes answer options. The answer “sometimes” was later recoded as “yes”.
Sleeping condition was assessed using the Sleep Condition Indicator (SCI),23 a questionnaire consisting of eight questions with five different response options monitoring the quality of sleep in the last month. The total score ranges from 0 to 32. Lower scores reflect more sleep disturbance, and a score ≤16 indicates probable insomnia,37 SCI has shown convergent validity across various study samples.23,38 The current version was constructed by a forward-backward translation in a previous study by our group.29
Mental distress was assessed using the Symptom Check List 10 (SCL-10), a short version of the Symptom Check List 90 (SCL-90).25 The SCL-10 is widely used and found to have acceptable validity in a Norwegian adult sample.39 The questionnaire measures psychological distress and consists of 10 questions about depression and anxiety symptoms in the last week, with response alternatives 1 = not bothered; 2 = slightly bothered; 3 = quite a bit bothered; 4 = very much bothered. The mean scores were calculated based on the answers. A score >1.85 has been considered to indicate symptoms of anxiety and depression.39
Disordered eating was measured using the 12-item version of the Eating Attitude Test (EAT),21 by Lavik, Clausen and Pedersen.22 The response options are as follows: 1) never; 2) rarely; 3) often; 4) always. The questionnaire is considered a valid instrument measuring symptoms of disordered eating in Norwegian adolescence.40,41 Higher scores indicate more disordered eating patterns. To maintain the focus on eating disorders, the scores of the three subscales were examined; “dieting”, related to an avoidance of fattening foods and preoccupation with being thinner; “bulimia and food preoccupation”, reflecting thoughts about food as well as those indicating bulimia; and “oral control”, related to self-control of eating and perceived pressure from others to gain weight.42
Mental disorders were based on the ICD-10 codes.27
The included instruments have, to our knowledge, not yet been validated in a sample of Norwegian trauma-exposed inpatients.
Sample Size Determination
The current study is a part of a larger project investigating the risk of T2DM in trauma-exposed patients. In this project, the calculation of statistical power was based on HbA1c. Normal values for HbA1c for non-diabetics are 4.3–6.1%, while the diagnostic criterion for diabetes is ≥6.5%.31 The average of HbA1c in the patient population was expected to be about 6.2%. Given the heterogeneity within the sample, we expected a large variation in the collected material and therefore based our calculations on a standard deviation (SD) of approximately 2.5. Assuming a one-sample t-test where the sample mean is compared against a normal mean of 5.2%, the following power levels were calculated: 80% power – 51 observations, 98% power – 100 observations. To accommodate the risk of potential dropout we aimed to recruit 150 inpatients and 70 blood donors (comparison group).
Statistical Analysis
Statistical analyses were performed by using SPSS version 28 for Windows (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test was used to test for normality. Groups were compared using the Independent Sample t-test for normally distributed continuous variables, chi-square test for categorical variables, Fisher’s exact test for tables with expected cell frequency ≤5, and Mann–Whitney U-test for non-normally distributed continuous variables. All statistical tests were two-tailed, with a significance level ≤0.05. Multivariable logistic regression models were applied to estimate the odds ratios (ORs) with 95% confidence intervals (95% CIs) of MetS in inpatients compared to blood donors. In addition, interaction analyses were performed to study the possible interactions between the groups and putative risk factors for MetS. The criteria for variables entering the multivariable logistic regression models were based on p-values ≥0.05 from the binary analyses. Additionally, selected nutrients (ie, salt, sugar and trans-fat) were included based on theoretical rationale. The univariate model presents crude ORs for MetS. The multivariable model presents age-, gender and risk factors (in separate models) adjusted ORs for MetS between inpatients (2) and blood donors (1). The interaction model presents age-, gender and risk factor (in separate models) adjusted interaction ORs for MetS for Group*risk factor. Risk factor variables with few observations were not included in the logistic regression model. The variance inflation factor (VIF) was used to detect multicollinearity for the variables included in the binary regression models. Variables with a VIF above 8.00 (ie, saturated fat, carbohydrates, and starch) were excluded.
Ethics
All participants received oral and written information about the study and provided written informed consent for participation. The authors assert that all procedures contributing to this work complied with the ethical standards of the relevant national and institutional committees on human experimentation and the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human subjects/patients were approved by the Ethics Committee of Regional Committees for Medical and Health Research Ethics (REK) (#78587 in REK South-East B) and the Data Protection Officer at Innlandet Hospital Trust (#135535).
Results
Sociodemographic Characteristics of the Study Sample
Table 1 presents a descriptive summary of the demographic characteristics of the study sample. A total of 134 adult (≥18 years) trauma-exposed inpatients, more females (n = 105, 78.4%) than males (n = 29, 21.6%), and 68 blood donors, more females (n = 40, 58.8%) than males (n = 28, 41.2%) were included. Compared to the blood donors, the proportion of females were significantly higher among the inpatients, and the median age was significantly lower (41.0 years, IQR = 31.0, 51.0 and 49.0 years, IQR = 34.0, 56.8).
