Back to Journals » Advances in Medical Education and Practice » Volume 17
Medical Students’ Perceptions of Clinical Learning Environments in Public and Private Hospitals in Jeddah: A Mixed-Methods Study
Authors Gouda E, Elzayat A, Qronfla GM, Almahabi RO, Eltouny S ![]()
Received 22 December 2025
Accepted for publication 27 March 2026
Published 13 April 2026 Volume 2026:17 575311
DOI https://doi.org/10.2147/AMEP.S575311
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Enas Gouda,1,2 Ayat Elzayat,3 Ghazal Murad Qronfla,4 Renad Omar Almahabi,4 Sarah Eltouny2
1Medical Education Department, Fakeeh College for Medical Sciences, Fakeeh Care Group, Jeddah, 21461, Saudi Arabia; 2Medical Education Department, Faculty of Medicine, Suez Canal University, Ismailia, Egypt; 3Clinical Sciences Department, MBBS Program, Fakeeh College for Medical Sciences, Fakeeh Care Group, Jeddah, 21461, Saudi Arabia; 4Bachelor of Medicine, Bachelor of Surgery Program, Fakeeh College for Medical Sciences, Fakeeh Care Group, Jeddah, 21461, Saudi Arabia
Correspondence: Enas Gouda, Email [email protected]
Purpose: The clinical learning environment (CLE) is essential in shaping the professional growth, competence, and well-being of medical students. Insufficient evidence exists on how medical students in Saudi Arabia perceive the CLE across diverse hospital settings, particularly in comparison between the public and private sectors. This study examined medical students’ perceptions of the CLE during clerkship rotations in both public and private hospitals in Jeddah, using the Undergraduate Clinical Education Environment Measure (UCEEM) and qualitative thematic analysis.
Methods: A Convergent mixed-methods study was conducted among all clerkship-phase students (Years 4– 6) at Fakeeh College for Medical Sciences (FCMS), during the academic year 2024– 2025. The quantitative component used a repeated- measures cross-sectional design using the UCEEM questionnaire, while the qualitative component consisted of open-ended questions exploring students’ experiences. 52.2% of participants completed the qualitative component. This mixed-methods approach enabled both the measurement of overall perceptions and the exploration of contextual factors influencing the CLE. Students provided informed consent before participation.
Results: The study included 255 students. Overall, UCEEM scores did not differ significantly between public and private placements across all years. Higher academic year and male gender were associated with more positive perceptions of the CLE. Qualitative findings revealed that private placements were characterized by supportive supervision, more structured organization, and adequate resources, whereas public placements offered broader clinical exposure but faced challenges in organization and feedback provision. Both settings were viewed as generally positive.
Conclusion: Medical students generally have a positive view of their clinical learning environments, and older students are more confident and satisfied. Improving clinical education and planning clinical placements and curriculum development requires better supervision, more efficient organizations, and solutions to logistical problems. It’s just as important to make sure that all students, including girls, feel welcome and supported. To make sure that clinical placements prepare skilled and caring doctors to work in a variety of healthcare systems, they need to be evaluated and given feedback on a regular basis.
Keywords: clinical learning environment, medical students, supervision, healthcare training, perception
Introduction
The clinical learning environment (CLE) is a fundamental component of undergraduate medical education, shaping how students acquire knowledge, develop clinical skills, and form professional identities.1 CLEs represent dynamic and multifaceted settings where learners engage with patients, healthcare teams, and educational structures simultaneously.2 Contemporary models frame CLEs as comprising several interconnected domains: the personal experiences of learners, social relationships and interactions, organizational culture and policies, and the physical and virtual spaces in which clinical learning occurs.2,3
The quality of the CLE is crucial for effective clinical education and professional development, making its evaluation an essential component of medical training programs.4,5 A positive CLE balances opportunities for hands-on experience with supportive supervision, feedback, and a culture that values learning and well-being.6,7 Effective CLEs promote patient safety, professionalism, teamwork, and psychological safety, creating an environment where students feel empowered to learn, make mistakes, and grow.1,7–9 Conversely, inadequate environments marked by inconsistent supervision, excessive workloads, or poor communication can contribute to stress, burnout, and reduced educational outcomes.10–12
In Saudi Arabia, medical students typically rotate through both public and private hospitals during their clerkship years. Each sector offers distinct advantages and challenges: private hospitals are often better resourced and more structured in their teaching, while public hospitals tend to expose students to larger patient volumes and more varied clinical presentations.13,14 This diverse range of clinical sites exposes students to varying healthcare settings that differ in infrastructure, patient demographics, case complexity, and supervisory styles. In addition, gender-related factors may also affect students’ experiences within the CLE. Learning opportunities, access, and clinical participation for male and female students can be shaped by several factors, such as cultural expectations, patient preferences, and patterns of interaction with supervisors or healthcare teams. Understanding these contextual influences is therefore important when evaluating students’ perceptions of the CLE.15
Although studies have examined the CLE in general, little attention has been paid to how medical students perceive their experiences across public and private hospitals, especially in the Saudi Arabian context. Previous studies from the Middle Eastern region, specifically Saudi Arabia, have shown limited data regarding the assessment of the clinical environment. A quantitative-only study conducted in the UAE evaluated medical students’ perceptions of CLE across public and private healthcare settings, using the UCEEM, and found that students’ perceptions of CLE were generally positive, with some significant differences in learning environments between the two sectors.13 Another study in Saudi Arabia explored how students in two Saudi dental institutes’ bachelor’s degree programs perceive their clinical learning environment, revealing that students from Qassim University scored significantly higher than students from Jouf University, highlighting the need for tailored interventions to improve the quality of clinical education, especially in areas related to supervision and experiential learning.16
Although these previous studies offer valuable insights into the medical students’ perception of the educational environment, they have not specifically explored the difference in students’ perceptions across public and private hospital settings, nor have they extensively used the UCEEM tool, which is designed to assess clinical placement contexts.17 To our knowledge, this study is one of the first in the region to employ a mixed-methods approach, integrating quantitative evaluation via the UCEEM Questionnaire with qualitative thematic analysis, to thoroughly examine medical students’ perceptions of CLE in both public and private sectors. The findings will inform stakeholders about strengths and challenges within each setting and guide interventions aimed at optimizing clinical learning environments for medical students across both sectors, thus supporting the development of competent future physicians who are prepared for the complexities of healthcare delivery.
