Back to Journals » Clinical Ophthalmology » Volume 17
Measurement Accuracy When Using Spot Vision Screener With or Without Cycloplegia in Young Adults
Authors Tatara S ![]() , Maeda F
, Maeda F ![]() , Ubukata H, Shiga Y, Yaoeda K
, Ubukata H, Shiga Y, Yaoeda K
Received 15 September 2023
Accepted for publication 7 November 2023
Published 21 November 2023 Volume 2023:17 Pages 3543—3548
DOI https://doi.org/10.2147/OPTH.S431202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Shunya Tatara,1,2 Fumiatsu Maeda,1,3 Hokuto Ubukata,1 Yuko Shiga,1 Kiyoshi Yaoeda3– 5
1Department of Orthoptics and Visual Sciences, Faculty of Medical Technology, Niigata University of Health and Welfare, Niigata, Japan; 2Department of Vision Science, Faculty of Sensory and Motor Control, Kitasato University Graduate School of Medical Science, Sagamihara, Kanagawa, Japan; 3Field of Orthoptics and Visual Sciences, Major in Medical and Rehabilitation Sciences, Niigata University of Health and Welfare Graduate School, Niigata, Japan; 4Department of Ophthalmology, Yaoeda Eye Clinic, Nagaoka, Niigata, Japan; 5Division of Ophthalmology and Visual Sciences, Niigata University Graduate School of Medical and Dental Sciences, Niigata, Japan
Correspondence: Shunya Tatara, Department of Orthoptics and Visual Sciences, Faculty of Medical Technology, Niigata University of Health and Welfare, 1398, Shimami-cho, kita-ku, Niigata-shi, Niigata, 950-3198, Japan, Tel/Fax +81 25 257 4752, Email [email protected]
Purpose: There are many unclear points about the accuracy of measurement of cycloplegic refraction using the Spot Vision Screener (SVS). This study aimed to investigate the accuracy of SVS measurements with cycloplegia for myopia.
Materials and Methods: Forty-nine healthy subjects were included, and refraction was measured. Objective refractions were measured by SVS, table-mounted autorefractometer (RT7000), and handheld autorefractometer (Retinomax Screeen) at noncycloplegic and cycloplegic conditions by 1% cyclopentolate. Subjective noncycloplegic refraction was obtained by a visual acuity and refraction test performed by certified orthoptists using a cross-cylinder. One-way repeated-measures analysis of variance was used to examine whether the measured refractions fluctuate due to different reflection tests.
Results: In the noncycloplegic condition, the mean (±standard deviation) spherical equivalent (SE) measured by subjective method, SVS, RT7000, and Retinomax Screeen were − 2.56 ± 3.00, − 2.62 ± 2.38, − 3.05 ± 2.84, and − 3.26 ± 2.97, respectively. The subjective SE and objective SE measured by SVS had significantly less myopic value than the objective SE measured by two autorefractometers (p < 0.001). In the cycloplegic condition, the mean (± standard deviation) SE measured by SVS, RT7000, and Retinomax Screeen were − 2.07 ± 2.66, − 2.62 ± 2.98, and − 2.66 ± 3.02, respectively. The objective SE measured by SVS had significantly less myopic value than SEs measured using other methods (p < 0.001). In the cycloplegic condition, SVS showed a fixed error wherein the SE was more hyperopic than that with the subjective method and SVS had a proportional error.
Conclusion: In the measurement under cycloplegic conditions, use of an autorefractometer rather than a photorefractometer such as SVS was preferable.
Keywords: refraction, refractive error, autorefractometer, photorefraction, screening, amblyopia risk factor
Introduction
Amblyopia is a unilateral or bilateral reduction in best-corrected visual acuity that is not directly attributed to a structural abnormality of the eye or posterior visual pathways.1 Unrecognized or untreated amblyopia in the early years of life can often lead to unsuccessful treatment and underdeveloped vision in the affected eye.1,2 The main risk factors for amblyopia include strabismus and refractive error. The American Association for Pediatric Ophthalmology and Strabismus (AAPOS) has established a cutoff value for “amblyopia risk factor” (ARF) based on strabismus and refractive error.3 Although refractive error is the most common cause of amblyopia,4 no gold standard cutoff value for refractive error has been established. In 2022, AAPOS revised the new cutoff values for ARFs for refractive error.5
A device that is specifically designed to screen for amblyopia due to refractive error is the Spot Vision Screener (SVS; Welch Allyn, NY, USA), which measures refractive error using a photorefraction method.6 SVS is frequently used for screening because it can measure both eyes at the same time and has an extremely high success rate, even in children.7,8 However, the characteristics of refraction obtained by SVS and the accuracy of screening have not been fully elucidated yet.
