Back to Journals » Advances in Medical Education and Practice » Volume 17
Mentoring in Specialty Training in Oman: Insights from Trainees’ Perspectives and Experiences
Authors Al Maawali A, AlMaashari K, AlRiyami B, Al Bualy R, AlSawafi A ![]()
Received 25 February 2026
Accepted for publication 13 June 2026
Published 9 July 2026 Volume 2026:17 599319
DOI https://doi.org/10.2147/AMEP.S599319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sateesh Arja
Ali Al Maawali,1,2 Kawthar AlMaashari,1 Bahia AlRiyami,1 Raghdah Al Bualy,1 Aza AlSawafi1,2
1Oman Medical Specialty Board, Muscat, Oman; 2Child health department, Royal Hospital, Ministry of Health, Muscat, Oman
Correspondence: Aza AlSawafi, Email [email protected]
Background: Mentorship is an important component of medical education, supporting trainees’ professional and personal development. However, limited evidence from Oman explores residents’ experiences with mentorship during specialty training.
Objective: To assess residents’ perspectives and experiences of mentorship during specialty training at the Oman Medical Specialty Board (OMSB), evaluate how mentorship addresses their needs, and identify perceived challenges.
Methodology: A cross-sectional study was conducted among all residents enrolled in OMSB training programs. A structured, self-administered questionnaire was developed based on literature review and expert input, and piloted to ensure clarity and content validity. The survey was distributed electronically via SurveyMonkey. Inclusion criteria included all active OMSB residents, while those not in training during the study period were excluded. Descriptive analysis was performed to summarize responses.
Results: Of 718 eligible OMSB residents, 450 complete responses were included after excluding 16 incomplete responses, yielding a complete-case response rate of 62.7%. Overall, 230 residents (51.1%) reported having a mentor, 217 (48.2%) reported not having one, and 3 (0.7%) were unsure. Among residents with mentors, 57.1% had a formally assigned mentor. Mentorship was perceived to support academic goals by 75.0% and career opportunities by 62.7%. Commonly reported barriers included insufficient time for mentorship (85.4%), lack of skilled mentors (81.2%), lack of formalized objectives (80.4%), lack of personal connection (78.9%), and lack of formalized meeting times (75.9%). Subgroup analyses showed selected differences by gender and residency level.
Conclusion: Mentorship was perceived positively by many residents; however, only about half reported access to a mentor, and experiences varied by subgroup. Several structural challenges were identified, particularly limited time, insufficient skilled mentors, lack of formalized objectives, and weak mentor–mentee connection. These findings suggest a need for more structured and consistently implemented mentorship approaches within OMSB, including clearer program frameworks, mentor training, protected mentorship time, and support for both mentors and mentees.
Keywords: mentorship, medical education, specialty training, residents, Oman
Introduction
Medical careers are demanding and require not only the acquisition of clinical knowledge and technical skills, but also an understanding of professional values, institutional cultures, and healthcare systems. Residency training represents a critical stage in this process, during which learners refine their competencies while adapting to complex clinical environments. Mentorship is widely recognized as an important mechanism to support this development.
Mentorship is commonly defined as a developmental relationship in which an experienced individual supports a less experienced learner in advancing their professional and personal growth.1 Evidence suggests that mentor training can improve communication, clarify expectations, and enhance the overall quality of mentoring relationships.1 Mentoring may take multiple forms, including traditional one-to-one relationships, as well as peer and group mentoring models.2,3 Peer relationships, in particular, can contribute to career development by offering mutual support and shared learning experiences.3 A systematic review further highlights that effective mentoring programs often include structured frameworks, trained mentors, and institutional support.2
Studies in residency settings suggest that mentorship is associated with positive professional outcomes. Mentorship during residency has been linked to improved professional development among practicing physicians.4 In addition, formal mentorship interventions have demonstrated benefits in enhancing resident satisfaction, perceived support, and engagement within training programs.5 Survey-based studies among anesthesia residents in Canada and Saudi Arabia report that trainees value mentorship, although access to structured and consistent mentoring varies across programs.6,7 These findings highlight both the perceived importance of mentorship and the variability in its implementation.
Despite these benefits, several challenges persist. Mentorship programs differ considerably in their design and delivery, and there is no universally accepted model.2 Barriers such as limited time, insufficient mentor training, and lack of institutional support may affect the consistency and effectiveness of mentoring relationships.1,2 Additionally, variability in trainees’ experiences and expectations underscores the need for context-specific approaches.6,7
In Oman, no prior studies have explored mentorship experiences during residency training. This represents an important gap, as understanding residents’ perspectives is essential for developing effective and contextually appropriate mentorship programs. Therefore, this study aims to explore residents’ experiences and perceptions of mentorship during residency training in Oman and to examine potential variations across specialties.
