Back to Journals » Advances in Medical Education and Practice » Volume 13
Measuring Readiness for Self-Directed Learning in Medical Undergraduates
Authors AlRadini F ![]() , Ahmad N
, Ahmad N ![]() , Ejaz Kahloon L
, Ejaz Kahloon L ![]() , Javaid A, Al Zamil N
, Javaid A, Al Zamil N ![]()
Received 29 January 2022
Accepted for publication 14 April 2022
Published 5 May 2022 Volume 2022:13 Pages 449—455
DOI https://doi.org/10.2147/AMEP.S360333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Faten AlRadini,1 Nadeem Ahmad,1 Lubna Ejaz Kahloon,1 Amrah Javaid,2 Norah Al Zamil2
1Department of Clinical Sciences, College of Medicine, Princess Nourah bint Abdulrahman University, Riyadh, Kingdom of Saudi Arabia; 2Department of Basic Sciences, College of Medicine, Princess Nourah bint Abdulrahman University, Riyadh, Kingdom of Saudi Arabia
Correspondence: Nadeem Ahmad, Department of Clinical Sciences, College of Medicine, Princess Nourah bint Abdulrahman University, Airport Road, King Khalid International Airport, Riyadh, 11564, Kingdom of Saudi Arabia, Tel +966531413328, Email [email protected]
Purpose: To measure the readiness for self-directed learning in medical students for the evaluation of self-directed learning in the study population.
Materials and Methods: The survey was conducted in undergraduate students. The instrument used was Fisher’s readiness scale comprising of self-management, desire for learning, and self-control domains. The data were analyzed by Mann–Whitney U-test and bivariate and partial correlations. The results were compared with the reported ones.
Results: Total students surveyed were 300. Of these, 96 responded - 73 (76%) of preclinical and 23 (24%) of clinical classes. The mean readiness score was 124. The mean domains’ scores for self-management, desire for learning, and self-control were 38, 38, and 48, respectively. The preclinical group had a mean score of 122 for readiness, 37 for self-management and desire for learning each, and 48 for self-control. The clinical group’s scores were 129, 40, and 49, respectively. Preclinical and clinical groups differed significantly in self-management domain (P = 0.03). The difference was not significant in desire for learning (P = 0.08), self-control domains (P = 0.40) and readiness score (P = 0.12). The domains of self-control and desire for learning had a positive correlation if self-management was controlled, and self-control and self-management had a positive correlation if desire for learning was controlled (P < 0.05).
Conclusion: The measurement of readiness for self-directed learning helps in knowing the true value of self-directed learning in a particular setting. Relatively lower scores in our study mean self-directed learning alone cannot be relied upon to achieve optimum students’ learning. There is also a need for implementing strategies that will help students in improving their readiness for independent learning.
Keywords: self-directed learning, readiness for self-directed learning
Introduction
Self-directed learning (SDL) means self-managed learning. First introduced by Malcolm Knowles in 1978, it became popular because it was considered superior to teacher-directed learning in achieving adult learning.1 SDL motivates students and generates their interest in learning, thereby enabling them to retain and utilize whatever they learn. It also prepares them to be lifelong learners so they may remain abreast with ever-expanding knowledge and new developments2–4 Not least, SDL is also an essential component of problem-based learning.3,5
SDL, however, can work only if learners possess certain key characteristics, such as self-confidence, curiosity, critical thinking, and decision-making abilities.6 SDL readiness (SDLR) is the degree to which an individual possesses these qualities.7 It varies widely amongst individuals – some being minimally self-directed and so heavily teacher dependent while others are entirely independent. It will be hard for a group of students with a low SDLR to cope with SDL, while the one with a high SDLR will make the best use of it. A teaching method that matches the students’ SDLR level offers the best opportunity for their learning. Thus measurement of SDLR can be vital for educational planning. It will reveal students’ strengths and weaknesses and, therefore, the areas to target for better learning. Further, knowledge of students’ SDLR will help in developing the most appropriate teaching model and the curriculum.
At the graduate level, our institution has adopted a hybrid problem-based curriculum, of which SDL is an essential component. Therefore, we conducted the present study to get undergraduate students’ perspectives regarding their SDLR. The information gathered could then be used to judge how much SDL can be relied upon to meet the learning needs of the students.
