Back to Journals » Clinical Ophthalmology » Volume 20
Mechanisms of Neuroperceptual Differences Between Subjective and Objective Refraction Based on Multimodal Imaging and Neurovisual Features
Authors Cao X, Shao J, Zhang Y, Zhang J ![]()
Received 17 April 2026
Accepted for publication 24 June 2026
Published 11 July 2026 Volume 2026:20 616337
DOI https://doi.org/10.2147/OPTH.S616337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Xinfang Cao, Jie Shao, Yonggang Zhang, Jun Zhang
Department of Ophthalmology, Hangzhou MSK Eye Hospital, Hangzhou, People’s Republic of China
Correspondence: Jun Zhang, Email [email protected]
Purpose: To quantify individual variations between subjective and objective refraction, explore correlations between multimodal imaging features, clinical parameters and refraction discrepancies, screen independent influencing factors, and construct a predictive model to provide technical support for personalized refractive surgery.
Methods: A total of 264 myopic patients (264 eyes) were enrolled. Paired t-test and Bland-Altman analysis were used to quantify refraction differences. Correlation analysis, multivariate regression, and machine learning algorithms were applied to explore influencing mechanisms and build a prediction model.
Results: There were significant individual differences between subjective and objective refraction, and the difference distribution was consistent with the normal distribution. The difference between subjective and objective refraction was moderately correlated with long-term daily maintained refraction (r=0.47, P< 0.001), weakly correlated with subjective refraction, objective refraction, corneal morphological features, and OCT optic nerve imaging features (r=0.17~0.25, P< 0.05), and extremely weakly correlated or uncorrelated with OCT macular imaging features and fundus color photography imaging features (r< 0.10, P> 0.05). Multivariate regression analysis showed that long-term daily maintained refraction, corneal higher-order aberrations, and OCT optic nerve imaging features were independent risk factors affecting the difference (P< 0.05). The prediction model constructed based on 126-dimensional radiomics key features, long-term daily maintained refraction, and core clinical parameters had a prediction accuracy of 87.2% and an area under the ROC curve (AUC) of 0.89.
Conclusion: Long-term daily maintained refraction is the core factor affecting the neuroperceptual difference between subjective and objective refraction. Among multimodal imaging features, only OCT optic nerve-related features have a weak correlation with the difference, and corneal higher-order aberrations are independent influencing factors. The results of this study can provide a theoretical basis and technical support for the precise diagnosis and treatment of refractive correction.
Keywords: multimodal imaging, subjective refraction, objective refraction
Introduction
Precise refractive correction is the cornerstone of clinical myopia intervention in ophthalmology, directly determining postoperative visual quality and patient quality of life.1–3 In current clinical practice, inconsistencies between subjective refraction (obtained via patient-reported visual perception) and objective refraction (measured by optical instruments) are common, with significant individual variability.4–8 This discrepancy directly hinders the translation of refractive surgery plans from subjectively formulated to objectively precise strategies.9–11
The core cause of this discrepancy lies in the physiological differences between the individual neurovisual system’s subjective perception of refractive status and the objective measurement by optical instruments. The neurovisual system refers to the complete visual perception system consisting of ocular optical structures, retina, optic nerve, and visual cortex, responsible for visual signal acquisition, transmission, and processing. Neuroperceptual differences in refraction are defined as subjective perceptual deviations of the neurovisual system from objective optical measurement results, which fundamentally cause subjective–objective refraction inconsistency.12 Existing studies have confirmed that neurovisual-related indicators—such as aberration characteristics and visual pathway structural integrity—are closely associated with visual perception function.13–16 However, the quantitative correlation between these indicators and the subjective-objective refraction difference remains unclear, as does the relative influence of different factors on this difference.
Given the clinical need for personalized refractive surgery, this study integrates multimodal radiomics and artificial intelligence (AI) algorithms to leverage multimodal imaging resources and enhance AI applications in precision ophthalmic diagnosis and treatment. In this study, we innovatively incorporated 126-dimensional radiomics features derived from multimodal ophthalmic imaging together with clinical parameters and machine learning algorithms. On this basis, we systematically investigated the distribution patterns and underlying correlative mechanisms of neuroperceptual differences reflected in subjective and objective refraction, clarified the associations between refraction discrepancies and diverse multimodal imaging features, and established a predictive model for such differences. Through the above four core research tasks including quantitative analysis of refraction difference, exploration of correlation mechanism, screening of independent influencing factors, and construction of a clinical predictive model, this research aims to provide a scientific basis for developing more objective, personalized refractive correction strategies and advancing precision ophthalmic diagnosis and treatment technologies.
