Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Measuring Our Impact: Validation of a Parenting Self-Efficacy Outcome Tool for Caregivers Participating in Developmental Interventions
Authors Nitsche K ![]() , Pieterse B
, Pieterse B ![]() , Lawrence N, Bear N
, Lawrence N, Bear N
Received 12 December 2025
Accepted for publication 14 April 2026
Published 20 May 2026 Volume 2026:19 588567
DOI https://doi.org/10.2147/JMDH.S588567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Karen Nitsche,1 Bridget Pieterse,1 Nicky Lawrence,1 Natasha Bear2
1Child Development Service, Child and Adolescent Health Service, Perth, W.A., Australia; 2Institute for Health Research, Notre Dame University, Perth, W.A., Australia
Correspondence: Karen Nitsche, Child Development Service, Child and Adolescent Health Service, 2 Mill St, Perth, W.A., 6000, Australia, Email [email protected]
Background: Evidence suggests that higher levels of parenting self-efficacy (PSE) result in positive caregiver–child interactions and improved developmental outcomes for children. Currently, there are few PSE tools specific to the domain of parenting a child with a developmental concern that are also applicable to a wide clinical cohort and range of multidisciplinary services.
Aim: This study aimed to develop and validate an outcome measurement tool to determine change in PSE for caregivers who participate in developmental interventions with their child. The development of a minimal clinically important difference (MCID) value was a secondary aim.
Methods: Based on existing literature, and clinician and consumer consultation, the SET and GO, a parenting Self-Efficacy Tool for Gathering Outcomes of developmental interventions, was developed. This nine-item retrospective pretest-posttest scale was validated with 204 caregivers at service discharge. Participants were predominantly mothers (91.7%) caring for children (average age of 5.7 years) presenting with a range of developmental concerns who had participated in intervention with one or more of a range of clinical disciplines.
Results: Exploratory factor analysis indicated that the SET and GO is a unidimensional tool with good internal consistency (Cronbach’s α = 0.94 and 0.93), strong test–retest reliability (quadratic weighted kappa = 0.80 and 0.76), and adequate construct validity. Ceiling effects were noted in some individual item “now” scores. A preliminary MCID value of ≥ 7 was established using a distribution-based method.
Conclusion: The SET and GO is a valid and reliable outcome measurement tool suitable for use with a wide range of caregivers taking part in developmental interventions with their child. Future research with a larger sample will allow investigations into the validity of using the tool with specific populations, and further refinement of the MCID value.
Keywords: child development, neurodevelopmental conditions, outcome measurement tool, patient reported outcome measure, PROM, multidisciplinary, allied health
Introduction
Routine evaluation of the impact of developmental interventions is important to ensure the provision of effective and efficient services and to provide accountability for resourcing.1,2 Best practice in early childhood intervention underscores the need to enhance caregivers’ capacity to support their child’s development; therefore, evaluating the impact of interventions on caregivers is essential.3,4
Parenting Self-Efficacy (PSE)
It is well established that higher levels of parenting self-efficacy (PSE) are related to improved outcomes for children3,5,6 and research demonstrates that change in PSE is a reliable indicator of the impact of a developmental intervention.6 As such, increasing PSE is central to the provision of specialist services for children with developmental concerns.3–5,7 Preliminary evidence suggests that even brief developmental interventions, such as diagnostic assessment, can improve a caregiver’s level of self-efficacy.8
The concept of self-efficacy was originally defined by Bandura as an individual’s belief in their capability to complete a task.9 Self-efficacy is task dependent, with PSE defined as a caregiver’s belief in their ability to successfully carry out the tasks needed in their parenting role.10 According to Bandura9 the concept of self-efficacy is influenced by four factors. These include 1) previous success at a task, 2) opportunities to watch others completing a task, 3) validation from others, and 4) an individual’s emotional state. Relational and participatory help-giving practices, which are the foundation of family-centred practice, work to support the development of PSE, as do the social supports that are available to a caregiver.3–5,11,12
There are also many other factors that have been shown to be negatively associated with PSE. These include parental level of stress,13,14 complexity of the child’s developmental needs,15 and family income.16 There is inconsistent evidence that other factors such as socio-economic status, and level of education are related to PSE.16
Throughout this paper we use the term “parenting” when referring to the role and tasks of any person taking on a parenting role (not just a child’s biological parent).
The Child Development Service Context
The Child Development Service (CDS) is the only government-funded community health service in the metropolitan area of Perth, Western Australia, that provides a multidisciplinary approach to the assessment and management of children aged 0 to 18 years with a range of developmental concerns. CDS is often the first specialised service accessed by families with children who have a range of clinical presentations such as speech and language delay, motor delays, emotional regulation difficulties, hearing loss and neurodevelopmental conditions such as attention deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD). Comparable models can be seen across Australia, as well as internationally, in which interventions take family-centred, capacity-building approaches to optimise developmental outcomes for children. CDS sought a tool to measure the impact of interventions on PSE across the range of clinical services provided. A domain-specific measure was required to assess caregivers’ confidence in supporting their child’s development within everyday contexts.
Existing PSE Tools
PSE tools can be mapped along a spectrum of specificity, from general (not linked to a specific parenting task or role) to domain specific (related to a more defined role such as parenting a child who needs developmental support) to those that are highly task-specific (with items detailing clearly delineated behaviours or skills within a narrow parenting role, for example, preventing challenging behaviours in children with Autism).16–20 Research suggests that task-specific self-efficacy tools demonstrate greater sensitivity to change and better predictive validity than more generalised tools,17 however, these tools are less applicable to a wider cohort of caregivers. CDS required a domain-specific tool to evaluate PSE in relation to the role of supporting a child with a developmental concern. The tool needed to be suitable for use with caregivers who had children aged 0 to 18 years and who had accessed one or several of the range of CDS clinical services.
