Back to Journals » International Journal of General Medicine » Volume 19
Medication Use and Guideline Adherence in Inflammatory Bowel Disease Management: A Retrospective Study from a Tertiary Care Hospital in Pakistan (2019–2024)
Authors Yasin H, Jamshed S ![]() , Balquis F
, Balquis F ![]() , Ibrar F, Chaudhry SR, Ahmad J, Mohamad Ibrahim MI
, Ibrar F, Chaudhry SR, Ahmad J, Mohamad Ibrahim MI ![]() , Sivanandy P
, Sivanandy P ![]() , Iqbal A, Syed W
, Iqbal A, Syed W ![]() , Alharbi BS
, Alharbi BS ![]() , Aljabri MM
, Aljabri MM ![]()
Received 28 September 2025
Accepted for publication 13 May 2026
Published 26 May 2026 Volume 2026:19 570992
DOI https://doi.org/10.2147/IJGM.S570992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Xudong Zhu
Hamad Yasin,1 Shazia Jamshed,1,2 Fatima Balquis,1 Fatima Ibrar,3 Shafqat Rasul Chaudhry,4 Jahanzaib Ahmad,5 Mohamad Izham Mohamad Ibrahim,6 Palanisamy Sivanandy,2 Ayesha Iqbal,7,8 Wajid Syed,9 Bandar S Alharbi,10 Majed M Aljabri10
1Pharmacy Practice Department, Shifa College of Pharmaceutical Sciences, Shifa Tameer-E-Millat University, Islamabad, Pakistan; 2Department of Pharmacy Practice, School of Pharmacy, IMU (Former International Medical University), Kuala Lumpur, Malaysia; 3Departments of Gastroenterology Hepatology, Surgery and Pathology, Shifa International Hospital, Islamabad, Pakistan; 4II-TECH College of Pharmacy, International Institute of Technology, Culture & Health Sciences (II-TECH), Gujranwala, Punjab, Pakistan; 5Sandeman Provincial Hospital Quetta, Quetta, Balochistan, Pakistan; 6Clinical Pharmacy and Practice, College of Pharmacy, QU Health, Qatar University, Doha, Qatar; 7Department of Pharmacy Practice and Policy, University of Nottingham, University Park Campus, Nottingham, NG72RD, UK; 8Office of Lifelong Learning and the Physician Learning Program, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB, T6G1C9, Canada; 9Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, 11451, Saudi Arabia; 10Department of Community and Psychiatric Mental Health Nursing, College of Nursing, King Saud University, Riyadh, 12372, Saudi Arabia
Correspondence: Wajid Syed, Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, 11451, Saudi Arabia, Email [email protected]
Background: Inflammatory bowel disease (IBD) remains understudied in Pakistan. This retrospective observational study assessed the management of IBD patients at Shifa International Hospital, Islamabad, from January 2019 to June 2024.
Methods: Adherence to UK NICE 2019 guidelines (NG129 for CD, NG130 for UC) was evaluated. Data from 167 adult IBD patients (from initial 238 identified; 141 ulcerative colitis, 26 Crohn’s disease) were extracted from electronic medical records after excluding inactive cases (n = 60), paediatric patients (n = 7), pregnant women (n = 3), and unconfirmed diagnoses (n = 1). Demographics, medications, comorbidities, surgeries, and diagnostic findings were analysed.
Results: Steroids were administered to 54.5% of patients (52.7% UC, 1.8% CD), aminosalicylates to 53.9% (50.3% UC, 3.6% CD), and immunosuppressants to 43.7% (40.2% UC, 3.5% CD). Discharge medications included steroids (46.1%), aminosalicylates (49.1%), and immunosuppressants (31.1%). Only 3/9 UC and 5/9 CD guideline recommendations were followed. Biologic use (anti-TNF) was low (8.9%), and 18% underwent surgery (total proctocolectomy most common). Diabetes (31%) and hypertension (28%) were prevalent comorbidities. Abdominal pain (52%) and diarrhea (46%) were frequent complaints. Colonoscopy (43%) and biopsies (20.4%) were key diagnostic tools. Histopathology revealed mild inflammation (29.4%) and moderate-severe inflammation (17.4%).
Conclusion: IBD management showed significant deviation from international guidelines, particularly regarding biologic utilization (8.9%) and surgical rates (18%). These findings highlight urgent need for resource-stratified treatment protocols and enhanced clinical training to bridge the gap between evidence-based recommendations and real-world practice in resource limited settings.
Keywords: inflammatory bowel disease, abdominal pain steroids, histopathology, inflammation
Introduction
A group of disorders that involve the gastrointestinal tract (GIT) becoming inflamed is known as inflammatory bowel disease (IBD).1 Relapsing and remitting inflammation of the gastrointestinal tract is what distinguishes IBD from other conditions.2 IBD can lead to disability and have a significant impact on the quality of life, with significant health problems.3 Moreover, patient may encounter social and professional obstacles that impede their work and recreational pursuits, leading to decreased sexual fulfillment compared to general population.4 Commensal microflora and the mucosal-associated immune system interact in an unregulated fashion, leading to IBD in patients who have a genetic predisposition and have been exposed to risk factors in their environment.5 IBD is characterized by ulcerative colitis (UC) and Crohn’s disease (CD) as the most common forms.6 While ulcerative colitis and Crohn’s disease represent the primary IBD phenotypes, IBD-unclassified (IBD-U) accounts for approximately 10–15% of cases, particularly in children, where definitive classification may be challenging. Our study focused on definitively diagnosed UC and CD cases, as IBD-U cases were not systematically classified in our patient records during the study period. Despite their distinct features in terms of inflammation, extent and location, both CD and UC significantly impact quality of life, particularly in young patients who face long-term disease burden during their most productive years.7 CD can have an impact on the entire digestive tract, from the mouth to the perianal region. Discontinuous and segmental injuries that affect all layers of the intestine (transmural inflammation) are the characteristics of the CD inflammatory process.8 The symptoms of CD vary, but they typically involve abdominal pain, weight loss, and chronic diarrhea.9 UC has the characteristic of diffuse inflammation of the colon restricted to the mucosa, which usually affects the rectum and reveals a proximal extension with a symmetrical and continuous pattern.10 Bloody diarrhea, rectal bleeding, urgency of the rectum are the symptoms that occur most often but fecal incontinence, bowel spasm and abdominal spasm are also common complaints among UC patients.4 IBD may present with extraintestinal manifestations including fever, weight loss, arthritis, mucocutaneous lesions like oral ulcers, erythema nodosum, pyoderma gangrenosum and ophthalmic complications like iritis and uveitis.2
In the past, IBD was considered a disease from the West. According to a 2012 systematic review,11 Europe had the highest annual incidence of IBD (UC: 24.3 per 100,000 person-years, CD: 12.7 per 100,000 person-years), followed by North America (UC: 19.2 per 100,000 person-years, CD: 20.2 per 100,000 person-years) and Asia plus Middle East (UC: 6.3 per 100,000 person-years, CD: 5.0 per 100,000 person-years). The incidence rate of IBD has remained stable or increased steadily in Western countries,12 but there has been a rapid increase among Asian countries.2,13 In Asia, there is a rising trend of IBD incidence and prevalence for the past two decades.14 IBD has historically been regarded as a rare disease in the Asia-Pacific area, however, ulcerative colitis and Crohn’s disease appear to be becoming more common.15
The lack of epidemiological studies is evident from the published literature but the incidence and prevalence of IBD in Asia have increased over time and Asia as a continent has the most IBD patients in the world.16 IBD was once considered a rare disease in the Asia-Pacific region, but within more than a decade Crohn’s disease and ulcerative colitis are becoming increasingly common in Asian populations.17 Although there is a lack of epidemiological studies on IBD from Pakistan,13 there is growing evidence to suggest rising incidence of IBD and therefore, recognizing the symptoms of IBD and diagnostic pathways in establishing the initial diagnosis in the clinical setting are challenging aspects.18
The present increasing outlook in Pakistani population necessitates the exploration of different therapeutic modalities in IBD patients. In the light of this, it was pertinent to design this exploratory research to generate baseline data in the current timeframe. Furthermore, Shifa International Hospital (SIH) is one of Islamabad’s most well-known tertiary care facilities. Therefore, in order to determine the degree to which standardized clinical practice guidelines were adhered to, the current study compared the treatment administered to IBD patients in SIH with that of the clinical practice guidelines to know that to which extent standardized clinical practice guidelines were followed. It provided an indicator about performance of doctors in SIH and whether or not they were adhering to the guidelines.
