Back to Journals » Hepatic Medicine: Evidence and Research » Volume 15
Medicinal Plants in Treating Hepatitis B Among Communities of Central Region of Ethiopia
Authors Beykaso G, Teklehaymanot T, Mulu A, Berhe N, Alemayehu DH, Giday M
Received 14 October 2023
Accepted for publication 21 December 2023
Published 29 December 2023 Volume 2023:15 Pages 265—277
DOI https://doi.org/10.2147/HMER.S440351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Gizachew Beykaso,1 Tilahun Teklehaymanot,2 Andargachew Mulu,3 Nega Berhe,2 Dawit Hailu Alemayehu,3 Mirutse Giday2
1Department of Public Health, College of Medicine and Health Science, Wachemo University, Hossana, Ethiopia; 2Department of Immunology and Molecular Biology, Aklilu Lemma Institute of Pathobiology, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Virology, Armauer Hansen Research Institute, Addis Ababa, Ethiopia
Correspondence: Gizachew Beykaso, Department of Public Health, College of Medicine and Health Science, Wachemo University, Hossana, Ethiopia, Tel +251-912066531, Email [email protected]
Purpose: In Ethiopia, most people rely heavily on traditional therapeutic plants that have been used for years. The practice of traditional medicines use to treat hepatitis is currently gaining popularity due to the limited availability and affordability of modern drugs. The aim of this study was, therefore, to assess the traditional medicinal plants use to treat viral hepatitis among communities of Central region of Ethiopia.
Methods: Data was collected from November 2018 to December 2021 in Central Ethiopia. An open-ended semi-structured interview was used among purposively selected herbalists, traditional medicine entrepreneurs, village heads, and patients visiting traditional healers for hepatitis treatments. A 5 mL blood sample was collected from patients who visited a traditional healers’ clinic for hepatitis treatment and tested for HBsAg and HCV-antibody by using ELISA. Among HBsAg-positives, further nucleic acid test for HBV-DNA load was assessed to measure the effects of prescribed medicinal plants.
Results: Herbalists cited 24 plants that were used for hepatitis treatment; of which Rumex nepalensis, Vangueria apiculata, and Solanum incanum were the most frequently cited plants. Remedies were commonly prepared by crushing or powdering, mixing them with water, and taken orally. Forty-two individuals were diagnosed and treated as hepatitis patients by herbalists, of which eight of them were HBsAg-positive but no positives for anti-HCV ELISA. At the third and sixth months of viral load assessment among HBsAg-positive, serum HBV-DNA suppression was observed in three individuals treated with different combinations of frequently cited plants.
Conclusion: In this study, traditional healers used various plants to treat hepatitis. HBV-DNA suppressive activity was detected in three NAT-positive individuals who were treated by using a mixture of these frequently cited and highest preference-ranked plants. This suggests that these plants have antiviral properties and serve as a basis for more pharmacological research in the quest for new antiviral agents.
Keywords: medicinal plants, hepatitis, Central Ethiopia
Introduction
Viral hepatitis is a liver disease that causes inflammation and can lead to permanent damage.1 Hepatitis B and C viruses, which cause chronic viral hepatitis, are the most widespread and serious public health issues, affecting millions of people and killing an estimated 1.5 million people each year globally.2,3 In developing countries, mainly in Sub-Saharan Africa, the burden of HBV infection remains disproportionately highly endemic (>8%) to intermediate (2–8%).4,5 Ethiopia is one of the developing countries with the highest hepatitis morbidity and mortality.6,7
In Ethiopia, the use of traditional medicine has been practiced for centuries as a treatment for various diseases and remedies.8,9 The majority of Ethiopian people depend on traditional remedy for most of their health problems. Most of these therapies were traditional preparations made of medicinal plants basis and are sometimes the solitary source of healing for the majority of the people.10,11 Ethiopia is also domestic to various cultures, beliefs and languages that have sequentially contributed to the great assortment of traditional understanding and exercise of the people to use therapeutic plants for various traditional treatment practices.12,13 Generally, therapeutic plants used for traditional remedy play an important role in the healthcare of the most of the people in Ethiopia.9,14
Traditional healers use a variety of plants as a primary basis of remedy to treat different types of illnesses, including hepatitis, and these plants are an important part of Ethiopian culture.9,15 This widespread use of medicinal plants in Ethiopian cultures to heal these ailments, including hepatitis, is due to lack of modern medicines used to treat and cure some diseases including viral hepatitis.16–18 As a result, affected patients seek alternative remedies and visit traditional healer’s treatment centers, particularly for herbal therapies due to their social acceptability, effectiveness, accessibility, and affordability since modern medicines used to treat some of diseases including viral hepatitis are expensive and out of reach for most people in developing countries.8,19–21 These traditional healers’ treatment for hepatitis diseases varies from place to place and among traditional healers. In some instances, it is treated with a single plant preparation in places and in others with a concoction of two or more plants.22,23
The usage of medicinal plants in Ethiopia is enormous, though the activities are poorly reported and difficult to access for modern study.18 As a result, the quest for plant-based antiviral hepatitis drugs in the country necessitates a comprehensive ethnobotanical investigation in various localities and districts to document the diverse information held by various ethnic groups and communities. In Ethiopia, there was limited studies in antihepatitis traditional medicinal plants, therefore, this study aimed to document and assess the practice of traditional therapeutic plants to treat viral hepatitis among communities of the Central region of Ethiopia.
Materials and Methods
Study Setting and Period
The study was done from November 2018 to December 2021 in three zonal or administrative districts of the Central Region of Ethiopia: namely Hadiya, Kambata, and Silte districts. The zones are located at 230 km from Addis Ababa, the capital city of the country. Most population are rural inhabitants with some living in zonal towns and other small towns with an average annual growth rate of 2.9%. According to the 2007 population census, the three zones have a total population of 3,062,431: Hadiya has a population of 1,231,196; Kambata has a population of 1,080,837 and Silte has a population of 750,398 with 251,264, 220,579 and 153,142 households, respectively.
