")
Back to Journals » Patient Preference and Adherence » Volume 13
Medication compliance and lifestyle adherence in renal transplant recipients in Kuwait
Authors Kenawy AS, Gheith O , Al-Otaibi T, Othman N, Abo Atya H, Al-Otaibi M, Nagy MS
Received 19 March 2019
Accepted for publication 25 July 2019
Published 30 August 2019 Volume 2019:13 Pages 1477—1486
DOI https://doi.org/10.2147/PPA.S209212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ahmed Saleh Kenawy,1 Osama Gheith,1 Torky Al-Otaibi,1 Nashwa Othman,2 Hasaneen Abo Atya,1 Mohamed Al-Otaibi,1 Mohamed Sobhy Nagy3
1Hamed Al-Essa Organ Transplant Center, Ibn Sina Group of Hospitals, Ministry of Health, Kuwait City, Kuwait; 2Dasman Diabetes Institute, Ministry of Health, Kuwait City, Kuwait; 3Kuwait Cancer Center, Ministry of Health, Kuwait City, Kuwait
Correspondence: Ahmed Saleh Kenawy
Hamed Al-Essa Organ Transplant Center, Ibn Sina Group of Hospitals, Pharmacy Department, Sabah Medical Area, Shuwikh, PO Box 25427, Kuwait City, Safat 13115, Kuwait
Tel +965 9 755 7486
Email [email protected]
Introduction and aim: Kidney transplantation is the optimal treatment choice for end stage renal disease; this option needs a major change in the recipients’ lifestyle and requires strict adherence to medications. The study aim was to assess the compliance of renal transplant patients to medications and lifestyle modifications in the Hamed Al-Essa Organ Transplant Center in Kuwait.
Patients and methods: One-hundred and twenty renal transplant patients were interviewed for their lifestyle behaviors after transplantation, including transplant adherence to their medications, healthy meals, personal hygiene, physical activity, regular out-patient follow up visits, and preventive measures against infection and cancer, in addition to sexual function. The questionnaire used was created by staff of the Faculty of Medicine, Mansura University, Egypt.
Results: Sixty percent of the renal transplant patients were compliant with medications and lifestyle. Risk factors associated with poor medication compliance were being Kuwaiti citizens, women, and having had unrelated living donors (p<0.05). Compliance with medications was associated with less transplant related complications (p=0.003). Only 15% of the participants were compliant with low-salt diet, 8% with low-fat, and 11% with low-carb. One fourth of patients were compliant with a daily shower and 20% were physically active. More than 70% of the patients were regularly visiting the out-patient clinic. Compliance to preventive measures against infection was observed in 85% of patients but only 5% were avoiding direct sun exposure. Half of the male patients had sexual dysfunction but only half of them were consulting their nephrologists about it.
Conclusion: Kidney transplant patients in Kuwait had moderate compliance with medications and lifestyle modifications. Closer assessment is needed to identify the risk factors before and after transplantation to avoid any complications associated with non-compliance.
Keywords: compliance, Kuwait, renal transplant
Introduction
Compliance with medication is a key factor in successful kidney transplantation.1,2 Immunosuppressive medications are crucial to the transplanted kidney as these prevent the rejection of the organ by the host immune system; consequently, poor compliance with these medications among kidney transplant patients is considered a serious healthcare problem.3
Despite its severe complications, poor adherence to medications can be found in more than 50% of kidney recipients, and the complications that result are evident as 35% or more of documented graft losses or general graft failures are caused by poor adherence to medication. In addition to using immunosuppressants, patients are required to adhere to other drugs, such as anti-hypertensives, glucose-lowering drugs, and cholesterol-lowering agents intended to treat other complications.4,5 Since hospital admissions due to medication non-compliance are frequently seen in Hamed Al-Essa Organ Transplant Center in Kuwait, it is necessary to gain greater understanding of the problem.
Renal transplant patients face higher risks than other groups of developing hyperglycemia, hypertension, and weight gain. Immunosuppressant medications such as prednisolone, mycophenolic acid, and tacrolimus have the tendency to increase blood pressure, blood glucose, cholesterol, and triglycerides. For this reason, it is important for the patient to follow a healthy lifestyle, such as eating a balanced diet and engaging in regular physical activity, as these are useful methods for decreasing these side effects and improving renal transplant outcomes by decreasing levels of interleukin-6, which stimulates inflammatory and auto-immune processes in the body.6,7
In general, transplant patients tend to be more compliant with medication than with lifestyle changes as less than 10% of renal transplant recipients are considered compliant with lifestyle modifications.8 In Hamed Al-Essa Organ Transplant Center, more than 65% of patients receive anti-hyperlipidemics, 56% receive anti-diabetics, and almost 75% of them are overweight. Consequently, it is important to assess patient adherence to the recommended lifestyle modifications to identify the causes of non-compliance.
Additionally, patients need to maintain their personal hygiene, follow up with their physician, and take vaccines on time. Adherence to outpatient visits is a significant factor for negative outcomes in transplant patients.9 Taber et al pointed out that patients who do not adhere to follow-up appointments have 1.5 times the risk of acute rejection. In addition, patients who were both medication and appointment non-adherent were at a very high risk of graft loss compared to those who were either medication or appointment non-adherent.10
There are several different methods of measuring patient compliance. Direct methods include measuring the concentration of drugs or their metabolites in the patient’s fluids; however, this method only provides information on patient adherence to specific drugs such as tacrolimus, but it is not usually used for fixed-dose medications such as mycophenolate. Direct methods also include electronic methods such as pill counting and electronic medication monitors, but this method is not widely used in hospitals. Indirect methods such as questionnaires or surveys are easy to carry out and can be used to assess patient adherence for medications and lifestyle recommendations.11
Many factors can contribute to medication or lifestyle compliance issues; these include internal factors such as age and gender and external factors such as family support and patient trust in the healthcare system. Other factors such as medication side effects and recommended food types must be considered as well.12
In the literature, there are numerous methods to improve compliance; these methods include removing unneeded medications, increasing patient satisfaction, treating depression, and patient participation in medication choice.9 Rupper et al have introduced a unique method to improve compliance; this method relies on studying the medication-taking behavior of transplant recipients who were able to preserve their kidneys for a long time as well as monitoring their daily routines and their attitudes during travel. This method can be described to non-compliant patients to help them find new ways to solve their problems.13
Aim of the study
In this study, we aimed to evaluate the patients’ compliance towards their medications, different recommended behaviors and life style, in addition to assess different risk factors for non-compliance among such patients.