Study objectives:
● Assess and compare the perception of medical students regarding CLE across Public and Private Hospitals in Jeddah using the UCEEM Questionnaire.
● Explore the insights of students regarding their training experiences in Public and Private Hospitals.
● Examine differences in students’ perceptions of the CLE across years.
Materials and Methods
Study Design and Population
The study employed a convergent parallel mixed-methods design to assess medical students’ perceptions of the CLE at Fakeeh College for Medical Sciences (FCMS) in Jeddah. The quantitative component employed a cross-sectional design, utilizing the UCEEM questionnaire to assess the dimensions of the CLE, thereby enabling the identification of strengths and weaknesses across different domains. Concurrently, qualitative insights were gathered through open-ended questions embedded at the end of the same questionnaire. These open-ended questions invited students to describe the strengths, areas for improvement, and additional reflections on their clinical learning experiences in each setting with a deeper insight. Combining quantitative and qualitative approaches enabled a more comprehensive understanding of the CLE. A repeated-measures design was used, where the same students evaluated their CLE in both public and private hospital settings.
The study enrolled medical students in the clinical clerkship years (Years 4–6) in the academic year 2024–2025. Inclusion criteria were students aged ≥18 years, males and females, any nationality, who had completed at least three clinical rotations in a hospital or clinical setting at the time of data collection, and had direct exposure to patients and clinical supervision, enabling them to provide meaningful reflections on their learning environment, while students who were on academic leave, externships, or absent from clinical placements during the study period were excluded.
Sample Size and Design
The sample size was calculated using the Epi-Info CDC software calculator based on the proportion of satisfied students with their learning placement in a CLE.18 Of the 320 students invited to participate, 255 completed the questionnaire, resulting in a response rate of 79.7%. A convenient sample was used, where all eligible medical students were invited to participate in the study until the required sample size was reached. This sample design was suitable because it enabled the inclusion of all eligible students who were readily accessible during the data collection period. While this non-probability design may limit the generalizability of the findings, it is considered practical and efficient as it allowed for the recruitment of an adequate number of participants within a defined timeframe, ensuring representation from various clinical rotations.
Data Collection Tool and Procedure
The quantitative instrument was the Undergraduate Clinical Education Environment Measure (UCEEM), a validated tool specifically designed for evaluating the CLE.19 Originally developed in Sweden, the UCEEM includes 25 items grouped into two overarching dimensions, each of which has two subscales. The first dimension is experiential learning (17 items) with subscales: opportunities to learn in and through work (11 items) and preparedness for student entry (6 items), and the second dimension is social participation (8 items) with subscales: workplace interaction patterns and student inclusion (6 items) and equal treatment (2 items). The original English version of the UCEEM questionnaire was adopted without modification, as English is the main language of instruction at the institution.
Each item is rated on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree), where higher scores represent more positive perceptions of the CLE. Following previous studies.13 Mean scores were interpreted as: scores ≥ 4 indicate strong areas, scores ≤ 3 indicate areas needing attention, and scores 3.1–3.9 indicate areas for improvement. The questionnaire included three open-ended questions that allowed students to reflect qualitatively on strengths, suggested improvements, and additional comments about their clinical learning experiences in each healthcare setting. This enabled a richer understanding of the contextual factors influencing student perceptions.
Data were collected electronically through Microsoft Forms to ensure convenient and anonymous participation. Students completed the questionnaire twice: once after completing clinical rotations in private hospitals affiliated with FCMS and again after rotations in governmental hospitals with which FCMS has formal agreements. To maximize participation, reminder emails were sent one week after the initial invitations were sent.
Ethical Considerations
The Institutional Review Board (IRB) of Fakeeh College for Medical Sciences in Jeddah gave the study ethical approval (Approval No. 425-IRB-2023). Before the start of collecting data, all eligible students were clearly informed about the purpose and procedures of the study. They were assured that participation was entirely voluntary, that they could withdraw at any time without penalty, and that their responses would remain confidential and anonymous.
At the start of the self-administered questionnaire, participants were presented with a mandatory informed consent section. Students were required to actively indicate their agreement before they could proceed to the questionnaire; those who did not provide consent were unable to access the survey items. The questionnaire required approximately 10–12 minutes to complete, and no rewards or incentives were provided.
Before distributing the electronic survey, the research team conducted a pilot test to ensure clarity, usability, and technical reliability. The Microsoft Forms platform automatically notified participants if a response had already been submitted from their device, preventing multiple entries. Students completed the questionnaire independently in a private setting to minimise external influences, and when clarification was needed, the researchers provided neutral guidance that did not affect participants’ responses.
Participants were also informed that anonymised quotes from their responses might be included in publications from this study and gave consent to publish. Only those who agreed to the use of their quotes were included in the qualitative findings.
Data Management and Statistical Analysis
Quantitative data were exported to Microsoft Excel and subsequently analyzed using IBM SPSS Statistics (version 25). Data were tested for normality to guide the use of appropriate parametric or non-parametric tests using the Kolmogorov–Smirnov test. Descriptive statistics were presented by frequencies and percentages for qualitative data and mean ± SD and median for quantitative data. The Wilcoxon Signed-Rank test was used to compare UCEEM scores between private and public hospital CLEs.