A review of existing tools found that none met the needs of CDS. Measures were either: (a) not specific to parenting a child with a developmental concern,21–25 (b) focused on health-seeking behaviours rather than supporting developmental needs,26 (c) not suitable for a broad cohort in terms of child age and developmental concerns,27–30 (d) included negatively worded statements that may be difficult for some caregivers to interpret and were incongruent with a strengths-based approach,31 or (e) contained additional content unrelated to PSE.32 These findings align with those of Imms et al3 who reported a lack of tools to measure outcomes for caregivers participating in developmental interventions with their child. Collectively, this highlights a gap in the availability of a strengths-based outcome measurement tool suitable for use within a multidisciplinary child development context where services are provided to a broad clinical cohort.
The aim of the current study was to develop a tool to measure PSE and evaluate its validity, reliability, and interpretability with a diverse sample of caregivers who had participated in developmental interventions with their child. To support interpretability of the tool, the development of a minimal clinically important difference (MCID) value was a secondary aim.
Method
Development of the SET and GO
The SET and GO tool was developed in two phases, guided by best practices in scale development33 and the COSMIN study design checklist for patient-reported outcome measurement instruments.34
Phase One – Conceptual Framework and Item Generation
A working group consisting of senior clinicians in the areas of developmental paediatric medical services, occupational therapy, physiotherapy, speech pathology, social work and clinical psychology was formed to establish a framework for PSE development within the context of family-centred developmental interventions. This framework was then used as the basis for item generation, with items developed through both deductive (literature review and assessment of existing scales) and inductive methods (working group discussion) until it was felt that saturation had been reached. A modified Delphi technique was then used by the working group to reach consensus on which items were most relevant and allowed for a comprehensive assessment of PSE, whilst avoiding duplication. The resulting items were reviewed for comprehensiveness, relevance, clarity, and simplicity by practising clinicians and staff with expertise in research and writing for consumers. The resulting ten items were then presented to consumers through informal interviews and existing consumer committees. Based on the consolidated feedback, minor refinements were made to improve acceptability of the items and to further simplify the wording.
Phase Two – Survey Development
Items were then used to develop an online survey within REDCap35,36 which was reviewed by a diverse range of consumers through three structured focus groups. Caregivers were either currently or had previously been involved with CDS services. The wording of items was refined through an iterative process over the course of these three groups.
A retrospective pretest-posttest design, administered at the point of discharge, was selected to reduce potential response shift bias.37,38 For each item, an 11-point bi-polar Likert-type response scale was used (0 – strongly disagree to 10 – strongly agree), with higher scores indicating higher levels of perceived self-efficacy. The scale requires caregivers to rate their current self-efficacy beliefs (“now” score) and reflect on how they were feeling before attending intervention (“before” score). See example item depicted in Figure 1.
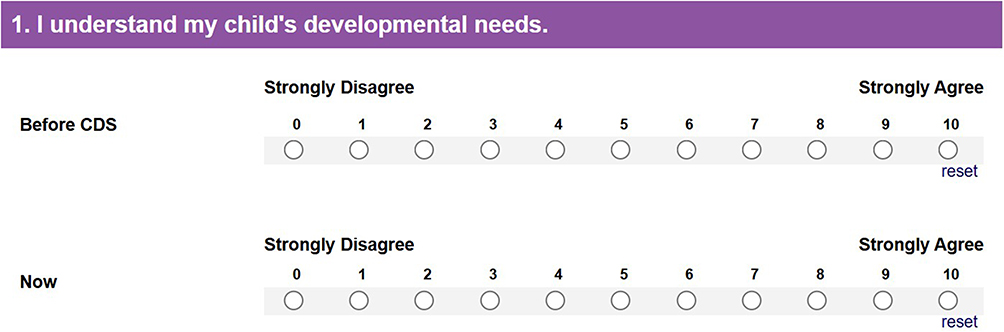 |
Figure 1 Example item from the SET and GO indicating response scale. |
For validation purposes a total score for both “before” intervention and “now”, as well as a change score (the difference in these scores), were calculated.
Validation Study
Recruitment
Participants were recruited from three CDS sites spread across the Perth metropolitan area. Sites were selected to increase the socio-economic and cultural and linguistic diversity of the sample. Caregivers were invited to participate by their discharging clinician if they were aged 18 years or older and were the primary caregiver involved in their child’s intervention. Participating clinicians were encouraged to invite every eligible caregiver to reduce sample bias. A pre-determined quota for each discipline was developed to guide the recruitment of participants. This ensured that the services received by the caregivers in the sample were broadly representative of the services provided by CDS. Recruiting clinicians were encouraged to continue recruitment until the quota for their discipline was reached. A minimum of 200 participants were required.33,34
Participation in the study was explained to caregivers by the discharging clinician, and an information sheet was provided. Caregivers were informed that participation was voluntary, that declining to participate would not impact any future care provided to their child, and that their participation and responses would be kept confidential. Participants were not compensated for taking part in this research. This research was reviewed and approved by the Human Research Ethics Committee at the Child and Adolescent Health Service (RGS0000004716) and by the Western Australian Aboriginal Health Ethics Committee (HREC1132).
Data Collection
All data was collected via electronic questionnaires using the REDCap data management tool.35,36 Prompts to respond to all questions were included in the SET and GO, comparison measures and key demographic details to ensure that there was no missing data. The discharging clinician completed several questions in relation to the service provided to the child and family, as well as specific information about the child’s clinical presentation. These questions included discipline of discharge, neurodevelopmental diagnosis (if applicable), and intervention length (brief intervention included assessment with advice about supporting development, while extended intervention included assessment, therapy and review sessions). The number of clinical disciplines involved in the child’s care was also recorded and used as a proxy measure of the child’s developmental complexity. Categories included: (a) low complexity, single discipline; (b) moderate complexity, multiple disciplines (excluding paediatrician); (c) high complexity, multiple disciplines (including paediatrician).