Study Design and Population
A cross-sectional study was done to assess the traditional practice of therapeutic plants to heal viral hepatitis among communities of Central Region of Ethiopia. The study participants were taken from purposively selected traditional healers, traditional medicine entrepreneurs, village heads, and patients who were visiting traditional healers for treatments and diagnosed as hepatitis patients by traditional healers in the district.
Sample and Sampling Techniques
Traditional healers, village heads, traditional medicine entrepreneurs, and individuals who were visiting traditional healers for their treatments and diagnosed as hepatitis patients by traditional healers were purposefully included in the study. For that reason, purposively selected 52 herbalists, 9 traditional medicine entrepreneurs, 48 village heads, and 42 individuals who came to traditional treatment remedies and traditionally diagnosed hepatitis patients were included in the study. However, these individuals who came to traditional healer and not diagnosed as hepatitis cases by traditional healers were excluded.
Data Collection Process and Tools
The ethnobotanical survey consisted of an open, semi-structured interview in which the interviewee was asked to answer exhaustively the questions asked by the interviewer. The questionnaire incorporated the particular information of the informants including name of the respondent, age, gender, and address, knowledge of hepatitis and traditional healing practice. The questions were asked in their languages. The themes dealt with mainly relating to the scientific and the local names, the parts used, time and plant material collecting season, its preparation, the dose, its route and the duration of the treatment, side effects, and antidotes used, and contraindications for these remedies. The interviewees concerned were mostly purposively selected herbalists, traditional medicine entrepreneurs, village heads, and patients who were visiting traditional healers’ clinics for treatments and diagnosed as hepatitis patients by traditional healers. Field trips were made in the presence of the interviewee, to see the medicinal plants mentioned, to photograph them, and to collect specimens. A market survey was also used to collect additional ethnobotanical information concerning hepatitis treatment.
Collection of Plants’ Specimen and Identification
Specimens of the documented therapeutic plants were collected from natural flora and home-gardens during the field gait. Voucher samples were labelled, dried up, and placed in Addis Ababa University (AAU) National Herbarium. The identification of the plants’ species was done by botanists at National Herbarium of Addis Ababa University and the Aklilu Lemma Institute of Pathobiology.
Blood Sample Collection
Five-milliliter of blood samples were collected from each individuals who were visiting traditional healers for treatment and diagnosed as a hepatitis patient by traditional healers. The blood sample was collected before taking the treatment which was given by traditional healers. Separation of serum from collected whole blood was done and stored at deep freeze of temperature below −80°C and screened for HBV (HBsAg) and HCV (anti-HCV) infections by using ELISA assay of Beijing WANTAI Biological, China, following the manufacturer’s instructions. From individuals whose blood samples were positive for ELISA test short assay or quantitative nucleic acid test, additional five-milliliter blood samples were collected on the third and sixth months after anti-hepatitis medicinal plants treatment and used for nucleic acid tests by using polymerase chain reaction (PCR) for treatment follow-up assessment.
Viral Load Quantifying
HBV-DNA detection was obtained in samples from people who tested positive for Hepatitis B surface antigen (ELISA) before starting typical anti-hepatitis medication, as well as three and six months later. Following the manufacturer’s instructions, HBV DNA was extracted from 200μL of plasma using the m2000sp, an automated sample preparation system designed to use magnetic micro-particle-based reagents for the purification of nucleic acids from samples (Abbott Laboratories, Abbott Park, IL, USA) with a lower quantification limit or sensitivity of 15 IU/mL for the 0.2 mL serum sample volume. Positive, negative, and high positive controls were employed. In the sample preparation technique, an internal controller DNA was supplied and processed alongside the calibrators, controls, and samples. During the extension and annealing steps, the presence of amplified HBV-DNA and an internal control was identified. The amplification cycle at which the Abbott m2000rt detected a normalized fluorescence signal was related to the log of the HBV DNA concentration in the original sample. An external calibration curve was then used to quantify each sample. About 10% of the samples were re-tested to ensure uniformity.
Data Entry and Analysis
MS Excel 2010 spreadsheet was used for data entry and determination of proportions, and percentiles, and to summarize the ethnobotanical data associated with the use of therapeutic plants for the treatment of hepatitis. A preference rating was carried out for the top seven medicinal plants that are used for the treatment of hepatitis. Ten informants were chosen at random from among traditional healers who reported using medicinal plants to treat hepatitis in order to determine the best favored species of medicinal plants and their level of efficacy. Seven medicinal plants that were chosen based on the frequency of citation order were given to the informants, who were then asked to rate each plant’s preference on a scale of 1 to 7. The plant that was most favored received a score of 7, while the least favored species received a score of 1. Each species’ value was added up, and the final score was used to establish each species’ rank. This helped to agree the rank order of the most effective medicinal plants used by the public to heal hepatitis.
Ethical Approval and Consent to Participate
The principles outlined in the Declaration of Helsinki were followed in the conduct of the study. Prior to collecting data, the study protocol was reviewed and approved by the ethical review committees of the Southern Nation Nationalities and People’s Regional State Health Bureau (Ref No. PN37-/86/19743) and the Aklilu Lemma Institute of Pathobiology, Addis Ababa University (Ref No. ALIPB IRB/002/2011/2018). After being asked about their voluntariness and provided with comprehensive information about the study’s goals, potential hazards, and significance in their languages, the participants were asked to provide signed, and informed permission. The participants received assurances of their complete autonomy to choose whether or not to engage in the study. After completing their herbal treatment, those who still tested positive for nucleic acids were counseled and connected to medical facilities for further care. Every piece of information gathered for the study was kept private.