Materials and Methods
Study Subjects
Myopic patients who presented to the ophthalmology department of our hospital from March 2026 to April 2026 were recruited as research subjects. Cases were strictly screened according to preset inclusion and exclusion criteria, and sample size was calculated to ensure statistical power.
Inclusion Criteria
1. Aged 18–45 years, regardless of gender, with myopia ranging from −0.50D to −10.00D, astigmatism ≤2.00D, and corrected visual acuity ≥20/20; 2. No organic ocular diseases (eg, cataracts, glaucoma, retinal diseases, corneal diseases) or history of ocular surgery/trauma; 3. No systemic diseases (eg, diabetes, hypertension, neurological diseases), mental illness, or cognitive impairment, and ability to cooperate with all examinations and evaluations; 4. No use of drugs affecting refractive status (eg, atropine eye drops) within 3 months and no prior orthokeratology lens wear.
Exclusion Criteria
1. Failure to meet the inclusion criteria; 2. Inability to cooperate with subjective refraction, multimodal imaging collection, or other study procedures; 3. Substandard imaging data quality (eg, motion artifacts, insufficient clarity) precluding extraction of effective 126-dimensional radiomics features via the AIIO intelligent diagnosis program; and 4. Loss to follow-up or withdrawal from the study during the follow-up period.
Sample Size Estimation
Sample size was estimated using the formula

(α=0.05, Z=1.96, δ=0.05), referring to clinical data processing experience and the coefficient of variation (CV=15.2%) of individual differences in subjective and objective refraction.17 This calculation estimated a required sample size of 240 subjects (240 eyes). Considering a potential 10% data variation rate (due to radiomics data processing exclusions), 264 subjects (264 eyes) were actually enrolled. One eye per patient was randomly selected as the study eye using Excel’s random number generator. Baseline characteristics of the study population were as follows: 136 males and 128 females, aged 18–45 years (mean ± SD: 28.6±7.2 years), including 84 cases aged 18–25 years, 114 cases aged 26–35 years, and 66 cases aged 36–45 years; myopia ranged from −0.50D to −10.00D (mean ± SD: −4.82±2.15D), including 96 eyes with low myopia (−0.50~-3.00D), 106 eyes with moderate myopia (−3.25~-6.00D), and 62 eyes with high myopia (>-6.00D); average daily close-up eye use time was 8.2±2.3 hours; 242 cases had a family history of myopia, and 22 cases had no family history of myopia.
Experimental Methods
Data Collection
General information (age, gender, spectacle use, etc.) was collected via a standardized questionnaire. Objective refraction was measured using the NIDEK ARK-1 autorefractor (NIDEK, Aichi, Japan). Subjective refraction was performed by two senior optometrists; a third optometrist resolved discrepancies >0.25D. Multimodal imaging was performed using the following instruments: Zeiss Cirrus 5000 OCT (Zeiss, Jena, Germany) for optic nerve and macular imaging, Sirius corneal topographer (CSO, Florence, Italy) for corneal parameter measurement, and Zeiss CLARUS 500 (Zeiss, Jena, Germany) for fundus photography.
The independently developed AIIO intelligent diagnosis program (Hangzhou MSK Eye Hospital, Hangzhou, China) was used for multimodal radiomics feature extraction. This program automatically extracts 126-dimensional radiomics features from uploaded optic nerve, macular, and fundus structure images, with independent extraction for each eye to ensure feature independence and integrity. The 126 features include 32-dimensional GLCM (Gray-Level Co-occurrence Matrix) texture features, 28-dimensional LBP (Local Binary Pattern) local features, 22-dimensional HOG (Histogram of Oriented Gradients) shape features, and 44-dimensional statistical features.
Data Processing and Analysis
SPSS 19.0 (IBM, Armonk, NY, USA) and Python (Python Software Foundation, Wilmington, DE, USA) with PyTorch (Facebook, Menlo Park, CA, USA) and PyRadiomics (Radboud University Medical Center, Nijmegen, Netherlands) were used for statistical data analysis, with a significance level of α=0.05. Paired t-tests and Bland-Altman analysis were used to quantify refraction differences. Pearson or Spearman correlation analysis was used to compare 126 radiomics features with refraction differences (grouped by feature type). Multivariate regression analysis was used to screen for independent risk factors, and machine learning algorithms (random forest, support vector machine [SVM]) were used to rank feature importance. A predictive model was constructed with a 7:3 training/validation set split, and its performance was evaluated using ROC curves, accuracy, and recall.