We used Fischer’s readiness scale for measuring SDLR. It was initially devised for nurses but later also validated for medical students.8–10
Materials and Methods
The undergraduate students in the first to fifth years of the session 2017–2018 at the College of Medicine, Princess Norah University, Riyadh, were included in the study. Informed consent was obtained from all the students prior to their participation in the study. The study complied with all the provisions of the Declaration of Helsinki. It was approved by the Institutional Review Board of Princess Nourah Bint Abdulra hman University vide its letter dated September 20, 2018 (IRB Log Number: 18–0234).
It was a cross-sectional study with non-probability convenient sampling. The questionnaire was sent online to 300 students and the responses were self-administered. The data was collected over three months. The first-year and second-year students were grouped as pre-clinical while the third, fourth and fifth-year ones as clinical. We used the Fisher’s readiness scale which comprised of 40 questions and 200 total point scores. It had three sections covering the domains - self-management [SM], desire for learning [DL], and self-control [SC] – each having 13, 12, and 15 questions which amounted to 65, 60, and 75 points per section respectively. Following Fisher’s lead, an SDLR score of more than 150 and SM, DL and SC domains’ score of 47, 44, and 59 or more respectively were considered optimum.
We recorded the response to each question on a Likert scale of 1 to 5. Items numbers 7, 20, 27, and 33 were scored in reverse order. The data was analyzed using the software SPSS version 23. The readiness score was calculated by summing up the domains’ scores. All the scores were calculated as mean ± standard deviation and rounded off for final analysis. Mann–Whitney U-test was used for comparing the clinical and preclinical groups. The correlation between the domains was determined by bivariate and partial correlation coefficients. A p-value < 0.05 was considered significant.
Results
Total number of students who responded to the questionnaire was 96. Of these, 73 (76%) were in the preclinical and 23 (24%) in the clinical group. The mean readiness score was 124. The mean domains’ scores for self-management, desire for learning, and self-control individually were 38, 38, and 48 