Back to Journals » Patient Preference and Adherence » Volume 20
Medication Regimen Complexity and Patient-Reported Adherence: A Cross-Sectional Study in Internal Medicine Outpatients
Authors Ertuna E ![]() , Guray I, Inci V, Sirmatel Bucuk P, Sozen Gencer N
, Guray I, Inci V, Sirmatel Bucuk P, Sozen Gencer N ![]() , Arun MZ
, Arun MZ ![]() , Kilavuz A
, Kilavuz A
Received 9 December 2025
Accepted for publication 18 February 2026
Published 25 February 2026 Volume 2026:20 587752
DOI https://doi.org/10.2147/PPA.S587752
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Elif Ertuna,1 Irem Guray,2 Veli Inci,3 Pinar Sirmatel Bucuk,4 Nagihan Sozen Gencer,5 Mehmet Zuhuri Arun,1 Asli Kilavuz6
1Department of Clinical Pharmacy, Faculty of Pharmacy, Ege University, Bornova, Izmir, Turkey; 2Farma-Tek Pharmaceutical Industry and Trade Inc., Kırklareli, Turkey; 3Hospital Pharmacy, Pamukkale University, Denizli, Turkey; 4Geriatrics Outpatient Clinic, Buca Seyfi Demirsoy Training and Research Hospital, Affiliated with the University of Health Sciences, Izmir, Turkey; 5Department of Internal Medicine, Division of Geriatrics, Balıkesir Atatürk City Hospital, Balıkesir, Turkey; 6Department of Internal Medicine, Division of Geriatrics, Faculty of Medicine, Ege University, Bornova, Izmir, Turkey
Correspondence: Mehmet Zuhuri Arun, Department of Clinical Pharmacy, Faculty of Pharmacy, Ege University, Bornova, Izmir, 35040, Turkey, Tel +90 532 655 74 95, Email [email protected]
Purpose: Medication non-adherence and regimen complexity are significant barriers to achieving therapeutic goals. This study aimed to determine the impact of medication regimen complexity, and clinical characteristics of patients on medication adherence in internal medicine outpatients.
Patients and Methods: This prospective cross-sectional study was conducted in the internal medicine and geriatric outpatient clinics of a tertiary university hospital. Adherence was assessed with Medication Adherence Report Scale (MARS-5), and regimen complexity was quantified using the Medication Regimen Complexity Index (MRCI) in 150 patients.
Results: The mean age of the participants was 57.53± 1.26 years. Only 44% of the participants demonstrated perfect adherence to therapy. The MRCI scores of geriatric patients (median: 11 (3– 44) vs 19 (5– 65)) and those hospitalized within the last six months (median: 12.75 (3– 47) vs 20 (6– 65.5)) were significantly higher. Complexity scores related to dosing schedule and instructions for use were especially higher in patients with hypertension or diabetes. No statistically significant correlation was found between the total MRCI score and patient-reported adherence scores (P=0.32). However, geriatric patients and recently hospitalized patients were less likely to fully adhere to therapy (χ2 (1, N=150) = 4.71, P=0.030 and 4.23, P=0.040, respectively).
Conclusion: Although a direct correlation between total regimen complexity and self-reported adherence was not observed, complexity poses a significant challenge for specific high-risk groups, including geriatric patients and those with recent hospitalizations. These findings may suggest that providing targeted medication counseling and medication regimen review, particularly in the early post-discharge period, might be crucial for optimizing adherence and clinical outcomes.
Keywords: medication adherence, medication regimen complexity index, MRCI, ambulatory patients, elderly
Introduction
While medications are essential for treating various health conditions, medication-related problems constitute a major cause of preventable hospital admissions.1 Poor medication adherence is one of the primary reasons for the failure to achieve therapeutic benefits, typically defined as taking less than 80% of prescribed doses, though excessive medication use also constitutes non-adherence.2 Many patients discontinue newly prescribed medications within the first few months without informing their physicians, and adherence generally decreases over time. Additionally, many patients who continue taking medications do not follow the prescribed regimen regularly. Consequently, treatment adherence rates are approximately 50%, and non-adherence is associated with poor health outcomes, adverse events, and increased mortality.2
Studies have demonstrated increasing per-capita medication use and polypharmacy prevalence over the years.3 As the number of daily medications, doses, and medication regimen complexity increase, hospitalization rates, readmissions, and medication non-adherence also rise.4,5 Polypharmacy and treatment non-adherence result in increased healthcare visits, hospitalization rates, and care costs.6
The Medication Regimen Complexity Index (MRCI) is a useful tool to identify patients who may benefit from medication therapy management.7 The MRCI provides a detailed assessment of regimen complexity by categorizing it into three distinct domains: dosage forms (Section A), dosing frequency (Section B), and additional instructions (Section C).8 While an elevated total MRCI score is generally associated with suboptimal adherence, the influence of these individual components may differ in clinical practice.9 For instance, dosing frequency is often cited as a more visible barrier, as the logistical requirement of multiple daily administrations tends to increase the likelihood of forgetfulness.8–10 Conversely, Section C, which encompasses specific requirements such as “taking with food” or “avoiding certain liquids”, might impose a more subtle cognitive burden on the patient. This complexity in instructions could potentially be more disruptive than the mere physical form of the medication itself, suggesting that adherence challenges are likely driven by the cognitive effort required to integrate these instructions into daily life rather than just the number of pills consumed.5,9
A high level of medication regimen complexity leads to poorer adherence and disease control in diabetes and hypertension patients,11,12 and worse adherence in the geriatric patients.5 The role of sex differences in medication adherence among patients with different diseases is not yet well established and should be addressed in future studies.13 Treatment non-adherence, adverse drug events, dosing errors and interactions are more likely with increased regimen complexity possibly leading to adverse outcomes including lower overall quality of life, higher hospitalization rates and higher mortality rates.4,14 Determining regimen complexity and its potential impact on treatment adherence in adult patients with various chronic conditions could facilitate identification of at-risk patients and tailor their care appropriately.
The primary objective of this study is to determine the impact of existing chronic diseases, comorbidity burden, and medication regimen complexity on medication adherence among adult outpatients. We hypothesized that higher MRCI scores would be significantly associated with reduced medication adherence in outpatients, with this effect being more pronounced in geriatric patients and in patients with specific medication classes.