Screening for amblyopia of children with SVS has a sensitivity of 87%–95% and specificity of 71%–85% using the 2013 AAPOS criteria.6,9–11 and a sensitivity of 88% and specificity of 78% using the revised 2022 AAPOS criteria.12 However, when refractive error is measured using SVS under cycloplegic and noncycloplegic conditions, sensitivity and negative predictive value are higher in noncycloplegic conditions, and specificity and positive predictive value are higher in cycloplegic conditions.13
The high success rate of SVS measurements (even in children) is a major advantage for a refraction test,7,8 and if the accuracy of SVS with cycloplegia is high, it could potentially be used as a diagnostic instrument as well. Yagasaki et al14 compared cycloplegic refraction measured by SVS and that measured by autorefractometer in children and reported that there was a proportional error in which the hyperopic power of the SVS decreased as hyperopia increased. However, because the measurement accuracy of SVS for cycloplegic refraction in patients with myopia is unknown, this study aimed to investigate the accuracy of SVS measurements with cycloplegia in young adults. The subjective refraction was measured and used as a reference standard, after which it was compared to that of the SVS and auto refractometers in young adults, where there may be numerous people with myopia.
Materials and Methods
Participants
The subjects included 49 university student volunteers who had no eye diseases. In this study, 45 right eyes of the subjects (35 women and 10 men) were analyzed. Four subjects whose refraction measured by SVS were outside the measurement range were excluded. The mean age of the study participants was 19.2 years (standard deviation, 0.3).
Methods
Objective refractions were initially measured by SVS, table-mounted autorefractometer (RT7000; TOMEY, Aichi, Japan), and handheld autorefractometer (Retinomax Screeen; Righton, Tokyo, Japan) at noncycloplegic conditions. Subjective refraction was obtained by a visual acuity test performed by certified orthoptists using a cross-cylinder.15 Next, cycloplegia was induced by adding 1% cyclopentolate drops at 10-min intervals (two drops in total, at 0 and 10 min); 60 min after the first eye drop, all objective refractive measurements were repeated.
For both noncycloplegic and cycloplegic SVS, one measurement was obtained, and for RT7000 and Retinomax Screeen, the average of five consecutive measurements was obtained. All measurements were obtained on the same day.
Analysis
For the obtained refraction, power vector analysis16 was used to calculate the spherical equivalent (SE), J0 astigmatic components (J0), and J45 astigmatic components (J45).
One-way repeated-measures analysis of variance (ANOVA) and Bonferroni correction for multiple comparisons were used to compare noncycloplegic SE, J0, and J45 obtained by subjective and objective refraction tests using three devices. Similarly, repeated-measures ANOVA was used to compare cycloplegic SE, J0, and J45 obtained by objective refraction tests using three devices and noncycloplegic SE, J0, and J45. In this study, we considered the subjective refraction as the subject’s true value and examined the difference between the subjective SE and objective SE using Bland–Altman analysis. We calculated the systematic error (fixed and proportional errors) regarding the difference between the subjective and objective SEs. To examine fixed errors, one-sample t-test was performed for differences in SE. To examine the proportionality error, a significance test of the regression coefficients was performed. Two-sided tests were used for statistical significance, and the significance level was set at a p-value of <0.05. Statistical analysis was performed using EZR (Easy R) version 1.41, which is an open-source software based on R and R commands.17
Ethics Approval and Consent to Participate
This study was conducted under the approval of the Niigata University of Health and Welfare committee (19153-230905). The experiment was conducted in accordance with the Declaration of Helsinki, and written informed consent was obtained from all subjects.