Patients and methods
Study population
The study was conducted at the outpatient clinic and causality department of Hamed Al-Essa Organ transplant Center of Kuwait. The study protocol, informed consent, and study questionnaire were approved by the ethical committee of the Kuwaiti ministry of health. Kidney transplant patients were randomly selected during their follow up with the following inclusion criteria: older than 21 years, 6 months post-transplant, and ability to sign the informed consent. We have excluded mentally impaired cases and pregnant ladies.
Data collection
One hundred and twenty kidney transplant recipients were interviewed by the investigators to obtain the required data. The investigator clarified the study objectives to the patient and signed informed consent was obtained. The data were collected over 4 months between September and December 2017. Medical assessment was done after the interview to collect the data required for part 3 of the questionnaire. The participants were divided into 3 groups according to their level of compliance (good, partial, or poor) based on their responses.
Questionnaire
The used questionnaire was created by the faculty of medicine, Mansoura University, Egypt, and tested by Gheith et al to investigate the degree of patient compliance in Urology and Nephrology Center, Mansoura, Egypt.14 The questionnaire consisted of 3 parts: Part 1 included the patient history and demographic data (age, sex, transplant date, marital status and number of children, education, occupation, and income) in addition to (duration and type of dialysis, donor type, rejection episodes, and co-morbidities); Part 2 was concerned with the knowledge and attitude on the prescribed medications and recommended lifestyle behaviors of the kidney transplant recipients. This part consisted of 9 items which covered the following issues: 1) Medications: compliance with prescribed medication, familiarity with medication names and doses compared to the patient prescription, 2) Nutrition: compliance with the recommended food instructions including (number of meals, daily consumption of carbohydrates and fats, food content and nutrition behavior), 3)Daily monitoring of body parameters like body weight, temperature, blood pressure, fluid intake and output in addition to the patient’s dealing with vomiting and diarrhea, 4) Regularity of patient’s follow up visits in outpatient clinic and visits for eye and teeth checkup, 5)Patient compliance with the recommended daily hygiene, dealing with infected persons and crowded public transportation facilities, 6)Physical activities, type of sports and regularity of exercises, 7) Smocking, number of daily cigarettes, attempts to quit smoking, 8)Exposure to sun rays, using sunscreens and regular breast self-examination, and 9)Sexual activities, problems associated with it and using contraception methods (female patients).
Part 3 concerned with routine clinical and laboratory assessment such as body weight, temperature, pulse, blood pressure, urine output, serum creatinine, and blood glucose level.