We hypothesize that mentorship experiences and preferred mentoring approaches vary across and within specialty programs, reflecting differences in trainee needs and program structures. In addition, we anticipate limited availability of structured mentorship programs and resources across the training programs.
Study Objectives and Hypothesis
Primary Objective
To describe the residents’ experiences, perceptions, and perceived challenges regarding mentorship within their current residency programs in Oman.
Secondary Objective
To explore trainees’ needs and their perceptions of the role of mentorship in their training.
Study Hypothesis
We hypothesize that mentorship within the residency programs in Oman receives limited emphasis, with insufficient resources dedicated to its development and sustainability. We further anticipate that formal, structured mentorship programs are lacking in many residency programs.
Material and Methods
This cross-sectional, questionnaire-based study was conducted at the Oman Medical Specialty Board (OMSB), the national postgraduate training body responsible for residency programs across multiple medical specialties in Oman. OMSB oversees structured training programs leading to physician specialization in various fields (eg., pediatrics, internal medicine).
Study Population
The study targeted all residents enrolled in OMSB residency programs across all specialties and training levels during the study period. At the time of data collection, approximately 700 residents across 19 residency programs were eligible to participate.
Inclusion Criteria
All residents enrolled in OMSB residency programs during the study period.
Exclusion Criteria
No specific exclusion criteria were applied.
Questionnaire Development and Validation
The survey instrument was developed by adapting items from previously published studies assessing mentorship in residency training, particularly those by Ergun et al6 and Bin Ghali et al7 The questionnaire included domains related to mentorship experiences, availability, perceived effectiveness, and trainee needs. A five-point Likert scale was used where appropriate.
As no single validated instrument fully addressed the study objectives within this context, an adapted questionnaire was utilized (The complete questionnaire is available in Supplementary Appendix 1).
Content Validity
Four experts in medical education independently reviewed the questionnaire to assess relevance, clarity, and representativeness of the constructs. Modifications were made based on their feedback.
Face Validity and Pilot Testing
The questionnaire was pilot tested among 11 residents from four different residency programs to evaluate clarity, comprehension, and feasibility. This sample was selected to ensure representation across specialties rather than to meet a predefined proportion of the study population. All participants reported that the questionnaire was clear, understandable, and easy to complete, and no major issues were identified. Minor revisions were made accordingly.
Data Collection
An invitation to participate was distributed via official OMSB Email to all eligible residents. The Email included a link to the online survey hosted on SurveyMonkey. The first section of the questionnaire outlined the study aim and rationale, and completion of the survey implied informed consent.
All eligible residents (N ≈ 700) were invited to participate. Based on published literature on online survey response rates,8 a response rate of ≥44% was considered acceptable to support meaningful analysis.
The survey remained open for 6 weeks (December 2023 to February 2024). Reminder emails were sent at 2, 4, and 6 weeks following the initial invitation to improve response rates.
Data Management and Quality Control
All questionnaire items were set as mandatory to minimize missing data. Responses were exported from SurveyMonkey for analysis. Data were reviewed for completeness and consistency prior to analysis. No reverse-coded items or response-time monitoring were implemented.
Statistical Analysis
Data were analyzed using [SPSS version 31]. Descriptive statistics were used to summarize participant characteristics and survey responses (frequencies, percentages, means, and standard deviations as appropriate). Comparative analyses (eg., chi-square test) were conducted where applicable to examine differences across specialties and training levels. A p-value < 0.05 was considered statistically significant.
Ethical Considerations
Ethical approval was obtained from the OMSB Research Ethics Committee (REC/06/2023). Participation was voluntary, and no incentives were provided. The survey was anonymous, and no identifiable information was collected. All researchers declared no conflicts of interest.
Results
Participant Characteristics and Mentorship Access
At the time of the study, 718 residents were enrolled in OMSB residency programs. After exclusion of 16 incomplete responses, the final complete-case analytic sample included 450 residents, representing 62.7% of the eligible resident population. In the survey, a mentor was defined as someone with experience who offers guidance.
Participant demographics are summarized in Table 1. Most respondents were aged 26–30 years (303/450, 67.3%). Female residents represented 335/450 respondents (74.4%), while male residents represented 115/450 (25.6%). For analysis by training level, residency level was grouped as junior residents (R1–R2) and senior residents (R3–R5). Junior residents accounted for 234/450 respondents (52.0%), and senior residents accounted for 216/450 (48.0%). For specialty-based analysis, programs were clustered into medical, surgical, and diagnostic specialties. Medical specialties represented 259/450 respondents (57.6%), surgical specialties 140/450 (31.1%), and diagnostic specialties 51/450 (11.3%).
