Back to Journals » Advances in Medical Education and Practice » Volume 16
Medical Students’ Perceptions of the Learning Environment in South Asia: A Systematic Review of Quantitative Studies
Authors Stanikzai MH ![]() , Stanikzai KA, Shanawa S, Sayam H
, Stanikzai KA, Shanawa S, Sayam H
Received 22 June 2025
Accepted for publication 27 October 2025
Published 31 October 2025 Volume 2025:16 Pages 2013—2023
DOI https://doi.org/10.2147/AMEP.S548871
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Muhammad Haroon Stanikzai,1 Khalid Ahmad Stanikzai,2 Samiullah Shanawa,1 Hadia Sayam2
1Department of Public Health, Faculty of Medicine, Kandahar University, Kandahar, Afghanistan; 2Department of Clinic, Faculty of Medicine, Malalay University, Kandahar, Afghanistan
Correspondence: Muhammad Haroon Stanikzai, Department of Public Health, Faculty of Medicine, Kandahar University, District # 10, Kandahar, 3801, Afghanistan, Tel +93704775578, Email [email protected]
Background: Measuring students’ perceptions of the learning environment has become widespread in medical education, with many benefits for both students and institutions. Despite its documented findings in small studies, there is a lack of systematic evidence on medical students’ perceptions of the learning environment in South Asian countries.
Objective: This systematic review aimed to determine the perceptions of medical students of the learning environment in South Asia and to identify the factors that influence these perceptions.
Methods: We limited this systematic review to studies published between 2000 and 2024 which reported on medical students perceptions of the learning environment in eight South Asian countries. Perceptions of the learning environment were assessed through self-rating scales in the included studies. Articles were retrieved from two electronic databases (PubMed and Scopus). In addition, we searched Google Scholar to identify relevant articles. This review was conducted in accordance with the PRISMA guidelines.
Results: Of 1191 identified articles, 15 studies fulfilled the pre-specified eligibility criteria and were included in the review. The Dundee Ready Education Environment Measure (DREEM) was the main instrument used in these studies. Of the 15 studies included, 13 studies reported a positive perception of the learning environment in South Asia. However, positive perception levels varied widely, reflecting disparities in learning environments across countries. Additionally, the influence of several factors (eg gender, education levels, and place of residence) on the perceptions of the learning environment was highlighted.
Conclusion: Results from this review suggest that medical students perceived the learning environment positively in most studies documented from the region. However, medical schools’ learning environments in this region have a lot of room for growth and development to meet the standards set on a global scale. Moreover, the current state of the literature underscores the need for further research on the topic and on the best strategies to optimize the learning environment for medical education in South Asia.
Keywords: learning environment, educational environment, perceptions, medical education, South Asia
Introduction
Over the past two decades, numerous policies and initiatives, such as curriculum reforms, faculty development programs, optimization of learning environments, the integration of technology-based learning, and accreditation systems, have been introduced to improve the quality of medical education in various contexts.1–5 Several previous studies have highlighted the crucial role of the learning environment in medical education and how its contribution to the learning experience can lead to high-quality medical education.1–3 The World Federation for Medical Education (WFME) also recognizes that the highest attainable standard of learning environment is a fundamental component of quality medical education.6
The medical school learning environment encompasses the physical, social, and psychological context that can shape students’ learning experiences.2,7 Previous studies have shown that the learning environment significantly influences students’ academic performance, satisfaction, and attitude.8,9 In recent years, students’ perceptions of the learning environment have been widely used to evaluate learning environments across countries.9 There is also a well-established body of educational literature on the role of students’ perceptions in enhancing learning environments and their effect on student learning.10,11
Over the past decades, several scales have been developed to assess learning environment perceptions from different stakeholders’ perspectives.12 Some of the most widely used scales in medical school settings are the Dundee Ready Education Environment Measure (DREEM), the Medical School Learning Environment Scale–Short Version (MSLES), the Johns Hopkins Learning Environment Scale (JHLES), and the Clinical Learning Environment Scale (CLES).12 These self-assessment tools are designed to measure perceptions across multiple dimensions of the learning environment, such as teaching, learning, self-perception, physical atmosphere, student–teacher interaction, student–student interaction, patient–student interaction, and social perception.12 However, there are marked variations among scales with respect to domains and interpretations.12,13
Published literature concerning students’ perception of the learning environment in medical school settings has shown varying results. For instance, a systematic review of 40 studies in Saudi Arabia found that health professional students overall had a positive perception of their learning environment.14 Similarly, a nationwide survey in Hungary found that medical and dental students had a more positive than negative perception of the learning environment, suggesting an overall satisfaction with the learning environment.15 Other educational literature from different countries has highlighted the varying degrees of satisfaction with the learning environment among medical students.1,8,9,16–18 Furthermore, a number of factors (eg gender, education levels, academic performance, and funding source for education) that could potentially influence students’ perception of the learning environment have been documented.1,14,16–18
There is evidence that assessing the learning environment has the potential benefit of improving the quality of medical education.9,19,20 This is of particular importance in countries where substandard medical education is commonplace. For example, South Asian nations (India, Sri Lanka, Afghanistan, Pakistan, Bangladesh, Nepal, Bhutan, and the Maldives) could consider these learning environment initiatives to improve the quality of medical education.21 A growing body of literature shows that the burden of several diseases is exceptionally high in this region.22,23 Moreover, limited capacity and insufficient numbers of medical doctors have been identified as other health sector challenges in these settings.24 A critical factor contributing to these poor health outcomes is the state of medical education and training, which directly affects healthcare service delivery, workforce competency, and access to quality care.21,25 Taken together, these points emphasize the importance of enhancing the quality of medical education in South Asian countries. As an example, poor-quality medical education has necessitated the exploration of learning environment initiatives as a potential solution, particularly in resource-limited settings.2
Several studies have examined medical students’ perceptions of their learning environment in South Asia.26–30 However, a comprehensive systematic review focusing on these perceptions is lacking. Therefore, our systematic review aimed to determine the perceptions of medical students of their learning environment in South Asian medical schools and identify the factors influencing these perceptions. These findings will inform the development of region-specific medical education policies to enhance students’ learning experiences in these settings. Further, this review will also highlight key areas for future research.