The questions were rated on a 4-point scale ranging from zero (never) to 3 (always) to determine the level of compliance of kidney transplant patients. This level was determined by a scale between zero and 100: those with scores less than 50% were poorly compliant, those with score between 51 and 80% were partially compliant, and those with scores more than 80% had good compliance. (Table 1)
 |
Table 1 Questions and rating system of medication compliance questionnaire |
The questionnaire results of the first 20 participants were analyzed by spss to assess reliability and validity with the following results: Cronbach s alpha =0.73, Pearson correlation (r) for the questions >0.444 (p=0.05).
Statistical analyses
SPSS software (Statistical Package for the Social Sciences, version 22) was used for data analysis. All reported data were considered significant if p<0.05. Unpaired T-test and ANOVA were used for continuous variables; the chi-square test was used for discrete variables. Binary and multinomial logistic regressions were used to explain the relationship between variables.
Results
Out of 133 patients approached by the investigators, 120 patients were eligible for enrollment in our study and further data collection. The majority of the participants (82.5%) were males, and almost 64% were married. Kuwaiti citizens represented 59% of the subjects, and most of the patients did their follow-up appointments for more than 8 years at Hamed Al-Essa Organ Transplant Center. Patient demographic data are summarized in Table 2.
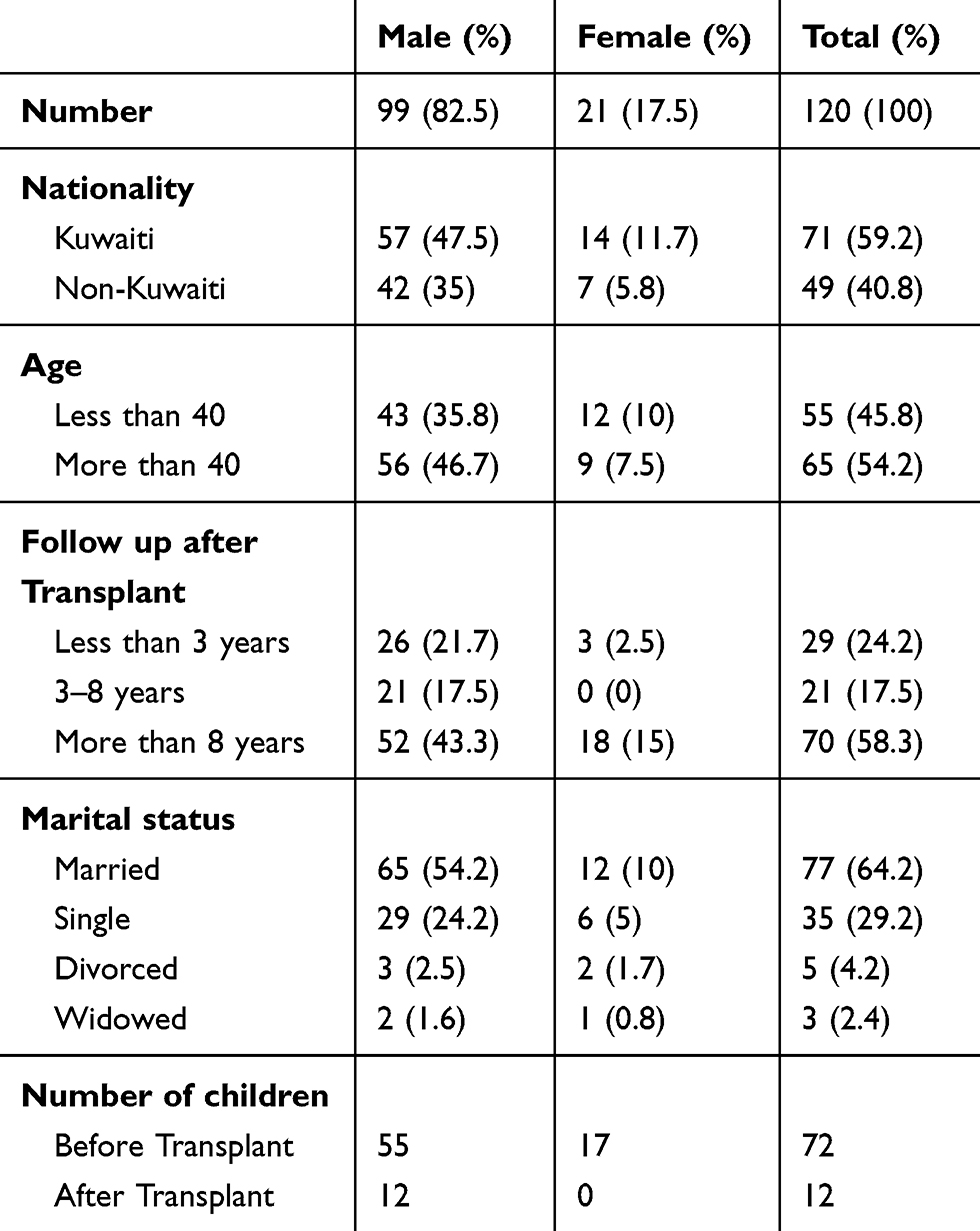 |
Table 2 Patients’ demographic data |
Before the transplant, hemodialysis was the most prominent method of dialysis used among patients. The most frequent post-transplant complications reported by participants were hypertension (27.5%), graft rejection (25.8%), and chest infections (22.5%). Half of the male patients had sexual dysfunction, but only half of them had consulted their nephrologists about it. More than 60% of women had regular menstrual cycles post-transplant. Table 3 summarizes pre- and post-transplant patients’ co-morbidities.
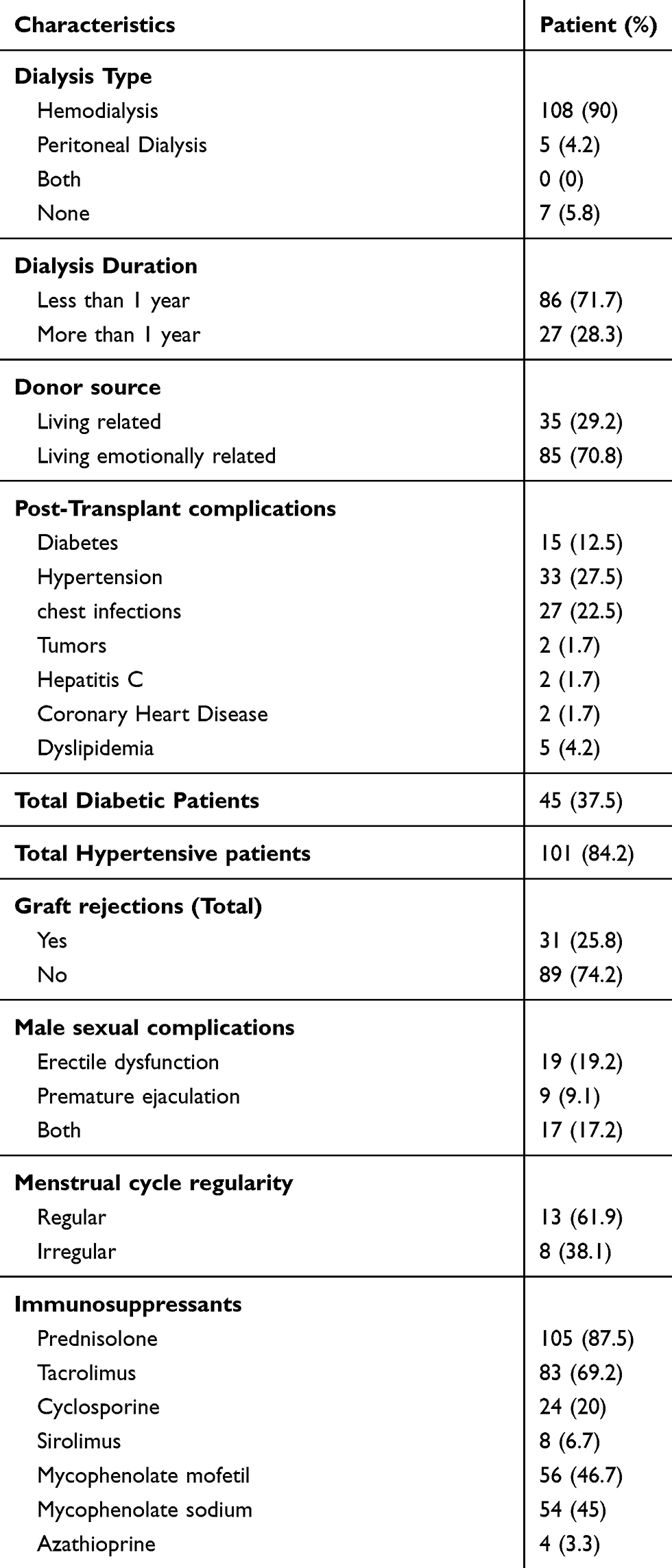 |
Table 3 Pre- and post-transplant patients’ co-morbidities and Immunosuppressants |
The majority of our patients (60%) were compliant with both medications and diet modifications, 25% were partially compliant, and 15% were poorly compliant. Forgetfulness was mentioned by 81% of the participants as the main reason for not taking their medications, 16% chose to not take medications, and 3% believed that medications have a lot of side effects. Of the partially and poorly compliant patients, 70% had issues with all types of their medications, 5% with their immunosuppressant agents and 30% with other types of medications. Kuwaiti citizens were more likely to be non-compliant with their medications than non-Kuwaiti patients (p=0.041; Exp(B) =3.5; 95% CI [1.051–11.66]). Live unrelated donation recipients and patients older than 40 had a 9 and 3 times higher chance of being non-compliant than live related donation recipients and younger patients, respectively (p=0.037 and 0.025, respectively; Exp(B) =9.04 and 3.64, respectively; 95% CI [1.136–71.97 and 1.17–11.3, respectively]). Males were more likely to be compliant than females (p=0.001; Exp(B) =0.117; 95% CI [0.032–0.436]). Other factors are mentioned in Table 4.