Participants completed a demographic questionnaire, the SET and GO, and four other validated tools within four days of discharge. The demographic questionnaire included questions relating to both the caregiver (relationship to child, age, highest level of education obtained, number of dependent children, postal area code, identification as Aboriginal and/or Torres Strait Islander and main language spoken at home) and the child who was being discharged (child age and gender). Not all responses to the demographic questions were mandatory. Additional validated tools included the 6-item Learning and Development subscale of the Tool to measure Parenting Self Efficacy (TOPSE),21 the 8-item Family-Centered Practices Scale short form (FCPS),39 the 12-item Multidimensional Scale of Perceived Social Support (MSPSS),40 and the 10-item Perceived Stress Scale (PSS).41 These tools were used to evaluate the convergent validity of the SET and GO. Participants were then invited to complete the SET and GO for a second time two-weeks following discharge for test–retest reliability purposes.
Index of Relative Socio-Economic Advantage and Disadvantage (IRSAD) scores were calculated for each participant based on their postal area code and the Australia Bureau of Statistics data cubes.42 This index considers the economic (income and employment) and social (education, occupation, housing, rate of disability, family structure) environments of households within the area.
Statistical Analysis
The COSMIN study design checklist for patient-reported outcome measurement instruments34 and the COSMIN taxonomy,43 as well as work by Terwee et al44 and Carpenter,45 were used to guide the analysis and reporting of psychometric properties. All data were analysed using Stata 16.1.46 Statistical significance was considered p < 0.05.
Validity
Structural Validity
Exploratory factor analysis (EFA) was performed to test the dimensionality of the SET and GO and to inform item reduction.45 The “before” item scores were used for EFA as it was anticipated that due to the impact of intervention, ceiling effects may be evident in the “now” scores. Principal axis factoring was used for extraction with a Pearson correlation matrix. Data suitability was evaluated using Kaiser–Meyer–Olkin (KMO) measure (preferred value >0.6) and Barlett’s test (p < 0.05 indicating significant correlations and factor analysis is appropriate). Eigen values and loadings were reviewed for all factors identified. As the pilot SET and GO were a 10-item tool the maximum number of factors was determined to be 3 (minimum of 3 items per factor). The final number of factors was determined by the scree test, parallel analysis, eigenvalue >1, and examining proportion of variance explained per factor. For scale item selection, we required communalities >0.4 (uniqueness<=0.6), significant loadings (>0.4) and Velicer’s MAP criteria, as well as interpretability. Inter-item correlations were analysed and any items with a correlation of higher than 0.75 were considered for exclusion to reduce item redundancy.
Construct Validity – Convergent, Known Groups and Correlation
Hypothesis testing was performed for construct validity. Convergent validity (comparison with other outcome measures) was performed using the TOPSE, FCPS, MSPSS and PSS tools. Relationships between the “now” total score of the SET and GO and these measures were examined using scatter plots, followed by the Spearman’s correlation coefficient. The “now” score was used in this instance as it represented the caregiver’s current perceived self-efficacy and was completed at the same time as the comparison measures. The results were interpreted as follows: negligible 0.0 to 0.10, weak 0.10 to 0.39, moderate 0.40 to 0.69, strong 0.7 to 0.89, very strong 0.9 to 1.0.47
To further establish the construct validity of the tool, relationships between “before” total scores on the SET and GO and the categorical measures of child’s developmental complexity, intervention length (brief intervention versus extended intervention), and caregiver level of education were examined using a Mann Whitney U or Kruskal Wallace test. Associations between “before” total scores on the SET and GO and the continuous measures IRSAD,42 number of dependent children, and caregiver age were then examined using Spearman’s correlation.
Reliability
Internal Consistency
Internal consistency was examined using Cronbach’s alpha, with a desirable cut-off of at least 0.7.33
Test-Retest Reliability
Test–retest reliability was determined using a quadratic weighted kappa due to the ordinal and skewed nature of the data. Interpretations are as follows: 0.0 to <0.2 slight, 0.2 to <0.4 fair, 0.40 to <0.6 moderate, 0.6 to <0.8 substantial, 0.8 to 1.0 almost perfect agreement.48
Interpretability
Floor and Ceiling Effects
Floor and ceiling effects were determined by analysing the spread of scores on an item-by-item basis. A ceiling or floor effect was deemed evident if ≥15% of responses for an individual item were at either extreme of the response scale.44 Ceiling effects were anticipated for “now” scale scores due to the impact of intervention.
Reported Change
Perceived change was analysed by comparing SET and GO total scores “before” and “now”, using the Wilcoxon signed rank test.
Minimal Clinically Important Difference (MCID) Value
To determine meaningful change, an anchor-based method was used as primary evidence for the MCID value followed by distribution-based methods.49,50 Anchor-based methods used a within-patient total score change. Respondents were asked whether the difference between the “before” and “now” ratings was meaningful to them using the anchor question “since coming to CDS my capacity to support my child’s development has improved/stayed the same/got worse”. This served as the anchor, with the mean change score calculated for respondents who said that their capacity to support their child had “improved”. A distribution-based approach was used as secondary evidence for the MCID value using a change value of >1 standard error of measurement (SEM).
Results
Participant Characteristics
A total of 243 eligible families were invited to participate in this study throughout the recruitment period. A sample of 204 caregivers (84% of those invited) consented to participate and completed all questionnaires in the validation study. A total of 136 of these participants also completed the SET and GO at time point 2 for test–retest reliability purposes. The only group difference noted in caregivers who completed the tool at both time points was level of education, with caregivers who had a higher level of education more likely to complete the survey at time point 2.
The sample included caregivers, aged from 23 to 64 years (mean age 37 years), who had accessed intervention for a range of concerns about their child’s development. Clinical presentations included delays in fine and gross motor skills, communication and social-emotional difficulties and neurodevelopmental conditions – ADHD (n=32), developmental language disorder (n=16) and ASD (n=15). The characteristics of the study sample are summarised in Table 1.