respectively. The preclinical group had a mean score of 122 for readiness, 37 for SM and DL each, and 48 for SM. The respective scores for the clinical group were 129, 40, and 49. The details are shown in Tables 1, 2 and 3.
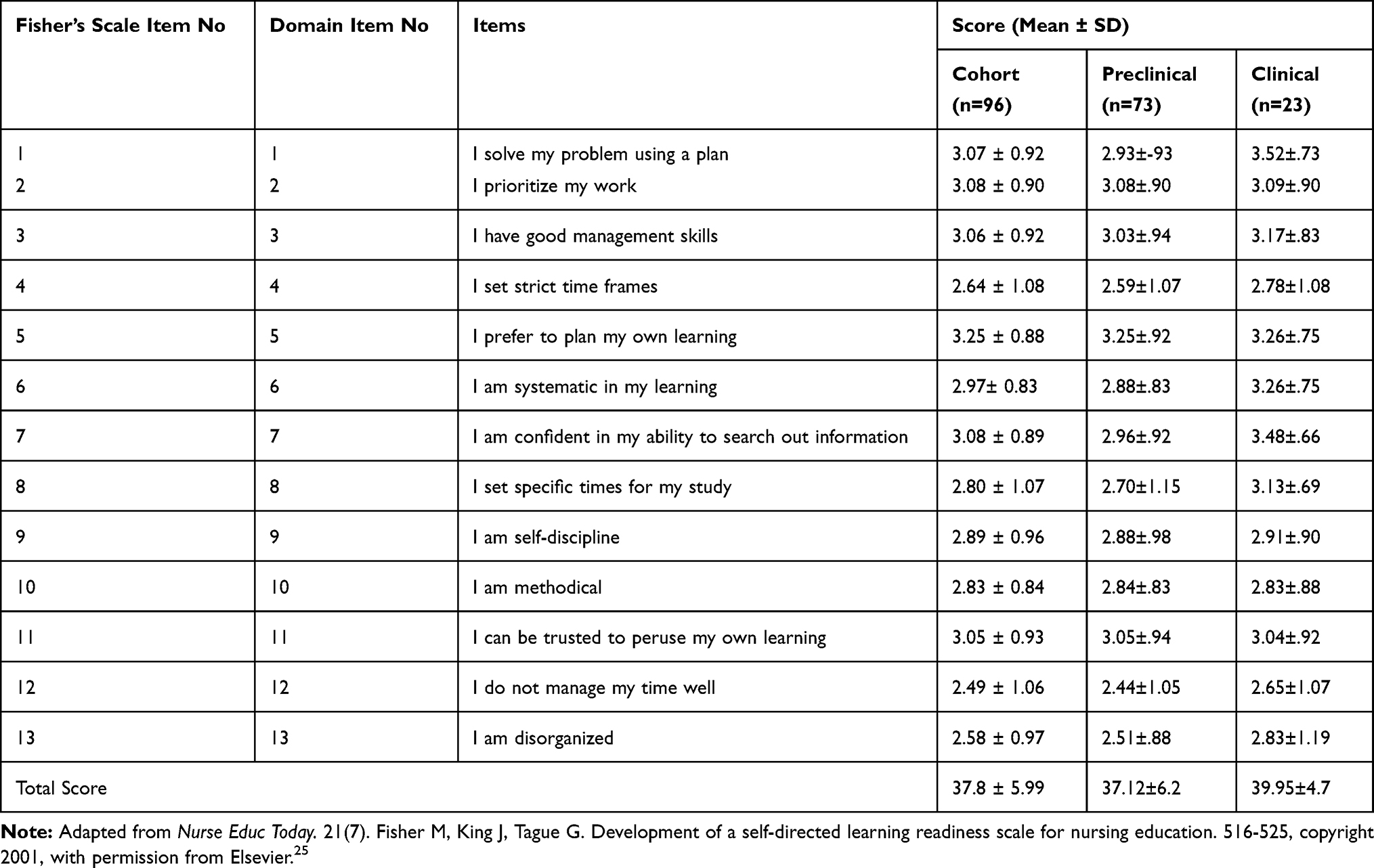 |
Table 1 Scores in Self-Management Domain |
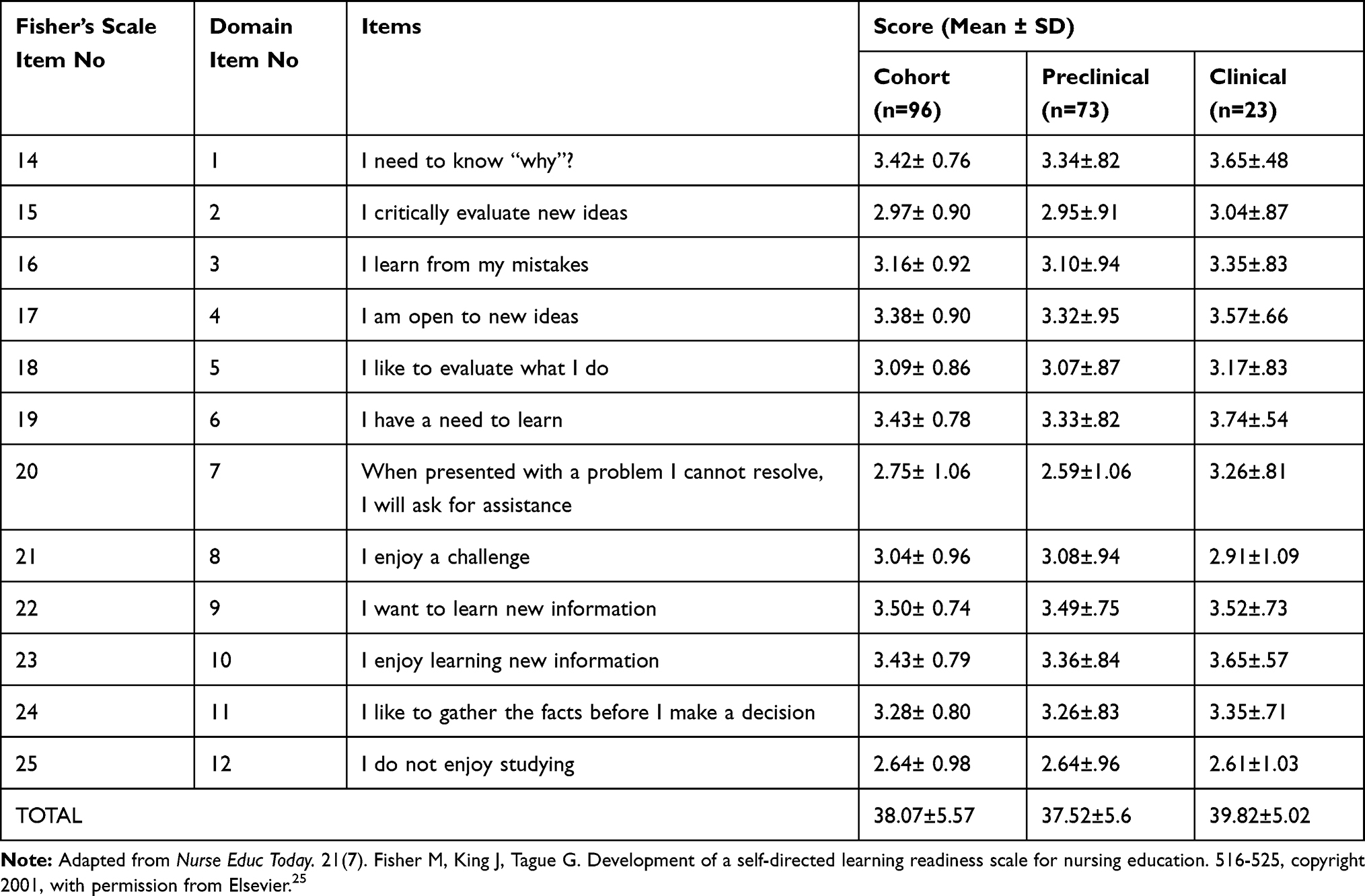 |
Table 2 Scores in “Desire for Learning” Domain |
 |
Table 3 Scores in “Self-Control” Domain |
Preclinical and clinical groups differed significantly in self-management domain (P=0.03) but not in desire for learning (P=0.08) and self-control domains (P=0.40) and the readiness score (P=0.12) [Table 4].
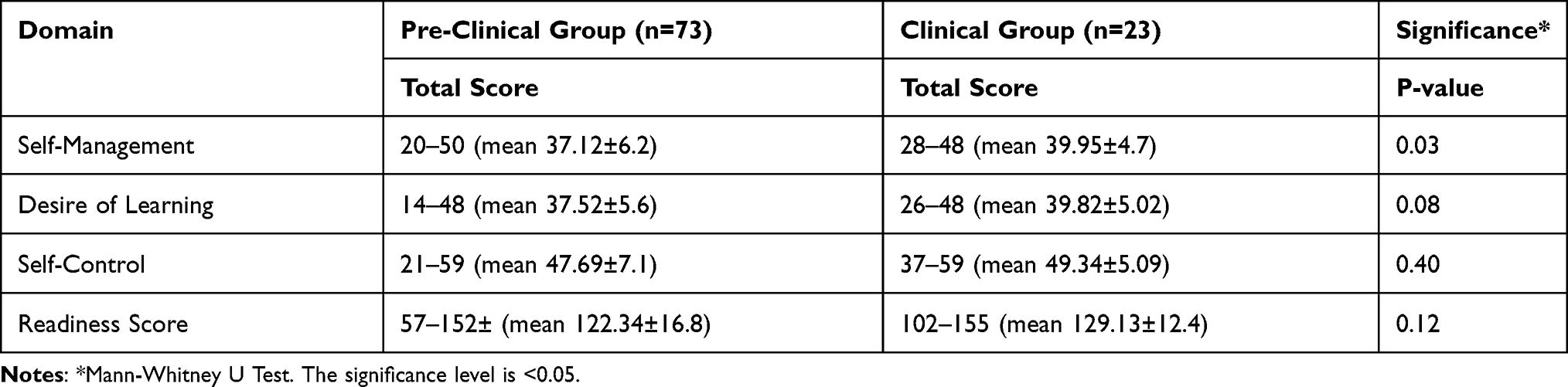 |
Table 4 Comparison of Scores in Pre-Clinical and Clinical Groups |
We did a bivariate and partial correlation – the latter by controlling one of the domains, to find out the relationship amongst the three domains. If either SM or DL was controlled, a strong positive correlation was found between the two remaining domains (p-value= < 0.05). However, a moderate negative correlation was found between SM and DL when SC was controlled (p-value =0.39). The details are shown in Table 5.
