Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
MDT Reduces Perioperative Thrombotic Events in Elderly Orthopedic Patients
Authors Chen T ![]() , Lei X, Tian J, Mai H, Yu Y, Wu W, Wen L, Saw PE
, Lei X, Tian J, Mai H, Yu Y, Wu W, Wen L, Saw PE ![]() , Zhang M
, Zhang M
Received 7 February 2025
Accepted for publication 24 July 2025
Published 8 August 2025 Volume 2025:18 Pages 4859—4870
DOI https://doi.org/10.2147/JMDH.S519129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Tonghua Chen,1,* Xiaojun Lei,1,* Jingwei Tian,1,* Haochen Mai,1 Yuanfang Yu,1 Wenxia Wu,1 Liqiang Wen,1 Phei Er Saw,1 Meng Zhang1,2
1Department of General Practice, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China; 2Department of General Practice, Shenshan Medical Center, Sun Yat-sen Memorial Hospital, Shanwei, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Phei Er Saw; Meng Zhang, Email [email protected]; [email protected]
Purpose: To minimize the occurrence of acute thromboembolic events in elderly patients during the perioperative period and prevent adverse clinical outcomes, this study explores an efficient, and precise approach to the formulation of antithrombotic regimens under a multidisciplinary team (MDT) consultation model.
Patients and Methods: This single-center retrospective study included elderly patients on long-term antithrombotic therapy who underwent orthopedic surgery in our hospital between January 2019 and May 2023. Patients were divided into two groups: the MDT group and the non-MDT group. The incidence of thrombotic and bleeding-related adverse events during the perioperative period was observed and compared between the two groups.
Results: A total of 436 patients were enrolled, among whom 32 (7.3%) experienced thromboembolic adverse events. The incidence was significantly lower in the MDT group compared to the non-MDT group (3.3% vs 8.9%, P = 0.043). Logistic regression analysis identified several significant factors associated with thromboembolic adverse events, including: type of antithrombotic medication (OR=1.508, P=0.009) and postoperative ICU transfer (OR=6.390, P=0.029) were positively associated with thrombotic events; multidisciplinary team (OR=0.215, P=0.011) demonstrated a protective effect (negative association).
Conclusion: The multidisciplinary consultation model improves perioperative antithrombotic management strategies for elderly patients, contributing to a reduced incidence of thrombotic events in orthopedic surgeries for this population.
Keywords: elderly, antithrombotic therapy, perioperative period, multidisciplinary team, thrombotic adverse events
Introduction
With the intensification of the aging population trend, the demand for orthopedic surgery among the elderly has significantly increased. Timely surgical correction is crucial for maintaining function and improving quality of life.1 These patients have a high risk of thrombosis due to comorbidities such as cardiovascular disease, which is further exacerbated by postoperative immobilization and a hypercoagulable state. Cardiovascular and thromboembolic complications are common adverse events during the perioperative period for these patients, potentially leading to functional decline, extended hospital stays, and mortality.2 In patients without thromboprophylaxis, the risk of venous thromboembolism during and after orthopedic surgery is approximately 50–80%, with the risk persisting for up to 3–6 months post-surgery.3 Continuing preoperative antithrombotic regimens lead to perioperative bleeding, while suspending them undoubtedly raises the risk of perioperative myocardial and cerebral infarctions.4,5 Special attention is needed for the discontinuation, bridging, and resumption of antithrombotic medications in elderly during the perioperative period to improve the management of anticoagulant therapy and reduce the risk of thromboembolic and hemorrhagic complications.6
Current guidelines5,7 lack elderly-specific antithrombotic protocols and effective risk stratification tools to accurately assess both thromboembolic and bleeding risks in patients receiving antithrombotic therapy.8,9 Furthermore, single-discipline decision-making often fails to adequately balance thrombosis prevention against surgical bleeding risks. To minimize the occurrence of acute thrombotic or hemorrhagic events in the elderly during the perioperative period and prevent adverse clinical outcomes, it is recommended that a multidisciplinary team be convened to develop the most appropriate individualized antithrombotic treatment plan, including adjustments in medication dosages, bridging agents, and timing of resumption.10 Multidisciplinary consultation can integrate expertise and experience from various specialties to comprehensively assess the patient’s condition and surgical risks, thereby formulating a more scientific and rational antithrombotic management plan.
Most studies strongly support multidisciplinary consultation to optimize perioperative antithrombotic treatment for elderly patients.11 Perioperative antithrombotic management under a multidisciplinary model enables clinicians to effectively use precious medical resources, standardize the use of antithrombotic medications, and reduce the incidence and mortality rates related to surgical thrombosis and bleeding.12 Therefore, this study aims to explore whether a multidisciplinary consultation is beneficial in reducing the incidence of thrombotic and hemorrhagic events related to antithrombotic medications in the elderly during the perioperative period.