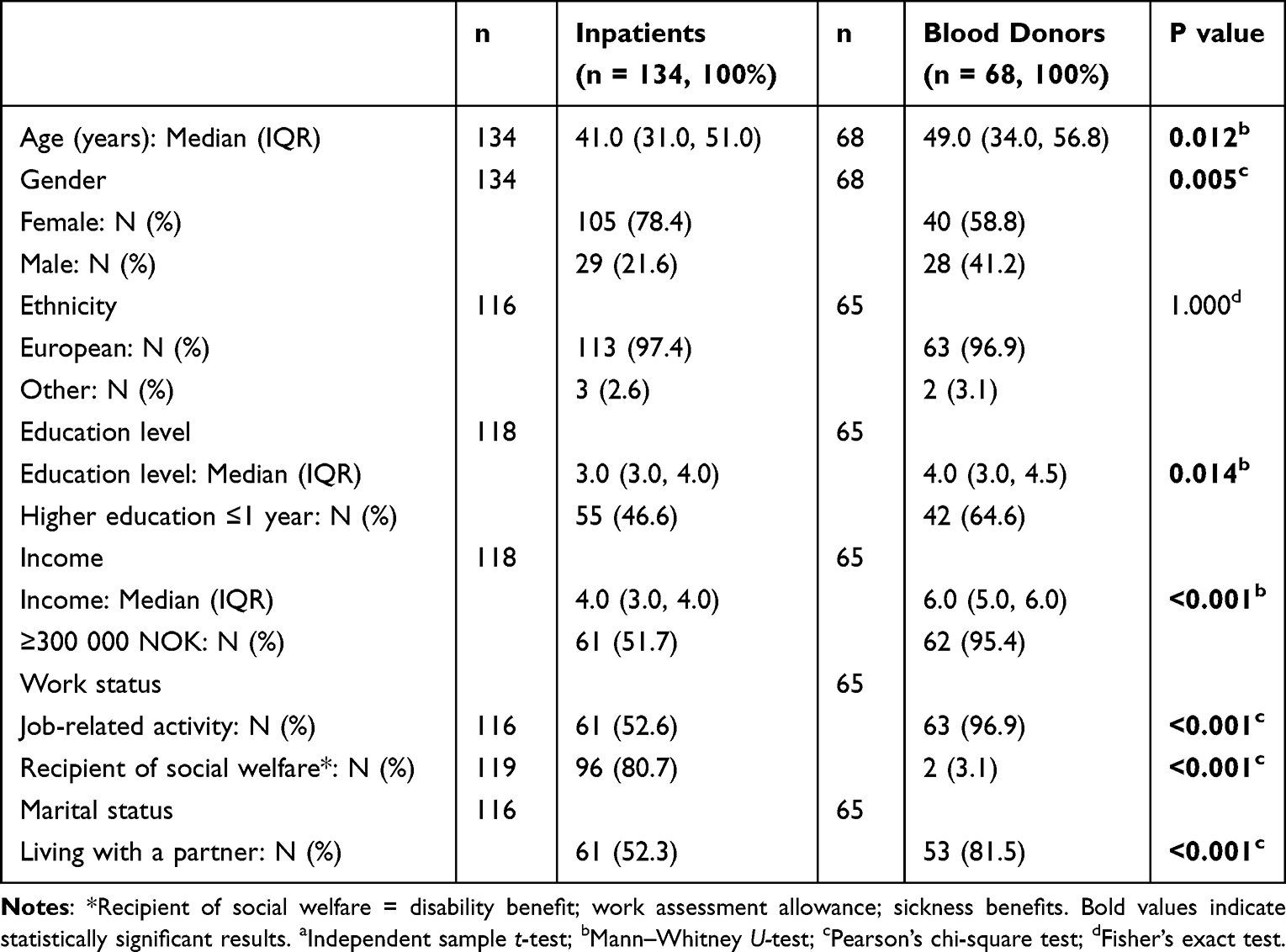 |
Table 1 Descriptive Summary of Demographics Differences in the Study Sample |
Compared to the blood donors, the inpatients had lower levels of education and income. Additionally, a significantly higher proportion of blood donors were involved in job-related activities, while a higher proportion of the inpatients were recipients of social welfare compared to blood donors. A significantly lower proportion of the inpatients lived with a partner compared to the blood donors.
Clinical, Metabolic, Lifestyle and Psychiatric Characteristics of the Study Sample
Table 2 presents differences in clinical, metabolic, lifestyle and psychiatric characteristics between trauma-exposed inpatients and blood donors. For an additional descriptive summary of the study sample, see Supplemental Material Table 1.