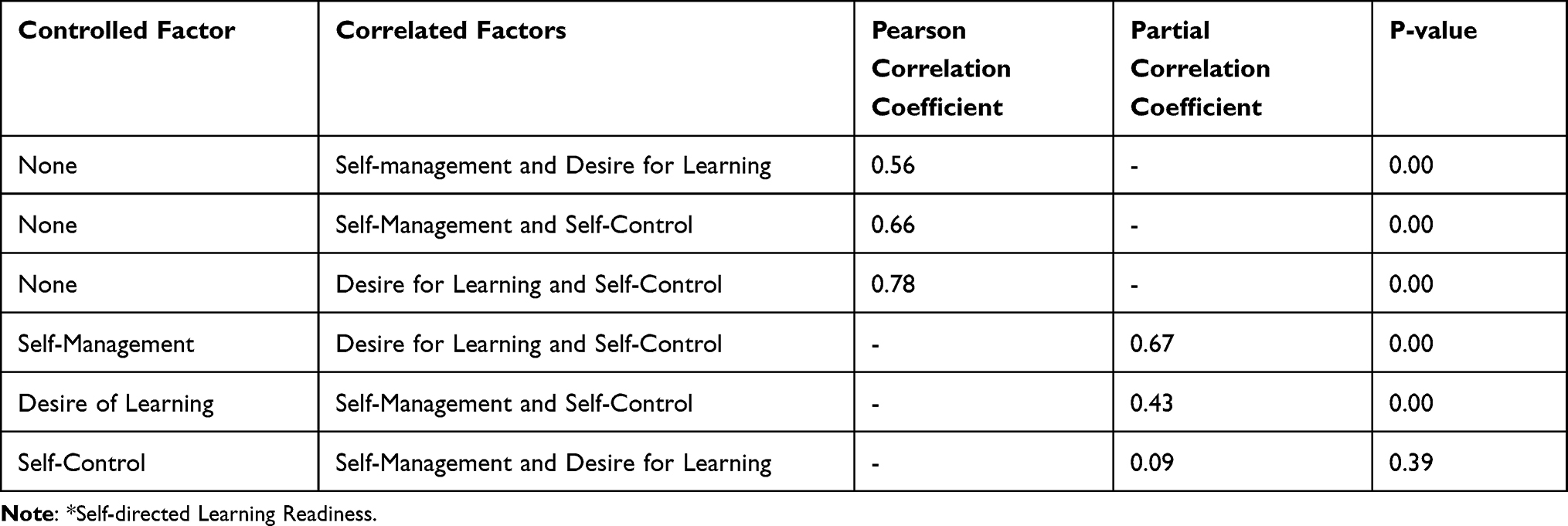 |
Table 5 Correlation between Domains of SDLR* |
Discussion
SDL has become the hallmark of higher education. This model hinges on extrinsic factors, such as learner’s instructional processes, and intrinsic factors, such as learner’s internal characteristics.11 SDLR, which denotes the latter, is the backbone of SDL. Its concept is not new but yet not given due weightage in educational planning. Our study brings to light its importance. Measuring SDLR among the local population highlights its variability in different settings and provides insight into the factors influencing students’ learning.
The majority of authors considered a mean SDLR score of > 150 to be optimum for the Fisher scale that we used in our study.9,12–14 However, in the survey by Devi et al15 the corresponding value was > 129. Our SDLR score of 124 falls short of both these values. Studies employing other instruments to measure SDLR had diverse rankings and threshold scores for optimum SDLR, making it challenging to do a straightforward conversion and numerical comparison of these studies with ours.16–19 Notably, though, their scores exceeded the minimum desired level for their respective standards for optimum SDLR. Our score, falling below the desired level by our scale, thus has the same ranking even when compared with the studies using different scales.
Low SDLR in our study could be due to many reasons, such as the students’ attributes, their cultural and educational background, and unfamiliarity with the process.6,20 To have good SDLR and be proficient independent learners, the students need to be fostered for SDL at a very young age. They have to be encouraged to participate in learning activities that promote their intellectual growth and cognitive functions to help control their behavior, emotions, motivation, and self-regulate. The techniques to improve self-direction skills in higher education are the individualized teaching-learning process and contract learning.21
SDLR score reflects the overall level of students’ disposition towards SDL while scores in various domains depict the students’ specific strengths and weaknesses. In our study, the score was highest in SC, and those in SM and DL were the same. As was true for the SDLR score, the domains’ scores were also lower than the desired ones for the respective domains though these matched in the ranking.9,10,14,15,20
We grouped our subjects as preclinical and clinical for a more revealing comparison given the paradigm shift in the curriculum of basic and clinical sciences and the consequent change in learning dynamics. The changeover is evident from the finding that early clinical exposure augments SDL skills irrespective of the type of curriculum.19 In line with this contention, our two groups differed in the SDLR and domains’ scores, though the difference was statistically significant in the SM domain only.