Research Methods
Data Sources
A retrospective analysis was conducted by retrieving data from the Sun Yat-sen Medical Research Data Repository and Electronic Medical Record System of our hospital. The study subjects were elderly patients who underwent orthopedic surgery between January 1, 2019, and May 1, 2023, and had regularly used antithrombotic medications prior to admission. This retrospective study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was reviewed and approved by the ethics committee of Sun Yat-sen Memorial Hospital (Ethics Approval Number: SYSKY-2023-457-01). As the study involved the use of anonymized data extracted from the hospital’s medical records system, the need for individual patient consent was waived by the ethics committee. All patient data were de-identified and handled confidentially to ensure the privacy and protection of patient information. The primary purpose of this study was to analyze and summarize the relevant data for research purposes, and no interventions or interactions with patients were conducted.
Inclusion criteria included (1) Age 60 years or older; (2) history of antithrombotic (including anticoagulant and antiplatelet) medication use; (3) underwent orthopedic surgery (including Joint replacement/revision, arthroscopic surgery, upper or lower limb fracture surgery, percutaneous spinal surgery, spinal surgery and local orthopedic surgery) during hospitalization. Exclusion criteria included patients (1) with malignant tumors; (2) with post-cardiac valve surgery; (3) users of warfarin medication; (4) with known bleeding disorders, coagulopathies, thrombocytopenia, chronic liver disease, or a history of recent major hemorrhage; (5) absence of complete medical history, disease history, personal history, or other key information in the medical record system.
Study Grouping
Patients were divided into a multidisciplinary team (MDT) group and a control group (Non-MDT) group. Patients in MDT group underwent two or more specialty consultations before the decision to discontinue antithrombotic medications, including anesthesiology, cardiology, neurology, vascular surgery, or pharmacy departments. MDT intervention addressed whether to stop antithrombotic medications, the timing of discontinuation, the need for bridging therapy and the type of bridging medication, and the timing for resuming antithrombotic therapy. Non-MDT group patients received preoperative antithrombotic management based on surgeons’ experience or conventional practice (all surgeons with ≥ 5-year experience).
Observational Indicators
Baseline demographics included age, gender, medical history, antithrombotic regimen, type of surgical procedure, and anesthesia type.
Primary outcomes included (1) rates of perioperative thrombotic events (including transient ischemic attacks /cerebral infarction, myocardial infarction, pulmonary embolism, deep vein thrombosis and Atrial fibrillation) and (2) bleeding events (including postoperative bleeding, gastrointestinal perforation, hypovolemic shock, hematuria, and other clinically relevant bleeding events). Secondary outcomes included (1) perioperative transfusion events; (2) length of hospital stay (LOS) and intensive care unit (ICU) admission rate following surgery; (3) medication management details (medication discontinuation, type of medication, bridging medication, and timing of medication resumption).
Statistical Description and Analysis
For quantitative data, if normally distributed, means ± standard deviations will be used for description; if not, medians will be used. Qualitative data will be described using numbers (percentages). Comparisons between the MDT group and the non-MDT group will involve independent sample t-tests for normally distributed quantitative data and non-parametric tests for non-normally distributed data. Qualitative data comparisons will be conducted using chi-square analysis. If the analysis of variance (ANOVA) indicates a statistically significant effect of a factor, post hoc pairwise comparisons using the Bonferroni correction are conducted to assess the differences among the factor’s levels. A logistic regression analysis was carried out to determine the independent risk factors of perioperative thrombotic events. The level of significance (α) is set at 0.05.
Results
Baseline Characteristics of the Study Population
Between January 1, 2019, and May 1, 2023, our hospital treated 6325 orthopedic patients aged 60 years and older, of which 601 had a regular history of antithrombotic medication use. After excluding 165 patients who did not undergo surgery, 436 patients were ultimately included in the study. The characteristics of the included patients are shown in Table 1. The overall average age of the study population was 73.67 ± 8.43 years, with a male to female ratio of 1:1.6. The patients were divided into MDT group and non-MDT group, with no significant differences between the groups in terms of gender, age, or anesthesia method used during surgery. However, there were statistically significant differences between the groups in terms of type of surgery (P=0.005), type of antithrombotic medication (P=0.004) and the number of underlying diseases (P<0.001). In MDT group, the population of coronary artery disease (P=0.046), arrhythmias (P=0.016), cerebral infarction (P=0.014), hypertension (P=0.030) and peripheral vascular disease (P<0.001) were more than those of non-MDT group. In pairwise comparisons of surgical types, the MDT group had a higher proportion of patients undergoing joint replacement/revision surgery compared to the non-MDT group (34.4% vs 24.5%, P=0.037); conversely, the MDT group showed fewer percutaneous lumbar procedures (5.7% vs 14.6%, P=0.011); and no significant differences were observed in other surgical categories. Regarding preoperative antithrombotic regimens, the MDT group demonstrated greater use of rivaroxaban (9.0% vs 3.8%, P=0.029) and dual antiplatelet therapy (10.7% vs 5.1%, P=0.036). However, aspirin monotherapy was less frequently prescribed in the MDT group (37.7% vs 53.2%, P=0.04).
