Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Metabolic Dysfunction-Associated Steatotic Liver Disease and Liver Fibrosis are Associated with Advanced Cardiovascular-Kidney-Metabolic Syndrome in Chinese and US Populations
Authors Hu S ![]() , Wang D, Yu Q, Chen Z, Lu W, Meng Y, Peng X, Liu L, Wan H
, Wang D, Yu Q, Chen Z, Lu W, Meng Y, Peng X, Liu L, Wan H ![]() , Shen J
, Shen J
Received 29 September 2025
Accepted for publication 11 December 2025
Published 23 December 2025 Volume 2025:18 Pages 4699—4713
DOI https://doi.org/10.2147/DMSO.S569698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jae Woong Sull
Shidi Hu,1,2,* Dongmei Wang,1,* Qingtao Yu,1,* Zhi Chen,1 Weiguo Lu,3 Yuan Meng,4 Xuetao Peng,4 Lan Liu,1,4 Heng Wan,1,4 Jie Shen1,4
1Department of Endocrinology and Metabolism, The Eighth Affiliated Hospital, Southern Medical University (The First People’s Hospital of Shunde), Foshan, Guangdong, People’s Republic of China; 2Department of Endocrinology and Metabolism, The Third Affiliated Hospital, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 3Department of General Medicine, Shunde Lunjiao Community Healthcare Center, Foshan, Guangdong, People’s Republic of China; 4GuangDong Engineering Technology Research Center of Metabolic Disorders Interdisciplinary Precision Prevention and Digital Healthcare, The Eighth Affiliated Hospital, Southern Medical University (The First People’s Hospital of Shunde), Foshan, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jie Shen, Department of Endocrinology and Metabolism, the Eighth Affiliated Hospital, Southern Medical University (The First People’s Hospital of Shunde), No. 1 of Jiazi Road, Lunjiao, Shunde District, Foshan, Guangdong, 528308, People’s Republic of China, Email [email protected] Heng Wan, Department of Endocrinology and Metabolism, the Eighth Affiliated Hospital, Southern Medical University (The First People’s Hospital of Shunde), No. 1 of Jiazi Road, Lunjiao, Shunde District, Foshan, Guangdong, 528308, People’s Republic of China, Email [email protected]
Purpose: Despite the pathophysiologic overlap between metabolic dysfunction-associated steatotic liver disease (MASLD) and cardiovascular-kidney-metabolic (CKM) syndrome, MASLD has not been incorporated into the current CKM framework. This study examined the associations of MASLD and MASLD-related fibrosis with advanced CKM syndrome in Chinese and US populations.
Patients and Methods: We enrolled 6186 participants in a community-based cross-sectional study conducted in China, with validation utilizing the National Health and Nutrition Examination Survey (NHANES). Advanced CKM syndrome was defined as stages 3 and 4. Hepatic steatosis and fibrosis were assessed via vibration-controlled transient elastography. Multivariable logistic regression and restricted cubic spline (RCS) analyses were employed.
Results: Advanced CKM syndrome was present in 8.8% of the Chinese and 14.9% of the US populations. MASLD participants exhibited a significantly higher prevalence of advanced CKM than those without (China: 12.6% vs 6.4%; US: 21.5% vs 9.9%). In addition, participants with MASLD were associated with increased odds of advanced CKM (China: OR 2.06, 95% CI: 1.64– 2.58; US: OR 1.60, 95% CI: 1.22– 2.10; both P < 0.01). Among participants with MASLD, advanced CKM syndrome was more prevalent in participants with fibrosis than without (China: 17.1% vs 11.2%; US: 28.4% vs 20.1%). MASLD-related fibrosis was also independently linked to higher odds of advanced CKM compared to non-fibrotic MASLD (China: OR 1.55, 95% CI: 1.09– 2.18; US: OR 1.44, 95% CI: 1.01– 2.05; both P < 0.05). Furthermore, RCS analysis revealed a positive linear relationship of controlled attenuation parameter (CAP) and liver stiffness measurement (LSM) values with the prevalence of advanced CKM syndrome (P non-linear > 0.05).
Conclusion: MASLD and MASLD-related fibrosis were significantly associated with a higher prevalence of advanced CKM syndrome, and higher CAP/LSM levels showed linear associations with advanced CKM syndrome in both Chinese and US populations. These findings support evaluating liver health (eg, CAP/LSM) when risk-stratifying CKM syndrome.
Keywords: advanced cardiovascular-kidney-metabolic syndrome, controlled attenuation parameter, fibrosis, liver stiffness measurement, metabolic dysfunction-associated steatotic liver disease
Introduction
Cardiovascular-kidney-metabolic (CKM) syndrome is a progressive condition characterized by a complex multisystem interplay involving chronic kidney disease (CKD), cardiovascular disease (CVD), and metabolic risk factors.1 The staging of CKM syndrome (0–4) is determined by its pathophysiological processes, providing an invaluable framework for risk stratification and the implementation of preventive strategies.2 Research has recently indicated that approximately 15% of American adults display advanced CKM syndrome (stages 3–4),3,4 highlighting its substantial public health burden. Consequently, as the prevalence of CKM syndrome components escalates globally, it becomes a major driver of morbidity and mortality,5 necessitating critical clinical research to mitigate its severe implications.
Metabolic dysfunction-associated steatotic liver disease (MASLD) is a common condition closely linked to the increased incidence of metabolic disorders. Additionally, MASLD afflicts more than 30% of adults worldwide, constituting both the leading chronic liver disorder and a pivotal cardiometabolic determinant.6 The new MASLD definition emphasizes the interplay between metabolic dysfunction and hepatic steatosis, thereby recognizing it not merely as an organ-specific disease but as a multisystem disorder.7 A study examining the overlap and synergistic effects of five cardiometabolic risk factors on MASLD and liver fibrosis found that more than 80% of patients had three or more risk factors.8 A greater number of cardiometabolic risk factors in MASLD, or the acquisition of these factors over time, is associated with a progressively elevated risk of subsequent adverse cardiorenal outcomes.9 Furthermore, hepatic steatosis accelerates endothelial dysfunction, atherosclerosis, systemic inflammation, and renal injury, thus directly fueling the progression of CKD and CVD.10,11
A growing body of research highlights the strong association between MASLD and cardiovascular and kidney diseases. Notably, MASLD serves as an independent predictor of atherosclerotic cardiovascular disease (ASCVD) risk, thereby increasing morbidity and mortality rates.12,13 Moreover, evidence from a large-scale Korean cohort study, which included 214,145 participants, revealed a robust correlation between MASLD and a heightened risk of developing CKD as well as abnormal proteinuria.14 A meta-analysis encompassing nine observational studies and a total of 96,595 adults indicated that MASLD was linked to a 37% higher long-term risk of incident CKD,15 emphasizing that hepatic steatosis is not merely a hepatic disorder but a multisystem metabolic condition. The recent conceptual framework of CARDIAL-MS (CArdio-Renal-DIAbetes-Liver-Metabolic Syndrome) integrates the liver into the cardio-renal-metabolic continuum, providing an actionable paradigm for clinical risk stratification and personalized prevention.16
Although it is well established that MASLD is linked to individual CKM components (eg, CKD, CVD),17 a critical knowledge gap remains regarding the integrated relationship between MASLD and the progressive continuum of CKM syndrome as a unified entity. The American Heart Association (AHA) has acknowledged the pathophysiologic overlap between MASLD and CKM syndrome; however, the current CKM framework inadequately incorporates hepatic contributions across the disease continuum.1,18 Furthermore, the progression from hepatic steatosis to metabolic dysfunction-associated steatohepatitis (MASH) and significant liver fibrosis represents a pivotal transition point in the disease continuum, substantially amplifying the risk of both hepatic and extrahepatic complications, particularly adverse cardiovascular events.19 However, whether the presence and severity of liver fibrosis confer an additional risk for advanced CKM syndrome beyond that of steatosis alone remains unclear. In addition, comprehensive investigations examining the prevalence and associations among MASLD, liver fibrosis, and advanced CKM syndrome are still lacking, especially in Chinese populations. Vibration-controlled transient elastography (VCTE)—which quantitatively evaluates hepatic steatosis via the controlled attenuation parameter (CAP) and fibrosis via liver stiffness measurement (LSM)—offers a superior, non-invasive approach.20 Determining whether VCTE-based CAP and LSM provide additional prognostic value beyond existing CKM staging frameworks is therefore of critical clinical importance.
Therefore, this study aimed to: (1) investigate the prevalence of MASLD and associated fibrosis across the spectrum of CKM syndrome, while exploring potential overlapping correlations in Chinese and US cohorts; and (2) examine the associations of CAP, LSM, MASLD and MASLD-related fibrosis with the prevalence of advanced CKM syndrome. Ultimately, our goal was to provide evidence on whether MASLD and the degree of liver fibrosis should be incorporated into risk stratification of CKM syndrome.
Materials and Methods
Study Participants
We conducted a community-based, cross-sectional observational study in China (the Speed-Shunde Cohort). The study was registered in the Chinese Clinical Trial Registry (Registration Number: ChiCTR2100054130; Website: http://www.chictr.org.cn/). The research subjects were derived from a multistage stratified random sampling survey conducted across ten towns in Shunde District between November 2021 and September 2022.6,21,22 Eligible residents were adults aged ≥18 years with ≥6 months’ tenure in Shunde. Residents with acute illness, infection, trauma, or pregnancy were excluded from the study. A survey involving 13,535 participants was conducted. Exclusions were applied to individuals under 20 years old (n = 31), those missing blood samples (n = 3403), CKM data (n = 2756), LSM data (n = 451), those with other liver diseases (n = 692), or a lack of data on MASLD (n = 16). Consequently, a total of 6186 subjects were enrolled in the study (Figure 1A). The study was approved by the ethics committee of the Eighth Affiliated Hospital (The First People’s Hospital of Shunde) of Southern Medical University, adhered to the 1975 Declaration of Helsinki’s ethical guidelines (protocol 20211103 in China), and obtained written informed consent from all subjects.