Materials and Methods
Study Population and Data Collection
This prospective cross-sectional study was conducted between March and May 2023 in the internal medicine outpatient clinic and the geriatric outpatient clinic of a tertiary university hospital in İzmir, Turkey. The 3-month study period was selected to ensure adequate sample size while maintaining feasibility. A previous study involving outpatients found a self-reported treatment adherence rate of 89%.15 Based on this finding, the sample size with a 5% margin of error and 95% confidence interval was calculated as 151 patients. Following the study period one patient was excluded due to inconsistent and incomplete responses. Patients who applied to the internal medicine or geriatrics outpatient clinic aged ≥18 years and being treated with at least one drug were included in the study. Exclusion criteria included patients not taking medication at the time of their visit and those unable to provide informed consent, particularly in cases of severe dementia or psychiatric illness. We also excluded participants unable to complete questionnaires independently to maintain the reliability of patient-reported data.
Patient demographics (age, sex, level of education, living conditions), clinical characteristics (complaints, chronic diseases, medications), and hospital admissions from the preceding six months were documented during face-to-face interviews. Medication adherence was also determined during direct patient interviews using the validated Turkish version of the Medication Adherence Report Scale (MARS).16 The MARS-5 consists of five different statements of negative behaviors related to medication adherence, and scores on this 5-point Likert scale range from 5 to 25 where higher scores signify better adherence. Patients were divided into two groups by the median MARS score (24), a MARS score of ≥24 was deemed as perfect adherence to therapy. Medication regimen complexity was assessed for each prescription using the MRCI, utilizing the Turkish version previously adapted and validated by Okuyan et al.17 The MRCI consists of 65 items and 3 sections; MRCI-A, dosage form; MRCI-B, dosage frequency; and MRCI-C, special instructions. The total MRCI score is derived by summing three weighted domains. Section A focuses on dosage forms, typically assigning lower weights to oral medications and higher values to more complex delivery systems like inhalers or injections. Section B calculates complexity based on the daily frequency of administration for each drug in the protocol. Lastly, Section C accounts for additional instructions, such as specific timing or food requirements, which may impose a further cognitive burden on the patient’s daily routine.
The participants’ Charlson Comorbidity Index (CCI) score was calculated. The Charlson Comorbidity Index operates by assigning numerical values to various medical conditions, then calculating the total score based on which conditions a patient has. This scoring system uses integer values ranging from one through six for different health conditions, where six indicates the highest severity level. The final comorbidity score is determined by adding together all the individual condition weights that apply to a specific patient.18
The active ingredients of the drugs were classified according to the Anatomical Therapeutic Chemical (ATC) code, and the pharmaceutical forms were classified using the New Form Codes (NFC).19 The ATC classification system has been sustained since 1982 by the WHO Collaborating Center for Drug Statistics Methodology in Oslo, Norway. This system provides a global standard for classifying medical substances and serves as a tool for drug utilization research. The main objective of the NFC is to maintain an international uniformity of the coding structure for the audits and the databases.
Ethics
The authors complied with Good Clinical Practice standards throughout the study. This study is approved by the Ethics Committee for Medical Research of the Faculty of Medicine at Ege University and TITCK (Turkish Medicines and Medical Devices Agency) (22-AKD-267, 22-AKD-268) and is conducted according to the World Medical Association Declaration of Helsinki. Informed written consent was obtained from all study participants prior to study commencement.
Statistical Analysis
