Back to Journals » Vascular Health and Risk Management » Volume 19
Mechanical Aortic Valve Thrombosis with Heart Failure Successfully Treated with Oral Anticoagulation: A Case Report
Authors Ababneh M ![]() , Al-Kasasbeh A, Algorani E
, Al-Kasasbeh A, Algorani E
Received 12 June 2023
Accepted for publication 27 August 2023
Published 14 September 2023 Volume 2023:19 Pages 617—620
DOI https://doi.org/10.2147/VHRM.S425525
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Muhannad Ababneh,1 Abdullah Al-Kasasbeh,1 Emad Algorani2
1Division of Cardiology, Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Muhannad Ababneh, Division of Cardiology, Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan, Tel +9622 799964654, Email [email protected]
Background: The use of anticoagulation is mandatory for prevention of prosthetic valve thrombosis (PVT) worldwide, regardless of the valve type or position in the heart. In case a thrombosis causes symptomatic dysfunction, treatment usually includes the use of thrombolytic therapy or surgery. We report a case of PVT involving a patient with a mechanical aortic valve which was treated entirely with the use of anticoagulation therapy (warfarin).
Case Presentation: A 58-year-old man had an aortic valve replacement using a Carbomedics® mechanical valve due to severe aortic stenosis as a result of a calcific bicuspid native aortic valve. He was commenced on warfarin after surgery which was continued thereafter. He presented to our hospital after three years with shortness of breath at rest. On clinical examination, his condition was poor with a New York Heart Association functional classification of IV. He was in sinus rhythm and had an enlarged heart shadow on chest X-ray. Transesophageal echocardiography (TEE) revealed aortic valve regurgitation with vegetations on the anterior valve leaflet causing reduced hemi leaflet motility and a mean pressure gradient of 50 mmHg. Cinefluoroscopy revealed a dysfunctional mechanical valve leaflet. Surgery was at high risk of mortality due to the patient’s clinical status and he was continued on warfarin therapy with close monitoring. Cinefluoroscopy and echocardiography done six months later revealed complete dissolution of thrombus and a normally functioning mechanical aortic valve.
Conclusion: Only a few cases of symptomatic, thrombotic mechanical aortic valve were entirely treated with anticoagulation only. Our patient is one such case who had resolution of symptoms and improvement on NYHA functional classification (IV to I).
Keywords: prosthetic valve thrombosis, PVT, anticoagulation, mechanical aortic valve, PVT management
A Letter to the Editor has been published for this article.
Introduction
A mechanical aortic valve has a lower rate of complications – whether dysfunction or obstruction – and usually has a better performance in comparison with mechanical mitral valves.1 Anticoagulation has been used for decades to reduce mechanical prosthetic heart valve thrombosis and thromboembolic complications.2 When such valve thrombosis occurs, acute decompensation of heart function usually ensues.
Treatment of aortic valve thrombosis is based upon the clinical presentation, the cause of thrombosis or obstruction, and the risk of surgery. The patient’s preference is taken into account when choosing the proper management option. Management options include optimization of antithrombotic therapy, fibrinolytic therapy, and surgery. We report a case of a mechanical aortic valve thrombosis treated entirely with warfarin.
Case Presentation
A 58-year-old gentleman presented to our facility after being diagnosed with aortic valve stenosis 3 years ago due to a calcified bicuspid valve. He underwent uncomplicated aortic valve replacement using a 21 mm Carbomedics® mechanical valve. He was started on warfarin therapy with a target INR of 2.0–3.0 which was established prior to discharge.
His disease course after surgery was complicated by multiple admissions for acute decompensated heart failure, which were managed with intravenous (IV) diuretics. Also, an episode of acute cholecystitis was managed with laparoscopic cholecystectomy, where the oral anticoagulation was temporarily replaced with intravenous heparin under monitoring of sufficient anticoagulation.