Results
In the noncycloplegic condition, the subjective SE and objective SE measured by SVS showed significantly less myopic value than the objective SE measured by RT7000 and Retinomax Screeen (p < 0.001) (Figure 1A). The J0 results in the noncycloplegic condition showed no significant difference (p = 0.182) between the measurement methods (Figure 1B). For J45, there was a significant difference between the results of the SVS and Retinomax Screeen measured in the noncycloplegic condition (p = 0.015), but the difference was 0.1 D (Figure 1C).
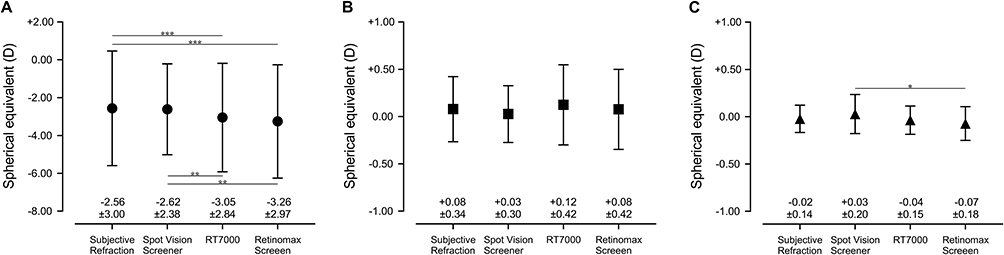 |
Figure 1 Comparison of objective refractions and subjective refraction measured under noncycloplegic condition. (A) Mean spherical equivalent (± standard deviation) measured by subjective method, SVS, RT7000, and Retinomax Screeen were −2.56 (3.00), −2.62 (2.38), −3.05 (2.84), and −3.26 (2.97), respectively. (B) J0 astigmatic component measured by subjective method, SVS, RT7000, and Retinomax Screeen were 0.08 (0.34), 0.03 (0.30), 0.12 (0.42), and 0.08 (0.42), respectively (C) J45 astigmatic component measured by subjective method, SVS, RT7000, and Retinomax Screeen were −0.02 (0.14), 0.03 (0.20), −0.04 (0.15), and −0.07 (0.18), respectively. *p < 0.05, **p < 0.01, ***p < 0.001. |
In the cycloplegic condition, the objective SE measured by SVS showed significantly less myopic value than SEs measured by other methods (p < 0.001) (Figure 2A). The J0 results in the cycloplegic condition showed no significant difference (p = 0.122) between the measurement methods (Figure 2B). The J45 results in the cycloplegic condition showed no significant difference (p = 0.167) between the measurement methods (Figure 2C).
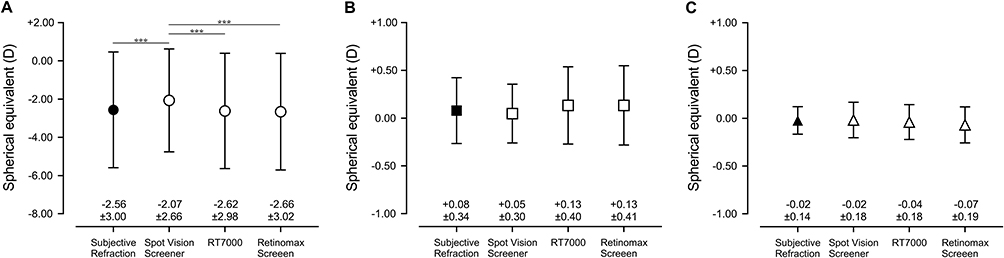 |
Figure 2 Comparison of objective refractions measured under cycloplegic condition and subjective refraction measured under noncycloplegic condition. Black symbols indicate results of non-cycloplegic condition and white symbols indicate results of cycloplegic condition. (A) Mean spherical equivalent (± standard deviation) measured by subjective method, SVS, RT7000, and Retinomax Screeen were −2.56 (3.00), −2.07 (2.66), −2.62 (2.98), and −2.66 (3.02), respectively. (B) J0 astigmatic component measured by subjective method, SVS, RT7000, and Retinomax Screeen were 0.08 (0.34), 0.05 (0.30), 0.13 (0.40), and 0.13 (0.41), respectively (C) J45 astigmatic component measured by subjective method, SVS, RT7000, and Retinomax Screeen were −0.02 (0.14), −0.02 (0.18), −0.04 (0.18), and −0.07 (0.19), respectively. ***p < 0.001. |
The SE differences between the subjective refraction and the three noncycloplegic objective refractions are shown in Bland–Altman plots (Figure 3). The noncycloplegic SEs measured by RT7000 and Retinomax Screeen had fixed errors that showed more myopic value, and SVS and RT7000 had proportional errors (Table 1). Similarly, the Bland–Altman plots showed the SE difference between the three objective refractions measured with the cycloplegic and subjective refraction (Figure 4). In the cycloplegic condition, SVS showed a fixed error wherein the measured value was more hyperopic and proportional error (Table 1).