The database was constructed using Microsoft Excel. Normality testing was performed using the Shapiro–Wilk test. Patients’ age and CCI scores were considered to have a normal distribution with a P value >0.05 or skewness and kurtosis values within ±2. Parametric and non-parametric continuous variables are expressed as means ± standard error of mean (SEM) or median (min-max), respectively. Categorical data were presented in terms of frequencies. The correlation statistics of data were calculated using the Pearson’s or Spearman’s test where appropriate. The independent-samples T test or Mann–Whitney U-test was used for comparisons between the subgroups of continuous variables. Categorical data were evaluated using Chi-Square test. All statistical tests were performed using SPSS version 25.0 (IBM SPSS Statistics for Windows, Version 25.0; IBM Corp., Armonk, NY, USA). A P value <0.05 was considered statistically significant.
Results
Demographic Characteristics of Patients
The mean age of the 150 patients included in this study was 57.53 ± 1.26 years (Table 1). There was no difference between the mean age of the male and female patients (male: 60.02 ± 16.62 years, N = 45 and female: 56.47 ± 14.77 years, N =105; P =0.20). Forty-three patients (28.7%) were 65 years or older.
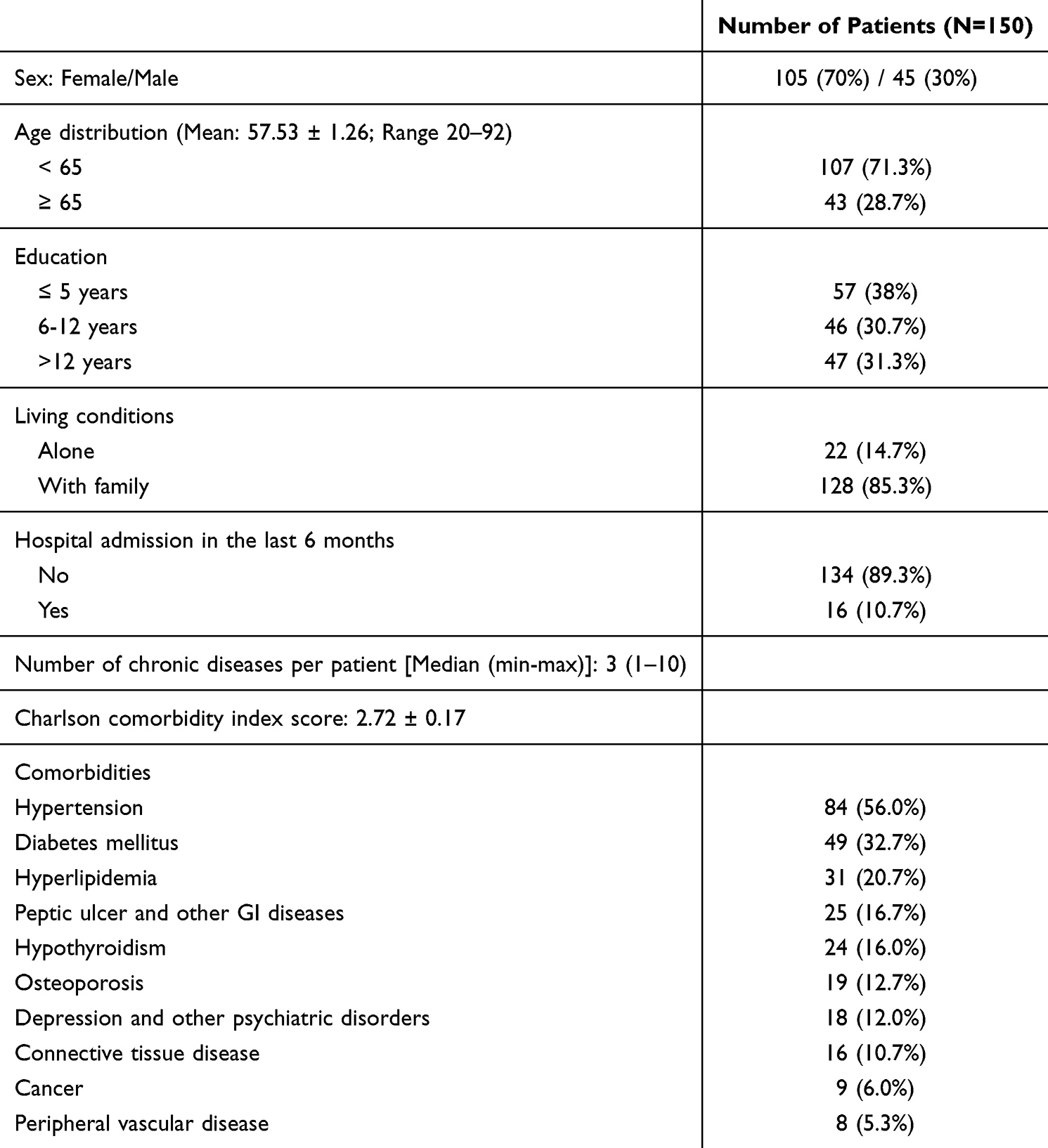 |
Table 1 Demographic Characteristics of Patients |
Most of the patients (n = 108, 72.0%) presented to the outpatient clinic for routine check-up or prescription refill. The median number of chronic diseases per patient was 3 (1–10). The most common chronic diseases were hypertension and diabetes (N = 84 and 49, respectively). Patients’ Charlson comorbidity index (CCI) was calculated as 2.72 ± 0.17. There was no significant difference between the number of diseases (2 (1–7) vs 3 (1–10); P =0.18) or CCI scores (2.91 ± 2.40 vs 2.64 ± 1.84; P =0.45) of male and female patients.
Sixteen (10.7%) patients were admitted to the hospital in the last 6 months. Patients with recent admission(s) had higher number of diseases (2 (1–10) vs (4.5 (1–10); P =0.001) and CCI scores (2.48 ± 0.16 vs 4.75 ± 0.64; P <0.001).
Consistent with general clinical expectations, age showed a strong positive correlation with both the number of diseases per patient (rs =0.665, P <0.001), and the CCI (R =0.770, P <0.001). This anticipated trend of increasing morbidity with age was further reflected in group comparisons; the number of diseases per patient was significantly higher in patients ≥65 years compared with patients <65 years (4 (1–10) vs 2 (1–6); P <0.001). Similarly, CCI scores were also substantially higher in the geriatric group (4.67 ± 0.30 vs 1.93 ± 0.14; P <0.001).
Prescription and Drug Use Patterns
Patients were prescribed 666 drugs and median number of drugs prescribed per patient was 4 (1–15). Oral solid (n=599, 89.9%) and liquid forms (n=22, 3.3%) were the most prescribed pharmaceutical forms, followed by parenteral drugs (n=25, 3.8%). According to the ATC classification, the most commonly prescribed drugs were the alimentary tract and metabolism (N=204, 30.63%), the cardiovascular system (N=161, 24.17%), nervous system (N=76, 11.86), blood and blood forming organs (N=63, 9.46%), and systemic hormonal preparations, excluding sex hormones and insulins (N=54, 8.11%) (Figure 1).
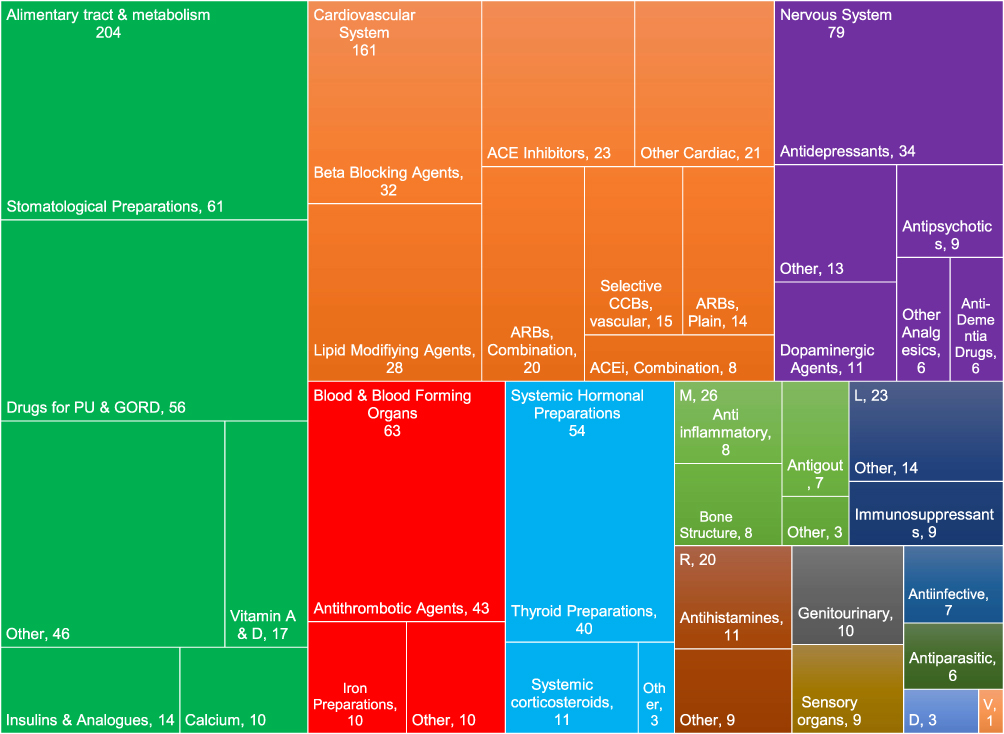 |
Figure 1 The distribution of the pharmacological groups of prescribed drugs based on the ATC classification system. Abbreviations: ACE, angiotensin converting enzyme; ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; D, dermatologicals; L, antineoplastic and immunomodulating agents; M, musculo-skeletal system; PU & GORD, Peptic ulcer & Gastroesophageal reflux disease; R, respiratory system; V, various. |
Polypharmacy, defined as using 5 or more drugs, was present in 61 (40.7%) patients. The number of drugs used per patient did not differ according to sex (male: 4 (1–15) vs female: 4 (1–14); P =0.31). As might be expected, there was a moderate positive correlation between age and the number of drugs used (rs =0.530; P <0.001). Geriatric patients used more drugs (5 (2–15) vs 3 (1–13); P <0.001) and were more likely to have polypharmacy than young adults (χ2 (1, N = 150) = 21.16, P <0.001), a finding that aligns with widely recognized clinical patterns of multimorbidity in aging.