Prior to data preprocessing, 126-dimensional radiomics feature data for each eye were standardized using the Z-score method:

where X is the original value of a specific feature for a single eye, μ is the mean value of that feature across all study eyes, and σ is the standard deviation of that feature across all study eyes. This standardization eliminated dimensional differences between different feature dimensions. Outliers were removed using the 3σ principle, excluding single-eye data deviating by ±3 times the standard deviation of the feature mean.18
Radiomics Feature Comparison Rules
Standardized comparison rules (Table 1) clarified analysis standards, image sources, and judgment criteria for 126 radiomics features to ensure repeatability.
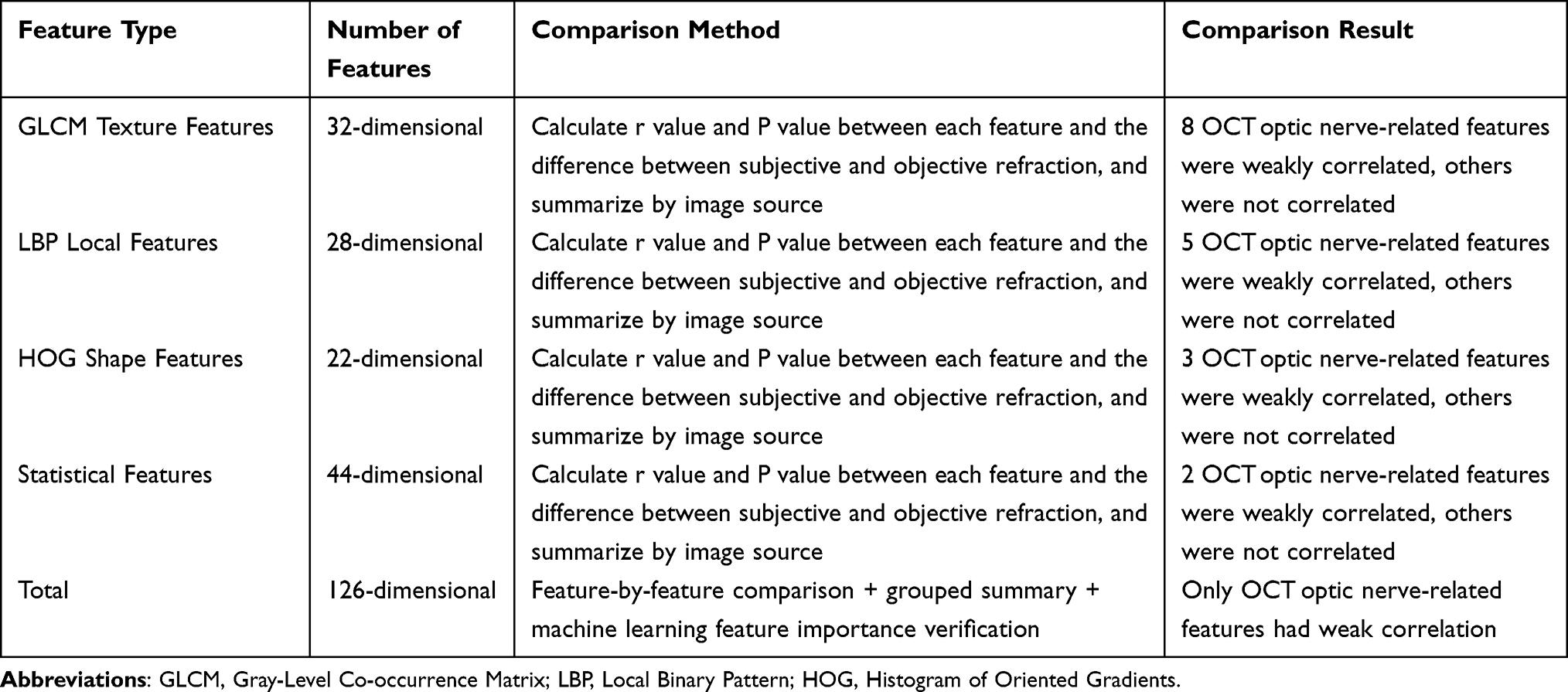 |
Table 1 Specific Comparison Rules of 126-Dimensional Radiomics Features and the Difference Between Subjective and Objective Refraction |
Ethical Approval
This study protocol complies with the ethical guidelines of the Declaration of Helsinki and has been registered with the Chinese Clinical Trial Registry (ChiCTR2600122125). All subjects signed written informed consent forms upon recruitment, and personal privacy and data security were strictly protected throughout the study.