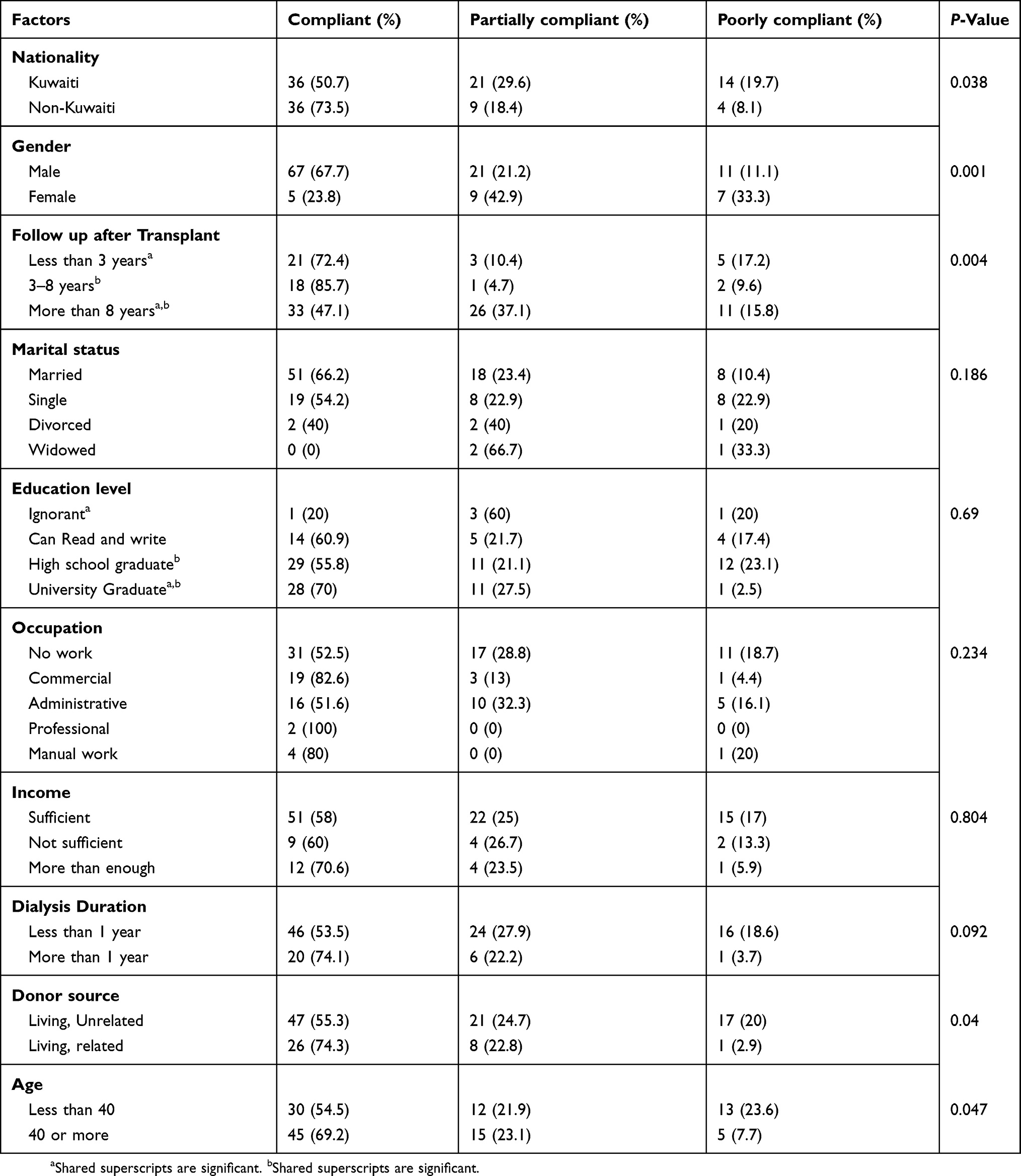 |
Table 4 Factors affecting compliance and their significance |
Regarding diet instructions, the majority of the poorly compliant patients (80%) did not like the prescribed food, and 11% stated that no one had clarified the food instructions to them after the transplant. Nearly 47.5% of the patients were compliant with calcium-rich meals, 32.5% with low-salt diets, and 16.7% with low-fat diets (Table 5).
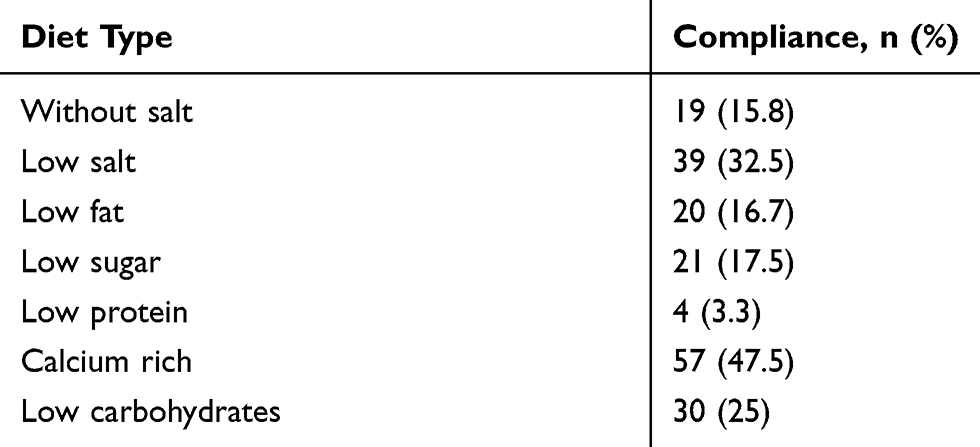 |
Table 5 Types of diets and patient compliance |
The number of daily prescribed medications had no significant impact on patient compliance (p=0.8). Poorly compliant patients had significantly more post-transplant complications, higher mean serum creatinine, higher mean serum cholesterol, and lower mean hemoglobin (p<0.05). We found that poorly compliant participants had higher number of second transplant cases. Non-compliant patients had a higher chance of a rejection episode than compliant patients (p=0.032; Exp(B) =3.314; 95% CI [1.106–9.934]). Compliant patients had a better chance of being free from transplant complications (such as diabetes and hypertension) than non-compliant patients (p=0.018; Exp(B) =3.76; 95% CI [1.26–11.22]) (Tables 6 and 7).