Patients with polypharmacy had more chronic diseases than patients using <5 drugs (4 (1–10) vs 2 (1–5); P <0.001). CCI score was also significantly higher in patients with polypharmacy (1.90 ± 0.17 vs 3.92 ± 0.26; P <0.001).
Patients who had been admitted to the hospital in the previous 6 months used more drugs (4 (1–14) vs 7 (2–15); P <0.001). A chi-square test of independence was performed to evaluate the relationship between using a specific therapeutic subgroup (ATC level 2) and hospital admission in the last 6 months. Patients using antidiabetics (χ2 (1, N = 150) = 4.53, P =0.033), antithrombotics (χ2 (1, N = 150) = 4.63, P =0.031) or thyroid products (χ2 (1, N = 150) = 4.20, P =0.040) were more likely to be admitted to hospital in the last 6 months.
Medication Regimen Complexity
Total MRCI score was 13 (3–65.5) (Table 2). There was a moderate positive correlation between patient’s age and MRCI score (rs =0.530, P <0.001). Geriatric patients’ drug regimens were more complex compared to younger patients (19 (5–65) vs 11 (3–44); P <0.001). MRCI scores were similar for male and female patients (12 (3–65.5) vs 14 (3–47); P =0.51).
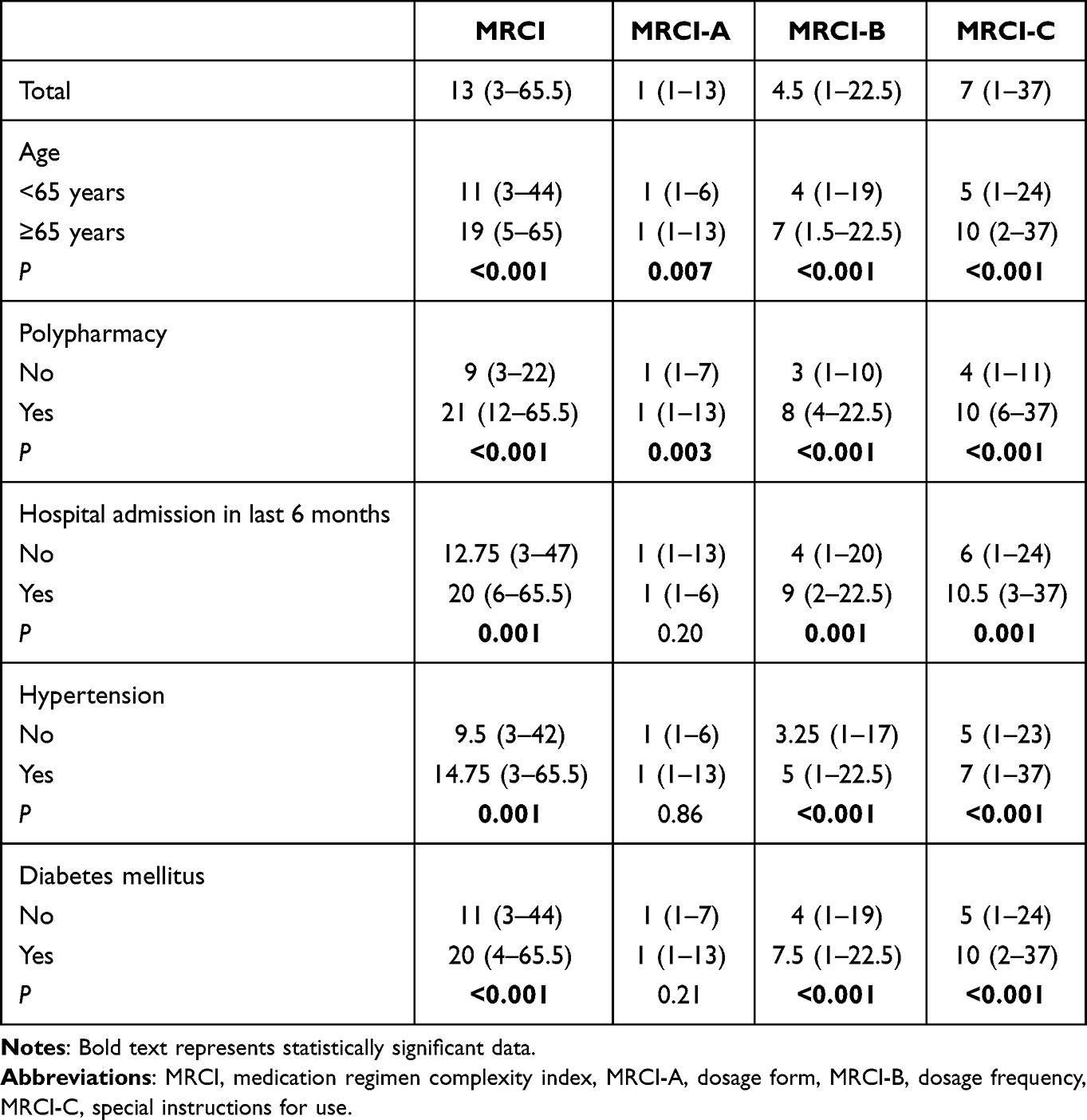 |
Table 2 Medication Regimen Complexity in Different Patient Subgroups |
Number of diseases per patient had a strong positive correlation with MRCI score (rs =0.636; P <0.001). MRCI scores of patients with hypertension or diabetes were higher than those who did not have the diseases (Table 2). Specifically, scores regarding the dosing schedule and instructions for use was higher in patients with hypertension or diabetes (Table 2).
The MRCI scores of patients who were admitted to the hospital in the last 6 months were higher (12.75 (3–47) vs 20 (6–65.5); P =0.001). Complexity scores related to dosing schedule and instructions for use were especially higher in patients with recent admissions (Table 2).