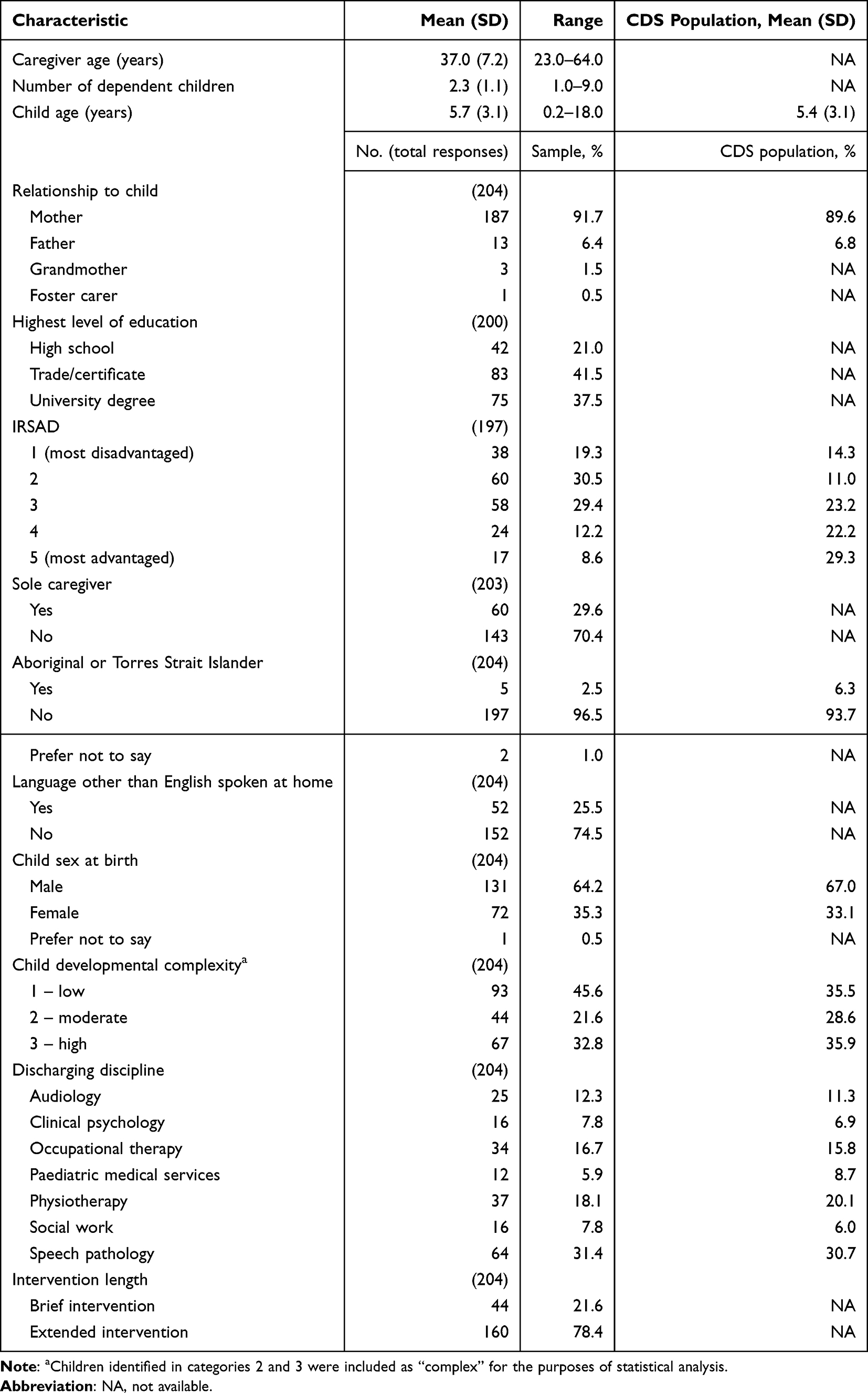 |
Table 1 Demographic and Intervention Characteristics of the Validation Sample with Comparison to CDS Population |
The sample was compared to CDS population data on routinely collected caregiver and child characteristics (Table 1). The sample was similar to the CDS population on the variables of caregiver’s relationship to child, child age, child sex at birth, and the discharging discipline. The study sample included more families with greater socio-economic disadvantage, fewer Aboriginal caregivers, and lower child developmental complexity.
Validity
Structural Validity - Excluded Items
Inter-item correlations of above 0.75 were reviewed for all items by both a biostatistician and the clinical working group. This resulted in the removal of the item “I can support my child’s development” as it was determined that there was redundancy with the item “I have the skills to support my child’s development”. Further statistical analysis was then based on the remaining nine items.
Structural Validity - Assessing the Factor Structure of the SET and GO
Suitability of the data for EFA was confirmed with a KMO of 0.934 and Bartletts test of p < 0.001. The EFA for the nine-item scale indicated a single factor with an eigenvalue of 5.8 accounting for 66% of the total variance. The scree plot supported a single-factor solution. The factor loading on all items was examined and ranged from 0.71 to 0.88. All items demonstrated a uniqueness of <0.5 indicating good fit with a single-factor solution.
Construct Validity
Convergent validity was assessed by comparing the results on the SET and GO across four validated measures (Table 2). A moderate positive relationship was shown with the SET and GO and the TOPSE, and the SET and GO and MSPSS. Weak correlations were found between scores on the SET and GO and FCPS and PSS.
