Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Mendelian Randomization Study in East Asian Populations Supports the Causal Relationship Between Blood Metabolites and COPD: Insights from Amino Acids, Phospholipids, Vitamin D, and Trace Elements
Authors Guo S, Li Z, Wei M, Hu L, Jiang S, Yang F, Yang Z, Zhu X, Shen X
Received 11 December 2025
Accepted for publication 3 April 2026
Published 16 April 2026 Volume 2026:21 588120
DOI https://doi.org/10.2147/COPD.S588120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Shixiang Guo,1,* Zheng Li,1,* Mingfeng Wei,1,* Lefei Hu,1 Shuai Jiang,1 Fuzhi Yang,1 Zhengyao Yang,2 Xunxia Zhu,1 Xiaoyong Shen1
1Department of Thoracic Surgery, Affiliated Huadong Hospital, Fudan University, Shanghai, People’s Republic of China; 2Department of General Surgery, Affiliated Huadong Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoyong Shen, Department of Thoracic Surgery, Affiliated Huadong Hospital, Fudan University, 221# West Yanan Road, Shanghai, 200040, People’s Republic of China, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is the most common respiratory disease among middle-aged and older adults worldwide, and its etiology remains incompletely understood. As intermediate products of biochemical reactions, blood metabolites have a debated role in the pathogenesis of COPD, with observational studies yielding conflicting results. Most existing genetic studies are based on European cohorts, whereas East Asian populations differ substantially in genetic architecture and environmental exposures, limiting the generalizability of current findings.
Methods: We performed two-sample Mendelian randomization (MR) leveraging the most recently released summary statistics from large-scale genome-wide association studies (GWAS) in East Asian populations. Independent SNPs significantly associated with circulating metabolite levels were selected from multiple East Asian datasets as instrumental variables (3432 Chinese participants, 2022). Outcome data were obtained from two independent East Asian COPD GWAS cohorts: ebi-a-GCST90018587 (4017 cases, 162,653 controls, BioBank Japan, 2021) and bbj-a-103 (3315 cases, 201,592 controls, BioBank Japan, 2019). Inverse-variance weighting (IVW) served as the primary estimator, with sensitivity analyses conducted using MR-Egger regression, the weighted median, and additional complementary approaches.
Results: Seven blood metabolites showed suggestive causal links with COPD. In the ebi-a-GCST90018587 cohort, genetically predicted platelet count was positively associated with COPD risk (OR = 1.51, 95% CI 1.01– 2.27, P = 0.0467), and in the bbj-a-103 cohort higher genetically predicted manganese levels likewise indicated increased risk (OR = 1.27, 95% CI 1.00– 1.62, P = 0.0460). Conversely, higher genetically predicted levels of leucine (OR = 0.56, 95% CI 0.34– 0.91, P = 0.0197), alpha-aminoadipic acid (OR = 0.75, 95% CI 0.59– 0.96, P = 0.0208), serum-alanine-transaminase (ALT)(OR = 0.87, 95% CI 0.76– 0.99, P = 0.0345), phosphoethanolamine (OR=0.75, 95% CI 0.56– 1.00, P = 0.0500), and 25-hydroxyvitamin-D2 (OR = 0.81, 95% CI 0.70– 0.94, P = 0.0045) were associated with lower COPD risk, with phosphoethanolamine and 25-hydroxyvitamin-D2 showing concordant directions and comparable effect sizes across the two independent COPD GWAS cohorts. For all exposures, Cochran’s Q tests and MR-Egger intercepts indicated no significant heterogeneity (P > 0.05), and Steiger directionality tests (P< 0.05) did not suggest reverse causation.
Conclusion: Leveraging large East Asian cohorts, this study provides MR evidence implicating amino-acid metabolism, phospholipid metabolism, vitamin D status, and selected trace elements in COPD pathophysiology. The replicated protective signals for phosphoethanolamine and 25(OH)D2, and the risk signals for platelet count and manganese, offer East Asian–specific genetic support for metabolically oriented prevention and precision interventions.
Keywords: mendelian randomization, blood metabolites, East Asian population, chronic obstructive pulmonary disease
Introduction
Chronic obstructive pulmonary disease (COPD) is a common chronic respiratory disease characterized by persistent airflow limitation and chronic airway inflammation; it is the third leading cause of death worldwide1,2 and imposes a heavy burden on public health and the socioeconomic system. Recent epidemiological studies indicate that, with population aging and shifts in environmental exposure profiles, the disease burden of COPD will continue to rise in East Asia and other low- and middle-income regions.3,4 The established modifiable risk factors primarily include cigarette smoking and occupational/environmental particulate matter exposures; however, marked inter-individual differences in disease risk at comparable smoking exposure levels suggest that endogenous metabolic status and host susceptibility also play critical roles in COPD development and progression.
Metabolic reprogramming is considered one of the key underpinnings of the systemic manifestations of COPD. Multiple metabolomics studies of serum/plasma and lung tissue have revealed widespread abnormalities in fatty acids, sphingolipids, acylcarnitines, and various amino acids and xenometabolites in patients with COPD;5 these metabolic signatures are closely linked to reductions in lung function, airway inflammation, and the risk of acute exacerbations.6,7 In addition, vitamin D deficiency shows an inverse association with COPD occurrence, disease severity, and acute exacerbations,8 while the relationships between COPD and traditional metabolic indices such as blood lipids and uric acid have also attracted considerable attention.9–11 However, these observational studies are unavoidably affected by confounding and reverse causation, making it difficult to determine the causal roles of metabolites in COPD.
In recent years, Mendelian randomization (MR) based on genome-wide association studies (GWAS) has emerged as a powerful tool for probing causal relationships between modifiable exposures and complex diseases. By leveraging genetic variants strongly associated with the exposure as instrumental variables, MR can, under appropriate assumptions, effectively mitigate residual confounding and reverse causation. Existing studies have used MR to evaluate causal links between blood lipids, immune traits, the gut microbiota and its metabolites, and COPD, suggesting that certain metabolic pathways may play key roles in COPD pathogenesis and progression.12 However, most current MR studies are based on European populations; MR analyses of metabolite–COPD causality in East Asians remain limited.13–15 East Asian populations differ substantially from European populations in genetic architecture, lifestyle, and environmental exposures,16–18 which may yield population-specific patterns in metabolomic profiles and susceptibility to COPD. Although there have been MR studies in the European population exploring the association between some metabolites and COPD, the results have been inconsistent – for instance, certain metabolites showed protective effects in one study, but had no significant association or even an opposite direction in other studies.13,19 These inconsistencies suggest that the impact of metabolites on COPD may have population heterogeneity, and confirmatory studies in different ancestral populations are urgently needed. Based on the existing metabolomics evidence and biological rationality, we hypothesize that specific types of metabolites (such as amino acids, phospholipids, and trace elements) have a causal effect on the risk of COPD. Some of these metabolites may exert protective effects (such asalpha-aminoadipic acid, leucine), while others may increase the risk (such as manganese, platelet-related traits).