As expected, patients with polypharmacy had a more complex medication regimen (9 (3–22) vs 21 (12–65.5); P <0.001) (Table 2). The effects of specific therapeutic subgroups on MRCI scores are given in Table 3.
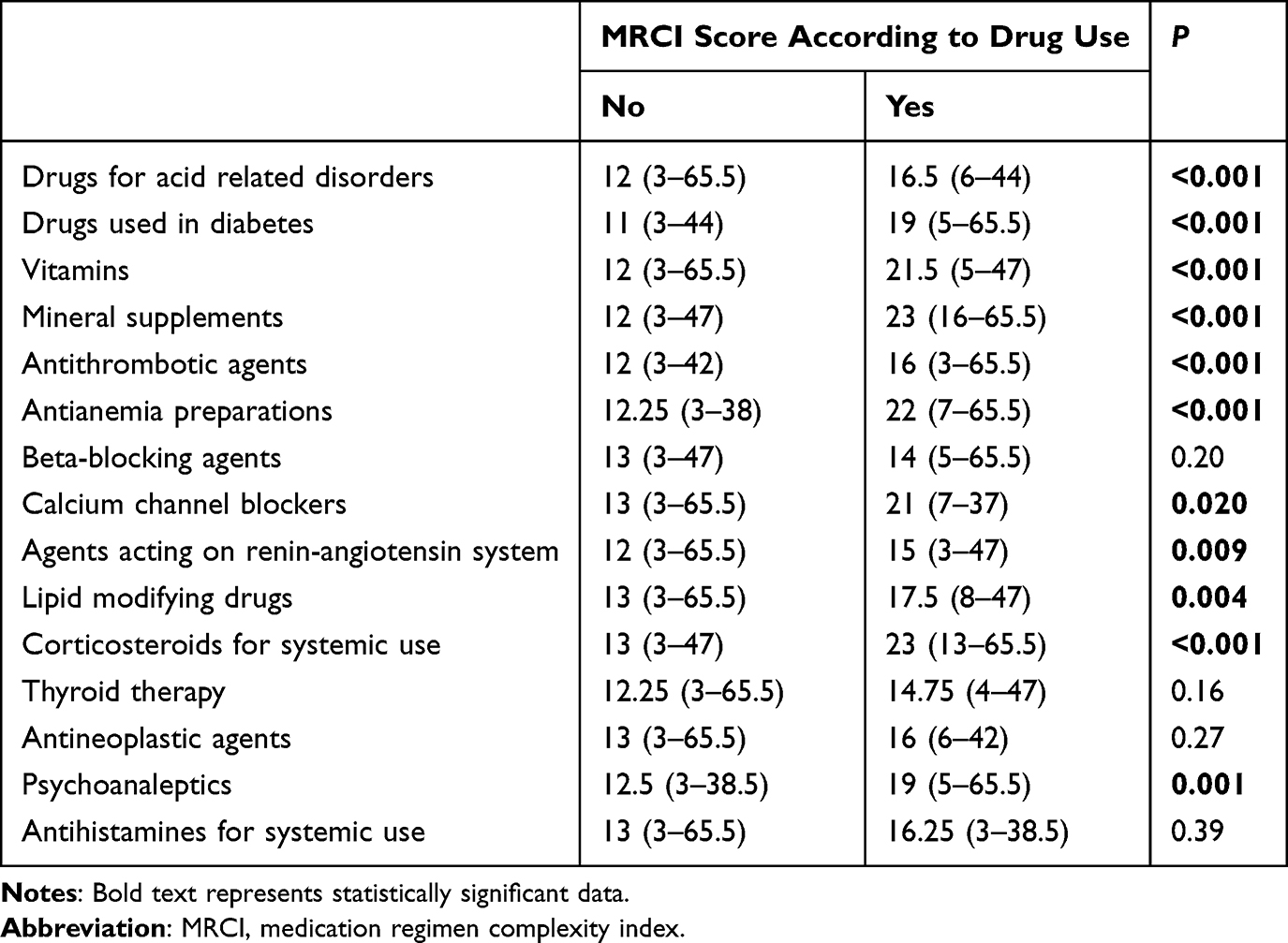 |
Table 3 The Effects of Therapeutic Subgroups on MRCI |
Patients’ Adherence to Therapy
The median medication adherence scores of patients was 24 (8–25). Patients’ responses to the adherence questionnaire are represented in Figure 2. Only 44% (N=66) of the patients showed perfect adherence to therapy.
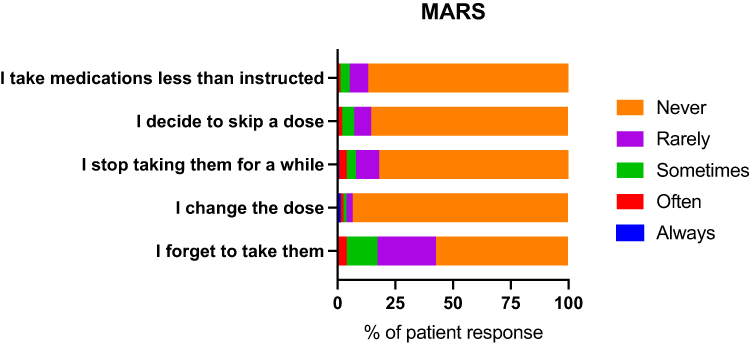 |
Figure 2 Patients’ responses to the Mars-5 questionnaire. |
Adherence scores were not different between male and female patients (24 (19–25) vs 24 (8–25); P =0.96). No correlation was found between patients’ age and adherence scores (rs = −0.021, P =0.80). Geriatric patients were less likely to fully adhere to the therapy (χ2 (1, N = 150) = 4.71, P =0.030). Patients who had 6–12 years of education were more likely to show perfect adherence to therapy than those who had <5 years or >12 years of education (χ2 (2, N = 150) = 10.23, P =0.006).
Presence of polypharmacy did not alter median adherence scores (24 (8–25) vs 24 (10–25); P =0.26). Median adherence scores were similar for those patients being admitted to hospital in the previous 6 months and those who did not (24 (8–25) vs 23 (20–25); P =0.20). However, patients who had been admitted to the hospital were less likely to fully adhere to therapy (χ2 (1, N = 150) = 4.23, P =0.040).