Methods
This systematic review was reported according to the “Preferred Reporting Items for Systematic review and Meta-Analysis” (PRISMA) guidelines, and has been registered on PROSPERO (CRD42023461971).31
Data Sources and Search Strategy
English-language studies were searched in electronic databases (PubMed and Scopus). Articles published earlier than 2000 did not match the inclusion criteria (as most learning environment scales were developed from 2000 onwards). To report on a broader scope of available information, we extended the search until December 2024. In addition, we searched Google Scholar to identify relevant articles.
In this search, the key words consisted of “Perception”, “learning environment”, and “educational environment”, for the outcome; “medical student”, “resident”, and “medical undergraduate”, for the population, and “Afghanistan”, “Bangladesh”, “Bhutan”, “India”, “Maldives”, “Nepal”, “Pakistan”, “Sri Lanka”, and “South Asia”, for the location. These terms were used in all searches with the appropriate truncations and Boolean operators (such as AND and OR) (see S1B).
Inclusion and Exclusion Criteria
Our eligibility criteria were: (1) publication type: original research, (2) study design: quantitative studies utilizing self-ratings measures to assess medical students’ perceptions of the learning environment, (3) population: medical students (4) location: studies conducted in South Asia, (5) language: English (facilitate comprehension and analysis), and (6) published between 2000 and December, 2024. We excluded articles that (1) were case reports and case series, (2) focused on a single domain of the learning environment, and (3) assessed perceptions of the virtual (online) learning environment.
Screening and Selection
Our total identified records were 1191. Initially, 592 duplicate records were removed. Second, at the title and abstract screening level, we excluded 576 more records due to our ineligibility criteria. Furthermore, 5 studies were excluded for either assessing only a single domain of the learning environment or not utilizing a structured scale to measure perceptions, leaving 18 pertinent studies for full review. Following a thorough examination of the records, we noticed that 3 studies did not match our inclusion criteria. Finally, we selected all the remaining 15 articles to be reviewed (Figure 1).
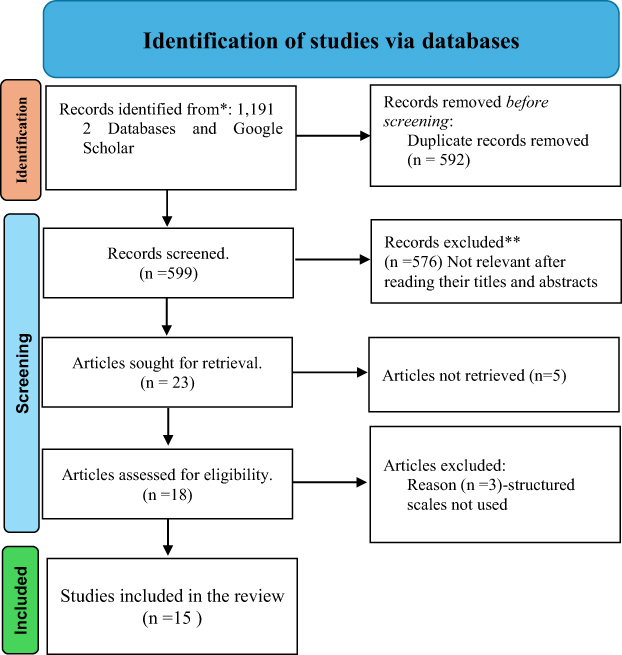 |
Figure 1 A PRISMA flow diagram of the article’s selection procedure. |
Data Extraction
Two reviewers (M.H.S and S.S) extracted data on the publication year, country setting, institution name, phases of medical education, sample size, measurement scale, and outcomes reported. The primary outcome was the perception of learning environment measured by a self-rating scale. Secondary outcomes were the perceptions regarding learning environment dimensions and factors influencing medical students’ perceptions of the learning environment in general (see S1A).
Quality Assessment
At the initial data extraction phase, all studies were found to be cross-sectional in design. Therefore, the methodological quality of the reviewed studies was evaluated by the Joanna Briggs Institute (JBI) checklist for cross-sectional studies.32 This consists of 8 items to assess the quality of cross-sectional research related to study design, measurements, and statistical analysis. All studies were rated by two senior researchers (M.H.S and H.S) on the JBI checklist. Discrepancies were solved by team discussion. The details of the JBI checklist for grading cross-sectional studies are summarized in S2.
Data Analysis and Data Synthesis
Due to the heterogeneity in the included studies in terms of medical education phases and measures of learning environment perception, a meta-analysis was not conducted. Therefore, the key findings of each included study were narratively summarized in Tables, which included publication year, country setting, institution name, medical education phase, sample size, measures, and key results.