Results
Refraction Difference Quantification
The mean spherical equivalent refraction was −5.21±2.12D for subjective refraction and −5.95±2.28D for objective refraction, with a mean difference of 0.73±0.25D (range: −0.52~1.78D). Specifically, 4 eyes (1.5%) had a difference <-0.50D, 18 eyes (6.8%) had a difference of −0.50~0.00D, 94 eyes (35.6%) had a difference of 0.00~+0.50D, and 148 eyes (56.1%) had a difference >+0.50D. Paired t-test showed a statistically significant difference between subjective and objective refraction (t=37.24, P<0.001, Cohen’s d=2.90). Bland-Altman analysis (95% CI: 0.68~0.78, bias=0.73D) showed that 97.3% of data points fell within the consistency limits. Shapiro–Wilk test confirmed that the refraction difference distribution was normal (W=0.987, P=0.12).
Correlation Analysis
The refraction difference was moderately correlated with long-term daily maintained refraction (r=0.47, P<0.001), weakly correlated with subjective refraction (r=0.21), objective refraction (r=0.19), corneal morphological features (corneal curvature r=0.17, corneal higher-order aberrations r=0.23), and OCT optic nerve features (r=0.25), and uncorrelated with OCT macular features and fundus color photography features (r=0.06~0.08).
Among the 126 radiomics features, 18 (14.3%) were weakly correlated with the refraction difference (r=0.17~0.26, P<0.05), all derived from OCT optic nerve images (8 GLCM texture features, 5 LBP local features, 3 HOG shape features, and 2 statistical features). The remaining 108 features (85.7%) were extremely weakly correlated or uncorrelated with the difference (r<0.10, P>0.05) (Table 2).
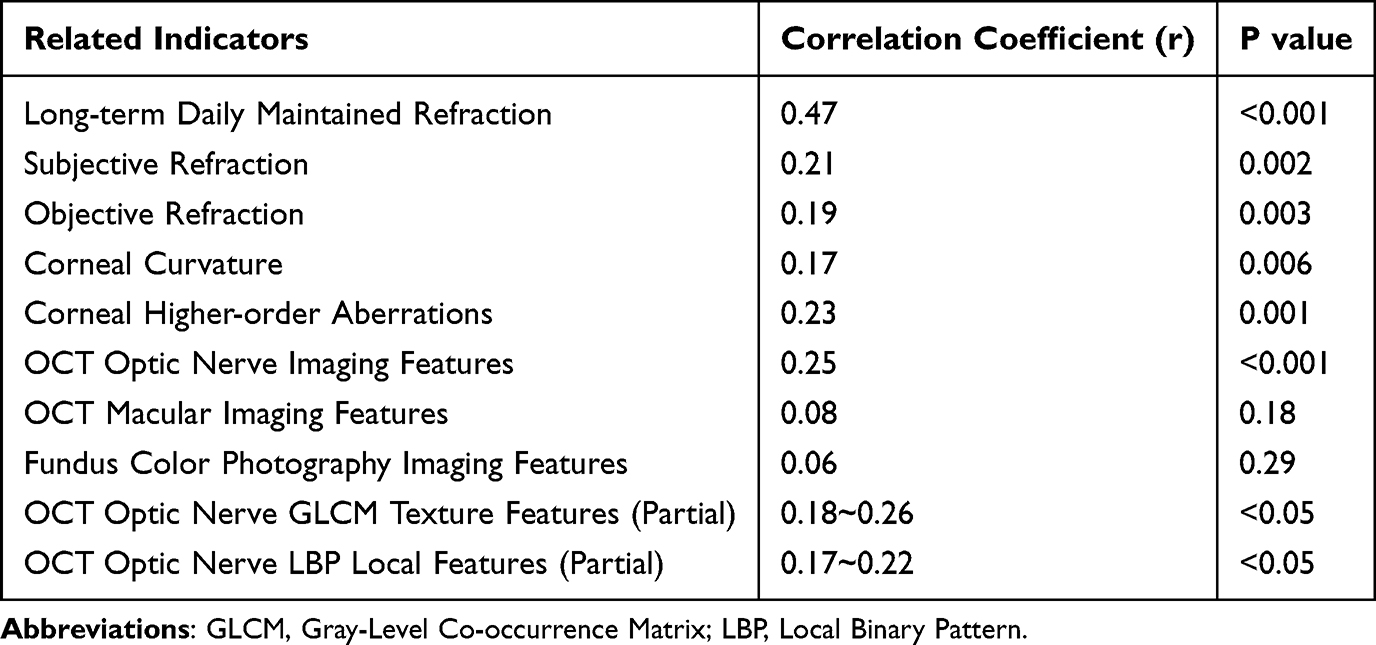 |
Table 2 Correlation Between the Difference Between Subjective and Objective Refraction and Related Indicators |