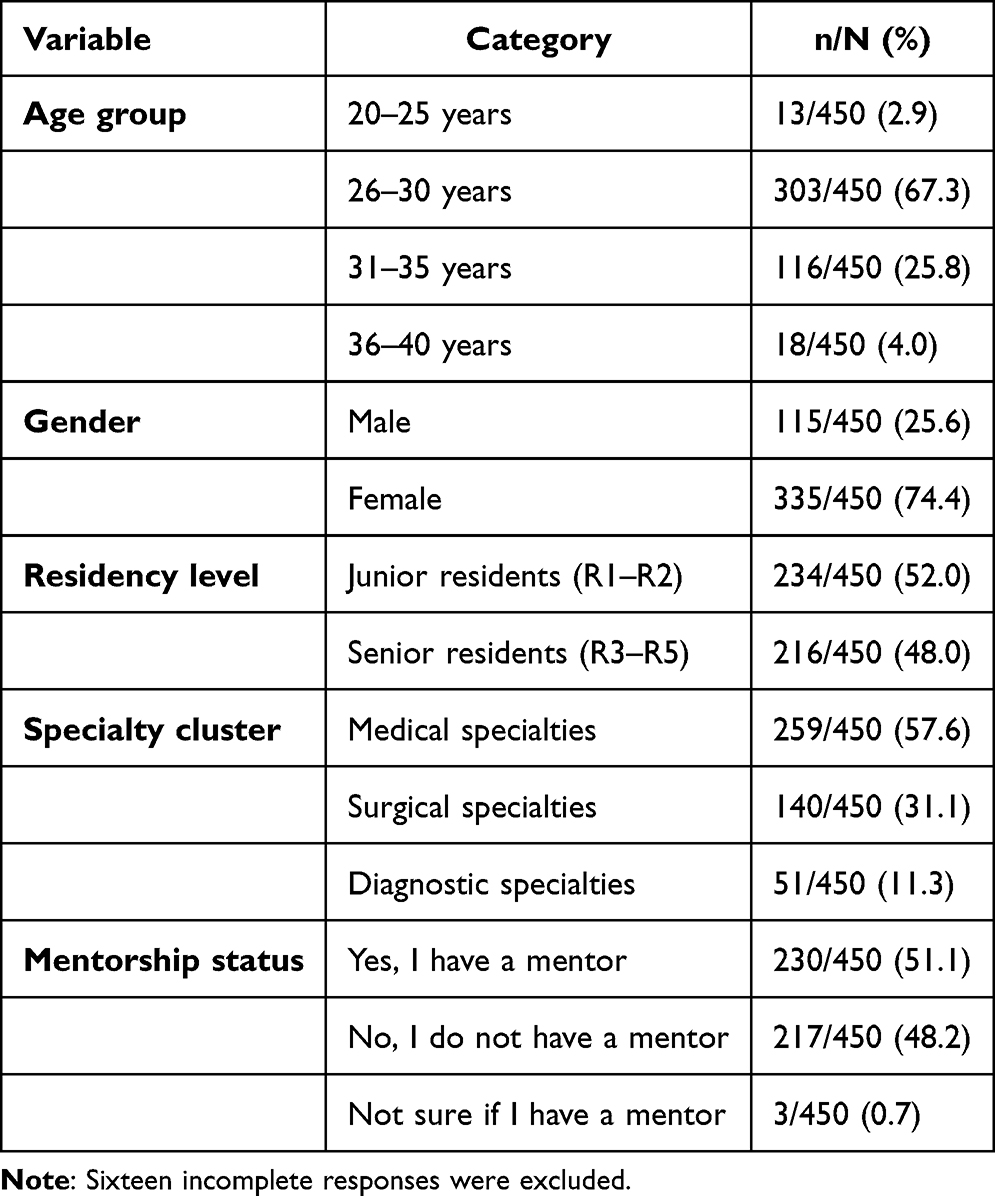 |
Table 1 Demographic Data and Mentorship Access |
Regarding mentorship status, 230/450 residents (51.1%) reported having a mentor, 217/450 (48.2%) reported not having a mentor, and 3/450 (0.7%) were unsure. Mentorship access did not differ significantly by residency level. Among junior residents, 117/234 (50.0%) reported having a mentor, compared with 113/216 senior residents (52.3%) (χ2=0.72, df=2, p=0.697). Among residents with mentors who completed the branch items, 138/206 (67.0%) reported having one mentor, 41/206 (19.9%) reported two mentors, 8/206 (3.9%) reported three mentors, and 19/206 (9.2%) reported more than three mentors. The number of mentors did not differ significantly by residency level (p=0.290). Mentor assignment was formal for (57.1%) residents, informal for (25.1%), and both formal and informal for (17.7%). Mentor-assignment method also did not differ significantly by residency level (p=0.939).