To test the above hypothesis, we leveraged summary statistics from GWAS of blood metabolites and related biochemical traits in Chinese populations as exposures and, together with two independent large East Asian COPD GWAS cohorts, applied two-sample Mendelian randomization to systematically assess the putative causal relationships between circulating metabolites—including trace elements—and COPD risk, aiming to delineate COPD-relevant metabolic pathways from a metabolomics perspective and to provide East Asia–specific genetic evidence for identifying modifiable targets and constructing metabolically based risk-stratification strategies.
Material and Methods
Principles of Mendelian Randomization Design
We used single nucleotide polymorphisms (SNPs) as genetic instruments and performed two-sample Mendelian randomization to evaluate the causal relationship between blood metabolite levels and COPD. The overall study framework is depicted in Figure 1. Assumption 1 (association): the genetic instruments are robustly associated with the exposure. Assumption 2 (independence): the genetic instruments must be independent of confounders, ensuring that the observed association is not influenced by factors such as lifestyle or genetic background. Assumption 3 (exclusivity hypothesis): the genetic instruments affect the outcome only through the exposure and are not independently associated with the outcome. In this study, blood metabolites were considered the exposures and COPD the outcome.
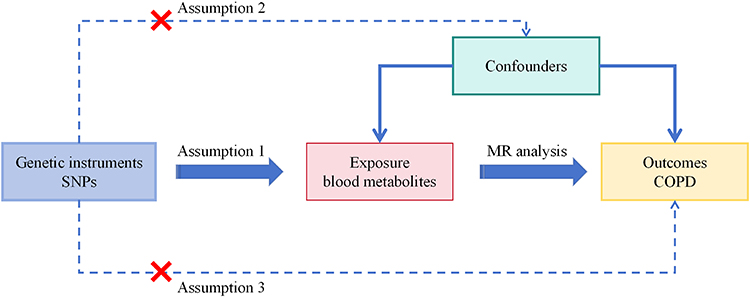 |
Figure 1 Mendelian Randomization Framework. Abbreviations: MR, Mendelian Randomization; SNP, Single Nucleotide Polymorphism. Notes: Assumption 1 (association): the genetic instruments are robustly associated with the exposure. Assumption 2 (independence): the genetic instruments must be independent of confounders, ensuring that the observed association is not influenced by factors such as lifestyle or genetic background. Assumption 3 (exclusivity hypothesis): the genetic instruments affect the outcome only through the exposure and are not independently associated with the outcome. |
Data Sources
Blood metabolite data were obtained from a published GWAS-related study20 encompassing 3432 Chinese individuals and integrating whole-genome, metagenomic, anthropometric, and blood-metabolite profiles. Outcome data came from two independent East Asian GWASs; for ebi-a-GCST90018587, the GWAS combined 4017 COPD cases and 162,653 controls, with all participants of East Asian ancestry. Bbj-a-103 (Biobank Japan): this GWAS, from the Biobank Japan project, included 3315 cases and 201,592 non-case participants. We ensured that there was no sample overlap among the GWAS datasets corresponding to exposures, outcomes, and mediators. Because all analyses used publicly available summary data, the original studies providing these datasets had obtained ethical approval. This study was conducted in accordance with the Declaration of Helsinki and its subsequent amendments.
IVs Selection
Prior to the data analyses, we prespecified several criteria to optimize the selection of instrumental variables (IVs): (I) Potential IVs were selected as SNPs significantly associated with blood metabolite levels at a threshold of P <5×10−6,(Findings based on this threshold are interpreted as suggestive causal evidence and should be validated in larger samples or experimental studies);(II) SNPs were excluded using an LD criterion of R2<0.001 with a clumping distance of 10,000 kb to account for linkage disequilibrium (LD); (III) SNPs with allele mismatches or anomalous frequencies (minor allele frequency, MAF≤0.01) were excluded; (IV) Instruments with an F-statistic <10 were removed to reduce potential weak-instrument bias.
Statistical Analysis
In our study, inverse-variance weighting (IVW) served as the primary method to estimate the causal effects of circulating metabolites on COPD. This approach aggregates the effects of all instrument SNPs to yield a combined estimate. To further probe instrument robustness and validity, we implemented complementary MR estimators, including MR-Egger, the weighted median, and the weighted mode. To address potential reverse causation, we applied the Steiger directionality test. To assess horizontal pleiotropy, we used MR-Egger regression (intercept test) to evaluate the influence of directional pleiotropy on the overall estimates. Cochran’s Q was used to evaluate heterogeneity across instrumental variables in the MR analyses. When the Cochran’s Q P-value exceeded 0.05, indicating no significant heterogeneity, we adopted the fixed-effects IVW estimator as the primary analysis. Conversely, upon detecting significant heterogeneity (P<0.05), we employed random-effects IVW to accommodate between-instrument variability. All statistical analyses were performed using the R version 4.4.2 and the R package TwoSampleMR (version 0.6.14).
Results
IVs
Using genome-wide association data from East Asian populations, we successfully identified genetic instruments that are significantly associated with COPD. Applying stringent quality-control criteria (P < 1×10−5; LD r2 < 0.001 within a 10,000-kb window), we obtained 1099 and 854 independent single-nucleotide polymorphisms (SNPs) from the ebi-a-GCST90018587 and bbj-a-103 datasets, respectively, as valid instrumental variables. These instruments satisfied the minimum strength requirements for Mendelian randomization analyses.
Main Mendelian Randomization Analysis Results
Using inverse-variance weighting (IVW) as the core analytical strategy, we identified six causal signals associated with COPD risk in the ebi cohort with IVW as the primary estimator (Figure 2A and Table 1). Notably, higher genetically predicted platelet count was associated with increased COPD risk (OR = 1.51, 95% CI 1.01–2.27, P = 0.0467). By contrast, several exposures showed protective directions: phosphoethanolamine displayed borderline significance for reduced risk (OR = 0.75, 95% CI 0.56–1.00, P = 0.0500); serum-alanine-transaminase (ALT) was associated with lower risk (OR = 0.87, 95% CI 0.76–0.99, P = 0.0345); alpha-aminoadipic acid was linked to lower risk (OR = 0.75, 95% CI 0.59–0.96, P = 0.0208); leucine showed a stronger protective effect (OR = 0.56, 95% CI 0.34–0.91, P = 0.0197); and 25-hydroxyvitamin D2 [25(OH)D2] was likewise associated with reduced risk (OR = 0.81, 95% CI 0.70–0.94, P = 0.0045). Overall, the cohort suggests that platelet count may represent a genetically determined risk factor for COPD, whereas amino acid–related metabolites, intermediates of phospholipid metabolism, and 25(OH)D2 are associated with lower risk.
