Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Measuring and monitoring skeletal muscle function in COPD: current perspectives
Authors Marklund S ![]() , Bui KL
, Bui KL ![]() , Nyberg A
, Nyberg A ![]()
Received 14 February 2019
Accepted for publication 25 June 2019
Published 19 August 2019 Volume 2019:14 Pages 1825—1838
DOI https://doi.org/10.2147/COPD.S178948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Sarah Marklund,1 Kim-Ly Bui,2 Andre Nyberg1
1Department of Community Medicine and Rehabilitation, Section of Physiotherapy, Umeå University, Umeå, Sweden; 2Rehabilitation Department, Faculty of Medicine Laval University and Centre de recherche, Laval University Quebec Heart and Lung Institute (CRIUCPQ), Québec, QC, Canada
Correspondence: Andre Nyberg
Department of Community Medicine and Rehabilitation, Section of Physiotherapy, Caring Science Building, Lasarettsbacken 7, Umeå University, Umeå 907 46, Sweden
Tel +46 090 786 6639
Fax +46 90 786 9267
Email [email protected]
Abstract: Skeletal muscle dysfunction is an important systemic consequence of chronic obstructive pulmonary disease (COPD) that worsens the natural cause of the disease. Up to a third of all people with COPD express some form of impairment which encompasses reductions in strength and endurance, as well as an increased fatigability. Considering this complexity, no single test could be used to measure and monitor all aspects of the impaired skeletal muscle function within the COPD population, resulting in a wide range of available tests and measurement techniques. The aim of the current review is to highlight current and new perspectives relevant to skeletal muscle function measurements within the COPD population in order to provide guidance for researchers as well as for clinicians. First of all, standardized and clinically feasible measurement protocols, as well as normative values and predictive equations across the spectrum of impaired function in COPD, are needed before assessment of skeletal muscle function can become a reality in clinical praxis. This should minimally target the quadriceps muscle; however, depending on the objective of measurements, eg, to determine upper limb muscle function or walking capacity, other muscles could also be tested. Furthermore, even though muscle strength measurements are important, current evidence suggests that other aspects, such as the endurance and power capacity of the muscle, should also be considered. Moreover, although static (isometric) measurements have been favored, dynamic measurements of skeletal muscle function should not be neglected as they, in a larger extent than static measurements, are related to tasks of daily living. Lastly, the often modest relationships between functional tests and skeletal muscle function measurements indicate that they evaluate different constructs and thus cannot replace one another. Therefore, for accurate measurements of skeletal muscle function in people with COPD, specific and formal measurements should still be prioritized.
Keywords: chronic obstructive pulmonary disease, measurement properties, muscle strength, muscle endurance, muscle power
Introduction
In people with chronic obstructive pulmonary disease (COPD), skeletal muscle dysfunction is a common extrapulmonary manifestation.1 Although both respiratory and limb muscles are altered, the latter are usually more severely affected.2 Furthermore, respiratory muscle dysfunction is mainly seen in advanced disease,2 and even though the extent of impaired function of the limb muscles is greater in more advanced disease, it may also occur in earlier stages of the disease. Quadriceps muscle weakness’ prevalence rate, for example, approximates up to 20% even in people with mild COPD.3 Thus, due to space constraints, the focus of the current perspective will be on measuring and monitoring the function of the limb muscles, henceforth denoted as skeletal muscle function.
Several morphological and structural deviances within the muscle comprise the impaired skeletal muscle function in COPD, most of which have been reported in the quadriceps.1 Importantly, impaired skeletal muscle function is intimately linked to key clinical and prognostic outcomes such as health care utilization,4 exercise intolerance5,6 and even life expectancy.7 For example, isometric quadriceps strength is more closely related to mortality than age, body mass index and forced expiratory volume in 1 s.7 Thus, impaired skeletal muscle function is an important extrapulmonary manifestation in COPD, whose potential identification should be included in the routine assessment of these patients in the clinic.1,2
Various objectives could be pursued when measuring the function of skeletal muscles, including diagnostic purposes in order to characterize the nature of dysfunction, or as a mechanism for monitoring progress when measured before and during pulmonary rehabilitation. The latter would also facilitate the prescription of targeted training programs. Whatever the objective of measurement, choice of measurement strategy should always be specific to the clinical question it should answer, considering both advantages and limitations of available techniques, equipment and clinical realities.2,8
In this paper, we aim to provide a brief overview on the features and mechanisms of muscle dysfunction of the limb muscles in COPD and summarize what we currently know on the topic of measuring and monitoring skeletal muscle function in COPD. More specifically, we will highlight important aspects and properties related to measurement strategies used to monitor and measure skeletal muscle function in COPD. In addition, we also aim to highlight some new perspectives relevant to skeletal muscle function measurements among people with COPD in research as well as within the clinical realm.
Features and mechanisms of skeletal muscle dysfunction
Although the clinical significance of skeletal muscle dysfunction is well established in COPD, the underlying mechanisms of this problem are not fully understood. An overview of etiological factors, morphological and structural abnormalities, as well as impaired aspects of skeletal muscle function in COPD, is summarized in Figure 1. In short, the etiology of skeletal muscle dysfunction is likely multifactorial with possible contribution from cigarette smoke, genetic and epigenetic alterations, metabolic, drugs (corticosteroids), comorbidities, exacerbations, systemic inflammation, malnutrition as well as chronic physical inactivity.1,2 Since the latter leads to deconditioning, a process that initiates intramuscular and functional alterations, this is arguably one of the most important contributing factors to skeletal muscle dysfunction in COPD.9 However, the discovered range of skeletal muscle abnormalities seems to need a broader explanation than the level of physical activity alone. This since muscle impairment in COPD is vaguely related to the degree of activity.10,11 and as differences in skeletal muscle structure and function persevere between people with COPD and healthy controls even when controlling for physical activity.11