Subgroup analysis by feature type revealed the following: ① GLCM texture features (32-dimensional): 8 features were correlated with the difference (r=0.18~0.26, P<0.05), all from OCT optic nerve images, with contrast (r=0.26, P<0.001) and correlation (r=0.23, P=0.001) showing the strongest associations; ② LBP local features (28-dimensional): 5 features were correlated with the difference (r=0.17~0.22, P<0.05), also from OCT optic nerve images, represented by energy (r=0.22, P=0.002) and entropy (r=0.20, P=0.004); ③ HOG shape features (22-dimensional): 3 features were correlated with the difference (r=0.17~0.19, P<0.05), all morphological features of OCT optic nerve images; ④ Statistical features (44-dimensional): 2 features were correlated with the difference (r=0.17~0.18, P<0.05), corresponding to gray statistical parameters of OCT optic nerve images. In contrast, radiomics features from OCT macular images and fundus color photography (76-dimensional total) showed no significant correlation with the refraction difference (r<0.10, P>0.05).
Influencing Factors
Multivariate regression analysis identified three independent risk factors for the refraction difference: long-term daily maintained refraction (β=0.38, P<0.001), corneal higher-order aberrations (β=0.19, P=0.004), and OCT optic nerve features (β=0.17, P=0.018). These three factors jointly explained 32.6% of the variation in the refraction difference (R2=0.326). Notably, the 18 correlated radiomics features did not enter the regression model. Machine learning analysis confirmed 18 key radiomics features (importance >0.02); SVM analysis showed that the accuracy of radiomics features alone was 78.3%, which was lower than the accuracy when combined with clinical parameters (Table 3).
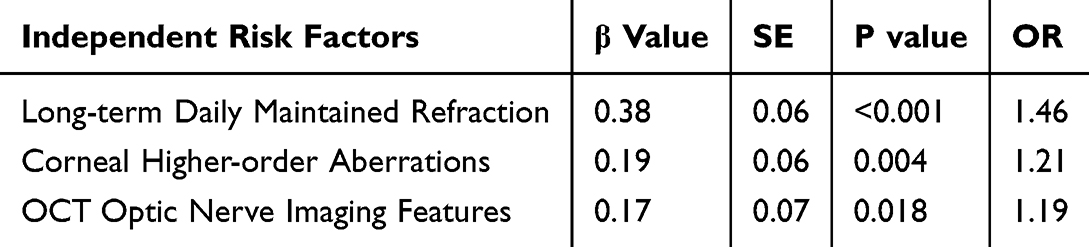 |
Table 3 Independent Risk Factors Affecting the Difference Between Subjective and Objective Refraction |
Prediction Model
The random forest model constructed using key radiomics features and clinical parameters achieved an accuracy of 89.7% (AUC=0.91) in the training set and 87.2% (AUC=0.89) in the validation set, demonstrating good generalization ability (Table 4).