Currently, no Pakistan-specific or South Asian regional clinical practice guidelines for IBD management exist. In the absence of local guidelines, the management of IBD patients in current study was compared with the May 2019 updated version of the National Institute for Health and Care Excellence (NICE) guidelines,19 and therefore used NICE guidelines 129 (NG129) for Crohn’s disease20 and NICE guidelines 130 (NG130) for ulcerative colitis.21 Since for the study the data collection was started in 2019, so the NICE 2019 guidelines were applied. This study aimed to examine IBD management practices at a tertiary care hospital in Pakistan by analyzing treatment approaches, evaluating compliance with clinical guidelines, investigating biologic therapy utilization, and assessing indications for surgical interventions. The findings provide valuable insights into current clinical practices and their alignment with international standards of care for inflammatory bowel disease.
Adherence to evidence-based clinical practice guidelines is critical for optimizing patient outcomes, preventing disease complications such as steroid dependence and surgical intervention, and reducing healthcare costs associated with suboptimal management. However, significant gaps exist in Pakistan-specific data regarding IBD treatment patterns and guideline concordance. The scarcity of published evidence from low- and middle-income countries (LMICs) limits our understanding of real-world management challenges, resource constraints, and barriers to implementing international treatment recommendations in resource-limited settings.
Methodology
Operational Definition
Guideline Adherence Assessment
Every recommendation made by the guidelines was compared to actual patient care. “Followed” denotes that every eligible patient received the suggested treatment; “Not followed” denotes that no eligible patient received it; and “Partially followed” denotes that some but not all eligible patients received it. Although we acknowledge the inability to fully account for access hurdles, insurance constraints, or patient choices from retrospective data, eligibility was established based on reported clinical features. Every recommendation made by the guidelines was compared to actual patient care. “Followed” denotes that every eligible patient received the suggested treatment; “Not followed” denotes that no eligible patient received it; and “Partially followed” denotes that some but not all eligible patients received it.
In the previously published IBD literature, generally guidelines were followed, however, it was not made clear that which specific clinical practice guideline was followed to manage IBD patients and to what extent it was followed.
Inactive Patients
It is imperative to report that patients who did not visit SIH in the last three years were considered inactive, and their medical records were sent to a warehouse located in Fateh Jang. These records were not accessible for research purpose. These records can only be accessed if the treating physician requested the record as resuming of the treatment was not possible without patient’s history.
Date of Diagnosis
The first endoscopic or radiological investigation in which the patient showed signs of IBD was referred to as date of diagnosis.
Study Design
It was a retrospective observational study design.
Study Setting
The study was conducted at a private tertiary care hospital (Shifa International Hospital (SIH)) in Islamabad, Pakistan.
Study Population
All the patients admitted in Shifa International Hospital (SIH) having confirmed diagnosis of ulcerative colitis (UC) or Crohn’s disease (CD) considered to be the study population in current research.
Sampling
Retrospective medical record review (RMRR) of IBD patients.
Sample Size
Sample size was determined by the availability of eligible IBD patients meeting inclusion criteria during the study period (January 2019 to June 2024) at our single tertiary care center. This represents a comprehensive census of all accessible, confirmed IBD cases during this timeframe. There was n = 238 patients initially, n = 201 of whom were UC and n = 37 of whom were CD. The sample size for the UC was n = 141; n = 60 were eliminated because n = 50 were inactive and n = 10 were excluded in accordance with the exclusion criteria. The sample size for the CD was n = 26, of which n = 11 were eliminated because n = 10 were inactive and n = 1 was rejected in accordance with the exclusion criteria. There were n = 167 people in the IBD sample overall (Figure 1).
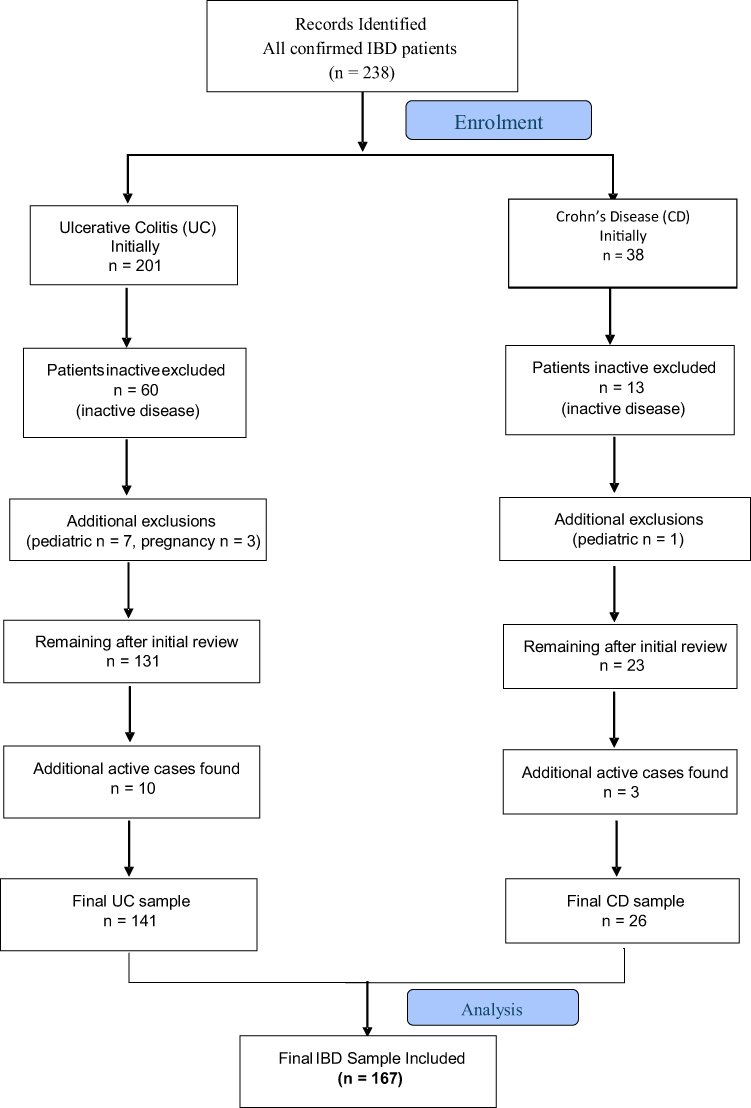 |
Figure 1 Consort Flow Chart for Sample Size. |
For Crohn’s Disease
Initially, the sample size was n = 37, out of which n = 13 patients were inactive and one patient was excluded as it came under the category of exclusion criteria (pediatric) and therefore, sample size seems to be reduced to n = 23. Again, the records of inactive patients were checked, as a result, n = 3 more patients came out to be active. Therefore, the final sample size for CD was reported to be n = 26 patients.
For Ulcerative Colitis
Initially, the total sample size was n = 201, out of which n = 60 patients were inactive and n = 10 patients were excluded as they came under the criteria of pediatric (n = 7) and pregnancy (n = 3), reducing the sample size to n = 131. On checking back again the records of inactive patients, n = 10 more patients found to be active. The final sample size for UC came out to be n = 141 patients.
Inclusion Criteria
All the patients who visited the gastroenterology department at Shifa international hospital and were diagnosed with either Crohn’s disease (CD) or ulcerative colitis between the date from January 2019 to June 2024 and in the age group of 18 years and above were identified and included in the study.
Exclusion Criteria
Pediatric patients (<18 years) were excluded because IBD in children differs in presentation, treatment strategies, and prognosis, and managing these cases typically follows separate guidelines, such as the ECCO-ESPGHAN pediatric IBD recommendations. Similarly, pregnant women were excluded due to the need for pregnancy-specific modifications to IBD therapy, medication contraindications, and unique management considerations. These exclusions help us focus on standard adult IBD care, providing a clearer picture of typical treatment patterns without the confounding influence of populations that require specialized approaches.
Data Collection Procedure
The data was collected from the electronic medical record (EMR) of patients who were hospitalized for the treatment of IBD from January 2019 to June 2024. The patient demographics (gender, age, weight, BMI, marital status, blood group, province, economic status, primary diagnosis, secondary diagnosis/co-morbidities), emergency complaints, medications used, procedure performed, severity, lesion polyps, family history, allergies, microscopic description/biopsies, abnormal laboratory findings were recorded. After complete information, primary and secondary endpoints were measured.
Disease location was extracted from endoscopy reports and classified according to anatomical distribution. For UC: proctitis (rectum only), left-sided colitis (up to splenic flexure), extensive colitis (beyond splenic flexure), and pancolitis (entire colon). For CD: ileal, colonic, ileocolonic, and upper GI involvement were documented when specified in diagnostic reports. Missing data like patients with incomplete diagnostic confirmation were excluded; For secondary variables (economic status, blood group), missing data were reported as “unknown” and their frequency documented in results; When severity scales or specific clinical indicators were not documented, this was explicitly stated in results to avoid misclassification.