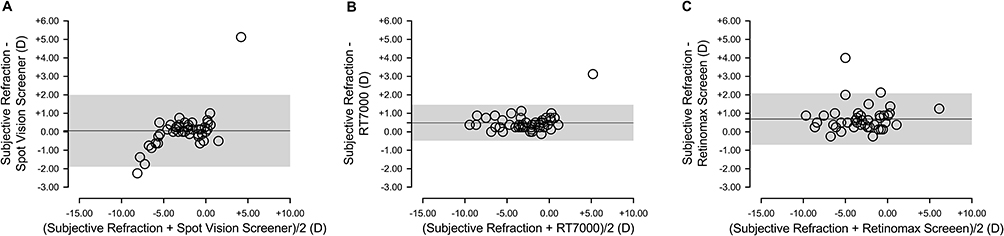 |
Figure 3 Difference in spherical equivalent between subjective refraction and three types of objective refraction under noncycloplegic condition visualized in Bland–Altman plots. (A) Bland–Altman plots of subjective refraction and objective refraction measured by Spot Vision Screener; Limits of agreement (LOA) was 0.05 ± 1.95. (B) Bland–Altman plots of subjective refraction and objective refraction measured by RT7000; LOA was 0.49 ± 0.97. (C) Bland–Altman plots of subjective refraction and objective refraction measured by Retinomax Screeen; LOA was 0.69 ± 1.39. |
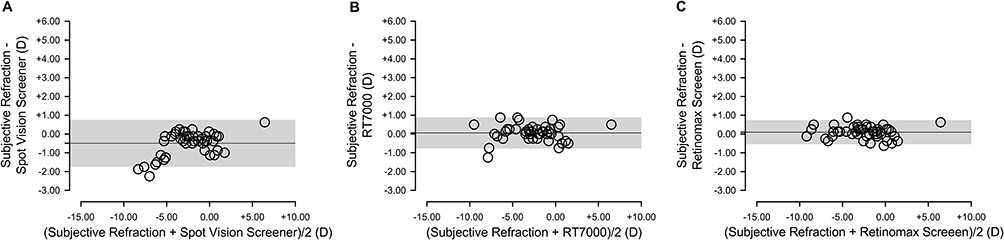 |
Figure 4 Difference in spherical equivalent between subjective refraction and three types of objective refraction under cycloplegic condition visualized in Bland–Altman plots. (A) Bland–Altman plots of subjective refraction and objective refraction measured by Spot Vision Screener; Limits of agreement (LOA) was −0.49 ± 1.25. (B) Bland–Altman plots of subjective refraction and objective refraction measured by RT7000; LOA was 0.06 ± 0.83. (C) Bland–Altman plots of subjective refraction and objective refraction measured by Retinomax Screeen; LOA was 0.10 ± 0.64. |
 |
Table 1 Fixed and Proportional Errors for Objective Refractions When Compared to Subjective Refraction |
Discussion
Retinoscopy is the most accurate objective refraction test when performed by an experienced clinician.18 However, because retinoscopy’s precision relies on the skills of the clinician, various refractive tests are performed under cycloplegic conditions. With cycloplegia during measurements, an autorefractometer provides accurate refraction, which is unknown for SVS under cycloplegic condition. In this study, we used the SVS before and after cycloplegic conditions and found that the refraction measured by cycloplegic SVS was different from those using other methods.