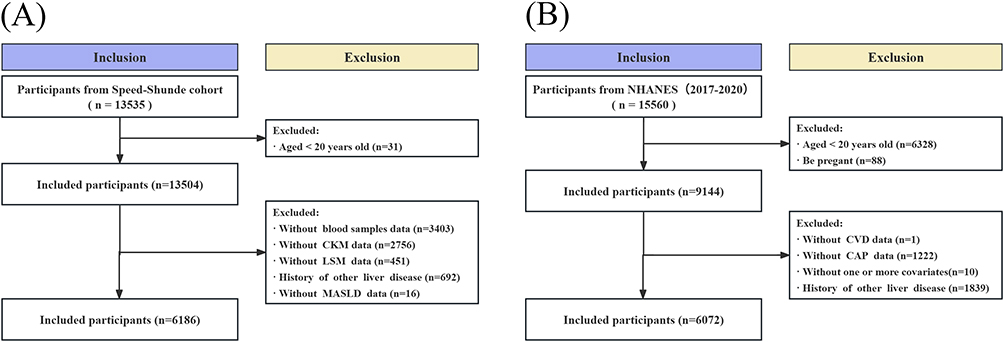 |
Figure 1 Flowchart of the study participants. (A) The Speed-Shunde Cohort; (B) The NHANES. Abbreviations: CKM, Cardiovascular-kidney-metabolic; CVD, cardiovascular disease; CAP, controlled attenuation parameter; LSM, liver stiffness measurement; MASLD, Metabolic dysfunction-associated steatotic liver disease. |
The National Health and Nutrition Examination Survey (NHANES) was utilized as an external validation cohort to investigate potential differences between China and the United States. The NHANES is a systematic survey by the National Center for Health Statistics (NCHS) that collects demographic, clinical, laboratory, lifestyle, and self-reported health data. The present analysis utilized data from the 2017–2020 NHANES cycle, and all procedures adhered to the official survey guidelines. Notably, the study included 9144 individuals aged 20 or older who were not pregnant. Participants were excluded if they lacked data on CVD (n=1), CAP data (n=1222), covariates (n=10), or had other liver diseases (n=1839). Ultimately, 6072 participants were included in the analysis (Figure 1B).
Data Collection
The Speed-Shunde cohort utilized a standardized protocol to collect comprehensive data on participants. Trained staff administered standardized questionnaires covering demographics, lifestyle, medical history, and medications. The questionnaire used was based on scales previously published by our team.6,22 Detailed information about these scales can be found in our prior publications. Physical examinations were also conducted. Fasting blood specimens were obtained in the morning hours (8:00–10:00 AM) and analyzed thereafter for plasma glucose concentration, glycosylated hemoglobin, and lipid profiles. For participants without self-reported diabetes, a 2-hour oral 75g glucose tolerance test was performed, and 2-hour plasma glucose was measured. Additionally, random urine samples were tested for microalbumin and creatinine using dipstick analysis. All biological samples were transported under cold chain conditions, centrifuged, and frozen at −20°C.
In the NHANES study, demographic data were obtained by self-reported variables, including age, gender, race/ethnicity, education level, smoking status, and alcohol consumption. NHANES provided detailed information describing the laboratory methodologies used to quantify numerous biomarkers, including plasma glucose levels, glycosylated hemoglobin, and lipid profiles. Data cleaning was conducted in accordance with the literature previously outlined.23 The study categorized education levels into three groups: less than high school, high school, and beyond high school. Furthermore, the number of cigarettes smoked in a lifetime determined whether a person was a current smoker (lifetime ≥100 cigarettes and ongoing), a nonsmoker, or a former smoker (quit ≥6 months).24
Definitions of MASLD and Fibrosis
In the Speed-Shunde cohort and the NHANES study, CAP and LSM were measured using VCTE with the FibroScan® 402 and 502 V2 Touch models, respectively. Prior to the examination, participants underwent a standardized fast of at least 3 hours. The procedure was conducted by trained technicians using VCTE, with the probe selection (medium (M) or extra-large (XL)) determined by the manufacturer’s BMI-based guidance. Measurements were considered reliable only if they achieved an interquartile range-to-median (IQR/M) ratio of ≤30% and a success rate of at least 60%. Measurements with <10 valid shots or that did not meet reliability criteria were repeated or excluded. Participants underwent VCTE assessment to identify hepatic steatosis (CAP ≥ 248 dB/m)20 and fibrosis (LSM ≥ 7.0 kPa).25 The diagnosis of MASLD required hepatic steatosis meeting the criteria of at least one of five cardiometabolic risk factors.7 Metabolic and alcohol-associated liver disease is defined as MASLD patients with high weekly alcohol intake (defined as 140–350 g for women and 210–420 g for men). Additionally, the history of other liver diseases includes hepatitis B or C, metabolic and alcohol-associated liver disease, alcohol-associated liver disease, and cryptogenic steatotic liver disease.
Definition of CKM Syndrome
We defined CKM syndrome stages as adherence to the criteria outlined in the AHA Presidential Advisory Statement.1 The estimated glomerular filtration rate (eGFR) was calculated using the 2021 race-free Chronic Kidney Disease Epidemiology Collaboration creatinine equation.26 Albuminuria was defined as a urinary albumin-to-creatinine ratio (UACR) ≥ 30 mg/g. The stage of CKD was determined using the KDIGO criteria based on eGFR and UACR. Using the PREVENT equations,18 a 10-year cardiovascular disease (CVD) risk ≥ 20% was considered high. Subclinical CVD was defined as having either a ≥ 20% 10-year CVD risk or a high-risk of CKD. A comprehensive variable-definition map is provided in Table S1. The stages are defined as follows: Stage 0 (characterized by the absence of CKM risk factors), Stage 1 (defined by the presence of excess or dysfunctional adiposity), Stage 2 (marked by the co-occurrence of metabolic risk factors and moderate to high-risk CKD), Stage 3 (where subclinical CVD manifests), and Stage 4 (which involves clinical CVD). Non-advanced CKM syndrome was considered present at stage ≤2, and advanced CKM syndrome stages were characterized by stages 3 and 0.1,2
Statistical Analysis
Appropriate statistical techniques were applied to respect the respective survey designs. In Speed-Shunde, we accounted for the multistage sampling using cluster-robust standard errors (SE) at the town level. The NHANES data were analyzed using the provided strata, primary sampling units (PSU), and examination weights (WTMEC2YR) as per the NCHS analytical guidelines. Baseline characteristics were summarized using frequencies and percentages (%) for categorical variables and means ± standard deviation for continuous variables. Differences between groups were assessed using t-tests, chi-square tests, or Mann–Whitney U-tests as appropriate. Baseline characteristics of included subjects and those excluded due to missing data are presented in Table S2. The patterns of co-existence and the frequency of overlapping combinations among CKM syndrome, MASLD, and hepatic fibrosis were quantified. A multivariable logistic regression model was applied in the Speed-Shunde cohort to evaluate odds ratios (ORs) and their 95% Confidence Intervals (CIs) for the relationship between CAP, LSM, MASLD, and MASLD-related fibrosis and the prevalence of advanced CKM syndrome. The comprehensive model in the Speed-Shunde Cohort was adjusted for age, sex, education, and smoking behavior. A survey-weighted multivariable logistic regression model in the NHANES study was employed to examine the associations between CAP, LSM, MASLD, and MASLD-related fibrosis and the prevalence of advanced CKM syndrome, with additional adjustment for race/ethnicity. All confounding variables exhibited variance inflation factors below 5, indicating no substantial multicollinearity. To assess the dose-response relationship between advanced CKM syndrome and CAP or LSM, a restricted cubic spline (RCS) with three knots (at the 10th, 50th, and 90th percentiles) was used, setting the cohort median as the reference point. Data analysis was conducted using IBM SPSS Statistics (version 24) and R (version 4.2.2), with a two-sided P-value of <0.05 indicating statistical significance for all hypothesis tests.
Results
Baseline Characteristics
Table 1 presents the baseline characteristics of the study participants from the Speed-Shunde cohort and the NHANES. The Speed-Shunde cohort included 6186 participants (mean age 48.61±12.6 years; 38.8% male; mean BMI 23.76±3.38 kg/m2). The majority (85.8%) reported never smoking, while 3.5% were former smokers and 10.7% were current smokers. The proportions of participants in CKM syndrome stages 0, 1, 2, 3, and 4 were 14.1%, 19.3%, 57.7%, 6.5%, and 2.3%, respectively. Notably, advanced CKM syndrome was observed in 8.8% of participants. Among the cohort, MASLD had a prevalence of 39.4%, and liver fibrosis was detected in 15.6% of individuals.