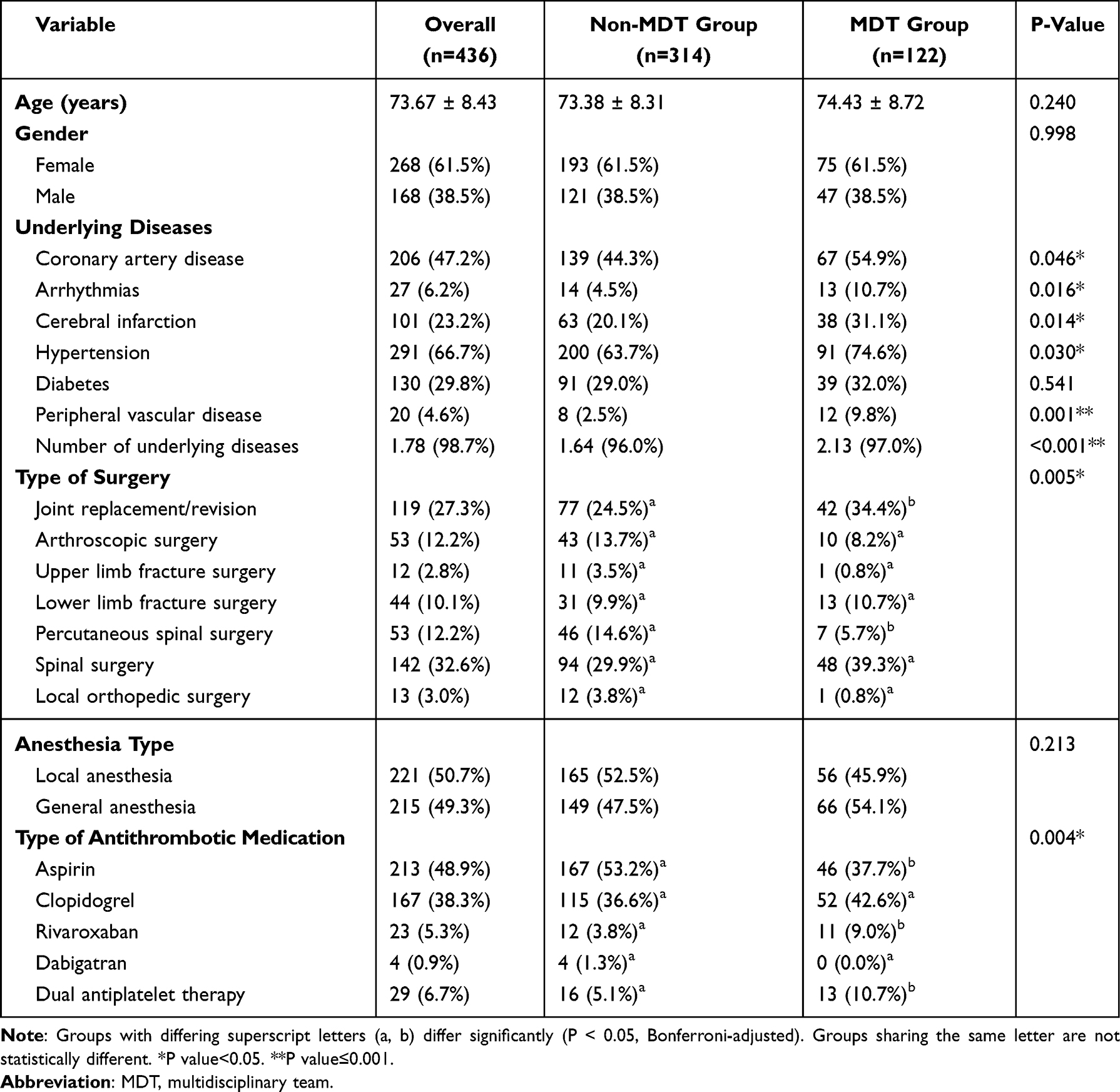 |
Table 1 General Characteristics of the Overall Study Population, MDT Group, and Non-MDT Group |
Perioperative Antithrombotic Medication Usage
The detailed perioperative management of antithrombotic drug discontinuation and resumption for all patients is presented in Table 2. The MDT group demonstrated significantly higher rates than the non-MDT group in postoperative antithrombotic therapy resumption (64.8% vs 44.6%, P=0.001), preoperative intravenous anticoagulation bridging (75.4% vs 45.9%, P<0.001), postoperative intravenous anticoagulation bridging (69.7% vs 48.1%, P<0.001), perioperative anticoagulation bridging (86.1% vs 61.8%, P<0.001) and reminder to resume antithrombotic therapy at discharge (50.0% vs 29.6%, P<0.001). The MDT group also had significantly longer bridging durations: preoperative (4.80 ± 4.24 vs 2.12 ± 2.83 days, P<0.001), postoperative (5.44 ± 5.06 vs 4.00 ± 5.30 days, P=0.010) and total (10.34 ± 7.04 vs 6.12 ± 6.69 days, P<0.001). Additionally, significant intergroup differences existed in postoperative antithrombotic regimen adjustments (P=0.003). The number of patients in the MDT group who were transferred to ICU after surgery was higher than that in the non-MDT group (5.7% vs 1.3%, P=0.008), and the length of hospital stay in the former group was significantly longer than that in the latter group (16.5± 11.51 vs 13.85± 8.45, P=0.009).