Data Analysis Procedure and Analytical Tool
Initially, data was collected on excel file and then transformed into statistical package for social sciences (SPSS) file for analysis. The SPSS version 2023 was used for analysis. Descriptive statistics were applied. The p-value was greater than 0.05 and the histogram showed symmetrical distribution indicating that the data was normally distributed.
Duration of Study
The data from January 2019 to June 2024 was included in the study and was accessed from July 2024 to August 2024.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and approval for the study was taken from institutional review board (IRB) and ethics committee (EC) of Shifa International Hospital and Shifa Tameer-e-Millat University. The approval number was IRB # 074–024.
Results
Demographics of IBD Patients
The gender distribution of CD, UC and overall IBD patients from the percentage point of view was almost equal in each case, which is 58% male and 42% female. The mean (±SD) age of IBD patients was 45.215 (±17.64) years [(for CD: 40.730 (±16.88) years with a range of 18 to 71 years; for UC: 46.042 (±17.70) years with a range of 18 to 84 years)]. About 47% (n = 78), 29% (n = 48) and 24% (n = 41) of IBD patients presented between 18 and 40, 41 to 60 and over 60 years of age, respectively. The mean (±SD) weight of IBD patients was 65.74 (±14.16) kg [(for CD: 61.92 (±10.85) kg; for UC: 66.43 (±14.61) kg)]. The mean (±SD) BMI of IBD patients was 23.86 (±5.11) kg/m2 [(for CD: 22.86 (±4) kg/m2 with a range of 15.2 to 33 kg/m2; for UC: 24.04 (±5.28) kg/m2 with a range of 14.3 to 48 kg/m2)]. From the marital status perspective, 138 IBD patients were married and 29 was unmarried. Almost 50% of the IBD patients were from Punjab (n = 79), followed by Islamabad (n = 37), KPK (n = 29), AJK (n = 10) and Afghanistan (n = 9). The blood group (for those who were suffering from anemia) and economical status was mentioned for few IBD patients (Table 1).
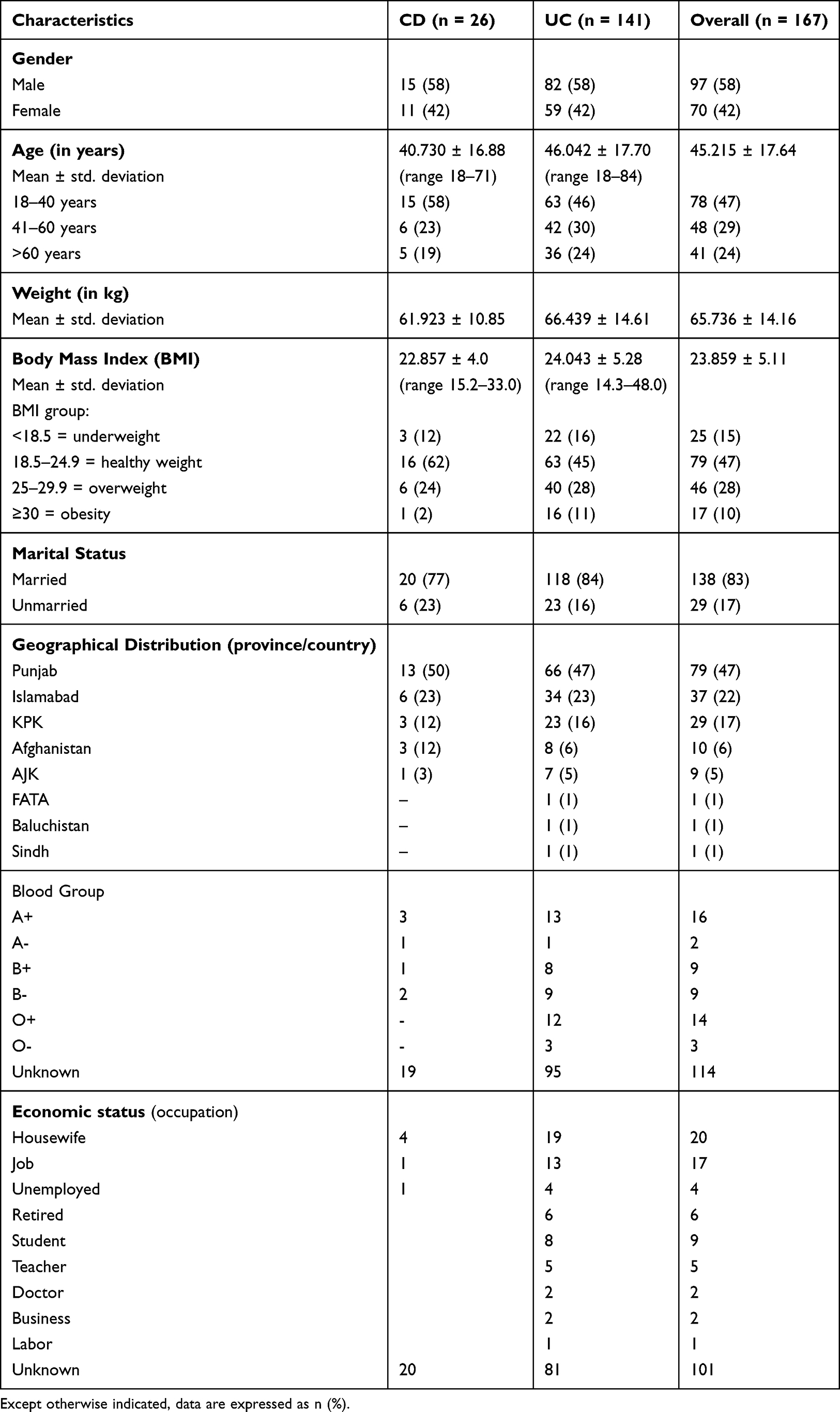 |
Table 1 Demographics of Patients with Inflammatory Bowel Disease (n = 167) |
In UC (n = 141), disease extent was documented in 78% of cases (n = 110), with pancolitis in 38% (n = 42), extensive colitis in 28% (n = 31), left-sided colitis in 22% (n = 24), and proctitis/proctosigmoiditis in 12% (n = 13); the location was unspecified in 22% (n = 31). In CD (n = 26), disease location was recorded in 69% of cases (n = 18), including ileocolonic involvement in 44% (n = 8), colonic in 28% (n = 5), ileal in 22% (n = 4), and upper GI involvement in 6% (n = 1); 31% (n = 8) had unspecified location.
Therapeutic Categories Used in IBD Patients
Medication therapeutic categories (classes) in IBD patients were divided into two types: hospitalized (inpatient) drugs and discharge medications. Medication used for IBD patients during their hospital stay was referred to as hospitalized (inpatient) medication, while medication used for IBD patients upon their exit from the hospital was referred to as discharge medication. They were also further divided into two categories: UC and CD discharge drugs and UC and CD inpatient medications.
Hospitalized Medications in IBD Patients
Steroids were given to 88 UC and 3 CD patients in various forms (prednisolone, hydrocortisone). Mesalamine (tablet, enema, suppository) was used in 81 UC and 6 CD patients. Dietary supplements, including folic acid, were provided to 29 UC and 3 CD patients. Immunosuppressants, mainly azathioprine, were prescribed to 67 UC and 6 CD patients. Antibiotics (fluoroquinolones, glycopeptides, carbapenems, etc.) were administered to 65 UC and 9 CD patients. Proton pump inhibitors and H2 blockers were used for both groups. Other treatments included laxatives, controlled drugs, analgesics, gastro prokinetics, antispasmodics, and antiemetics (Table 2).