Results
Socio-Demographic Characteristics of the Study Participants
A total of 48 village heads consisting of 30 (62.5%) males and 18 (37.5%) females; 9 traditional medicine entrepreneurs consisting of 7 (77.7%) males and 2 (22.3%) females; 52 traditional herbalists consisting of 37 (71.2%) males and 15 (28.8%) females; and 42 individuals diagnosed as hepatitis patients by traditional healers based on signs and symptoms of the disease. Of the hepatitis-diagnosed individuals, 17 (40.5%) were males and 25 (59.5%) were females with ages ranging from 25 to 86 with mean age ± SD = 47 ±15.4 years).
Anti-Hepatitis Medicinal Plants Documented
It was reported that residents of the study districts employed a total of 24 medicinal plants from 22 families to treat hepatitis. Three medical plants from the Asteraceae family and one plant from each other represented the other families. The most frequently cited anti-hepatitis medicinal plants were R. nepalensis, V. apiculata, S. incanum, and C. macrostachyus. R. nepalensis was reported by 12 informants, V. apiculata by 11 informants, S. incanum by 10 informants, and C. macrostachyus by 9 informants (Table 1).
 |
Table 1 Medicinal Plants Identified in Treating Hepatitis B in the Study Districts |
Methods of Medicinal Remedy Preparation
The primary methods of remedy preparations were shown to be crushing (37.5%), squeezing (29.2%), and powdering (20.3%). Majority (79.2%) of the anti-hepatitis plants were prepared fresh while some (12.5%) were used either fresh or dried, and small proportions (8.3%) were reported to be dried and kept for future uses. Majority (71.0%) of the healers used mixtures of different species to treat hepatitis. Plant parts were collected when required, and there was no fixed time needed for its collection. Additives like tea, milk, coffee, honey, and sugar were used in most (78.0%) preparations of the remedy.
Dosage Preparation and Route of Administration
In this study, all remedies were administered orally. In most cases, the prepared therapies or remedies were given once a day and completed within one week. In some cases, remedies could be extended beyond one month until recovery from the ailment evidenced by the absence or disappearance of the signs and symptoms. Dosages were estimated using spoons, glasses, and tea or coffee cups (Table 1). Remedy prescription was reported to be based on the patient’s age, the degree and duration of the illness, the presence of other diseases, and the experiences of traditional healers. Children were given lower doses than adults; physically strong patients took a higher dose or amount than weak patients.
The absence of several adverse effects of traditional remedies or medicines after administration was often mentioned by the traditional healers, but some preparations from the plants R. nepalensis, V. amygdalina, and P. falcatus were indicated to have some adverse or side effects characterized by abdominal pain, vomiting, and diarrhea. Treatment with O. rochetiana and A. abyssinicus was reported to rarely cause loss of consciousness. The majority (66.0%) of the traditional healers indicated that they used milk, “tella”, and meat soup with butter as antidotes to mitigate the adverse effects of some remedies. Most (81.5%) of the healers reported that milk, honey, coffee, sugar, or “tella” were used as additives for most of the remedies to make them more palatable and/or improve their effectiveness.
Traditional Knowledge and Its Transfer Modality in the Districts
Most (85.0%) of the respondents reported that if they had hepatitis or were diagnosed with hepatitis, they would prefer traditional herbal treatments to modern medications because they believed that they would not get better medications for hepatitis in modern health services. About 82.0% of them believed that traditional healers could cure hepatitis with medication, and they could easily access it at a low price. Traditional healers used to diagnose hepatitis mainly based on jaundice and others such as fatigue, joint pain, fever, nausea, vomiting, and loss of appetite, abdominal pain, and dark urine. In these treated patients, traditional healers reported improvements in these symptoms after the treatment period.
Most (84.6%) of the medicinal plants were cited by traditional healers of age greater than forty-six years. On average, significantly higher numbers (74.0%) of medicinal plants were reported by men than women. The majority (79.6%) of healers reported that they acquired the indigenous knowledge from their parents, while some (11.4%) stated that they gained it from their tribal local elders and few (9.0%) mentioned acquiring the knowledge by other means such as through observation and self-trial. Of the traditional healers who used to transfer their knowledge on medicinal plant use, almost all (96.0%) reported doing it orally to their family members. All healers kept their knowledge secret, exposing it only to their sons or close family members in their old age. Of the total interviewed healers, 79.6% reported that they preferred to transfer their knowledge to their trusted eldest sons, but few (9.0%) reported transferring it to any member of their family. All healers reported that they transferred their knowledge without any payment to their trusted eldest sons and some other members of their family. However, all healers reported that they were not willing to share their knowledge with people outside their family circle.
Preference Ranking
Seven medicinal plants that were described to be the most useful plants to treat hepatitis were ranked by each of 10 randomly selected traditional healers based on their perceived level of importance. Accordingly, R. nepalensis was found to be the most preferred medicinal plant to treat hepatitis followed by S. incanum and V. apiculata (Table 2).