Mentorship Experiences Among Residents with Mentors
Among residents with mentors who answered the mentorship-experience items, (75.0%) agreed or strongly agreed that their mentor assisted them with academic goals. In addition, (62.7%) reported assistance with career opportunities, (43.1%) reported assistance with personal or family goals, and (22.1%) reported assistance with financial goals. Overall, among residents who rated the benefit gained from their mentorship relationship, (62.1%) rated the benefit as good or very good, (28.0%) as acceptable, and (10.0%) as poor or very poor.
Gender-based subgroup analysis showed statistically significant differences in two mentorship-experience outcomes. Male residents were more likely than female residents to report that mentors assisted them with financial goals (36.0% vs 17.5%; χ2=7.56, df=2, p=0.023). Male residents were also more likely than female residents to rate the overall benefit gained from mentorship as good or very good (74.0% vs 58.4%; χ2=8.55, df=2, p=0.014). No statistically significant gender differences were observed for mentor assistance with academic goals, career opportunities, or personal/family goals.
Residency-level analysis showed no significant differences between junior and senior residents in reported mentor assistance with academic goals, career opportunities, personal or family goals, or financial goals. However, the overall rating of mentorship benefit differed significantly by residency level (χ2=6.37, df=2, p=0.041). Junior residents were more likely than senior residents to rate mentorship benefit as good or very good (64.8% vs 59.4%), while senior residents were more likely to rate the benefit as poor or very poor (15.1% vs 4.8%).
Perceived Challenges and Barriers
Across the challenge items, the most frequently endorsed barriers were insufficient time available for mentorship (85.4%), lack of skilled mentors (81.2%), mentorship programs without formalized objectives (80.4%), lack of personal connection between mentor and mentee (78.9%), and mentorship programs without formalized meeting times (75.9%). Other reported barriers included lack of mentors with similar personal and professional goals (66.6%), lack of mentors from the same background or specialty (56.9%), and lack of mentors of the same gender (32.9%) (Table 2).
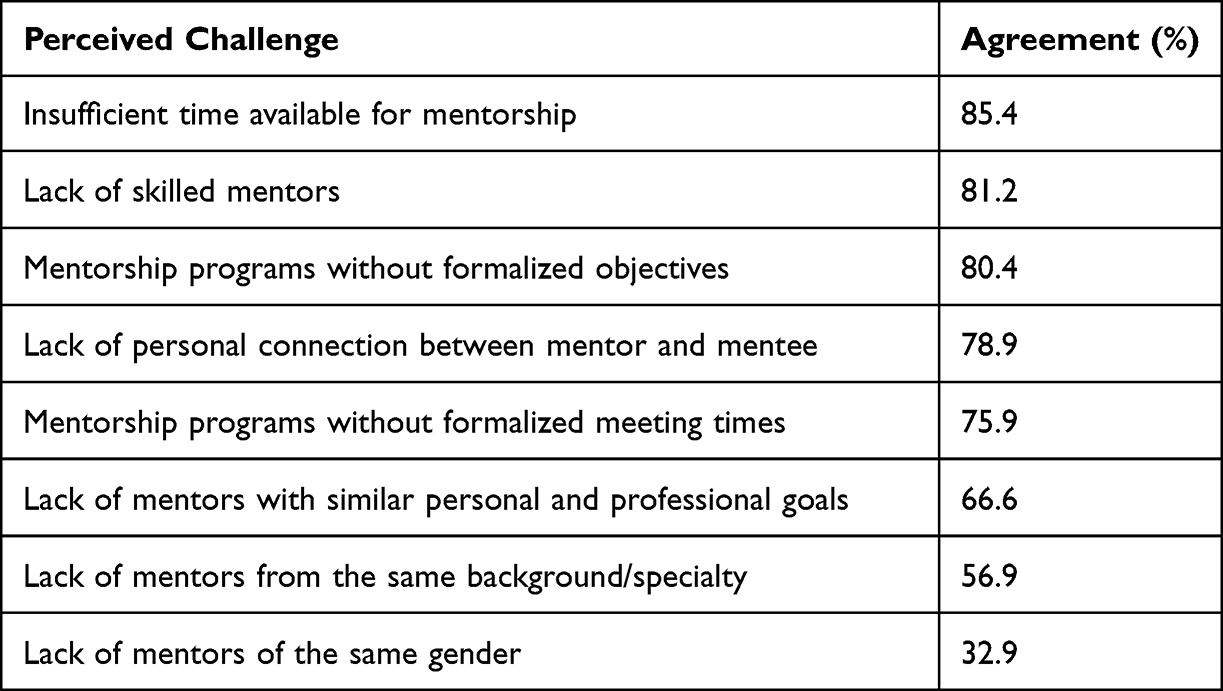 |
Table 2 Mentorship Challenges and Barriers |
Perceived barriers differed by residency level for selected items. Senior residents were more likely than junior residents to agree that lack of skilled mentors was a barrier to effective mentorship (86.2% vs 76.7%; χ2=7.36, df=2, p=0.025). Senior residents were also more likely to agree that mentorship programs lacked formalized objectives (85.6% vs 75.7%; χ2=8.48, df=2, p=0.014) and that lack of personal connection between mentor and mentee was a barrier (82.4% vs 75.7%; χ2=14.02, df=2, p=0.001).