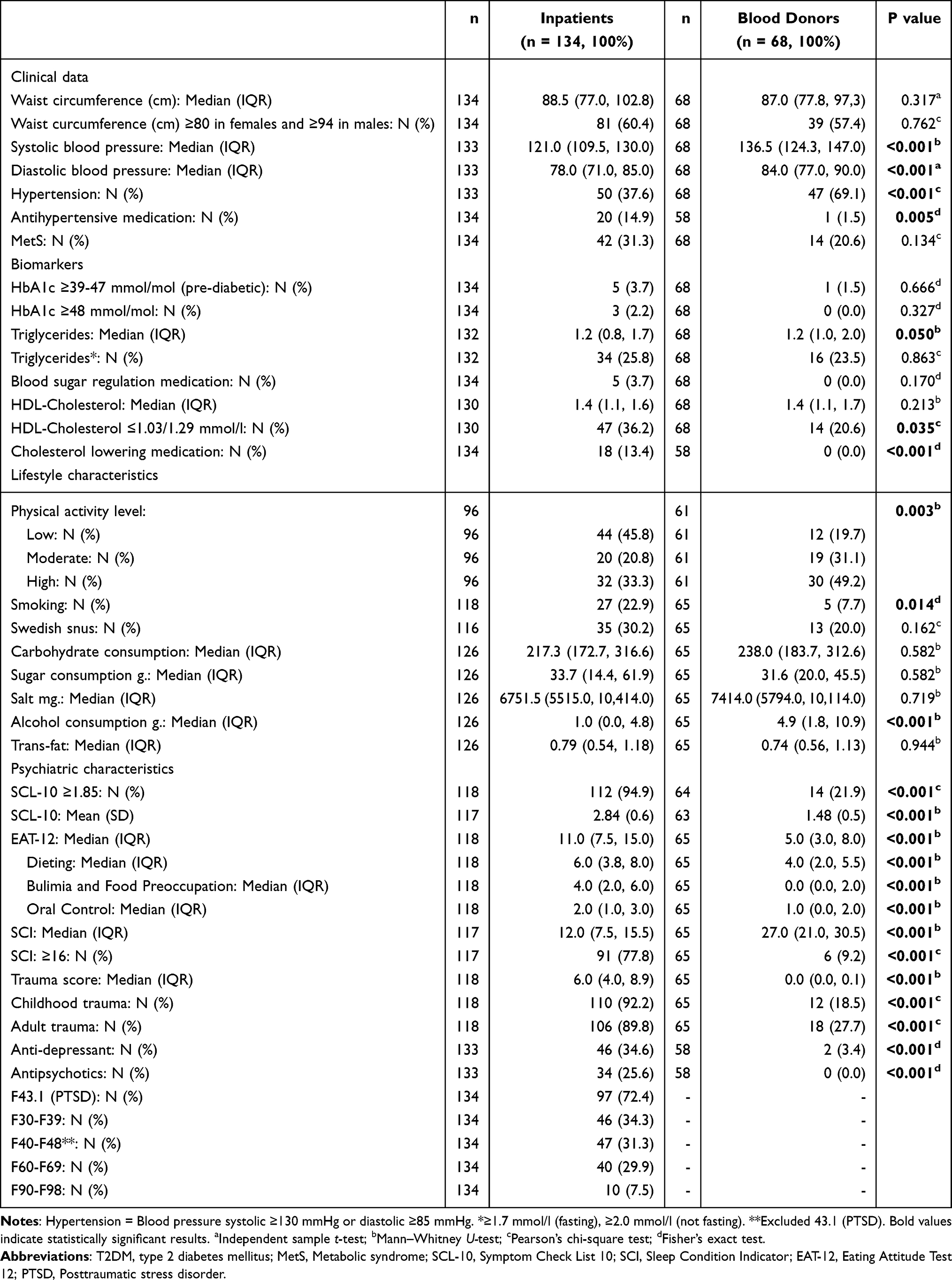 |
Table 2 Differences in Clinical, Metabolic, Lifestyle and Psychiatric Characteristics Between Trauma-Exposed Inpatients and Blood Donors |
Of the inpatients, 6.0% had HbA1c ≥39 mmol/mol compared to 1.5% of the blood donors. Significant differences were found for median triglycerides, probably because the patients’ samples were collected in a fasting state, whereas the blood donors were collected in a non-fasting state. While none of the blood donors reported using blood sugar regulation medications, 3.7% of the inpatients did so. Compared to the blood donors, a significantly higher proportion of the trauma-exposed inpatients had HDL cholesterol ≤1.03 in males and ≤1.29 females compared to the blood donors. While none of the blood donors reported using cholesterol-lowering medications, 13.4% of the trauma-exposed inpatients did. Compared to the blood donors, the inpatients had significantly lower systolic and diastolic blood pressure than the blood donors. However, a significantly higher proportion of the trauma-exposed inpatients used antihypertensive medication. While significantly lower physical activity levels, lower alcohol consumption, and a higher proportion of cigarette smokers were found among the inpatients compared to the blood donors, no significant differences were found in the proportion of those using Swedish snus or in the consumption of monitored nutrients.
The inpatients showed a significantly higher frequency of symptoms of mental distress (SCL-10), insomnia (SCI), disordered eating (EAT-12), and trauma scores compared to the blood donors. Among the inpatients, 72.4% were diagnosed with PTSD, 34.3% were diagnosed with affective disorders, 31.3% were diagnosed with neurotic, stress-related, and somatoform disorders (excluding PTSD), 29.9% were diagnosed with personality and behavioral disorders, and 7.5% were diagnosed with behavioral and emotional disorders with onset usually occurring in childhood and adolescence.
Risk of MetS in Trauma-Exposed Inpatients, and the Interaction Effects Between Group and Risk Factors for MetS
Table 3 presents the results (OR with 95% CI) from binary logistic regression models, reporting crude OR for MetS in the bivariate models, age, gender and risk factor (in separate models) adjusted OR for MetS between trauma-exposed inpatients and blood donors in the multivariable models, and age, gender and risk factor (in separate models) adjusted interaction OR for MetS for Group*risk factor in the interaction models.