To identify factors associated with overall perceptions of the CLE, a multivariate linear regression analysis was conducted with the total UCEEM score as the dependent variable. Independent variables included gender, academic year, and type of hospital (public or private). This analysis examined the relationships between these variables and students’ overall CLE perceptions. Regression assumptions were checked, including assessment of multicollinearity and inspection of residuals for normality. Unstandardized coefficients (B), standardized coefficients (Beta), t-values, as well as 95% confidence intervals were reported. P-value <0.05 was considered statistically significant based on the level of confidence of 95%. Regression coefficients were interpreted to assess the direction and strength of the association between the independent variables and the total UCEEM score. The findings were presented through tables and a bar chart.
Qualitative data from open-ended responses were analyzed thematically. Responses were read repeatedly to identify recurring ideas, which were then initially coded and organized into broader themes that represented the strengths and challenges of the CLE in each setting. To further enhance the trustworthiness of the qualitative analysis, the process of coding and theme identification was reviewed by more than one member of the research team. Differences in interpretation were discussed until agreement was reached. The research team members also reflected on their own perspectives to ensure that interpretations remained grounded in the participants’ responses. The themes were then refined and clearly labelled with names.
Results
The study included 255 students from the MBBS program, distributed across academic years four, five, and six, with 80, 86, and 89 students, respectively. The average age was 21±0.5, 22±0.1, and 23±0.1 years for years four, five, and six, respectively. Most of the students were females, as 72.5%, 75.6%, and 66.9% for years four, five, and six, respectively, as shown in Table 1.
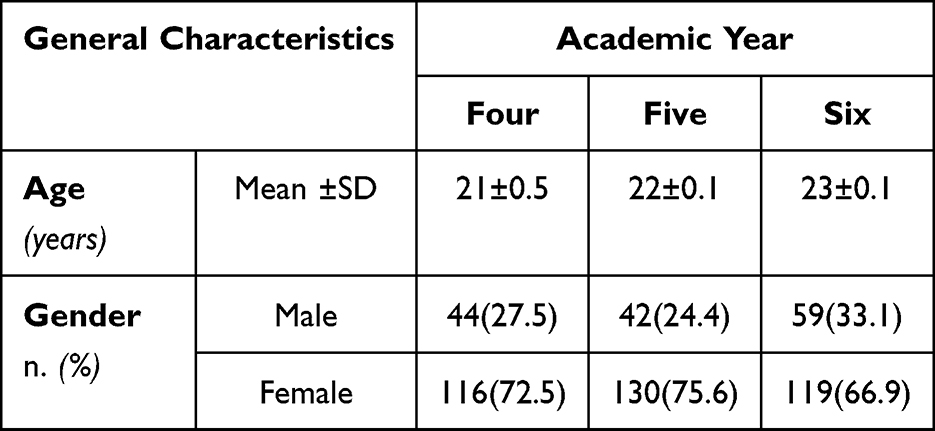 |
Table 1 General Characteristics of the Students Across the Academic years |