In contrast, residency level was not significantly associated with perceived insufficient time for mentorship (p=0.872), lack of mentors of the same gender (p=0.636), lack of mentors from the same background or specialty (p=0.913), lack of formalized meeting times (p=0.380), or lack of mentors with similar personal and professional goals (p=0.099). No statistically significant differences by gender were observed for the perceived challenge items. Across specialty clusters, most perceived barriers did not differ significantly. The association between specialty cluster and agreement that mentorship programs lacked formalized objectives approached statistical significance but did not meet the predefined threshold (p=0.051).
Perceptions of Mentorship and Preferred Mentorship Models
Residents expressed strong overall agreement that mentorship is important during residency. Agreement or strong agreement was reported for increasing academic productivity by residents (90.6%), successful career advancement by (90.2%), increasing personal productivity by (88.9%), clinical skills development by (87.6%), fostering teaching skills by (86.9%), building confidence by (84.3%), and increasing the chance of research grant funding by (81.5%). In addition, (92.4%) residents agreed or strongly agreed that mentorship programs could improve overall success during residency (Table 3).
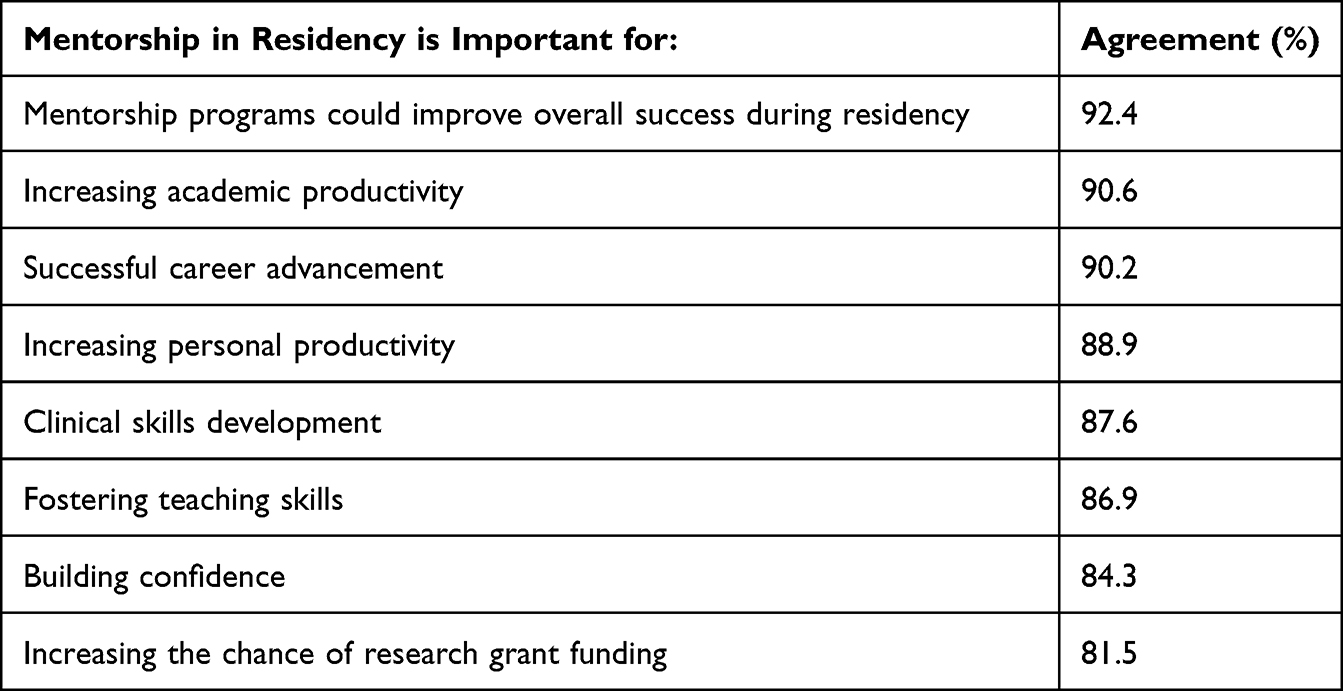 |
Table 3 Perceptions of Mentorship |
No significant residency-level differences were observed for perceived importance of mentorship in successful career advancement (p=0.081), academic productivity (p=0.387), research grant funding (p=0.729), personal productivity (p=0.274), clinical skills development (p=0.258), fostering teaching skills (p=0.137), building confidence (p=0.197), or overall belief that mentorship improves residency success (p=0.946).