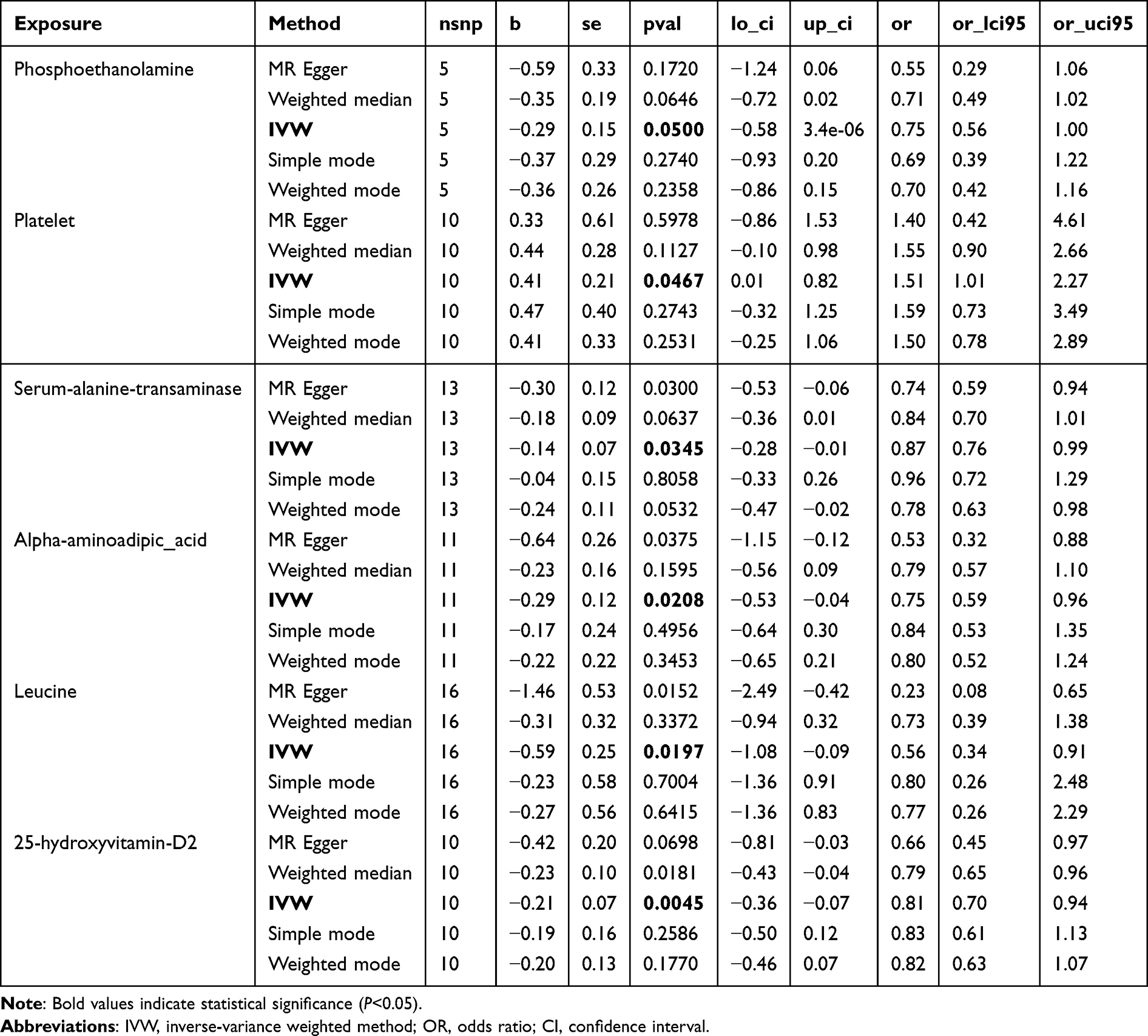 |
Table 1 Mendelian Randomization Analysis Results of Blood Metabolites and COPD, Using the Query Code “Ebi-a-GCST90018587” |
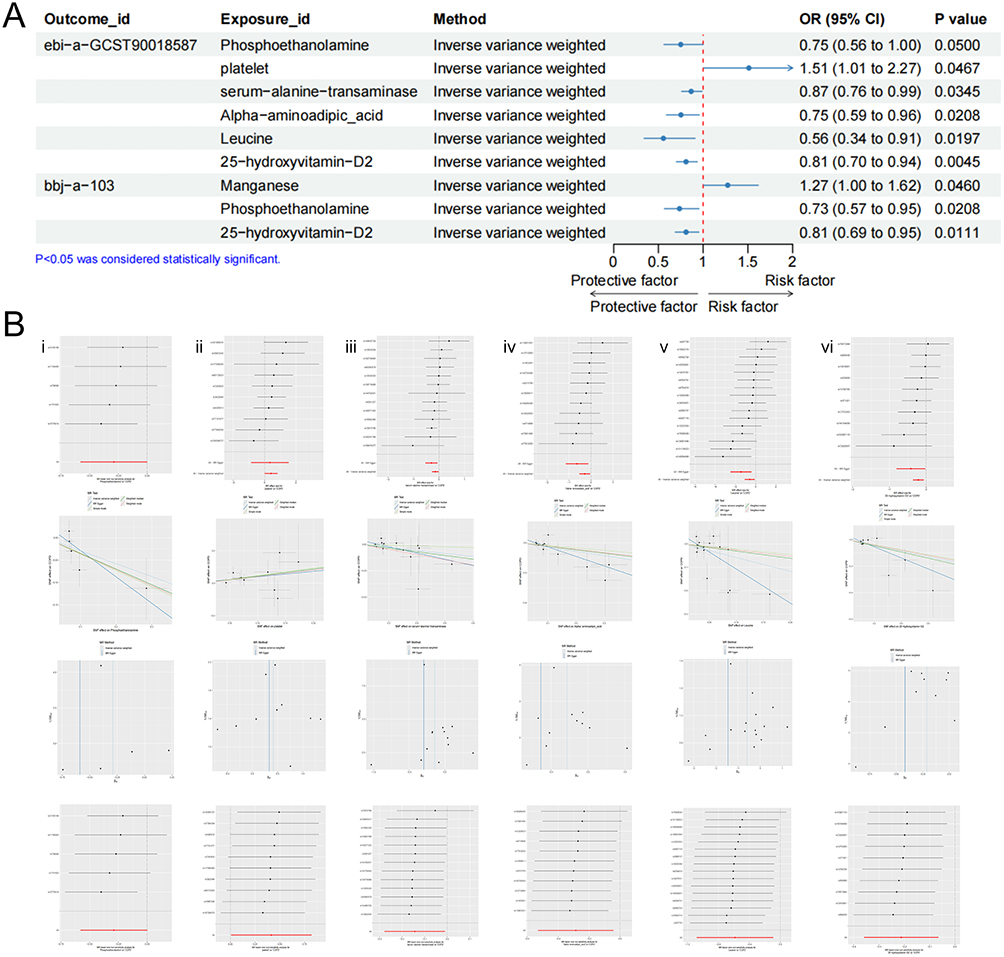 |
Figure 2 Continued. |
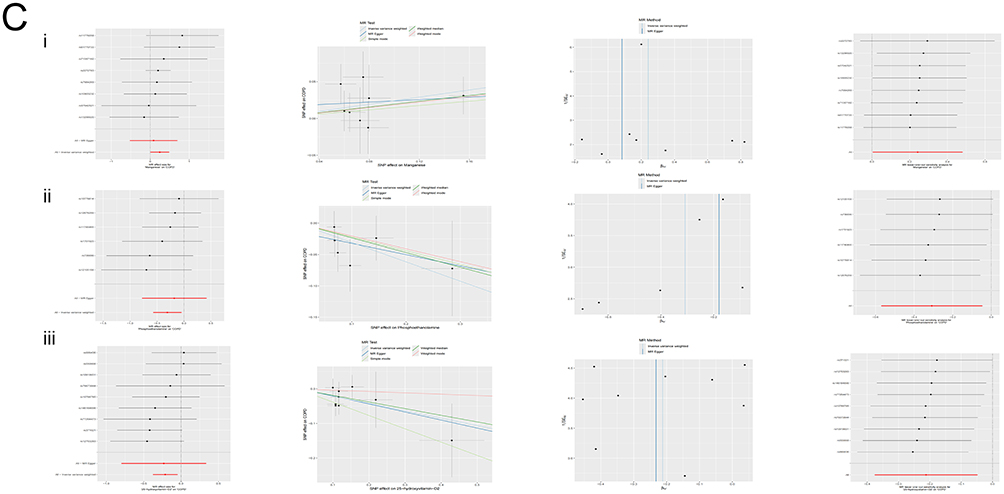 |
Figure 2 (A) Forest plot of the relationship between blood metabolites and COPD based on Mendelian analysis. The red dashed vertical line indicates the null value (OR = 1). Points to the left of this line suggest a protective effect (OR < 1), while points to the right suggest a harmful effect (OR > 1). (B) Mendelian analysis between blood metabolites and the ebi-a-GCST90018587 dataset. i: Phosphoethanolamine ii: Platelet iii: Serum-alanine-transaminase iv: Alpha-aminoadipic acid v: Leucine vi: 25-hydroxyvitamin D2. From top to bottom: forest plot, scatter plot, funnel plot, leave-one-out plot. (C) Mendelian analysis between blood metabolites and the bbj-a-103 dataset. i: Manganese ii: Phosphoethanolamine iii: 25-hydroxyvitamin D2. From left to right: corresponding forest plot, scatter plot, funnel plot, leave-one-out plot. Notes: Corresponding forest plot: Black horizontal solid lines represent the causal effect estimates of individual SNPs and their 95% confidence intervals; the red horizontal solid line represents the pooled causal effect estimate of all SNPs combined (using the IVW method) and its 95% confidence interval. The vertical dashed