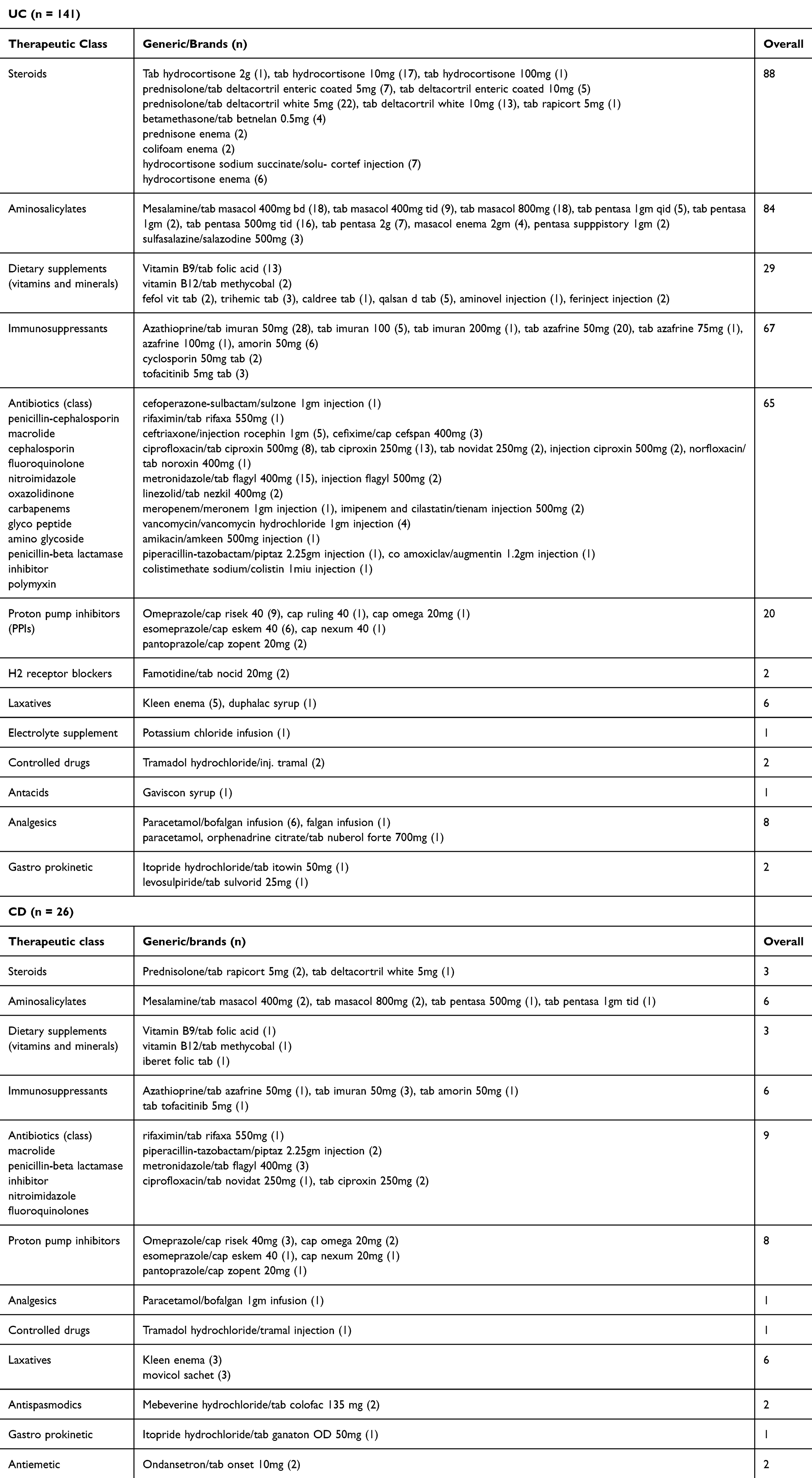 |
Table 2 Hospitalized Medications Used in IBD Patients |
Discharge Medications in IBD Patients
Steroids were given to 66 UC and 11 CD patients in various forms (hydrocortisone, prednisolone, dexamethasone, betamethasone). Mesalamine (tablet, enema) was used by 74 UC and 8 CD patients. A few UC patients also received sulfasalazine. Dietary supplements, including folic acid and various multivitamins, were given to 32 UC and 5 CD patients. Immunosuppressants like azathioprine were prescribed to 50 UC and 2 CD patients. Antibiotics (fluoroquinolones, macrolides, glycopeptides, etc.) were used in 57 UC and 6 CD patients. Proton pump inhibitors and H2 blockers were used for both UC and CD. Other treatments included laxatives, controlled medications, analgesics, gastro prokinetics, antispasmodics, and antiemetics (Table 3).
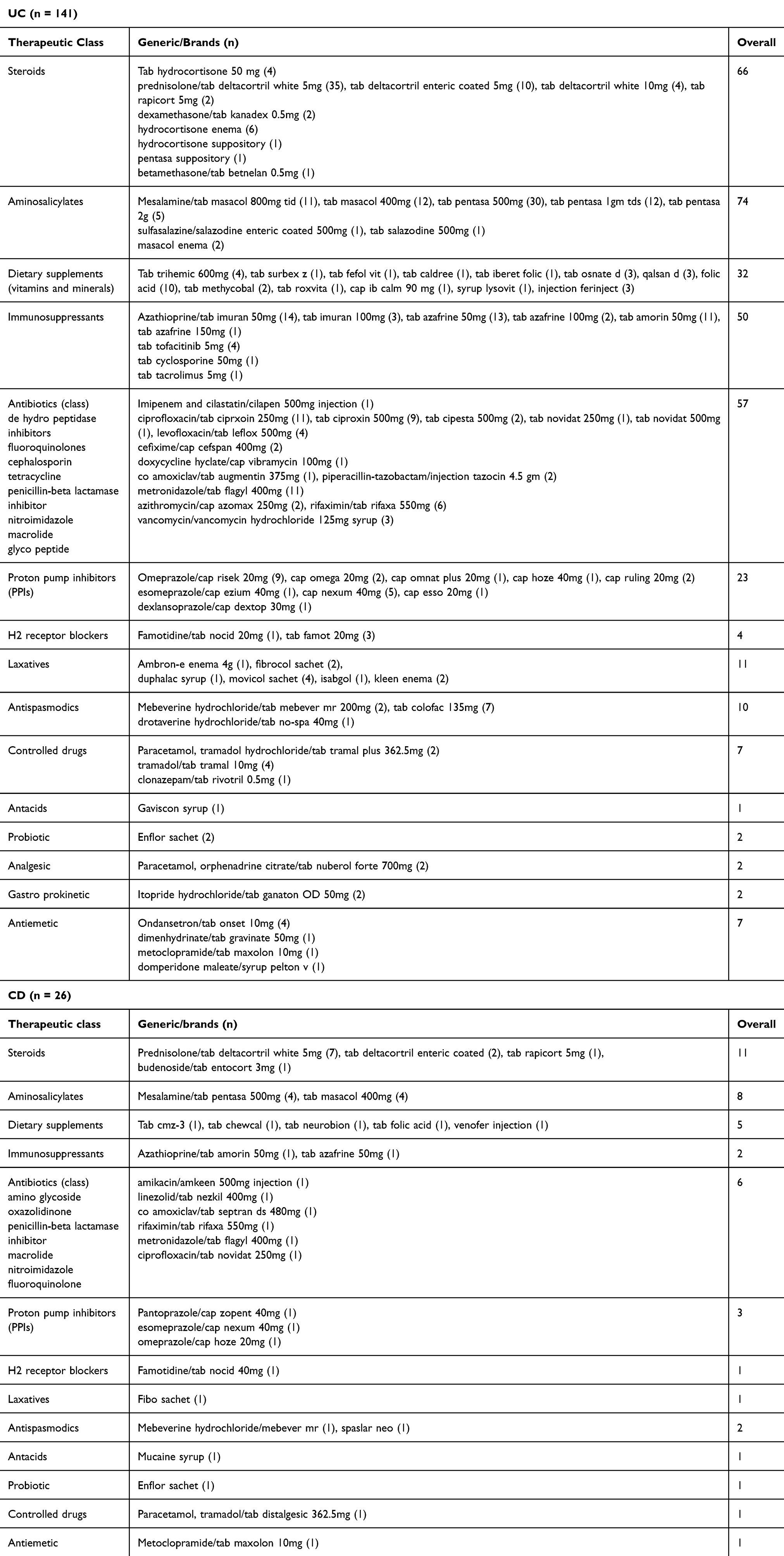 |
Table 3 Discharge Medications Used in IBD Patients |
Clinical Practice Guidelines and Management of IBD Patients
The management of IBD patients in current study was compared with the May 2019 updated version of the National Institute for Health and Care Excellence (NICE) guidelines and therefore used NICE guidelines 129 (NG129) for Crohn’s disease and NICE guidelines 130 (NG130) for ulcerative colitis.