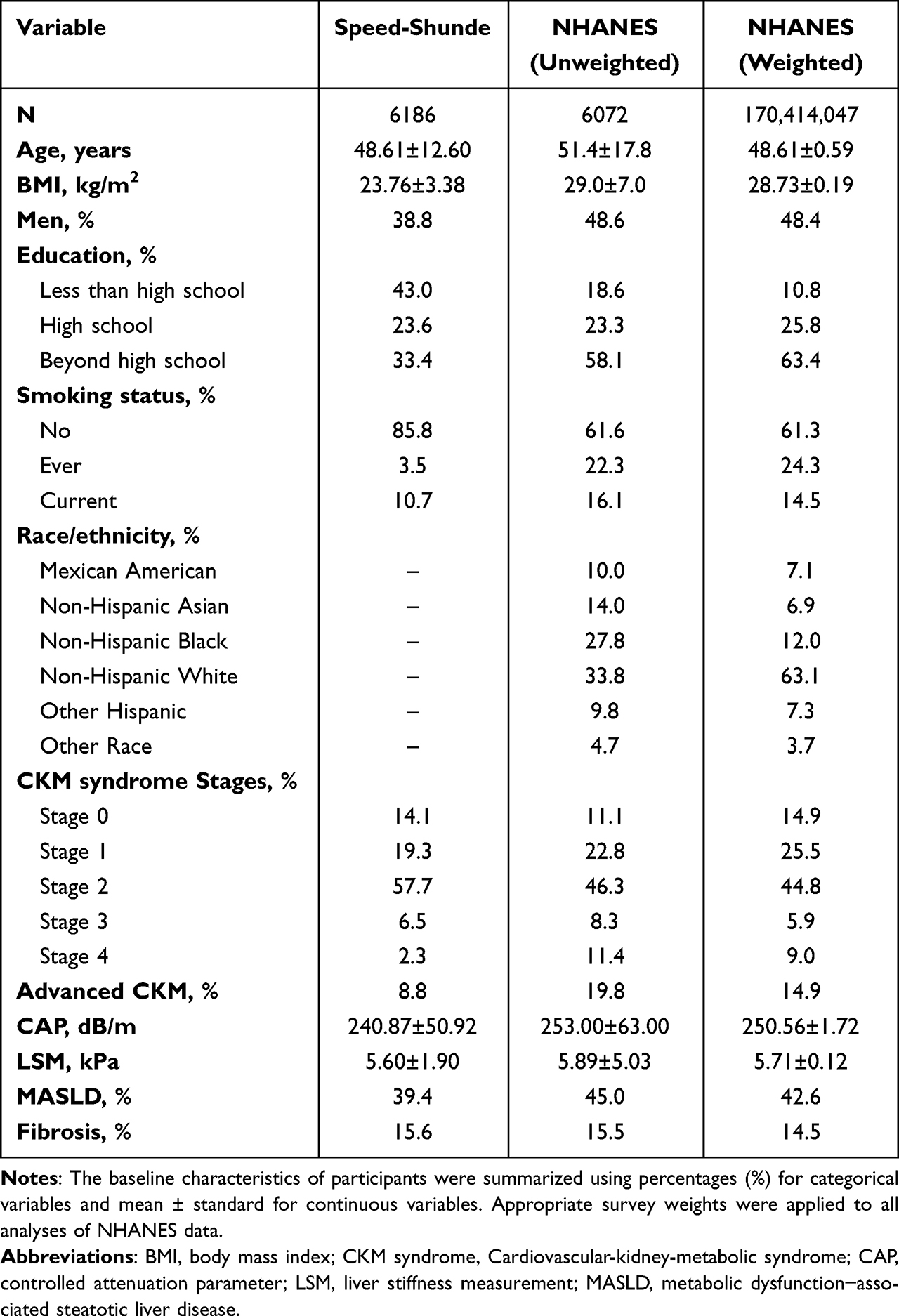 |
Table 1 Baseline Characteristics of Participants |
The NHANES population sample, weighted to represent approximately 170 million United States adults (mean age 48.61 ± 0.59 years; 48.4% male; mean BMI 28.73 ± 0.19 kg/m2). Regarding smoking habits, the majority of participants (61.3%) reported never having smoked, while 24.3% were former smokers and 14.5% were current smokers. The racial/ethnic composition included 7.1% Mexican American, 6.9% non-Hispanic Asian, 12.0% non-Hispanic Black, 63.1% non-Hispanic White, 7.3% other Hispanic, and 3.7% other race. The proportions of participants with CKM syndrome stages 0, 1, 2, 3, and 4 were 14.9%, 25.5%, 44.8%, 5.9%, and 9.0%, respectively, while advanced CKM syndrome was observed in 14.9% of participants. Among the NHANES, MASLD had a prevalence of 42.6%, and liver fibrosis was detected in 14.5% of individuals.
The Overlaps Between CKM Syndrome, MASLD, and Fibrosis
Figure 2 depicts a Venn diagram showing the frequencies and overlaps of CKM syndrome, MASLD, and fibrosis. In the Speed-Shunde cohort of 6186 participants, 98.9% of individuals with MASLD met criteria for CKM stages 1–4, compared with 89.5% of individuals with fibrosis. There were 1862 participants of overlap between MASLD and CKM stages 1–4, 317 participants of overlap between fibrosis and CKM stages 1–4, and 548 overlaps across all three categories (Figure 2A). Furthermore, overlaps were observed in 457 with both MASLD and fibrosis, 212 with MASLD and advanced CKM, 35 with fibrosis and advanced CKM, and 94 with all three conditions (Figure 2B).
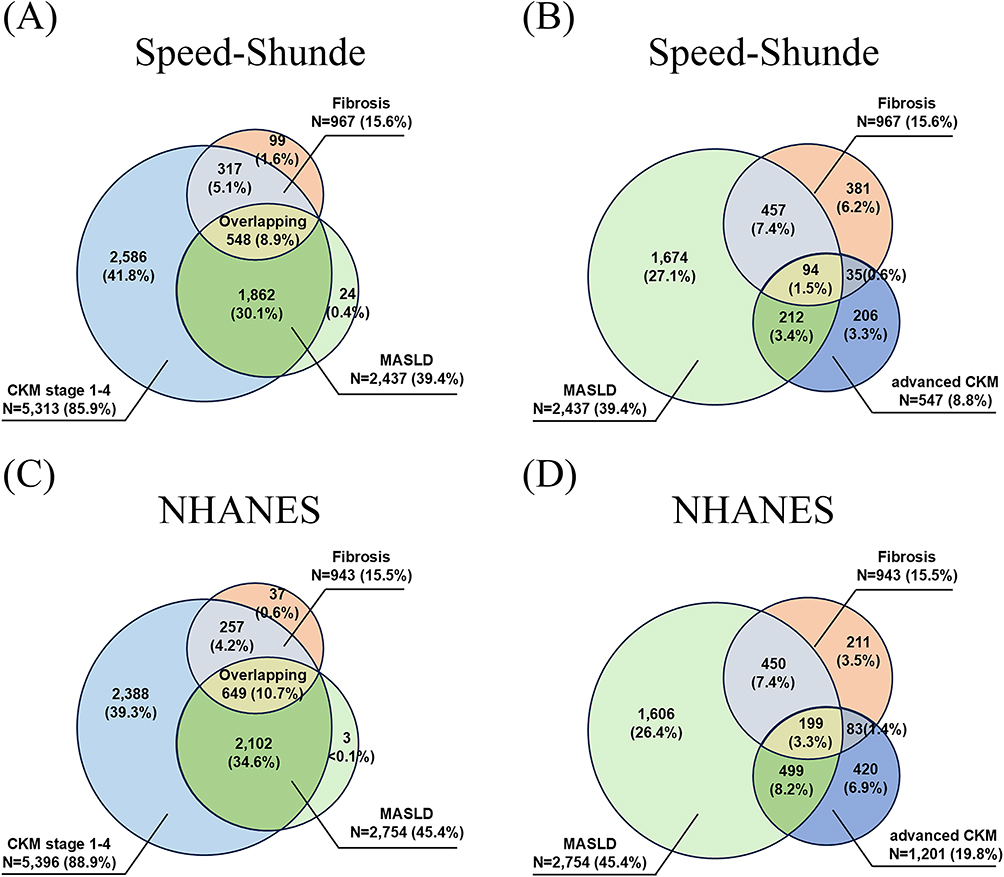 |
Figure 2 Venn diagram indicating the frequency and overlap of CKM syndrome, MASLD, and fibrosis. (A) Overlap of CKM stages1-4, MASLD, and fibrosis in the Speed-Shunde Cohort; (B) Overlap of advanced CKM, MASLD, and fibrosis in the Speed-Shunde Cohort; (C) Overlap of CKM stages1-4, MASLD, and fibrosis in the NHANES study; (D) Overlap of advanced CKM, MASLD, and fibrosis in the NHANES study; Numbers and proportions of the population within each overlapping segment are provided. Abbreviations: CKM, Cardiovascular-kidney-metabolic; MASLD, Metabolic dysfunction-associated steatotic liver disease. |
In the NHANES population sample of 6,72 persons in the United States, 99.9% of participants met the criteria for CKM stages 1–4, whereas 96.1% of individuals with fibrosis also met these criteria. There were 2102 cases of overlap between MASLD and CKM stages 1–4, 257 cases of overlap between fibrosis and CKM stages 1–4, and 649 cases involving all three conditions (Figure 2C). Further overlap analyses demonstrated that 450 had both MASLD and fibrosis,499 had MASLD and advanced CKM, 83 had fibrosis and advanced CKM, and 199 presented with all three conditions concurrently (Figure 2D).