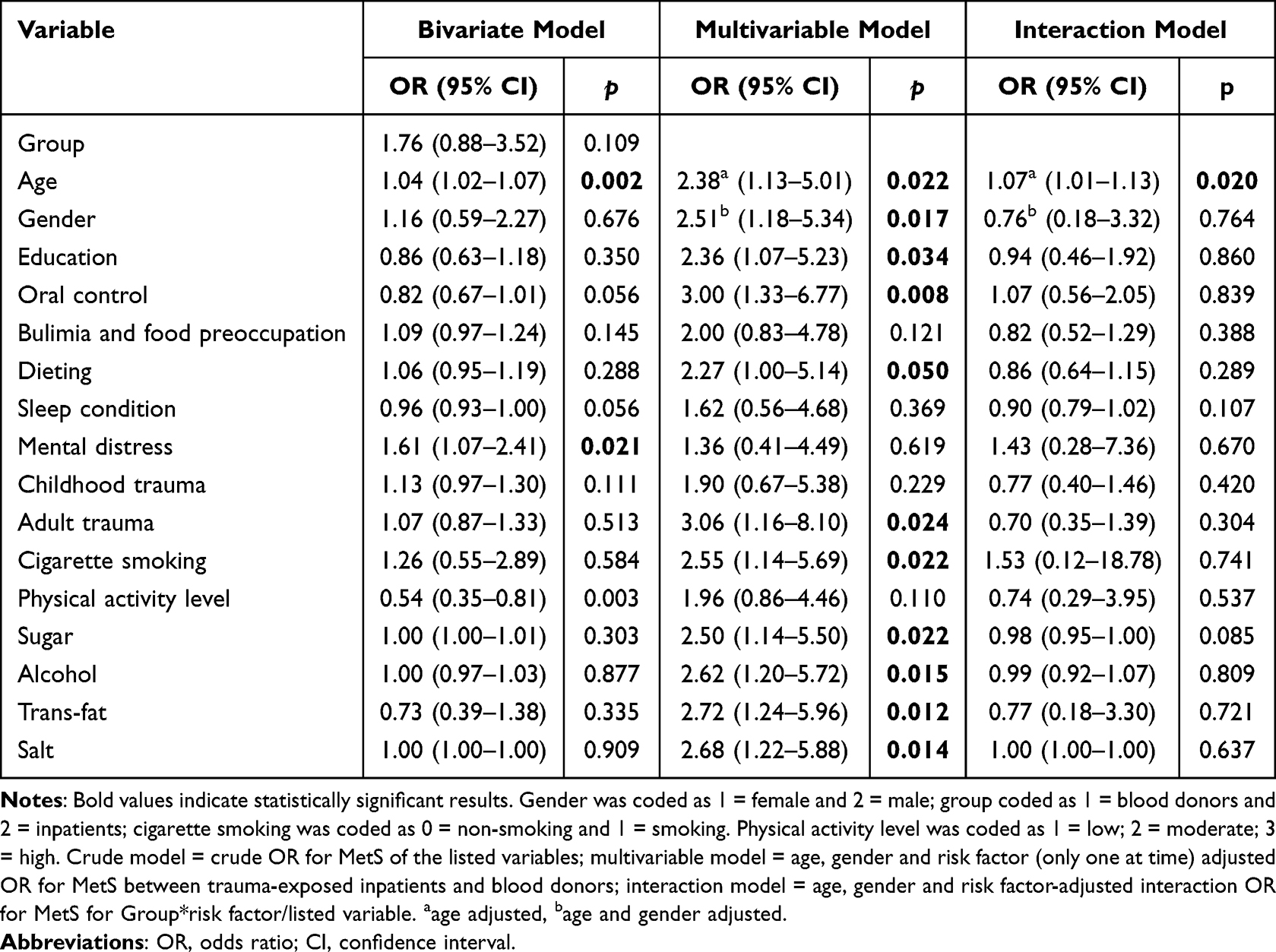 |
Table 3 Bivariate and Multivariable Binary Logistic Regression Models Showing Adjusted OR for MetS in Trauma-Exposed Inpatients Compared to Blood Donors and Interaction OR for MetS of Group*risk Factor |
Age- and gender adjusted ORs for MetS in the multivariable model showed a significantly higher risk of MetS among the inpatients compared to the blood donors. Upon adding, in separate models (one at a time), education, smoking, symptoms of disordered eating (ie, oral control and dieting), adult trauma, consumption of sugar, alcohol, trans-fat, and salt, the increased OR of MetS among inpatients compared to the blood donors remained significant, ranging from an OR of 2.27 adjusted for dieting, to an OR of 3.06, adjusted for adult trauma. Adding (only one at time) symptoms of bulimia and food preoccupation, physical activity level, mental distress, sleep condition, and childhood trauma, the significantly higher OR of MetS among inpatients compared to the blood donors did not remain. A significant interaction effect was observed only for age, with an OR of 1.07.