Summary of the NG129 and CD Patient’s Management
NG129 was summed up as In managing Crohn’s disease, conventional glucocorticoids such as prednisolone, methylprednisolone, or intravenous hydrocortisone are recommended as monotherapy for up to 12 months to induce remission. If glucocorticoids are contraindicated or not tolerated, aminosalicylates may be considered, though they are less effective but have fewer side effects. Budesonide and aminosalicylates should not be used for severe cases or acute exacerbations. Immunosuppressants like azathioprine, mercaptopurine, and methotrexate are not recommended as monotherapy for inducing remission, and TPMT activity should be tested prior to use. For severely active Crohn’s disease, biologics such as infliximab and adalimumab may be used based on clinical and investigative findings, given as a planned course up to treatment failure or 12 months. To maintain remission, azathioprine or mercaptopurine can be continued if previously used with steroids or budesonide, or considered in those not previously treated, especially with poor prognostic indicators. Glucocorticoids and budesonide are not advised for maintenance therapy. Following complete macroscopic resection of ileocolonic Crohn’s within three months, azathioprine with up to three months of postoperative metronidazole may be considered, but biologics should not be used to maintain remission post-surgery.20
The table’s rows were numbered in accordance with the guidelines’ numerical points to indicate the degree to which the recommendations for the treatment of CD patients were followed. Guidelines were used to analyse the management, and the results were divided into three categories: partially followed, not followed and followed. Five of the guidelines recommendations were followed, three were not followed and one was partially followed. (Table 4)
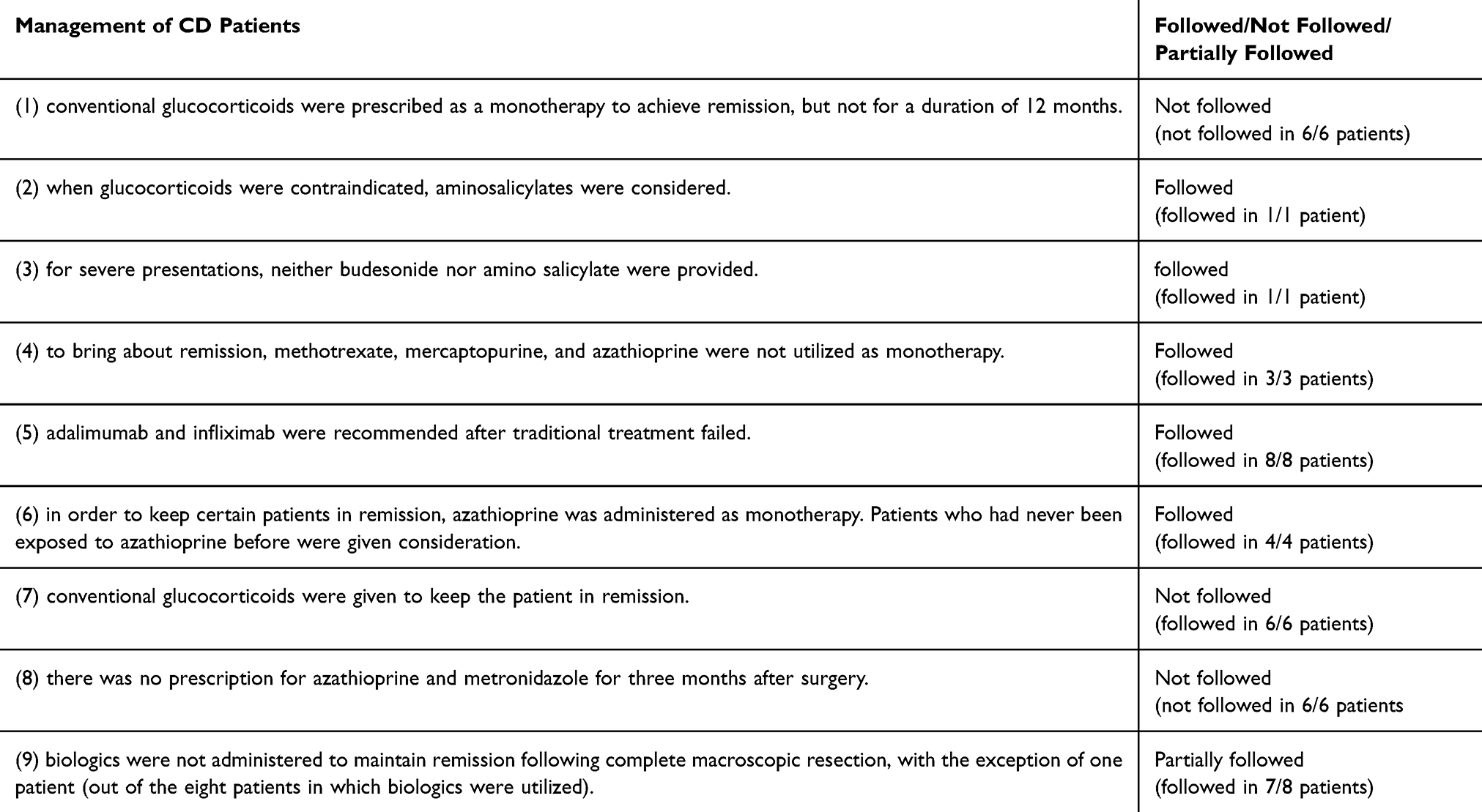 |
Table 4 Management of CD Patients in Accordance with NICE Guidelines 129 |
Summary of the NG130 and UC Patient’s Management
NG130 was summed up as for mild-to-moderate first presentations or inflammatory exacerbations of proctitis or proctosigmoiditis, topical aminosalicylates are the first-line treatment to induce remission. If remission is not achieved within 4 weeks, consider adding a high-dose oral amino salicylate and a short course of topical corticosteroids. If still ineffective, discontinue topical treatments and switch to a high-dose oral amino salicylate with a short course of oral corticosteroids. For those intolerant to aminosalicylates, a time-limited course of oral corticosteroids may be used. In cases where intravenous corticosteroids are not tolerated or contraindicated, intravenous ciclosporin or surgery may be considered. To maintain remission after a mild-to-moderate exacerbation, options include topical aminosalicylates alone, oral plus topical aminosalicylates, or oral aminosalicylates alone. For patients experiencing two or more corticosteroid-treated exacerbations in 12 months, oral azathioprine or mercaptopurine may be considered for maintenance. Acute severe ulcerative colitis is typically managed with intravenous corticosteroids to induce remission, while infliximab is reserved for severe cases where ciclosporin is contraindicated or inappropriate.21
To show the extent to which the suggestions for the treatment of UC patients were adhered to, the rows in the table were numbered according to the numerical points in the guidelines. Three categories were created from the results of the analysis of the management using guidelines: partially followed, not followed, and followed. One of the guidelines recommendations was partially followed, five were not followed, and three of the recommendations were followed. (Table 5)
 |
Table 5 Management of UC Patients in Accordance with NICE Guidelines 130 |
Biologics and Reasons Which Necessitates Biologic Therapies in IBD Patients
Out of 167 IBD patients (15 treated with biologics, 152 not), 7 UC and 8 CD patients received biologic therapy. All UC patients were treated with infliximab—five without clear indication, one due to treatment failure, and one due to disease severity. Among CD patients, three biologics were used: infliximab (5 patients, no reasons given), adalimumab (2 patients—one unspecified, one post-surgical), and vedolizumab (1 patient). Of the remaining 152 patients, 134 UC and 18 CD did not receive biologics. Biologic use ratio: 1 per 3.25 CD patients, 1 per 20.1 UC patients (Table 6).
 |
Table 6 Biologics and Reasons for Biologic Therapies in IBD Patients (n = 167) |
Surgery and Reasons Which Necessitates Surgery in IBD Patients
Out of 30 IBD patients who underwent surgery (6 CD, 24 UC), various procedures were performed. For UC patients: 14 had total proctocolectomy (9 with reasons like treatment failure, bleeding, and severe illness), 7 had laparoscopic subtotal hemicolectomy, 2 had pan proctocolectomy, and 1 had right hemicolectomy. For CD patients: 3 had right hemicolectomy, 1 had laparoscopic subtotal hemicolectomy, 1 had total proctocolectomy with j pouch, and 1 had jejunal resection. The surgical rate was 1 per 4.3 CD patients and 1 per 5.8 UC patients (Table 7).
 |
Table 7 Surgery Type and Reasons for Surgical Procedure in IBD Patients (n = 167) |
Comorbidities in Patients with IBD
About 31% (n = 52) of IBD patients reported having diabetes mellitus as their most prevalent comorbidity, followed by hypertension in about 28% (n = 46) of patients. Then, comorbidities were categorized based on body systems. For instance, comorbidities related to the cardiovascular and digestive systems affected roughly 33% (n = 20) of the patients in each case. Urinary system comorbidities followed, at 15% (n = 25), respiratory system 13% (n = 21), haematology 8.5% (n = 14), and carcinomas 7.8% (n = 13), which were followed by comorbidities related to the central nervous system and arthritis, 5.4% (n = 9) in each case (Table 8).
 |
Table 8 Comorbidities in Patients with Inflammatory Bowel Disease (n = 167) |
Discussion
This study addresses a critical evidence gap in LMIC IBD management by providing the first comprehensive analysis of medication utilization patterns and guideline adherence from Pakistan within this timeframe. While international studies document similar treatment patterns, our findings uniquely quantify the extent of deviation from evidence-based guidelines in a resource-constrained setting, revealing that only 3/9 UC and 5/9 CD NICE recommendations were followed. This systematic documentation of guideline non-adherence, coupled with identification of specific barriers (low biologic use: 8.9%; high steroid exposure: 54.5%), provides actionable data for policy development and resource allocation in similar healthcare settings.