Prevalence of Overlapping CKM Syndrome Stages in Participants with MASLD and MASLD-Related Fibrosis
Table 2 illustrates the prevalence of overlapping CKM syndrome stages among individuals with MASLD. In the Speed-Shunde cohort, the distribution of CKM syndrome stages differed significantly between participants without MASLD (n = 3749) and those with MASLD (n = 2437) (P < 0.001). In the non-MASLD group, 22.6%, 23.2%, 47.9%, 4.3%, and 2.1% were classified as stages 0–4, respectively. In contrast, in the MASLD group, the proportions were 1.1%, 13.4%, 73.0%, 10.0%, and 2.6%, respectively. In addition, the prevalence of advanced CKM syndrome (stages 3–4) was higher in the MASLD group compared with the non-MASLD group (12.6% vs 6.4%, P < 0.001). Similarly, in the NHANES population, the stage distribution also showed significant differences (P < 0.001). In the non-MASLD group, 25.8%, 28.4%, 35.8%, 3.9%, and 6.0% were classified as stages 0–4, respectively, compared with 0.1%, 21.5%, 56.8%, 8.5%, and 13.1% in the MASLD group. Furthermore, the prevalence of advanced CKM syndrome was higher in the MASLD group compared with the non-MASLD group (21.5% vs 9.9%, P < 0.001).
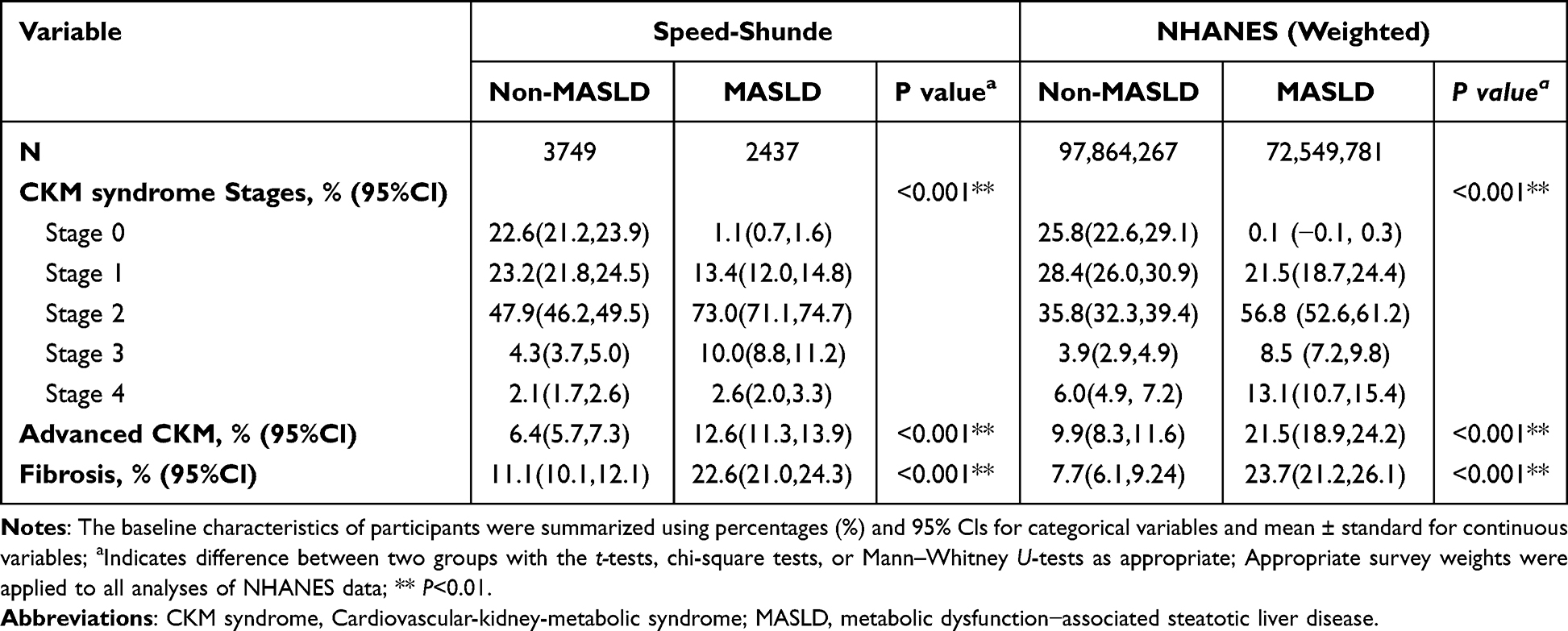 |
Table 2 Prevalence of Overlapping CKM Syndrome Stages in Participants with MASLD |
Table 3 illustrates the prevalence of overlapping CKM syndrome stages among individuals with MASLD-related fibrosis. The distribution of CKM syndrome stages in the Speed-Shunde cohort exhibited a significant difference between MASLD individuals without fibrosis (n = 1886) and those with fibrosis (n = 551) (P < 0.001). In the non-fibrosis group, the distribution across stages 0–4 was 1.3%, 14.8%, 72.6%, 9.1%, and 2.1%, respectively. In the MASLD-related fibrosis group, the proportions for stages 0 to 4 were 0.5%, 8.3%, 74.0%, 12.9%, and 4.2%, respectively. The prevalence of advanced CKM syndrome (stages 3–4) was greater in the MASLD-related fibrosis group compared to the non-fibrosis group (17.1% vs 11.2%, P < 0.001). In the NHANES population, the distribution of CKM stages exhibited substantial variations (P < 0.001). In the non-fibrosis group, the percentages classified as stages 0–4 were 0.1%, 23.9%, 55.8%, 8.2%, and 12.0%, respectively. In the MASLD-related fibrosis group, the percentages were 0%, 9.7%, 62.0%, 10.0%, and 18.4%, respectively. The prevalence of advanced CKM syndrome was again higher in the MASLD-related fibrosis group than in the non-fibrosis group (28.4% vs 20.1%, P = 0.002). Table S3 presents the unweighted prevalence of overlapping CKM syndrome stages with MASLD and MASLD-related fibrosis among NHANES participants.
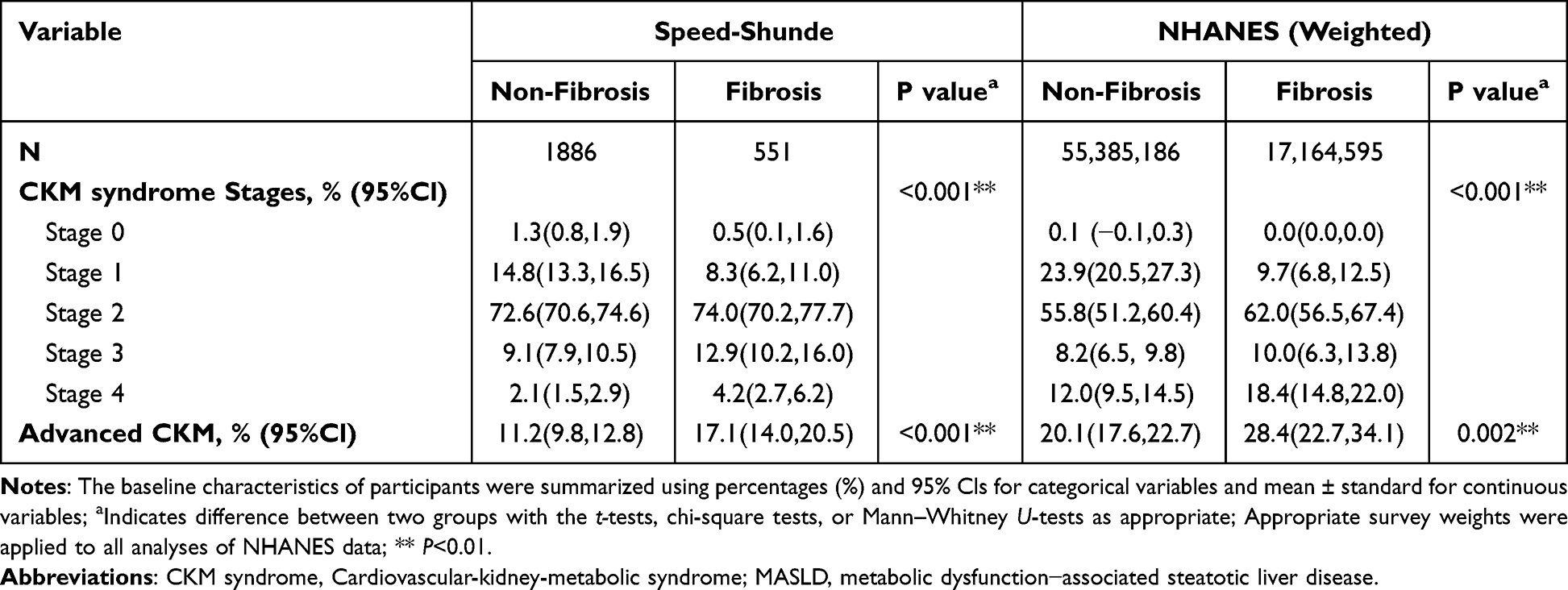 |
Table 3 Prevalence of Overlapping CKM Syndrome Stages in Participants with MASLD-Related Fibrosis |
Associations of CAP and MASLD with Advanced CKM Syndrome
Figure 3 depicts the results of a multivariable logistic regression analysis of the association between CAP and MASLD with advanced CKM syndrome. CAP was evaluated as a continuous and a categorical variable, based on quartiles in the general population. Each 10-unit increase in CAP values was positively associated with the prevalence of advanced CKM syndrome in both the Chinese (OR: 1.09, 95% CI: 1.06, 1.11) and the United States (OR: 1.04, 95% CI: 1.01, 1.06) populations. Compared to the lowest quartile (Q1), in the highest quartile of CAP (Q4) was associated with an increased odds of advanced CKM syndrome in both the Chinese (OR:2.61, 95% CI:1.89,3.63) and United States (OR:1.55, 95% CI: 1.07, 2.27) populations, with a significant linear trend across quartiles (P for trend < 0.001 for both). Compared with non-MASLD individuals, MASLD was independently associated with increased odds of advanced CKM stages, with ORs of 2.06 (95% CI: 1.64, 2.58) in the Chinese and 1.60 (95% CI: 1.22, 2.10) in the United States (both P < 0.01).
