Back to Journals » Patient Preference and Adherence » Volume 20
Medical Coping as a Mediator Between Social Support and Illness Uncertainty in Cancer Patients Across Age Groups: A Mediation Analysis
Authors Wei Y, Wang Y, Cao P, Gong Y, Gong J, Yang L, Chen J, Wang J, Li X
Received 14 November 2025
Accepted for publication 14 February 2026
Published 23 February 2026 Volume 2026:20 581624
DOI https://doi.org/10.2147/PPA.S581624
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yuxuan Wei,1,2,* Yongli Wang,3,* Peichun Cao,4,* Yuanyuan Gong,1 Jingjing Gong,1 Li Yang,1 Jin Chen,5 Jingli Wang,4 Xiaodan Li1
1Department of Obstetrics and Gynecology, Peking University People’s Hospital, Beijing, People’s Republic of China; 2School of Nursing, Hebei University, Baoding, People’s Republic of China; 3Department of Pediatrics, Peking University People’s Hospital, Beijing, People’s Republic of China; 4Department of Musculoskeletal Tumor Center, Peking University People’s Hospital, Beijing, People’s Republic of China; 5Department of Breast Center, Peking University People’s Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaodan Li, Email [email protected]
Objective: To examine the mediating role of medical coping in the relationship between social support and illness uncertainty among patients with malignant tumors, and to explore differences across age groups.
Methods: A secondary analysis was conducted using cross-sectional data from 905 hospitalized patients. Patient-reported outcomes were measured using the Mishel Uncertainty in Illness Scale–Adult, the Social Support Rating Scale, and the Medical Coping Modes Questionnaire. Pearson correlation analyses were conducted using SPSS version 25.0, and mediation effects were tested using the PROCESS macro with bootstrap resampling.
Results: In the overall sample, medical coping partially mediated the relationship between social support and illness uncertainty (indirect effect: β = 0.177, SE = 0.061, bootstrap 95% CI [0.067, 0.306]). Age-stratified analyses showed a full mediation effect in younger patients (β = 1.362, SE = 0.218, 95% CI [0.875, 1.737]). In contrast, the mediation effects were weaker in middle-aged and older patients, accounting for only 2.96% and 17.65% of the total effect, respectively. These findings indicate that the mediating role of medical coping varies across age groups, with distinct patterns observed among younger, middle-aged, and older patients.
Conclusion: In this cross-sectional sample, the results were statistically consistent with an indirect association between social support and illness uncertainty via medical coping, with age-related differences. Younger patients showed a stronger indirect association via coping, whereas middle-aged and older patients showed relatively stronger direct associations between social support and illness uncertainty.
Keywords: neoplasms, uncertainty in illness, social support, adaptation, psychological, nursing care
Introduction
Cancer remains a major global public health challenge. According to the 2022 Global Cancer Statistics, more than 20 million new cancer cases occur annually, with China accounting for approximately 24% of cases, and the incidence rate continues to rise.1,2 Long-term treatment and uncertainty regarding prognosis contribute to high levels of illness uncertainty, which in turn adversely affect treatment adherence and quality of life. At the same time, notable differences have been observed in illness uncertainty across age groups. These differences may reflect variations in social roles and life-stage characteristics, supporting the use of age-stratified analyses in psychosocial oncology research.3 Studies have shown that younger patients experience significantly higher levels of illness uncertainty compared with older patients, and newly diagnosed young patients are more concerned about treatment regimens, prognosis, and changes in family and occupational roles.4–6 Among middle-aged patients, illness uncertainty is positively associated with fatigue, insomnia, and negative emotions, with relatively younger individuals reporting greater symptom intensity and stronger emotional fluctuations than older patients. Similarly, research on older cancer patients has indicated that although illness uncertainty remains present, its associations with mental health and quality of life appear to follow different patterns in this population.7
Current studies have shown that social support is associated with lower illness uncertainty and may be linked to more positive coping strategies, and this pathway is particularly evident among middle-aged and older adults.8,9 Empirical research in older populations has found that social support not only enhances active coping and psychological resilience but also improves health self-management behaviors and psychological adaptation.10–12 These studies are often based on psychosocial intervention systems and multidisciplinary collaboration, emphasizing the crucial role of confrontive coping in information seeking and emotional regulation.13 In contrast, domestic studies highlight the central role of family support, indicating that Chinese patients tend to rely more on close relatives for emotional and decision-making support.14–16 Under a collectivist cultural context, the relationship between social support and medical coping shows patterns distinct from those observed in Western research—for instance, family members are more involved in decision-making processes, and social expectations as well as familial responsibilities may influence patients’ coping choices and perceptions of uncertainty.
Existing studies have explored the associations among social support, medical coping, and illness uncertainty; however, several gaps remain. First, most research has focused on general cancer populations without incorporating age into the analytical framework, thus lacking differentiated examinations across age groups. Second, international findings are largely derived from Western cultural and healthcare settings, and their applicability to Chinese populations has not been sufficiently verified.