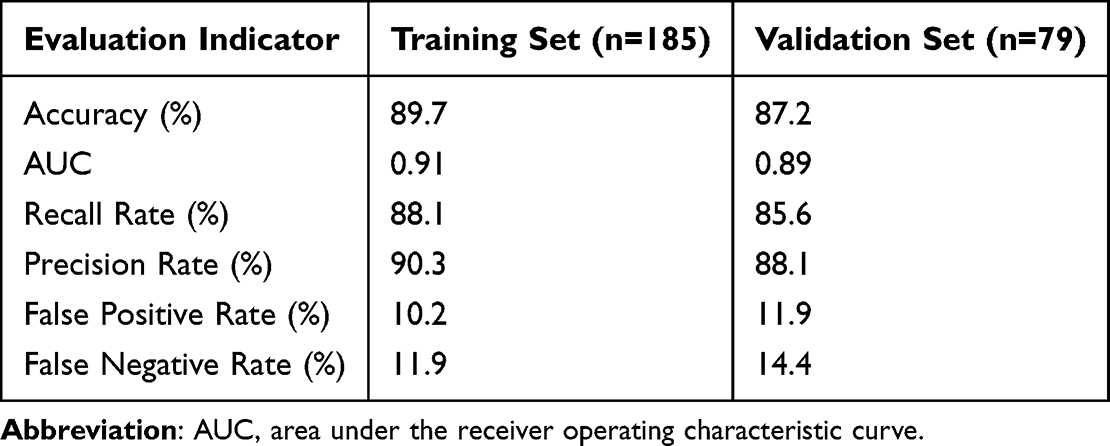 |
Table 4 Evaluation Results of the Prediction Model for the Difference Between Subjective and Objective Refraction |
Discussion
The neuroperceptual difference between subjective and objective refraction is a critical issue in refractive correction. Clarifying its individual variation patterns and correlative mechanisms is essential for improving the personalization of refractive surgery and enhancing postoperative visual quality.19 Through systematic clinical experiments, this study clarified the distribution characteristics of the subjective-objective refraction difference and the strength of associations with various influencing factors, aligning with the preset research objectives.
As the core factor influencing the refraction difference, the moderate correlation between long-term daily maintained refraction and the difference suggests that an individual’s long-term visual habits (eg, spectacle-wearing status) significantly affect the neurovisual system’s subjective perception of refractive status. For long-term spectacle wearers, the eyes adapt to the refractive power of the glasses, leading to a discrepancy between the perceived refractive state during subjective refraction and the objective measurement by instruments. Moreover, longer spectacle-wearing duration and greater deviation between spectacle refraction and subjective refraction are associated with a larger subjective-objective refraction difference. This finding is consistent with clinical observations that subjective refraction results in long-term spectacle wearers with overcorrected myopia often deviate from objective measurements, providing a scientific basis for formulating personalized refractive correction plans that consider patients’ spectacle-wearing habits.
This study found that subjective and objective refraction values themselves were only weakly correlated with the difference, indicating that the magnitude of refraction has limited influence on the discrepancy between the two. Instead, the core influencing factor is the individual’s subjective perception and regulation of refractive status. The weak correlation between corneal morphological features (corneal curvature, corneal higher-order aberrations) and the difference suggests that corneal structure exerts a mild regulatory effect on neuroperceptual differences. This may be because corneal morphology primarily affects the light refraction pathway, while the neurovisual system’s subjective perception is also regulated by multiple links, including the retina and visual pathway. The weak correlation between OCT optic nerve imaging features and the difference indicates that visual pathway structural integrity has a modest impact on neuroperceptual differences, consistent with existing studies showing that retinal nerve fiber layer (RNFL) thickness mainly affects visual acuity,20 not refractive perception.
Feature-by-feature analysis of the 126-dimensional radiomics features further confirmed that only 18 features (14.3%) were weakly correlated with the neuroperceptual difference, all derived from OCT optic nerve images. In contrast, radiomics features from OCT macular images and fundus color photography (76-dimensional total) showed no significant correlation. This finding underscores that the neuroperceptual difference in refractive status is closely associated with optic nerve structural characteristics but not with macular or fundus structural features. The underlying mechanism may be that the optic nerve, as the key pathway for transmitting visual signals from the retina to the visual cortex, its structural integrity and texture characteristics directly affect signal transmission efficiency and processing, thereby interfering with the individual’s subjective perception of refractive status. In contrast, the macular area is primarily responsible for central visual acuity and color vision, and fundus structure is more closely linked to systemic diseases and retinal lesions—factors that have minimal impact on the subjective judgment of refractive status.
Among the 18 correlated radiomics features, GLCM texture features and LBP local features of the optic nerve showed the strongest correlations. This suggests that optic nerve texture uniformity and local gray-level changes may be important factors influencing neuroperceptual differences. These features reflect the density and arrangement of optic nerve fibers; changes in these parameters may alter the neurovisual system’s sensitivity to light refraction signals, leading to discrepancies between subjective perception and objective measurement.
Multivariate regression analysis and machine learning algorithms further supplemented the correlative mechanism: long-term daily maintained refraction, corneal higher-order aberrations, and OCT optic nerve imaging features are independent risk factors for the neuroperceptual difference, jointly explaining 32.6% of the variation. Notably, although the 18 key radiomics features are weakly correlated with the difference, they lack independent predictive value, with their influence indirectly reflected through the overall structural features of the optic nerve. This indicates that the neuroperceptual difference is the result of multiple factors acting synergistically, with long-term visual adaptation playing a dominant role, followed by corneal optical characteristics and optic nerve structural integrity.
