Back to Journals » Advances in Medical Education and Practice » Volume 17
Mental Health First Aid Training as a Wellness Initiative for First Year Medical Students
Authors Thilges S ![]() , Goldhaber K, Shahid R
, Goldhaber K, Shahid R ![]()
Received 26 September 2025
Accepted for publication 16 January 2026
Published 24 March 2026 Volume 2026:17 565745
DOI https://doi.org/10.2147/AMEP.S565745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Sarah Thilges,1 Kate Goldhaber,1 Ramzan Shahid2
1Department of Psychiatry and Behavioral Neurosciences, Loyola University Medical Center, Maywood, IL, USA; 2Department of Pediatrics; Loyola University Medical Center, Maywood, IL, USA
Correspondence: Sarah Thilges, Department of Psychiatry and Behavioral Neurosciences, Loyola University Medical Center Maywood, IL, USA, Tel +1 708 327 2154, Email [email protected]
Purpose: The vital need to identify mental health concerns and appropriate supportive interventions has, rightfully so, been an area of concern within medical education. However, barriers such as mental health stigma and isolation within experiences may inaccurately amplify students’ concerns that if mental health needs are acknowledged, they will represent a threat to achieving personal and professional goals. In turn, this may decrease receptivity and impact of mental health interventions. This initiative sought to assess whether a standardized wellness training which addresses mental health stigma would be feasible and well-received by medical students.
Patients and Methods: Within our medical school, we have implemented Mental Health First Aid (MHFA) training to all incoming first-year medical students prior to the start of their academic training. This empirically based program is provided in the institution and utilizes peer support to recognize and intervene on mental health challenges while also educating on recovery-based models. Students completed MHFA training and exit surveys assessing perceptions of the training and benefits.
Results: Eighty-nine of 170 students completed the post-MHFA survey. About 81.6% indicated they would take another MHFA course while 96.6% found it “somewhat” or “very relevant.” Addressing the applicability of MHFA, 35.7% had a family member with a lived experience of mental illness and 22.6% indicated they identify as a person with a mental health experience. Overall, 71% felt this course better prepared for the work that they do professionally.
Conclusion: Although there are limitations including possibility of response bias of those who completed the survey, we posit that MHFA is a well-received intervention which provides tangible wellness tools within a context of reducing mental health stigma.
Plain Language Summary: Medical school is challenging and students deserve wellness interventions that will support their needs. However, fears about mental health stigma and losing out on career goals can impact willingness to get support. Mental Health First Aid is a well received intervention that can address these concerns.
Keywords: mental health stigma, medical student distress, peer support, medical school wellness curriculum
Introduction
Medical Student Distress
The high levels of distress among medical students have been well established within multiple mental and physiological domains of health. In an umbrella review,1 30.3% of medical students experienced psychological and behavioral symptoms; 35.8% reported burnout, while anxiety and depression were both endorsed within 32.5% of the respondents and 25.2% had substance use. Subsequently, medical students also have higher rates of suicidal ideation and suicide than matched peers in the general population with greater rates of completed suicide in males, although higher rates of suicidal ideation in females2 and those in later years of medical training.3 The consistently high rates of mental health concerns amongst medical students have been acknowledged within the literature and on many levels of medical training including in the entry to medical school.4
Response to Distress
The growing alarm to address mental health includes responses at individual institutions – more than 90% of Canadian and United States medical schools have wellness programs, and more than half have dedicated mental health providers5 as well as accrediting bodies. The Liaison Committee on Medical Education developed Standard 12 to require that an accredited program has in place an effective system of counseling services for its medical students that includes programs to promote their well-being and to facilitate their adjustment to the physical and emotional demands of medical education.6 However, despite the considerable attention to understanding the mental health needs of medical students and related interventions, overall prevalence rates of distress do not seem to be improving. Highlighting this is the change to pass/fail grading for the United States Medical Licensing Exam Step 1 in 2022 which aimed to reduce anxiety although distress remains high and there may be indications that anxiety towards Step 2 has increased because of this policy.7
Mental Health Stigma Amongst Medical Students