This study targets patients with malignant tumors and employs an age-stratified design to examine the mediating role of medical coping in the relationship between social support and illness uncertainty, while comparing differences across age groups. By constructing a hierarchical mediation model, this study aims to reveal the unique characteristics of medical coping and social support utilization at different life stages, thereby providing empirical evidence to guide nurses in developing individualized psychosocial intervention strategies.
Methods
Study Design and Participants
A single-center cross-sectional survey was conducted among patients with malignant tumors who visited the hospital between January 2025 and August 2025. The inclusion criteria were: (1) primary malignant tumor confirmed by histopathology; (2) age ≥18 years; (3) basic cognitive and communication abilities, enabling independent completion of questionnaires or completion with the assistance of the researcher; and (4) ability to provide informed consent. The exclusion criteria were: (1) severe cognitive impairment or psychiatric disorders that precluded effective participation in the study; (2) patients in the terminal stage of disease, receiving palliative care, or too critically ill to complete the survey; (3) experience of major stressors or psychological trauma within the past three months, such as death of a close relative or severe family crises; (4) clinically or laboratory-confirmed severe dysfunction of major organs, including heart, liver, or kidneys; and (5) current participation in other interventional clinical studies. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Peking University People’s Hospital (No. 2024PHB227). Written informed consent was obtained from all participants.
Initially, 1,100 patients with malignant tumors were recruited, of whom 980 met the inclusion criteria and agreed to participate (response rate: 89.10%). Among these 980 eligible participants, 75 were excluded due to incomplete questionnaires (n = 26) or missing data (n = 49). Consequently, 905 valid questionnaires were retained, yielding an effective response rate of 92.35%.
Age Group Classification
Participants will be categorized into three age groups—young adults (18–39 years), middle-aged adults (40–59 years), and older adults (≥60 years)—based on prior research on age-related psychosocial development and coping strategies.17,18 This classification will be consistent with commonly used age ranges in psychosocial oncology research and will reflect developmental differences in social roles, health perception, and coping behaviors across the lifespan. The age stratification will enable us to examine potential age-specific patterns in medical coping, social support, and illness uncertainty.
Measures
Demographics
A general information questionnaire was used to collect patients’ demographic and clinical data, including: (1) demographic characteristics, such as age, education level, economic status, and marital status; (2) disease-related characteristics, including type of diagnosis, time since diagnosis, smoking history, and alcohol consumption history.
Mishel Uncertainty in Illness Scale (MUIS)
The Uncertainty in Illness Scale was originally developed by Mishel to assess patients’ perceptions of uncertainty related to their illness.19 The Chinese version was translated and culturally adapted by Yang et al, and its reliability and validity have been confirmed in Chinese populations.20 The scale consists of 33 items across four dimensions: ambiguity (13 items), complexity (7 items), lack of information (7 items), and unpredictability (5 items). (see Supplementary File 1 for the author-translated English version). Responses are rated on a 5-point Likert scale ranging from “strongly disagree” to “strongly agree”, scored 1 to 5, with a total score range of 33–165. Higher scores indicate greater illness uncertainty. In this study, the scale demonstrated excellent internal consistency, with a Cronbach’s α of 0.926.
Social Support Rating Scale (SSRS)
The Social Support Rating Scale was originally developed by Xiao Shuiyuan in 1986 to assess the level of social support among Chinese populations.21 The scale consists of 10 items across three dimensions: subjective support (4 items), objective support (3 items), and support utilization (3 items). (see Supplementary File 1 for the author-translated English version). Responses are scored on a 4-point scale depending on the item, with a total score range of 12–66, where higher scores indicate greater levels of social support. In this study, the scale demonstrated good internal consistency, with a Cronbach’s α of 0.784.
Medical Coping Modes Questionnaire (MCMQ)
The Medical Coping Modes Questionnaire was originally developed by Feifel et al in 1987 and was later introduced and revised in China by Han Xiaoling et al in 1992.22,23 The scale consists of 20 items across three dimensions: confrontive (8 items), avoidant (7 items), and resigned (5 items). (see Supplementary File 1 for the author-translated English version). Each item is scored on a 4-point scale (1–4), and the score for each dimension is the sum of its corresponding items. In the current study, the total coping score was used for mediation analyses, rather than individual subscales, to reflect overall coping tendency. Higher scores indicate a stronger tendency toward the coping style represented by that dimension. In this study, the scale demonstrated good reliability, with a Cronbach’s α of 0.762.
Data Collection
All questionnaires were completed through face-to-face interviews conducted by uniformly trained researchers. The training covered: (1) standardized administration procedures; (2) detailed explanations of each questionnaire item; (3) standardized quality control protocols for response assessment. Data collection was carried out in a quiet and private setting, with each questionnaire taking approximately 15–20 minutes to complete. Upon completion, the researchers immediately checked the questionnaires for completeness and promptly supplemented any missing items to ensure the accuracy and integrity of the data.