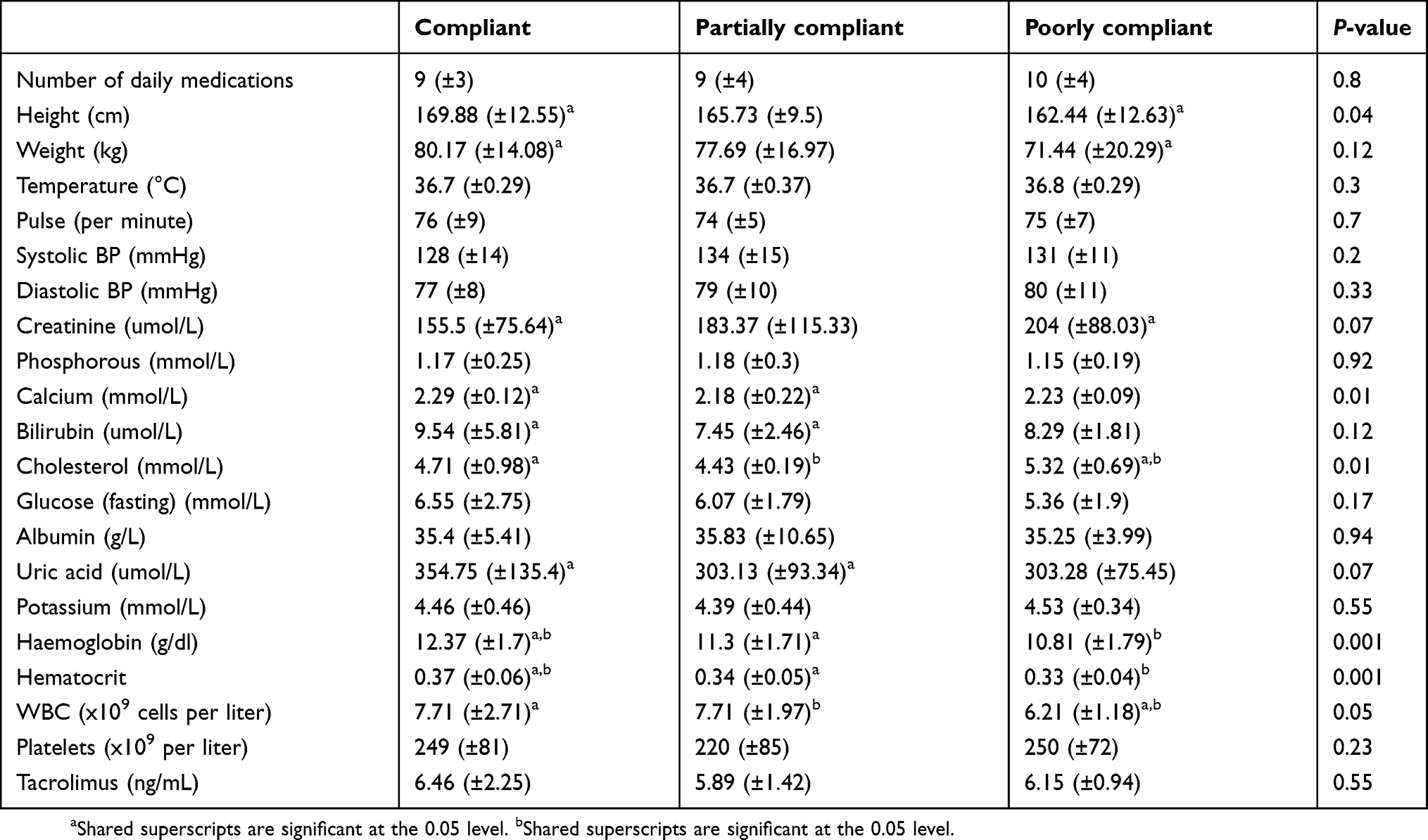 |
Table 6 Medical checkup and laboratory results (medication compliance) |
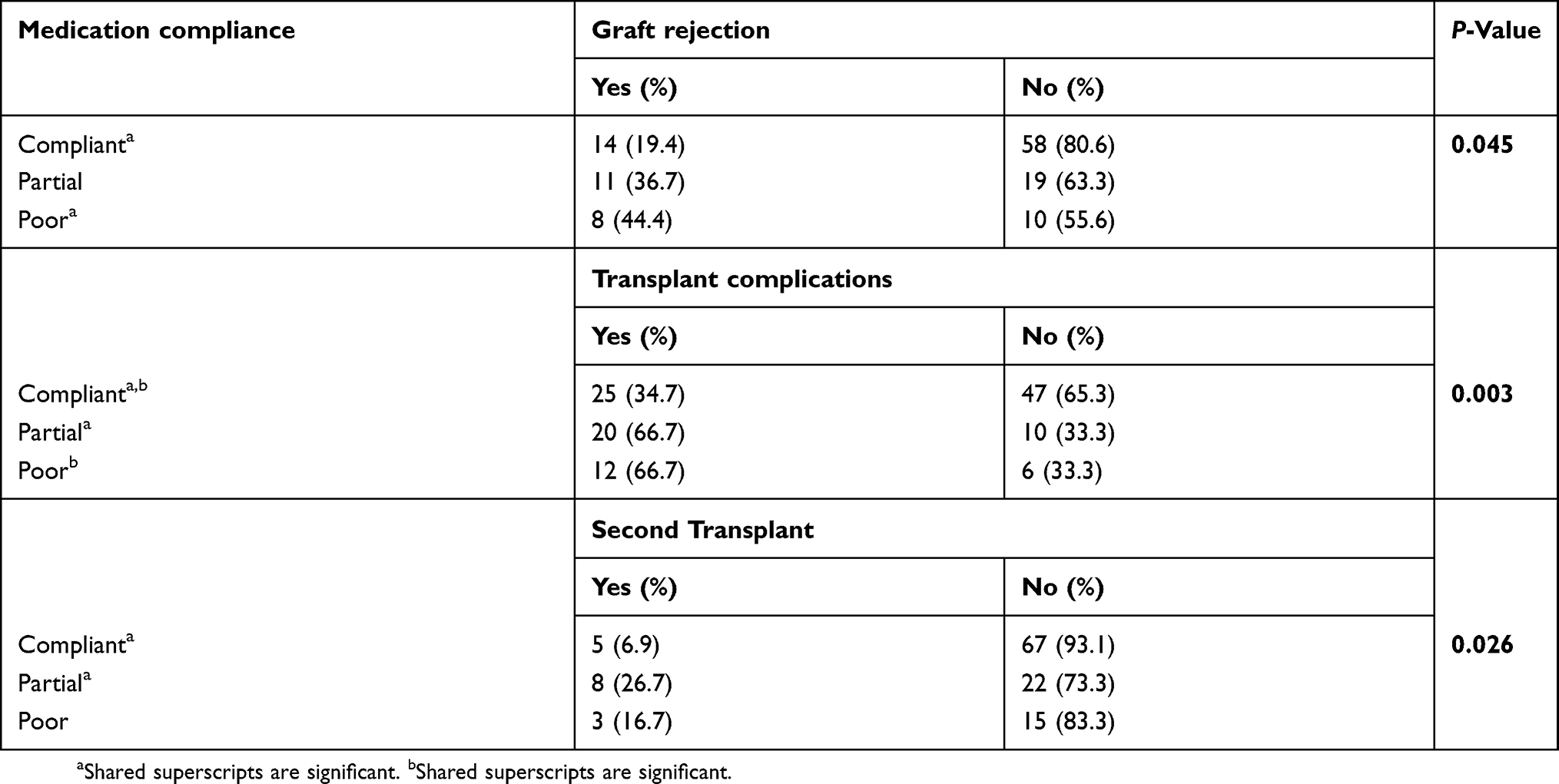 |
Table 7 Graft rejection and transplant complications after transplant |
Compliance with daily measurement of blood pressure, body temperature, fluid intake, urinary output, and body weight were observed in 44%, 31%, 25%, 26% and 17% of the participants, respectively, and 73% of the patients visited their nephrologists regularly.
The reasons for irregular outpatient visits mentioned by half of the patients included having enough medication while the other half reported problems with their work schedule. None of the patients visited a dermatologist for regular checkups, and only 8% had their eyes checked periodically. Only 40% of women used correct hygiene methods after sex, and 60% used good hygiene during their menstrual periods.
We observed that most of the patients (86%) did not use crowded transportation. Additionally, the percentages of patients who brushed their teeth before sleep and after every meal were 60% and 55%, respectively. Only 11% of the participants used sunblock to guard against skin cancer. Nine patients were smokers, most of whom had tried to quit and failed. Moreover, 56% of the patients were physically active, but only 21% of them engaged in regular exercise.
Discussion
Despite using several methods to improve medication compliance, it still represents a challenge for renal transplant patients. Non-adherence to immunosuppressants is a major risk factor for poor outcomes in renal transplant recipients and so has gained increasingly more research attention as an issue that needs tackling.15 Determining risk factors of poor compliance is crucial as it can help in recognizing high-risk patients before transplant and enable physicians to offer proper compliance education. Previous studies have provided some information about these risk factors, but the inconsistency of the effect of these factors on compliance, in addition to the different socio-economic structure of the country, complicate the application of these results for kidney transplant patients in Kuwait.16
In this study, 60% of the patients complied well with diet instructions and medications, including immunosuppressant agents; this result was lower than that in previous reports, which demonstrated good compliance (between 72% and 78%) among kidney transplant patients.4,5,17 Our finding was also far lower than the prevalence of good compliance noticed by Gheith et al, with 97% compliance with immunosuppressants.14