We posited that the disconnect between student distress and unmet mental health needs is due in large part to mental health stigma. Erving Goffman developed his seminal framework for stigma (1963)8 as it pertains to self-identity and the internalization of shame pertaining to characteristics which differentiate an individual from a majority group. Contact with an experience that is perceived to be undesirable may further heighten stigma as projected inward and escalate isolation from other identity groups. This relates to medical students given previous research which highlighted concerns for seeking mental health services as it pertains to peer perception and impact on future career.9,10 The stigmatization of mental health generally may be especially potent among medical students who are trained in models which pathologize and manage acute outcomes (ie. suicide attempt, active psychosis) and thus increase the likelihood students inhibit their own mental health outreach. This concern has been acknowledged by the American Medical Association which is lobbying for state licensing boards to reduce stigmatizing language about previous mental health treatment as this may inhibit medical providers from seeking necessary care.11 There have been a dearth of published intervention studies possibly reflective of the challenges at the institutional level to address the self-stigma medical students may have towards their own mental health symptoms.12 However, interventions to improve peer support which can directly confront the isolation of stigma have robust indications for bolstering wellness in the young adult population broadly13 and along with bolstering resiliency, in medical students specifically.14
Stigma and Mental Health First Aid
Thus, Mental Health First Aid (MHFA), which relies on educating individuals to recognize mental health symptoms in others while promoting a recovery-based model to inspire hope for treatment, was seen as a novel approach to address stigma and ultimately bridge the gap between mental health needs and engagement in wellness interventions. By empowering students to identify the early warning signs of distress in themselves and peers, MHFA could facilitate peer support to alleviate isolation and resistance to the alienation perceived in seeking mental health support.14 In addition, as the program instills awareness of recovery and the efficacy of interventions, students receive a message that “this is not forever” which may also address perceptions that mental health symptoms will impact their long-term career. Our program assessed the longitudinal relationship between MHFA and these domains, including mental health stigma, resiliency and burnout, which will be discussed in other disseminated work. Importantly, interventions are only as effective as the receptivity and engagement of those it seeks to help. After refining our application of MHFA, we have found students anecdotally and within the post-completion surveys generally perceive benefit to the course. Given the noted barriers of mental health stigma to engagement with psychological based initiatives, we believe MHFA could be easily adapted to other medical schools and is particularly appropriate for the Wellness programs within institutions.
Materials and Methods
Mental Health First Aid
Mental Health First Aid (MHFA; https://www.mentalhealthfirstaid.org/15 is an empirically based training disseminated by the National Council for Behavioral Health (NCBH) and modeled after physical first aid in its approach to teach participants to identify and respond to warning signs of mental health and substance use concerns (eg. irritability, poor hygiene, risk taking) while also teaching specific skills (eg. active listening) to increase their confidence and competence in providing support. Participants are also taught to recognize crises (eg. overdose, suicidality) and triage appropriately to higher levels of care. This learning occurs through a step wise but nonlinear intervention utilizing the acronym ALGEE.
A – Approach, assess for risk of suicide or harm
L – Listen nonjudgmentally
G – Give reassurance and information
E – Encourage Appropriate Help
E – Encourage self-help and other support strategies
The MHFA curriculum is manualized and can be completed entirely in-person, entirely virtually, or as a hybrid. Standardized slides, videos, and activities provided by NCBH are utilized to ensure program fidelity although references are made to adaptations available within different countries. For all formats, the total training time is approximately 8 hours. During in-person administration, participants gather in a group setting and take part in a combination of lectures, discussions, and learning activities. Slides and videos are projected, and a white board is utilized for group brainstorming and activities. This same structure can be delivered entirely virtually through MHFA’s zoom platform. In this format, the same slides and videos are shared, and the activities are conducted using the virtual whiteboard and breakout rooms. In the hybrid model, participants first watch the lectures individually online in advance of the training. They later assemble in person as a group to practice applying them in discussions and activities. In all formats, participants receive a manual that loosely follows the presentation and provides references for further reading. Instructors first complete MHFA training as a participant and then receive intensive training and feedback toward becoming instructors.