Data Analysis
All statistical analyses were performed using SPSS 25.0, and mediation analyses were conducted with Hayes’ PROCESS macro. Continuous variables were expressed as mean ± standard deviation (M ± SD), and categorical variables were presented as frequency (n). Pearson correlation analysis was used to examine the associations between the three dimensions of social support and the total and subscale scores of illness uncertainty. Furthermore, PROCESS macro (Model 4) was applied to test the mediating role of medical coping in the relationship between social support and illness uncertainty in the overall sample and across different age groups. A bias-corrected bootstrap method with 5,000 resamples was employed to estimate indirect effects and their 95% confidence intervals. All tests were two-tailed, with a significance level set at α = 0.05.
To evaluate the robustness of the mediation effects, sensitivity analyses were conducted both in the overall sample and within each age group. These analyses included gender, education level, and disease duration as covariates to examine whether the observed mediation effects of medical coping between social support and illness uncertainty were influenced by these potential confounders.
Results
Descriptive Statistics of Sociodemographic Characteristics and Illness Uncertainty
A total of 905 patients with malignant tumors were included in this study, comprising 198 young patients (21.9%), 476 middle-aged patients (52.6%), and 231 older patients (25.5%). In the young group, the proportion of unmarried individuals was relatively high (65.7%), and those with a bachelor’s degree or above accounted for the largest share (53.5%). In contrast, the older group had higher proportions of patients with lower education and income levels, showing an overall trend of increasing prevalence of low-income individuals with advancing age. In the middle-aged group, 21.0% of patients had a longer disease duration, and this group also had the highest scores of illness uncertainty. Regarding gender, female patients in the middle-aged and older groups reported slightly higher levels of illness uncertainty compared with males. All three groups reported relatively high levels of social support, and their illness uncertainty decreased as social support increased (see Table 1).
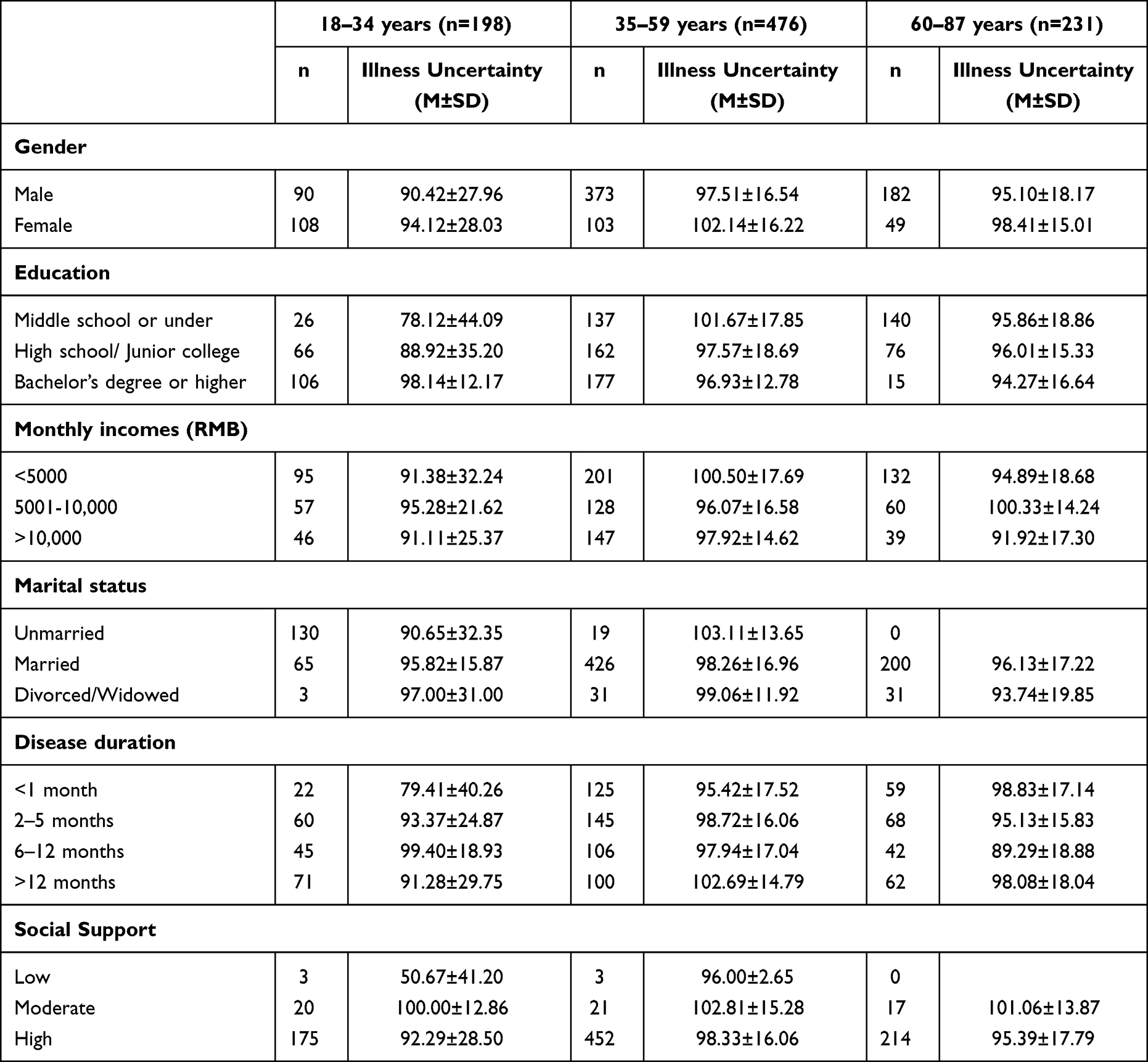 |
Table 1 Participants Demographic and Illness Uncertainty for Each Age Group (n = 905) |
Correlation Analysis of Illness Uncertainty, Medical Coping, and Social Support Across Age Groups
The results of Pearson correlation analysis are shown in Table 2. In the overall sample, confrontive coping was significantly negatively correlated with the total score of illness uncertainty, complexity, and ambiguity of information, while resigned coping was positively correlated with complexity. Subjective support and utilization of support were significantly negatively correlated with illness uncertainty.