However, preferred mentorship assignment strategy differed significantly by residency level (χ2=12.71, df=3, p=0.005). Junior residents more commonly preferred both formal and informal mentorship models (47.1%) compared with senior residents (36.6%). Senior residents more commonly preferred informal mentor selection (46.2%) compared with junior residents (30.0%). Preferences for formal assignment were similar among junior and senior residents (14.8% vs 13.4%, respectively).
Specialty cluster was significantly associated with the perception that mentorship is important for fostering teaching skills (χ2=9.70, df=4, p=0.046). Agreement was highest among diagnostic specialties (92.5%) and surgical specialties (92.2%), compared with medical specialties (82.8%). No statistically significant specialty-cluster differences were observed for other mentorship perception items, including career advancement, academic productivity, research grant funding, personal productivity, clinical skills development, confidence building, assignment strategy preference, gender preference, or belief that mentorship improves overall success.
Regarding preferred mentorship models overall, residents (42.2%) preferred both formal and informal mentorship, (37.6%) preferred informal mentor selection, (14.1%) preferred formal assignment by the program, and (6.1%) were unsure. Most residents were comfortable with a mentor of either gender (60.7%), while (32.5%) preferred a same-gender mentor, (5.1%) did not prefer a same-gender mentor, (1.8%) were unsure. Same-gender mentor preference did not differ significantly by residency level (p=0.873).
Discussion
This study provides the first multi-specialty assessment of mentorship experiences and perceptions among residents at the Oman Medical Specialty Board (OMSB). The findings demonstrate that mentorship is highly valued by residents and is perceived to contribute to academic productivity, career advancement, clinical skills development, teaching skills, confidence, and overall residency success. However, despite this positive perception, only about half of respondents reported having access to a mentor.
The findings are consistent with previous literature showing that mentorship is associated with professional development, academic productivity, career planning, and personal growth in medical education.2,4,9–12 Ramanan et al demonstrated the importance of mentorship during internal medicine residency and reported an association between mentoring and perceived career preparation, supporting the relevance of mentorship during postgraduate training.11 Similar observations have been reported among anesthesia residents in Canada and Saudi Arabia, where residents valued mentorship but reported variability in access, structure, and implementation.6,7 The present study adds to the existing literature by describing mentorship across multiple residency programs in Oman, a setting where mentorship experiences during specialty training have not previously been examined.