The distribution of UCEEM categories differed significantly across years (Figure 1). Year 5 students most frequently rated the CLE as “needs attention,” whereas Year 4 students most often identified “areas for improvement.” In contrast, Year 6 students were more likely to rate the CLE as demonstrating “strong areas,” indicating a more positive perception among senior students. The comparison of UCEEM scores between public and private sector clinical settings showed no statistically significant differences across the sub-scales and total score for years four, five, and six (P-value >0.05), as shown in Table 2.
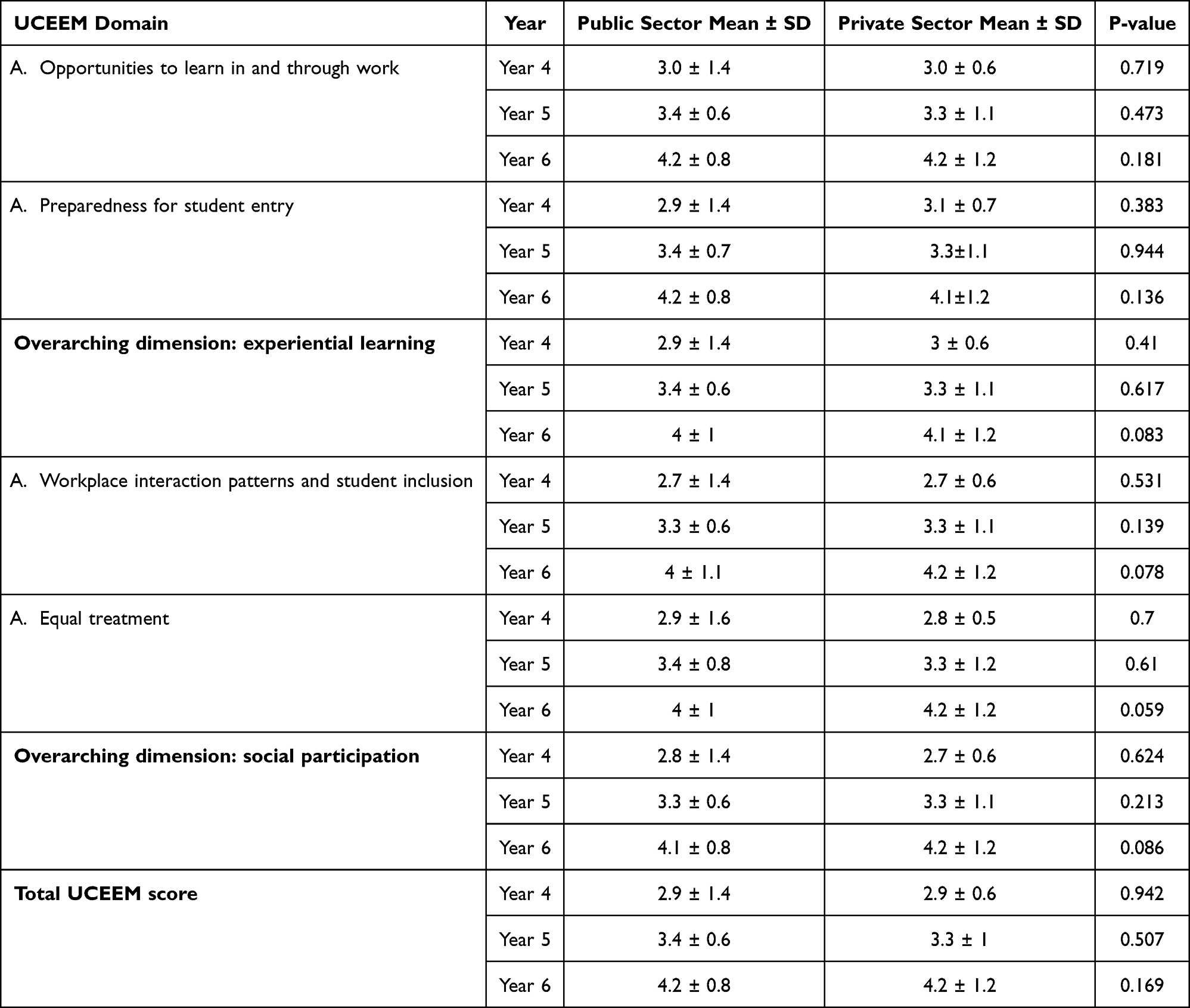 |
Table 2 Comparison Between Public and Private Sectors as CLE for years 4,5 and 6 Students (n=255) |
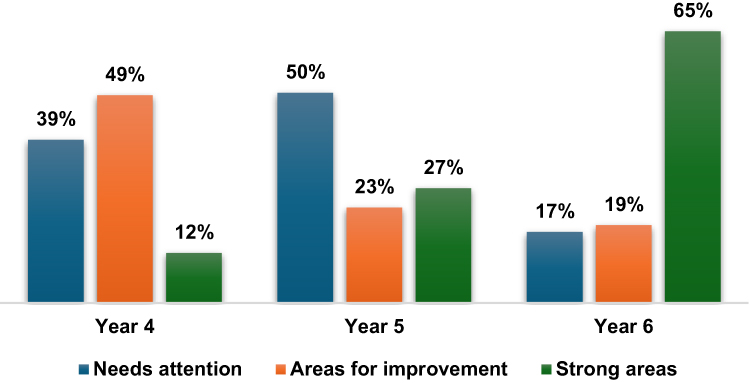 |
Figure 1 The association between the clinical learning environment as per UCEEM and the year. FIGURE 1 illustrates the association between the year and CLE by UCEEM categories, showing that the proportion of students rating the environment as “Needs attention” was highest in Year 5 (50%) and lowest in Year 6 (17%). Meanwhile, “Areas for improvement” were most frequently reported by Year 4 students (49%). Conversely, “Strong areas” were predominantly reported by Year 6 students (65%) compared with 12% in Year 4 and 27% in Year 45. |
The Multivariate regression analysis of factors affecting total UCEEM score showed that being a male student (β = 0.139, P-value <0.05) and at a higher academic year (β = 0.445, P-value <0.05) were positively affecting the total score, while the type of hospital as a CLE was not affecting this score, as shown in Table 3.
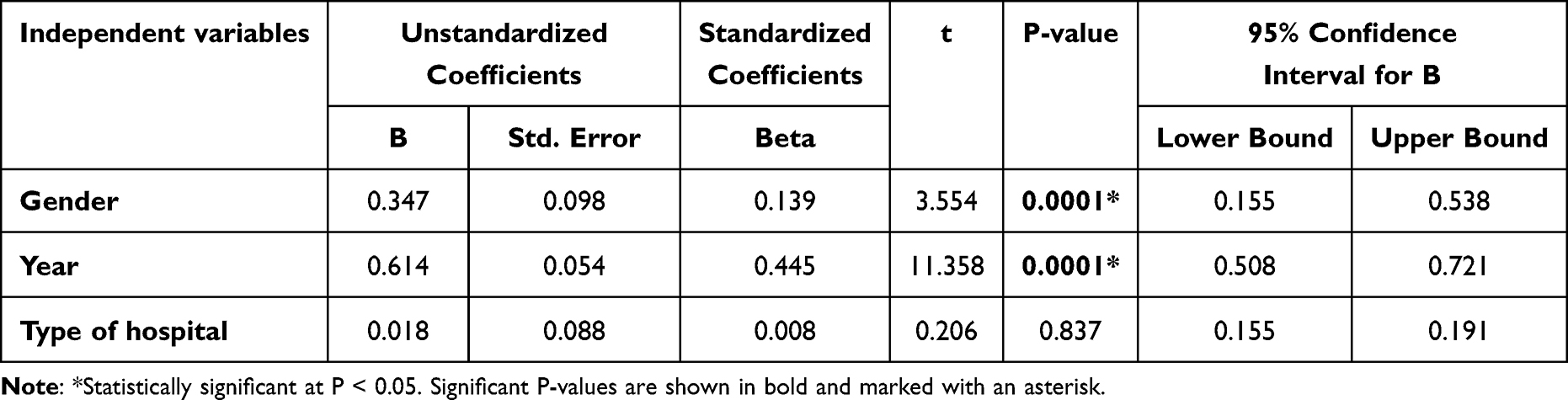 |
Table 3 Multivariate Regression Analysis of Factors Affecting Total UCEEM Score |
Thematic Analysis
The analysis of student qualitative feedback revealed both shared and distinct themes across private and public clinical placements. Four themes were identified, which are listed in Boxes 1 and 2 along with their subthemes and illustrative quotes. Private placements were perceived by the students to offer structured teaching, supportive supervisors, and well-organized sessions, but lacked the needed case variety. Public placements were reported to provide more diverse case exposure and trainers acting as dedicated role models; however, they were perceived to face the issue of inconsistent supervision, limited resources, and coordination challenges. Across both settings, respectful clinical environments that encouraged learning were reported, with private placements identified as more systematic and supportive overall.