line indicates the null effect line (β = 0). A line segment entirely to the left of the dashed line suggests a negative (protective) effect of the SNP, while a segment to the right suggests a positive (risk) effect. Leave-one-out plot: Each black horizontal solid line in the figure represents the pooled causal effect estimate of the remaining SNPs after sequentially excluding the corresponding SNP, along with its 95% confidence interval; the red horizontal solid line represents the overall causal effect estimate of all SNPs (using the IVW method) without excluding any SNP; the vertical dashed line indicates the null effect line (β = 0). If the estimate changes minimally after excluding a particular SNP (remaining around the red line), it indicates that the results are robust. |
In the bbj cohort, inverse-variance–weighted (IVW) analysis again identified three exposures associated with COPD risk (see Figure 2C and Table 2). Elevated manganese levels were associated with increased risk (OR = 1.27, 95% CI 1.00–1.62, P = 0.0460). By contrast, phosphoethanolamine (OR = 0.73, 95% CI 0.57–0.95, P = 0.0208) and 25(OH)D2 (OR = 0.81, 95% CI 0.69–0.95, P = 0.0111) again exhibited protective effects in this cohort. Notably, the effects of phosphoethanolamine and 25(OH)D2 were directionally concordant and of similar magnitude across two independent East Asian cohorts, demonstrating good cross-cohort reproducibility (Figure 2A).