One important finding was that among residents with mentors, more than half reported that their mentor was formally assigned by the program. Formal assignment of a mentor does not necessarily indicate the presence of a fully structured mentorship program. A resident may have a named mentor without protected meeting time, clear objectives, mentor training, systematic follow-up, or evaluation of the mentorship relationship. The results suggest that mentorship may exist across training programs in variable forms, ranging from simple mentor allocation to more structured mentorship relationships. This emphasizes the need to distinguish between mentor assignment and effective mentorship.9,13,14
The preference for both formal and informal mentorship models further supports this interpretation. A substantial proportion of residents preferred a combined model, suggesting that residents value the accountability and equity provided by formal assignment while also recognizing the importance of personal compatibility, trust, and shared interests that often emerge through informal mentorship. Informal mentorship may allow residents to seek guidance from faculty members whose career paths, research interests, communication styles, or professional values align with their own needs. Previous literature has similarly emphasized that mentorship may extend beyond a single dyadic relationship and may include peer relationships, multiple mentors, or broader mentoring networks.3,15,16
The most frequently reported barriers were insufficient time for mentorship, lack of skilled mentors, absence of formalized objectives, lack of personal connection between mentor and mentee, and lack of formalized meeting times. These barriers suggest that the challenges are mainly structural and institutional rather than related to residents’ attitudes toward mentorship. Residents appear to recognize the value of mentorship, but effective implementation may be limited by clinical workload, competing service responsibilities, limited faculty availability, and lack of a shared framework for mentorship. These findings are consistent with previous studies identifying time constraints, unclear expectations, inadequate mentor preparation, and limited institutional structure as barriers to successful mentorship.1,2,7,9,13,14 The Omani postgraduate training context may add further complexity to these barriers. In hierarchical medical training environments, residents may perceive mentors as supervisors or evaluators rather than developmental guides, which may affect openness within the mentor-mentee relationship, particularly when discussing academic difficulties, career uncertainty, work-life balance, or personal challenges. The importance of interpersonal trust, accessibility, communication, and alignment of expectations has also been emphasized in qualitative literature on successful mentoring relationships.13,17,18
Residency level provided additional insight into residents’ mentorship needs. Using the grouping of junior residents as R1–R2 and senior residents as R3–R5, mentorship access did not differ significantly by training level. However, senior residents were more likely to identify lack of skilled mentors, lack of formalized objectives, and lack of personal connection as barriers. They were also more likely to prefer informal mentor selection, whereas junior residents more often preferred a combined formal and informal model. This pattern suggests that mentorship expectations evolve during residency. Junior residents may benefit from more structured guidance as they transition into specialty training, while senior residents may seek more individualized mentorship related to career planning, fellowship opportunities, leadership, research, and professional identity formation. These findings support a flexible mentorship approach that recognizes the changing needs of residents across training stages.
The gender-related findings are also important. Male residents were more likely than female residents to report mentor assistance with financial goals and to rate the overall benefit of mentorship more positively. These differences may reflect variation in access to informal networks, comfort discussing financial or career-related issues, mentor availability, or specialty distribution. At the same time, most residents reported comfort with a mentor of either gender, while about one-third preferred a same-gender mentor. This suggests that gender matching may be important for some residents but should not be the sole criterion for mentor assignment. Rather, mentor-mentee matching should consider expertise, accessibility, communication style, trust, and the resident’s stated preferences. These findings are consistent with literature suggesting that gender can influence mentorship experiences, while systematic reviews also indicate that mentorship programs for women in academic medicine are generally well received but should be designed carefully rather than assumed to automatically correct gender inequities.19–21
A strength of this study is the inclusion of residents from multiple specialties and training levels, which provides a broad overview of mentorship within OMSB. However, several limitations remain. The cross-sectional design limits causal interpretation, and the findings reflect residents’ self-reported perceptions rather than objective measures of academic performance, career progression, well-being, or mentorship quality. Nonresponse bias is possible, as residents with particularly positive or negative mentorship experiences may have been more likely to participate.
These findings have practical implications for postgraduate medical education in Oman. They suggest that mentorship should be approached as a structured educational process rather than simply the assignment of a mentor. At the same time, the preference for informal and combined mentorship models indicates that flexibility is important.
Conclusion
Mentorship was highly valued by OMSB residents and was perceived to support academic development, career advancement, confidence, and overall residency success. However, access to mentorship was inconsistent, with only about half of residents reporting having a mentor. The main barriers were structural, including limited time, lack of skilled mentors, absence of formalized objectives, and weak mentor–mentee connection. Differences by gender and training level suggest that mentorship needs vary across resident groups. These findings highlight the need for a structured yet flexible mentorship framework within OMSB that moves beyond mentor assignment alone and supports meaningful, accessible, and developmentally appropriate mentorship throughout residency training.