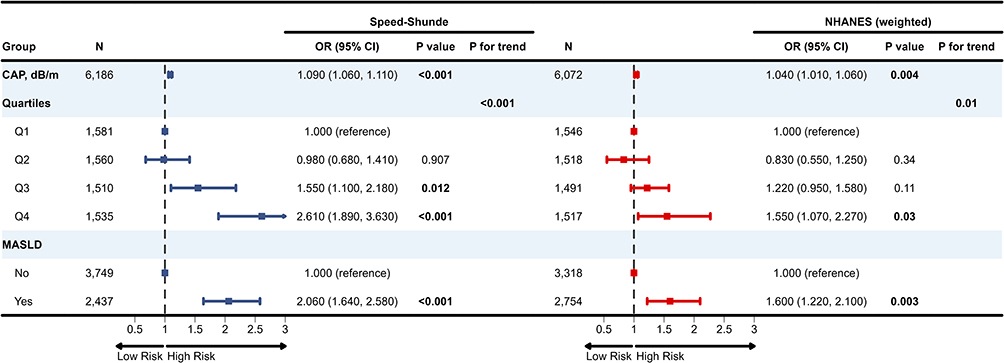 |
Figure 3 CAP and MASLD associations with advanced CKM syndrome, as assessed by multivariable logistic regression models. CAP values (dB/m) in the Speed-Shunde Cohort were categorized into quartiles: Q1 (100–205), Q2 (205–235), Q3 (235–270), and Q4 (270–400). CAP values (dB/m) in the NHANES study were categorized into quartiles: Q1 (100–209), Q2 (209–243), Q3 (243–296), and Q4 (296–400). The associations between advanced CKM syndrome and MASLD or CAP in the total population were analyzed using multivariable logistic regression models. The comprehensive model in the Speed-Shunde Cohort was controlled for age, sex, education, and smoking status, while in the NHANES study, it was further adjusted for race/ethnicity. Bold font indicates statistically significant differences (P<0.05). Abbreviations: OR, odds ratio; CI, confidence interval; CKM, Cardiovascular-kidney-metabolic; CAP, controlled attenuation parameter; MASLD, Metabolic dysfunction-associated steatotic liver disease. |
Associations of LSM and MASLD-Related Fibrosis with Advanced CKM Syndrome
Figure 4 depicts the results of a multivariable logistic regression analysis of the association between LSM and MASLD-related fibrosis with advanced CKM syndrome. Higher LSM values were positively associated with the prevalence of advanced CKM syndrome in both Chinese (OR: 1.16, 95% CI: 1.08, 1.24) and United States (OR: 1.04, 95% CI: 1.02, 1.07) MASLD participants. Moreover, MASLD participants with fibrosis were associated with higher odds of advanced CKM syndrome stages compared to those without fibrosis, with ORs of 1.55 (95% CI: 1.09, 2.18) in the Speed-Shunde cohort and 1.44 (95% CI: 1.01, 2.05) in the NHANES.
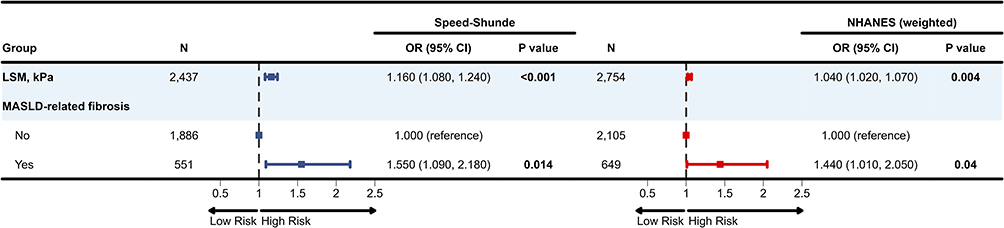 |
Figure 4 LSM and MASLD-related fibrosis associations with advanced CKM syndrome, as assessed by multivariable logistic regression models. The associations between advanced CKM syndrome and MASLD-related fibrosis or LSM among individuals with MASLD were analyzed using multivariable logistic regression models. The comprehensive model in the Speed-Shunde Cohort was controlled for age, sex, education, and smoking status, while in the NHANES study, it was further adjusted for race/ethnicity. Bold font indicates statistically significant differences (P<0.05). Abbreviations: OR, odds ratio; CI, confidence interval; CKM, Cardiovascular-kidney-metabolic; LSM, liver stiffness measurement; MASLD, Metabolic dysfunction-associated steatotic liver disease. |
Non-Linear Relationships Among CAP, LSM, and Advanced CKM Syndrome
Figure 5 demonstrates the dose-response correlation between advanced CKM syndrome and CAP in the general population, as well as between advanced CKM and LSM in individuals with MASLD. RCS analyses showed a positive linear relationship of CAP values with advanced CKM syndrome in both the Chinese and United States populations (P non-linear >0.05 and P overall <0.05). The OR crossed 1.0 at CAP values of approximately 235 dB/m in China and 243 dB/m in the United States, as shown in the spline curves (Figure 5A and B). Similarly, RCS analyses revealed a positive linear relationship between LSM values and advanced CKM syndrome in both Chinese and United States MASLD participants (P non-linear >0.05 and P overall <0.05). Furthermore, the OR crossed 1.0 at LSM values of approximately 5.7 kPa in China and 5.5 kPa in the United States, as shown in the spline curves (Figure 5C and D).
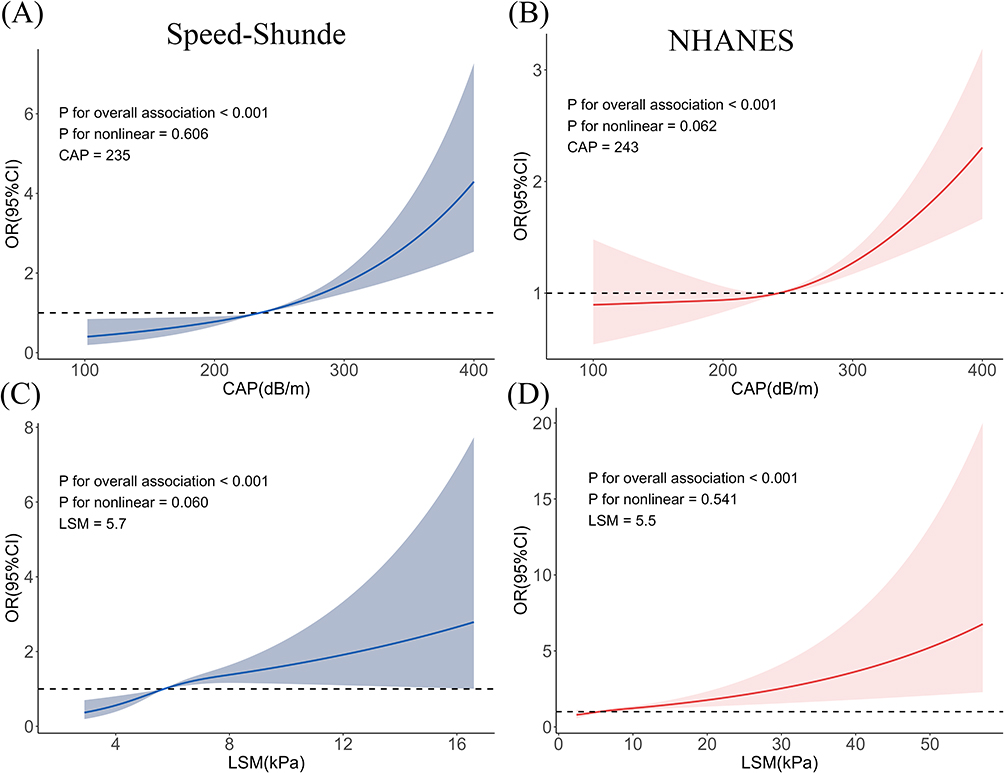 |
Figure 5 Non-linear associations among CAP, LSM, and advanced CKM syndrome. (A) Non-linear associations between CAP and advanced CKM in the Speed-Shunde Cohort; (B) Non-linear associations between CAP and advanced CKM in the NHANES study; (C) Non-linear associations between LSM and advanced CKM in the Speed-Shunde Cohort; (D) Non-linear associations between LSM and advanced CKM in the NHANES study; Non-linear associations between advanced CKM and CAP in the general population, as well as between advanced CKM and LSM in individuals with MASLD. An analysis employing RCS was conducted. The comprehensive model in the Speed-Shunde Cohort was controlled for age, sex, education, and smoking status, while in the NHANES study, it was further adjusted for race/ethnicity. The solid lines and shaded areas represent the central risk estimates and 95% CIs. Abbreviations: RCS, restricted cubic splines; CKM, Cardiovascular-kidney-metabolic; CAP, controlled attenuation parameter; LSM, liver stiffness measurement; MASLD, Metabolic dysfunction-associated steatotic liver disease. |
Discussion
To our knowledge, this work is an initial effort to investigate the associations of MASLD and its related fibrosis (via VCTE-based CAP/LSM) with the likelihood of having advanced CKM syndrome (stages 3–4) in a large, community-based Chinese population, with findings externally validated in the US NHANES cohort. Our primary findings are as follows: First, higher CAP values and MASLD were significantly correlated with elevated odds of advanced CKM syndrome. Second, higher LSM values and MASLD-related fibrosis were significantly associated with a higher likelihood of being in advanced CKM syndrome compared to individuals without fibrosis. Third, both CAP and LSM values exhibited positive, linear relationships with advanced CKM syndrome. Notably, these robust associations were consistent in both the Chinese and US populations, which vary in ethnicity and lifestyle. These findings support the importance of evaluating liver health, particularly MASLD and associated fibrosis (eg, via VCTE-based CAP/LSM), for risk stratification in CKM syndrome.