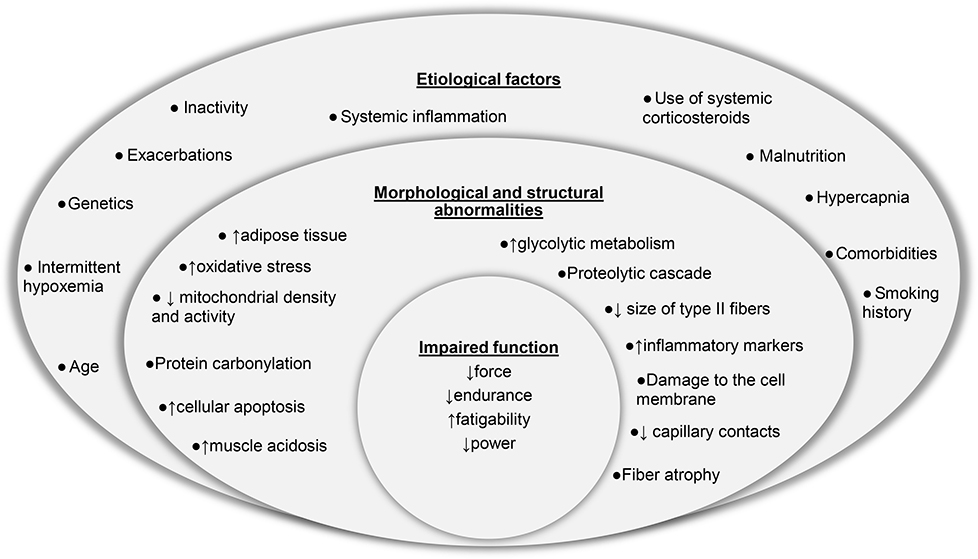 |
Figure 1 Overview of etiological factors, morphological and structural abnormalities and impaired skeletal muscle function in chronic obstructive pulmonary disease. |
Features of skeletal muscle dysfunction include atrophy, a shift in fiber-type distribution from type I to type IIx fibers, reduced oxidative capacity, mitochondrial function and capillarization,1 most of which have been reported in the quadriceps muscle,1 even in mild disease.12 The fiber-type shift is seen in about one-third of people with COPD, fiber atrophy in 20%.10 In a similar way, mid-thigh cross-sectional area has been reportedly reduced by 15–20% in people with moderate COPD.13 Furthermore, the shift in skeletal muscle fiber-type proportion opposes what is typically seen with aging,14 contributes to the muscles' susceptibility to fatigue15 and has been associated with premature mortality.16 Consistent with this shift, the reduced oxidative capacity and impaired mitochondrial function of the quadriceps muscle17 contribute to impaired performance during endurance-based activities.18 However, intrinsic muscle alterations alone cannot fully explain the decreased skeletal muscle function observed in people with COPD. In fact, aspects of skeletal muscle dysfunction such as increased susceptibility to muscle fatigue also seem to be related to the central nervous system. For example, mechanical and metabolic changes caused by exercise and activities have shown to stimulate metaboreceptive group III and IV muscle afferent fibers. These signals lead to the inhibition of the central motor drive, which thus prevent subsequent locomotor recruitment and the development of potentially dangerous and irreversible fatigue.19,20 At the functional level, these lead to decreased exercise capacity as well as increased limb muscle fatigue.21 Estimations of impaired skeletal muscle function in COPD vary according to disease severity and the criteria used to define dysfunction. Nevertheless, up to a third of all people with COPD expresses some form of impaired skeletal muscle function and encompasses reductions in strength, endurance, and power as well as an increased fatigability.1,22,23
Measuring and monitoring skeletal muscle function in COPD
The 2014 American Thoracic Society and European Respiratory Society statement on Limb Muscle Dysfunction in COPD recommends that assessment of isometric skeletal muscle function, at least quadriceps muscle function, should be an integrative part of the routine assessment of people with COPD.1 In addition, measurements of different aspects of skeletal muscle function (eg, strength or endurance) during exercise training would provide a mechanism for monitoring progress.24 However, several factors influence the choice of strategy when measuring and monitoring skeletal muscle function in people with COPD (Figure 2).
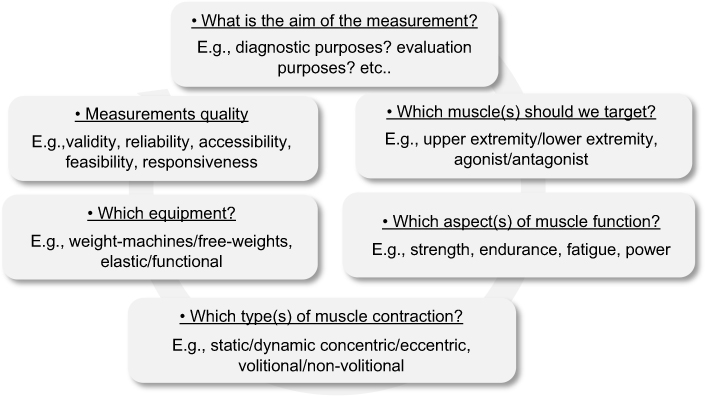 |
Figure 2 Factors that influence the choice of the measurement technique. |
First of all, all measurements of skeletal muscle function are muscle group–specific as well as heavily dependent on the type of contraction, velocity of movement and equipment used. In COPD, measurements of quadriceps muscle function should always be considered due to its clinical and prognostic value, but other lower and upper limb muscles may be evaluated to provide valuable information.1,8 Furthermore, the availability of measurement equipment will evidently impact on the selection of measurement technique; however, it is important to acknowledge that different measurement techniques are not interchangeable and may provide different information since they measure different aspects of skeletal muscle function. Thus, in a similar way to exercise training adaptations that are specific to the stimulus applied,25 the choice of skeletal muscle measurement strategy should also be specific to the clinical question it aims to answer.8,26 For example, during static testing (isometric), the tested limb is fixed and there is no change in muscle length throughout the contraction. This would suggest that this parameter may be less informative about the ability to perform functional activities as a part of daily living which often include dynamic components (except for isometric grip strength, more associated to carrying groceries in daily life for example). Thus, specific dynamic measurements in which information is provided on skeletal muscle function throughout the full range of motion might more accurately reflect functional activities.27,28 Dynamic contractions could be isotonic, that is when there is no noticeable change in the load applied to the muscle or isokinetic where the speed of the movement is constant.8 Even though isokinetic dynamometer measurements of skeletal muscle function often are considered the gold standards of skeletal muscle strength measurements, the availability of isokinetic dynamometers is limited, mostly because of the cost of equipment and need of trained personnel,8 reducing the clinical applicability. Furthermore, as skeletal muscle dysfunction is evident by a decrease in various aspects of skeletal muscle function (eg, reduced strength or endurance),1,8 this implies that no single test could be used to measure and monitor skeletal muscle function among people with COPD.8
All measurement techniques mentioned, so far, consist of voluntary contraction measurements. However, since skeletal muscle function may be affected by external factors such as motivation and cooperation of the patient,1 nonvolitional measurements of skeletal muscle function using electrical or magnetic twitch stimulation of peripheral nerves have been developed. The latter technique activates the neuromuscular system without stimulating skin nociceptors, resulting in less discomfort and pain.29 Such measurements can be performed in a rested muscle (unpotentiated twitch stimulation) or seconds after a maximum volitional contraction (potentiated twitch stimulation).1,30 Nonvolitional muscle function assessment can be especially relevant in investigating the mechanistic and functional aspects of muscle fatigue.31