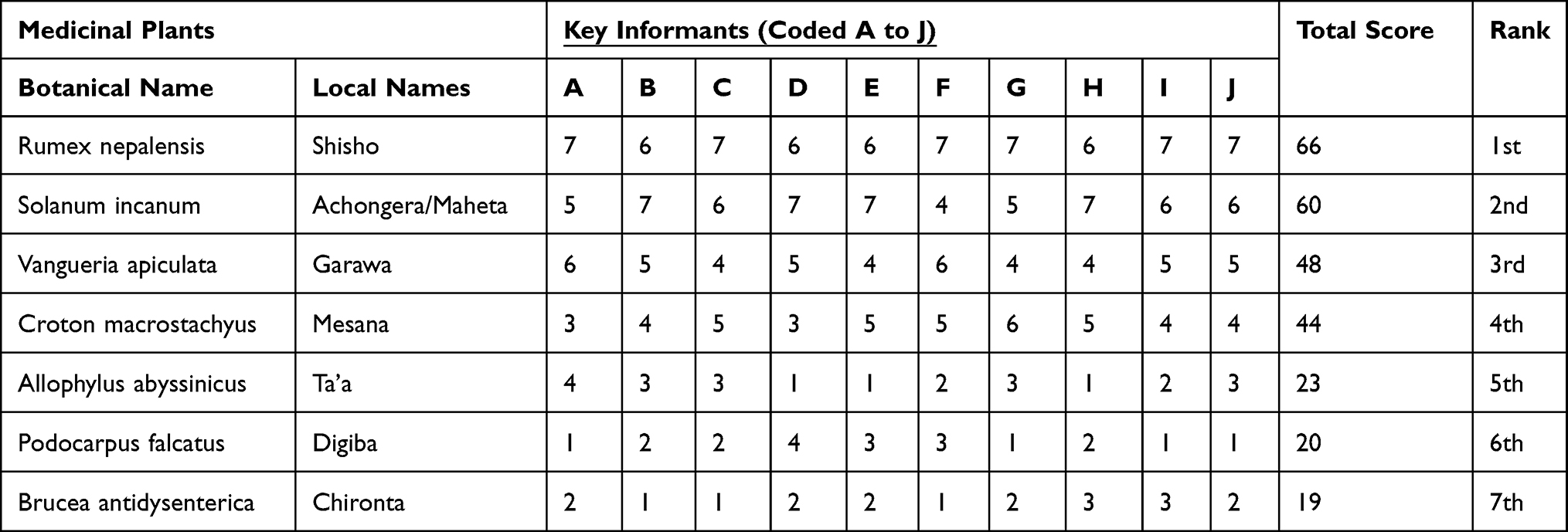 |
Table 2 Preference Ranking Exercise on Six Selected Plant Species Used to Treat Hepatitis |
Serological Results
A total of forty-two individuals were diagnosed as hepatitis patients by traditional healers for anti-hepatitis herbal treatments. Eight (19.1%) out of the forty-two individuals who were diagnosed as hepatitis patients by traditional healers were found to be positive for HBsAg, but all (100%) individuals’ blood samples were negative for the anti-HCV ELISA test. The eight individuals who tested positive for HBsAg before the initiation of the anti-hepatitis medicinal plants treatment was also tested positive for HBsAg at three and six months after the initiation of anti-hepatitis medicinal plants treatment (Table 3).
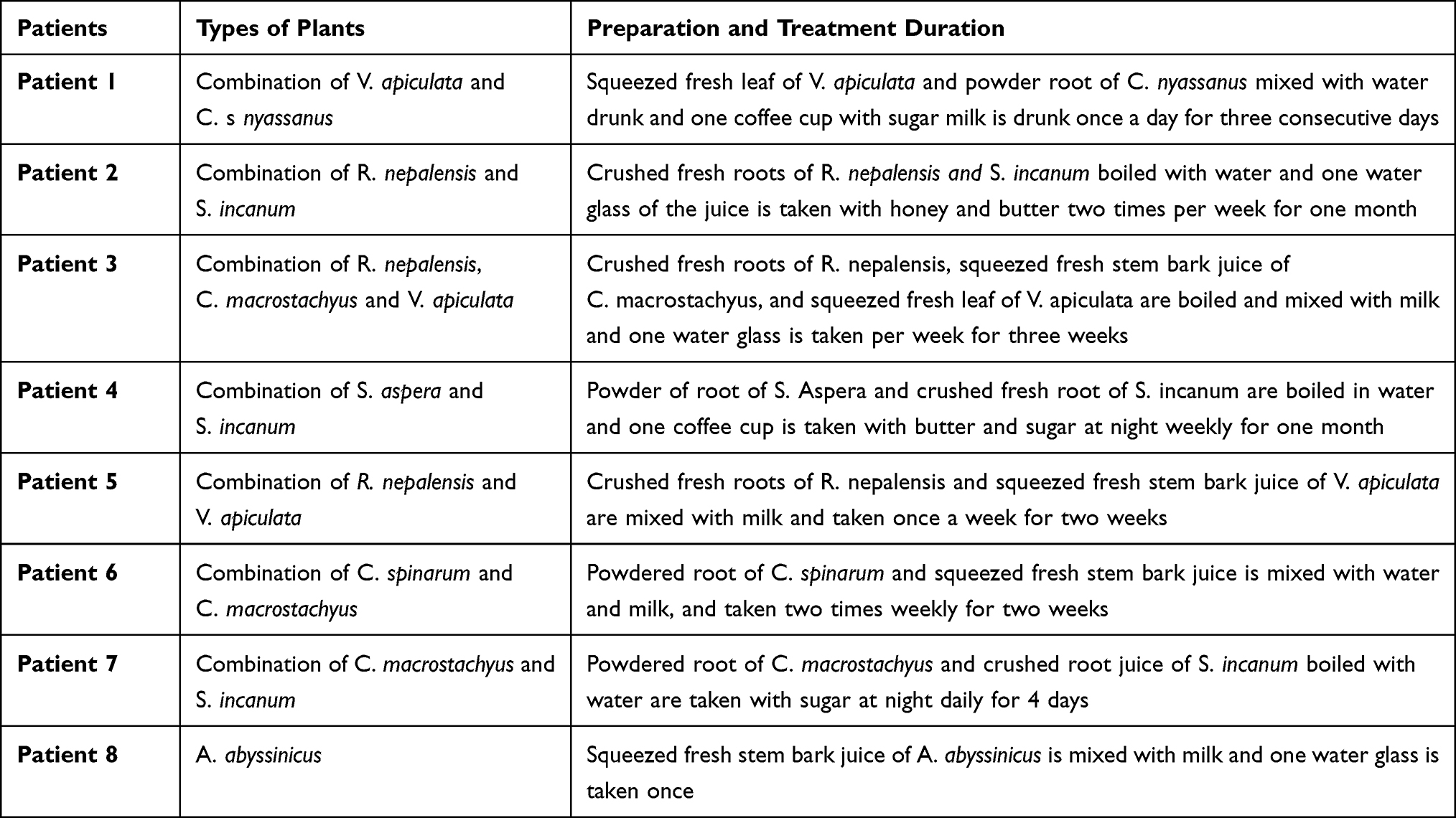 |
Table 3 Progression of the HBV Viral Loads in Hepatitis Patients Treated with the Different Plant Combinations in Central Ethiopia |
HBV Viral Load Assessment
HBV DNA was detected in all eight (100%) blood samples that tested positive for HBsAg before the initiation of the antihepatitis medicinal plants’ treatment. HBV DNA was also detected in seven (87.5%) of the HBsAg-positive individuals’ second samples at the third month of initiation of medicinal plants treatment and five (62.5%) individuals out of eight HBsAg-positive individuals’ third samples at six months of anti-hepatitis medicinal plants treatment. All blood samples taken before the initiation, at the third, and six months after initiation of the traditional antihepatitis medicinal plant were found positive for HbsAg (Table 4).