Considering the common risk factors, overlapping physiological mechanisms, and management strategies in both MASLD and CKM frameworks,16,27 there is an appeal to graft the two together. In this study, we quantified the prevalence of MASLD and associated fibrosis across the CKM syndrome spectrum and characterized their overlap and correlations in Chinese and US populations. Approximately 90% of patients were classified in CKM stages 1–4, with high prevalences of MASLD (39.4% in China; 42.6% in the US) and liver fibrosis (15.6% in China; 14.5% in the US), consistent with the global epidemiology of these diseases.3,6,7,28 Notably, there was substantial overlap among MASLD, fibrosis, and the stages of CKM syndrome, with nearly all individuals with MASLD and the majority with fibrosis presenting with CKM syndrome stages 1–4. The significant overlap is partially due to a definitional tautology, as CKM stage ≥1 embeds metabolic criteria that overlap with MASLD definitions,1,7 the near-universal co-occurrence should not be over-interpreted. Advanced CKM syndrome (Stages 3–4)—a high-risk condition characterized by a significantly increased burden of overt clinical disease and a worse prognosis—was present in 8.8% of the Chinese and 14.9% of the US populations. The study further identified a subset of individuals with co-occurring MASLD and/or fibrosis and advanced CKM syndrome. Given this context, we therefore focused on characterizing the relationships between MASLD, its associated fibrosis, and advanced CKM syndrome.
MASLD is increasingly acknowledged as a pivotal contributor to development and progression of subclinical ASCVD,12,29–31 clinical CVD,13,32,33 and CKD.14,15 A cohort study encompassing 26,676 patients with steatotic liver disease demonstrated that MASLD exhibited a 2.52-fold elevated risk of heart failure.34 Furthermore, a meta-analysis of sixteen retrospective cohort studies identified a significant connection between MASLD and an increased long-term risk of developing atrial fibrillation.35 It is also well-documented that MASLD significantly increases the risk of both incident CKD and abnormal proteinuria.14,36,37 However, previous research has primarily examined the link between hepatic steatosis (or MASLD) and single-organ diseases (eg, type 2 diabetes, CKD, or CVD). There is still a significant knowledge gap concerning how MASLD and CKM syndrome are interconnected as part of a unified, progressive continuum. In the present study, the prevalence of advanced CKM syndrome was significantly higher in the MASLD group compared to the non-MASLD group. Correspondingly, MASLD and higher CAP values were significantly associated with elevated odds of advanced CKM syndrome (stages 3–4). More recently, a cross-sectional study by Yang et al38 found that the hepatic steatosis (assessed by the Framingham Steatosis Index, FSI) was significantly associated with an increased risk of advanced CKM syndrome. Similarly, a retrospective Korean cohort study by Kim et al39 reported that hepatic steatosis (defined by a fatty liver index (FLI) ≥ 60) was also associated with a higher risk of cardiovascular events across the spectrum of CKM stages. Liu et al40 identified non-alcoholic fatty liver disease (NAFLD) as a key driver accelerating CKM progression and mortality. In contrast to above studies that relied on surrogate markers for hepatic steatosis (eg, FSI/FLI) and did not evaluate the new MASLD definition, our study employed VCTE-based CAP as a non-invasive method to diagnose and quantify MASLD, providing more direct evidence for its independent association with advanced CKM syndrome.
It is also increasingly recognized that the presence and severity of liver fibrosis in MASLD are independently associated with both cardiovascular and renal outcomes. Studies using non-invasive fibrosis assessment tools, such as the Fibrosis-4 (FIB-4) Index, NAFLD Fibrosis Score (NFS), and VCTE, indicate that higher fibrosis scores are linked to a greater risk of major adverse cardiovascular events, CKD, and mortality.41–43 In addition, the AHA scientific statement on CKM syndrome endorses screening for advanced liver fibrosis using the FIB-4 index every 1–2 years in patients with MASLD who have coexisting metabolic risk factors (typically CKM stage 2 or higher).1 However, whether the presence and severity of liver fibrosis (VCTE-based LSM) in MASLD confer a risk of advanced CKM syndrome remains unclear. In the present study, we observed that elevated LSM values and MASLD-related fibrosis were significantly associated with a higher risk of advanced CKM syndrome. This finding is consistent with earlier studies that employed non-invasive liver fibrosis scores like FIB-4 and NFS. Liu et al40 showed that the prevalence of advanced liver fibrosis (defined by FIB-4) increased markedly in individuals at higher CKM stages. Additionally, research by Ren et al44 demonstrated that the relationship between liver fibrosis, as measured by NFS, and increased cardiorenal disease risk, as well as CKM stage, exists independently of traditional risk factors in diabetic patients. In a cohort of individuals with similar CKM stages, those with advanced liver fibrosis were significantly associated with higher all-cause mortality.40 Collectively, the existing literature indicates that the extent of liver fibrosis is an important modifier of the global risk profile among individuals with CKM. Notably, the presence of MASH and liver fibrosis thus provides extra rationale for the lifestyle and pharmacologic interventions (eg, incretin therapies) already recommended for CVD prevention in patients with CKM syndrome.2 Therefore, our findings provide insight that individuals diagnosed with MASLD, particularly those with advanced liver fibrosis identified by LSM, should be regarded as high-risk populations (CKM stages 3 to 4).
The strong correlation between MASLD, MASLD-related fibrosis, and advanced CKM syndrome could be mechanistically plausible. The liver’s central role in metabolic homeostasis means that hepatic steatosis initiates a cascade of systemic disturbances.45 The lipotoxic environment exacerbates oxidative stress,46 activating inflammatory pathways (eg, NF-κB) and prompting the steatotic liver to secrete pro-inflammatory cytokines (eg, TNF-α, IL-6)47 and pro-thrombotic factors (eg, PAI-1).48 These mediators induce systemic inflammation, endothelial dysfunction, and hepatic and peripheral insulin resistance, which are essential contributors to the progression of ASCVD and CKD.49 The progression to liver fibrosis signifies a significant intensification, significantly worsening this systemic metabolic and inflammatory dysregulation.50 The fibrotic process extends beyond hepatic scarring; it enhances the secretion of profibrotic and inflammatory mediators that can cause direct or indirect harm to extrahepatic tissues. This multifactorial injury to the vascular endothelium and renal glomeruli provides a mechanistic basis for the progression of CKM syndrome to its advanced stages,51 thereby contributing to an increased risk of advanced CKM syndrome. Nonetheless, higher CKM stages may also accelerate MASLD progression. Thus, whether the relationship between MASLD, MASLD-related fibrosis, and advanced CKM syndrome is causal or primarily driven by shared metabolic risk factors remains uncertain. Further longitudinal studies and mechanistic investigations are warranted.
Interestingly, CAP values in the general population and LSM values among individuals with MASLD both showed linear positive associations with advanced CKM risk. Our earlier work demonstrated independent associations of CAP and LSM with 10-year ASCVD risk in the general population, with CAP ≥ 301 dB/m marking a sharp rise in ASCVD risk,52 providing a potential threshold for family physicians to intensify cardiovascular risk stratification. In addition, findings from a cross-sectional study by Zhang et al53 indicated that LSM is linearly and positively associated with carotid atherosclerosis and brachial-ankle pulse wave velocity, suggesting that LSM may serve as a useful predictor of subclinical atherosclerosis in patients with MASLD. Notably, We observed that the OR crossed 1.0 at CAP values of 235–243 dB/m and LSM values of 5.5–5.7 kPa—thresholds that lie near, or even slightly below, commonly accepted cut-offs for hepatic steatosis and clinically significant fibrosis.20 Together, these findings support the potential utility of VCTE as quantitative imaging biomarkers for CKM risk stratification. CAP and LSM, employed for early MASLD detection and liver fibrosis assessment within the CKM framework, can effectively identify high-risk populations (CKM stages 3 to 4). Moreover, future research should evaluate whether incorporating VCTE parameters, such as CAP and LSM, into CKM staging and established prediction models, such as the PREVENT equations, provides incremental prognostic value.
The study’s strengths include the use of a large, community-based Chinese cohort and external validation with US NHANES data. Despite the US population having a higher average BMI and greater prevalence of advanced CKM syndrome (14.9% vs 8.8%), the associations of MASLD and liver fibrosis with advanced CKM were consistent across both populations. This cross-validation improves the data’s generalizability and reliability. The study also used objective, quantitative, non-invasive tools, such as VCTE, to assess hepatic steatosis and fibrosis, addressing the limitations of conventional biochemical scores and ultrasonography. Despite its strengths, this study has limitations. First, both the Speed-Shunde and NHANES investigations are cross-sectional. Since the data only show prevalence and associations at a single point, it is not possible to draw direct conclusions about causality. The critical question of whether MASLD directly drives the progression of CKM syndrome or, conversely, if severe CKM syndrome promotes the development of MASLD and hepatic fibrosis, remains unanswered. Furthermore, the possibility that a common underlying pathophysiological factor drives both conditions warrants careful consideration. We need longitudinal studies to understand the sequence of events and causal pathways linking the progression of MASLD, the development of fibrosis, and the progression of CKM syndrome. Second, the presence of missing data represents a limitation, potentially introducing bias to our estimates and reducing the generalizability of the results. Third, only clinical characteristics present in the Speed-Shunde and NHANES cohorts were considered in the analysis. The absence of data on subclinical heart failure, peripheral arterial disease, subclinical ASCVD, and atrial fibrillation in both datasets may have resulted in underestimation of CKM stages 3 and 4. The observed comorbidity between MASLD and CKM syndrome in this study is based solely on the Speed-Shunde (China) and NHANES (United States) cohorts. While the findings are context-specific to these populations, it is crucial to acknowledge that the Speed-Shunde cohort used robust sampling techniques, thereby improving its generalizability to the broader Chinese population.