The original program was developed in Australia but has since been adapted to 23 countries and has multiple specific population versions (ie. emergency responders, teachers, etc). A growing list of studies have assessed various aspects of MHFA within medical training including in Australia16 and France17 A recent meta-analysis18 assessed 11 published studies of MHFA implementation for healthcare workers and students and found improvements in participants’ mental health literacy as well as willingness to provide MHFA while also decreasing stigma. They highlighted the need to maintain fidelity to the curriculum while making the application flexible to the needs of the targeted population.
Training at Our Institution
Stritch School of Medicine at Loyola Medical Center in Maywood, Illinois enrolls 170 students each academic year and launched MHFA training as a wellness initiative in 2018. Two licensed clinical psychologists who are both MHFA instructors certified by the NCBH and faculty at Stritch School of Medicine (SSOM) provided the MHFA training. All incoming M1 students, as a pre-matriculation requirement, complete MHFA training at our institution or provide confirmation of MHFA training done elsewhere to accommodate logistical constraints (ie. those students who may be arriving immediately before M1 Orientation). Initially this training was provided in an entirely in-person format as an 8-hour course teaching both the content and the application of MHFA skills during a full day session. However, with the transition to virtual learning due to COVID in 2020 and 2021; MHFA was offered fully virtually with students completing the self-guided learning individually and then gathering in small groups, also virtually, for the application of MHFA skills provided by the facilitators. In 2022, we began offering the hybrid option which includes the self-guided virtual portion and then the in-person group format. After experimenting with all three options at SSOM, we have decided to maintain the hybrid models as the self-guided learning followed by the collaborative group work represents the “flipped classroom” style that our students prefer.
Results