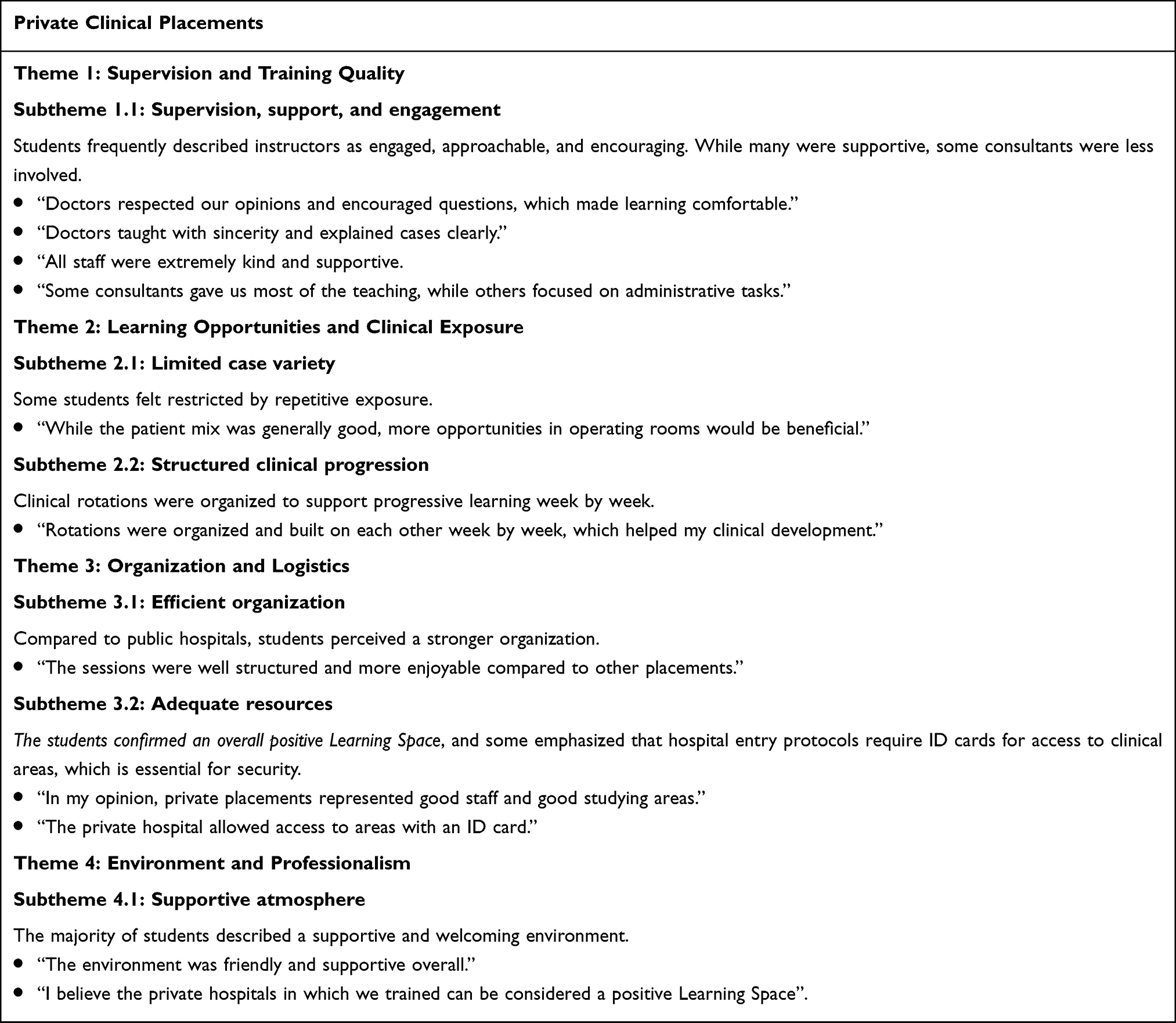 |
Box 1 Qualitative results for Clinical Environment Across Private Placements |
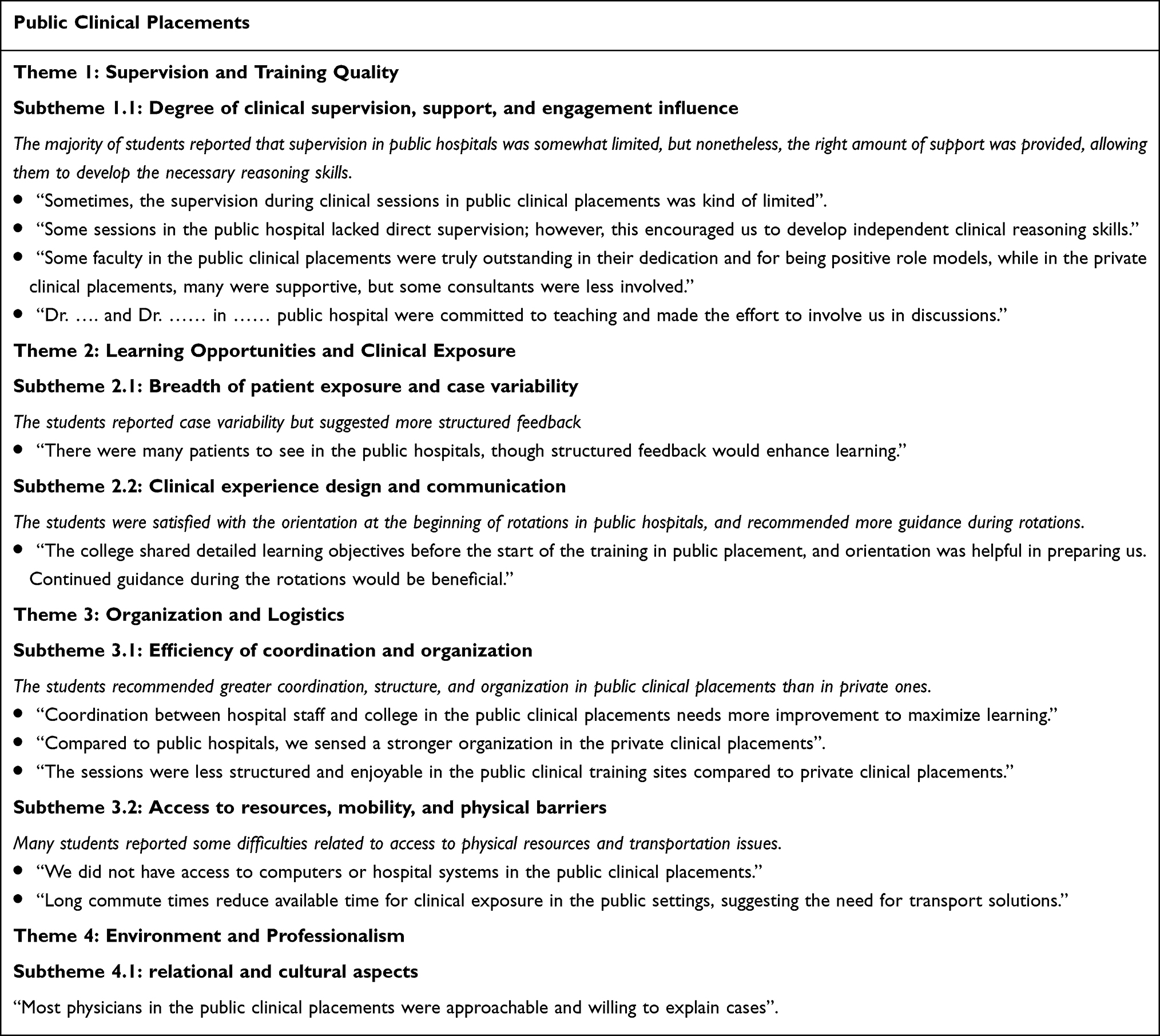 |
Box 2 Qualitative results for Clinical Environment Across Public Placements |
Theme 1: Supervision and Teaching Quality
Students in private hospitals often described their supervisors as supportive and approachable, which fosters a comfortable learning environment. For example, one student stated, “Doctors respected our opinions and encouraged questions, which made learning comfortable.” Conversely, public placement students noted inconsistencies in supervision, with some sessions lacking direct faculty presence, but also highlighted positive role models who actively engaged learners.
Theme 2: Learning Opportunities and Case Exposure
Private placements were characterized by structured clinical sessions building progressively on weekly topics, helping students develop systematically. One shared, “Rotations were organized and built on each other week by week, which helped my clinical development.” Some students expressed a desire for greater case variety: “While the patient mix was generally good, more opportunities in operating rooms would be beneficial.” Public placement students reported exposure to a diverse range of cases. However, they noted that feedback and reinforcement of objectives during clinical learning could be improved: “Exposure to a wide variety of cases was valuable, though structured feedback would enhance learning.”
Theme 3: Organization and Logistics
Compared to public hospitals, private placements were perceived as better organized, with positive remarks such as, “The sessions were well structured and more enjoyable compared to other placements.” Public placements encountered challenges related to coordination between hospital and college staff, which some students felt limited effective learning: “Improved coordination between hospital staff and college would maximize learning.” Additionally, public clinical sites faced resource availability issues, including limited computer access and transportation challenges, which reduced clinical exposure time.
Theme 4: Environment and Professionalism