About a year after AV replacement, the patient was admitted to the hospital as a case of suspected infective endocarditis. He complained of fatigue and exertional dyspnea. There was no fever, no chills, and no stigmata of infective endocarditis. Transesophageal echo study resulted in finding multiple vegetations on the mitral valve but the study was suboptimal and prosthetic endocarditis was not ruled out despite low probability (absence of fever, negative blood cultures, persistence of symptoms despite treatment with antibiotics). TEE study showed: EF 50%, severe right ventricle (RV) impairment, pulmonary hypertension, pulmonary arterial pressure (PAP) 45 mmHg, multiple vegetations on his native mitral valve, Mitral Regurgitation (MR) III, the prosthetic aortic valve showed a mean gradient of 56 mmHg and Aortic Regurgitation (AR) II–III, and prosthetic endocarditis could not be ruled out. He was discharged in a clinically improved situation after receiving 6 weeks of antibiotic therapy (rifampin, gentamicin and vancomycin).
He had recurrent sub-therapeutic INR readings of 1.2–1.8 despite warfarin dosage modification. Follow-up trans-thoracic echocardiogram one month later revealed no vegetations but revealed aortic valve regurgitation with a mean pressure gradient of 46 mmHg.
He was admitted four months later due to acute decompensated heart failure; he complained of severe shortness of breath at rest (New York Heart Association functional classification of IV). He had bilateral crackles on auscultation extending to his mid lung zone. His weight at admission was 83.6 kg and his chest X-ray revealed marked congestion of the lung field and enlarged heart shadow. After initiation of IV diuretics, his symptoms significantly improved. Trans-thoracic echocardiography revealed a stable ejection fraction of 55%, aortic valve regurgitation with mean pressure gradient of 50 mmHg with Grade II aortic valve regurgitation and restricted motion of one valve leaflet, Grade I–II mitral regurgitation, right ventricular systolic pressure (RVSP) of 45 mmHg, and no vegetations were identified.
He underwent cinefluoroscopy for PVR which revealed a stuck leaflet (Figure 1).
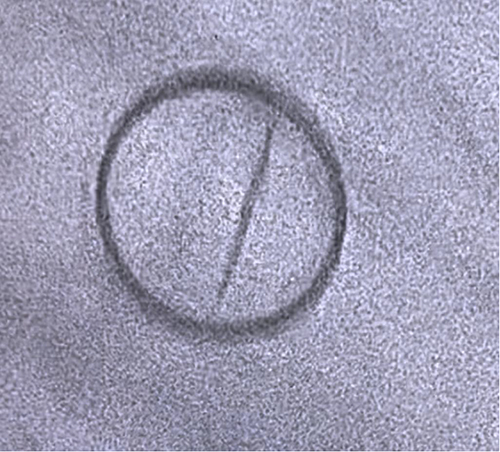 |
Figure 1 Cinefluoroscopy of AVR showing motion restriction to one valve leaflet. |
Surgery as the first therapeutic option was refused because of the high risk of mortality according to the patient's clinical situation, so the patient was continued on anticoagulation and IV diuretics. His condition kept improving until his discharge one month after admission. His weight at discharge was 72.1 kg (weight loss of 11.5 kg). His INR was 3.6 at discharge. He was continued on warfarin therapy with close follow up with a target INR (2.5–3.5).
After 6 months of close follow up, repeated cinefluoroscopy for aortic valve was done which revealed normal motion of both PVR leaflets (Figure 2).
 |
Figure 2 Cinefluoroscopy of AVR showing normal function of both valve leaflets. |
Trans-thoracic echo study done later revealed a stable ejection fraction, Grade II leaking aortic prosthetic valve with a mean pressure gradient of 30 mmHg, Grade I–II mitral regurgitation, RVSP of 40 mmHg, and no vegetation or thrombus was observed.
The patient is currently in a fair condition with New York Heart Association functional class I.