We present the post-evaluation survey created by the National Council for Mental Wellbeing to assess perceptions of MHFA completed by 89 of the 170 first-year medical students of the 2024–2025 academic year at our institution (Table 1). After completion of the in-person learning, students are asked to complete the survey online through the National Council and the results are then available to the course instructors with identity removed.
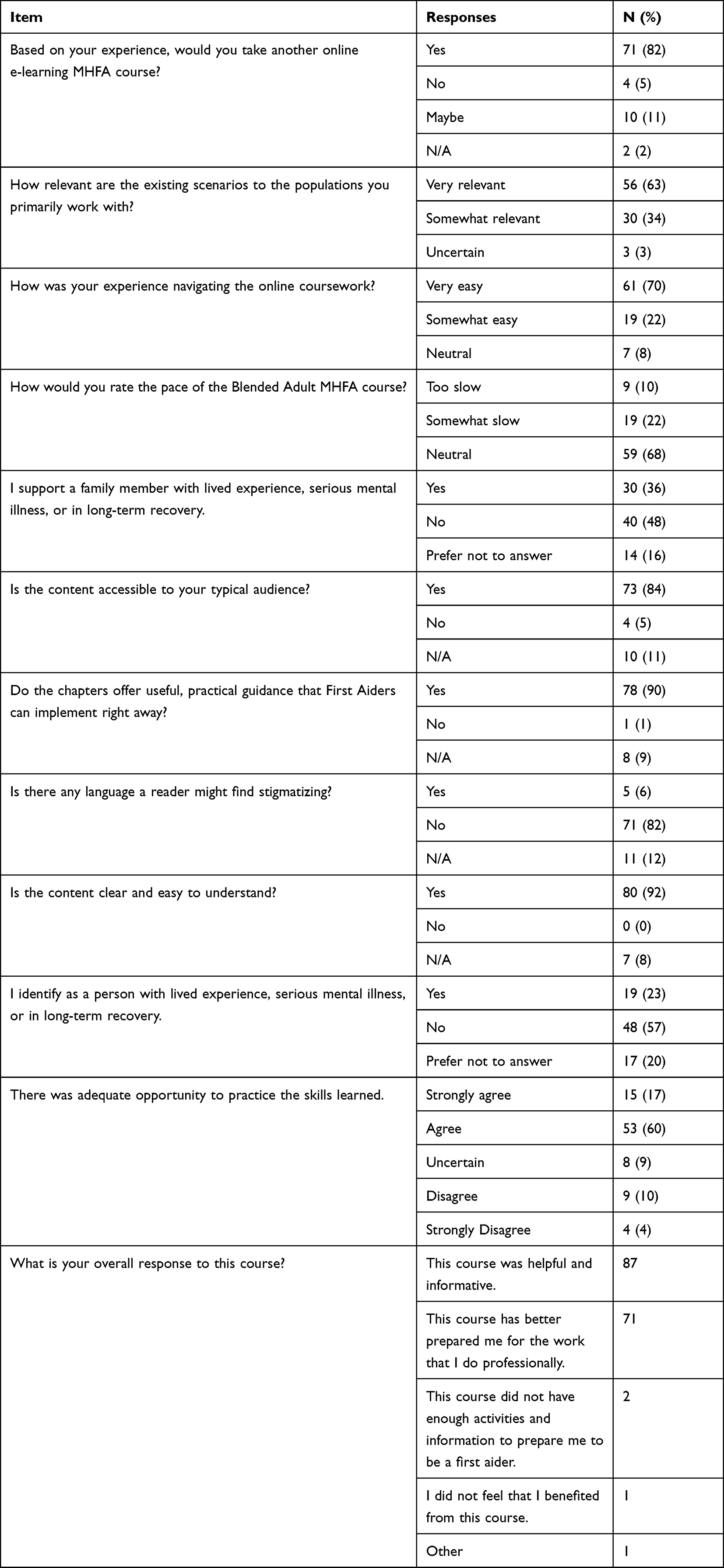 |
Table 1 Post Mental Health First Aid Survey |
Regarding satisfaction – 81.6% of respondents indicated they would take another MHFA course while 96.6% indicated they found it “somewhat” or “very relevant.” Related to the interaction with the program, 92% said it was “somewhat” to “very easy” to navigate the online coursework and 67.8% were “neutral” about the pace. Addressing the applicability of MHFA, 35.7% said they had a family member with a lived experience of mental illness and 22.6% indicated they identify as a person with a mental health experience. Overall, 81.6% indicated this course left them better prepared for the work that they do professionally.
Discussion
Although specific assessments of stigma were not obtained in this study, the findings indicate that a majority of first year medical students do find stigma reducing mental health curriculum to be beneficial. Stigma towards expressed mental health needs and willingness to engage in treatment has been shown to be a concern amongst medical students; thus tolerance of interventions directly targeting these needs may not be well received. However, within this sample, the majority of students who completed the post-MHFA survey endorsed the training as relevant to their experiences. Given that they reported both familial and personal experiences with mental health needs as well as feeling they were prepared professionally; MHFA may target wellness related to their individual and medical student identities and thus improve receptivity. Providing students tangible tools, such as the ALGEE intervention, appears to improve their readiness for the work of medical training potentially by providing an evidence based model of treatment and recovery.