The current study presented data on the management of IBD patients at a tertiary care facility in Islamabad, Pakistan, for the first time in current time frame. It was a retrospective analysis of 167 IBD cases. There were 167 people with IBD overall (UC 84.43% and CD 15.57%). The sample size of UC and CD patients differed significantly; (UC/CD ratio, 5.42:1). It showed a significant predominance of UC over CD, which was similar to previously reported data from an Egyptian tertiary care hospital (200 patients – 88% UC and 12% CD);22 but differs from the research conducted in north-central region of Saudi Arabia where there was a limited predominance of CD over UC (257 patients – CD 51% and UC 49%)23 and also differs from a study in Kuwait which showed a significant predominance of CD over UC (130 patients – UC 34% and CD 66%).24 Males were reported to be predominated in current study; there were 58% males (n = 97) and 42% females (n = 70) (male/female ratio: 1.40:1). A Malaysian tertiary care hospital reported research likewise observed a male majority (61.5% vs. 38.5%).2 The mean (±SD) age in this study was 45.21 (±17.64) years, which was nearly identical to the mean age (44 ± 15.1 years) found in a Chinese retrospective review.15
In the current research, the mean (±SD) BMI for CD patients was 22.85 (±4.0) kg/m,2 whereas the mean (±SD) BMI for UC patients was 24.04 (±5.28) kg/m2. Of all the IBD patients, 47% were normal weight, 28% were overweight, 15% were underweight, and 10% were obese. A Brazilian study reported higher BMI for both CD (27.5 ± 3.7) and UC (25.4 ± 7.5).25 An Iranian study revealed that about 60% IBD patients had normal weight.26 Additionally, the current study presented information on the IBD patients’ occupation, blood group, regional distribution (almost half of the patients were from Punjab), and marital status (n = 138 married, n = 29 unmarried). The blood group was mentioned by those with anaemia (as they required blood transfusion) and the information about employment was provided by the n = 66 patients.
The current study was distinct in that it classified the drugs into hospitalized and discharged medications and also specifying dosage forms, strengths and brands of the drugs, whereas prior IBD literature mentioned medications without categorizing it. About 54.5% (n = 91) IBD patients (UC 52.7% and CD 1.8%) received steroid preparations (hydrocortisone, prednisolone, betamethasone), 53.9% (n = 90) IBD patients (UC 50.3% and CD 3.6%) received aminosalicylates (mesalamine, sulfasalazine) and 43.7% (n = 73) IBD patients (UC 40.2% and CD 3.5%) received immunosuppressants (azathioprine, cyclosporine, tofacitinib) to manage the disease in hospital. About 46.1% (n = 74) and 20.6% (n = 32) hospitalized IBD patients received different antibiotics and dietary supplements, respectively, according to their requirements. Among the discharged medications, about 46.1% (n = 77) IBD (39.5% UC and 6.6% CD) patients were treated with steroids, 49.1% (n = 82) IBD patients (44.3% UC and 4.8% CD) with aminosalicylates, 31.1% (n = 52) IBD patients (29.9% UC and 1.2% CD) received immunosuppressants as discharged medications. About 22.2% (n = 37) and 37.7% (n = 63) IBD patients were treated with dietary supplements and antibiotics, respectively, according to their requirements. Other discharged and hospitalized drug classes that were used, in few patients for management of IBD, were PPIs, laxatives, antispasmodics, antacids, controlled drugs and antiemetics. A study in Bahrain reported that 5-ASA (90%), azathioprine (75%) and steroids (67%) were the most common drug treatments.1 In a study, at a Malaysian tertiary care hospital, majority of patients remained on 5-ASA (94%) and immunosuppressants (26%).2
The current study specifically observed the management of IBD patients against the international clinical practice guidelines. For this purpose, UK (NICE 2019 revisions) guidelines were selected, separately for CD (NG129) and UC (NG130). Only three of the nine suggestions in the guidelines were followed for UC, whereas five of the nine guidelines recommendations were followed for CD. Guidelines’ recommendation was referred to as followed if every patient complied with it (where necessary). A recommendation of the guidelines was considered not followed if it was not followed by every patient. A recommendation of the guideline was considered partially followed if it was followed by some patients and not by others. In the previously published IBD literature, generally guidelines were followed, however, it was not made clear that which specific clinical practice guideline was followed to manage IBD patients and to what extent it was followed. The high steroid exposure rate (54.5% inpatient, 46.1% discharge) without corresponding increase in steroid-sparing agents raises significant clinical concerns. Prolonged corticosteroid use is associated with serious adverse events including osteoporosis, avascular necrosis, opportunistic infections, diabetes, and increased mortality risk. The low biologic utilization (8.9%) suggests delayed treatment escalation, which may result in increased complications, higher hospitalization rates, and ultimately greater healthcare burden. Steroid-dependent patients who do not receive timely immunosuppressive or biologic therapy face substantially elevated risks of surgical intervention and disease-related complications, as evidenced by our 18% surgical rate.
The current study specifically focused on biologic (anti-TNF) therapies and surgeries performed for the management of IBD patients and the factors which necessitate biologic therapies and surgeries. Both surgery and biologic were quiet low in current study. In recent years, an increase in the use of immunosuppressants and biologics for IBD has been observed to delay the need for surgery and slow the progression of disease.27 In general, studies have revealed that around one third to one half of patients do not respond to anti-tumor necrosis factor (anti-TNF) treatments and when the first one fails, a second biologic is frequently prescribed.28 Half of patients who quit their first biologic treatment do not return to or switch to another therapy.29 Despite the success of many patients in remission, there are others who may discontinue biologic treatment due to side effects or lack of efficacy.30
About 8.9% (n = 15) IBD patients (4.2% UC and 4.7% CD) received anti-TNF (mainly infliximab). A Saudi Arabian study reported that 33.3% IBD patients were on anti-TNF (almost four times the current study).23 The factors which necessitate biologics were mentioned for few patients. Surgeries were performed in about 18% (30) of IBD patients (14.5% UC and CD 3.5%). The most common surgery was total proctocolectomy and j pouch in 15 out of 30 patients. A study at Aga Khan University Hospital, Karachi, Pakistan, reported that 47 patients underwent surgical procedure, but records of 36 were available. About 75% underwent elective surgery and 25% underwent surgical procedure in emergency. Most commonly performed procedure was colectomy in 11 patients. Most common indication was resistant medical therapy.31 A study in Bahrain reported that most common surgical intervention was colectomy.1 A study in KSA reported that overall rate of surgery (18%) was almost equal to the current study with opposite rates (1.2% UC and 16.8% CD).23 The reasons for surgery were mentioned for few patients.
Among the IBD patients, DM was the most comorbidity occurring in 31% (n = 52) and hypertension in 28% (n = 46) of cases. Comorbidities of the respiratory, cardiovascular and digestive systems were also present in IBD patients. An Iranian study reported that 16.1% IBD patients were hypertensive (lower than current study), 6.4% IBD patients had rheumatoid arthritis (close to current study, which was 5.4%), DM in 15.7% IBD patients (half than current study).26
In the current study, the most common emergency complaint among the IBD patients was abdominal pain (52%) with diarrhea following closely behind (46%). An Indian study revealed that diarrhoea was found to be most common complaint followed by abdominal pain and weight loss.32 The most common diagnostic procedure among the IBD patients was colonoscopy in 43% (35.9% UC and 7.1% CD) patients. In about 19% (n = 32) IBD patients, it was not clear that which diagnostic procedure was used to diagnose IBD. Different type of biopsy examinations was also performed for diagnosis in about 20.4% (34) IBD patients, among them colon biopsy was performed in 11 patients, followed by rectum and gastric biopsy, 6 in each case. In different biopsy types, different abnormalities (inflammation, crypt abscess, surface ulceration, reflux gastropathy, lamina propria irregularities) were identified. In a Pakistani study at Lahore, 36% IBD patients were diagnosed by colonoscopy.33 Another Chinese retrospective study reported that about 95% UC patients were diagnosed via colonoscopy and biopsy exam was performed in about 62.3% UC patients and the most common findings were ulcer and erosions.15 The small percentage of biopsy examination in current study might be because the pathological examination had not been given due consideration as required.