In noncycloplegic measurements, the SE measured by SVS was closer to subjective test than to other objective tests. Jorge et al18 reported that noncycloplegic SE measured by table-mounted autorefractometer, retinoscopy, and subjective refraction were −0.74, −0.32, and −0.29 D, respectively. Teberik et al19 revealed that noncycloplegic SE measured by Retinomax Screeen is more myopic than those measured by other photorefractometers. From these facts, it can be said that the refraction measured by the autorefractometer is myopic. Conversely, it has been reported that the refraction measured by SVS is more hyperopic than those measured by other autorefractometers.20 The same trend was observed in this study. However, there was a significant proportional error in the SE measured by SVS under noncycloplegic condition, indicating the higher the myopia, the lower the SVS value. SVS is a specialized screening device. The measurement accuracy of the SVS published by the manufacturer is ±0.50 D for −3.50 D to +3.50 D, and ±1.00 D for the range beyond this.21 Thus, the error is unavoidable due to the characteristics of the device wherein the measurement accuracy becomes unstable at strong refractive values.
Under cycloplegic condition, there was no significant difference between subjective refraction and objective refraction measured by RT-7000 and Retinomax Screeen, nor was there any proportional error or fixed error. Payerols et al22 reported mean (standard deviation) SEs of +1.06 (2.29) and +1.06 (1.57) for cycloplegic table-mounted autorefractometer and Retinomax Screeen, respectively, in children. The same was true in this study, with cycloplegic SEs measured by RT7000 and Retinomax Screeen having high measurement accuracy. Conversely, cycloplegic SE measured by SVS was significantly hyperopic compared to that by other measurement methods, and SVS had fixed and proportional errors. Yagasaki et al14 compared the SVS and autorefractometer under cycloplegic condition in subjects with hyperopia and reported that there was a proportional error, with higher hyperopia resulting in lower refractive value measured by SVS. In our study, which focused primarily on subjects with myopia, there was a proportional error in which the higher the degree of myopia, the lower the refractive values measured by SVS. The SVS is an off-axis23 photorefraction device. Therefore, it is assumed that the refraction is calculated based on a built-in fixed value of pupil diameter. Since SVS is a device specialized for screening, it can be expected that the refraction is calculated based on the pupil under noncycloplegic condition (ie, under natural pupil). Therefore, for SVS, the accuracy of the measurement may be worse with cycloplegic condition.
A limitation of this study is that the average age of the subjects was 19.2 years. Generally, the SVS is used for children, but this study aimed to examine the measurement accuracy in patients with myopia, so it was necessary to increase the age of the subjects. In addition, because the experiment was conducted at a single institution, there is a possibility that bias may have been introduced.
Conclusion
The SVS is characterized by its ability to measure both eyes simultaneously in a 1-s fixation period and by its extremely high measurement possibility. Therefore, SVS is beneficial in screening and in children, for whom cooperation from the patient is difficult to obtain. However, cycloplegic SVS measurement showed poor measurement accuracy of refraction. In addition, the measurement under cycloplegic condition has fixed and proportional errors. Therefore, in the measurement under cycloplegic conditions, it was considered preferable to use an autorefractometer rather than a photorefractometer such as SVS.
Acknowledgment
This research was funded by JSPS KAKENHI, grant number JP22K02470.
Disclosure
F. M. borrowed equipment free of charge from RIGHT MFG. CO., LTD (Tokyo, Japan). The authors report no other conflicts of interest in this work.