 |
Table 4 The Serological HBV HBsAg and HBV-DNA at the Different Time Duration |
In one individual (Patient 2) treated with medicinal plants of crushed fresh root extracts of R. nepalensis and S. incanum boiled in water, HBV-DNA suppression was observed during the third and sixth months of viral load assessment. Similarly, at six months of viral load evaluation, HBV-DNA suppression was also observed in individuals who were treated with medicinal plants extract of three plants combined including R. nepalensis, C. macrostachyus, and V. apiculata, (Patient 3) and a combination of two plants (R. nepalensis mixed with V. apiculata) (Patient 5). In addition to this, the serum HBV-DNA suppression effects were also observed during viral load assessment in individuals treated with the combination of R. nepalensis, C. macrostachyus, and V. apiculata, and a combination of B.antidysenterica with S. incanum (Table 4). In serum HBV-DNA-positive individuals, suppression of HBV-DNA level was observed after treatment with different herbal medicines, commonly with combination of R. nepalensis by traditional healers.
Discussion
According to the respondents’ beliefs in the districts, the preference for traditional medicine in treating hepatitis was a result of the lack of better medications for hepatitis in modern healthcare facilities; however, the identity of medicines used to treat hepatitis is unknown except to the healers, who probably pass their knowledge through generations in the family line. This is similar with study findings done in Ethiopia and other countries.12,24,25
In the study area, traditional healers largely transfer knowledge of medicinal plants use orally to a selected family member, especially to the trusted elder sons, when they get very old. This indicates that traditional medicinal healers need their knowledge to be held in secret and thus there is a great danger of losing it. Traditional healers reported that they strongly believed traditional medicine was effective if done within a family or with close relatives and when it was kept secret; if not medicinal plants would lose their healing power. The traditional healer’s strong belief in keeping the knowledge secret could be due to the fear of losing societal recognition and the reputation that traditional healers have earned through time. This is also supported by other similar findings from Ethiopia and other countries.12,26,27
Most of the knowledge was owned by older people who were responsible for maintaining the well-being of their communities. The fact that traditional medical practice in the study area is dominated by old people indicates the extent of danger the transfer of knowledge is facing. Comparable results were reported in other studies conducted in Ethiopia and elsewhere in Africa.23,28 It was reported that considerably greater numbers of medicinal plants species were reported by males than females. The small number of females serving as respondents might be because the knowledge is mostly transferred through the male line. Similar results were reported in studies conducted elsewhere in Ethiopia and other countries in Africa.22,29
Some of the traditional medicinal plants species used to treat hepatitis in this study are also used elsewhere in Ethiopia and other countries for the same purpose. These include C. macrostachyus,30 C. africana,31 B. antidysenterica, M. foetida,32 Ficus sur,33 A. aspera,32 and R. nepalensis.34 The reason for the similarity in use may be due to the existence of biologically active compounds that are effective against hepatitis. As shown by preference ranking exercises, R. nepalensis followed by S. incanum and V. apiculata were the most preferred plants by traditional healers to treat hepatitis, possibly indicating their high healing potential in the treatment of the disease. This finding is also supported by other similar findings reported elsewhere in Ethiopia.35–37
The finding of this study indicated that more than one species of the medicinal plants were commonly used by traditional medicinal healers to prepare therapies. This could be attributed to the synergistic or additive effects that they possibly have for the duration of treatment. This is supported by other similar study findings reported elsewhere in Ethiopia.38–40 However, a study done in other countries indicated that most preparations were prepared from a single healing plant species.41,42 This could be explained by the socio-cultural differences of traditional healers. The most of antihepatitis medications in the study area were prepared as of freshly harvested plant parts. These remedies were prepared by boiling in water, and the healers commonly believed that additives like milk, sugar, honey, tea, coffee could improve palatability and also potentiate the effects of prescribed remedies which are also similar with the findings done somewhere else in Ethiopia.43–47
Most traditional healers were found to have inconsistent knowledge of dosage and use of antidotes while prescribing medicinal preparations to their patients. This could be due to the experiences and socio-cultural differences of traditional healers. Most of these medicinal preparations were reported to have no serious adverse effects except for certain minor effects like abdominal pain, diarrhea, and vomiting. The low toxicity of the remedying preparations of the healing plant species is reflected in the high tendency of the community to use them. This is consistent with other studies done in Ethiopia and some other countries.47,48 The prescribed differences in dosage, duration, the unit of measurement, and time for treatment of hepatitis were also determined by age, physical fitness, and the presence or absence of any other diseases. The finding is in consistent with the result of different ethnobotanical studies done somewhere else in Ethiopia that have also discussed the lack of standardization and precision as a shortcoming of the traditional healthcare system.33,43