There were about 7.1% (n = 12) IBD patients who had positive family history (4.7% UC and 2.4% CD). About 5% positive family history was reported in a Saudi Arabian study.6 Another study in Lahore, Pakistan, reported that about 40% IBD patients had a positive family history of the disease.33 Another study in Turkey reported a positive family history in 4.4% UC patients and 8.3% CD patients.34 In the current study, about 15% (n = 25) IBD patients were allergic to different medications and foods, 8 were allergic to different antibiotics and 7 were allergic to azathioprine and food allergies were reported in 3 patients. In a retrospective hospital-based study in China, it was reported that food specific IgG antibodies were found in 75.9% (60/79) of CD patients and 63.6% (21/33) of UC patients and the six most common food allergens which caused positive food specific IgG antibodies among IBD patients were egg, milk, rice, corn, tomato and soybean.35 In a Turkish study, CD patients had higher levels of IgG4 against salmon, millet and onion whereas UC patients had higher levels of IgG4 against cuttlefish and onion.36
The current research also reported elevations in CRP and ESR. CRP was raised, in about 14.4% (n = 24) IBD patients, followed by ESR in 10.1% (n = 17). Among the patients with infectious IBD, 4.2% (n = 7) had CMV colitis while 3.6% (n = 6) reported with C. diff. colitis and 1.8% (n = 3) with H. pylori colitis. The current findings were in concordance with previously published research from KSA which reported 2.5% (n = 11) patients with C. diff colitis and 2.1% (n = 9) patients with H. pylori infection.6 The severity was noted for 65.9% (n = 110) IBD patients. The severity of the disease was noted from the patients’ file. About 13.8% of patients had mild form, 16.1% had moderate form and 17.4% had severe form of the disease. However, it was not mentioned on patient’ file that which scale was used to assess the severity. An Egyptian study reported the severity of UC (using Mayo score) and CD (using Crohn’s disease activity index).22 The current investigation documented histopathological abnormalities and the degree of inflammation (mild, mild to moderate, moderate, moderate to severe, severe) in the upper and lower GIT, which were further divided according to location. Based upon the information given in patients’ file, the lower GIT was classified into histopathological abnormalities from rectum to cecum, rectum to transverse colon, rectum, sigmoid colon, rectum and sigmoid colon, descending and transverse colon, ascending colon, ileum, pancolitis, hemorrhoids and anal verge whereas the upper GIT was grouped into stomach, duodenum and esophagus. Among the lower GIT histopathological abnormalities were loss of vascularity, edema, crypt abscess, erythema, superficial ulceration and pseudo polyps whereas small ulcer, pseudo polyps, esophageal cancer, pangastritis were among the upper GIT histopathological abnormalities. A retrospective study conducted at Holy Family hospital in Rawalpindi, Pakistan, reported histopathological abnormalities in CD patients. Among them, pseudo polyps were seen in 54.4% (12/22) patients, followed by crypt abscess in 22.7% (5/22) patients and distortion of crypt architecture in 9.1% (2/22) patients.37 The other published literature documented UC and CD severity using Montreal classification (for both), Truelove and Witts severity index (for UC) or Crohn’s disease activity index (for CD). The current study categorized the severity of the disease based on the available information because the patient files included limited information regarding the criteria of these severity standards. This study has several limitations affecting its generalizability and interpretation. The small sample size (n = 167) may not reflect the broader IBD population. Its retrospective design risks data inaccuracies due to incomplete records. Exclusion of pediatric and pregnant patients limits applicability, while complex comorbidities complicated data extraction. Additionally, treatment effects on disease outcomes were not assessed. Larger, prospective studies with standardized data collection are needed for more reliable and clinically relevant findings.
Our findings reveal treatment patterns that are troubling in the context of contemporary IBD care, with a high dependence on systemic corticosteroids (54.5% inpatient and 46.1% at discharge) and very limited biologic use (8.9%), reflecting a management approach more consistent with pre-2010 practices than with current guidelines. This is not intended to normalize such patterns but to highlight a persistent and concerning reality in our setting, where prolonged or repeated steroid use without adequate steroid-sparing therapy contradicts evidence-based recommendations and exposes patients to significant risks, including infection, metabolic complications, bone disease, and increased mortality. These gaps are driven by barriers such as the high cost of biologics, limited insurance coverage, formulary restrictions, and infrastructural limitations, all of which contribute to suboptimal care. By documenting these challenges, we aim to emphasize the urgent need for systemic improvements rather than endorse the current practice landscape.
Limitations
Our analysis of guideline adherence was limited by the retrospective and descriptive nature of the study, which prevented detailed evaluation of each patient and indication, and made it difficult to fully account for access barriers, payer restrictions, or phenotype-specific contraindications. As a result, the “followed, partially followed, or not followed” classifications reflect observed patterns but may misclassify cases where apparent non-adherence was clinically appropriate. The descriptive design also limits our ability to identify the factors driving treatment patterns or guideline adherence. Future prospective studies with detailed, patient-level data and analyses that account for factors such as age, disease extent, and comorbidities will be needed to more accurately assess the appropriateness of treatment decisions.
Other limitations include incomplete recording of ethnicity, which prevented analysis of its influence on disease presentation or management, and missing or approximate socioeconomic data, limiting assessment of how economic status may affect treatment patterns. We were also unable to evaluate delays in diagnosis, and the reasons for guideline deviations, whether related to clinical judgment, patient preference, or resource constraints could not be determined. Addressing these gaps will require prospective studies with standardized documentation and input from both patients and clinicians.
Conclusion
This study provides the first comprehensive baseline data on IBD management practices at a Pakistani tertiary care center, revealing significant gaps in guideline adherence with only five of nine CD and three of nine UC NICE recommendations being followed. The notably low rates of biologic utilization and surgical intervention, coupled with detailed characterization of medication patterns, comorbidities, and diagnostic approaches, underscore substantial deviations from contemporary evidence-based care standards. While the single-centre design and modest sample size (n = 167) limit generalizability, and the descriptive methodology precludes causal inference regarding determinants of guideline non-adherence, these findings identify actionable targets for quality improvement and establish the urgent need for multicenter validation studies and development of context-appropriate, resource-stratified clinical guidelines tailored to LMIC healthcare settings.
Future Prospective
The limitations of our single-center design underscore the necessity for larger, multicenter investigations that can validate findings across diverse Pakistani healthcare ecosystems and strengthen the evidence base for inflammatory bowel disease management in resource-constrained settings. Prospective cohort studies employing robust methodological approaches including comparative analyses using chi-square or Fisher’s exact tests for categorical variables, appropriate parametric or non-parametric tests for continuous outcomes, and multivariable regression modeling to identify independent predictors of treatment success are essential to advance our understanding. Moreover, survival analyses and time-to-event methodologies could illuminate critical questions regarding disease progression, treatment escalation patterns, and factors influencing surgical intervention. Concurrently, outcome-focused research must prioritize linkage between current treatment patterns and clinically meaningful endpoints, including steroid-free remission, mucosal healing, hospitalization rates, quality of life measures, and long-term surgical requirements. Such investigations will provide the empirical foundation necessary for evidence-based refinement of care delivery practices within Pakistani IBD populations.
Equally pressing are investigations addressing the diagnostic and therapeutic challenges unique to the Pakistani healthcare landscape. Research elucidating diagnostic delays, systemic barriers to timely treatment initiation, and their consequent effects on disease trajectory represent a significant knowledge gap that directly impacts patient outcomes in this region. Fundamentally, Pakistan requires the development of context-appropriate, resource-stratified management protocols that integrate international best practices with the practical realities of medication accessibility, infrastructure constraints, and economic considerations. Such locally relevant guidelines should aim to minimize preventable complications while remaining operationally feasible within existing healthcare structures. By systematically addressing these research priorities, future initiatives can establish an evidence-driven framework that transforms IBD care in Pakistan toward locally achievable standards of clinical excellence.
Data Sharing Statement
All data generated during the study are presented in this paper.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgment
The authors of this study extend their appreciation to the Ongoing research Funding Program (ORF-2026-1099), King Saud University, Riyadh 11451, Saudi Arabia.