We acknowledge that there is debate regarding mandating wellness activities and as our feedback shows satisfaction and learning occurred with the course, we do not feel that requiring this negatively impacted student engagement as have been noted by others.19 Instead, the mandated aspect may deter mental health stigma by equalizing all students and offering exposure to topics which may not be independently sought out, despite need, because of concerns for judgement from others. In addition, the peer support model of MHFA aligns with research indicating that medical students prompted to seek mental health care by peers are more likely to receive those services than those who do not receive such encouragement.20 As medical students may perceive their mental health needs are dismissed or exacerbated by a lack of support from their institution,21 it is also important to demonstrate investment in their wellness through an initiative such as MHFA. Relatedly, we believe it is important that the MHFA facilitators are faculty members who interact with medical students in the learning and clinical setting; thus, establishing credibility for shared experiences and personal knowledge of the stressors the medical students may experience. This matches other findings which indicate that skepticism can be a barrier when interventions are too broad and not considered relevant to the specific demands medical students face.22
Limitations include the potential for sampling bias as 89 out of 170 students (52%) completed the post-training survey and it is plausible that students who did so were more likely to find it beneficial. It is also important to note that this MHFA training occurs during the pre-matriculation period in which students have certainly faced stressors in the medical school admission process as well as concurrent life events but have not yet been exposed to medical school demands. Thus, we are uncertain how robust the training is as students progress through their education. We have discussed as an institution whether the training in its entirety should be repeated later in medical training or if “Best Practice” reinforcements should be virtually disseminated throughout the M1 year. As of yet, we have not implemented any additional MHFA training.
Conclusion
We do feel the implementation of this training is novel as an intervention for an entire cohort of students yet generalizable to other medical schools as the framework of identifying a concern, responding with an intervention and facilitating additional care is consistent with the medical model familiar to students. We are not aware of any other published manuscripts outlining implementation of MHFA as a proactive and mandated mental health intervention in medical education. In addition, the peer support component conveys a network of support rather than relying solely on individual reporting which can be dampened by mental health stigma. By instilling the recovery based model, MHFA also depicts the survivorship of mental health challenges which may further reduce the catastrophic fears students have for career ending reporting of symptoms. Taken together, this training offers medical schools a unique opportunity to destigmatize and advance the wellness interventions for students.
Ethics Approval and Informed Consent
This research study was reviewed by Loyola University IRB and deemed to be exempt. The IRB determined informed consent was sufficient to cover publication of anonymized results which were maintained with confidentiality as data was aggregated and identifying information removed.
Per the Loyola University Medical Center Institutional Review Board the project met the criteria for Exemption category 45 CFR 46.104(d)(2)(i-ii). Research only includes interactions involving educational tests, surveys, interviews, public observation if the following criteria is met: (i) Recorded information cannot readily identify the subject (directly or indirectly/linked); and (ii) any disclosure of responses outside of the research would not reasonably place subject at risk (criminal, civil liability, financial, employability, educational advancement, reputation).
Informed consent was not required for this research project as per federal regulations, it was “exempt” as it did not involve more than minimal risk and the secondary data analysis did not require a formal consent process (U.S. Department of Health and Human Services (HHS) regulations, specifically 45 CFR 46.101(b)).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jahrami H, AlKaabi J, Trabelsi K, et al. The worldwide prevalence of self-reported psychological and behavioral symptoms in medical students: an umbrella review and meta-analysis of meta-analyses. J Psychosom Res. 2023;173:111479. doi:10.1016/j.jpsychores.2023.111479
2. Mateen A, Kumar V, Singh AK, Yadav B, Mahto M, Mahato S. Suicide and suicidal ideation in medical students: a systematic review. Cureus. 2024;16(7):e65246. doi:10.7759/cureus.65246
3. Varshney K, Patel H, Panhwar MA. Risks and warning signs for medical student suicide mortality: a systematic review. Arch Suicide Res. 2024;28(4):1058–7. doi:10.1080/13811118.2024.2310553
4. Nair M, Moss N, Bashir A, et al. Mental health trends among medical students. Proc. 2023;36(3):408–410. doi:10.1080/08998280.2023.2187207
5. Schutt A, Chretien KC, Woodruff JN, Press VG, Vela M, Lee WW. National survey of wellness programs in u.s. and canadian medical schools. Acad Med. 2021;96(5):728–735. doi:10.1097/ACM.0000000000003953
6. Liaison Committee on Medical Education. (2025). Functions and structure of a medical school: standards for accreditation of medical education programs leading to the md degree. [Effective 2026-27]. Available from: https://lcme.org/publications/.