Results
Characteristics of the Included Studies
Table 1 summarizes the characteristics of the included studies. Of the 15 studies included in this review, 6 were conducted in India,16,33–36 five in Pakistan,17,18,26,28–30,37 two in Sri Lanka,26,29 and there was one each in Nepal,38 and Bangladesh.39 We found no studies from Bhutan, Afghanistan, and Maldives. The majority of the studies (10 articles; 66%) were conducted on medical students’ learning environment in general. The remaining 5 (34%) studies included medical students at diverse phases of their education, such as curricula transition phase (2; 13%), clinical rotation phase (2; 13%), and clinical posting (1; 8%). The latter perceptions were often evaluated in a specific context. While the sample size of the studies varied greatly, it ranged from 100 to 300 in the majority of the papers (65%).
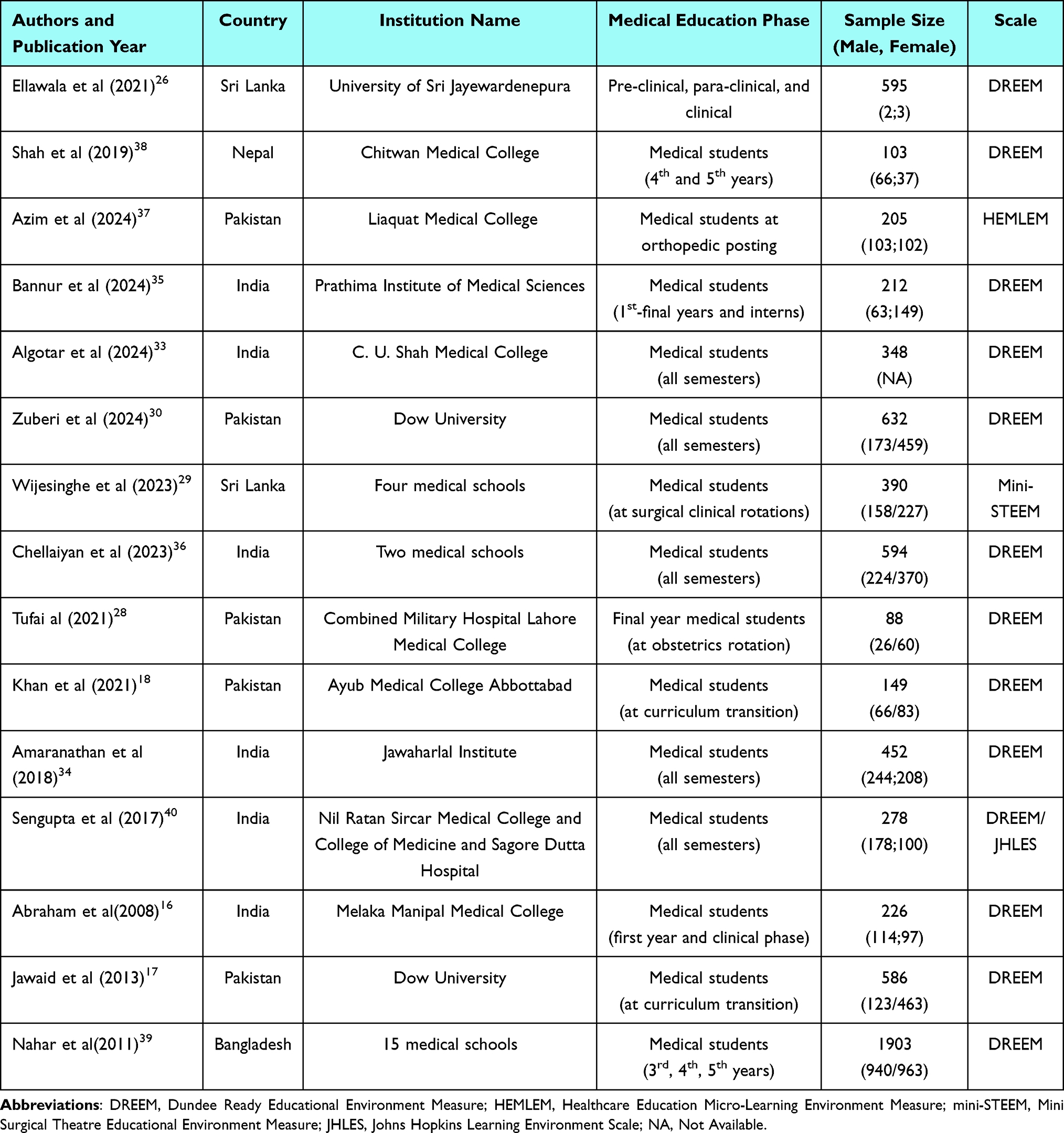 |
Table 1 Descriptive Summary of the Studies Assessing the Perceptions of Medical Students of Their Learning Environment in South Asia (n=15) |
Most of the included studies utilized the DREEM scale to assess medical students’ perceptions of their learning environment.30,38,39 However, one study by Azim et al used the Healthcare Education Micro-Learning Environment Measure (HEMLEM),37 as well as another study, which was conducted by Wijesinghe et al, used the mini Surgical Theatre Educational Environment Measure (mini-STEEM).29 For a comparative assessment, however, some scales, such as the DREEM and JHLES, were used together (Table 1).40
Medical Students’ Perceptions of the Learning Environment
Our systematic review included 15 studies, thirteen of which used the DREEM scale to measure medical students’ perceptions of the learning environment in South Asia.16,17,28,30,38–40 The overall DREEM score obtained in these studies varied greatly, ranging from 91.8 to 127.4 (possible range 0–200). Based on the DREEM scoring rubric,41 several studies indicated that medical students had a positive perception of their learning environment. Zuberi et al and Chellaiyan et al observed a total score of 91.8 and 100.1, respectively.30,36 This implies that medical students in these settings perceived their learning environment as having many problems. In contrast, Tufail et al, found a total score in the range of 126–127.28 This was an extremely favorable score, indicating that medical students had an optimistic view of the learning environment.