Irrespective of which measurement techniques that are used, important aspects, including but not limited to the feasibility, validity, responsiveness, and reliability of the selected measurement technique, need to be considered when deciding on how to measure and monitor skeletal muscle function in people with COPD.26 For example, the selected measurement technique should be feasible in the intended clinical context, which could relate to the time needed to perform the test or the availability of the measurement equipment. Another example is related to the reliability of skeletal muscle function measurements, for which standardization plays a key role. For example, standardization of measurement instructions, positioning, rhythm and external visual/audio feedback are all important factors that could influence the degree to which the measurement is free from error.32,33 Readers are invited to refer to the following section for detailed information about these aspects in relation to what we currently know on skeletal muscle strength, endurance/fatigue and functional measurements in people with COPD. Lastly, standardization of preparation guidelines, including, but not limited to, use of medications or caffeine prior the assessment or avoidance of strenuous physical activities the day(s) before measurements, etc., should also be standardized. An overview of key aspects to consider with regard to standardization of measurement procedures is summarized in Table 1
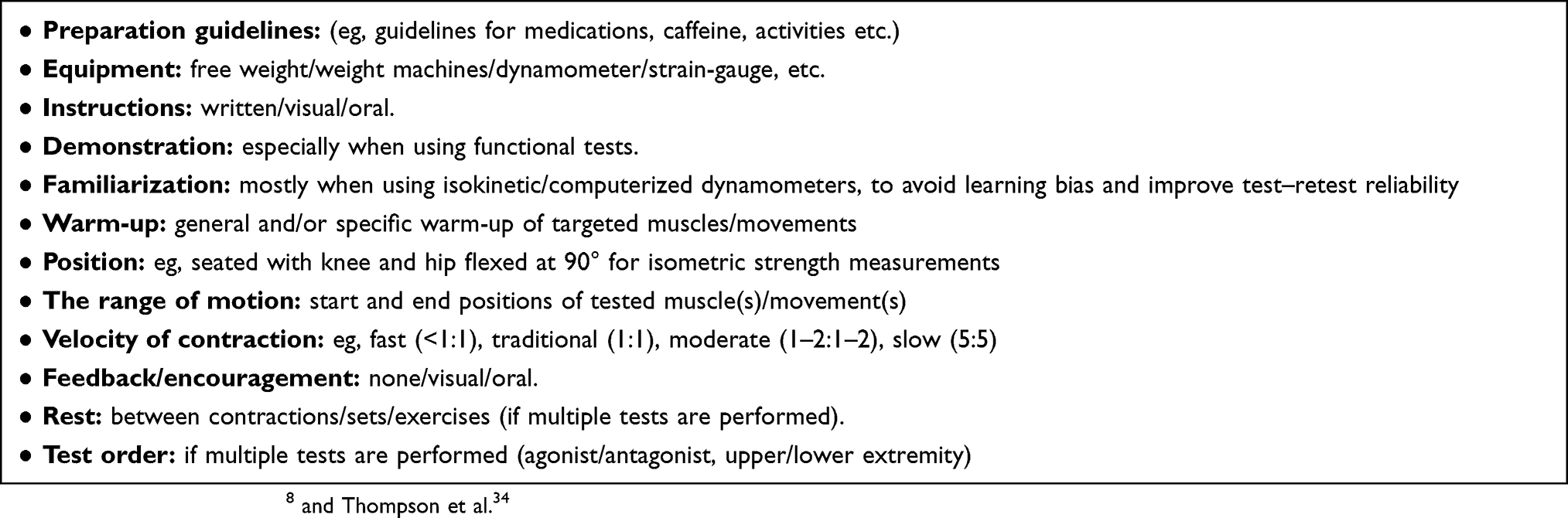 |
Table 1 Standardization of measurement procedure. |
What is currently known?
Skeletal muscle strength measurements
The most commonly measured aspect of skeletal muscle function in COPD is skeletal muscle strength, defined as the force-generating capacity of the muscle and often measured as the maximal voluntary contraction (MVC).35 Skeletal muscle strength measurements could be performed using numerous devices including strain gauge, handheld or fixed portable dynamometer, weight machines or manual muscle testing techniques as well as more complex systems such as computerized dynamometers.8,35 Even though skeletal muscle strength can also be assessed independently from the patient’s motivation and effort with electrical or magnetic stimulations of the muscle or its motor nerve,36,37 these techniques are almost solely used in the realm of clinical research. Thus, this section will focus on volitional measurements of quadriceps muscle strength that include static (isometric) as well as dynamic (isokinetic and isotonic) measurement techniques.
Isometric strength measurements
Isometric quadriceps strength measurements have been highly recommended in COPD1 since they provide important prognostic information.7 Recently, these measurements have also been shown to respond to interventions such as exercise training, with a suggested minimal important difference of 7.5 Nm.38 With regard to measurement properties, isometric quadriceps strength measurements have shown very high relative test–retest reliability, intraclass correlation coefficient (ICC) >0.9 and a minimal detectable change of 18–22% for strain-gauge as well as isokinetic dynamometer measurements, respectively.37,39 With regard to measurements of upper limbs, handgrip strength has been commonly assessed in COPD studies.35 However, the clinical purpose of isometric strength measurements is still uncertain in COPD since it does not appear to be associated with disease severity or to be decreased more than in the general older population.40
During isometric strength measurements, standardization of limb position, performing ≥3 MVC held for 4–5 s, spaced with 30–60-s rest periods, is important to obtain valid and reproducible results.8,35,37 When using portable dynamometers, fixation on rigid support is of utmost importance to avoid a possible underestimation of strength measurements and to provide reliable and valid results.41,42
Dynamic strength measurements
Dynamic measurements of skeletal muscle strength are performed using either isokinetic (fixed speed of movement) or isotonic (fixed resistance applied to the muscle during the movement) techniques.
Isokinetic measurements are usually performed at a fixed angular velocity of 60°–90°/s35 while isotonic skeletal muscle strength can be assessed with hydraulic resistance devices, force transducer platforms adapted to weightmachines or with 1-repetition maximum (1-RM) tests.35 The latter represents the highest load that can be lifted once throughout the whole range of motion, while the former represents the peak torque obtained at any specific joint angle.35 In addition to the standardized procedure from the American College of Sports Medicine,43 the velocity of the movement, positioning, warm-up, rest period as well as familiarization should also be standardized (Table 1), although this is often missing in COPD studies.35
Skeletal muscle endurance and fatigue measurements
Skeletal muscle endurance refers to a muscle’s ability to sustain or repeat a specific task over time,43 while fatigue refers to a reversible reduction in force generated by the muscle during a given task.43 Reduced quadriceps endurance is common in COPD,44 often reported decreased to a larger magnitude than weakness,23 and has also shown to have relevance to tasks of daily living.44 Importantly, the impairment in skeletal muscle endurance cannot be predicted from muscle strength, highlighting that both aspects of muscle function should be evaluated.6
Furthermore, skeletal muscle endurance could be evaluated in various ways, using either sustained or repeated contractions and using a variety of different techniques.44 In people with COPD, isometric, isotonic and isokinetic skeletal muscle endurance measurements have recently demonstrated high to very high relative reliability (ICC 0.76–0.94, 0.85–0.94 and 0.78–0.99, respectively). Meanwhile, isokinetic work fatigue index, eg, the ratio of work performed during the last ten repetitions to the work performed during the first ten repetitions, has demonstrated very low to high relative reliability (ICC −0.24 to 0.77).32,33 All techniques were also clinically feasible with a mean time consumption of <7.5 mins.33 Isokinetic shoulder flexion and knee extension endurance measurements have also found to be moderately to largely responsive to resistance training.45
How to perform measurements of skeletal muscle endurance
Static measurements of skeletal muscle endurance are performed by asking the subject to sustain a muscle contraction at an intensity corresponding to a pre-specified intensity of their MVC, normally from 20% to 60% of individual MVC until exhaustion using visual feedback.33,44 To get dynamic measurements, the recommendations are that isokinetic endurance and fatigue measurements are recorded/observed at a fixed angular velocity of 90°/s during maximal contraction(s) (normally 30), and throughout the whole joint range of motion.32,33 Isotonic endurance protocols are performed with constant external loading and standardization of range of motion, and speed of movement (eg, using a metronome) is recommended in order to minimize variation in testing.33 In COPD, external loads corresponding to 10% up to 50% of the individual MVC have been used during repeated contractions performed until failure.6,33,46 Results are quantified by reporting the time or number of repetitions performed.33,44,46 An advantage of isotonic muscle testing over isometric and isokinetic techniques is that it could be performed using simple equipment such as elastic bands,46 exercise platforms/benches6 or pulley systems.47