 |
Table 2 Perioperative Antithrombotic Medication Management Among Overall Population, Non-MDT Group, and MDT Group |
Incidence of Perioperative Thrombotic and Bleeding Adverse Events
The incidence of perioperative thrombotic and bleeding adverse events among the 436 patients is presented in Table 3. In total, 32 patients (7.3%) experienced adverse thrombotic events, with the MDT group showing a significantly lower rate of these events compared to the non-MDT group (P=0.043, 3.3% vs 8.9%). In the non-MDT group, 3 patients experienced TIA or cerebral infarction (1.0%), 13 had myocardial infarction (4.1%), 3 developed pulmonary embolism (1.0%), 6 presented with deep vein thrombosis (1.9%), and 3 exhibited atrial fibrillation (1.0%). However, the MDT group demonstrated single occurrences (0.8%) of each complication: transient ischemic attack or stroke, myocardial infarction, deep venous thrombosis and atrial fibrillation. There were no statistically significant differences between the groups in terms of postoperative bleeding events and perioperative transfusion incidents.
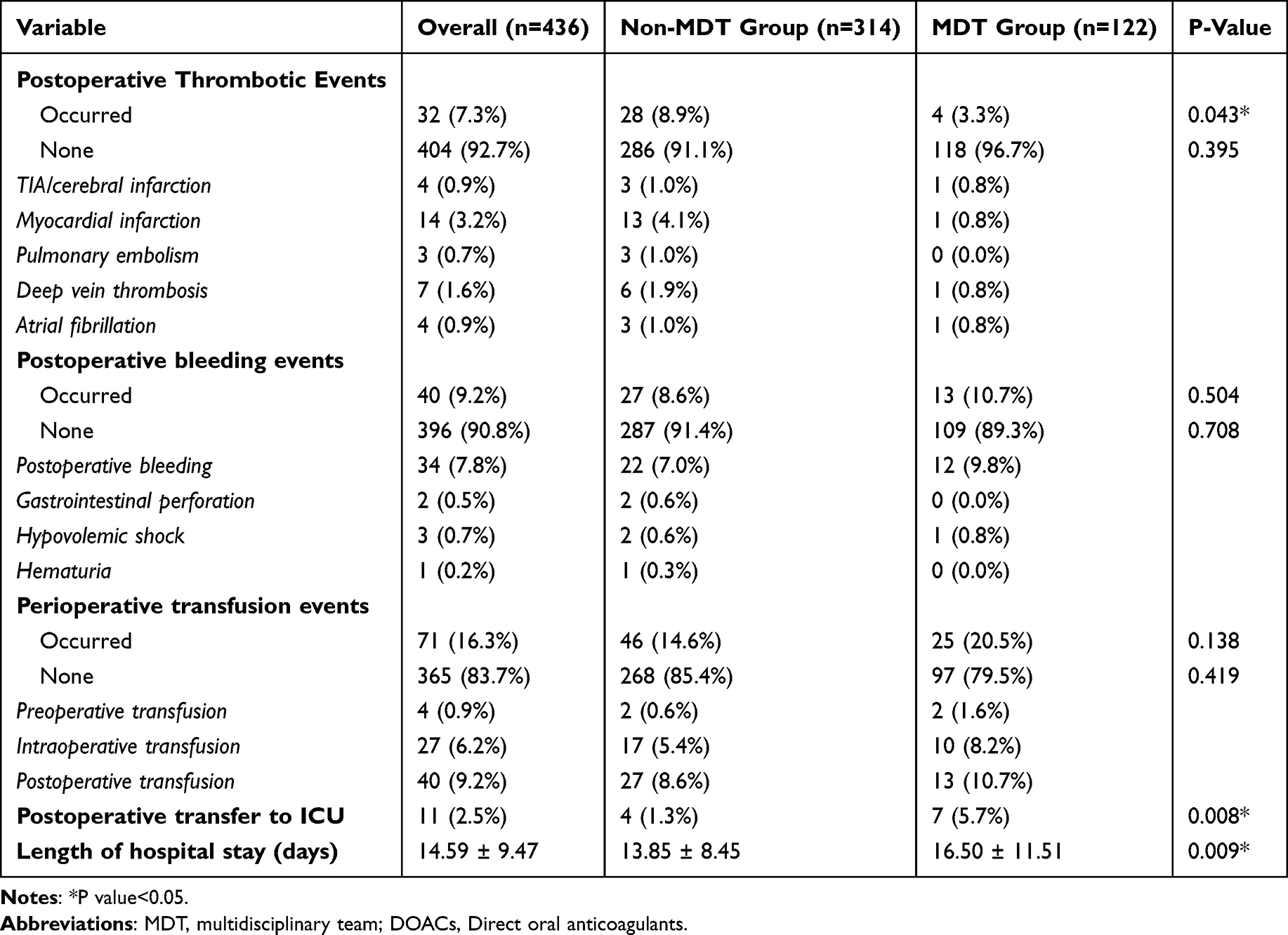 |
Table 3 Incidence of Perioperative Thrombotic and Bleeding Adverse Events |
Independent Risk Factors for Thrombotic Adverse Events and Logistic Analysis
We defined the Thrombosis group as patients with postoperative thrombotic events, and the non-Thrombosis group as those without these events. Table 4 presents the univariate analysis results, identifying the following as risk factors for postoperative thrombotic events: type of Antithrombotic Medication (P=0.026), multidisciplinary team involvement (P=0.043), postoperative resumption of antithrombotics (P=0.013), type of anticoagulant initiated postoperatively (P=0.002), anticoagulant bridging during perioperative period (P=0.046), adjustment of postoperative