Compared to age- and gender adjusted ORs of MetS among the inpatients compared to the blood donors in model 2, ORs decreased by 6.0% adjusted for education; 20.3% adjusted for symptoms of bulimia and food preoccupation; 9.6% adjusted for symptoms of dieting; 35.5% adjusted for sleep condition; 45.8% adjusted for mental distress; 24.3% adjusted for childhood trauma; 21.9% adjusted for physical activity level; 0.4% adjusted for sugar consumption; and increased by 19.5% adjusted for symptoms of oral control; 21.9% adjusted for adult trauma; 1.6% adjusted for smoking; 4.4% adjusted for consumption of alcohol; 8.4% adjusted for consumption of trans-fat; and 6.8% adjusted for salt consumption.
Discussion
This study aimed to explore the risk of MetS in trauma-exposed inpatients compared with blood donors, including the interaction effects of associated psychological, biological, and behavioral risk factors for MetS. The main finding of the present study was that being in the trauma-exposed inpatient group was associated with a significantly higher age- and gender adjusted risk for MetS. Adjusted for level of education, cigarette smoking, symptoms of disordered eating (ie, “dieting” and “oral control”) and consumption of selected nutrients, the significantly higher risk of MetS among the inpatients remained. However, the increase in MetS risk was abolished upon adjustment for symptoms of bulimia and food preoccupation, mental distress, sleep condition, childhood trauma, and physical activity level, indicating these factors to be important MetS-associated predictors.
The higher age- and gender adjusted risk of MetS among the inpatients, including the influence of age, supports previous research.5,9,43 The association between trauma exposure and MetS is, however, complex,10,11 consisting of psychological, biological, and behavioral responses to stress, which directly or indirectly affect the metabolism of the body and thus increase the risk of metabolic disease.44
The decreased OR for MetS among the inpatients, after adjusting for childhood trauma, may indicate childhood trauma to be an important risk factor for MetS in this sample and support previous research.9 Experiencing trauma early in life has been associated with allostatic overload,45 which in turn is associated with low socioeconomic status, physical inactivity, cigarette smoking, alcohol consumption, unhealthy eating and thus poorer metabolic and cardiovascular health.45 The impact of socioeconomic status on health is well known,46 and experiencing trauma, especially in childhood, can contribute to a lower chance of completing higher education.47
The association between depressive symptoms and increased risk of MetS is well established,48 and comorbid depression in PTSD patients has been associated with further increased risk of MetS.43 The results of this study support this as evidenced in the decreased OR for MetS in the inpatients after adjustment for mental distress. In addition, the decreasing OR for MetS among the inpatients after adjusting for sleep condition (SCI) may be explained by the effect of poor sleep upon the metabolic and cardiovascular systems.49
Symptoms of “bulimia and food preoccupation” and “dieting” were both associated with increased risk of MetS among the inpatients, which is consistent with previous observations.50 Disordered eating may reflect a need to regulate emotions and avoid traumatic memories, and some may experience an addiction to food and sweets.20 The significant OR of MetS among the inpatients did not remain after adjustment for symptoms of “bulimia and food preoccupation”, pointing to bulimia as an important risk factor of MetS in trauma-exposed inpatients.
Furthermore, cigarette smoking, physical inactivity, and excessive consumption of food and snacks with high amounts of sugar, trans-fat, and salt are associated with an increased risk of MetS.12 The higher risk of MetS among the inpatients remained significant after adjustment for cigarette smoking and nutrients, but not for physical activity level. This suggests that physical inactivity is an important risk factor for MetS in trauma-exposed inpatients and might be explained by its positive effects on metabolic health.51 The lower consumption of alcohol among the inpatients compared to the blood donors may be explained by the clinic’s exclusion criteria. The increased OR of MetS among the inpatients after adjusting for trans-fat contradicts previous observations on the impact of trans-fat on metabolic and cardiovascular health.52 The significantly higher OR of MetS after adjusting for cigarette smoking might be due to cigarette smokers tending to have a lower body weight than non-smokers.53
The rather high prevalence of MetS among the blood donors may reflect the increasing incidence of MetS in the general population.2 Furthermore, results from a study of blood donors compared to the general population showed blood donors to be more often overweight for several reasons, including medical requirements for blood donation.54
Strengths and Limitations
This study does not come without limitations. There is a risk of detection bias in MetS, which could potentially have led to overestimation among the blood donors since fasting blood samples were collected from the inpatients at the clinic, while samples were collected from blood donors in a non-fasting state. Additionally, blood pressure and waist circumference were measured only once, potentially impacting the accuracy of these measures and thus the results. Information bias may have occurred due to incomplete dietary records, as there may be food that the informant ate regularly, which was not listed in their records. Furthermore, the recruited samples were not age- and gender matched. Moreover, given the present study sample size, there is a risk of underpowered stratified analyses, and thus type II errors. In addition, convenience sampling has its limitations,55 and using active blood donors as a comparison group can present a number of challenges, such as bias from the healthy donor effect.56 Active blood donors are a selected group, representing a generally healthier subgroup of the population, with a generally healthy cardiovascular status and lifestyle,54,56 which potentially have led to an overestimated effect in the patient group of this study. However, attempts have been made to adjust for confounding factors in the analyses, allowing transferable validity of the conclusions.