The role of functional tests
Since there is more to skeletal muscle function than strictly the ability to exert a certain torque over a certain period of time and since muscle impairments do not fully explain impaired daily functional activities,48 increased interest has been given in the last few years to examine the relationships between muscle dysfunction and limitations in functional activities of patients with COPD, among others through tools that represent patients’ global functioning and that assess activities that are meaningful to them.8,49–51 Functional tests assess in a standardized environment patients’ ability to perform activities that mirror what they actually do in their daily life. They can help to provide insights on how the physiological, structural and functional changes happening in peripheral muscles impact and contribute to limitations and restrictions of participation in the daily life of patients and ultimately their quality of life.51
Determinants of performance in functional tests in COPD include sensory integration, balance, age, psychological factors, the severity of airflow limitation, exercise tolerance and often various muscle groups coordinated work.50,52 Muscles’ contribution differs in functional tests: some seem to require more muscle endurance (such as the unsupported upper limb exercise test), some muscle strength (such as a five-repetition-sit-to-stand test) and others muscle power (such as the stair power climbing test – SCPT). Other functional tests rely more importantly on exercise tolerance and patients’ cardiorespiratory limitations, such as the six-minute walk test, incremental and endurance shuttle tests, the Glittre-Activities of Daily Life (ADL) test, the thirty-second, and one-minute sit-to-stand tests, and the step tests. Based on the lesser implication of upper or lower muscle function, these tests were not included in this paper. Recent literature reviews49,50 detailed standardized assessments, psychometric properties, and main advantages and limitations of upper- and lower-extremity functional tests commonly used to assess functional performance in COPD. In Table 2, major characteristics of functional tests in COPD that seem to rely more heavily on muscle strength, power or endurance are presented. Interestingly, the SCPT, Short Physical Performance Battery (SPPB), usual gait speed test, and the Timed-Up and Go tests were all recommended to assess physical functional performance by the European Working Group on Sarcopenia in Older People53 in the sarcopenia diagnosis process. Their definition and diagnosis of sarcopenia rely on impaired muscle strength or physical functional performance (or both in severe conditions), combined with impaired muscle mass,53 a clinical syndrome prevalent in people with COPD (14.5% [95% CI 11.8%–17.4%]).54
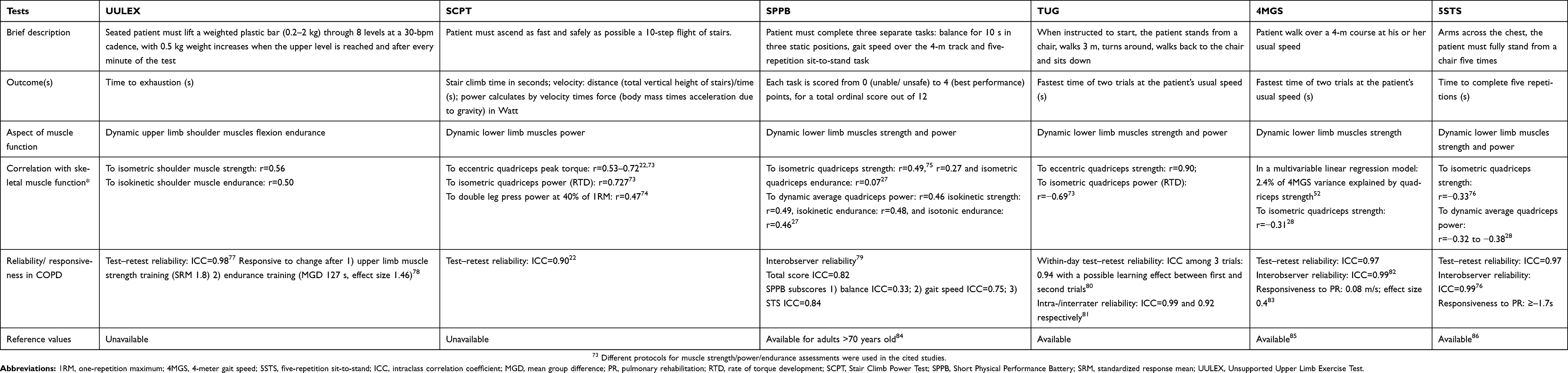 |
Table 2 Main characteristics of physical function tests in COPD and their associations with skeletal muscle function |
However, one should keep in mind that functional tests and muscle function assessments evaluate different constructs (as shown by the low to moderate strengths of their correlations and often lack studies looking at correlations between the proper required muscle aspect and the functional test) and thus cannot replace one another.42,49,50 For example, impaired skeletal muscle strength could indicate a potential difficulty to stand from a chair without using one’s arms and could thus hint a professional toward administering a five-repetition-sit-to-stand test to that patient. However, less is known about functional tests’ ability to detect muscle dysfunction in patients with COPD and their use in prescribing and individualizing muscle resistance training for these patients.50 Further studies investigating these links and muscle training specifically designed according to the impaired skeletal muscle parameter (strength, endurance, fatigability or power) required for specific functional activities are necessary.
New perspectives
Measuring and monitoring skeletal muscle power
An aspect of skeletal muscle function that, to date, has received less attention among people with COPD is muscle power, defined as the ability to generate an increase in contractile force over a certain unit of time (product of force and velocity).55 Interestingly, this aspect of skeletal muscle function declines faster with aging than muscle strength does.56 The decline in skeletal muscle power may be linked to various age-related neuromuscular changes, including but not limited to loss of size of fast-twitch muscle fibers, a reduction in the number of spinal motor neurons and excitable motor units, as well as a decrease in muscle fiber contraction time.57 In COPD, leg muscle power has been found to be reduced with approximately 28% compared to healthy age, sex and body mass matched adults when estimated using the functional SCPT.22 However, even though these findings suggest that leg muscle power is possibly impaired in people with COPD, formal assessments of leg muscle power using more mechanistic measures of muscle power are needed to confirm these results. Various protocols could be used, eg, measuring peak velocity during isotonic contractions, the rate of torque development (RTD) from isometric contractions,58 or peak/average power during dynamic isokinetic and isotonic contractions.59
Even though not yet used to determine the presence of a possibly reduced skeletal muscle power in COPD, these measurement techniques have been found to be more strongly associated with physical capacity and mobility, such as walking distance, gait speed and balance, than muscle strength in people with COPD and older adults.59–61 Indeed, Hernandez et al60 found that dynamic muscle power at 50% 1RM in COPD was positively correlated with objectively measured light-intensity physical activity, while they found no associations with skeletal muscle strength. Thus, measuring dynamic skeletal muscle power in people with COPD may provide important clinical value. Recently, data from our laboratory (unpublished) indicate high to very high relative reliability (ICC 0.78–0.99) for dynamic power measurements in people with COPD while static RTD measurements demonstrated moderate to very high relative reliability (ICC 0.63–0.86). Measures of absolute reliability (SEM%) was <10% for dynamic techniques while >30% for RTD. Furthermore, all participants were able to perform the test and no adverse events were reported, thus indicating that the procedure used for assessing muscle power seems to be safe. Even though detailed information regarding muscle power deficits in people with COPD is not yet available, the closer link between dynamic muscle power and physical capacity60 and with daily life physical activity than muscle strength60 highlights a need to explore this aspect of skeletal muscle function more thoroughly.