The majority of private hospital students described a respectful and encouraging atmosphere, with one student noting, “The environment was friendly and supportive overall.” In public placements, students acknowledged that many staff were approachable and willing to explain cases, which facilitated learning.
Discussion
Senior medical students spend most of their time immersed in clinical settings, rotating through various specialties to gain diverse medical experience and insight. CLEs encompass elements such as learning opportunities, role modelling, and attitudes toward teaching and patients, all of which affect learning, learner well-being, and satisfaction. Recent research shows that students’ perceptions of the CLE influence their ability to meet training milestones and impact their future practice. Therefore, monitoring the quality of CLE is vital in medical education, as structured evaluation of learner perceptions can help identify areas for improvement and enhance the quality of education.20
This mixed-methods study explored medical students’ perceptions of clinical learning experiences in both public and private hospitals in Jeddah, Saudi Arabia, using the UCEEM questionnaire. Analysis of the UCEEM categories across years revealed that the proportion of students rating the environment as “Needs attention” was highest in Year 5 and lowest in Year 6. Meanwhile, “Areas for improvement” were most often reported by Year 4 students. Conversely, “Strong areas” were mainly reported by Year 6 students compared to Years 4 and 5, with these differences being statistically significant. These findings suggest that the medical students’ perceptions of the CLE improve with development and progression through the medical program, most likely indicating increased student self-efficacy, confidence, clinical competence, and familiarity with the healthcare system. The lower ratings in Year 4 may be attributed to the challenging transition from the preclinical to the clinical phase, while Year 5 calls for more attention to CLS, possibly due to mid-program fatigue or unmet expectations. By Year 6, students may have developed greater resilience and adaptive learning strategies and have begun to form their professional identity, which enhances their ability to engage positively with the clinical environment.