The random forest predictive model, constructed by combining key radiomics features, long-term daily maintained refraction, and core clinical parameters, demonstrated high prediction accuracy and good generalization ability. This model provides a novel technical tool for clinical practice, enabling clinicians to preoperatively predict potential subjective-objective refraction differences, adjust refractive correction plans in a timely manner, and improve the precision of refractive surgery—representing the practical application value of this study’s findings. This model can quantitatively evaluate the risk of individual refraction discrepancies before surgery, help clinicians adjust surgical schemes in advance, and improve the accuracy of refractive correction, with important clinical translational value.
This study aligns with some existing research but also introduces key innovations. As noted in the Introduction, most previous studies have focused on the correlation between single clinical indicators and the subjective-objective refraction difference, with few systematically analyzing the association between multimodal imaging radiomics features and neuroperceptual differences. In contrast, this study integrates 126-dimensional radiomics features extracted from multimodal imaging, combines clinical parameters and machine learning algorithms, clarifies key influencing factors and their correlation strengths, and constructs a practical predictive model—enriching research on the mechanisms of neuroperceptual differences in refractive correction. Additionally, this study uses the “single eye” as the independent research unit, avoiding interference from inter-eye differences and enhancing the scientific rigor and reliability of the results.
This study also has limitations that require further refinement in future research. First, the study population is limited to myopic patients aged 18–45 years, which may restrict the generalizability of the results. Given the research objective of providing technical support for personalized refractive surgery, future studies should expand the sample scope to include hyperopic, astigmatic patients, and different age groups to verify the universality of the conclusions. Second, the radiomics features in this study are extracted from static multimodal images, without considering dynamic changes in the optic nerve and visual pathway. Future research could integrate functional imaging technologies to explore the dynamic mechanisms of neuroperceptual differences, further clarifying the regulatory role of the neurovisual system in refractive perception. Third, the predictive model is based on a single-center sample; its performance requires validation with multi-center, large-sample clinical data to improve its clinical applicability and promote its widespread use in clinical practice.
Conclusion
Based on the systematic analysis of 264 myopic eyes, this study confirms that the neuroperceptual difference between subjective and objective refraction exhibits significant individual variability, with long-term daily maintained refraction as its core influencing factor. Among multimodal imaging features, only OCT optic nerve-related radiomics features show a weak correlation with the difference, and corneal higher-order aberrations and OCT optic nerve imaging features are independent risk factors. The predictive model constructed based on key features can accurately evaluate the neuroperceptual difference, providing a theoretical basis and technical support for the precise diagnosis and treatment of refractive correction. With the continuous advancement of multimodal imaging and AI technology, future research can further explore the underlying mechanisms of neuroperceptual differences, optimize the predictive model, and promote the development of personalized refractive correction technologies to better meet clinical patient needs.
Clinical Trial Registration
This study was registered in the Chinese Clinical Trial Registry (ChiCTR2600122125).
Data Sharing Statement
No individual deidentified participant data, raw ophthalmic imaging data, or original individual-level clinical records will be shared publicly. Only the aggregated analytical data and statistical results presented in this manuscript are available. Study-related documents including the research protocol, sample size calculation formula, and statistical analysis scripts are retained by the research team and not publicly released. Qualified researchers requiring supplementary materials for legitimate academic research may contact the corresponding author via the published Email address ([email protected]) to submit access requests. All data access applications will be valid and processed for 2 years after the official publication of this manuscript.