Table 2 illustrates the comparison of students’ perceptions across different dimensions of learning environment. Several reviewed articles indicate that certain dimensions of the learning environment were rated less favorable by students. For instance, social self-perception and atmosphere were the lowest rated dimensions in almost all reviewed studies.11,21,28–30,38 On the other hand, the majority of studies found a positive perceptions toward teaching and learning dimensions (details in Table 2).11,21,28–30,38
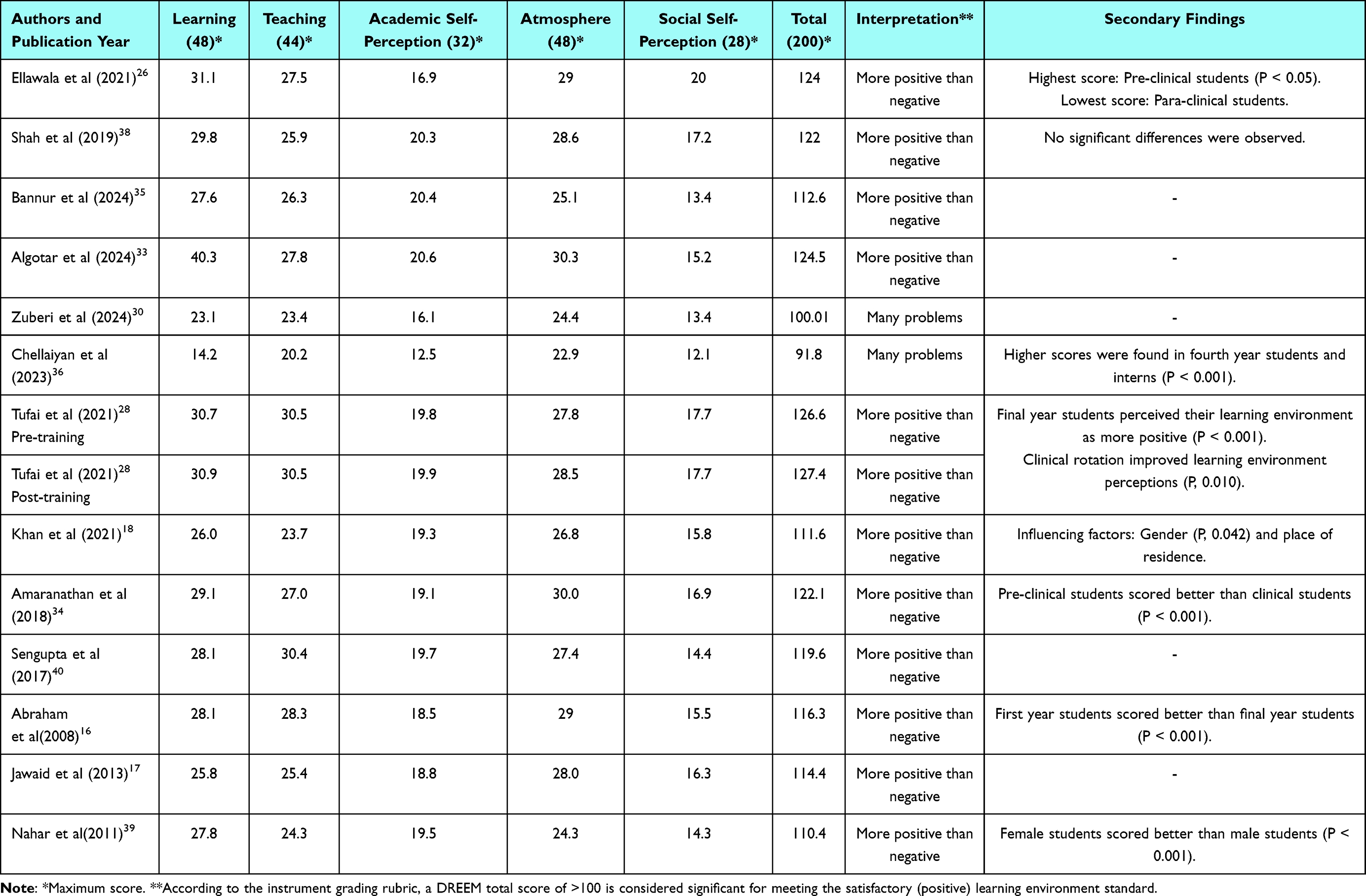 |
Table 2 Total and Subscales Scores, Interpretation, and Secondary Findings of Studies Using DREEM Scale to Assess Medical Students’ Perceptions of the Learning Environment in South Asia (n=13) |
Azim et al and Wijesinghe et al employed different instruments to assess medical students’ perceptions of the learning environment. Azim et al used the HEMLEM scale, which includes 12 items in two dimensions (teaching quality and staff attitude).37 The mean scores for teaching quality and staff attitude were above 50%. On the other hand, the surgical clinical rotation, which was assessed by mini-STEEM, was found satisfactory.29 Additionally, the JHLES and DREEM, which were employed together in an Indian medical school, observed no significant difference.40 Key findings of studies using HEMLEM, mini-STEEM, and JHLES are summarized in Table 3.