The higher scale and subscale values in the clinical than in the preclinical group reflect the maturational process of developing self-directedness. It also means that SDLR is not a static attribute but is improvable by adopting appropriate strategies. Our results conform those of many studies that have shown an upward trend in the readiness score as the students move from junior to senior classes.15,19 In some studies, a decline or little change was found in the readiness score with the increasing year of study;16,17,19 one reported higher scores for the first and fourth-year than those of other students.14 The author attributed it to the changes in students’ attitudes and enthusiasm at the start and end of the course.
Partial correlation analysis showed various domains of SDLR to be inter-dependent and not mutually exclusive. For example, students with good SC are likely to have better SM and DL and greater readiness for SDL. It further showed that certain attributes are complementary to one other.
Some researchers have tried to find a correlation between the readiness score and students’ academic performance. Their findings, however, have been quite contradictory - many reporting a poor relationship between the two.15,18 It might be due to the difference in their determinants - the former depending upon the ability to utilize a particular learning method and the latter, on the depth and breadth of learners’ knowledge base.14 On the contrary, a few studies have shown a higher SDLR associated with a significantly higher academic success19,22 – indicating an overlap of the skills required for either SDL or academic success – particularly those related to self-management.
One of the studies has reported a positive correlation between self-direction skills and lifelong learning.19 With one-time data and without a follow-up, our study could not explain the relationship between SDLR and academic performance or lifelong learning.
A self-reporting questionnaire in our study provides the students’ perspective of their readiness. Being subjective, however, it might not reflect the actual level of their readiness.15 The teachers’ perspective about students’ readiness might be quite the opposite of students themselves.4,5 It is also worth noting that the readiness scale is a predictor and not the measure of students’ success in self-direction.
Readiness for SDL is only one determinant of the effectiveness of SDL. Equally crucial in this regard is the learning environment to which the students are exposed and which depends on many factors, such as the instructional processes, teachers’ collaboration, use of technology, and administrative and technical support services. All these components need to be also evaluated for a comprehensive assessment of SDL’s utility in a particular setting.23 Ideally, the SDL model chosen should fit both the level of students’ readiness and the prevailing learning environment.3 The model thus could vary from a very structured process grounded in behaviorism to complete learner’s autonomy based on a humanistic approach.21
Self-direction, despite its attraction, may not be applicable in all situations.4,5,24 Further, a person’s ability of self-direction may vary with the circumstances. SDL needs to be implemented more consciously where the SDLR is modest and the learning environment less conducive.3 The employment of an integrated or a hybrid curriculum in such situations might be the better option.4
The response rate in our study seems low, particularly in higher classes. It could be because, unlike 1st and 2nd-year students, third, fourth, and 5th-year students, were too busy in their clinical rotations to remain in touch with college tutors who could have persuaded them to participate in the study. Furthermore, SDL surveys might attract junior students because they are less familar with the existing education system and more open and inquisitive about novel learning techniques.
Our data was about a limited number of students who belonged to a single institution. Large, multi-institutional, multidimensional, and longitudinal studies would be required to define the true scope and value of SDL.
Conclusion
The measurement of readiness for self-directed learning is essential to determine the utility of self-directed learning in a particular setting. Relatively lower scores in our study mean a hybrid system incorporating both self-directed and teacher-based learning may be more appropriate for the institutions like us. Strategies may also be implemented in lower education to assist students to improve their readiness for independent learning for the coming times.
Abbreviations
SDL, self-directed learning; SDLR, self-directed learning readiness; SC, self-control; DL, desire for learning; SM, self-management.
Data Sharing Statement
The data of the study is being kept by the corresponding author and is accessible through him.
Consent for Publication
All the authors have consented for the submission and publication of the manuscript.
Acknowledgments
Our thanks are due to Dr. Patrick Ottoman of Abington-Jefferson Hospital, U.S, for proofreading the manuscript and giving valuable suggestions in this regard.