 |
Table 2 Pearson Correlations Between Illness Uncertainty Dimensions, Coping Styles, and Social Support |
When analyzed by age group, in the young group, confrontive coping showed strong negative correlations with complexity and unpredictability (r = −0.462, r = −0.880, p < 0.01). Avoidant coping was strongly positively correlated with illness uncertainty (r = 0.694, p < 0.01), while resigned coping was strongly negatively correlated with the total score of illness uncertainty (r = −0.807, p < 0.01). Utilization of social support was also strongly negatively correlated with illness uncertainty (r = −0.796, p < 0.01).In the middle-aged group, correlations between medical coping and illness uncertainty were weaker, while all three dimensions of social support were negatively correlated with the total score of illness uncertainty. In the older group, both avoidant and resigned coping were positively correlated with illness uncertainty (r = 0.186, r = 0.190, p < 0.01), whereas subjective support and utilization of support were negatively correlated with illness uncertainty (r = −0.180, r = −0.191, p < 0.01) (see Table 2).
Figure 1 shows the correlation patterns among illness uncertainty, medical coping, and social support in the 18–34 years subgroup compared with the total sample. Overall, the 18–34 years heatmap displays more numerous and stronger correlations, whereas correlations in the total sample appear weaker overall, suggesting that the aggregate pattern may be diluted when combining middle-aged and older participants (see Figure 1).
 |
Figure 1 Correlation Heatmap of Illness Uncertainty Dimensions with Coping Styles and Social Support. ***p < 0.001, **p < 0.01, *p < 0.05. Description: This heatmap shows the correlation between the illness uncertainty dimensions, coping styles, and social support. The values are color-coded, with warmer colors representing stronger positive correlations and cooler colors indicating weaker correlations. |
Mediation Effect of Medical Coping on the Relationship Between Social Support and Illness Uncertainty
In the main effect analysis of the overall sample, medical coping played a partial mediating role in the relationship between social support and illness uncertainty (β = 0.177, bootstrap 95% CI [0.067, 0.306]), accounting for approximately 30.52% of the total effect. Stratified analysis showed that in the young group, medical coping served as a full mediator between social support and illness uncertainty (β = 1.362, bootstrap 95% CI [0.875, 1.737]), accounting for approximately 91.16% of the total effect. In contrast, the indirect effects in the middle-aged and older groups were only 0.014 and 0.096, corresponding to 2.96% and 17.65%, respectively Figure 2 illustrates the specified mediation model with path coefficients for the total sample and each age group. (see Table 3, Figure 2).