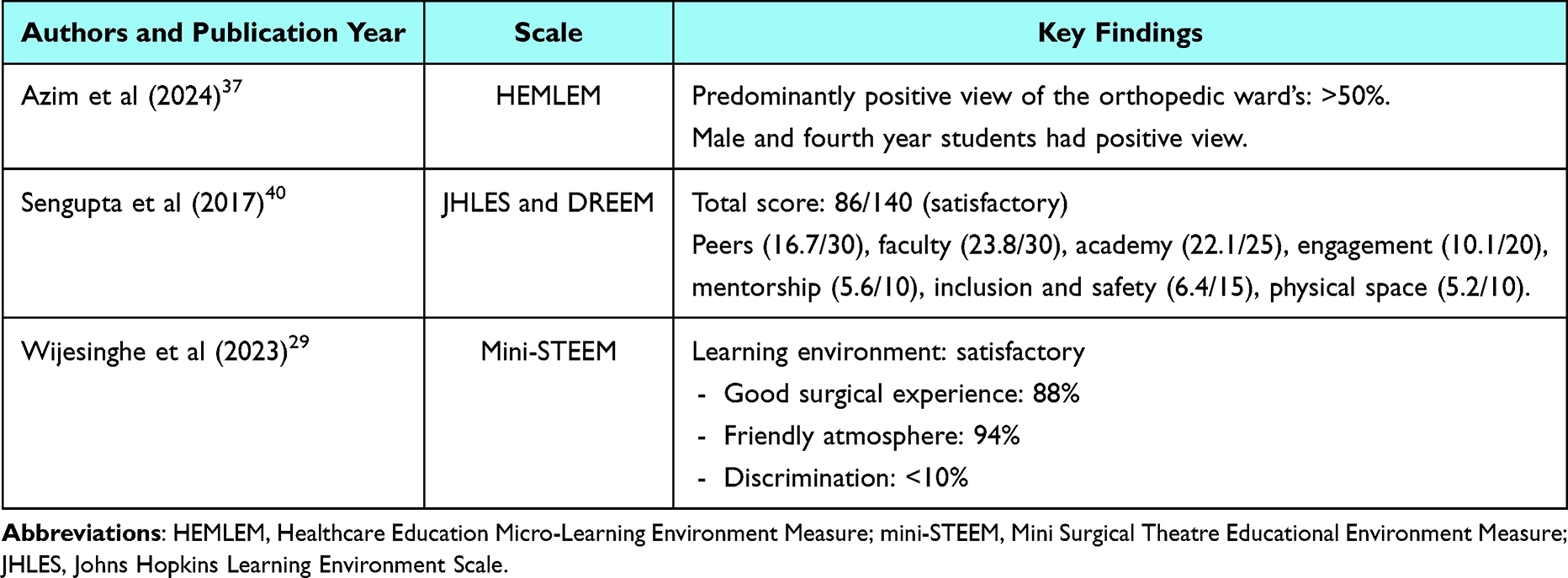 |
Table 3 Key Findings of Studies Using Scales Other Than DREEM to Assess Medical Students’ Perception of the Learning Environment in South Asia (n=3) |
Factors Influencing Medical Students’ Perceptions of the Learning Environment
Due mostly to the diversity of the medical school settings, there are a couple of factors that play a crucial role in influencing students’ perceptions of the learning environment.
Three studies reported the gender of students as a possible influencing factor on their perceptions. For instance, studies done in Pakistan and Bangladesh have reported a more satisfactory perception of female students than male students.18,39 However, Azim et al reported a more positive perception of the learning environment among male students at an orthopedic ward posting in Pakistan.37
Some studies (6/15; 40%) show a significant association between students’ perceptions of the learning environment and education levels, particularly between the first and final year students. Three of these studies reported a favorable view among first (pre-clinical) year students,16,26,34 while three others reported a more positive perception among final-year students.28,36,37
In addition, residential area was identified as a factor influencing medical students’ perceptions in Pakistan.18 Students from rural areas were reported to have a more positive perception of the learning environment.
Discussion
This review aims to examine and summarize the existing credible literature on measuring medical students’ perceptions of the learning environment in South Asia. We found that medical students positively perceived the learning environment in most of the studies documented in South Asia. However, positive perception levels varied widely, reflecting disparities in learning environment perceptions among medical students across countries. Moreover, we observed that several factors (eg gender, education levels, and place of residence) were reported to influence medical students’ perceptions of the learning environment in the documented studies.
Several scales are available for measuring perceptions of the learning environment in health professional education. However, only four scales were reported in the current review. The DREEM was the most common scale used (13/15), followed by HEMLEM (1/15), mini-STEEM (1/15), and JHLES (1/15). This finding signifies that learning environment research, in particular, has not received the attention it calls for over the past two decades in South Asia. Therefore, the validation and use of various learning environment measures are potential areas for future research in these settings.
This review indicates that the majority of studies (86%) reported a positive perception of the learning environment. Of the 13 studies that used the DREEM scale, eleven studies specifically reported a positive perception of the learning environment, with total scores ranging from 110.4 to 127.4 (possible range 0–200).28,29,38–40 According to the instrument grading rubric,41 a DREEM total score of >100 is considered significant for meeting the satisfactory (positive) learning environment standard. Although these studies indicated a positive perception, the reported DREEM scores were lower compared to some studies conducted in other countries. The DREEM total scores were found to be 137 and 145 in studies conducted in Australia,42 and the UK,43 respectively. Given these findings, medical schools’ learning environments in South Asia have a lot of room for growth and development to meet the standards set on global grounds.