Implications and Further Research
Care provided to inpatients who have experienced trauma should aim to reduce both mental and somatic health conditions, and health-care personnel should be aware of the increased risk of MetS that trauma-exposed patients may carry. MetS increases the risk of T2DM and CVD and can be largely prevented57 through increased physical activity and healthy dietary habits. However, it is important to note that people suffering from traumatic experiences can struggle with disordered eating and that symptoms of bulimia and binge eating can contribute to an increased risk of MetS. Therefore, mapping symptoms of disordered eating should be considered in this population.
However, the limitations of this study suggest the need for future studies to include larger samples, including a comparison group from the general population, who are followed over time.
Conclusion
Trauma-exposed inpatients in this study had a significantly higher age- and gender-adjusted risk of MetS compared to the blood donors. Several psychological and behavioral lifestyle factors indicated increased risk of MetS. In particular, childhood trauma, higher levels of mental distress, poor sleep and physical inactivity appeared to be associated with an increased risk of MetS. The results suggest health-care professionals to be aware of the potential increased risk of MetS among trauma-exposed inpatients and prioritize addressing their somatic health conditions. However, given this study cross-sectional design, the results of the current study should be interpreted with caution. Future prospective research is needed, within larger samples.
Abbreviations
CI, Confidence Interval; CVD, Cardiovascular diseases; EAT-12, Eating Attitude Test 12; ICD-10, International Classification of Diseases 10th Revision; IPAQ-SF, International Physical Activity Questionnaire Short Form; MET, Metabolic equivalent of task; MetS, Metabolic syndrome; NSD, Norwegian Centre for Research Data; OR, Odds Ratio; PCOS, Polycystic ovary syndrome; PTSD, Posttraumatic stress disorder; REK, Regional Committees for Medical and Health Research Ethics; SCI, Sleep Condition Indicator; SCL-10, Symptom Check List 10; T2DM, Type 2 diabetes mellitus; VIF, Variance inflation factor.
Data Sharing Statement
The data that support the findings of this study are available upon reasonable request from the corresponding author, GER, and with permission from the Regional Committees for Medical and Health Research Ethics (REK) and the Data Protection Officer at Innlandet Hospital Trust. The data are not publicly available owing to restrictions on the written consent form.
Ethics Approval and Consent to Participate
The study was assessed and approved by the Regional Committees for Medical and Health Research Ethics (REK) (#78587 in REK South-East B, 20 March 2020, leader REK South-East B, Professor Dr. med. Ragnhild Emblem), and the Data Protection Officer at Innlandet Hospital Trust (#135535, June 16, 2020, Privacy Advisor Innlandet Hospital Trust).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
Thank you to all participants in the study for their time and important contributions. Many thanks to Friskstiftelsen, donation site Gjøvik, and Hege Skirbekk for their help with the recruitment and data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Innlandet Hospital Trust, Norway (project number 150632) through the research project awarded to Ph.D. student Roer “Is traumatic experience a risk factor for metabolic syndrome and type 2 diabetes mellitus?”
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang PL. A comprehensive definition for metabolic syndrome. Dis Model Mech. 2009;2(5–6):231–237. doi:10.1242/dmm.001180
2. Saklayen MG. The global epidemic of the metabolic syndrome. Curr Hypertens Rep. 2018;20(2):12. doi:10.1007/s11906-018-0812-z
3. Giangregorio F, Mosconi E, Debellis MG, et al. A systematic review of metabolic syndrome: key correlated pathologies and non-invasive diagnostic approaches. J Clin Med. 2024;13(19):5880. doi:10.3390/jcm13195880
4. Sumner JA, Cleveland S, Chen T, Gradus JL. Psychological and biological mechanisms linking trauma with cardiovascular disease risk. Transl Psychiatry. 2023;13(1):25. doi:10.1038/s41398-023-02330-8
5. Osode E, Cook E, Tomlin A. Child maltreatment and metabolic syndrome: a systematic review. Diabetes Metab Syndr Obes. 2024;17:3163–3176. doi:10.2147/dmso.S460058
6. Balaji S, Sankaranarayanan A. The association between adverse childhood experiences and metabolic syndrome in severe mental illness: a literature review. Australas Psychiatry. 2023;31(3):381–388. doi:10.1177/10398562231167782
7. Islam SJ, Hwan Kim J, Joseph E, et al. Association between early trauma and ideal cardiovascular health among black Americans: results from the Morehouse-Emory Cardiovascular (MECA) center for health equity. Circ Cardiovasc Qual Outcomes. 2021;14(9):e007904. doi:10.1161/circoutcomes.121.007904