antithrombotic medication (P=0.026), days of postoperative anticoagulant initiation (P=0.010), total bridging days (P=0.005), perioperative transfusion (P<0.001) and postoperative transfer to ICU (P=0.010). A binary logistic regression analysis (Enter method) was performed to evaluate the impact of these factors (including all variables with P<0.1 in univariate analysis) on thrombotic adverse events (see Table 5). The final model incorporated three significant predictors: type of antithrombotic medication (OR=1.508, P=0.009) and postoperative ICU transfer (OR=6.390, P=0.029) were positively associated with thrombotic events; multidisciplinary team (OR=0.215, P=0.011) demonstrated a protective effect (negative association). Subgroup analysis of antithrombotic regimens revealed the thrombotic group had a higher proportion of patients on dual antiplatelet therapy preoperatively (18.8% vs 5.7% in non-thrombotic group, P=0.004). Conversely, aspirin monotherapy was less frequent in the thrombotic group (31.3% vs 50.2% in non-thrombotic group, P=0.038). The number of patients in the Thrombotic group who were transferred to ICU after surgery was higher than that in the non-Thrombotic group (9.4% vs 2.0%, P=0.010), and the two groups showed no significant difference in length of hospitalization (P= 0.151).
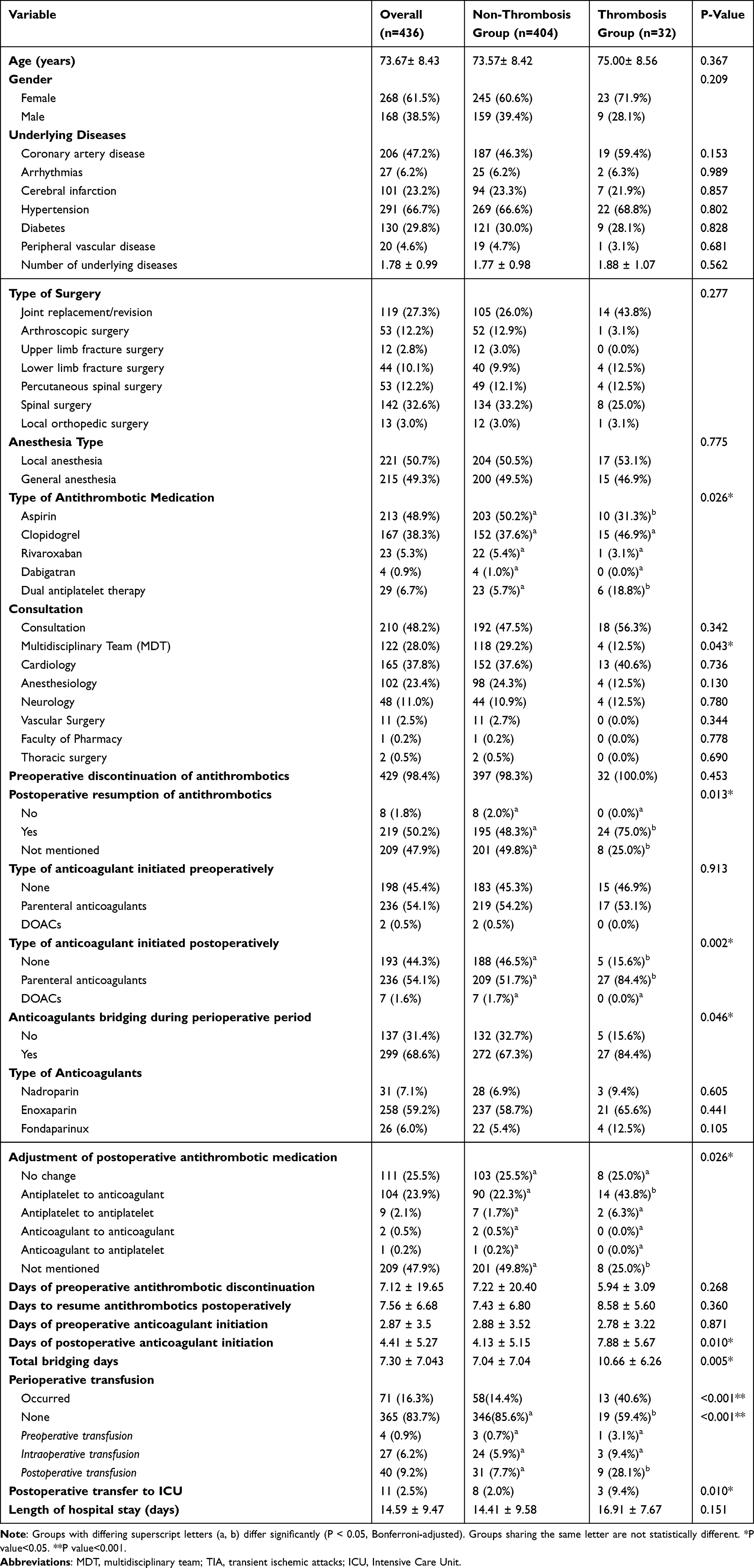 |
Table 4 Comparison of Characteristics Between Thrombosis Group and Non-Thrombosis Group |
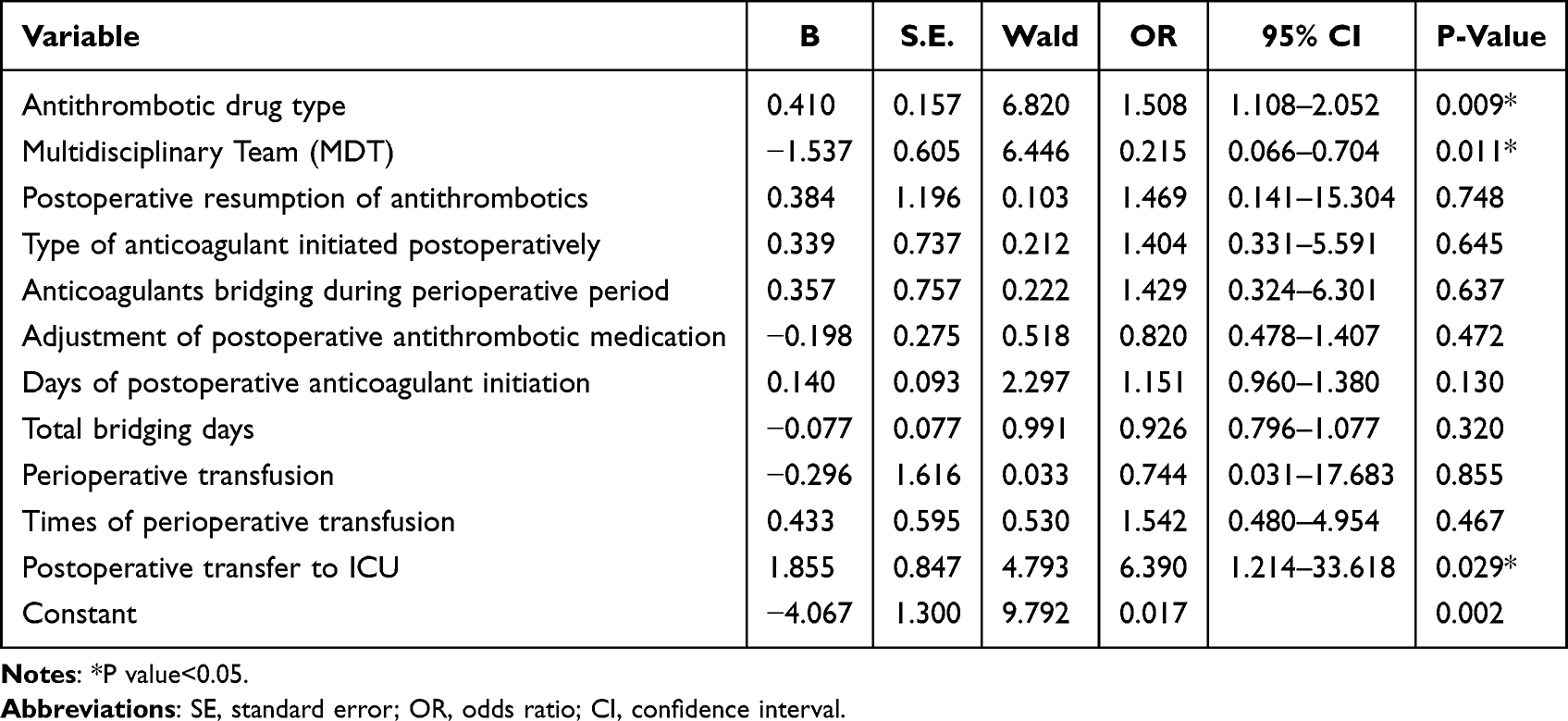 |
Table 5 Independent Risk Factors for Thrombotic Adverse Events in Logistic Analysis |
Discussion