7. Rothka AJ, Nguyen M, King TS, Choi KY. Impact of USMLE pass/fail step 1 scoring on current medical students. J Med Educ Curric Dev. 2024;11:23821205241281650. doi:10.1177/23821205241281650
8. Goffman E. Stigma: Notes on the Management of Spoiled Identity. Simon and Schuster; 2009.
9. Berliant M, Rahman N, Mattice C, Bhatt C, Haykal KA. Barriers faced by medical students in seeking mental healthcare: a scoping review. MedEdPublish. 2022;12:70. doi:10.12688/mep.19115.1
10. Wilkinson E. Medical students face high levels of mental health problems but stigma stops them getting help. BMJ. 2023;381:933. doi:10.1136/bmj.p93
11. AMA. ARC Issue Brief: campaign to support medical student, resident and physician health and wellbeing. Available from: https://www.ama-assn.org/system/files/issue-brief-physician-health-wellnesspdf2024.
12. Bannatyne AJ, Jones C, Craig BM, Jones D, Forrest K. A systematic review of mental health interventions to reduce self-stigma in medical students and doctors. Front Med. 2023;10:1204274. doi:10.3389/fmed.2023.1204274
13. Richard J, Rebinsky R, Suresh R, et al. Scoping review to evaluate the effects of peer support on the mental health of young adults. BMJ Open. 2022;12(8):e061336. doi:10.1136/bmjopen-2022-061336
14. Klein HJ, McCarthy SM. Student wellness trends and interventions in medical education: a narrative review. Humanit Soc Sci Commun. 2022;9(1):92. doi:10.1057/s41599-022-01105-8
15. Mental Health First Aid. National Council for Mental Wellbeing. Available from: https://mentalhealthfirstaid.org.
16. Pham L, Moles RJ, O’Reilly CL, Carrillo MJ, El-Den S. Mental Health First Aid training and assessment in Australian medical, nursing and pharmacy curricula: a national perspective using content analysis. BMC Med Educ. 2022;22(1):70. doi:10.1186/s12909-022-03131-1
17. Sibeoni J, Ellul P, Bubola T, Debiche Y, Piot MA. Mental health first aid training among healthcare French students: a qualitative study. Front Med Lausanne. 2023;10:1268277. doi:10.3389/fmed.2023.1268277
18. Li L, Ma X, Wu Z, Xie C, Li Y. Mental health first aid training and assessment for healthcare professionals and medical nursing students: a systematic review [published correction appears in BMC. Psychol. 2025;13(1):396. doi:10.1186/s40359-025-02697-x.]
19. Waechter R, Stahl G, Rabie S, et al. Mitigating medical student stress and anxiety: should schools mandate participation in wellness intervention programs? Med Teach. 2021;43(8):945–955. doi:10.1080/0142159X.2021.1902966
20. Phillips M, Danielle L, Steelesmith G, Benedict J, Muñoz J, Fontanella C. Mental health service utilization among medical students with a perceived need for care. Acad Psychiatry. 2022;46(2):223–227. doi:10.1007/s40596-021-01584-y
21. Christy R. Medical students’ attitudes towards mental health disclosure: a qualitative study. J Public Mental Health. 2021;20(1):51–59. doi:10.1108/JPMH-05-2020-0051
22. Chatterjee K, Edmonds VS, Girardo ME, Vickers KS, Hathaway JC, Stonnington CM. Medical students describe their wellness and how to preserve it. BMC Med Educ. 2022;22(1):510. doi:10.1186/s12909-022-03552-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.