8. Li M, Tao Z, Hongbin M, Hui W, Caihong J, Xiaolian J. Metabolic syndrome risk in relation to posttraumatic stress disorder among trauma-exposed civilians in Gansu Province, China. Medicine. 2020;99(1):e18614. doi:10.1097/md.0000000000018614
9. Souama C, Milaneschi Y, Lamers F, et al. Metabolic syndrome after childhood trauma: a 9-year longitudinal analysis. Psychol Med. 2023:1–9. doi:10.1017/S0033291723003264
10. Ryder AL, Azcarate PM, Cohen BE. PTSD and physical health. Curr Psychiatry Rep. 2018;20(12):116. doi:10.1007/s11920-018-0977-9
11. Koenen KC, Sumner JA, Gilsanz P, et al. Post-traumatic stress disorder and cardiometabolic disease: improving causal inference to inform practice. Psychol Med. 2017;47(2):209–225. doi:10.1017/S0033291716002294
12. Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735–2752. doi:10.1161/circulationaha.105.169404
13. Mohamed SM, Shalaby MA, El-Shiekh RA, El-Banna HA, Emam SR, Bakr AF. Metabolic syndrome: risk factors, diagnosis, pathogenesis, and management with natural approaches. Food Chem Adv. 2023;3:100335. doi:10.1016/j.focha.2023.100335
14. Chomiuk T, Niezgoda N, Mamcarz A, Śliż D. Physical activity in metabolic syndrome. Front Physiol. 2024;15:1365761. doi:10.3389/fphys.2024.1365761
15. Banjarnahor RL, Javadi Arjmand E, Onni AT, et al. Umbrella review of systematic reviews and meta-analyses on consumption of different food groups and risk of type 2 diabetes mellitus and metabolic syndrome. J Nutr. 2025;155(5):1285–1297. doi:10.1016/j.tjnut.2025.03.021
16. Kim Y, Roberts AL, Rimm EB, et al. Posttraumatic stress disorder and changes in diet quality over 20 years among US women. Psychol Med. 2021;51(2):310–319. doi:10.1017/s0033291719003246
17. van den Berk-Clark C, Secrest S, Walls J, et al. Association between posttraumatic stress disorder and lack of exercise, poor diet, obesity, and co-occuring smoking: a systematic review and meta-analysis. Health Psychol. 2018;37(5):407–416. doi:10.1037/hea0000593
18. Hall KS, Hoerster KD, Yancy WS Jr. Post-traumatic stress disorder, physical activity, and eating behaviors. Epidemiol Rev. 2015;37:103–115. doi:10.1093/epirev/mxu011
19. Theal R, Tay VXP, Hickman IJ. Conflicting relationship between dietary intake and metabolic health in PTSD: a systematic review. Nutr Res. 2018;54:12–22. doi:10.1016/j.nutres.2018.03.002
20. Roer GE, Solbakken HH, Abebe DS, Aaseth JO, Bolstad I, Lien L. Inpatients experiences about the impact of traumatic stress on eating behaviors: an exploratory focus group study. J Eat Disord. 2021;9(1):119. doi:10.1186/s40337-021-00480-y
21. Garner DM, Garfinkel PE. The eating attitudes test: an index of the symptoms of anorexia nervosa. Psychol Med. 1979;9(2):273–279. doi:10.1017/s0033291700030762
22. Lavik NJ, Clausen SE, Pedersen W. Eating behaviour, drug use, psychopathology and parental bonding in adolescents in Norway. Acta Psychiatr Scand. 1991;84(4):387–390. doi:10.1111/j.1600-0447.1991.tb03164.x
23. Espie CA, Kyle SD, Hames P, Gardani M, Fleming L, Cape J. The sleep condition indicator: a clinical screening tool to evaluate insomnia disorder. BMJ Open. 2014;4(3):e004183. doi:10.1136/bmjopen-2013-004183
24. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.Mss.0000078924.61453.Fb
25. Derogatis LR, Lipman RS, Covi L. SCL-90: an outpatient psychiatric rating scale–preliminary report. Psychopharmacol Bull. 1973;9(1):13–28.
26. CheckWare. Available from: https://www.checkware.no/.
27. World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. World Health Organization; 1992.
28. Toft H, Neupane SP, Bramness JG, Tilden T, Wampold BE, Lien L. The effect of trauma and alcohol on the relationship between level of cytokines and depression among patients entering psychiatric treatment. BMC Psychiatry. 2018;18(1):95. doi:10.1186/s12888-018-1677-z
29. Bolstad I, Toft H, Lien L, Moe JS, Rolland B, Bramness JG. Longitudinal determinants of insomnia among patients with alcohol use disorder. Alcohol. 2023;108:10–20. doi:10.1016/j.alcohol.2022.11.002
30. Mezhal F, Ahmad A, Abdulle A, et al. Metabolic syndrome in fasting and non-fasting participants: the UAE healthy future study. Int J Environ Res Public Health. 2022;19(21):13757. doi:10.3390/ijerph192113757
31. Committee ADAPP. 2. diagnosis and classification of diabetes: standards of care in diabetes—2025. Diabetes Care. 2024;48(Supplement_1):S27–S49. doi:10.2337/dc25-S002
32. Brunvoll SH, Thune I, Frydenberg H, et al. Validation of repeated self-reported n-3 PUFA intake using serum phospholipid fatty acids as a biomarker in breast cancer patients during treatment. Nutr J. 2018;17(1):94. doi:10.1186/s12937-018-0402-6
33. Andersen LF, Tomten H, Haggarty P, Løvø A, Hustvedt BE. Validation of energy intake estimated from a food frequency questionnaire: a doubly labelled water study. Eur J Clin Nutr. 2003;57(2):279–284. doi:10.1038/sj.ejcn.1601519
34. Sjostrom M, Ainsworth BE, Bauman A, Bull FC, Hamilton-Craig CR, Sallis JF. Guidelines for data processing analysis of the International Physical Activity Questionnaire (IPAQ) - short and long forms. 2005.