Funding
This study was supported by the Zhejiang Province Science and Technology Plan Project (Grant No. 2026C02A1186) and the Zhejiang Province Medical and Health Science and Technology Plan Project (Grant No. 2025KY1201).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang J, Zheng L, Zheng C, Sun P. A comparison of three cylindrical treatment strategies for topography-guided LASIK: manifest, topographic, and ZZ VR cylinders. Clin Ophthalmol. 2023;17:1335–8. doi:10.2147/OPTH.S408101
2. Zhang J, Shao J, Cao X, Zhang Y, Zheng L. Fitting-shape-based strategy for topography-guided LASIK: a prospective study. J Refract Surg. 2024;40(5):e336–e343. doi:10.3928/1081597X-20240415-01
3. Cao X, Zhang J, Shao J, Zhang Y, Zheng L. Study of the innoveyes sightmap platform in comparing ray-tracing-guided LASIK and topography-guided LASIK. J Refract Surg. 2024;40(12):e994–e1002. doi:10.3928/1081597X-20241030-03
4. Cao X, Zhang J, Shao J, Zhang Y, Zheng L. Optimization of ray-tracing-guided LASIK outcomes: a prospective comparative study of ZZ innoveyes strategy versus automated strategy. Clin Ophthalmol. 2024;18:1879–1888. doi:10.2147/OPTH.S468069
5. Fukushima M, Hirota M, Yukimori T, et al. Evaluation of objective and subjective binocular ocular refraction with looking in type. BMC Ophthalmol. 2024;24(1):170. PMID: 38627750; PMCID: PMC11020990. doi:10.1186/s12886-024-03449-y
6. Lei Y, Chen X, Cheng M, et al. Comparisons of objective and subjective refraction with and without cycloplegia using binocular wavefront optometer with autorefraction and retinoscopy in school-age children. Graefes Arch Clin Exp Ophthalmol. 2023;261(5):1465–1472. doi:10.1007/s00417-022-05936-8
7. Kemchoknatee P, Sunlakaviset P, Khieokhoen N, Srisombut T, Tangon D. A comparison of autorefraction and subjective refraction in an academic optometry clinic. Cureus. 2023;15(4):e37448. doi:10.7759/cureus.37448
8. Müller J, Chen X, Ohlendorf A, Li L, Wahl S. Method comparison and overview of refractive measurements in children: implications for myopia management. BMJ Open Ophthalmol. 2024;9(1):e001322. doi:10.1136/bmjophth-2023-001322
9. Jorge J, Fernandes P. Comparative accuracy of Plusoptix A16, vision screener V100, and grand seiko WAM-5500 autorefractors versus subjective refraction. Clin Exp Optom. 2025;108(8):1047–1054. doi:10.1080/08164622.2025.2458161
10. Hashemi H, Mirzaeian M, Narooie F, et al. Agreement of fixation disparity curve between two different instruments. Optom Vis Sci. 2021;98(6):629–635. doi:10.1097/OPX.0000000000001708
11. Xian S, Tang Y, Ji P, et al. Comparison of agreement and accuracy using binocular wavefront optometer with autorefractor and phoropter. J Vis Exp. 2025;(223). doi:10.3791/68422.
12. Vaphiades MS. Imaging the neurovisual system. Ophthalmol Clin North Am. 2004;17(3):465–80, viii. doi:10.1016/j.ohc.2004.05.013
13. Russell GE, Bergmanson JP, Barbeito R, Cross WD. Differences between objective and subjective refractions after radial keratotomy. Refract Corneal Surg. 1992;8(4):290–295. doi:10.3928/1081-597X-19920701-09
14. Jinabhai A, O’Donnell C, Radhakrishnan H. A comparison between subjective refraction and aberrometry-derived refraction in keratoconus patients and control subjects. Curr Eye Res. 2010;35(8):703–714. doi:10.3109/02713681003797921
15. Kozlov Y, Kinori M, Armarnik S, et al. Subjective versus objective refraction in healthy young adults. BMC Ophthalmol. 2024;24(1):79. doi:10.1186/s12886-024-03340-w
16. Nemeth G, Lipecz A, Szalai E, Berta A, Modis L Jr. Accommodation in phakic and pseudophakic eyes measured with subjective and objective methods. J Cataract Refract Surg. 2013;39(10):1534–1542. doi:10.1016/j.jcrs.2013.04.030
17. Cochran WG. Sampling Techniques. 3rd Ed. 1977.
18. Akçay MB, Oğuz K. Speech emotion recognition: emotional models, databases, features, preprocessing methods, supporting modalities, and classifiers. Speech Communication. 2020;116:56–76. doi:10.1016/j.specom.2019.12.001
19. Nemeth G, Kemeny-Beke A, Modis L Jr. Comparison of accuracy of different intraocular lens power calculation methods using artificial intelligence. Eur J Ophthalmol. 2022;32(1):235–241. doi:10.1177/1120672121994720
20. Park JY, Choi J, Oh WH, Kim JS. Influence of RNFL thickness on visual acuity and visual field in bilateral temporal optic atrophy. J Korean Ophthalmoll Soc. 2016;57(6):969. doi:10.3341/jkos.2016.57.6.969
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.