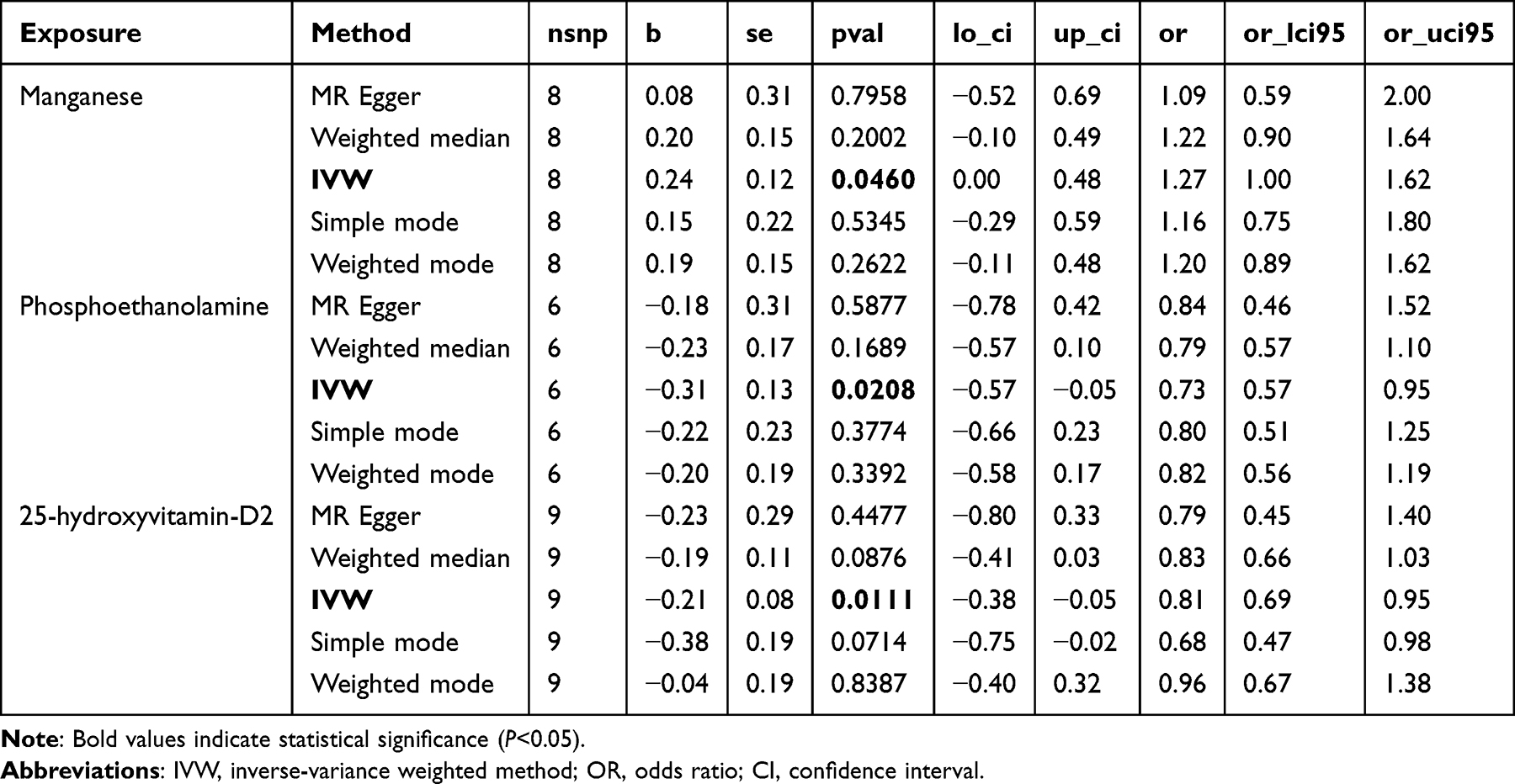 |
Table 2 Mendelian Randomization Analysis Results of Blood Metabolites and COPD, Using the Query Code “Bbj-a-103” |
Sensitivity Analysis and Robustness Testing
Multi-Method Consistency Validation
Beyond IVW, to verify the robustness of the primary analysis, we applied four complementary MR estimators—MR-Egger, weighted median, weighted mode, and simple mode—to all positive or borderline-positive exposures in both East Asian cohorts for triangulation. Across the weighted median, MR-Egger, simple-mode, and weighted-mode models, regression slopes were directionally concordant with the IVW estimates and point estimates were of similar magnitude; notably, for the two protective exposures replicated across cohorts—phosphoethanolamine and 25(OH)D2—the effect intervals from alternative methods largely overlapped those of IVW, yielding consistent direction and comparable magnitude in both the ebi and bbj cohorts. For the two risk-increasing exposures—platelet count and manganese—apart from MR-Egger showing reduced significance due to lower precision, the directions from the other methods were consistent with IVW, with no stable signals contradicting the main conclusions.
Heterogeneity Testing and Horizontal Pleiotropy Evaluation
Cochran’s Q test showed that no significant heterogeneity was observed for the 7 exposures (P > 0.05). The MR-Egger intercept test indicated no significant horizontal pleiotropy (intercept P > 0.05). Additionally, we considered the possibility of bidirectional associations, where COPD may cause changes in blood metabolites. To reduce the risk of this scenario, we conducted the Steiger directional test to enhance the reliability of our findings. The results indicated that all associations pointed correctly from “exposure → outcome”, with no evidence of reverse causality (p < 0.05).
Leave-One-Out Sensitivity Analysis
After sequentially excluding individual SNPs, the repeated IVW analysis showed that all OR point estimates fluctuated within the original 95% CI range, with no extreme changes driven by a single genetic variant (Figure 2B and C), indicating that the results are robust.
Summary
This study systematically identified 7 blood metabolites with stable and directionally consistent causal associations with COPD risk in two large independent East Asian COPD GWAS cohorts. Among these, phosphoethanolamine and 25-hydroxyvitamin D2 showed significant protective effects in both cohorts; platelet count and blood manganese were associated with potential pathogenic effects; amino acids (leucine), organic acids (alpha-aminoadipic acid), and liver enzymes (ALT) also indicated a lower COPD risk. These results were verified through multiple sensitivity analyses, with no significant heterogeneity, horizontal pleiotropy, or reverse causality detected, making the causal inference robust and reliable.
Discussion
COPD is a high-burden disease with highly heterogeneous phenotypes. Previous MR studies on the “metabolite–COPD” causal relationship have mostly been based on European populations. For instance, Zhang et al conducted a large-scale MR analysis using 486 blood metabolites and the FinnGen COPD cohort, identifying several metabolites potentially influencing COPD risk, though the exposure GWAS was entirely based on European cohorts.21 In contrast, this study is based on blood metabolite GWAS data from the Chinese population and integrates two independent East Asian COPD GWAS cohorts, with exposures and outcomes more consistent in terms of ancestral composition, helping to reveal the specific metabolic risk profiles of East Asian populations. We found that genetically predicted elevated platelet count and manganese levels were associated with higher COPD risk, while elevated levels of leucine, alpha-aminoadipic acid, serum-alanine-transaminase, phosphoethanolamine, and 25-hydroxyvitamin D2 were associated with lower risk, with phosphoethanolamine and 25(OH)D2 showing consistent effects in both cohorts, providing robust causal evidence. This echoes recent metabolomics findings on “amino acid and glycerophospholipid dysregulation involved in COPD development”, providing genetic evidence supporting this view.7,22–27
In terms of amino acid metabolism, COPD patients exhibit significant metabolic abnormalities at rest, including systematic alterations in branched-chain amino acids, aromatic amino acids, and sulfur-containing amino acids. These changes are closely related to declines in lung function, disease phenotypes (such as emphysema, airway-dominant), and cachexia/muscle wasting syndrome.7,24–27 We found that genetically increased levels of leucine and alpha-aminoadipic acid were associated with a lower COPD risk, suggesting that a relatively “favorable” amino acid metabolic state may have a protective role in COPD. Leucine, a branched-chain amino acid, is a key activator of the mTOR pathway, involved in skeletal muscle protein synthesis and energy metabolism. Several studies have shown that leucine depletion is linked to muscle atrophy, exercise intolerance, and poor prognosis in COPD patients, and nutritional interventions targeting branched-chain amino acids (BCAA) have shown potential in improving muscle function.24 Alpha-aminoadipic acid, an important metabolic intermediate at the junction of lysine and the tricarboxylic acid cycle, is closely related to insulin sensitivity, lipid metabolism, and oxidative stress regulation.28,29 Its protective signal may reflect a healthier energy metabolism state, which in turn reduces the systemic inflammatory burden, thereby indirectly lowering the risk of COPD. Serum-alanine-transaminase links amino acid and carbohydrate metabolism, and its levels partly reflect skeletal muscle mass and function. We observed that genetically predicted increased ALT levels were associated with a lower risk, and previous population studies also suggest that lower ALT levels predict the occurrence of COPD and adverse outcomes.30,31 These findings jointly support the idea that a “complete amino acid–carbohydrate metabolic pathway” helps combat chronic inflammation and oxidative stress. In terms of lipid pathways, lung tissue metabolomics indicates that various glycerophospholipids are rearranged in COPD, with significant abnormalities in phosphoethanolamine (PE), phosphatidylcholine (PC), and other phospholipids. These changes are closely linked to dysfunction of surfactant, alveolar wall destruction, and impaired gas exchange.26,27,32 Phosphoethanolamine is a key precursor in the synthesis of PE through the Kennedy pathway.33 This study is the first to observe its protective effect in two East Asian COPD cohorts, suggesting that maintaining phospholipid homeostasis may be an important factor in protecting the alveolar–capillary interface.