The Relationship Between MRCI and Patient Reported Adherence
MRCI scores were not correlated with patient adherence scores (rs = −0.082; P =0.32). MRCI scores of patients who fully adhered to the therapy were similar to patients who did not adhere to therapy (13 (3–44) vs 14.5 (4–65.5); P =0.15). When a chi-square test of independence was performed to evaluate the relationship between taking a therapeutic subgroup (ATC level 2) and perfect adherence, patients who were using mineral supplements were found to be less likely to fully adhere to therapy (χ2 (1, N = 150) = 5.33, P =0.021).
The relationship between MRCI and patient adherence was also evaluated in patients taking specific subgroups of medicine. In patients that were using antianemia preparations; MRCI was moderately and negatively correlated with patient adherence (rs = −0.509; P =0.044) and MRCI score was lower in patients who reported full adherence to therapy (16.5 (7–44) vs 42 (17–65.5); P =0.038). Also, the instructions for use component of the MRCI score was strongly negatively correlated with adherence (rs = −0.625; P =0.010) and it was significantly lower in patients with perfect adherence (9 (4–24) vs 23 (10–37); P =0.019) in patients using antianemia preparations.
Patients who used systemic corticosteroids and who did not fully adhere to therapy had higher total MRCI scores (30 (21–65.5) vs 17.25 (13–25); P =0.017), higher MRCI B scores (dose frequency score, 12.5 (9–22.5) vs 7.5 (4.5–11); P =0.009) and higher MRCI C scores (instructions for use score, 15 (9–37) vs 9 (7–13); P =0.030) than patients who reported full adherence.
Patients who used thyroid therapy and who did not fully adhere to therapy had higher MRCI C scores than patients who reported full adherence (instructions for use score, 10 (6–24) vs 7 (2–20); P =0.033).
Discussion
Patients presenting to internal medicine outpatient clinics in tertiary hospitals likely have significant comorbidity burdens and complex health problems. Determining disease burden, medication regimen complexity, and the impact of regimen complexity on treatment adherence in this patient population is crucial. To reduce medication regimen complexity associated with various chronic diseases or multimorbidity, appropriate interventions should be implemented to minimize medication numbers or simplify treatment regimens while maximizing patient benefit. Identifying patient and disease-related risk factors contributing to medication regimen complexity and non-adherence is essential for determining intervention strategies.
No correlation was found between the complexity of the medication regimen and patient-reported adherence in our study. There is variability in previous studies regarding the association between MRCI and adherence. A systematic review assessing 54 studies found that complexity was associated with adherence in 38 studies, but 16 studies found no correlation between complexity and adherence.14 Measurement of adherence to therapy with self-reported methods can be subjective, and patients may report deceptively higher adherence rates, but they are also low-cost and low-burden adherence measures.20 However, our study determined that only 44% of patients were fully adherent to their treatment. Self-report adherence tools, such as MARS, are considered to have good specificity and weak sensitivity.20 Consequently, high levels of self-reported non-adherence in our study can be considered reliable and suitable for analyzing factors associated with non-adherence. Nonetheless, the lack of adherence assessment using other methods in our study is one of its limitations. To accurately determine the effects of medication regimen complexity on adherence, we believe further research utilizing more objective methods, such as pill counts or prescription refill rates, in addition to self-reported measures, is necessary.
Education level has been identified as a significant determinant of medication adherence.21 Lower educational status may result in negative attitudes toward pharmacotherapy, thus may pose a barrier by limiting the comprehension of therapeutic goals and specific medications.22 However, the relationship between education and adherence was not linear; instead, patients with 6 to 12 years of education demonstrated the highest likelihood of full adherence in our study. This finding may suggest that the extent of formal education does not always reflect the patients’ competency in health literacy. Thus, regardless of educational background, all patients, particularly those at high risk, should be educated on the importance of treatment adherence.
Evidence regarding the relationship between age and medication adherence remains inconsistent in literature. In a cross-sectional health survey self-reported medication non-adherence was higher in younger adults.23 Another study suggested that adherence increased until age 69 and started to decline thereafter.24 Geriatric patients were less likely to fully adhere to the therapy in our study. As individuals age, the number of medications used and the prevalence of polypharmacy increase, leading to more complex medication regimens. Given that geriatric patients had more complex medication regimens and were found to be less likely to fully adhere to their therapy in our study, it is advisable to review and optimize their medication regimens.
Medication non-adherence is not solely attributable to the quantity of medications used. Medication regimens containing similar numbers of drugs vary in complexity due to multiple dosage forms, dosing frequencies, and additional administration instructions.25 Studies examining the relationship between medication regimen complexity and adherence in geriatric patients have demonstrated a significant negative association between MRCI scores and medication adherence.5,26 Measures to address adherence problems include explaining the importance and consequences of treatment adherence to the patient; providing information about potential outcomes of the disease and treatment failure; and, where feasible, reducing the number of medications, dosing frequency, and treatment duration. Other strategies involve utilizing patient aids such as pill organizers, large-print labels, calendar and telephone reminders; increasing the frequency of post-discharge visits and follow-ups; and providing education to raise patient awareness.27
A diagnosis of diabetes, hypertension or dyslipidemia was found to be related to higher odds of non-compliance in community-dwelling geriatric patients in a previous study.23 In another study, medication adherence in hypertensive patients was found to vary depending on age and medications count.24 Therefore, we evaluated the association between MRCI scores and adherence in patients with diabetes or hypertension in our study.
Patients using antidiabetic or antithrombotic agents have both higher MRCI scores and a greater likelihood of hospitalization within the previous six months compared to those not using these medications. Additionally, diabetic patients are more likely to have been hospitalized in the past six months. Therefore, the prescriptions of patients on antidiabetic or antithrombotic drugs should be carefully reviewed, and these patients should be closely monitored. Our results show that patients with hospitalizations in the past six months, patients with hypertension or diabetes had higher MRCI scores, with more complex dosing schedules and instructions for use. Treatment regimen complexity and adherence patterns vary among patients with different chronic conditions. A 2017 study of outpatient heart failure patients revealed high medication regimen complexity that increased with age, with researchers noting the need for further investigation into whether regimen complexity affects medication adherence.28 Research in hypertensive patients indicated that medication regimen complexity, rather than the number of medications, was associated with treatment non-adherence.12 Despite similar medication numbers, diabetic patients exhibit higher regimen complexity than hypertensive patients.25 Considering our findings, we recommend simplifying medication dosing regimens and place a strong emphasis on explaining usage instructions during patient education especially in patients with hypertension or diabetes.