Dynamic versus static measurements and specificity of measurement techniques
As highlighted previously, isometric measurements of quadriceps strength using strain gauges are recommended when measuring skeletal muscle function in people with COPD.1 However, the best measurement strategy is the one that fits the goal of the measurement.26 Thus, even though isometric measurements have shown to provide important prognostic information, this does not denote that isometric measurements should always be favored. For example, if the goal of the measurement is to provide information on factors associated with functional tasks, such as walking or standing up from a chair, recent studies have actually highlighted that dynamic measurements seem to be superior, independent of whether the strength or the endurance capacity of the skeletal muscle is targeted. Indeed, Géphine et al27 found closer relationships between dynamic than isometric measurements of quadriceps muscle strength and endurance and common functional tests such as the 6-min walk test, the one-minute sit-to-stand test, the Glittre-ADL test as well as the SPPB test. With regard to the latter, similar findings were seen by Bui et al28 when exploring the relationship between isometric and dynamic measurements of quadriceps muscle strength and the SPPB. If we considered that activities such as walking or standing from sitting require skeletal muscles to work over a dynamic range of motion at the joint in a similar way as during dynamic measurements, rather than at a specific joint angle (which is the case during isometric measurements62), these findings seem reasonable.
Furthermore, even though isometric, isokinetic, as well as isometric measurements have been reported to be responsive to exercise training,38,63,64 the magnitude of effect seems to differ between techniques.63 For example, in a systematic review by De Brandt et al,63 percentage changes in isokinetic quadriceps endurance following different exercise interventions were on average 16%, while corresponding numbers for isometric and isotonic measurement strategies were 42% and 67%, respectively. One important explanatory factor for these observed differences could be related to the specificity of the exercise technique or equipment used with the exercise(s) performed, a concept that has been referred to as mechanical specificity.65 To our knowledge, this was first exemplified in 1990 in a study by Boyer et al66 in which participants exercised similar muscle groups with similar exercise set-ups but with different exercise equipment (either free weights or weight machines). After the intervention period, the free-weight group showed significantly greater strength gains than the weight machine group when tested using free weights (20.8% vs 12.3%). In the opposite way, the weight machine group showed significantly greater strength gains than the free weight group when tested using weight machines (40.7% vs 19.9%). If this is applied in the studies involved in the review by de Brandt et al,63 it could be noted that neither of the studies that evaluated quadriceps muscle endurance using isokinetic measurement techniques performed training exercises using isokinetic equipment while all studies that evaluated quadriceps endurance using an isotonic measurement technique also included isotonic exercises. Similar findings were seen by our research group, in which larger increases in elastic knee extension endurance than isokinetic knee extension endurance (37% vs 11%) were seen after 8 weeks of elastic band resistance training (unpublished data). Even though these findings need further investigation, they suggest that the choice of measurement technique and equipment should mirror what was or will be used during training.
Indirect measurements of muscle function
In addition to direct measurements of skeletal muscle function using dynamic or static measurements, indirect measurements of skeletal muscle function, eg, with the addition of motion sensors or electromyography may provide additional and clinically relevant information. For example, Ehsani et al67 found that by adding low-cost wearable motion sensors to a dynamic elbow flexion/extension test, in addition to the number of repetitions, they could also record speed, range of motion, speed reduction and speed variability. From these results, they produced a “frailty score” for the inpatients that was better than the number of repetitions alone or other measurements such as the COPD assessment test scores to predict both all-cause 30-day readmission and unfavorable discharge disposition following exacerbations. In another study with outpatients, the same test scores were also strongly correlated to clinical measurements such as the six-minute walk test and lung function parameters.68 Furthermore, Boccia et al69 used multichannel surface electromyography to measure muscle fiber conduction velocity during an isometric knee extension endurance test, providing useful insight into muscle fatigability and muscle abnormalities in COPD. Additionally, multichannel surface electromyography has also shown to be moderately to very strongly correlated to lung function measurements, six-minute walk distance as well as direct measurements of quadriceps endurance (time to exhaustion).70 However, to our knowledge, research on the topic of using, for example, motion sensors or electromyography as an “add-on” to direct measurements of muscle function in COPD is relatively sparse and more research is necessary. For example, we need to determine the clinical feasibility, reliability and the responsiveness of the test procedures and further investigate the potential additional benefit of using these measurement techniques on different muscles and muscle groups.
Measurement of skeletal muscle function – how to become a reality in the clinical setting?
Despite the prognostic and clinical relevance of skeletal muscle function in people with COPD,4–7 measurements and monitoring of skeletal muscle function remain to be an integrated part of the routine assessment and management of COPD. In order to facilitate the implementation of skeletal muscle function measurements into the clinical arena, we believe that are some key aspects that need to be considered.
Development of clinically feasible and standardized measurement protocols
First of all, clinically feasible and standardized measurement protocols that are valid, reliable and responsive are needed. With regard to the standardization of measurement properties, some key aspects that should be considered when measuring or monitoring skeletal muscle function have been outlined (Table 1). Furthermore, in order to increase clinical feasibility, measurement protocols need to minimize time consumption and include equipment that are widely available across different clinical context. With regard to the latter, the use of functional tests is intriguing. However, as highlighted previously, the often modest relationships between functional tests and skeletal muscle function measurements indicate that they evaluate different constructs and thus cannot replace one another. Thus, for accurate assessments of skeletal muscle function, specific and formal assessments of muscle function should be prioritized. Furthermore, and of utmost importance, the validity and reliability of measurement techniques need to be established in the targeted population in order to ensure accurate and reproducible measurements. About the latter, the add-on of, for example, motion sensors may be one way to accurately estimate both range of motion and speed of motion during dynamic measurements of skeletal muscle function, which is crucial to maximize the reliability of measurements for the individual patient. Lastly, in order to identify changes in skeletal muscle function following a clinical intervention that is meaningful for the patient, the minimal clinically important difference of different aspects of skeletal muscle function needs to be established.
Predictive equations and normative values
Secondly, equations to predict normative values that are widely applicable have to be developed, and normative values that will be obtained from these predictive equations have to be validated in the population of interest. To date, predictive equations and normative values are available for some aspects of skeletal muscle function, eg, isometric quadriceps strength.3,5,71 However, to our knowledge, no equation has been widely accepted within the pulmonary community. This is an issue because if used, large variations are seen between available equations. For example, if utilized on a random sample of isometric knee extension strength data from our laboratory, the percentage of patients with an isometric knee extension strength <70% of predicted would be 10%,5 22%3 and 76%,71 respectively, using available equations. In addition, the predictive ability of the best equation explained 51% of the variance in actual isometric knee extension strength.3 This can be compared with the best predictive equations for the 6-min walk test that explained 77% of the total variance in walking distance.72 Furthermore, to our knowledge, no predictive equations or normal values exist for other aspects of skeletal muscle function, for eg, endurance or power at least not that has been validated among people with COPD.
Conclusion
Considering the complexity of skeletal muscle dysfunction in COPD,1 no single test could be used to measure and monitor skeletal muscle function within the COPD population. Nevertheless, due to its clinical and prognostic value, measuring and monitoring skeletal muscle function should be a part of the routine assessment of people with COPD, even though this is yet to become a clinical reality. In order to achieve this goal, standardized and clinically feasible measurement protocols, as well as normative values and predictive equations across the spectrum of impaired function in COPD, are needed. This should minimally target the quadriceps muscle; however, depending on the objective of measurements, other muscles could also be tested in order to aid design and individualization of exercise programs or to evaluate effects of various interventions.8 Even though quadriceps muscle strength measurements are of utmost importance, current evidence suggests that other aspects of skeletal muscle function such as the endurance and power capacity of the muscle should also be considered. Moreover, current evidence also suggest that even though isometric measurements have been recommended, dynamic measurements of skeletal muscle function should not be neglected as they, in a larger extent than isometric measurements, are related to functional daily life tasks in patients with COPD.