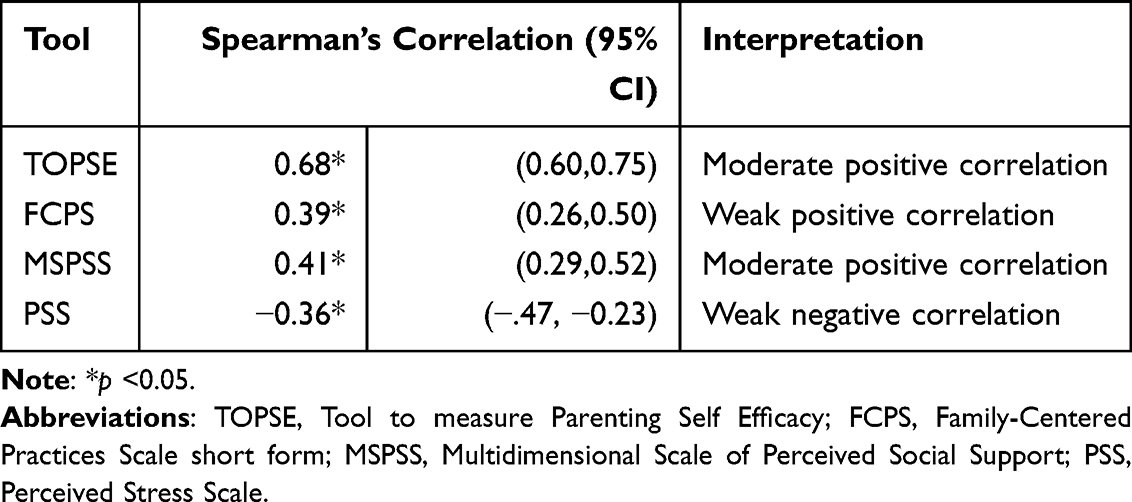 |
Table 2 Spearman’s Correlation Coefficients Between SET and GO Total “Now” Score and Validated Measures of Caregiver Self-Efficacy, Family Centred Practices, Social Support, and Stress |
The relationship between the SET and GO and other caregiver and child factors was explored for known groups validity. Group differences based on child developmental complexity were found for the SET and GO total “before” score, with caregivers of children with increased developmental complexity reporting lower PSE (SET and GO “before” median (IQR) score: not complex 63 (52, 75) vs complex 56 (40, 69), p=0.007). Group differences were also found based on length of intervention, with caregivers who participated in an extended intervention with their child more likely to report lower pre-service levels of PSE (SET and GO “before” median (IQR) score: brief intervention 71.5 (61.5, 83) vs extended intervention 58 (46, 69.5), p<0.001).
Negligible correlations were found between the SET and GO and IRSAD, number of dependent children, and caregiver age. No statistically significant group differences in SET and GO scores were found for level of caregiver education (p=0.910).
Reliability
Internal Consistency
The SET and GO demonstrated excellent internal consistency with a Cronbach’s alpha of 0.94 for the “before” score and 0.93 for the “now” scale score.
Test-Retest Reliability
Test–retest reliability results for each item ranged from moderate to substantial. The weighted kappa for the total “before” score was 0.80 (95% CI 0.74 to 0.87) and for the “now” score was 0.76 (95% CI 0.68 to 0.85). These results indicate stability of the SET and GO across a short period of time and provide evidence for adequate test–retest reliability.
Interpretability
Floor and Ceiling Effects
Floor effects were not evident for either “before” or “now” item or total scale scores. Ceiling effects were evident across some individual items in the “before” scale scores, however, were not present for the total scale score with only 8.3% of participants providing the highest rating for the entire scale before attending CDS. As anticipated, ceiling effects were evident for the “now” scale score with 45% of participants providing the maximum scale score at point of discharge from the service.
Reported Change
As the SET and GO ratings were collected using a retrospective pretest–posttest design at discharge, reported differences represent caregivers’ perceived change in PSE over the course of intervention, rather than prospectively observed change. Results indicated that there was a significant difference between caregivers’ “before” and “now” ratings for both the brief and extended intervention groups. The median perceived change score for the brief intervention group was 14.5 (median (IQR) scores: “before” 71.5 (61.5, 83.0) vs “now” 86.0 (77.5, 90.0), p<0.001). The median perceived change score for the extended intervention group was 26.0 (median (IQR) scores: “before” 58.0 (46.0, 69.5) vs “now” 84.0 (78.0, 88.5), p<0.001).
Minimal Clinically Important Difference (MCID)
It was not possible to use an anchor-based method to determine the MCID value as insufficient participants indicated that their capacity to support their child’s development had “got worse” or “stayed the same” (n=16/204). The distribution method was therefore used to calculate a preliminary MCID value. Using internal consistency as a measure of the scale’s reliability, the calculated MCID value was 6.9, indicating that a change score of ≥7 was required to suggest a change in self-efficacy that was beyond the measurement error. Based on this MCID value, 164/204 (80.4%) participants reported a clinically meaningful difference in PSE. As this estimate is derived solely from a distribution-based method, it should be interpreted cautiously and requires confirmation in future studies using an anchor-based approach.
Discussion
Clinical and Service Implications
The SET and GO is a valid and reliable 9-item tool that provides services delivering developmental interventions with an efficient method for assessing perceived change in PSE as part of routine outcome measurement. This brief outcome tool is uniquely placed as it is suitable for a wide range of caregivers participating in developmental interventions with their child and has applicability within multidisciplinary child development services both nationally and internationally. Use of the tool will support research into the effectiveness of clinical interventions and inform service improvement activities. Specifically, measuring changes in perceived PSE will enable services to better understand how intervention characteristics, such as length and format of intervention (individual versus group, facilitated versus self-directed), influence caregiver self-efficacy.
Psychometric Properties of the SET and GO
EFA demonstrated that the SET and GO is a unidimensional tool, and hypothesis testing for construct validity (convergent and known-groups) further indicated that it is a domain-specific measure of PSE associated with supporting a child with a developmental concern. Significant differences in perceived PSE were noted for both the brief and extended intervention groups, demonstrating the applicability of the scale for use with caregivers accessing a range of intervention services.
Consistent with previous research, the SET and GO was positively correlated with perceived level of social support15 and the family-centred help-giving practices of the clinician providing intervention.11 Additionally, a negative correlation between stress and PSE was found, which reflects findings from previous studies.13,14 Whilst these relationships were significant, the strength of these relationships may have been impacted by the ceiling effect noted on the “now” score of the SET and GO, limiting the range and variability of the available data.