 |
Table 3 Bootstrap Test for the Mediating Effect of Medical Coping in the Relationship Between Social Support and Illness Uncertainty |
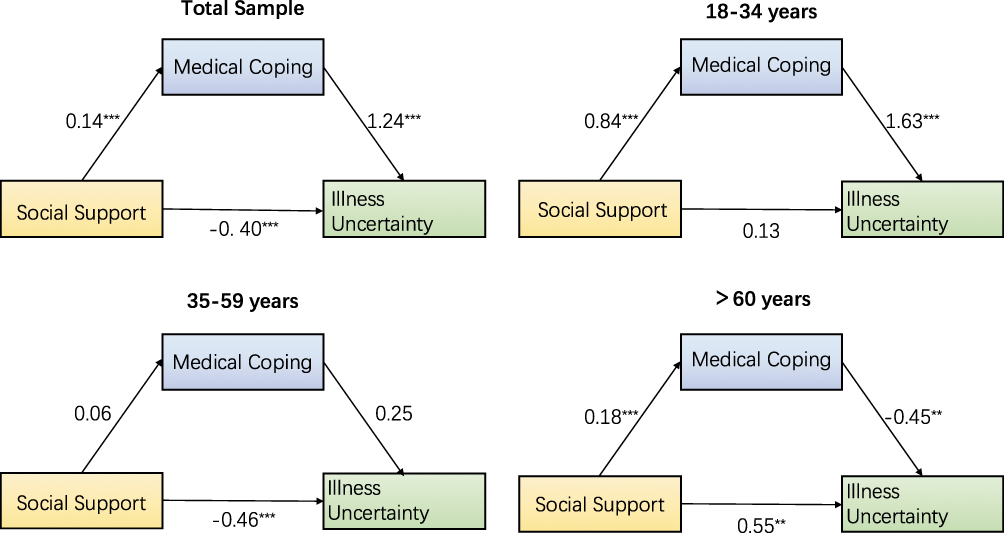 |
Figure 2 Age-Stratified Mediation Paths among Social Support, Medical Coping, and Illness Uncertainty. ***p < 0.001, **p < 0.01. Description: The mediation paths illustrate the relationships between social support, medical coping, and illness uncertainty across different age groups. The analysis is stratified by age to identify potential variations in mediation effects. |
The sensitivity analyses suggested that the mediation effects remained broadly consistent in the overall sample and across all age groups after controlling for gender, education, and disease duration, suggesting that the observed associations are robust to these covariates. The detailed results are presented in Supplementary Table S1.
Discussion
Our mediation model indicated that medical coping served as a partial mediator between social support and illness uncertainty. Moreover, the mediating effect of medical coping and the associations among social support, medical coping, and illness uncertainty showed substantial variation across age groups.
Age-Related Differences in the Association Between Medical Coping and Illness Uncertainty
In the overall sample, avoidant coping was significantly positively correlated with illness uncertainty, consistent with findings from other studies.24,25 Multiple studies have shown that avoidant coping strategies typically reflect an individual’s reluctance to engage with illness-related issues, which hinders the acquisition of a clear understanding of the disease and may maintain or even exacerbate illness uncertainty.26,27 This aligns with the basic framework of coping theory.
However, unlike previous studies, our results showed that confrontive coping was also significantly positively correlated with illness uncertainty. Further stratified analysis revealed that this effect was extreme in the young group, while the middle-aged and older groups buffered the relationship, with the correlation gradually shifting toward negative with increasing age. This pattern may be related to differences in resource availability and coping experience across the life span. Prior studies have shown that young patients, who are in critical stages of career and family development, are more vulnerable to uncertainty about illness, which triggers anxiety about future planning.28–30 As a result, they tend to actively seek information, but this process may instead heighten their perception of unknown risks. By contrast, with accumulated life experience, middle-aged and older patients are more capable of effectively employing confrontive strategies for emotional regulation, which may be associated with lower illness uncertainty.31
In addition, resigned coping was found to be significantly negatively correlated with illness uncertainty, with the strongest effect again observed in the young group. This finding may suggest that, in this age group, resigned coping does not reflect passive surrender but rather an acceptance of change, whereby patients adjust their expectations to regulate their emotions and thus effectively reduce uncertainty.32,33
Age-Related Differences in the Association Between Social Support and Illness Uncertainty
In the overall sample, subjective support and objective support were significantly positively correlated with illness uncertainty, while utilization of social support was significantly negatively correlated with illness uncertainty. Further age-stratified analyses revealed that middle-aged patients were better able to utilize social support to reduce illness uncertainty, with all three dimensions of social support showing negative correlations with illness uncertainty. These findings are consistent with previous research, highlighting that middle-aged adults are able to strategically utilize social support to manage uncertainty.8,11
Individuals in midlife often occupy central positions in their social networks, carrying clear social responsibilities and having accumulated substantial experience in coping with adversity. Therefore, they are not only able to obtain more effective and targeted social support but are also more skilled in actively filtering and applying these resources to address practical problems.34,35
Studies have further indicated that the “executive social function” of middle-aged individuals plays a key role in coping with chronic illness.36,37 Specifically, they are more inclined to transform social support into concrete problem-solving strategies and tools for emotional regulation, rather than relying solely on emotional comfort, thereby more effectively reducing illness uncertainty.
By contrast, in the young group, subjective support showed an opposite or weaker association with illness uncertainty, potentially linked to developmental needs for autonomy and self-identity in young adulthood38–40 Some young patients may perceive excessive concern from family or friends as a threat, which can transform social support into a source of stress.
Mediating Role of Medical Coping in the Relationship Between Social Support and Illness Uncertainty
In the overall sample, medical coping partially mediated the relationship between social support and illness uncertainty, which is consistent with previous findings.39,41 Further age-stratified analyses revealed that in the young group, medical coping served as a full mediator between social support and illness uncertainty, whereas the mediating effect was weak among middle-aged and older patients. We note that the reported high proportion of the total effect mediated by medical coping in young adults (91.16%) may reflect statistical phenomena such as suppression or scaling effects in stratified models, rather than indicating a substantive psychological dominance of coping in this group.