This review also observed differences in perception levels across dimensions of learning environments. The DREEM scale measures perceptions in teaching, learning, academic self-perceptions, atmosphere, and social self-perceptions (possible maximum scores shown in Table 2). We found that atmosphere and social self-perceptions were less positive perceived dimensions in most studies.11,21,28–30,38 Several other studies have also reported significant differences in learning environment dimensions.9,14 The lowest positively perceived dimensions—atmosphere and social self-perceptions—in the South Asian context may, to some extent, reflect the socioeconomic challenges students in these regions encounter. Extending this narrative, several studies have reported infrastructural constraints in South Asian medical schools.4,21,44,45 Moreover, mental health symptoms among medical students in these settings are widely documented.46,47 As a policy measure, it is imperative to assess the overall learning environment and address multiple dimensions when designing educational interventions and programs.
This review also revealed that learning environments can be examined in specific contexts. For instance, Azim et al used a self-structured scale (HEMLEM) to assess students’ perceptions of an orthopedic learning environment in Pakistan.37 Similarly, Wijesinghe et al used mini-STEEM to evaluate students’ perceptions of clinical rotation phases.29 Both studies reported a relatively satisfactory experience in the mentioned environments. Additionally, a study conducted at an Indian University used two scales (DREEM and JHLES) to assess medical students’ perceptions of the learning environment and reported a positive experience in both scales.40 These findings emphasize the significance of various scales that can be utilized in medical school learning environments.
We also observed that studies reported a significant influence of only a limited number of factors on medical students’ perceptions of their learning environment in South Asia. These factors included gender, education level, and place of residence. As such, studies conducted in other developing countries have found the influence of several factors in determining the perceptions of medical students of their learning environment. For instance, a study conducted in an Iranian medical science university also found that gender and education levels (academic years) were strongly associated with students’ perceptions of the learning environment.9 Other factors, such as accommodation type, financing source for education, and year of enrollment, were found to be critical determinants of learning environment perceptions.2,8,14 These associations may highlight cultural and contextual influences. Nevertheless, studies that explore factors influencing learning environment experience, eg gender, residence, education levels, accommodation, and financing source for education, epitomize only a subset of factors related to learning environment perceptions. Therefore, future studies should consider a wide range of internal and external factors when examining the elements that influence learning environment perceptions and experiences. Understanding these factors may provide significant evidence for shaping educational policies and programs to optimize a particular learning environment.
Recommendations and Implications for Future Research
The current state of the literature on the learning environment in medical schools in South Asia warrants concern and action. To improve the learning environment in medical schools in this region, the following measures are recommended. First, develop and validate scales to measure students’ perception of the learning environment at different phases of medical education. Second, the development of context-specific scales in conflict-affected countries (eg Afghanistan) is highly recommended to have an understanding of the context-specific findings, address the specific problems, and highlight the strength of the particular learning environment. Finally, designing and implementing programs aimed at enhancing the learning environment is mandatory to improve the overall quality of medical education in these settings.
Limitations
This systematic review does have its limitations. First, limiting the review to quantitative studies reduces the generalizability of the overall findings. Second, the use of various measures and dimensions in perception assessment makes cross-study comparisons challenging. Third, the exclusion of dimensions of learning environments, such as optimistic bias, as search terms. Nonetheless, even studies that examined one dimension of the learning environment perception can add value to the overall perception of the learning environment. Fourth, according to the JBI results, several studies lacked information about sampling strategy and accounting for confounders. Finally, the review is limited by the number of included studies (n=15) and the lack of studies from Afghanistan, Bhutan, and the Maldives, which affects the generalizability of the findings.
Conclusion
This review provides systematic evidence, for the first time to our knowledge, about learning environment research in medical schools across South Asian countries. Findings from this review indicated that the learning environment was perceived positively by medical students in the majority of studies documented from the region. However, the medical school learning environment in this region has a lot of room for growth and development to meet the standards set on a global scale. Moreover, the limited data on the medical school learning environment research in the area calls for additional research, ideally in the form of evaluating various phases of medical education through validated scales as well as the influence of several factors on the medical school learning environment. With a better understanding of learning environment perceptions and influencing factors, interventions and programs can be developed or enhanced accordingly.
Data Sharing Statement
All data generated in this systematic review are included in this published article and its supporting information files.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Karani R. Enhancing the medical school learning environment: a complex challenge. J Gen Intern Med. 2015;30(9):1235–1236. doi:10.1007/s11606-015-3422-3
2. Gruppen LD, Irby DM, Durning SJ, Maggio LA. Conceptualizing learning environments in the health professions. Acad Med. 2019;94(7):969–974. doi:10.1097/ACM.0000000000002702
3. Khanipoor F, Bazrafkan L, Aramesh S, Shojaei M, Ghasemi A. A study of medical students’ experiences at Shiraz University of medical sciences from the implementation of integration in medical education: a qualitative study. BMC Med Educ. 2024;24(1):1042. doi:10.1186/s12909-024-05983-1
4. Stanikzai MH, Shanawa S, Karimkhil AT, Dadras O. Medical education in Afghanistan: challenges and policy implications. Adv Med Educ Pract. 2025;16:477–482. doi:10.2147/AMEP.S510309
5. Masoumian Hosseini ST, Qayumi K, Pourabbasi A, et al. Are we ready to integrate modern technologies into the medical curriculum for students a systematic review. Discover Educ. 2025;4(1):114. doi:10.1007/s44217-025-00521-7