Forty-two individuals were traditionally diagnosed as hepatitis patients for herbal treatment by traditional herbalists tested for HBsAg and anti-HCV ELISA. Eight (19.1%) of these individuals were positive for HBsAg but no positives for the anti-HCV ELISA test. This may explain the fact that most of the individuals who were diagnosed as hepatitis patients and treated for hepatitis by traditional medicine were not actual viral hepatitis patients, rather they may be non-viral hepatitis or misdiagnosed as hepatitis patients by traditional herbalists. The result is also in similar with other findings of different ethnobotanical studies done in somewhere else in Ethiopia and other countries, which have a lack of missed diagnosis and precision as a shortcoming of the traditional healers’ treatment.8,9,49
In some HBV-DNA-positive individuals, the suppression of serum levels of HBV-DNA was observed after treatment with a combination of different extracts of herbal medicines by traditional healers. The suppression effects were detected in individuals treated with the combination of R. nepalensis and S. incanum, and the combination of R. nepalensis and A. abyssinicus. Similarly, the serum HBV-DNA suppression effects were also observed in individuals treated with the combination of R. nepalensis, C. macrostachyus, and V. apiculata, and the combination of B. antidysenterica and S. incanum. These suppression effects observed by extracts of these plants might be associated with the presence of chemical ingredients that have antihepatitis properties. The result is also supported by the findings of other studies done somewhere else.50 More other studies also reported the antihepatitis properties of R. nepalensis,51 S. incanum,42 and A. abyssinicus.50
Serum HBV-DNA-positive patients treated with these plants, particularly when combined with R. nepalensis, showed serum viral suppression effects in this finding. This indicates R. nepalensis has an action of antihepatitis properties even though the mechanisms of its action and ingredients were not studied. There are also other studies in agreement with this finding that R. nepalensis has antihepatitis properties.51
Conclusion
This study established that the communities have been using different traditional therapeutic plant species and the associated indigenous knowledge as a primary choice while contemporary health services are expanding in the Districts. The reported new antihepatitis traditional therapeutic plant types in this study have confirmed the call for further on ethnobotanical and other scientific research studies. The use of these plants to treat hepatitis is still needed by the communities as a result of the lack of substitutes for better medication by modern healthcare programs in health facilities. This study also established that indigenous knowledge transfer is declining after generation to generation as the main method of transmission is oral. Therefore, this study recommends the urgent documentation of the medicinal plants’ knowledge before it is completely lost. Increased use-value recorded and higher preference ranking scores on the mentioned therapeutic plant species would empower upcoming pharmaceutical investigations and conservation practices.
In some HBV-DNA positive patients treated with the combination of frequently sited and highest preference ranked plants revealed viral suppression activities, which partly explains some antiviral properties of the plants and is used as a basis for further pharmacological investigations in the effort of the search for new and locally affordable anti-hepatitis viral agents beside isolating and identifying their active principles. Pharmaco-chemical investigations are required to assess the efficacy and safety of all claimed therapeutic plants. The priority to assess bioassay and toxicity investigations should, however, be taken to therapeutic plants that have the highest preference score and HBV DNA suppressive effects before they are recommended for broader use and advance pharmacological analysis. Further efforts should also be taken by concerned bodies to lead into the results of any future studies on the efficacy and safety of the reported therapeutic plants back to the owners of the knowledge.
Data Sharing Statement
The data and resources used to provide the conclusions of this study are available upon rational request from the corresponding author.
Acknowledgments
The authors would like to grateful Wachemo and Addis Ababa Universities for grants provided to support this work. We also owe a great deal to the study districts’ administrative offices, the local populace, informants who kindly shared their traditional wisdom with us, and participants who provided us with relevant data and blood samples. We would also want to express our gratitude to Armauer Hansen Research Institute and the Hossana Blood Bank District for providing laboratory kits. We also acknowledge Melaku Wondafrash of the National Herbarium, Addis Ababa University, for his assistance in the identification of plants.
Author Contributions
Significant contributions were made by each author to the conception and design, data collection, analysis, and interpretation processes; writing of the article or substantial intellectual content revisions; reading and approval of the completed manuscript before it was submitted to the current journal; and acceptance of responsibility for all aspects of the work.
Funding
The grants provided by Wachemo and Addis Ababa Universities allowed for the funding of this study. The decision to publish, data collection and analysis, study design, or paper preparation were all done without the funder’s involvement.
Disclosure
In accordance with the authors, they have no competing interests with this work.