Research has shown that Mishel’s Uncertainty in Illness Theory emphasizes the close relationship between the formation of illness uncertainty and individuals’ information processing and coping mechanisms.40,41 Young patients are often in transitional stages of social roles and life patterns; when faced with major illness, they are more likely to experience higher levels of uncertainty and tend to adopt flexible coping strategies to regulate stress.42,43 In contrast, middle-aged and older patients, owing to accumulated life experience and greater adaptation to illness, are more capable of directly relying on social support resources to alleviate uncertainty.42 These findings suggest that differentiated strategies should be adopted in clinical interventions, taking into account age-specific patterns in mediation mechanisms.
Implications for Nursing Practice and Research
This study revealed the mediating role of medical coping in the relationship between social support and illness uncertainty among patients with malignant tumors. The findings suggest that differences exist across age groups in how social support is transformed into coping behaviors, highlighting the need for greater individualization in nursing practice.43
First, nurses may utilize standardized assessment tools to actively identify patients with high levels of illness uncertainty and determine their core influencing factors. Second, targeted strategies may be implemented according to the characteristics of different populations. For young patients, interventions may focus on cultivating and optimizing medical coping styles. Systematic psychoeducation and cognitive-behavioral techniques may be applied to guide them toward a positive problem-solving orientation, with the goal of illness uncertainty. For middle-aged and older patients, the emphasis may be on strengthening their social support networks. Practical approaches may include facilitating peer support groups and integrating or referring to community care resources, thereby buffering the psychological impact of illness uncertainty through enhanced social support. Finally, attention may be paid to the acceptability and adherence of interventions. Interdisciplinary collaboration should be encouraged, and interventions should be integrated into routine nursing care processes to establish a closed-loop management system from screening to intervention. Such an approach can improve both the precision and the effectiveness of nursing services.
Limitations
First, this was a cross-sectional study, so causal relationships between variables cannot be established. Second, the sample was drawn from medical institutions in a single region, and it remains unclear whether these findings can be generalized to patients in other regions. Third, all variables were assessed using self-reported instruments, which are subject to recall bias, social desirability effects, and other forms of response bias, potentially influencing the accuracy of the data collected. Finally, this study only conducted age-stratified analyses and did not further explore the potential effects of other moderating factors. These limitations should be considered when interpreting the results and in the design of future research.
Conclusion
This study found that medical coping partially mediates the relationship between social support and illness uncertainty, and that this mechanism exhibits significant age-related differences. Among young patients, medical coping serves as a key pathway through which social support may link illness uncertainty, whereas in middle-aged and older patients, the mitigating effect of social support on uncertainty is more direct, as evidenced by age-stratified mediation analyses. Medical coping is an important mediating variable in how social support alleviates illness uncertainty in patients with malignant tumors, and its effect varies significantly with age. Clinical nursing practice may take age into account, emphasizing coping skills training for young patients and strengthening support systems for middle-aged and older patients, thereby providing more targeted psychological care.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Peking University People’s Hospital (No. 2024PHB227). Written informed consent was obtained from all participants prior to participation. All data were collected anonymously and used solely for research purposes.
Acknowledgment
We would like to thank the participants for their contributions to this trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure statement
The authors declare no conflicts of interest in this work.
Funding
Funding for this study was provided by the National Key Technology Research and Developmental Program of China (Program Nos.2022YFC2704400 and 2022YFC2704405). The funders had no role in the study’s design or conduct, the collection, management, analysis, or interpretation of the data, the preparation, review, or approval of the manuscript, or the decision to submit the manuscript for publication.
References
1. Hu D, Yu J, Feng J, Liu P, Chen JM, Zhang HL. Comparison and trend analysis of cancer incidence in China and globally in 2022. World J Clin Oncol. 2025;16(6):107016.