Conclusion
In conclusion, within a community-based Chinese cohort, validated in the United States NHANES, both MASLD and MASLD-related fibrosis were associated with a higher prevalence of advanced CKM syndrome (stages 3–4), and higher CAP/LSM levels showed positive linear associations with advanced CKM syndrome. Collectively, these findings support evaluating liver health (eg, VCTE-based CAP/LSM) when risk-stratifying CKM, while recognizing the cross-sectional design and measurement constraints. Prospective, mediation-aware, and mechanistic studies are needed to establish temporality, incremental prognostic value, and clinical utility.
Abbreviations
AHA, the American Heart Association; ASCVD, atherosclerotic cardiovascular disease; BMI, body mass index; CAP, controlled attenuation parameter; CARDIAL-MS, CArdio-Renal-DIAbetes-Liver-Metabolic Syndrome; CI, Confidence Intervals; CKM, Cardiovascular-kidney-metabolic syndrome; CKD, chronic kidney disease; CVD, cardiovascular disease; eGFR, estimated glomerular filtration rate; FIB-4, Fibrosis-4 Index; FLI, fatty liver index; FSI, Framingham Steatosis Index; IL-6, interleukin-6; KDIGO, Kidney Disease, Improving Global Outcomes; LSM, liver stiffness measurement; MASLD, Metabolic dysfunction-associated steatotic liver disease; MASH, metabolic dysfunction–associated steatohepatitis; NAFLD, non-alcoholic fatty liver disease; NCHS, National Center for Health Statistics; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; NFS, NAFLD Fibrosis Score; NHANES, National Health and Nutrition Examination Survey; OR, odds ratios; PAI-1, plasminogen activator inhibitor-1; PSU, primary sampling units; RCS, restricted cubic spline; SE, standard errors; SPSS, Statistical Package for the Social Sciences; TNF-α, tumor necrosis factor-alpha; UACR, urinary albumin-to-creatinine ratio; VCTE, Vibration-controlled transient elastography.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study protocol of the Speed-Shunde study (20211103) was approved by the Ethics Committee of the Eighth Affiliated Hospital (The First People’s Hospital of Shunde) of Southern Medical University in accordance with the ethical guidelines of the 1975 Declaration of Helsinki. Informed and written consent was obtained from all participants before enrollment. Trial registration: Registry: http://www.chictr.org.cn/, TRN: ChiCTR2100054130, Registration date: 9 December, 2021. Moreover, the NHANES data are publicly available and fully de-identified. The NHANES study protocol was approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board, and all participants provided written informed consent. The NHANES procedures complied with the Declaration of Helsinki. Further details are available at https://www.cdc.gov/nchs/nhanes/. In accordance with Item 1 and Item 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (February 18, 2023, China), and as confirmed by the Ethics Committee, this study is exempt from additional ethical approval.
Acknowledgments
The authors would like to offer their heartfelt thanks to everyone who contributed their time and expertise to this project. The authors thank AiMi Academic Services (www.aimieditor.com) for English language editing and review services.
Author Contributions
Shidi Hu: Data Curation, Methodology, Investigation, Formal Analysis, Writing - Original Draft;
Dongmei Wang: Data Curation, Methodology, Investigation, Writing - Original Draft;
Qingtao Yu: Visualization, Investigation, Software, Writing - Original Draft;
Zhi Chen: Resources, Data Curation, Investigation, Writing - Review & Editing;
Weiguo Lu: Resources, Data Curation, Investigation, Writing - Review & Editing;
Yuan Meng: Data Curation, Validation, Writing - Review & Editing;
Xuetao Peng: Data Curation, Validation, Writing - Review & Editing;
Lan Liu: Conceptualization, Resources, Supervision, Writing - Review & Editing;
Heng Wan: Conceptualization, Project Administration, Writing - Original Draft;
Jie Shen: Conceptualization, Funding Acquisition, Resources, Supervision, Writing - Review & Editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Foshan Medical Research Project [20240470], the Foshan Self-funded Science and Technology Innovation Project [2320001006901], the Department of Education Higher Education Special Project-Teaching Reform Category [2023GXJK093], the Guangdong Provincial Department of Education General Higher Education Special Innovation Project [2023WTSCX011], the Clinical Research Start Plan of the Eighth Affiliated Hospital of Southern Medical University [CRSP2022001], and the Foshan Self-funded Science and Technology Innovation Projects [No.2420001004610].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ndumele CE, Rangaswami J, Chow SL, et al. Cardiovascular-kidney-metabolic health: a presidential advisory from the American Heart Association. Circulation. 2023;148(20):1606–1635. doi:10.1161/CIR.0000000000001184
2. Ndumele CE, Neeland IJ, Tuttle KR, et al. A synopsis of the evidence for the science and clinical management of Cardiovascular-Kidney-Metabolic (CKM) syndrome: a scientific statement from the American Heart Association. Circulation. 2023;148(20):1636–1664. doi:10.1161/CIR.0000000000001186
3. Aggarwal R, Ostrominski JW, Vaduganathan M. Prevalence of cardiovascular-kidney-metabolic syndrome stages in US adults, 2011-2020. JAMA. 2024;331(21):1858–1860. doi:10.1001/jama.2024.6892
4. Minhas AMK, Mathew RO, Sperling LS, et al. Prevalence of the cardiovascular-kidney-metabolic syndrome in the United States. J Am Coll Cardiol. 2024;83(18):1824–1826. doi:10.1016/j.jacc.2024.03.368
5. Carney EF. Cardiovascular mortality increases with stage of cardiovascular-kidney-metabolic syndrome. Nat Rev Nephrol. 2025;21(5):283. doi:10.1038/s41581-025-00957-y
6. Liu S, Wan H, Yang L, Shen J, Qi X. LiverHome study g. high prevalence of steatotic liver disease and fibrosis in the general population: a large prospective study in China. J Hepatol. 2025;82(1):e23–e25. doi:10.1016/j.jhep.2024.07.026
7. Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79(6):1542–1556. doi:10.1016/j.jhep.2023.06.003
8. Zhao D, Zheng X, Wang L, Xie Y, Chen Y, Zhang Y. Overlap prevalence and interaction effect of cardiometabolic risk factors for metabolic dysfunction-associated steatotic liver disease. Nutr Metab. 2025;22(1):10. doi:10.1186/s12986-025-00903-6
9. Lee HH, Lee HA, Kim EJ, et al. Cardiovascular risk from metabolic dysfunction-associated steatotic liver disease, cardiometabolic risk factor count, and their longitudinal changes: a nationwide cohort study. Am J Gastroenterol. 2025;120(10):2321–2329. doi:10.14309/ajg.0000000000003274
10. Bilson J, Mantovani A, Byrne CD, Targher G. Steatotic liver disease, MASLD and risk of chronic kidney disease. Diabetes Metab. 2024;50(1):101506. doi:10.1016/j.diabet.2023.101506
11. Targher G, Day CP, Bonora E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med. 2010;363(14):1341–1350. doi:10.1056/NEJMra0912063
12. Duell PB, Welty FK, Miller M, et al. Nonalcoholic fatty liver disease and cardiovascular risk: a scientific statement from the American Heart Association. Arterioscler Thromb Vasc Biol. 2022;42(6):e168–e185. doi:10.1161/ATV.0000000000000153
13. Muzurovic E, Peng CC, Belanger MJ, Sanoudou D, Mikhailidis DP, Mantzoros CS. Nonalcoholic fatty liver disease and cardiovascular disease: a review of shared cardiometabolic risk factors. Hypertension. 2022;79(7):1319–1326. doi:10.1161/HYPERTENSIONAHA.122.17982
14. Heo JH, Lee MY, Kim SH, et al. Comparative associations of non-alcoholic fatty liver disease and metabolic dysfunction-associated steatotic liver disease with risk of incident chronic kidney disease: a cohort study. Hepatobiliary Surg Nutr. 2024;13(5):801–813. doi:10.21037/hbsn-23-558
15. Mantovani A, Zaza G, Byrne CD, et al. Nonalcoholic fatty liver disease increases risk of incident chronic kidney disease: a systematic review and meta-analysis. Metabolism. 2018;79:64–76. doi:10.1016/j.metabol.2017.11.003
16. Godoy-Matos AF, Valerio CM, Junior WSS, de Araujo-Neto JM, Sposito AC, Suassuna JHR. CARDIAL-MS (CArdio-Renal-DIAbetes-Liver-Metabolic Syndrome): a new proposition for an integrated multisystem metabolic disease. Diabetol Metab Syndr. 2025;17(1):218. doi:10.1186/s13098-025-01796-4