The multi-national nature of renal transplant patients in Kuwait has necessitated the analysis of compliance according to nationality. In our results, we observed that Kuwaiti nationality was a significant risk factor in non-compliance. Lemay et al point out that Kuwaiti patients are inclined to have negative beliefs toward medications, and their level of medication compliance was lower than that of other nationalities.18 The Kuwaiti lifestyle may be another reason for non-compliance as many Kuwaitis are accustomed to traveling abroad more than twice a year, and these trips might affect their ability to take their medications regularly.13 It is crucial to consider these factors during the treatment process of Kuwaiti patients. Inaccurate beliefs about medication need to be corrected, and a full understanding of the treatment regimen needs to be ensured before discharge.
The effect of gender on compliance was not consistent with previous studies; male patients were more compliant than females in Gheith et al’s report while young females were more adherent to medications in Boucquemont et al.14,19 The male patients in our study were also more compliant than the female patients. The varying responsibilities of the genders in Kuwaiti society might have a role in their compliance behavior. Male patients usually have more support from their wives and other family members regarding medication timing while family issues and obligations might prevent female patients from being compliant with their medications.
Adherence to long-term medications usually decreases over time, which is because of the presence of little or no change in the patient’s health condition.20 The results of Gheith et al did not prove this as post-transplant follow-up time did not affect patient compliance in their study.14 In contrast, our results showed that patients at 8 years or more post-transplant were less compliant than other groups. This outcome highlights the importance of continuous follow up with all patients, including stable cases. Physicians and pharmacists need to frequently discuss the importance of medications and their role in maintaining the patient’s condition in addition to assessing patient adherence from time to time.
In addition to the previously mentioned factors, higher education levels significantly affected compliance rates. Fido and Husseini report and Al-Majed et al linked lower education levels to increased non-compliance rates in psychiatric and diabetic patients in Kuwait.21,22 Additionally, Loghman-Adham found that lower education levels in patients with chronic diseases decreased their compliance with medication.23 In our study, we observed that education levels explained the difference in compliance rates between Kuwaiti and non-Kuwaiti patients. It was higher as 37% in non- Kuwaiti patients who had a high level of education (university level in most) compared to only 29% in Kuwaiti patients with middle level of education in most.