References
1. DeSantis D. Amblyopia. Pediatr Clin North Am. 2014;61(3):505–518. doi:10.1016/j.pcl.2014.03.006
2. Pediatric Eye Disease Investigator Group. A randomized trial of atropine vs. patching for treatment of moderate amblyopia in children. Arch Ophthalmol. 2002;120(3):268–278. doi:10.1001/archopht.120.3.268
3. Donahue SP, Arthur B, Neely DE, et al. Guidelines for automated preschool vision screening: a 10-year, evidence-based update. J AAPOS. 2013;17(1):4–8. doi:10.1016/j.jaapos.2012.09.012
4. Xiao O, Morgan IG, Ellwein LB, He M; Refractive Error Study in Children Study Group. Prevalence of amblyopia in school-aged children and variations by age, gender, and ethnicity in a multi-country refractive error study. Ophthalmolo. 2015;122(9):1924–1931. doi:10.1016/j.ophtha.2015.05.034
5. Arnold RW, Donahue SP, Silbert DI, et al. AAPOS uniform guidelines for instrument-based pediatric vision screen validation. J AAPOS. 2022;26(1):1.e1–1.e6. doi:10.1016/j.jaapos.2021.09.009
6. Peterseim MM, Papa CE, Wilson ME, et al. The effectiveness of the spot vision screener in detecting amblyopia risk factors. J AAPOS. 2014;18(6):539–542. doi:10.1016/j.jaapos.2014.07.176
7. Tatara S, Maeda F, Mizuno N, Noguchi A, Yaoeda K, Abe H. Refraction and pupil diameter in 3-year- and 1-month-old children as measured by spot vision screener. Sci Rep. 2019;9(1):15622. doi:10.1038/s41598-019-51993-1
8. Hayashi S, Suzuki I, Inamura A, et al. Effectiveness of the spot vision screener in screening 3-year-old children with potential amblyopia in Japan. Jpn J Ophthalmol. 2021;65(4):537–545. doi:10.1007/s10384-021-00823-x
9. Silbert DI, Matta NS. Performance of the spot vision screener for the detection of amblyopia risk factors in children. J AAPOS. 2014;18(2):169–172. doi:10.1016/j.jaapos.2013.11.019
10. Qian X, Li Y, Ding G, et al. Compared performance of spot and SW800 photoscreeners on Chinese children. Br J Ophthalmol. 2019;103(4):517–522. doi:10.1136/bjophthalmol-2018-311885
11. Mu Y, Bi H, Ekure E, et al. Performance of spot photoscreener in detecting amblyopia risk factors in Chinese pre-school and school age children attending an eye clinic. PLoS One. 2016;11(2):e0149561. doi:10.1371/journal.pone.0149561
12. Peterseim MMW, Trivedi RH, Monahan SR, et al. Effectiveness of the spot vision screener using updated. J AAPOS. 2023;27:24.e21–24.e27.
13. Yakar K. Clinical performance of the spot vision photo screener before and after induction of cycloplegia in children. J Ophthalmol. 2019;2019:5329121. doi:10.1155/2019/5329121
14. Yagasaki T, Toya A, Haga Y, Yokoyama Y, Yamamoto M, Yagasaki A. Comparison of cycloplegic refractions with 1% atropine sulfate when measured by an autorefractometer and spot vision screener [in Japanese]. J Eye. 2022;39:1549–1553.
15. Puntenney I. The principles of the cross cylinder and its uses in refraction. Q Bull Northwest Univ Med Sch. 1954;28(4):342–346.
16. Thibos LN, Wheeler W, Horner D. Power vectors: an application of Fourier analysis to the description and statistical analysis of refractive error. Optom Vis Sci. 1997;74(6):367–375. doi:10.1097/00006324-199706000-00019
17. Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. doi:10.1038/bmt.2012.244
18. Jorge J, Queirós A, Almeida JB, Parafita MA. Retinoscopy/autorefraction: which is the best starting point for a noncycloplegic refraction? Optom Vis Sci. 2005;82(1):64–68.
19. Teberik K, Eski MT, Kaya M, Ankarali H. A comparison of three different photoscreeners in children. J Pediatr Ophthalmol Strabismus. 2018;55(5):306–311. doi:10.3928/01913913-20180405-03
20. Peterseim MM, Papa CE, Wilson ME, et al. Photoscreeners in the pediatric eye office: compared testability and refractions on high-risk children. Am J Ophthalmol. 2014;158(5):932–938. doi:10.1016/j.ajo.2014.07.041
21. Welch Allyn® Spot™ VisionScreener Model VS100. Available from: https://www.welchallyn.com/content/dam/welchallyn/documents/upload-docs/user-testing/80024081A.pdf.
22. Payerols A, Eliaou C, Trezeguet V, Villain M, Daien V. Accuracy of PlusOptix A09 distance refraction in pediatric myopia and hyperopia. BMC Ophthalmol. 2016;16(1):72. doi:10.1186/s12886-016-0247-8
23. Kaakinen K. A simple method for screening of children with strabismus, anisometropia or ametropia by simultaneous photography of the corneal and the fundus reflexes. Acta Ophthalmol. 1979;57(2):161–171. doi:10.1111/j.1755-3768.1979.tb00481.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The UCI EyeMobile Preschool Vision Screening Program: Refractive Error and Amblyopia Results from the 2019–2020 School Year
Hunter SC, He J, Han M, Suh DW
Clinical Ophthalmology 2022, 16:4249-4255
Published Date: 20 December 2022