These findings are consistent with those reported by Palmgren and Sundberg’s study, which used UCEEM in assessing a chiropractic training context, and reported variability over time, highlighting that perceptions may shift with curricular changes or institutional culture.17
This finding aligns with the results of a bi-institutional study conducted in Saudi Arabia, which aimed to characterize how students in two dental programs perceive their CLE, using the modified UCEEM questionnaire. The mean total score for all students was 138.45, indicating significant differences between universities and highlighting the need for tailored interventions to improve the quality of clinical education.16 The findings of the current study are also consistent with those of Benamer et al (2023), who assessed medical clerkship students’ perceptions of their CLE across public and private training settings in the UAE using the same questionnaire. The study revealed that the students’ CLE perceptions were generally positive.13
However, comparisons of UCEEM scores between public and private sector clinical settings in the current study showed no significant differences in subscale and total scores across Years 4, 5, and 6, which contradicts the findings of Benamer et al (2023), who showed that the majority (63%) of the case load exposure responses scored a mean of ≥ 4. Compared to the private sittings, there is a significant reduction in total UCEEM, preparedness for student entry, and the overarching dimension of social participation scores for the public sector. Similarly, both workplace interaction patterns and student inclusion and equal treatment scored significantly lower for the public sector.13
The lack of statistically significant differences between public and private clinical settings is especially notable Although qualitative findings revealed detailed differences in supervision, case exposure, and logistics, the quantitative data suggest that, overall, medical students perceive both settings as similar in educational value. This may be due to the shared curricular structure and institutional oversight across both clinical placements, which helps unify student experiences. This suggests that the perceived differences between the two settings are limited to specific contextual aspects of the CLE setting that require a closer look at students’ insights, rather than fundamental differences.
Multivariate regression analysis revealed that being male and being in a higher academic year were associated with higher total UCEEM scores. At the same time, the type of hospital as a CLE did not have an impact. This suggests subtle gender dynamics in clinical training contexts, where access to opportunities or cultural expectations may shape experiences differently. This finding could help inform proposed recommendations for ensuring equity in the CLE. The positive association with higher academic year reaffirms the progressive nature of clinical learning, reinforcing that medical students’ capacity to perceive their environment evolves over time. The difference in gender that was seen may be due to cultural and institutional factors that affect how people learn in clinical settings. In some cases, the way patients want to interact with healthcare providers and the way society thinks people should interact with healthcare providers may affect students’ ability to attend certain clinical encounters. This underscores the necessity of guaranteeing equitable access to clinical learning opportunities and mentorship for all students.15
Qualitative analysis of the open-ended questions, using thematic analysis, revealed more profound insights into the medical students’ perceptions of the CLE and the differences between public and private clinical environments. It highlighted four themes: Supervision and Training Quality, Learning Opportunities and Clinical Exposure, Organization and Logistics, and Learning Opportunities and Clinical Exposure. These themes closely correspond to key UCEEM categories, including opportunities to learn in and through work, preparedness for student entry, workplace interaction patterns, student inclusion, and equal treatment. Thematic analysis revealed that while public hospitals offered diverse case exposure and positive role models, they faced challenges with supervision, organization, and logistics. In contrast, private hospitals provided structured, supportive, and well-organized environments; nevertheless, they faced the problem of limited case variety. The quantitative UCEEM scores showing no significant differences between the public and private placement can be explained by these complementary strengths across the two settings. Overall, integrating the strengths of both settings could create a more balanced and effective clinical learning environment. The qualitative findings of the current study are consistent with those of Jones et al (2023), which was conducted in the UK, aiming to characterize how the UCEEM relates to qualitative evaluation. It employed a thematic analysis where data were coded under three categories that emerged during the discussion: ideas relating to clinical placements in general, the placement under investigation, and learning methodology.21
In the thematic analysis, three key themes relating to what students found important in their view of any CLE were identified, each with three subthemes. Thematic analysis revealed that while students sought integration into a community of practice with responsibility, respect, and guidance, this was often hindered by placement structures and variable clinician engagement. However, inequalities in student experiences persisted due to variations in placement and course administration.
Practical implications for clinical education can be drawn from these findings, such as strengthening collaboration between medical schools and clinical training sites, supporting faculty development for clinical supervisors, and improving coordination between hospitals and academic programs, which may help enhance supervision and optimize students’ clinical learning experiences.
Limitations of the Study
The present study was performed at a single medical school in Jeddah, potentially constraining the applicability of the findings to other institutions or healthcare organizations. Second, a non-probability convenience sampling method was used, which may not fully reflect the views of all medical students and could lead to selection bias. Lastly, while the repeated-measures design enabled students to assess both public and private placements, participants’ perceptions may have been influenced by fluctuations in rotation timing, supervisors, and clinical rounds. Subsequent research that includes a broader range of institutions and more comprehensive qualitative methodologies would enhance the evidence regarding clinical learning environments in various healthcare settings.