Our study results were consistent with the majority of previous reviews showing that compliance has an inverse relationship with age.24 The percentage of non-compliance was significantly higher in patients younger than 40 years old; this finding matched with that reported by Ghods et al, who observed similar findings in patients aged 35 years or younger. Their general conclusion was that younger patients are less compliant with medications than other age groups.25 Cochat et al mention that the desire to feel normal and live freely without obstacles, in addition to avoiding side effects such as obesity and acne, may give younger patients the courage required to challenge medical advice by not taking their medications.26 In addition to these reasons among younger patients, it has been found that extra care must be taken with older patients, who might have cognitive or sensory impairments.27
Unlike age and education level, the donor source has conflicting effects on compliance. The donor source did not affect compliance rates in Tielen et al’s report; on the other hand, patients with related donors were more compliant in Gheith et al, possibly due to regular visits from relatives (including the donor), and this associated family support is likely to have a role in increasing patient compliance.14,28
Renal transplant patients tend to be less compliant with nutritional and lifestyle modifications than with medications. The belief that medications are more important than other measures might be the cause of this attitude.29 Although diet modifications are essential for these patients, more than 10% of the non-compliant patients mentioned that they did not receive any dietary instructions. This finding indicates that more attention to nutritional guidance is needed from medical caregivers, and it might be helpful to integrate nutritional instructions into the requirements that need to be fulfilled before discharge.
In our study, 25% of the patients complied well with low-carbohydrate diets, and 16.7% were adherent to a low-fat diet. These compliance results were lower than Alsayed et al’s and Gheith et al’s, who demonstrated 23% and 50% compliance rates, respectively.8,14 Financial factors also need to be considered in determining a patient’s ability to be compliant with lifestyle modifications because low-fat and low-carbohydrate food is usually more expensive than other alternatives. Surprisingly, the high income levels in Kuwait, in addition to the availability of many low-fat and low-carbohydrate products, did not increase patient compliance to the nutritional modifications. Lack of family support, less palatable food products, and improper follow up from physicians might be the causes behind this result.14
Only 21% of our patients exercised regularly, which was considerably fewer than Talas et al, who observed that more than 50% of patients in their sample exercised regularly.30 The low prevalence of regular exercise among our patients may be explained by the unsuitably hot weather during most days in summer and spring. Methods such as tailoring exercise regimens according to patient condition, organizing group exercise, and asking patients about their physical activities during follow-up visits may improve adherence to physical activity.31
In this study, more than 25% of the participants were partially or non-compliant with their appointments, and 16% of the patients were partially or non-compliant with medications and appointments. These results were higher than Yavus et al’s, in which fewer than 20% of patients were partially compliant.32 This may be explained by the travel habits of patients in Kuwait, which can make them miss their appointments, or to the lack of proper education before discharge. Those with a high risk of graft loss need to be targeted by medical caregivers to provide the required support to improve patient compliance and prevent negative outcomes.
Kuwait has sunny, hot weather during summer and spring; for this reason, physicians need to inform patients about the importance of sunblock to protect themselves from skin cancer and encourage periodic skin examinations for early detection as transplant patients have a higher risk of skin cancer compared to other patients.33 In our study, only 11% of the patients used sunblock. In previous studies, compliance with skin protective measures was reported between 30% and 60%.34 Our lower prevalence may be explained by factors related to culture and religion, which restrict sun exposure; moreover, the use of sunblock protection is not common in Middle Eastern societies.
Patients with sexual problems or depression need to be more open about discussing these issues with their nephrologists as the presence of these issues can affect patient compliance with medications and out-patient visits.21 In our study, we found that half of the male patients were suffering from sexual problems. This may be related to lower haemoglobin (HB) in the poorly compliant group or to associated post-transplant complications. This result was consistent with Wong et al, who demonstrated similar results.35 Physicians need to encourage their patients to discuss these issues in order to find appropriate solutions as only half of them consulted their nephrologists about their sexual problems. The patients’ sense of shame and their belief that there is no adequate treatment for transplant patients may play a role in their refusal to talk to their doctors.
As in previous studies, the effects of compliance on transplant complications and graft rejection were apparent. Good compliance led to a significant reduction (32%) in post-transplant complications, a 25% reduction in acute rejection episodes, and a 20% reduction in second transplants. The effect of compliance was close to Folkmane et al, who showed a 25.1% reduction in acute rejection episodes and a 22.8% reduction in chronic allograft dysfunction rates in compliant patients.16
Medication-compliant patients had significantly lower serum creatinine; this result was consistent with Lalić et al, who verified higher estimated glomerular filtration rates in the adherent group.36 Compliant patients also had significantly lower cholesterol, higher hemoglobin, and higher calcium levels than the other groups in this study, which is likely due to their adherence to other medications such as vitamins and cholesterol-lowering agents.
Conclusion
Our study sample of kidney transplant patients had non-satisfactory adherence to medications and lifestyle modifications. Risk factors of non-compliance among our patients included younger age, female gender, and patients with a non-related donor. These risk factors need to be dealt with early to prevent any compliance-related complications.
Acknowledgment
This study owes its existence to the help and support of all the members of Hamed Alessa Organ Transplant Center, Kuwait. Special thanks go to the Casualty Department that provided the assistance needed for data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Oniscu G, Brown H, Forsythe J. How great is the survival advantage of transplantation over dialysis in elderly patients? Nephrol Dial Transplant. 2004;19(4):945–951. doi:10.1093/ndt/gfh022
2. Theofilou P. Identifying risk factors associated with compliance to medication in elderly kidney transplant patients. J Transplant Technol Res. 2012;2:e109. doi:10.4172/2161-0991.1000e109
3. Kamran F. Factors of non-compliance in renal transplant recipients: a systematic review. J Behav Sci. 2015;25(2):65–82.
4. Denhaerynck K, Dobbels F, Cleemput I, et al. Prevalence, consequences, and determinants of nonadherence in adult renal transplant patients: a literature review. Transplant Int. 2005;18(10):1121–1133. doi:10.1111/j.1432-2277.2005.00176.x
5. Butler JA, Roderick P, Mullee M, Mason JC, Peveler RC. Frequency and impact of nonadherence to immunosuppressants after renal transplantation: a systematic review. Transplantation. 2004;77(5):769–776. doi:10.1097/01.tp.0000110408.83054.88
6. National Kidney Foundation. Nutrition and transplant; 2018. Available from: https://www.kidney.org/nutrition/transplant.