Disclosure
Dr Andre Nyberg reports grants from Swedish Research Council, Swedish Heart and Lung Foundation, Swedish Heart and Lung Association, Strategic Research Area in Care Sciences, Harald Jeanssons Stiftelse samt Harald och Greta Jeanssons Stiftelse, Erika och Rudolf Gustavssons fond, Insamlingsstiftelsen and personal fees from AstraZeneca, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Maltais F, Decramer M, Casaburi R, et al. An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014;189(9):e15–e62. doi:10.1164/rccm.201402-0373ST
2. Barreiro E, Bustamante V, Cejudo P, et al. Guidelines for the evaluation and treatment of muscle dysfunction in patients with chronic obstructive pulmonary disease. Arch Bronconeumol. 2015;51(8):384–395. doi:10.1016/j.arbres.2015.04.011
3. Seymour JM, Spruit MA, Hopkinson NS, et al. The prevalence of quadriceps weakness in COPD and the relationship with disease severity. Eur Respir J. 2010;36(1):81–88. doi:10.1183/09031936.00104909
4. Decramer M, Gosselink R, Troosters T, Verschueren M, Evers G. Muscle weakness is related to utilization of health care resources in COPD patients. Eur Respir J. 1997;10(2):417–423.
5. Gosselink R, Troosters T, Decramer M. Peripheral muscle weakness contributes to exercise limitation in COPD. Am J Respir Crit Care Med. 1996;153:976–980. doi:10.1164/ajrccm.153.3.8630582
6. Coronell C, Orozco-Levi M, Mendez R, Ramirez-Sarmiento A, Galdiz JB, Gea J. Relevance of assessing quadriceps endurance in patients with COPD. Eur Respir J. 2004;24(1):129–136.
7. Swallow EB, Reyes D, Hopkinson NS, et al. Quadriceps strength predicts mortality in patients with moderate to severe chronic obstructive pulmonary disease. Thorax. 2007;62(2):115–120. doi:10.1136/thx.2006.062026
8. Nyberg A, Saey D, Maltais F. Why and how limb muscle mass and function should be measured in patients with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2015;12(9):1269–1277. doi:10.1513/AnnalsATS.201505-278PS
9. Remels AH, Schrauwen P, Broekhuizen R, et al. Peroxisome proliferator-activated receptor expression is reduced in skeletal muscle in COPD. Eur Respir J. 2007;30(2):245–252. doi:10.1183/09031936.00144106
10. Natanek SA, Gosker HR, Slot IG, et al. Heterogeneity of quadriceps muscle phenotype in chronic obstructive pulmonary disease (COPD); implications for stratified medicine? Muscle Nerve. 2013;48:488–497. doi:10.1002/mus.23784
11. Gifford JR, Trinity JD, Kwon OS, et al. Altered skeletal muscle mitochondrial phenotype in COPD: disease vs. disuse. J Appl Physiol (1985). 2018;124(4):1045–1053. doi:10.1152/japplphysiol.00788.2017
12. Shrikrishna D, Patel M, Tanner RJ, et al. Quadriceps wasting and physical inactivity in patients with COPD. Eur Respir J. 2012;40(5):1115–1122. doi:10.1183/09031936.00170111
13. Bernard S, Leblanc P, Whittom F, et al. Peripheral muscle weakness in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;158(2):629–634. doi:10.1164/ajrccm.158.2.9711023
14. Larsson L. Histochemical characteristics of human skeletal muscle during aging. Acta Physiol Scand. 1983;117(3):469–471. doi:10.1111/j.1748-1716.1983.tb00024.x
15. Allaire J, Maltais F, Doyon JF, et al. Peripheral muscle endurance and the oxidative profile of the quadriceps in patients with COPD. Thorax. 2004;59(8):673–678. doi:10.1136/thx.2003.020636
16. Patel MS, Natanek SA, Stratakos G, et al. Vastus lateralis fiber shift is an independent predictor of mortality in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014;190(3):350–352. doi:10.1164/rccm.201404-0713LE
17. Maltais F, Leblanc P, Whittom F, et al. Oxidative enzyme activities of the vastus lateralis muscle and the functional status in patients with COPD. Thorax. 2000;55(10):848–853. doi:10.1136/thorax.55.10.848
18. Saey D, Lemire BB, Gagnon P, et al. Quadriceps metabolism during constant workrate cycling exercise in chronic obstructive pulmonary disease. J Appl Physiol. 2011;110(1):116–124. doi:10.1152/japplphysiol.00153.2010
19. Gandevia SC. Spinal and supraspinal factors in human muscle fatigue. Physiol Rev. 2001;81(4):1725–1789. doi:10.1152/physrev.2001.81.4.1725
20. Amann M, Dempsey JA. Locomotor muscle fatigue modifies central motor drive in healthy humans and imposes a limitation to exercise performance. J Physiol. 2008;586(1):161–173. doi:10.1113/jphysiol.2007.141838
21. Gagnon P, Bussieres JS, Ribeiro F, et al. Influences of spinal anesthesia on exercise tolerance in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(7):606–615. doi:10.1164/rccm.201203-0404OC
22. Roig M, Eng JJ, MacIntyre DL, Road JD, Reid WD. Associations of the stair climb power test with muscle strength and functional performance in people with chronic obstructive pulmonary disease: a cross-sectional study. Phys Ther. 2010;90(12):1774–1782. doi:10.2522/ptj.20100091
23. Van’t Hul A, Harlaar J, Gosselink R, Hollander P, Postmus P, Kwakkel G. Quadriceps muscle endurance in patients with chronic obstructive pulmonary disease. Muscle Nerve. 2004;29(2):267–274. doi:10.1002/mus.10552
24. Frykholm E, Klijn P, Saey D, et al. Effect and feasibility of non-linear periodized resistance training in people with COPD: study protocol for a randomized controlled trial. Trials. 2019;20(1):6. doi:10.1186/s13063-019-3242-6
25. American College of Sports M. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009;41(3):687–708. doi:10.1249/MSS.0b013e3181915670
26. Diehr P, Chen L, Patrick D, Feng Z, Yasui Y. Reliability, effect size, and responsiveness of health status measures in the design of randomized and cluster-randomized trials. Contemp Clin Trials. 2005;26(1):45–58. doi:10.1016/j.cct.2004.11.014
27. Géphine S, Frykholm E, Nyberg A, Bui K-L, Maltais F, Saey D. Relationship between functional capacity, dynamic and static muscle function assessments in people with Chronic Obstructive Pulmonary Disease (COPD). Eur Respir J. 2018;52(suppl 62):PA4154. doi:10.1183/13993003.01675-2018
28. Bui K-L, Mathur S, Maia N, et al. Associations between isometric and dynamic quadriceps measures with functional capacity in chronic obstructive pulmonary disease (COPD). Eur Respir J. 2018;52(suppl 62):PA3344. doi:10.1183/13993003.01675-2018
29. Han TR, Shin HI, Kim IS. Magnetic stimulation of the quadriceps femoris muscle: comparison of pain with electrical stimulation. Am J Phys Med Rehabil. 2006;85(7):593–599. doi:10.1097/01.phm.0000223239.93539.fe
30. Polkey MI, Kyroussis D, Hamnegard CH, Mills GH, Green M, Moxham J. Quadriceps strength and fatigue assessed by magnetic stimulation of the femoral nerve in man. Muscle Nerve. 1996;19(5):549–555. doi:10.1002/(SICI)1097-4598(199605)19:5<549::AID-MUS1>3.0.CO;2-B
31. Burtin C, Saey D, Saglam M, et al. Effectiveness of exercise training in patients with COPD: the role of muscle fatigue. Eur Respir J. 2012;40(2):338–344. doi:10.1183/09031936.00111811
32. Ribeiro F, Lepine PA, Garceau-Bolduc C, et al. Test-retest reliability of lower limb isokinetic endurance in COPD: A comparison of angular velocities. Int J Chron Obstruct Pulmon Dis. 2015;10:1163–1172. doi:10.2147/COPD.S81806
33. Frykholm E, Gephine S, Saey D, et al. Inter-day test-retest reliability and feasibility of isokinetic, isometric, and isotonic measurements to assess quadriceps endurance in people with chronic obstructive pulmonary disease: A multicenter study. Chron Respir Dis. 2019;16:1479973118816497.