Factors Associated With PSE
While PSE has been the subject of significant research over the past thirty years, there is still conflicting evidence in relation to the association between PSE and socio-economic status, parental education and number of children in a family.15,16 Research into the relationship between PSE and child developmental complexity is largely uni-directional with most studies focussing on the impact of PSE on a child’s development6 or measuring parental stress rather than self-efficacy.51,52 The current study found caregivers of children with more complex developmental needs reported significantly lower levels of self-efficacy prior to receiving services. This finding was in line with research by Greenlee et al,51 who found that child symptom severity was related to distress in parents of children with autism. Similar findings were reported by Bonifacci et al52 with parents of children with specific learning disorders being more likely to have higher levels of distress than parents of typically developing children.
Results indicated that caregivers reported statistically and clinically meaningful increases in self-efficacy following intervention, irrespective of intervention duration. This finding suggests that even a brief intervention, typically including a developmental assessment and strategies to support future development, provides the caregiver with meaningful support to address their child’s unique developmental needs. This finding is in line with evidence from Bates,8 who reported that a diagnostic assessment can result in positive changes to PSE.
Results from the current study indicated no association between IRSAD and PSE. This contrasts with findings by Glatz et al,53 who reported that socioeconomic status predicted PSE among parents of school-aged children and adolescents. However, Fang et al16 identified evidence for a relationship between family income and PSE, while noting inconsistent findings regarding the broader association between socioeconomic status and PSE. These discrepancies may reflect variation in how socioeconomic status is defined and measured across studies.
The current study found no significant group differences in PSE based on caregiver level of education or number of dependent children. These results add to the body of evidence presented by Fang et al16 which found inconsistent evidence for the relationship between PSE and these factors.
Limitations
Recruitment to the study relied on clinicians inviting all eligible families to participate. Perception that the study may cause significant burden to some caregivers, or a reluctance to invite families who expressed a negative experience with the service, may have resulted in recruitment bias. However, based on comparison to the CDS population, participants were similar across a number of variables including the caregiver’s relationship to child, child age, child sex at birth, and the discharging discipline. In addition, the sample displayed greater variability in socioeconomic disadvantage than the broader CDS population. This increased variation enabled examination of potential associations between PSE and socioeconomic status, particularly in light of the inconsistent findings reported in the literature.16,53
An additional limitation was the limited representation of Aboriginal and Torres Strait Islander caregivers within the sample. While approximately 6% of children currently receiving services from CDS are Aboriginal, only 2% of the caregivers in the study identified as Aboriginal or Torres Strait Islander. This limits the generalisability of the results to Aboriginal caregivers and is an area for further investigation.
A further limitation was participant attrition, with only 136 of the 204 participants completing the SET and GO at time point two for test–retest reliability purposes. As there was a group difference in terms of educational attainment for the caregivers who completed the measure at time point 2, this may have introduced selection bias, potentially influencing the test–retest reliability estimates.
Ceiling effects were observed, with a substantial proportion of respondents achieving the maximum total score at the “now” time point. These effects were anticipated, as reduced sensitivity at higher score ranges is commonly reported in domain-specific PSE measures.17 Nonetheless, this result may indicate limited sensitivity of the measure to detect differences among caregivers reporting higher levels of PSE, potentially restricting discrimination at the upper end of the scale and inflating reliability estimates. In addition, these ceiling effects may have attenuated correlations with related measures, thereby influencing the magnitude of observed convergent validity.
Finally, while a preliminary MCID value of ≥7 has been determined using distribution-based methods, this needs to be interpreted with caution. Research with a larger sample that enables calculation of an MCID value using an anchor-based method will support the development of a more clinically robust value.49,50
Future Directions
Future research will involve pilot implementation of the SET and GO within CDS, enabling collection of data on a larger sample. This will allow for investigation of the validity of the tool with a more diverse sample, including Aboriginal caregivers, fathers and grandparents. A larger sample will also allow analysis of caregiver responses on a discipline-specific basis and enable the refinement of an MCID value using an anchor-based method.
While the SET and GO was purposefully developed for use as a retrospective pretest–posttest scale, future research could examine its responsiveness to change using prospective longitudinal designs. Administering the measure before and after a discrete intervention (such as an 8-week group program) and across longer follow-up periods would enable evaluation of the scale’s sensitivity when used in a prospective manner. Such research would provide further evidence regarding the utility of the SET and GO as an outcome measurement tool.
There are few studies available on the relationship between child developmental complexity and PSE, with studies specific to developmental diagnosis measuring adjacent constructs such as parental stress or parenting conflict52 or looking at PSE as a mediating factor to parental wellbeing.54 While the results presented in this study indicate an inverse relationship between PSE and child developmental complexity (ie. PSE is lower for caregivers of children who are more developmentally complex), a larger sample could provide further details on this relationship, such as whether this relationship is related to particular diagnoses or developmental concerns.
Conclusion
The current study provides evidence that the SET and GO is a valid and reliable nine-item domain-specific PSE tool, suitable for use with caregivers who have a child (aged 0 to 18 years) accessing intervention for any of a range of developmental concerns. Results also add to the existing body of knowledge about the relationship between PSE and service, socio-economic, parent and child factors. The proposed minimal clinically important difference (MCID) value should be considered preliminary, and the presence of ceiling effects, along with the limited representation of Aboriginal caregivers in the sample, may constrain the generalisability of the findings. Future piloting of the SET and GO will allow investigation of the validity of the tool for Aboriginal caregivers, refinement of the MCID estimate, and further exploration into the relationship between PSE and child developmental complexity. Overall, the findings from this study support the potential utility of the SET and GO in child development settings to measure caregiver outcomes, inform intervention planning, and guide service delivery decisions.
Availability of the SET and GO
Access to the SET and GO: A parenting Self-Efficacy Tool for Gathering Outcomes of developmental interventions is free and available from https://redcap.link/CDS-SET-and-GO.