Funding
No funding has been received.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Knowles M. Self-Directed Learning: A Guide for Learners and Teachers. New York, USA: Association Press; 1975. 135.
2. Kar S, Premarajan K, Ramalingam A, Iswarya S, Sujiv A. Self-directed learning readiness among fifth-semester MBBS students in a teaching institution of South India. Education Health. 2014;27:289.
3. Loyens SMM, Magda J, Rikers RMJ. P. Self-directed learning in problem-based learning and its relationships with self-regulated learning. Educ Psychol Rev. 2008;20:411–427.
4. Greveson GC, Spencer JA. Self-directed learning - the importance of concepts and contexts. Med Edu. 2005;39:348–349.
5. Chang BJ. Problem-based learning in medical school: a student’s perspective. Ann Med Surg. 2016;12:88–89.
6. Kindy S, Kindy F, Kindy AAI. The advantages and disadvantages of self-directed learning: a survey - study of Saudi medical students. MedEdPublish. 2018;2:11–16.
7. Gould J, Dalziel S, Petropolis H, Mann K, Arseneau I. Student use of self-directed learning time in an undergraduate medical curriculum. Dalhousie Med J. 2015;42(1):8–12.
8. Fisher MJ, King J, Tague G. Development of a self-directed learning readiness scale for nursing education. Nurse Educ Today. 2001;21:516–525.
9. Fisher MJ, King J. The self-directed learning readiness scale for nursing education revisited: a confirmatory factor analysis. Nurse Educ Today. 2010;30:44–48.
10. Hendry GD, Ginns P. 2009) Readiness for self-directed learning: validation of a new scale with medical students. Med Teach. 2009;31(10):918–920.
11. Saks K, Leijen A. Distinguishing self-directed and self-regulated learning and measuring them in the E-learning context. Procedia Social Behav Sci. 2014;112:190–198.
12. Abraham RR, Fisher M, Asha K, A T I, Nabila S, Atikah NN. Exploring first-year undergraduate medical students’ self-directed learning readiness to physiology. Adv Physiol Educ. 2011;35:393–395.
13. Gyawali S, Jauhari AC, Shanker PR, Saha A, Ahmed M. Readiness for self-directed learning among first semester students of a medical school in Nepal. JCDR. 2011;5:20–23.
14. Balamurugan S, Kumar H. Self-directed learning readiness (SDLR) among medical students: a questionnaire-based study from an Indian medical school. South East Asian J Med Edu. 2015;99:59–64.
15. Devi V, Devan D, Chen Soon P, Han WP. Comparison of self-directed learning readiness among students experiencing hybrid and traditional curriculum. JCDR. 2012;6:1047–1050.
16. Premkumar K, Pahwa P, Banerjee A, Baptiste K, Bhatt H, Hyun L. Does medical training promote or deter self-directed learning? A longitudinal mixed- methods study. Acad Med. 2013;88:1744–1746.
17. Premkumar K, Vinod E, Sathishkumar S, et al. Self-directed learning readiness of Indian medical students: a mixed-method study. BMC Med Educ. 2018;18:134.
18. Kidane HH, Roebertsen H, van der Vleuten CPM. Students’ perceptions towards self-directed learning in Ethiopian medical schools with new innovative curriculum: a mixed-method study. BMC Med Educ. 2020;20:1–10.
19. Askin Tekkol I, Demirel M. An investigation of self-directed learning skills of undergraduate students. Front Psychol. 2018;9:1–14.
20. Madhavi KVP, Madhavi B. Readiness for self-directed learning among undergraduate medical students of Andhra Medical College, Visakhapatnam. Int J Community Med Public Health. 2017;4:2836–2840.
21. Hiemstra R. Self-directed learning: why do most instructors still do it wrong? Int J Self Directed Learning. 2013;10:23–34.
22. Cazana AM, Schiopca BA. Self-directed learning, personality traits, and academic achievement. Procedia Social Behav Sci. 2014;127:640–644.
23. Din N, Haron S, Rashid RM. Can self-directed learning environment improve quality of life? Procedia Social Behav Sci. 2016;222:219–227.
24. Schmidt HG. Assumptions underlying self-directed learning may be false. Med Ed. 2000;34:243–245.
25. Fisher M, King J, Tague G. Development of a self-directed learning readiness scale for nursing education. Nurse Educ Today. 2001;21(7):516–525.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.