Funding
This study was Funded by Ongoing research Funding Program (ORF-2026-1099), King Saud University, Riyadh 11451, Saudi Arabia.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Abdulla M, Al Saeed M, Fardan RH, et al. Inflammatory bowel disease in Bahrain: single-center experience. Clin. Exp. Gastroenterol. 2017;Volume 10:133–20. doi:10.2147/CEG.S127909
2. Mokhtar NM, Nawawi KNM, Verasingam J, et al. A four-decade analysis of the incidence trends, sociodemographic and clinical characteristics of inflammatory bowel disease patients at single tertiary centre, Kuala Lumpur, Malaysia. BMC Public Health. 2019;19:1–10. doi:10.1186/s12889-019-6858-2
3. Pizzi LT, Weston CM, Goldfarb NI, et al. Impact of chronic conditions on quality of life in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2006;12(1):47–52. doi:10.1097/01.MIB.0000191670.04605.e7
4. Nóbrega VG, INdN SILVA, Brito BS, Silva J, MCMd SILVA, Santana GO. The onset of clinical manifestations in inflammatory bowel disease patients. Arquivos de gastroenterologia. 2018;55(03):290–295. doi:10.1590/s0004-2803.201800000-73
5. Estevinho MM, Leão Moreira P, Silva I, Laranjeira Correia J, Santiago M, Magro F. A scoping review on early inflammatory bowel disease: definitions, pathogenesis, and impact on clinical outcomes. Ther Adv Gastroenterol. 2022;15:17562848221142673. doi:10.1177/17562848221142673
6. Aljohani RS, Alaklabi A, Alsitary YM, et al. Clinical profile, course and outcomes of adults with inflammatory bowel disease over a decade: a single center experience. Ann Saudi Med. 2022;42(6):397–407. doi:10.5144/0256-4947.2022.397
7. Guedes ALV, Lorentz AL, LFdAR R, et al. Hospitalizations and in-hospital mortality for inflammatory bowel disease in Brazil. World J Gastrointest Pharmacol Ther. 2022;13(1):1. doi:10.4292/wjgpt.v13.i1.1
8. Pasternak G, Chrzanowski G, Aebisher D, et al. Crohn’s disease: basic characteristics of the disease, diagnostic methods, the role of biomarkers, and analysis of metalloproteinases: a review. Life. 2023;13(10):2062. doi:10.3390/life13102062
9. Feuerstein JD, Cheifetz AS. Crohn disease: epidemiology, diagnosis, and management.
10. D’Errico A, Malvi D. Diagnosis of ulcerative colitis: morphology and histopathological characteristics. In: Ulcerative colitis. Springer; 2019:61–92.
11. Gasparetto M, Guariso G. Highlights in IBD epidemiology and its natural history in the paediatric age. Gastroenterol res pract. 2013;2013(1):829040. doi:10.1155/2013/829040
12. Roberts S, Thorne K, Thapar N, et al. A systematic review and meta-analysis of paediatric inflammatory bowel disease incidence and prevalence across Europe. J Crohns Colitis. 2020;14(8):1119–1148. doi:10.1093/ecco-jcc/jjaa037
13. Zaman Z, ZJWJoGP M. Therapeutics. Inflammatory bowel disease in Pakistan: low prevalence or underdiagnosis? World J Gastrointest Pharmacol Ther. 2024;15(6):99226. doi:10.4292/wjgpt.v15.i6.99226
14. Thia KT, Loftus JEV, Sandborn WJ, Yang S-K. An update on the epidemiology of inflammatory bowel disease in Asia. Official J Am College Gastroenterol. 2008;103(12):3167–3182. doi:10.1111/j.1572-0241.2008.02158.x
15. Wang Y, Ouyang Q, Group ACIW. Ulcerative colitis in China: retrospective analysis of 3100 hospitalized patients. J. Gastroenterol. Hepatol. 2007;22(9):1450–1455. doi:10.1111/j.1440-1746.2007.04873.x
16. Park J, Park S, Lee SA, Park SJ, Cheon JH. Improving the care of inflammatory bowel disease (IBD) patients: perspectives and strategies for IBD center management. Korean J Intern Med. 2021;36(5):1040. doi:10.3904/kjim.2021.114
17. Yang A, Chen Y, Scherl E, Neugut AI, Bhagat G, Green PH. Inflammatory bowel disease in patients with celiac disease. Inflamm. Bowel Dis. 2005;11(6):528–532. doi:10.1097/01.MIB.0000161308.65951.db
18. Anjum RM. Inflammatory bowel disease in pakistani population: an important diagnosis, not to be overlooked. 2022.
19. Garbi MJH. National Institute for Health and Care Excellence clinical guidelines development principles and processes. Heart. 2021;107(12):949–953. doi:10.1136/heartjnl-2020-318661
20. Martins R, Carmona C, George B, Epstein JJB. Management of Crohn’s disease: summary of updated NICE guidance. BMJ. 2019;367. doi:10.1136/bmj.l5940
21. Abdulrazeg O, Li B, Epstein J. Management of ulcerative colitis: summary of updated NICE guidance. BMJ. 2019;367. doi:10.1136/bmj.l5897
22. El-Atrebi K, Taher E, El Aguizy F, et al. A descriptive study of inflammatory bowel disease at an Egyptian tertiary care center. Revista de Gastroenterología de México. 2023;88(1):12–18. doi:10.1016/j.rgmx.2021.03.004
23. Al-Fawzan AA, Al-Radhi SA, Al-Omar AS, et al. A study of the epidemiology, clinical, and phenotypic characteristics of inflammatory bowel disease in the northen-central region of Saudi Arabia. Diagnostics. 2023;13(13):2135. doi:10.3390/diagnostics13132135
24. Al-Jarallah K, Shehab D, Al-Azmi W, Al-Fadli A. Rheumatic complications of inflammatory bowel disease among A rabs: a hospital-based study in K uwait. Int. J. Rheum. Dis. 2013;16(2):134–138. doi:10.1111/j.1756-185X.2012.01811.x
25. Sassaki LY, Miszputen SJ, Junior RLK, et al. Real-world treatment patterns and disease control over one year in patients with inflammatory bowel disease in Brazil. World J Gastroenterol. 2021;27(23):3396. doi:10.3748/wjg.v27.i23.3396
26. Zabihi A, Kashifard M, Amiri SRJ, Sepidarkish M, Padehban V, Qalehsari MQ. Investigation of chronic diseases in patients with inflammatory bowel disease: a hospital-based case-control study. Caspian j intern med. 2022;13(2):363. doi:10.22088/cjim.13.2.7
27. Lelli F, Nuhoho S, Lee XY, Xu W. Systematic review: treatment pattern and clinical effectiveness and safety of pharmaceutical therapies for Crohn’s disease in Europe. Clin. Exp. Gastroenterol. 2016:311–323.
28. Gisbert J, Marín A, McNicholl A, Chaparro M. Systematic review with meta-analysis: the efficacy of a second anti-TNF in patients with inflammatory bowel disease whose previous anti-TNF treatment has failed. Aliment Pharmacol Ther. 2015;41(7):613–623. doi:10.1111/apt.13083
29. Null KD, Xu Y, Pasquale MK, et al. Ulcerative colitis treatment patterns and cost of care. Value Health. 2017;20(6):752–761. doi:10.1016/j.jval.2017.02.005
30. Sandborn WJ, Targan SR. Biologic therapy of inflammatory bowel disease. Gastroenterology. 2002;122(6):1592–1608. doi:10.1053/gast.2002.33426
31. Nasim S, Chawla T, Sheikh GM. Surgical management of inflammatory bowel disease: a low prevalence, developing country perspective. JPMA. 2016;66(3):247.
32. Oli AK, Maidur RN, Hurkadli PS, Javalgi AP, Javaregowda PK, Goni M. Incidence of inflammatory bowel disease: a single centre retrospective study. Arq. Gastroenterol. 2022;59(3):345–351. doi:10.1590/s0004-2803.202203000-63
33. Safdar R, Qamber JH, SAFDER A, Jalil V. A morphological study of inflammatory bowel disease; manifestatons, incidence and management at different tertiary care hospitals at Lahore, Pakistan. Pak. J. Med. Health Sci. 2018;12(3):1129–1131.
34. Tozun N, Atug O, Imeryuz N, et al. Clinical characteristics of inflammatory bowel disease in Turkey: a multicenter epidemiologic survey. J Clin Gastroenterol. 2009;43(1):51–57. doi:10.1097/MCG.0b013e3181574636
35. Cai C, Shen J, Zhao D, et al. Serological investigation of food specific immunoglobulin G antibodies in patients with inflammatory bowel diseases. PLoS One. 2014;9(11):e112154. doi:10.1371/journal.pone.0112154
36. Dinçer D, Karancı EU, Akın M, Adanır H. NSAID, antiaggregant, and/or anticoagulant-related upper gastrointestinal bleeding: is there any change in prophylaxis rate after a 10-year period? Turk J Gastroenterol. 2019;30(6):505. doi:10.5152/tjg.2019.19057
37. Akhtar TS, Ashraf B, Zahid K, et al. Evaluation of factors contributing to diagnosis of crohn’s disease in the face of increasing trend in Pakistan. Crohn’s Colitis. 2024;6(1):otae015. doi:10.1093/crocol/otae015
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.