The relationship between vitamin D deficiency and the onset, acute exacerbations, and mortality risk of COPD has been a recent research focus. Previous systematic reviews and cohort studies have suggested that lower levels of 25(OH)D2 are non-linearly negatively correlated with COPD incidence and mortality, while severe vitamin D deficiency significantly increases the risk of severe acute exacerbations.34–37 However, it remains unclear whether vitamin D deficiency affects the onset and progression of COPD, or if COPD patients experience low vitamin D levels due to the disease itself. In our study, we observed that genetically predicted elevated 25(OH)D2 levels were associated with a lower COPD risk in East Asian populations, with no bidirectional causal relationship between the two. These findings were replicated across cohorts, suggesting that vitamin D status is likely an “upstream causal factor” rather than merely a disease-associated phenotype. Furthermore, COPD is regarded as a syndrome that combines pulmonary and systemic vascular diseases, with cardiovascular comorbidities contributing significantly to mortality. Multiple studies have shown that both stable and acute exacerbation phases of COPD patients exhibit enhanced platelet activation,38–40 characterized by increased mean platelet volume and elevated urine/blood biomarkers. These changes are closely associated with an increased risk of cardiovascular events and mortality. In our study, genetically predicted elevated platelet count was associated with a higher COPD risk, providing causal clues for the “platelet activation-microthrombi-impaired pulmonary microcirculation” pathway, which forms a feedback loop with previous observations of “thrombosis/cardiopulmonary comorbidities”.
Trace element dysregulation has been considered an important component of the oxidative stress and inflammation imbalance in COPD, with abnormal levels being closely associated with the onset, acute exacerbations, and severity of COPD.41,42 Manganese (Mn) is an essential trace element at normal levels, playing a key role in various physiological processes, including antioxidant defense, carbohydrate and lipid metabolism, and free radical neutralization. However, excessive exposure leads to oxidative stress and inflammatory responses, exacerbating airway damage.43 In this study, genetically predicted elevated manganese levels were associated with an increased risk of COPD, suggesting that its impact on COPD is likely U-shaped: both deficiency and excess are detrimental, and the specific dose-response curve remains to be further elucidated.
From a clinical perspective, these findings have direct implications: on the one hand, amino acid metabolism (especially branched-chain amino acids), phospholipid metabolic intermediates, and vitamin D status hold promise as potential biomarkers for early identification and risk stratification of high-risk COPD populations; on the other hand, elevated platelet count and imbalances in trace elements such as manganese may represent a harmful metabolic phenotype characterized by “high inflammation – high coagulation – high oxidative stress”, indicating that these patients are at higher risk for cardiovascular events and acute exacerbations. Therefore, based on MR results, we put forward the following hypotheses that require validation through future intervention studies.: 1) regularly assess and optimize vitamin D levels in high-risk populations, particularly for those with baseline severe deficiency; 2) combine nutritional support (improving protein and BCAA intake) with exercise rehabilitation to delay COPD-related sarcopenia and frailty; 3) explore personalized antiplatelet or anticoagulant strategies for COPD patients with significant platelet elevation or hypercoagulability in preventing cardiopulmonary events; 4) enhance monitoring and intervention of heavy metal exposure from environmental and occupational health perspectives, particularly in exposure scenarios related to manganese, lead, and other metals. These assumptions need to be rigorously evaluated in randomized controlled trials before they can be translated into clinical recommendations.
It is necessary to clearly distinguish between causal inference in the context of Mendelian randomization and clinical causal relationships. The MR estimates reflect the lifetime effects of genetic differences in exposure levels and are less susceptible to confounding and reverse causality. However, these estimates cannot be directly equated with the effects of short-term drug or lifestyle interventions. For instance, although we observe a protective association between vitamin D levels and the risk of COPD, this does not necessarily mean that supplementing with vitamin D in adulthood will bring the same benefits. MR captures the cumulative effect of lifetime exposure differences, while clinical interventions typically involve short-term changes and may involve different biological mechanisms or be affected by compensatory responses. Therefore, our research results should be interpreted as evidence of the causal role of these metabolites in the pathogenesis of COPD, but their clinical application needs to be verified through intervention studies.
This study has significant methodological advantages. The use of Mendelian randomization design fills an important gap in research for East Asian populations. Notably, the MR-Egger regression results show no significant horizontal pleiotropy, which further strengthens the specificity of the causal inference, indicating that the supporting instrumental variables mainly affect COPD risk through the targeted metabolic pathways. Finally, compared to previous MR studies in European populations, we are the first to use Chinese population metabolite GWAS as the exposure, which makes the results more aligned with the East Asian metabolic background and more likely to suggest potential interventions for specific metabolites. The complementary nature of both the population and methodology enriches the “metabolite–COPD causal map”.
However, there are several limitations that need cautious interpretation. First, the exposure and outcome data are derived from GWAS summary statistics, and we are unable to perform nonlinear or stratified analyses at the individual level, making it impossible to answer whether the causal effects of metabolites on COPD differ across age, gender, or smoking status. Second, we used a threshold of P < 5×10−6 for selecting instrumental SNPs, and the genetic explainability of some metabolites is limited, potentially leading to weak instrument bias. Thirdly, this Mendelian randomization study provides genetic evidence for causal associations, but does not include functional experiments (such as in vivo gene knockout mouse models or in vitro experiments) to verify the underlying biological mechanisms. Future research needs to conduct such experimental studies to confirm the causal role of the identified metabolites and elucidate the involved molecular pathways. Fourthly, due to the use of aggregated level data, we are unable to explore the relationship between the identified SNPs or metabolites and other clinical prognostic indicators of COPD (such as the frequency of acute exacerbations, the rate of lung function decline, or mortality). This limits the direct clinical application of the research results. Future studies that combine individual-level data and longitudinal outcomes are needed to assess the prognostic value of these metabolites. Additionally, due to the strictness of multiple testing, the results of this study are better suited as “suggestive causal evidence”, requiring independent validation in larger samples and other populations.