7. Takahashi A, Hu SL, Bostom A. Physical activity in kidney transplant recipients: A review. Am J Kidney Dis. 2018;72(3):433–443. doi:10.1053/j.ajkd.2017.12.005
8. El Said SH, Abd El-Raouf SE, El-Dahashan KF, Gad R. Lifestyle modification among post renal transplant recipients. IOSR J Nurs Health Sci. 2017;6(3):92–113. doi:10.9790/1959-06030792113
9. Cukor D. Adherence in kidney transplant recipients. Am J Nephrol. 2017;45(1):89–90. doi:10.1159/000455389
10. Taber DJ, Fleming JN, Fominaya CE, et al. The impact of health care appointment non-adherence on graft outcomes in kidney transplantation. Am J Nephrol. 2017;45:91–98. doi:10.1159/000453554
11. Zullig LL, Mendys P, Bosworth HB. Medication adherence: A practical measurement selection guide using case studies. Patient Educ Couns. 2017;100(7):1410–1414. doi:10.1016/j.pec.2017.02.001
12. Hedayati P, Shahgholian N, Ghadami A. Nonadherence Behaviors and Some Related factors in kidney transplant recipients. Iran J Nurs Midwifery Res. 2017;22(2):97–101. doi:10.4103/ijnmr.IJNMR_220_15
13. Ruppar TM, Russell CL. Medication adherence in successful kidney transplant recipients. Prog Transplant. 2009;19(2):167–172.
14. Gheith OA, EL-Saadany SA, Abuo Donia SA, Salem YM. Compliance with recommended life style behaviors in kidney transplant recipients. Iran J Kidney Dis. 2008;2(4):218–226.
15. Denhaerynck K. Exploring risk factors of non-adherence to immunosuppressive medication in kidney transplant recipients: improving methodology & reorienting research goals; 2006. Available from: https://edoc.unibas.ch/573/.
16. Folkmane I, Adamsone I, Bicans J, Babarykin D, Amerika D, Rozental R. Clinical impact of non-compliance after renal transplantation. Acta Med Litu. 2008;15(4):216–221.
17. Takemotoa SK, Pinskya BW, Schnitzlera MA, et al. A retrospective analysis of immunosuppression compliance, dose reduction and discontinuation in kidney transplant recipients. Am J Transplant. 2007;7(12):2704–2711. doi:10.1111/j.1600-6143.2007.01966.x
18. Lemay J, Waheedi M, Al-Sharqawi S, Bayoud T. Medication adherence in chronic illness: do beliefs about medications play a role? Patient Prefer Adherence. 2018;12:1687–1698. doi:10.2147/PPA.S169236
19. Boucquemont J, ALH P, Dharnidharka VR, Hebert D, Furth SL, Foster BJ. Gender differences in medication adherence among adolescent and young adult kidney transplant recipients. Transplantation. 2018. https://www.ncbi.nlm.nih.gov/pubmed/29994983.
20. Kalogianni A. Factors affect in patient adherence to medication regimen. Health Sci J. 2011;5(3):157–158.
21. Fido A, Husseini A. Noncompliance with treatment among psychiatric patients in Kuwait. Med Princ Pract. 1998;7:28–32. doi:10.1159/000026019
22. Al-Majed HT, Ismael AE, Al-khatlan HM, El-Shazly MK. Adherence of type-2 diabetic patients to treatment. Kuwait Med J. 2014;46(3):225–232.
23. Loghman-Adham M. Medication noncompliance in patients with chronic disease: issues in dialysis and renal transplantation. Am J Manag Care. 2003;9(2):155–171.
24. Butler JA, Peveler RC, Roderick P, Smith PW, Horne R, Mason JC. Modifiable risk factors for non-adherence to immunosuppressants in renal transplant recipients: a cross-sectional study. Nephrol Dial Transplant. 2004;19(12):3144–3149. doi:10.1093/ndt/gfh505
25. Ghods AJ, Nasrollahzadeh D. Noncompliance with immunnosuppressive medications after renal transplantation. Exp Clin Transplant. 2003;1(1):39–47.
26. Cochat P, De Geest S, Ritz E. Drug holiday: a challenging child– adult interface in kidney transplantation. Nephrol Dial Transplant. 2000;15:1924–1927. doi:10.1093/ndt/15.12.1924
27. Majchrzak TA, Chakravorty A Improving the compliance of transplantation medicine patients with an integrated mobile system.
28. Tielen M, Van Exel J, Laging M. el al. Attitudes to medication after kidney transplantation and their association with medication adherence and graft survival: a 2-year follow-up study. J Transplant. 2014;2014:1–9. doi:10.1155/2014/675301
29. Zeltzer SM, Taylor DO, Tang WH. Long-term dietary habits and interventions in solid-organ transplantation. J Heart Lung Transplant. 2015;34(11):1357–1365. doi:10.1016/j.healun.2015.06.014
30. Talas MS, Bayraktar N. Kidney transplantation: determination of the problems encountered by Turkish patients and their knowledge and practices on healthy living. J Clin Nurs. 2004;13:580–588. doi:10.1111/j.1365-2702.2004.00966.x
31. Gordon EJ, Prohaska T, Siminoff LA, Minich PJ, Sehgal AR. Needed: Tailored exercise regimens for kidney transplant recipients. Am J Kidney Dis. 2005;45(4):769–774. doi:10.1053/j.ajkd.2005.01.002
32. Yavuz A, Tuncer M, Erdogan O, et al. Is there any effect of compliance on clinical parameters of renal transplant recipients? Transplant Proc. 2004;36:120–121. doi:10.1016/j.transproceed.2003.11.052
33. Bordea C, Wojnarowska F, Millard PR, Doll H, Welsh K, Morris PJ. Skin cancers in renal-transplant recipients occur more frequently than previously recognized in a temperate climate. Transplantation. 2004;77(4):574–579. doi:10.1097/01.tp.0000108491.62935.df
34. Mahé E, Morelon E, Fermanian J, et al. Renal-transplant recipients and sun protection. Transplantation. 2004;78(5):741–744. doi:10.1097/01.tp.0000131818.24302.b8
35. Wong JA, Lawen J, Kiberd B, Alkhudair WK. Prevalence and prognostic factors for erectile dysfunction in renal transplant recipients. Can Urol Assoc J. 2007;1(4):383–387. doi:10.5489/cuaj.446
36. Lalić J, Veličković-Radovanović R, Mitić B, Paunović G, Cvetković T. Immunosuppressive medication adherence in kidney transplant patients. Med Prin Pract. 2014;23(4):351–356. doi:10.1159/000362792
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.