With the incidence rate of cardiovascular diseases increasing year by year, more and more elderly people need to use antithrombotic drugs for a long time to prevent major adverse cardiovascular and cerebrovascular events.13 For elderly patients who have received antithrombotic therapy but require surgery, continuing to take antithrombotic drugs increases the risk of surgical bleeding, while discontinuing the medication increases the occurrence of adverse thrombotic events. In addition, the risk of other complications, such as bleeding risk, should also be considered.14 However, there are currently no detailed and specific recommendations for perioperative antithrombotic management in elderly patients.15 The ‘Guidelines for Prevention of Venous Thromboembolism in Chinese Orthopedic Surgery’16 proposes the concept of deepening comprehensive perioperative treatment. Orthopedic surgeons assess surgical approaches and recovery time; cardiologists and neurologists evaluate stroke risks post-antithrombotic treatment; and departments of hematology, vascular surgery, and pharmacy guide medication dosage and bridging. MDT optimizes and integrates existing medical resources to provide patients with the best diagnosis and treatment decisions, becoming an important guarantee for perioperative management of elderly patients17 At present, multiple orthopedic hospitals in China have applied multidisciplinary collaboration to the diagnosis and treatment of elderly patients in orthopedics,18,19 but there is little precise adjustment of antithrombotic drugs, and they have still not been widely applied in orthopedic clinical practice.20 In our study, we found that MDT can assess patients’ risks of thrombosis and bleeding, decide whether to interrupt anticoagulation therapy or apply a bridging strategy during the perioperative period, and devise personalized perioperative antithrombotic medication management plans for elderly patients to minimize perioperative risks.21,22 It can also monitor postoperative coagulation function and bleeding status, adjusting treatment plans promptly to ensure patient safety.23