Conclusion
This study shows that medical students generally perceive their CLEs positively across different hospital settings. Senior students tend to feel more confident and satisfied, highlighting the need to better support those early in clinical training. Improving the quality of supervision, streamlining organization, and addressing practical challenges like access and resources are key steps toward enhancing clinical education. It is equally important to foster an inclusive and supportive environment that meets the needs of all students, including female learners. To improve the quality of clinical education, medical schools should put structured supervision as a priority, make sure that training sites are better coordinated, and that everyone has equal access to learning opportunities. These findings may guide institutional policies and curriculum development by highlighting the significance of structured supervision, equitable learning opportunities, and effective coordination among training sites to enhance clinical education. Furthermore, future research could explore these findings in other institutions and healthcare settings, as well as examine how targeted interventions may improve clinical learning experiences for medical students. Ongoing feedback and evaluation should guide continuous improvements, ensuring clinical placements remain effective, supportive, and aligned with the goal of graduating skilled, compassionate physicians ready to meet the challenges of different healthcare systems.
Disclosure
The authors report there are no competing interests to declare.
References
1. Buxton GL. Understanding experiences of medical students’ clinical learning in the paediatric environment. 2025.
2. Nordquist J, Hall J, Caverzagie K, et al. The clinical learning environment. Med Teach. 2019;41(4):366–11. doi:10.1080/0142159X.2019.1566601
3. Gruppen LD, Irby DM, Durning SJ, et al. Conceptualizing learning environments in the health professions. Acad Med. 2019;94(7):969–974. doi:10.1097/ACM.0000000000002702
4. Walter MM, Rogan S, Schurz AP, et al. How to evaluate the quality of the clinical learning environment in health professions education? Protocol of a systematic review. PLoS One. 2025;20(4):e0293773. doi:10.1371/journal.pone.0293773
5. Sellberg M, Palmgren PJ, Möller R. –A cross-sectional study of clinical learning environments across four undergraduate programs using the undergraduate clinical education environment measure. BMC Med. Edu. 2021;21(1):258. doi:10.1186/s12909-021-02687-8
6. Ferri P, Stifani S, Morotti E, et al. Nursing students’ evaluation of clinical learning environment and supervision models before and during the COVID-19 pandemic: a comparative study. Acta Bio Medica: Atenei Parmensis. 2023;94(6):e2023256. doi:10.23750/abm.v94i6.14750
7. Hall J, Atkinson A, Chan M-K, et al. The clinical learning environment in CanMEDS 2025. Can Med Educ J. 2023;14(1):41. doi:10.36834/cmej.75537
8. Hardie P, O’Donovan R, Jarvis S, et al. Key tips to providing a psychologically safe learning environment in the clinical setting. BMC Med. Edu. 2022;22(1):816. doi:10.1186/s12909-022-03892-9
9. Almansour M, Abouammoh N, Idris RB, et al. Exploring medical students’ experience of the learning environment: a mixed methods study in Saudi medical college. BMC Med. Edu. 2024;24(1):723. doi:10.1186/s12909-024-05716-4
10. Oshodi TO, Sookhoo D. Nursing students’ perceptions of inadequate nurse staffing in the clinical learning environment–a systematic narrative review. Nurse Educ. Pract. 2025;82:104221. doi:10.1016/j.nepr.2024.104221
11. Patidar V, Gaur R, Mudgal SK, et al. Perception of undergraduate nursing student towards clinical learning environment and supervision: a cross-sectional study. J Med Evidence. 2024;5(3):223–231. doi:10.4103/JME.JME_12_24
12. Zhou AY, Panagioti M, Esmail A, et al. Factors associated with burnout and stress in trainee physicians: a systematic review and meta-analysis. JAMA Netw Open. 2020;3(8):e2013761–e2013761. doi:10.1001/jamanetworkopen.2020.13761
13. Benamer HT, Alsuwaidi L, Khan N, et al. Clinical learning environments across two different healthcare settings using the undergraduate clinical education environment measure. BMC Med. Edu. 2023;23(1):495. doi:10.1186/s12909-023-04467-y
14. Meyer R, Archer E, Van Schalkwyk SC. The private healthcare setting as a place for educating nurses: a qualitative exploration. Int. J. Afr. Nurs. Sci. 2022;17:100483. doi:10.1016/j.ijans.2022.100483
15. Mohammed G, Bennett D. Effect of gender on medical students’ clinical learning experience in a multicultural setting. Adv. Biomed. Res. 2023;2(3):131–138. doi:10.4103/abhs.abhs_31_23
16. Sghaireen MG, Kanwal H, Shah SA, et al. Undergraduate Clinical Education Environment Measure (UCEEM) of a dental program in jouf university and qassim university: a bi-institutional study. WORK. 2025;81(2):2553–2562. doi:10.1177/10519815241311753
17. Palmgren PJ, Sundberg T, Laksov KB. Reassessing the educational environment among undergraduate students in a chiropractic training institution: a study over time. J. Chiropr. Edu. 2015;29(2):110–126. doi:10.7899/JCE-14-37
18. Rashawn Mohamed Abd-Elhady T, Abdelhalim EHN, Elghabbour GMM, Mosaad Mohamed Elghabbour G. Nursing students’ experience and satisfaction with the clinical learning environment. Int. Egypt. J. Nurs. Sci. Res. 2022;3(1):437–454. doi:10.21608/ejnsr.2022.247221
19. Strand P, Sjöborg K, Stalmeijer R, et al. Development and psychometric evaluation of the undergraduate clinical education environment measure (UCEEM). Med Teach. 2013;35(12):1014–1026. doi:10.3109/0142159X.2013.835389
20. Roberts R, Cleland J, Strand P, et al. Medical students’ views of clinical environments. The Clinical Teacher. 2018;15(4):325–330. doi:10.1111/tct.12691
21. Jones A, Hartley J, Jones N. Validity of the UCEEM in use: how does it triangulate with qualitative data in measuring the effect of an educational intervention? J. Med. Educ. Curric. Dev. 2023;10:23821205231202335. doi:10.1177/23821205231202335
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.