35. Cheng HL. A simple, easy-to-use spreadsheet for automatic scoring of the International Physical Activity Questionnaire (IPAQ Short Form. 2016. doi:10.13140/RG.2.2.21067.80165
36. Kurtze N, Rangul V, Hustvedt BE. Reliability and validity of the international physical activity questionnaire in the Nord-Trøndelag health study (HUNT) population of men. BMC Med Res Methodol. 2008;8:63. doi:10.1186/1471-2288-8-63
37. Espie C, Machado P, Carl J, et al. The sleep condition indicator: reference values derived from a sample of 200 000 adults. J Sleep Res. 2017:27. doi:10.1111/jsr.12643
38. Espie CA, Farias Machado P, Carl JR, et al. The sleep condition indicator: reference values derived from a sample of 200 000 adults. J Sleep Res. 2018;27(3):e12643. doi:10.1111/jsr.12643
39. Strand BH, Dalgard OS, Tambs K, Rognerud M. Measuring the mental health status of the Norwegian population: a comparison of the instruments SCL-25, SCL-10, SCL-5 and MHI-5 (SF-36). Nord J Psychiatry. 2003;57(2):113–118. doi:10.1080/08039480310000932
40. Wichstrøm L. Social, psychological and physical correlates of eating problems. A study of the general adolescent population in Norway. Psychol Med. 1995;25(3):567–579. doi:10.1017/s0033291700033481
41. Wichstrø L, Skogen K, Øia T. Social and cultural factors related to eating problems among adolescents in Norway. J Adolesc. 1994;17(5):471–482. doi:10.1006/jado.1994.1040
42. Garner DM, Olmsted MP, Bohr Y, Garfinkel PE. The eating attitudes test: psychometric features and clinical correlates. Psychol Med. 1982;12(4):871–878. doi:10.1017/s0033291700049163
43. Roer GE, Lien L, Bolstad I, Aaseth JO, Abebe DS. The impact of PTSD on risk of cardiometabolic diseases: a national patient cohort study in Norway. BMC Psychiatry. 2023;23(1):349. doi:10.1186/s12888-023-04866-x
44. Kivimäki M, Bartolomucci A, Kawachi I. The multiple roles of life stress in metabolic disorders. Nat Rev Endocrinol. 2023;19(1):10–27. doi:10.1038/s41574-022-00746-8
45. McEwen BS, Stellar E. Stress and the individual: mechanisms leading to disease. Arch Intern Med. 1993;153(18):2093–2101. doi:10.1001/archinte.1993.00410180039004
46. Mackenbach JP, Stirbu I, Roskam A-JR, et al. Socioeconomic inequalities in health in 22 European countries. N Engl J Med. 2008;358(23):2468–2481. doi:10.1056/NEJMsa0707519
47. Pan J, Zaff JF, Porche M. Social support, childhood adversities, and academic outcomes: a latent class analysis. J Educ Stud Placed Risk. 2020;25(3):251–271. doi:10.1080/10824669.2019.1708744
48. Moradi Y, Albatineh AN, Mahmoodi H, Gheshlagh RG. The relationship between depression and risk of metabolic syndrome: a meta-analysis of observational studies. Clin Diabetes Endocrinol. 2021;7(1):4. doi:10.1186/s40842-021-00117-8
49. Sharma S, Kavuru M. Sleep and metabolism: an overview. Int J Endocrinol. 2010;2010:1–12. doi:10.1155/2010/270832
50. Hudson JI, Javaras KN, Pope HG Jr. The challenges of metabolic syndrome in eating disorders. Psychiatr Ann. 2020;50(8):346–350. doi:10.3928/00485713-20200713-02
51. Thyfault JP, Bergouignan A. Exercise and metabolic health: beyond skeletal muscle. Diabetologia. 2020;63(8):1464–1474. doi:10.1007/s00125-020-05177-6
52. Micha R, Mozaffarian D. Trans fatty acids: effects on metabolic syndrome, heart disease and diabetes. Nat Rev Endocrinol. 2009;5(6):335–344. doi:10.1038/nrendo.2009.79
53. Chiolero A, Faeh D, Paccaud F, Cornuz J. Consequences of smoking for body weight, body fat distribution, and insulin resistance. Am J Clin Nutr. 2008;87(4):801–809. doi:10.1093/ajcn/87.4.801
54. Atsma F, Veldhuizen I, Verbeek A, de Kort W, de Vegt F. Healthy donor effect: its magnitude in health research among blood donors. Transfusion. 2011;51(8):1820–1828. doi:10.1111/j.1537-2995.2010.03055.x
55. Stratton SJ. Population research: convenience sampling strategies. Prehosp Disaster Med. 2021;36(4):373–374. doi:10.1017/S1049023X21000649
56. Atsma F, de Vegt F. The healthy donor effect: a matter of selection bias and confounding. Transfusion. 2011;51(9):1883–1885. doi:10.1111/j.1537-2995.2011.03270.x
57. Nordisk Ministerråd. Nordic Nutrition Recommendations 2012: Integrating Nutrition and Physical Activity. Copenhagen: Nordisk Ministerråd; 2014.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.