Acknowledgment
Dr Siham Al Senani, Dr Asma Al Balushi for their valuable time in reviewing the survey.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pfund C, Maidl Pribbenow C, Branchaw J, Miller Lauffer S, Handelsman J. The merits of training mentors. Science. 2006;311(5760):473–9. doi:10.1126/science.1123806
2. Kashiwagi DT, Varkey P, Cook DA. Mentoring programs for physicians in academic medicine: a systematic review. Acad Med. 2013;88(7):1029–1037. doi:10.1097/ACM.0b013e318294f368
3. Kram KE, Isabella LA. Mentoring alternatives: the role of peer relationships in career development. Acad Manage J. 1985;28(1):110–132. doi:10.2307/256064
4. Fernando SM, Cheung WJ, Choi SB, Thurgur L, Frank JR. Faculty mentorship during residency and professional development among practising emergency physicians. CJEM. 2018;20(6):944–951. doi:10.1017/cem.2018.42
5. Zhang H, Isaac A, Wright ED, Alrajhi Y, Seikaly H. Formal mentorship in a surgical residency training program: a prospective interventional study. J Otolaryngol Head Neck Surg. 2017;46(1):13. doi:10.1186/s40463-017-0186-2
6. Ergun S, Busse JW, Wong A. Mentorship in anesthesia: a survey of perspectives among Canadian anesthesia residents. Can J Anaesth. 2017;64(4):402–410. doi:10.1007/s12630-017-0816-1
7. Bin Ghali K, AlSubaie A, Nawab A. Mentorship in anesthesia: a perspective survey among anesthesia residents in Riyadh, Saudi Arabia. Saudi J Anaesth. 2021;15(2):144–148. doi:10.4103/sja.sja_1145_20
8. Wu MJ, Zhao K, Fils-Aime F. Response rates of online surveys in published research: a meta-analysis. Comput Human Behav Rep. 2022;7:100206. doi:10.1016/j.chbr.2022.100206
9. Joe MB, Cusano A, Leckie J, et al. Mentorship programs in residency: a scoping review. J Grad Med Educ. 2023;15(2):190–200. doi:10.4300/JGME-D-22-00415.1
10. Sambunjak D, Straus SE, Marusic A. Mentoring in academic medicine: a systematic review. JAMA. 2006;296(9):1103–1115. doi:10.1001/jama.296.9.1103
11. Ramanan RA, Taylor WC, Davis RB, Phillips RS. Mentoring matters. Mentoring and career preparation in internal medicine residency training. J Gen Intern Med. 2006;21(4):340–345. doi:10.1111/j.1525-1497.2006.00346.x
12. Ramanan RA, Phillips RS, Davis RB, Silen W, Reede JY. Mentoring in medicine: keys to satisfaction. Am J Med. 2002;112(4):336–341. doi:10.1016/S0002-9343(02)01032-X
13. Straus SE, Johnson MO, Marquez C, Feldman MD. Characteristics of successful and failed mentoring relationships: a qualitative study across two academic health centers. Acad Med. 2013;88(1):82–89. doi:10.1097/ACM.0b013e31827647a0
14. Sheri K, Too JYJ, Chuah SEL, Toh YP, Mason S, Radha Krishna LK. A scoping review of mentor training programs in medicine between 1990 and 2017. Med Educ Online. 2019;24(1):1555435. doi:10.1080/10872981.2018.1555435
15. Zerzan JT, Hess R, Schur E, Phillips RS, Rigotti N. Making the most of mentors: a guide for mentees. Acad Med. 2009;84(1):140–144. doi:10.1097/ACM.0b013e3181906e8f
16. DeCastro R, Sambuco D, Ubel PA, Stewart A, Jagsi R. Mentor networks in academic medicine: moving beyond a dyadic conception of mentoring for junior faculty researchers. Acad Med. 2013;88(4):488–496. doi:10.1097/ACM.0b013e318285d302
17. Cho CS, Ramanan RA, Feldman MD. Defining the ideal qualities of mentorship: a qualitative analysis of the characteristics of outstanding mentors. Am J Med. 2011;124(5):453–458. doi:10.1016/j.amjmed.2010.12.007
18. Niazi M, Mahboob U, Shaheen N, Gul S, Saeed MHB, Kiyani A. Exploring the factors affecting career progression in informal faculty mentoring sessions within mentor and mentee relationships: a qualitative study. BMC Med Educ. 2024;24(1):1242. doi:10.1186/s12909-024-06170-y
19. Lin G, Murase JE, Murrell DF, Godoy LDC, Grant-Kels JM. The impact of gender in mentor-mentee success: results from the Women’s Dermatologic Society Mentorship Survey. Int J Womens Dermatol. 2021;7(4):398–402. doi:10.1016/j.ijwd.2021.04.010
20. Farkas AH, Bonifacino E, Turner R, Tilstra SA, Corbelli JA. Mentorship of women in academic medicine: a systematic review. J Gen Intern Med. 2019;34(7):1322–1329. doi:10.1007/s11606-019-04955-2
21. House A, Dracup N, Burkinshaw P, Ward V, Bryant LD. Mentoring as an intervention to promote gender equality in academic medicine: a systematic review. BMJ Open. 2021;11(1):e040355. doi:10.1136/bmjopen-2020-040355
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.