6. Education WFFM. Enhancing the Quality of Medical Education Worldwide. Available from: https://wfme.org/.
7. Shirazi B, Riaz Q, Jafarey AM, Ahmed R, Shamim MS. The current status and challenges of bioethics education in undergraduate medical education in Karachi, Pakistan. BMC Med Educ. 2024;24(1):737. doi:10.1186/s12909-024-05599-5
8. Alblooshi A, Bashir N, Shaban S, AlMarzooqi S, Souid A-K, Fischer K. Assessment of the medical school learning environment at United Arab Emirates University. BMC Med Educ. 2024;24(1):871. doi:10.1186/s12909-024-05860-x
9. Bakhshialiabad H, Bakhshi G, Hashemi Z, Bakhshi A, Abazari F. Improving students’ learning environment by DREEM: an educational experiment in an Iranian medical sciences university (2011–2016). BMC Med Educ. 2019;19(1):397. doi:10.1186/s12909-019-1839-9
10. Davies D, Jindal-Snape D, Collier C, Digby R, Hay P, Howe A. Creative learning environments in education—A systematic literature review. Thinking Skills Creativity. 2013;8:80–91. doi:10.1016/j.tsc.2012.07.004
11. Eley DS, Cortes C, Arja S, et al. Perspectives on medical education in an increasingly globalized society: recognizing and embracing our diversity. Med Sci Educ. 2023;33(1):247–254. doi:10.1007/s40670-022-01705-8
12. Lommi M, De Benedictis A, Ricci S, et al. Appraisal and evaluation of the learning environment instruments of the student nurse: a systematic review using COSMIN methodology. Healthcare. 2023;11(7). doi:10.3390/healthcare11071043
13. Soemantri D, Herrera C, Riquelme A. Measuring the educational environment in health professions studies: a systematic review. Med Teach. 2010;32(12):947–952. doi:10.3109/01421591003686229
14. Al-Ahmari MM, Al Moaleem MM, Khudhayr RA, et al. A systematic review of publications using the Dundee Ready Education Environment Measure (DREEM) to monitor education in medical colleges in Saudi Arabia. Med Sci Monit. 2022;28:e938987. doi:10.12659/msm.938987
15. Dávidovics A, Makszin L, Németh T. A national DREEM: exploring medical and dental students’ perceptions on their learning environment across Hungary. BMC Med Educ. 2024;24(1):1211. doi:10.1186/s12909-024-06197-1
16. Abraham R, Ramnarayan K, Vinod P, Torke S. Students’ perceptions of learning environment in an Indian medical school. BMC Med Educ. 2008;8:20. doi:10.1186/1472-6920-8-20
17. Jawaid M, Raheel S, Ahmed F, Aijaz H. Students’ perception of educational environment at public sector medical university of Pakistan. J Res Med Sci. 2013;18(5):417–421.
18. Khan MJ, Jamil B, Sethi A, Noor U, Javed H, Adeeb H. Educational environment in the transition phase of curriculum At Ayub Medical College Abbottabad, Pakistan. J Ayub Med Coll Abbottabad. 2021;33(3):456–461.
19. Keržič D, Alex JK, Pamela Balbontín Alvarado R, et al. Academic student satisfaction and perceived performance in the e-learning environment during the COVID-19 pandemic: evidence across ten countries. PLoS One. 2021;16(10):e0258807. doi:10.1371/journal.pone.0258807
20. Xu X, Schönrock-Adema J, Bos NA. Development and evaluation of the measure of the international learning environment status (MILES) in international higher education. PLoS One. 2023;18(8):e0288373. doi:10.1371/journal.pone.0288373
21. Shah SR, Ahmed R, Munir M, et al. Medical education system in South Asia and its consequences on our health: a review. J Clin Diagn Res. 2017;11(12). doi:10.7860/JCDR/2017/29484.10983
22. Naghavi M, Ong KL, Aali A, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021;2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2100–2132. doi:10.1016/S0140-6736(24)00367-2
23. Rijal A, Adhikari TB, Khan JAM, Berg-Beckhoff G. The economic impact of non-communicable diseases among households in South Asia and their coping strategy: a systematic review. PLoS One. 2018;13(11):e0205745. doi:10.1371/journal.pone.0205745
24. Dhillon I, Jhalani M, Thamarangsi T, Siyam A, Singh PK. Advancing universal health coverage in the WHO South-East Asia Region with a focus on human resources for health. Lancet Regional Health - Southeast Asia. 2023;18. doi:10.1016/j.lansea.2023.100313
25. Stanikzai MH, Wafa MH, Akbari K, et al. Afghan medical students’ perceptions, and experiences of their medical education and their professional intentions: a cross-sectional study. BMC Med Educ. 2023;23(1):569. doi:10.1186/s12909-023-04577-7
26. Ellawala A, Marasinghe RB. Measuring the educational environment in a Sri Lankan medical school following curricular revision. BMC Med Educ. 2021;21(1):187. doi:10.1186/s12909-021-02625-8
27. Kohli V, Dhaliwal U. Medical students’ perception of the educational environment in a medical college in India: a cross-sectional study using the Dundee Ready Education Environment questionnaire. J Educ Eval Health Prof. 2013;10:5. doi:10.3352/jeehp.2013.10.5
28. Tufail S, Baqai S, Aslam P, Mustafa N, Nawaz Q, Bashir A. Perceptions of medical students about the educational environment at the start and end of obstetrics and gynaecology rotation and its impact on career choice. J Ayub Med Coll Abbottabad. 2021;33(3):502–506.