34. Thompson WRG, Neil F Pescatello, Linda S, et al. ACSM's guidelines for exercise testing and prescription.
35. Robles PG, Mathur S, Janaudis-Fereira T, Dolmage TE, Goldstein RS, Brooks D. Measurement of peripheral muscle strength in individuals with chronic obstructive pulmonary disease: a systematic review. J Cardiopulm Rehabil Prev. 2011;31(1):11–24. doi:10.1097/HCR.0b013e3181ebf302
36. Man W, Moxham J, Polkey MI. Magnetic stimulation for the measurement of respiratory and skeletal muscle function. Eur Respir J. 2004;24:846–860. doi:10.1183/09031936.04.00029004
37. Nyberg A, Saey D, Martin M, Maltais F. Test–re-test reliability of quadriceps muscle strength measures in people with more severe chronic obstructive pulmonary disease. J Rehabil Med. 2018;50:759–764. doi:10.2340/16501977-2354
38. Vaidya T, Beaumont M, de Bisschop C, et al. Determining the minimally important difference in quadriceps strength in individuals with COPD using a fixed dynamometer. Int J Chron Obstruct Pulmon Dis. 2018;13:2685–2693. doi:10.2147/COPD.S161342
39. Machado Rodrigues F, Demeyer H, Hornikx M, et al. Validity and reliability of strain gauge measurement of volitional quadriceps force in patients with COPD. Chron Respir Dis. 2017;14:1479972316687210.
40. Jeong M, Kang HK, Song P, et al. Hand grip strength in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2017;12:2385–2390. doi:10.2147/COPD.S140915
41. Beaumont M, Kerautret G, Peran L, Pichon R, Le Ber C, Cabillic M. Reproductibilité de la mesure de la force et de l’endurance du quadriceps dans la BPCO. Rev Mal Respir. 2017;34(9):1000–1006. doi:10.1016/j.rmr.2016.11.004
42. Bui K-L, Mathur S, Dechman G, Maltais F, Camp PG, Saey D. Fixed handheld dynamometry provides reliable and valid values for quadriceps isometric strength in patients with COPD: a multicenter study. Phys Ther. 2019;
43. Enoka RM, Duchateau J. Muscle fatigue: what, why and how it influences muscle function. J Physiol. 2008;586(1):11–23. doi:10.1113/jphysiol.2007.139477
44. Evans R, Kaplovitch E, Beauchamp MK, et al. Is quadriceps endurance reduced in COPD? Chest J. 2015;147(3):673. doi:10.1378/chest.14-1079
45. Nyberg A, Tornberg A, Wadell K. Correlation between limb muscle endurance, strength, and functional capacity in people with chronic obstructive pulmonary disease. Physiother Can. 2016;68(1):46–53. doi:10.3138/ptc.2014-93
46. Nyberg A, Lindstrom B, Rickenlund A, Wadell K. Low-load/high-repetition elastic band resistance training in patients with COPD: a randomized, controlled, multicenter trial. Clin Respir J. 2015;9(3):278–288. doi:10.1111/crj.12141
47. Nyberg A, Saey D, Martin M, Maltais F. Acute effects of low-load/high-repetition single-limb resistance training in COPD. Med Sci Sports Exerc. 2016;48(12):2353–2361. doi:10.1249/MSS.0000000000001027
48. Clark CJ, Cochrane L, Mackay E. Low intensity peripheral muscle conditioning improves exercise tolerance and breathlessness in COPD. Eur Respir J. 1996;9:2590–2596.
49. Rausch-Osthoff A-K, Kohler M, Sievi NA, Clarenbach CF, van Gestel A
50. Johnston KN, Potter AJ, Phillips A. Measurement properties of short lower extremity functional exercise tests in people with chronic obstructive pulmonary disease: systematic Review. Phys Ther. 2017;97(9):926–943. doi:10.1093/ptj/pzx063
51. Mathur S, Dechman G, Bui K-L, Camp PG, Saey D. Evaluation of limb muscle strength and function in people with chronic obstructive pulmonary disease. Cardiopulm Phys Ther J. 2018;30(1):24–34. doi:10.1097/CPT.0000000000000090
52. Bui K-L, Nyberg A, Maltais F, Saey D. Functional tests in chronic obstructive pulmonary disease, part 1: clinical relevance and links to the international classification of functioning, disability, and health. Ann Am Thorac Soc. 2017;14(5):778–784. doi:10.1513/AnnalsATS.201609-733AS
53. Bernabeu-Mora R, Gimenez-Gimenez LM, Montilla-Herrador J, Garcia-Guillamon G, Garcia-Vidal JA, Medina-Mirapeix F. Determinants of each domain of the short physical performance battery in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2539–2544. doi:10.2147/COPD.S138402
54. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: european consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in older people. Age Ageing. 2010;39(4):412–423. doi:10.1093/ageing/afq034
55. Jones SE, Maddocks M, Kon SS, et al. Sarcopenia in COPD: prevalence, clinical correlates and response to pulmonary rehabilitation. Thorax. 2015;70(3):213–218. doi:10.1136/thoraxjnl-2014-206440
56. Sapega A, Drillings G. The definition and assessment of muscular power. J Orthop Sports Phys Ther. 1983;5(1):7–9. doi:10.2519/jospt.1983.5.1.7
57. Izquierdo M, Ibanez J, Gorostiaga E, et al. Maximal strength and power characteristics in isometric and dynamic actions of the upper and lower extremities in middle-aged and older men. Acta Physiol Scan. 1999;167(1):57–68. doi:10.1046/j.1365-201x.1999.00590.x
58. Aagaard P, Suetta C, Caserotti P, Magnusson SP, Kjaer M. Role of the nervous system in sarcopenia and muscle atrophy with aging: strength training as a countermeasure. Scand J Med Sci Sports. 2010;20(1):49–64. doi:10.1111/j.1600-0838.2009.01084.x
59. Webber S, Porter M. Reliability of ankle isometric, isotonic and isokinetic strength and power testing in older women. Phys Ther. 2010;90(10):1165–1175. doi:10.2522/ptj.20090394
60. Reid KF, Fielding RA. Skeletal muscle power: a critical determinant of physical functioning in older adults. Exerc Sport Sci Rev. 2012;40(1):4–12. doi:10.1097/JES.0b013e31823b5f13
61. Hernandez M, Zambom-Ferraresi F, Cebollero P, Hueto J, Cascante JA, Anton MM. The relationships between muscle power and physical activity in older men with chronic obstructive pulmonary disease. J Aging Phys Act. 2017;25(3):360–366. doi:10.1123/japa.2016-0144
62. Bean J, Leveille S, Kiely D, Bandinelli S, Guralnik J, Ferrucci L. A comparison of leg power and leg strength within the InCHIANTI study: which influences mobility more? J Gerontol. 2003;58A(8):728–733.