Conclusion
In summary, this study provides preliminary genetic evidence of the causal relationship between blood metabolites and COPD risk based on a two-sample Mendelian randomization analysis in East Asian populations, particularly highlighting the potential key roles of amino acid metabolism, phospholipid metabolism, vitamin D status, and the homeostasis of trace elements like manganese in the pathophysiology of COPD. Compared to previous studies mainly based on European populations, this research emphasizes the significance of population specificity, offering new insights and evidence for understanding the metabolic basis of COPD, formulating precision prevention strategies, and designing metabolically targeted interventions. Future integrated research combining multi-ancestral, multi-omics, and interventional trials is expected to further elucidate the specific roles of these metabolic pathways in the development of COPD and accelerate the clinical translation of these findings. However, these findings are not yet sufficient for clinical decision-making. Their main value lies in guiding future mechanism research and identifying priority targets for intervention studies.
Data Sharing Statement
All of the datasets used in this study came from publicly accessible resources found at (https://gwas.mrcieu.ac.uk/).44 All data were accessed and used in accordance with the database’s terms of use.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Measures for the Ethical Review of Life Science and Medical Research Involving Human Subjects issued in the People’s Republic of China. According to Article 32, Items 1 and 2 of this regulation, this study met the criteria for exemption from ethical review. Therefore, formal ethical approval and informed consent were not required.
Specifically:
- Use of publicly available data:This study exclusively utilized publicly accessible datasets (including GWAS summary-level data), which do not contain identifiable personal information and pose no risk to individual privacy.
- Use of anonymized data:All data analyzed were fully de-identified and anonymized prior to access. The study involved secondary analysis of existing data and did not include any human subject intervention, collection of biological samples, or activities related to genetic manipulation, reproductive cloning, or germline modification.
Based on the above conditions, this study qualifies for exemption from ethical review. All procedures were conducted in accordance with relevant guidelines and regulations.
Acknowledgments
Shixiang Guo, Zheng Li and Mingfeng Wei have contributed equally to this work and should be regarded as co-first authors for this study. We gratefully acknowledge the authors and participants of all data from which we used in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the National Natural Science Foundation of China (Grant No. 82372611).
Disclosure
The authors declare no competing interests in this work.
References
1. GBD 2019 Chronic Respiratory Diseases Collaborators. Global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the Global Burden of Disease Study 2019. EClinicalMedicine. 2023;59:101936. doi:10.1016/j.eclinm.2023.101936
2. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the Global Burden of Disease Study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
3. Boers E, Barrett M, Su JG, et al. Global Burden of Chronic Obstructive Pulmonary Disease Through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
4. Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28(1):29–12. doi:10.1111/resp.14349
5. Godbole S, Bowler RP. Metabolome features of COPD: a scoping review. Metabolites. 2022;12(7):621. doi:10.3390/metabo12070621
6. Kim J, Suresh B, Lim MN, et al. Metabolomics reveals dysregulated sphingolipid and amino acid metabolism associated with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:2343–2353. doi:10.2147/COPD.S376714
7. Casadevall C, Agranovich B, Enríquez-Rodríguez CJ, et al. Metabolomic plasma profile of chronic obstructive pulmonary disease patients. Int J Mol Sci. 2025;26(10):4526. doi:10.3390/ijms26104526
8. Zhou L, Han C, Zhou Y. The role of severe vitamin d deficiency in predicting the risk of severe exacerbation in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2025;20:171–179. doi:10.2147/COPD.S489650
9. Liang Z, Zhao M, Wang Y, et al. The higher serum uric acid to high-density lipoprotein cholesterol ratio is associated with increased risk of chronic obstructive pulmonary disease: result from NHANES 2011–2018. BMC Pulm Med. 2025;25:322. doi:10.1186/s12890-025-03743-5
10. Jia G, Guo T, Liu L, He C. Lipids, lipid-lowering drug target genes and COPD risk: a mendelian randomization study. Chronic Obstr Pulm Dis. 2025;12(6):512–521. doi:10.15326/jcopdf.2025.0632
11. Vicol C, Buculei I, Melinte OE, et al. The lipid profile and biochemical parameters of COPD patients in relation to smoking status. Biomedicines. 2022;10(11):2936. doi:10.3390/biomedicines10112936
12. Cao Z, Wu T, Fang Y, et al. Dissecting causal relationships between immune cells, plasma metabolites, and COPD: a mediating Mendelian randomization study. Front Immunol. 2024;15:1406234. doi:10.3389/fimmu.2024.1406234
13. Wu H, Li H, Tang W, et al. Multi-ancestry mendelian randomization reveals lipid-associated genetic risk factors for COPD. Int J Chron Obstruct Pulmon Dis. 2025;20:2979–2992. doi:10.2147/COPD.S532361
14. Jia G, Guo T, Liu L, He C. Observational and genetic evidence reveals the effect of serum lipid levels on COPD risk. Int J Chron Obstruct Pulmon Dis. 2025;20:2705–2714. doi:10.2147/COPD.S503030
15. Cao Z, Zhao S, Wu T, et al. Genetic information supports a causal relationship between trace elements, inflammatory proteins, and COPD: evidence from a Mendelian randomization analysis. Front Nutr. 2024;11:1430606. doi:10.3389/fnut.2024.1430606
16. Tian Y, Shan S, Bao Q, et al. Identification of novel candidate genes in East Asian COPD patients by the functional summary-based imputation and the unified test for molecular signatures: a transcriptome-wide association study. Chin Med J. 2023;136(13):1612–1614. doi:10.1097/CM9.0000000000002473