29. Wijesinghe K, Lunuwila S, Gamage H, et al. Medical students’ perception and attitudes on operating theatre learning experience in Sri Lanka. Surg Open Sci. 2023;15:12–18. doi:10.1016/j.sopen.2023.07.020
30. Zuberi BF, Shaikh MA, Zuberi FF, Rasheed T, Ali FS, Nawaz Z. Medical students’ perceptions at dow university of health sciences using Dundee ready education environment measure inventory. Pak J Med Sci. 2024;40(4):711–717. doi:10.12669/pjms.40.4.7712
31. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
32. Moola S, Munn Z, Tufanaru C, et al. Systematic reviews of etiology and risk. Joanna Briggs Inst Rev Manual. 2017;5:217–269. doi:10.46658/JBIMES-24-06
33. Algotar GN, Chauhan VN, Mehta SJ. Evaluating the perception of undergraduate medical students about the educational environment by using the Dundee Ready Educational Environment Measure (DREEM) questionnaire. Cureus. 2024;16(3):e57245. doi:10.7759/cureus.57245
34. Amaranathan A, Dharanipragada K, Lakshminarayanan S. Medical students’ perception of the educational environment in a tertiary care teaching hospital in India. Natl Med J India. 2018;31(4):231–236. doi:10.4103/0970-258x.258226
35. Bannur S, Vadakedath S, Veggalam S, Kandi V. A study on the medical students’ perspectives of their educational environment using the Dundee ready educational environment measure (DREEM) at a tertiary care teaching hospital in Telangana, India. Cureus. 2024;16(11):e73272. doi:10.7759/cureus.73272
36. Chellaiyan VG, Bhushan K, Maruthupandian J, Gupta S, Liaquathali F, Jenniferbritto J. Perception of the educational environment and its impact on the academic performance of medical school students: a cross-sectional study. Maedica. 2023;18(1):80–87. doi:10.26574/maedica.2023.18.1.80
37. Azim SR, Azfar SM, Baig M. Students’ perceptions of and satisfaction with their orthopaedic posting learning environment by using the healthcare education micro-learning environment measure (HEMLEM) questionnaire. PLoS One. 2024;19(7):e0306971. doi:10.1371/journal.pone.0306971
38. Shah DK, Piryani S, Piryani RM, Islam MN, Jha RK, Deo GP. Medical students’ perceptions of their learning environment during clinical years at Chitwan Medical College in Nepal. Adv Med Educ Pract. 2019;10:555–562. doi:10.2147/amep.S203377
39. Nahar N, Talukder MHK, Khan MTH, Mohammad S, Nargis T. Students’ perception of educational environment of medical colleges in Bangladesh. Bangabandhu Sheikh Mujib Med Univ J. 2011;3(2):97–102. doi:10.3329/bsmmuj.v3i2.7060
40. Sengupta P, Sharma A, Das N. Perception of learning environment among undergraduate medical students in two different medical schools through DREEM and JHLES questionnaire. J Clin Diagn Res. 2017;11(2):Jc01–jc04. doi:10.7860/jcdr/2017/23810.9248
41. Miles S, Swift L, Leinster SJ. The Dundee ready education environment measure (DREEM): a review of its adoption and use. Med Teach. 2012;34(9):e620–34. doi:10.3109/0142159x.2012.668625
42. Brown T, Williams B, Lynch M. The Australian DREEM: evaluating student perceptions of academic learning environments within eight health science courses. Int J Med Educ. 2011;2:94. doi:10.5116/ijme.4e66.1b37
43. Edgren G, Haffling A-C, Jakobsson U, Mcaleer S, Danielsen N. Comparing the educational environment (as measured by DREEM) at two different stages of curriculum reform. Med Teach. 2010;32(6):e233–e238. doi:10.3109/01421591003706282
44. Sood R. Medical education in India. Med Teach. 2008;30(6):585–591. doi:10.1080/01421590802139823
45. Stanikzai MH. Need for rapid scaling-up of medical education in Afghanistan: challenges and recommendations. Indian J Med Ethics. 2023;Viii:342–343. doi:10.20529/ijme.2023.032
46. Cuttilan AN, Sayampanathan AA, Ho RC. Mental health issues amongst medical students in Asia: a systematic review [2000-2015]. Ann Transl Med. 2016;4(4):72. doi:10.3978/j.issn.2305-5839.2016.02.07
47. Pokhrel NB, Khadayat R, Tulachan P. Depression, anxiety, and burnout among medical students and residents of a medical school in Nepal: a cross-sectional study. BMC Psychiatry. 2020;20(1):298. doi:10.1186/s12888-020-02645-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medical Students’ Knowledge and Perceptions of Herbal Medicine in Saudi Arabia: Should Medical Schools Take Immediate Action?
Almech M, Alissa A, Baghdadi RA, Abujamai JZ, Hafiz W, Alwafi H, Shaikhomer M, Alshanberi AM, Alshareef MH, Alsanosi SM
Advances in Medical Education and Practice 2024, 15:1243-1253
Published Date: 18 December 2024