17. Kawaharata W, Tanaka M, Sato T, et al. Incorporation of metabolic dysfunction-associated steatotic liver disease in the health stage of cardiovascular-kidney-metabolic syndrome improves predictive ability for coronary artery disease in a Japanese general population. J Am Heart Assoc. 2025;14:e043173. doi:10.1161/JAHA.125.043173
18. Khan SS, Matsushita K, Sang Y, et al. Development and validation of the American Heart Association’s PREVENT equations. Circulation. 2024;149(6):430–449. doi:10.1161/CIRCULATIONAHA.123.067626
19. Chan KE, Ong EYH, Chung CH, et al. Longitudinal outcomes associated with metabolic dysfunction-associated steatotic liver disease: a meta-analysis of 129 studies. Clin Gastroenterol Hepatol. 2024;22(3):488–498e414. doi:10.1016/j.cgh.2023.09.018
20. Lin H, Lee HW, Yip TC, et al. Vibration-controlled transient elastography scores to predict liver-related events in steatotic liver disease. JAMA. 2024;331(15):1287–1297. doi:10.1001/jama.2024.1447
21. Wan H, Yu G, Xu S, et al. Central sensitivity to free triiodothyronine with MAFLD and its progression to liver fibrosis in euthyroid adults. J Clin Endocrinol Metab. 2023;108(9):e687–e697. doi:10.1210/clinem/dgad186
22. Wan H, Yao N, Yang J, et al. Cohort profile: the prospective cohort study on the incidence of metabolic diseases and risk factors in Shunde, China (Speed-Shunde cohort). Eur Heart J Qual Care Clin Outcomes. 2025;11(1):3–9. doi:10.1093/ehjqcco/qcae077
23. Wan H, Yu G, He Y, et al. Associations of thyroid feedback quantile-based index with diabetes in euthyroid adults in the United States and China. Ann Med. 2024;56(1):2318418. doi:10.1080/07853890.2024.2318418
24. Wang D, Ye H, Liu S, et al. Sex- and age-specific associations of serum essential elements with diabetes among the Chinese adults: a community-based cross-sectional study. Nutr Metab. 2024;21(1):44. doi:10.1186/s12986-024-00801-3
25. Leung CW, Tapper EB. Sugar-sweetened beverages are associated with increased liver stiffness and steatosis among apparently healthy adults in the United States. Clin Gastroenterol Hepatol. 2022;20(4):959–961e951. doi:10.1016/j.cgh.2021.05.052
26. Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med. 2021;385(19):1737–1749. doi:10.1056/NEJMoa2102953
27. Theodorakis N, Nikolaou M. From cardiovascular-kidney-metabolic syndrome to cardiovascular-renal-hepatic-metabolic syndrome: proposing an expanded framework. Biomolecules. 2025;15(2):213. doi:10.3390/biom15020213
28. Huang Q, Li Y, Zhou X, Zou X, Ji L. Prevalence of the cardiovascular-kidney-metabolic syndrome in 3 Chinese cohorts. JACC Asia. 2025;5(1):116–118. doi:10.1016/j.jacasi.2024.10.016
29. VanWagner LB, Wilcox JE, Colangelo LA, et al. Association of nonalcoholic fatty liver disease with subclinical myocardial remodeling and dysfunction: a population-based study. Hepatology. 2015;62(3):773–783. doi:10.1002/hep.27869
30. Baek JW, Yang YS, Jung KJ, et al. Metabolic dysfunction-associated steatotic liver disease, liver fibrosis and risk of cardiovascular disease: a prospective cohort study. Nutr Metab Cardiovasc Dis. 2024;34(12):2623–2629. doi:10.1016/j.numecd.2024.09.001
31. Chimakurthi CR, Rowe IA. Establishing the Independence and clinical importance of non-alcoholic fatty liver disease as a risk factor for cardiovascular disease. J Hepatol. 2016;65(6):1265–1266. doi:10.1016/j.jhep.2016.06.034
32. Ogawa T, Sato T, Tanaka M, et al. Metabolic dysfunction-associated steatotic liver disease (MASLD) Is an independent risk factor for the development of ischemic heart disease - a 10-year cohort study. Circ Rep. 2025;7(5):350–358. doi:10.1253/circrep.CR-25-0019
33. Prasad M, Gupta S, Sarin SK. The Independent association of non-alcoholic fatty liver disease with incident cardiovascular disease: a GRADE evaluation of the evidence through a systematic review and meta-analysis. J Clin Exp Hepatol. 2024;14(1):101277. doi:10.1016/j.jceh.2023.08.013
34. Chang KC, Su TH, Wu CK, et al. Metabolic dysfunction-associated steatotic liver disease is associated with increased risks of heart failure. Eur J Heart Fail. 2025;27(3):512–520. doi:10.1002/ejhf.3567
35. Mantovani A, Morandin R, Sani E, et al. MASLD is associated with an increased long-term risk of atrial fibrillation: an updated systematic review and meta-analysis. Liver Int. 2025;45(1):e16128. doi:10.1111/liv.16218
36. Chen WY, Zhang JH, Chen LL, et al. Bioactive metabolites: a clue to the link between MASLD and CKD? Clin Mol Hepatol. 2025;31(1):56–73. doi:10.3350/cmh.2024.0782
37. Gao J, Li Y, Zhang Y, et al. Severity and remission of metabolic dysfunction-associated fatty/steatotic liver disease with chronic kidney disease occurrence. J Am Heart Assoc. 2024;13(5):e032604. doi:10.1161/JAHA.123.032604
38. Yang F, Gao X, Tang R, Yang K. The Framingham steatosis index as a predictor of advanced CKM syndrome in US adults: evidence from NHANES 2001 to 2018. Medicine. 2025;104(39):e44800. doi:10.1097/MD.0000000000044800
39. Kim BS, Kim HJ, Kim H, et al. Hepatic steatosis in cardiovascular-kidney-metabolic syndrome: fatty liver index as a predictor of cardiovascular outcomes. Eur J Prev Cardiol. 2025. doi:10.1093/eurjpc/zwaf396
40. Liu J, Gao L, Chen J, et al. Prevalence and long-term outcomes of NAFLD and cardiovascular-kidney-metabolic health in the United States. Am J Prev Cardiol. 2025;23:101049. doi:10.1016/j.ajpc.2025.101049
41. Jung CY, Ryu GW, Kim HW, Ahn SH, Kim SU, Kim BS. Advanced liver fibrosis measured by transient elastography predicts chronic kidney disease development in individuals with non-alcoholic fatty liver disease. Diabetologia. 2022;65(3):518–527. doi:10.1007/s00125-021-05627-9
42. Ye Z, Xie E, Guo Z, et al. Association of liver fibrosis markers with mortality outcomes in patients with chronic kidney disease and coronary artery disease: insights from the NHANES 1999-2018 data. Cardiorenal Med. 2025;15(1):153–163. doi:10.1159/000543500
43. Anstee QM, Berentzen TL, Nitze LM, et al. Prognostic utility of Fibrosis-4 Index for risk of subsequent liver and cardiovascular events, and all-cause mortality in individuals with obesity and/or type 2 diabetes: a longitudinal cohort study. Lancet Reg Health Eur. 2024;36:100780. doi:10.1016/j.lanepe.2023.100780
44. Ren H, Hu M, Yan Y, et al. Association of the metabolic dysfunction-associated steatotic liver disease with cardiovascular and kidney disease in patients with type 2 diabetes mellitus: a cross-sectional study. Diabet Res Clin Pract. 2025;229:112927. doi:10.1016/j.diabres.2025.112927
45. Byrne CD, Armandi A, Pellegrinelli V, Vidal-Puig A, Bugianesi E. Muetabolic dysfunction-associated steatotic liver disease: a condition of heterogeneous metabolic risk factors, mechanisms and comorbidities requiring holistic treatment. Nat Rev Gastroenterol Hepatol. 2025;22(5):314–328. doi:10.1038/s41575-025-01045-z
46. Polimeni L, Del Ben M, Baratta F, et al. Oxidative stress: new insights on the association of non-alcoholic fatty liver disease and atherosclerosis. World J Hepatol. 2015;7(10):1325–1336. doi:10.4254/wjh.v7.i10.1325
47. Rafaqat S, Gluscevic S, Mercantepe F, Rafaqat S, Klisic A. Interleukins: pathogenesis in non-alcoholic fatty liver disease. Metabolites. 2024;14(3):153. doi:10.3390/metabo14030153
48. Stupia R, Lombardi R, Cattazzo F, et al. Prevalence of portal vein thrombosis in non-alcoholic fatty liver disease: a meta-analysis of observational studies. J Thromb Thrombolysis. 2024;57(2):330–336. doi:10.1007/s11239-023-02912-9
49. Bo T, Gao L, Yao Z, et al. Hepatic selective insulin resistance at the intersection of insulin signaling and metabolic dysfunction-associated steatotic liver disease. Cell Metab. 2024;36(5):947–968. doi:10.1016/j.cmet.2024.04.006
50. Povero D, Busletta C, Novo E, et al. Liver fibrosis: a dynamic and potentially reversible process. Histol Histopathol. 2010;25(8):1075–1091. doi:10.14670/HH-25.1075
51. Kimura T, Yamazaki T, Estrela GR. Editorial: multi-organ linkage pathophysiology and therapy for NAFLD and NASH. Front Endocrinol. 2024;15:1418066. doi:10.3389/fendo.2024.1418066
52. Gui Z, Chen X, Wang D, et al. Inflammatory and metabolic markers mediate the association of hepatic steatosis and fibrosis with 10-year ASCVD risk. Ann Med. 2025;57(1):2486594. doi:10.1080/07853890.2025.2486594
53. Zhang H, Lin F, Miao M, Yu C, Guo W. Liver fibrosis increases the risk of subclinical atherosclerosis in patients with MASLD: a cross-sectional and longitudinal study. Nutr Metab. 2025;22(1):68. doi:10.1186/s12986-025-00951-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.