63. Cheng AJ, Rice CL. Fatigue and recovery of power and isometric torque following isotonic knee extensions. J Appl Physiol (1985). 2005;99(4):1446–1452. doi:10.1152/japplphysiol.00452.2005
64. De Brandt J, Spruit MA, Hansen D, et al. Changes in lower limb muscle function and muscle mass following exercise-based interventions in patients with chronic obstructive pulmonary disease: A review of the English-language literature. Chron Respir Dis. 2018;15(2):182–219. doi:10.1177/1479972317709642
65. Zanini A, Aiello M, Cherubino F, et al. The one repetition maximum test and the sit-to-stand test in the assessment of a specific pulmonary rehabilitation program on peripheral muscle strength in COPD patients. Int J Chron Obstruct Pulmon Dis. 2015;10:2423–2430. doi:10.2147/COPD.S91176
66. Carpinelli R. A critical analysis of the national strength and conditioning association’s opinion that free weights are superior to machines for increasing muscular strength and power. Medicina Sportiva Practica. 2017;18(2):21–39.
67. Boyer BT. A comparison of the effects of three strength training programs on women. J Appl Sport Sci Res. 1990;4(5):88–94.
68. Ehsani H, Mohler MJ, Golden T, Toosizadeh N. Upper-extremity function prospectively predicts adverse discharge and all-cause COPD readmissions: a pilot study. Int J Chron Obstruct Pulmon Dis. 2019;14:39–49. doi:10.2147/COPD.S182802
69. Toosizadeh N, Berry C, Bime C, Najafi B, Kraft M, Mohler J. Assessing upper-extremity motion: an innovative method to quantify functional capacity in patients with chronic obstructive pulmonary disease. PLoS One. 2017;12(2):e0172766. doi:10.1371/journal.pone.0172766
70. Boccia G, Coratella G, Dardanello D, et al. Severe COPD alters muscle fiber conduction velocity during knee extensors fatiguing contraction. COPD. 2016;13(5):583–588. doi:10.3109/15412555.2016.1139561
71. Boccia G, Dardanello D, Rinaldo N, Coratella G, Schena F, Rainoldi A. Electromyographic manifestations of fatigue correlate with pulmonary function, 6 min walk test, and time to exhaustion in COPD. Respir Care. 2015;60(9):1295–1302. doi:10.4187/respcare.04138
72. Harbo T, Brincks J, Andersen H. Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body mass, height, and sex in 178 healthy subjects. Eur J Appl Physiol. 2012;112(1):267–275. doi:10.1007/s00421-011-1975-3
73. Singh SJ, Puhan MA, Andrianopoulos V, et al. An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1447–1478. doi:10.1183/09031936.00150414
74. Butcher SJ, Pikaluk BJ, Chura RL, Walkner MJ, Farthing JP, Marciniuk DD. Associations between isokinetic muscle strength, high-level functional performance, and physiological parameters in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2012;7:537–542. doi:10.2147/COPD.S34170
75. Bean JF, Kiely DK, LaRose S, Alian J, Frontera WR. is stair climb power a clinically relevant measure of leg power impairments in at-risk older adults? Arch Phys Med Rehabil. 2007;88(5):604–609. doi:10.1016/j.apmr.2007.02.004
76. Bernabeu-Mora R, Medina-Mirapeix F, Llamazares-Herran E, Garcia-Guillamon G, Gimenez-Gimenez LM, Sanchez-Nieto JM. The short physical performance battery is a discriminative tool for identifying patients with COPD at risk of disability. Int J Chron Obstruct Pulmon Dis. 2015;10:2619–2626. doi:10.2147/COPD.S94377
77. Jones SE, Kon SSC, Canavan JL, et al. The five-repetition sit-to-stand test as a functional outcome measure in COPD. Thorax. 2013;68(11):1015–1020. doi:10.1136/thoraxjnl-2013-203576
78. Takahashi T, Jenkins SC, Strauss GR, Watson CP, Lake FR. A new unsupported upper limb exercise test for patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil. 2003;23:430–437.
79. Janaudis-Ferreira T, Hill K, Goldstein RS, Wadell K, Brooks D. Relationship and responsiveness of three upper-limb tests in patients with chronic obstructive pulmonary disease. Physiother Can. 2012;1(1):1–4.
80. Medina-Mirapeix F, Bernabeu-Mora R, Llamazares-Herran E, Sanchez-Martinez MP, Garcia-Vidal JA, Escolar-Reina P. Interobserver reliability of peripheral muscle strength tests and short physical performance battery in patients with chronic obstructive pulmonary disease: a prospective observational study. Arch Phys Med Rehabil. 2016;97(11):2002–2005. doi:10.1016/j.apmr.2016.05.004
81. Mesquita R, Janssen D, Wouters EFM, Schols J, Pitta F, Spruit M. Within-day test-retest reliability of the timed up & go test in patients with advanced chronic organ failure. Arch Phys Med Rehabil. 2013;94(11):2131–2138. doi:10.1016/j.apmr.2013.03.024
82. Marques A, Cruz J, Quina S, Regencio M, Jacome C. Reliability, agreement and minimal detectable change of the timed up & go and the 10-meter walk tests in older patients with COPD. Chronic Obstr Pulm Dis. 2016;13(3):279–287. doi:10.3109/15412555.2015.1079816
83. Kon SSC, Patel MS, Canavan JL, et al. Reliability and validity of 4-metre gait speed in COPD. Eur Respir J. 2013;42:333–340. doi:10.1183/09031936.00162712
84. Kon SSC, Canavan JL, Nolan CM, et al. The 4-metre gait speed in COPD: responsiveness and minimal clinically important difference. Eur Respir J. 2014;43:1298–1305. doi:10.1183/09031936.00088113
85. Cabrero-Garcia J, Munoz-Mendoza CL, Cabanero-Martinez MJ, Gonzalez-Llopis L, Ramos-Pichardo JD, Reig-Ferrer A. [Short physical performance battery reference values for patients 70 years-old and over in primary health care]. Aten Primaria. 2012;44(9):540–548. doi:10.1016/j.aprim.2012.02.007
86. Bohannon RW, Williams Andrews A. Normal walking speed: a descriptive meta-analysis. Physiotherapy. 2011;97(3):182–189. doi:10.1016/j.physio.2010.12.004
87. Bohannon RW. Reference values for the five-repetition sit-to-stand test: a descriptive meta-analysis of data from elders. Percept Mot Skills. 2006;103(1):215–222. doi:10.2466/pms.103.1.215-222
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.