This study found that despite comprising a higher proportion of patients at elevated thrombotic risk (eg, those undergoing joint replacement/revision surgery, with more comorbidities, or receiving rivaroxaban/dual antiplatelet therapy), the MDT group demonstrated a significantly lower incidence of thrombotic events (3.3% vs 8.9%, P=0.043). Furthermore, the MDT group showed statistically superior performance in multiple key aspects of antithrombotic management compared to the non-MDT group, including: postoperative resumption of antithrombotic therapy, perioperative intravenous anticoagulation bridging (both pre- and postoperatively), duration of bridging anticoagulation and adjustment of postoperative antithrombotic regimens. This suggests that multidisciplinary antithrombotic management enhances the creation of personalized perioperative antithrombotic medication plans for elderly patients, improving medication appropriateness during the perioperative period.
Concurrently, this study identified preoperative antithrombotic medication type and postoperative ICU admission as independent risk factors for thrombotic adverse events in elderly orthopedic patients. Specifically, dual antiplatelet therapy increased the risk by 50.8% (OR=1.508), while patients requiring ICU transfer demonstrated a 6.39-fold higher risk (OR=6.390). Notably, multidisciplinary team (MDT) consultation significantly reduced thrombosis risk (OR=0.215), exhibiting particularly strong protective effects for high-risk patients receiving complex antithrombotic regimens like dual antiplatelet therapy. These findings suggest that clinical practice should prioritize implementing MDT management protocols to optimize anticoagulation strategies for patients either on preoperative dual antiplatelet therapy or those anticipated to require postoperative ICU care.