References
1. van Meer S, van Erpecum KJ, Sprengers D, et al. Hepatocellular carcinoma in cirrhotic versus noncirrhotic livers: results from a large cohort in the Netherlands. Eur J Gastroenterol Hepatol. 2016;28(3):352–359. doi:10.1097/MEG.0000000000000527
2. Smith S, Harmanci H, Hutin Y, et al. Global progress on the elimination of viral hepatitis as a major public health threat: an analysis of WHO Member State responses 2017. JHEP Rep. 2019;1(2):81–89. doi:10.1016/j.jhepr.2019.04.002
3. Bartenschlager R, Urban S, Protzer U. Towards curative therapy of chronic viral hepatitis. Z Gastroenterol. 2019;57(01):61–73. doi:10.1055/a-0824-1576
4. Franco E, Bagnato B, Marino MG, et al. Hepatitis B: epidemiology and prevention in developing countries. World J Hepatol. 2012;4(3):74. doi:10.4254/wjh.v4.i3.74
5. Stanaway JD, Flaxman AD, Naghavi M, et al. The global burden of viral hepatitis from 1990 to 2013: findings from the Global Burden of Disease Study 2013. Lancet. 2016;388(10049):1081–1088. doi:10.1016/S0140-6736(16)30579-7
6. Yazie TD, Tebeje MG. An updated systematic review and meta-analysis of the prevalence of hepatitis B virus in Ethiopia. BMC Infect Dis. 2019;19(1):1–13. doi:10.1186/s12879-019-4486-1
7. Belyhun Y, Maier M, Mulu A, et al. Hepatitis viruses in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2016;16(1):1–14. doi:10.1186/s12879-016-2090-1
8. Tadele A. Ethiopian Herbal Medicine Research Article Profile. Ethiopian Public Health Institute; 2017:1–343.
9. Tesfahuneygn G, Gebreegziabher G. Medicinal plants used in traditional medicine by Ethiopians: a review article. J Respir Med Lung Dis. 2019;4(1):1–3.
10. Tuasha N, Petros B, Asfaw Z. Medicinal plants used by traditional healers to treat malignancies and other human ailments in Dalle District, Sidama Zone, Ethiopia. J Ethnobiol Ethnomed. 2018;14(1):1–21. doi:10.1186/s13002-018-0213-z
11. Yineger H, Kelbessa E, Bekele T, Lulekal E. Plants used in traditional management of human ailments at Bale Mountains National Park, Southeastern Ethiopia. J Med Plants Res. 2013;2(6):132–153.
12. Fenetahun Y, Eshetu G. A review on ethnobotanical studies of medicinal plants use by agro-pastoral communities in, Ethiopia. J Med Plants. 2017;5(1):33–44.
13. Araya S, Abera B, Giday M. Study of plants traditionally used in public and animal health management in Seharti Samre District, Southern Tigray, Ethiopia. J Ethnobiol Ethnomed. 2015;11(1):1–25. doi:10.1186/s13002-015-0015-5
14. Giday M, Asfaw Z, Woldu Z. Ethnomedicinal study of plants used by Sheko ethnic group of Ethiopia. J Ethnopharmacol. 2010;132(1):75–85. doi:10.1016/j.jep.2010.07.046
15. Moges Y, Moges Y. Ethiopian Common Medicinal Plants: Their Parts and Uses in Traditional Medicine-Ecology and Quality Control. London, UK: IntechOpen; 2020.
16. Demie G, Negash M, Awas T. Ethnobotanical study of medicinal plants used by indigenous people in and around Dirre Sheikh Hussein heritage site of South-eastern Ethiopia. J Ethnopharmacol. 2018;220:87–93. doi:10.1016/j.jep.2018.03.033
17. Aschale Y, Wubetu M, Abebaw A, et al. A systematic review on traditional medicinal plants used for the treatment of viral and fungal infections in Ethiopia. J Exp Pharmacol. 2021;13:807. doi:10.2147/JEP.S316007
18. Tegen D, Dessie K, Damtie D. Candidate anti-COVID-19 medicinal plants from Ethiopia: a review of plants traditionally used to treat viral diseases. Evid Based Complement Alternat Med. 2021;2021:1–20. doi:10.1155/2021/6622410
19. Alinia-Ahandani E, Nazem H, Boghozian A, Alizadeh Z. Hepatitis and some effective herbs: a review. EAS J Parasitol Infect Dis. 2019;1(1):20–27.
20. Muluye AB, Ayicheh MW. Medicinal plants utilized for hepatic disorders in Ethiopian traditional medical practices: a review. Clin Phytosci. 2020;6(1):1–11. doi:10.1186/s40816-020-00195-8
21. Rajaratnam M, Prystupa A, Lachowska-Kotowska P, Zaluska W, Filip R. Herbal medicine for treatment and prevention of liver diseases. J Pre-Clin Clin Res. 2014;8(2):55–60.
22. Teklay A, Abera B, Giday M. An ethnobotanical study of medicinal plants used in Kilte Awulaelo District, Tigray Region of Ethiopia. J Ethnobiol Ethnomed. 2013;9(1):1–23. doi:10.1186/1746-4269-9-65
23. Lulekal E, Asfaw Z, Kelbessa E, et al. Ethnomedicinal study of plants used for human ailments in Ankober District, North Shewa Zone, Amhara region, Ethiopia. J Ethnobiol Ethnomed. 2013;9(1):1–13. doi:10.1186/1746-4269-9-63
24. Eshete MA, Molla EL. Cultural significance of medicinal plants in healing human ailments among Guji semi-pastoralist people, Suro Barguda District, Ethiopia. J Ethnobiol Ethnomed. 2021;17(1):1–18. doi:10.1186/s13002-021-00487-4
25. Pandey A, Tripathi S. Concept of standardization, extraction and pre phytochemical screening strategies for herbal drug. J Pharmacogn Phytochem. 2014;2(5):115–119.
26. Misonge OJ, Kamindu GN, Sabina W, Muita G. An ethnobotanical survey of plants used for the treatment and management of cancer in Embu County, Kenya. J Med Plants. 2019;7(4):39–46.