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–12. doi:10.3322/caac.21834
3. Mehnert‐Theuerkauf A, Goerling U, Zimmermann T, et al. Early cancer survivorship distress trajectories associated with socioeconomic status and age: findings from a multicenter prospective study. Cancer Medicine. 2025;14(15):e71076. doi:10.1002/cam4.71076
4. Guan T, Chapman MV, de Saxe Zerden L, Sharma A, Chen D-G, Song L. Correlates of illness uncertainty in cancer survivors and family caregivers: a systematic review and meta-analysis. Support Care Cancer. 2023;31(4):242. doi:10.1007/s00520-023-07705-7
5. Sammarco A. Quality of life of breast cancer survivors: a comparative study of age cohorts. Cancer Nurs. 2009;32(5):347–358. doi:10.1097/NCC.0b013e31819e23b7
6. Guan T, Santacroce SJ, Chen D-G, Song L. Illness uncertainty, coping, and quality of life among patients with prostate cancer. Psychooncology. 2020;29(6):1019–1025. doi:10.1002/pon.5372
7. Verduzco-Aguirre HC, Babu D, Mohile SG, et al. Associations of uncertainty with psychological health and quality of life in older adults with advanced cancer. J Pain Symptom Manage. 2021;61(2):369–376.e1. doi:10.1016/j.jpainsymman.2020.08.012
8. Li Y, Peng J. Does social support matter? The mediating links with coping strategy and anxiety among Chinese college students in a cross-sectional study of COVID-19 pandemic. BMC Public Health. 2021;21(1):1298. doi:10.1186/s12889-021-11332-4
9. Lee I, Park C. The mediating effect of social support on uncertainty in illness and quality of life of female cancer survivors: a cross-sectional study. Health Quality Life Outcomes. 2020;18(1):143. doi:10.1186/s12955-020-01392-2
10. Jiang C, Jiang S. Influence of social participation and support on self-rated health among Chinese older adults: mediating role of coping strategies. Curr Psychol. 2023;42(17):14368–14375. doi:10.1007/s12144-022-02727-6
11. Lin C, Zhu X, Wang X, et al. The impact of perceived social support on chronic disease self-management among older inpatients in China: the chain-mediating roles of psychological resilience and health empowerment. BMC Geriatrics. 2025;25(1):284.
12. Li X, He L, Wang J, Wang M. Illness uncertainty, social support, and coping mode in hospitalized patients with systemic lupus erythematosus in a hospital in shaanxi, China. PLoS One. 2019;14(2):e0211313. doi:10.1371/journal.pone.0211313
13. Li J, Yu H. The impact of social support on the improvement of positive coping styles among disadvantaged breadwinner mothers. Sci Rep. 2025;15(1):24753. doi:10.1038/s41598-025-10112-z
14. Morey BN, Valencia C, Park HW, Lee S. The central role of social support in the health of Chinese and Korean American immigrants. Soci Sci Med. 2021;284:114229. doi:10.1016/j.socscimed.2021.114229
15. Wang L, Geng X, Ji L, Lu G, Lu Q. Treatment decision-making, family influences, and cultural influences of Chinese breast cancer survivors: a qualitative study using an expressive writing method. Support Care Cancer. 2020;28(7):3259–3266. doi:10.1007/s00520-019-05161-w
16. Tan J, Kong D, Hu L, Pu C. Impacts of financial, caregiving, and emotional support on mental health: case of hypertensive patients in China. Front Public Health. 2025;13. doi:10.3389/fpubh.2025.1601168
17. Andersen NH, Christiansen JA, la Cour K, et al. Differences in functioning between young adults with cancer and older age groups: a cross-sectional study. Eur J Cancer Care. 2022;31(6):e13660. doi:10.1111/ecc.13660
18. Minahan J, Falzarano F, Yazdani N, Siedlecki KL, Meeks S. The COVID-19 pandemic and psychosocial outcomes across age through the stress and coping framework. Gerontologist. 2021;61(2):228–239. doi:10.1093/geront/gnaa205
19. Mishel MH. The measurement of uncertainty in illness. Nurs Res. 1981;30(5):258. doi:10.1097/00006199-198109000-00002
20. 楊恩慈 [Enci Yang]. Mishel疾病不確定感量表中文版之信效度研究. 臺灣大學護理學研究所學位論文 [Reliability and Validity of the Chinese Version of the Mishel Uncertainty in Illness Scale. (Thesis, Graduate Institute of Nursing, National Taiwan University)]. 2008; 1–72. doi:10.6342/NTU.2008.10384
21. 肖水源, 杨德仁, 刘晓静 [Shuiyuan Xiao, Deren Yang, Xiaojing Liu]. 社会支持评定量表 (SSRS) 在中国人群中的信度与效度研究 [Reliability and Validity of the Social Support Rating Scale (SSRS) in Chinese Populations]. 中国心理卫生杂志 [Chinese Journal of Mental Health]. 1997;11(4):175–177.
22. Feifel H, Strack S, Tong Nagy V. Degree of life-threat and differential use of coping modes. J Psychosomat Res. 1987;31(1):91–99. doi:10.1016/0022-3999(87)90103-6
23. 韩晓玲, 王建国, 李春玲 [Xiaoling Han, Jianguo Wang, Chunling Li]. 医学应对方式量表的修订与信效度检验 [Revision of the Medical Coping Modes Questionnaire and Its Reliability and Validity Testing]. 中国心理卫生杂志 [Chinese Journal of Mental Health]. 1992;6(2):98–102.