Discussion
Prosthetic heart valve thrombosis is a serious PVR complication with high morbidity and mortality, even though it can happen within the first few years after surgery in an uncomplicated and mostly unnoticed manner.3 In some cases, it can take a devastating course with the need for urgent treatment. Thrombus on the PVR limiting the valve functionality and elevating the risk of systemic embolization represents a serious and a feared complication after the procedure.4 The significant morbidity and mortality associated with this condition – mainly a dysfunctioning valve with its effect on circulation and the potential for thromboembolism – warrants rapid diagnostic evaluation and management. However, diagnosis can be challenging, mainly because of variable clinical presentations and the degree of valvular obstruction. Clinical presentation may vary from mild dyspnea to severe respiratory failure, rapid worsening of heart failure, and signs of systemic embolization. Transthoracic echocardiography, transesophageal echocardiography, and cinefluoroscopy (for mechanical valves) represent the main diagnostic procedures.5 In addition, prosthesis location, impaired cardiac function, the presence of atrial fibrillation, and previous thromboembolism are all factors that elevate the risk of thrombosis.6
The optimal management for prosthetic heart valve thrombosis remains controversial. The different therapeutic modalities include intensive anticoagulation therapy, thrombolytic treatment, and emergency surgery. Prosthesis location, thrombus size, and clinical status will guide the choice between surgery and medical treatment.7
Clearly, surgery or thrombolytic therapy remains the treatment of choice in patients with prosthetic valve thrombosis, associated with hemodynamic instability, and in those with large mobile thrombi and high embolic risk. However, both reoperation and fibrinolytic therapy carry significant risk.3
In hemodynamically stable patients with PVT, clinically in NYHA class I–II and small thrombus (<0.8 cm2), treatment with continuing a sufficient anticoagulation with a vitamin K antagonist (VKA) seems to be reasonable, and in most cases the treatment of choice.8
In patients with hemodynamic instability, a regimen of intravenous heparin should be started, followed by either thrombolysis or surgery.9 If NYHA functional class is III–IV and a large thrombus is present, emergent surgery is usually recommended.9,10
Conclusions
In conclusion, this study demonstrates that in the case of prosthetic valve thrombosis, medical management can be a choice when surgery is not a feasible option. Keeping an appropriate anticoagulation beside medical therapy of the resulting symptoms.
In our symptomatic patient with severely decompensated clinical situation (NYHA functional class IV) where surgery was not a valid option, the medical therapy was restricted to treatment of heart failure and anticoagulation with VKA under narrow monitoring of his INR. This case of PVT was entirely treated medically, what was a sufficient option to completely resolve the thrombus and improve the clinical findings.
Ethics and Consent Statements
The patient in this study has given written consent to participate as well as consent to publish his data. Institutional approval was not required to publish the case details.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lim WY, Lloyd G, Bhattacharyya S. Mechanical and surgical bioprosthetic valve thrombosis. Heart. 2017;103(24):1934–1941. doi:10.1136/heartjnl-2017-311856
2. Leiria TLL, Lopes RD, Williams JB, et al. Antithrombotic therapies in patients with prosthetic heart valves: guidelines translated for the clinician. J Thromb Thrombolysis. 2011;31(4):514–522. doi:10.1007/s11239-011-0574-9
3. Lengyel M. Management of prosthetic valve thrombosis. J Heart Valve Dis. 2004;13(3):329–334.
4. Tiede DJ, Nishimura RA, Gastineau DA, et al. Modern management of prosthetic valve anticoagulation.
5. Vahanian A, Alfieri O, Andreotti F, et al.; Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC), European Association for Cardio-Thoracic Surgery (EACTS). Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012;33(19):2451. doi:10.1093/eurheartj/ehs109
6. Mohamed H. Antithrombotic therapy in patients with prosthetic heart valves. Libyan J Med. 2009;4(1):54–56. PMID: 21483507; PMCID: PMC3066703. doi:10.4176/090115
7. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561–632. Erratum in: Eur Heart J. 2022 Feb 18. PMID: 34453165. doi:10.1093/eurheartj/ehab395
8. Mutuberría-Urdaniz M, Rodríguez-Palomares JF, Ferreira I, et al. Non-obstructive prosthetic heart valve thrombosis (NOPVT): really a benign entity? Int J Cardiol. 2015;197:16. PMID: 26113471. doi:10.1016/j.ijcard.2015.06.021
9. Özkan M, Gündüz S, Gürsoy OM, et al. Ultraslow thrombolytic therapy: a novel strategy in the management of PROsthetic MEchanical valve Thrombosis and the prEdictors of outcome. The Ultra-Slow PROMETEE trial. Am Heart J. 2015;170(2):409–418. PMID 26299240.
10. Deviri E, Sareli P, Wisenbaugh T, Cronje SL. Obstruction of mechanical heart valve prostheses: clinical aspects and surgical management. J Am Coll Cardiol. 1991;17(3):646. PMID 1993782. doi:10.1016/S0735-1097(10)80178-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.