17. Ishigaki K, Akiyama M, Kanai M, et al. Large scale genome-wide association study in a Japanese population identifies novel susceptibility loci across different diseases. Nat Genet. 2020;52(7):669–679. doi:10.1038/s41588-020-0640-3
18. Sang S, Chu C, Zhang T, Chen H, Yang X. The global burden of disease attributable to ambient fine particulate matter in 204 countries and territories, 1990-2019: a systematic analysis of the global burden of disease study 2019. Ecotoxicol Environ Saf. 2022;238:113588. doi:10.1016/j.ecoenv.2022.113588
19. Liu ZM, Chen YM, Chen CG, Wang C, Li MM, Guo YB. Genetically determined circulating saturated and unsaturated fatty acids and the occurrence and exacerbation of chronic obstructive pulmonary disease-A two-sample mendelian randomization study. Nutrients. 2024;16(16):2691. doi:10.3390/nu16162691
20. Liu X, Tong X, Zou Y, et al. Mendelian randomization analyses support causal relationships between blood metabolites and the gut microbiome. Nat Genet. 2022;54(1):52–61. doi:10.1038/s41588-021-00968-y
21. Zhang Y, Ma X, Wu F, et al. The relationship between genetic prediction of 486 blood metabolites and the risk of COPD: mendelian randomization study. Sci Rep. 2025;15(1):7349. doi:10.1038/s41598-025-92216-0
22. Wu W, Li Z, Wang Y, Huang C, Zhang T, Zhao H. Advances in metabolomics of chronic obstructive pulmonary disease. Chin Med J Pulm Crit Care Med. 2023;1(4):223–230. doi:10.1016/j.pccm.2023.10.001
23. Gea J, Enríquez-Rodríguez CJ, Agranovich B, Pascual-Guardia S. Update on metabolomic findings in COPD patients. ERJ Open Res. 2023;9(5):00180–02023. doi:10.1183/23120541.00180-2023
24. Zheng H, Hu Y, Dong L, et al. Predictive diagnosis of chronic obstructive pulmonary disease using serum metabolic biomarkers and least-squares support vector machine. J Clin Lab Anal. 2021;35(2):e23641. doi:10.1002/jcla.23641
25. Choi B, San José Estépar R, Godbole S, et al. Plasma metabolomics and quantitative interstitial abnormalities in ever-smokers. Respir Res. 2023;24(1):265. doi:10.1186/s12931-023-02576-2
26. Huang Q, Wu X, Gu Y, et al. Detection of the disorders of glycerophospholipids and amino acids metabolism in lung tissue from male COPD patients. Front Mol Biosci. 2022;9:839259. doi:10.3389/fmolb.2022.839259
27. Feng Y, Xie M, Liu Q, et al. Changes in targeted metabolomics in lung tissue of chronic obstructive pulmonary disease. J Thorac Dis. 2023;15(5):2544–2558. doi:10.21037/jtd-22-1731
28. Shi M, Wang C, Mei H, et al. Genetic architecture of plasma alpha-aminoadipic acid reveals a relationship with high-density lipoprotein cholesterol. J Am Heart Assoc. 2022;11(11):e024388. doi:10.1161/JAHA.121.024388
29. Danhauser K, Sauer SW, Haack TB, et al. DHTKD1 mutations cause 2-aminoadipic and 2-oxoadipic aciduria. Am J Hum Genet. 2012;91(6):1082–1087. doi:10.1016/j.ajhg.2012.10.006
30. Choi YJ, Kwon DS, Kim T, et al. Low alanine aminotransferase as a risk factor for chronic obstructive pulmonary disease in males. Sci Rep. 2021;11(1):14829. doi:10.1038/s41598-021-94385-0
31. Lasman N, Shalom M, Turpashvili N, et al. Baseline low ALT activity is associated with increased long-term mortality after COPD exacerbations. BMC Pulm Med. 2020;20(1):133. doi:10.1186/s12890-020-1169-z
32. Telenga ED, Hoffmann RF, t’Kindt Null R, et al. Untargeted lipidomic analysis in chronic obstructive pulmonary disease. Uncovering sphingolipids. Am J Respir Crit Care Med. 2014;190(2):155–164. doi:10.1164/rccm.201312-2210OC
33. Gibellini F, Smith TK. The Kennedy pathway--De novo synthesis of phosphatidylethanolamine and phosphatidylcholine. IUBMB Life. 2010;62(6):414–428. doi:10.1002/iub.337
34. Williamson A, Martineau AR, Jolliffe D, et al. Vitamin D for the management of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2024;9(9):CD013284. doi:10.1002/14651858.CD013284.pub2
35. Yumrutepe T, Aytemur ZA, Baysal O, Taskapan H, Taskapan CM, Hacievliyagil SS. Relationship between vitamin D and lung function, physical performance and balance on patients with stage I-III chronic obstructive pulmonary disease. Rev Assoc Med Bras. 2015;61(2):132–138. doi:10.1590/1806-9282.61.02.132
36. Ferrari R, Caram LMO, Tanni SE, Godoy I, Rupp de Paiva SA. The relationship between Vitamin D status and exacerbation in COPD patients- a literature review. Respir Med. 2018;139:34–38. doi:10.1016/j.rmed.2018.04.012
37. Lokesh KS, Chaya SK, Jayaraj BS, et al. Vitamin D deficiency is associated with chronic obstructive pulmonary disease and exacerbation of COPD. Clin Respir J. 2021;15(4):389–399. doi:10.1111/crj.13310
38. Maclay JD, McAllister DA, Johnston S, et al. Increased platelet activation in patients with stable and acute exacerbation of COPD. Thorax. 2011;66(9):769–774. doi:10.1136/thx.2010.157529
39. Muñoz-Esquerre M, Ferreiro JL, Huertas D, et al. Impact of acute exacerbations on platelet reactivity in chronic obstructive pulmonary disease patients. Int J Chron Obstruct Pulmon Dis. 2018;13:141–148. doi:10.2147/COPD.S152660
40. Fawzy A, Putcha N, Raju S, et al. Urine and plasma markers of platelet activation and respiratory symptoms in COPD. Chronic Obstr Pulm Dis. 2023;10(1):22–32. doi:10.15326/jcopdf.2022.0326
41. Fekete M, Lehoczki A, Csípő T, et al. The role of trace elements in COPD: pathogenetic mechanisms and therapeutic potential of zinc, iron, magnesium, selenium, manganese, copper, and calcium. Nutrients. 2024;16(23):4118. doi:10.3390/nu16234118
42. Hua X, Zhu L, Chen H. Association between blood heavy metal levels and COPD risk: a cross-sectional study based on NHANES data. Front Public Health. 2025;13:1494336. doi:10.3389/fpubh.2025.1494336
43. Pajarillo E, Kim S, Digman A, et al. Dopaminergic REST/NRSF is protective against manganese-induced neurotoxicity in mice. J Biol Chem. 2024;300(9):107707. doi:10.1016/j.jbc.2024.107707
44. IEU OpenGWAS. “IEU OpenGWAS database: summary statistics for metabolic traits and COPD”. MRC Integrative Epidemiology Unit; [dataset] 2024. Available from: https://gwas.mrci.eu.uk/.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.