Data Sharing Statement
The data that supports the findings of this study is available from the authors upon reasonable request and with the permission of Child and Adolescent Health Service. Only aggregated data will be provided in order to protect the privacy of all participants.
Ethics Approval and Consent to Participate
This research was conducted in accordance with the principles of the Declaration of Helsinki. The protocol was reviewed and approved by the Human Research Ethics Committee at the Child and Adolescent Health Service (RGS0000004716) and by the Western Australian Aboriginal Health Ethics Committee (HREC1132) and informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the significant contribution of both staff and families of the Child Development Service, Child and Adolescent Health Service in the development and validation of the SET and GO.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research project was fully funded by the Government of Western Australia – Child and Adolescent Health Service.
Disclosure
Ms Natasha Bear reports personal fees from Natasha Bear Statistics, during the conduct of the study. The authors have no other conflicts of interest to declare that are relevant to the content of this article.
References
1. Hughes-Scholes CH, Gavidia-Payne S. Early childhood intervention program quality: examining family-centered practice, parental self-efficacy and child and family outcomes. Early Child Educ J. 2019;47(6):719–13. doi:10.1007/s10643-019-00961-5
2. Duncan EA, Murray J. The barriers and facilitators to routine outcome measurement by allied health professionals in practice: a systematic review. BMC Health Serv Res. 2012;12:96. doi:10.1186/1472-6963-12-96
3. Imms C, Moore T, Bull K, et al. Review of best practice in early childhood intervention: desktop review full report; 2024. Available from: https://healthy-trajectories.com.au/wp-content/uploads/2024/11/ECI-TAP-Deliverable-1-Desktop-Review-Full-Report-V1.0_Nov2024.pdf.
4. Moore T, Imms C, Luscombe D, et al. National best practice framework for early childhood intervention; 2025. Available from: https://www.health.gov.au/resources/collections/national-best-practice-framework-for-early-childhood-intervention?language=en#the-framework.
5. Dunst CJ, Trivette CM. Capacity-building family-systems intervention practices. J Fam Soc Work. 2009;12(2):119–143. doi:10.1080/10522150802713322
6. Albanese AM, Russo GR, Geller PA. The role of parental self-efficacy in parent and child well-being: a systematic review of associated outcomes. Child Care Health Dev. 2019;45(3):333–363. doi:10.1111/cch.12661
7. Bailey DB, McWilliam RA, Hebbeler K, Simeonsson RJ, Spiker D, Wagner M. Family outcomes in early intervention: a framework for program evaluation and efficacy research. Except Child. 1998;64(3):313–328. doi:10.1177/001440299806400302
8. Bates G. What impact does the child development assessment process have on parental self-efficacy? Adv Ment Health. 2019;18(1):27–38. doi:10.1080/18387357.2019.1633936
9. Bandura A, Adams N. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
10. Jones TL, Prinz RJ. Potential roles of parental self-efficacy in parent and child adjustment: a review. Clin Psychol Rev. 2005;25(3):341–363. doi:10.1016/j.cpr.2004.12.004
11. Trivette CM, Dunst CJ, Hamby DW. Influences of family-systems intervention practices on parent-child interactions and child development. Topics Early Child Spec Educ. 2010;30(1):3–19. doi:10.1177/0271121410364250
12. Angley M, Divney A, Magriples U, Kershaw T. Social support, family functioning and parenting competence in adolescent parents. Matern Child Health J. 2015;19(1):67–73. doi:10.1007/s10995-014-1496-x
13. Osborne LA, McHugh L, Saunders J, Reed P. Parenting stress reduces the effectiveness of early teaching interventions for autistic spectrum disorders. J Autism Dev Disord. 2008;38(6):1092–1103. doi:10.1007/s10803-007-0497-7
14. Kendall S, Bloomfield L, Appleton J, Kitaoka K. Efficacy of a group-based parenting program on stress and self-efficacy among Japanese mothers: a quasi-experimental study. Nurs Health Sci. 2013;15(4):454–460. doi:10.1111/nhs.12054
15. Sevigny PR, Loutzenhiser L. Predictors of parenting self-efficacy in mothers and fathers of toddlers. Child Care Health Dev. 2010;36(2):179–189. doi:10.1111/j.1365-2214.2009.00980.x
16. Fang Y, Boelens M, Windhorst DA, Raat H, van Grieken A. Factors associated with parenting self-efficacy: a systematic review. J Adv Nurs. 2021;77(6):2641–2661. doi:10.1111/jan.14767
17. Crncec R, Barnett B, Matthey S. Review of scales of parenting confidence. J Nurs Meas. 2010;18(3):210–240. doi:10.1891/1061-3749.18.3.210
18. Wittkowski A, Garrett C, Calam R, Weisberg D. Self-report measures of parental self-efficacy: a systematic review of the current literature. J Child Fam Stud. 2017;26(11):2960–2978. doi:10.1007/s10826-017-0830-5
19. Seetharaman M, Benjamin A, McGrath JM, Vance AJ. Parenting self-efficacy instruments for parents of infants and toddlers: a review. Int J Nurs Stud Adv. 2022;4:100082. doi:10.1016/j.ijnsa.2022.100082
20. Kabashima Y, Tadaka E, Arimoto A. Development of the parental self-efficacy scale for preventing challenging behaviors in children with autism spectrum disorder. PLoS One. 2020;15(9):e0238652. doi:10.1371/journal.pone.0238652
21. Kendall S, Bloomfield L. Developing and validating a tool to measure parenting self-efficacy. J Adv Nurs. 2005;51(2):174–181. doi:10.1111/j.1365-2648.2005.03479.x
22. Gibaud-Wallston J, Wandersmann LP. Development and Utility of the Parenting Sense of Competence Scale. Toronto, ON: The American Psychological Association; 1978.