24. Obispo B, Cruz‐Castellanos P, Fernández‐Montes A, et al. Coping strategies as mediators of uncertainty and psychological distress in patients with advanced cancer. Psychooncology. 2023;32(11):1694–1701. doi:10.1002/pon.6219
25. Liang T, Mao L, Du X, Chen F. Hematological cancer patients’ social support, coping strategies, anxiety, depression and posttraumatic growth: a structural equation model. Front Oncol. 2025;15:1540973. doi:10.3389/fonc.2025.1540973
26. Panjwani AA, Applebaum AJ, Revenson TA, Erblich J, Rosenfeld B. Intolerance of uncertainty, experiential avoidance, and trust in physician: a moderated mediation analysis of emotional distress in advanced cancer. J Behav Med. 2024;47(1):71–81. doi:10.1007/s10865-023-00419-5
27. Davis S, Serfaty M, Low J, Armstrong M, Kupeli N, Lanceley A. Experiential avoidance in advanced cancer: a mixed-methods systematic review. Int J Behav Med. 2023;30(5):585–604. doi:10.1007/s12529-022-10131-4
28. Allard NC, Orom H. Examining beliefs and information-seeking behaviors of young adults aged 20–39 to help inform cancer prevention communication. Prev Med. 2023;166:107353. doi:10.1016/j.ypmed.2022.107353
29. Mack JW, Fasciano KM, Block SD. Communication about prognosis with adolescent and young adult patients with cancer: information needs, prognostic awareness, and outcomes of disclosure. J Clin Oncol. 2018;36(18):1861–1867. doi:10.1200/JCO.2018.78.2128
30. Cheng Q, MSN N, Choi KC, WKW S. Unmet needs, anxiety, depression, and quality of life among caregivers of adolescents and young adults with cancer: a cross-sectional study. Asia Pacific J Oncol Nurs. 2022;9(10):100108. doi:10.1016/j.apjon.2022.100108
31. Sardella A, Lenzo V, Basile G, Martino G, Quattropani MC. Emotion regulation strategies and difficulties in older adults: a systematic review. Clin Gerontolog. 2023;46(3):280–301. doi:10.1080/07317115.2022.2128706
32. Burgers VWG, van den Bent MJ, Rietjens JAC, et al. “Double awareness”—adolescents and young adults coping with an uncertain or poor cancer prognosis: a qualitative study. Front Psychol. 2022:13. doi:10.3389/fpsyg.2022.1026090
33. Lie N-EK, Larsen TMB, Hauken MA. Coping with changes and uncertainty: a qualitative study of young adult cancer patients’ challenges and coping strategies during treatment. Eur J Cancer Care. 2018;27(6):e12743. doi:10.1111/ecc.12743
34. Seeman TE, Miller-Martinez DM, Stein Merkin S, Lachman ME, Tun PA, Karlamangla AS. Histories of social engagement and adult cognition: midlife in the U.S. study. J Gerontol B Psychol Sci Soc Sci. 2011;66B(Suppl 1):i141–i152. doi:10.1093/geronb/gbq091
35. Fiori KL, Denckla CA. Social support and mental health in middle-aged men and women: a multidimensional approach. J Aging Health. 2012;24(3):407–438. doi:10.1177/0898264311425087
36. Yu C, Barr AB, Gaugler JE. Social activities and cognitive functioning across mid- and late life: evidence from China. Gerontologist. 2025;65(4):gnaf014. doi:10.1093/geront/gnaf014
37. Costa-Cordella S, Arevalo-Romero C, Parada FJ, Rossi A. Social support and cognition: a systematic review. Front Psychol. 2021;12. doi:10.3389/fpsyg.2021.637060
38. Maqbool Z, Aggarwal P, Pammi VSC, Dutt V. Cyber security: effects of penalizing defenders in cyber-security games via experimentation and computational modeling. Front Psychol. 2020;11:11. doi:10.3389/fpsyg.2020.00011
39. Assor A, Soenens B, Yitshaki N, Ezra O, Geifman Y, Olshtein G. Towards a wider conception of autonomy support in adolescence: the contribution of reflective inner-compass facilitation to the formation of an authentic inner compass and well-being. Motiv Emot. 2020;44(2):159–174. doi:10.1007/s11031-019-09809-2
40. Beyers W, Soenens B, Vansteenkiste M. Autonomy in adolescence: a conceptual, developmental and cross-cultural perspective. Euro J Develop Psychol. 2025;22(2):121–141. doi:10.1080/17405629.2024.2330734
41. Zhang W, Lv J, Zhao J, et al. Proactive risk assessment of intrahospital transport of critically ill patients from emergency department to intensive care unit in a teaching hospital and its implications. J Clin Nurs. 2022;31(17–18):2539–2552. doi:10.1111/jocn.16072
42. Reinken DN, Reed SM. Mishel’s uncertainty in illness theory: informing nursing diagnoses and care planning. Int J Nurs Knowledge. 2023;34(4):316–324. doi:10.1111/2047-3095.12406
43. Kang Y, Son H. Age differences in the coping strategies of patients with colorectal cancer. Cancer Nurs. 2019;42(4):286. doi:10.1097/NCC.0000000000000604
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Implementing a Self-Efficacy-Based Nursing Bundle to Enhance Social Support in Patients with Enterostomies: A Single-Centre Quality Improvement Study
Xing X, Rong X, Xue M, Zhou L, Wang Y
Patient Preference and Adherence 2026, 20:555746
Published Date: 23 July 2026