27. Siew -Y-Y, Yew H-C, Neo S-Y, et al. Evaluation of anti-proliferative activity of medicinal plants used in Asian Traditional Medicine to treat cancer. J Ethnopharmacol. 2019;235:75–87. doi:10.1016/j.jep.2018.12.040
28. Suleman S, Alemu T. A survey on utilization of ethnomedicinal plants in Nekemte town, East Wellega (Oromia), Ethiopia. J Herbs Spices Med Plants. 2012;18(1):34–57. doi:10.1080/10496475.2011.645188
29. Jima TT, Megersa M. Ethnobotanical study of medicinal plants used to treat human diseases in Berbere district, Bale zone of Oromia regional state, south east Ethiopia. Evid Based Complement Alternat Med. 2018;2018:1–16. doi:10.1155/2018/8602945
30. Begeno TA, Abose YM. Phytochemical investigation and characterization on the stem bark extract of Croton macrostachyus. Wounds. 2020;19:20.
31. Talema A. Review of Phytochemical Analysis of Selected Traditional Medicinal Plants in Ethiopia. Int J Homeopath Nat Med. 2020;6(2):23. doi:10.11648/j.ijhnm.20200602.13
32. Teklehaymanot T. Ethnobotanical study of knowledge and medicinal plants use by the people in Dek Island in Ethiopia. J Ethnopharmacol. 2009;124(1):69–78. doi:10.1016/j.jep.2009.04.005
33. Abera B. Medicinal plants used in traditional medicine by Oromo people, Ghimbi District, Southwest Ethiopia. J Ethnobiol Ethnomed. 2014;10(1):1–15. doi:10.1186/1746-4269-10-40
34. Devkota SR, Paudel KR, Sharma K, et al. Investigation of antioxidant and anti-inflammatory activity of roots of Rumex nepalensis. World J Pharm Pharm Sci. 2015;4(3):582–594.
35. Mosissa D, Atinafu H. Applied ethnobotany: people, medicinal plants use and conservation practices in Benishangul Gumuz Regional State of Ethiopia: the future cursed natural resource in the Region. Int J Pharma Sci. 2021;1(1):18–30.
36. Moshi MJ, Otieno DF, Mbabazi PK, et al. Ethnomedicine of the Kagera Region, north western Tanzania. Part 2: the medicinal plants used in Katoro Ward, Bukoba district. J Ethnobiol Ethnomed. 2010;6(1):1–5. doi:10.1186/1746-4269-6-19
37. Al-Fatimi M. Ethnobotanical survey of medicinal plants in central Abyan governorate, Yemen. J Ethnopharmacol. 2019;241:111973. doi:10.1016/j.jep.2019.111973
38. Tefera BN, Kim Y-D. Ethnobotanical study of medicinal plants in the Hawassa Zuria District, Sidama zone, Southern Ethiopia. J Ethnobiol Ethnomed. 2019;15(1):1–21. doi:10.1186/s13002-019-0302-7
39. Chekole G. Ethnobotanical study of medicinal plants used against human ailments in Gubalafto District, Northern Ethiopia. J Ethnobiol Ethnomed. 2017;13(1):1–29. doi:10.1186/s13002-017-0182-7
40. Asfaw A, Lulekal E, Bekele T, et al. Ethnobotanical investigation on medicinal plants traditionally used against human ailments in ensaro district, north Shewa zone, Amhara regional state, Ethiopia; 2021.
41. Sheikh DK, Dixit AK. Ethnomedicinal importance of some invasive plants of Chhattisgarh, India. Bull Pure Appl Sci Bot. 2018;37(2):58–66. doi:10.5958/2320-3196.2018.00009.5
42. Malik ZA, Bhat JA, Ballabha R, et al. Ethnomedicinal plants traditionally used in health care practices by inhabitants of Western Himalaya. J Ethnopharmacol. 2015;172:133–144. doi:10.1016/j.jep.2015.06.002
43. Getaneh S, Girma Z. An ethnobotanical study of medicinal plants in Debre Libanos Wereda, Central Ethiopia. Afr J Plant Sci. 2014;8(7):366–379. doi:10.5897/AJPS2013.1041
44. Birhane E, Aynekulu E, Mekuria W, Endale D. Management, use and ecology of medicinal plants in the degraded dry lands of Tigray, Northern Ethiopia. J Med Plants Res. 2011;5(3):308–319.
45. Gebrezgabiher G, Kalayou S, Sahle S. An ethno-veterinary survey of medicinal plants in woredas of Tigray region, Northern Ethiopia. Int J Biodivers Conserv. 2013;5(2):89–97.
46. Kewessa G, Abebe T, Demessie A. Indigenous knowledge on the use and management of medicinal trees and shrubs in Dale District, Sidama Zone, Southern Ethiopia. Ethnobot Res Appl. 2015;14:171–182. doi:10.17348/era.14.0.171-182
47. Regassa R, Bekele T, Megersa M. Ethnobotanical study of traditional medicinal plants used to treat human ailments by Halaba people, southern Ethiopia. J Med Plants Stud. 2017;5(4):36–47.
48. Fenetahun Y, Eshetu G, Worku A, Abdella T. A survey on medicinal plants used by traditional healers in Harari regional State, East Ethiopia. J Med Plants Stud. 2017;5(1):85–90.
49. Hosseinzadeh S, Jafarikukhdan A, Hosseini A, et al. The application of medicinal plants in traditional and modern medicine: a review of Thymus vulgaris. Int J Clin Med. 2015;6(09):635. doi:10.4236/ijcm.2015.69084
50. Kainsa S, Kumar P, Rani P. Medicinal plants of Asian origin having anticancer potential: short review. Asian J Biomed Pharm Sci. 2012;2(10):1–11.
51. Siddiqui MH, Alamri SA, Al-Whaibi MH, et al. A mini-review of anti-hepatitis B virus activity of medicinal plants. Biotechnol Biotechnol Equip. 2017;31(1):9–15.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.