Furthermore, patients who had been hospitalized within the past six months were less likely to fully adhere to their treatment in our study. Similarly, in a Canadian study it was shown that 44% of patients were not adherent to some or all changes made to their medications at hospital discharge, and non-adherence is a risk factor for adverse events, emergency visits or readmission to hospital.29 Consistent with our findings, a study by Alves-Conceição et al demonstrated a positive association between hospital admissions, the number of medications, and MRCI scores.4 The results support the conclusion that patients with greater medication regimen complexity are at higher risk of hospitalization; notably, MRCI scores were higher among readmitted patients compared to those who were not readmitted. Therefore, we believe that medication regimen review by a pharmacist during the early post-discharge period is crucial.
The lower likelihood of full adherence to treatment among those using mineral supplements is noteworthy and requires explanation. In osteoporosis, irregular calcium intake can compromise treatment success. This may suggest that the rationale for using mineral supplements needs to be clearly explained to patients. Furthermore, considering that patients using minerals might be more prone to self-medicate, their medication regimens should be monitored closely.
Studies have shown that simplifying medication regimens —such as switching to fixed-dose combinations or once-daily dosing— can improve medication adherence in patients undergoing long-term treatment for chronic diseases.30 In some drug classes, including antianemic and thyroid medications, administration instructions regarding timing or food intake are essential to achieve optimal bioavailability and cannot be altered. Likewise, corticosteroids require strict dosing schedules to avoid adverse effects. Such non-modifiable administration requirements increase regimen complexity and may render adherence more difficult for patients. In our study, patient adherence is negatively affected by medication regimen complexity in patients using antianemia preparations. Especially, the complexity of instructions for use strongly and negatively affects patient adherence. Efforts to simplify medication regimen and utilizing once daily dosing of iron supplements might have positive effects on full adherence to therapy.
Perfect adherence to corticosteroid therapy is of utmost importance as taking higher doses than recommended can raise the risks of adverse events, while taking lower than prescribed doses or skipping a dose can compromise effectiveness as well as risking adrenal insufficiency.31 Patient adherence might be compromised due to adverse effects such as insomnia and stomach upset. Administering corticosteroids alongside meals is a common clinical recommendation, primarily intended to mitigate potential gastric irritation. Such instructions, while necessary for gastrointestinal protection, naturally increase the complexity of Section C and may subtly influence how a patient navigates their daily medication schedule. One of the alarming results of our study is that total MRCI scores and instructions for use scores were higher in patients who did not fully adhere to therapy. Complex instructions for use might affect patients’ medication taking behavior in patients using systemic corticosteroids. As the administration schedule cannot be changed and taking the drug with food is imperative, reducing the medication regimen complexity might not always be possible for these patients. Given that patient education represents a modifiable factor, we recommend strengthening educational interventions focused on the importance of adherence to corticosteroid therapy, supported by individualized information leaflets, visual aids, personalized alerts and pill organizers, and written medication schedules. The same approach may be extended to patients undergoing thyroid therapy, as higher MRCI C scores were observed among non-adherent patients and administration instructions cannot be altered. To identify patients in need of targeted education and to detect modifiable risk factors affecting adherence, regular pharmacist-led medication therapy reviews should be conducted at defined intervals.
Limitations of this study include its single-center design and small sample size. In the present study, the associations between medication adherence and clinical or regimen-related variables were primarily explored using univariable analyses. Future studies with larger sample sizes incorporating multivariable analytical approaches may better elucidate independent associations and clarify the role of potential confounding factors. This study did not focus on any specific age group. Therefore, age-specific studies may be required to identify factors influencing medication adherence that are unique to, or more relevant for, particular age groups. The results may not fully represent the general patient population. Additionally, our assessment of medication adherence relied exclusively on self-reported data, as objective measures such as pharmacy refill records or pill counts were not accessible. While the MARS-5 is a validated and practical tool, it is inherently susceptible to recall bias and social desirability. This suggests that our findings might reflect an overestimation of actual adherence levels. To minimize this effect, interviews were conducted in a private setting by pharmacists who emphasized the non-judgmental nature of the study, yet the possibility of patients providing more favorable responses than their actual behavior remains a factor to consider in the interpretation of these results.
Conclusion
Addressing adherence barriers and refining medication regimen complexity appear fundamental to improving healthcare delivery. Although this study did not identify a direct universal correlation between total complexity and self-reported adherence, simplifying dosing schedules remains a prudent strategy. Providing highly explicit instructions through targeted counseling might be particularly advisable for high-risk individuals, such as geriatric patients and those with recent hospitalizations. Our findings suggest that instead of relying on generic education, prioritized counseling should be tailored to specific MRCI components. This could include addressing the practical challenges of complex dosage forms or reducing the cognitive load of intricate administration instructions. Pharmacists can facilitate this through post-discharge regimen reviews by performing medication reconciliation to consolidate redundant therapies and simplifying dosing schedules. Focusing on these modifiable factors is likely more effective than addressing static clinical demographics. Ultimately, targeted pharmacist-led interventions during the post-discharge period might serve as a critical window for optimizing adherence and enhancing overall patient outcomes.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Guthrie B, Makubate B, Hernandez-Santiago V, Dreischulte T. The rising tide of polypharmacy and drug-drug interactions: population database analysis 1995-2010. BMC Med. 2015;13(1):1–11. doi:10.1186/s12916-015-0322-7
2. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;2014(11). doi:10.1002/14651858.CD000011.pub4
3. Wastesson JW, Morin L, Tan ECK, Johnell K. An update on the clinical consequences of polypharmacy in older adults: a narrative review. Expert Opin Drug Saf. 2018;17(12):1185–1196. doi:10.1080/14740338.2018.1546841
4. Alves-Conceição V, Rocha KSS, Silva FVN, et al. Are clinical outcomes associated with medication regimen complexity? A systematic review and meta-analysis. Ann Pharmacother. 2020;54(4):301–313. doi:10.1177/1060028019886846
5. Mansur N, Weiss A, Beloosesky Y. Looking beyond polypharmacy: quantification of medication regimen complexity in the elderly. Am J Geriatric Pharmacother. 2012;10(4):223–229. doi:10.1016/j.amjopharm.2012.06.002
6. Chisholm-Burns MA, Spivey CA. The “cost” of medication nonadherence: consequences we cannot afford to accept. J Am Pharm Assoc. 2012;52(6):823–826. doi:10.1331/JAPhA.2012.11088
7. Hirsch JD, Metz KR, Hosokawa PW, Libby AM. Validation of a patient-level medication regimen complexity index as a possible tool to identify patients for medication therapy management intervention. Pharmacotherapy. 2014;34(8):826–835. doi:10.1002/PHAR.1452
8. George J, Phun YT, Bailey MJ, Kong DCM, Stewart K. Development and validation of the medication regimen complexity index. Ann Pharmacother. 2004;38(9):1369–1376. doi:10.1345/APH.1D479
9. Alves-Conceição V, Rocha KSS, Silva FVN, Silva ROS, Silva DT, Lyra-Jr DP. Medication regimen complexity measured by MRCI: a systematic review to identify health outcomes. Ann Pharmacother. 2018;52(11):1117–1134. doi:10.1177/1060028018773691
10. Corsonello A, Pedone C, Lattanzio F, et al. Regimen complexity and medication nonadherence in elderly patients. Ther Clin Risk Manag. 2009;5(1):209. doi:10.2147/tcrm.s4870
11. Ayele AA, Tegegn HG, Ayele TA, Ayalew MB. Medication regimen complexity and its impact on medication adherence and glycemic control among patients with type 2 diabetes mellitus in an Ethiopian general hospital. BMJ Open Diabetes Res Care. 2019;7(1):e000685. doi:10.1136/BMJDRC-2019-000685
12. Wakai E, Ikemura K, Kato C, Okuda M. Effect of number of medications and complexity of regimens on medication adherence and blood pressure management in hospitalized patients with hypertension. PLoS One. 2021;16(6 June):1–10. doi:10.1371/journal.pone.0252944
13. Venditti V, Bleve E, Morano S, Filardi T. Gender-related factors in medication adherence for metabolic and cardiovascular health. Metabolites. 2023;13(10):1087. doi:10.3390/metabo13101087
14. Pantuzza LL, Ceccato MGB, Silveira MR, Junqueira LMR, Reis AMM. Association between medication regimen complexity and pharmacotherapy adherence: a systematic review. Eur J Clin Pharmacol. 2017;73(11):1475–1489. doi:10.1007/S00228-017-2315-2
15. Zeller A, Schroeder K, Peters TJ. An adherence self-report questionnaire facilitated the differentiation between nonadherence and nonresponse to antihypertensive treatment. J Clin Epidemiol. 2008;61(3):282–288. doi:10.1016/j.jclinepi.2007.04.007
16. Temeloğlu Şen E, Sertel Berk Ö, Sindel D. The validity and reliability study of the Turkish adaptation of medical adherence report scale. J Ist Faculty Med. 2019;82(1):52–61. doi:10.26650/iuitfd.413637
17. Okuyan B, Babi B, Sancar M, et al. Validation of the Turkish version of medication regimen complexity index among elderly patients. J Eval Clin Pract. 2016;22(5):732–736. doi:10.1111/JEP.12526
18. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
19. New Form Code Classification Guidelines Version 2025 | EPHMRA. Available from: https://www.ephmra.org/new-form-codes.
20. Stirratt MJ, Dunbar-Jacob J, Crane HM, et al. Self-report measures of medication adherence behavior: recommendations on optimal use. Transl Behav Med. 2015;5(4):470–482. doi:10.1007/S13142-015-0315-2
21. Jin H, Kim Y, Rhie S. Factors affecting medication adherence in elderly people. Patient Prefer Adherence. 2016;10:2117–2125. doi:10.2147/PPA.S118121
22. Lemay J, Waheedi M, Al-Sharqawi S, Bayoud T. Medication adherence in chronic illness: do beliefs about medications play a role? Patient Prefer Adherence. 2018;12:1687–1698. doi:10.2147/PPA.S169236
23. Ge L, Heng BH, Yap CW. Understanding reasons and determinants of medication non-adherence in community-dwelling adults: a cross-sectional study comparing young and older age groups. BMC Health Serv Res. 2023;23(1). doi:10.1186/S12913-023-09904-8
24. Kim SJ, Kwon OD, Han EB, et al. Impact of number of medications and age on adherence to antihypertensive medications: a nationwide population-based study. Medicine. 2019;98(49):e17825. doi:10.1097/MD.0000000000017825
25. Libby AM, Fish DN, Hosokawa PW, et al. Patient-level medication regimen complexity across populations with chronic disease. Clin Ther. 2013;35(4):385–398.e1. doi:10.1016/J.CLINTHERA.2013.02.019
26. Smaje A, Weston-Clark M, Raj R, Orlu M, Davis D, Rawle M. Factors associated with medication adherence in older patients: a systematic review. Aging Med. 2018;1(3):254–266. doi:10.1002/AGM2.12045
27. Krueger KP, Berger BA, Felkey B. Medication adherence and persistence: a comprehensive review. Adv Ther. 2005;22(4):313–356. doi:10.1007/BF02850081
28. Cobretti MR, Deininger KM, Linnebur SA, Page RL, Lindenfeld J, Aquilante CL. Medication regimen complexity in older adults with heart failure. J Heart Lung Transplant. 2016;35(4):S419–S420. doi:10.1016/j.healun.2016.01.1211
29. Weir DL, Motulsky A, Abrahamowicz M, et al. Failure to follow medication changes made at hospital discharge is associated with adverse events in 30 days. Health Serv Res. 2020;55(4):512–523. doi:10.1111/1475-6773.13292
30. Elnaem MH, Irwan NA, Abubakar U, Sulaiman SAS, Elrggal ME, Cheema E. Impact of medication regimen simplification on medication adherence and clinical outcomes in patients with long-term medical conditions. Patient Prefer Adherence. 2020;14:2135. doi:10.2147/PPA.S268499
31. Liu D, Ahmet A, Ward L, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol. 2013;9(1). doi:10.1186/1710-1492-9-30
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Adherence and Its Associated Determinants in Older Adults with Type 2 Diabetes and Cardiovascular Comorbidities
Al-Azayzih A, Kanaan RJ, Altawalbeh SM, Al-Qerem W, Smadi S
Patient Preference and Adherence 2023, 17:3107-3118
Published Date: 29 November 2023
Adherence Behaviors and Related Factors Among Elderly Hypertensive Patients in China: Evidence from the China Health and Retirement Longitudinal Study
Liu F, Chang H, Liu X
Patient Preference and Adherence 2023, 17:3539-3553
Published Date: 23 December 2023
Development and Validation of a Machine Learning Model for Predicting Medication Adherence Among Home-Dwelling Elderly Patients: A Retrospective Cross-Sectional Study
Zhang Y, Han Y, Yin X, Tian Y, Wu M
Patient Preference and Adherence 2026, 20:611334
Published Date: 19 May 2026