23. Suzuki S, Holloway SD, Yamamoto Y, Mindnich JD. Parenting self-efficacy and social support in Japan and the United States. J Fam Issues. 2009;30(11):1505–1526. doi:10.1177/0192513X09336830
24. Freiberg K, Homel R, Branch S. The Parent Empowerment and Efficacy Measure (PEEM): a tool for strengthening the accountability and effectiveness of family support services. Aust Soc Work. 2014;67(3):405–418. doi:10.1080/0312407X.2014.902980
25. Hamilton VE, Matthews JM, Crawford SB. Development and preliminary validation of a parenting self regulation scale: “Me as a parent. J Child Fam Stud. 2014;24(10):1–12. doi:10.1007/s10826-014-0089-z
26. Purssell E, While A. Development of a scale to measure parental self-efficacy in the care of pre-school children during periods of health and minor illness: integrating health and social policy methods. J Clin Nurs. 2011;20(11–12):1623–1631. doi:10.1111/j.1365-2702.2010.03591.x
27. Teti DM, Gelfand DM. Behavioral competence among mothers of infants in the first year: the mediational role of maternal self-efficacy. Child Dev. 1991;62(5):918–929. doi:10.1111/j.1467-8624.1991.tb01580.x
28. Emser TS, Mazzucchelli TG, Christiansen H, Sanders MR. Child Adjustment and Parent Efficacy Scale-Developmental Disability (CAPES-DD): first psychometric evaluation of a new child and parenting assessment tool for children with a developmental disability. Res Dev Disabil. 2016;53–54:158–177. doi:10.1016/j.ridd.2015.09.006
29. Sofronoff K, Farbotko M. The effectiveness of parent management training to increase self-efficacy in parents of children with Asperger syndrome. Autism. 2002;6(3):271–286. doi:10.1177/1362361302006003005
30. Woolgar M, Humayun S, Scott S, Dadds MR. I know what to do; I can do it; It will work: the Brief Parental Self Efficacy Scale (BPSES) for parenting interventions. Child Psychiatry Hum Dev. 2025;56(3):619–628. doi:10.1007/s10578-023-01583-0
31. Guimond AB, Wilcox MJ, Lamorey SG. The Early Intervention Parenting Self-Efficacy Scale (EIPSES). Empirical Study; Quantitative Study. J Early Interv. 2008;30(4):295–320. doi:10.1177/1053815108320814
32. Bailey DB, Raspa M, Olmsted MG, et al. Development and psychometric validation of the Family Outcomes Survey–Revised. J Early Interv. 2011;33(1):6–23. doi:10.1177/1053815111399441
33. Boateng GO, Neilands TB, Frongillo EA, Melgar-Quinonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health. 2018;6:149. doi:10.3389/fpubh.2018.00149
34. Mokkink LB, Prisen CA, Patrick DL, et al. COSMIN Study Design checklist for Patient-reported outcome measurement instruments; 2019. Available from: https://www.cosmin.nl/wp-content/uploads/COSMIN-study-designing-checklist_final.pdf.
35. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
36. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
37. Howard GS. Response-shift bias: a problem in evaluating interventions with pre/post self-reports. Eval Rev. 1980;4(1):93–106. doi:10.1177/0193841x8000400105
38. Chang R, Little TD. Innovations for evaluation research: multiform protocols, visual analog scaling, and the retrospective pretest–posttest design. Eval Health Prof. 2018;41(2):246–269. doi:10.1177/0163278718759396
39. Dunst CJ, Trivette CM. Family-Centered Practices Scale: Short Form. Orelena Hawks Puckett Institute; 2002.
40. Zimet GD, Powell SS, Farley GK, Werkman S, Berkoff KA. Psychometric characteristics of the multidimensional scale of perceived social support. J Pers Assess. 1990;55(3–4):610–617. doi:10.1080/00223891.1990.9674095
41. Kamarck T, Mermelstein R, Cohen S. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
42. Australian Bureau of Statistics. Data From: Socio-Economic Indexes for Areas (SEIFA). Australia; 2021.
43. Mokkink LB, Terwee CB, Patrick DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res. 2010;19(4):539–549. doi:10.1007/s11136-010-9606-8
44. Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. doi:10.1016/j.jclinepi.2006.03.012
45. Carpenter S. Ten steps in scale development and reporting: a guide for researchers. Commun Methods Meas. 2018;12(1):25–44. doi:10.1080/19312458.2017.1396583
46. Han X. Stata Statistical Software: Release 16.1. StataCorp LLC; 2019.
47. Schober P, Boer C, Schwarte LA. Correlation coefficients: appropriate use and interpretation. Anesth Analg. 2018;126(5):1763–1768. doi:10.1213/ANE.0000000000002864
48. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174.
49. Copay AG, Subach BR, Glassman SD, Polly DW, Schuler TC. Understanding the minimum clinically important difference: a review of concepts and methods. Spine J. 2007;7(5):541–546. doi:10.1016/j.spinee.2007.01.008
50. Revicki D, Hays RD, Cella D, Sloan J. Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J Clin Epidemiol. 2008;61(2):102–109. doi:10.1016/j.jclinepi.2007.03.012
51. Greenlee JL, Hickey E, Stelter CR, Huynh T, Hartley SL. Profiles of the parenting experience in families of autistic children. Autism. 2023;27(7):1919–1932. doi:10.1177/13623613221147399
52. Bonifacci P, Storti M, Tobia V, Suardi A. Specific learning disorders: a look inside children’s and parents’ psychological well-being and relationships. J Learn Disabil. 2016;49(5):532–545. doi:10.1177/0022219414566681
53. Glatz T, Lippold M, Chung G, Jensen TM. A systematic review of parental self-efficacy among parents of school-age children and adolescents. Adolesc Res Rev. 2024;9(1):75–91. doi:10.1007/s40894-023-00216-w
54. Molero F, Recio P, Sarriá E. Affiliate stigma and marital satisfaction in Spanish parents of children with intellectual disabilities. Stigma Health. 2024;9(2):181–190. doi:10.1037/sah0000478
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.