Multidisciplinary consultation effectively reduces postoperative thrombotic events such as pulmonary embolism, myocardial infarction, and deep vein thrombosis. Similarly, a prospective, multicenter study demonstrated that MDTs significantly decrease complications related to anticoagulant use, reducing both bleeding and thrombotic events within three months post-discharge.24 Hu et al25 applied a multidisciplinary thrombosis prevention model, mainly by enhancing patient awareness, strengthening rehabilitation exercises, physical thrombosis prevention, and early management of venous thromboembolism in orthopedic patients, and found that this model significantly reduced the overall incidence of venous thromboembolism to 6.56%, with no postoperative fatal pulmonary embolism occurring.25 Wang et al found that a multidisciplinary medical-nursing collaboration model (led by orthopedics, supported by internal medicine, and enhanced by surgical nursing) resulted in significantly lower incidence rates of respiratory, cardiovascular, cerebrovascular diseases, and lower limb deep vein thrombosis compared to the control group.26 The primary goal of implementing a multidisciplinary antithrombotic management plan is to enhance patient-centered outcomes by significantly reducing complications associated with anticoagulation. Utilizing a multidisciplinary approach in perioperative antithrombotic management ensures the efficient use of medical resources, standardizes antithrombotic medication protocols, and decreases both the incidence and mortality from surgical thrombosis and bleeding.12 Current research, both domestic and international, generally involves forming MDT teams led by orthopedic physicians, from admission to discharge, to create personalized diagnostic and treatment plans focused more on perioperative chronic disease management and surgical care.27–29 This study pointed to the importance of MDT in reducing postoperative thrombotic adverse events through the management of perioperative antithrombotic medications in elderly patients.
These findings provide robust validation of established clinical consensus: for high-risk patient populations undergoing major orthopedic procedures, particularly those with multiple comorbidities or receiving potent antithrombotic medications, the multidisciplinary team (MDT) approach - incorporating comprehensive evaluations by anesthesiologists, cardiologists, and clinical pharmacists - demonstrates significant advantages in optimizing perioperative anticoagulation strategies. This collaborative model not only effectively reduces postoperative thrombosis incidence but also maintains a favorable safety profile without substantially increasing bleeding risks. The results offer compelling real-world evidence supporting the MDT recommendations outlined in the Chinese Guideline for Prevention of Venous Thromboembolism in Major Orthopedic Surgery. Although the MDT group demonstrated prolonged hospitalization durations and higher ICU admission rates, these outcomes likely reflect appropriate intensive monitoring for high-risk patients rather than clinical inefficiency, particularly given the superior clinical outcomes observed. Notably, this vigilant monitoring protocol potentially contributed to the prevention of recurrent thrombotic events in our study cohort (No recurrent thrombotic events were observed in our study).
This study demonstrates that the multidisciplinary consultation model significantly improved the management of perioperative antithrombotic medications, providing personalized guidance to patients both before and after surgery. Research on perioperative antithrombotic medication use in patients with chronic orthopedic conditions revealed several real-world problems, such as inappropriate preoperative planning, incorrect timing for discontinuing and resuming medications, failure to resume medications postoperatively, improper bridging techniques, and inappropriate use of low-molecular-weight heparins.30 Managing perioperative antithrombotic medications is complex, with risks of adverse reactions like bleeding and thrombosis. Effective management requires personalized patient assessments within a standardized, systematic framework, a thorough understanding of antithrombotic pharmacodynamics, and collaborative multidisciplinary efforts.31 Implementing a multidisciplinary collaborative model leads to better treatment and management outcomes for elderly patients with fractures, allowing for more rational and effective use of medical resources.32
In our study, we also found that the MDT model significantly increased the number of patients reminded to resume antithrombotic therapy post-discharge compared to the control group, promoting standardized use of antithrombotic drugs and enhancing perioperative antithrombotic awareness among cardiovascular disease patients. The MDT approach improves the quality of orthopedic surgery management,17 tailoring treatment plans for patients with various conditions and needs, actively improving patient outcomes, and standardizing orthopedic diagnostic and treatment strategies while optimizing the overall allocation of medical resources. MDT not only focuses on the surgical outcomes but also emphasizes the overall treatment effects and quality of life for patients. By conducting comprehensive evaluations of patients’ health statuses and surgical risks, personalized treatment plans are developed, which help increase the success rates of surgeries and patient satisfaction. Furthermore, MDT provides postoperative rehabilitation guidance and follow-up management, aiding patients in better recovery of physical functions and enhancing their quality of life. Importantly, MDT leverages the expertise and experience from various disciplines to offer a one-stop, comprehensive service, which improves the efficiency and quality of medical services.33
However, this study has limitations: (1) As a retrospective analysis, missing data on comorbidities and medication histories in some cases may have introduced potential selection bias. Although we performed multivariate adjustments in our study, residual confounding factors may persist. Additionally, potential selection bias could exist in the allocation of MDT interventions. (2) The single-center design limits external validity, and the observed incidence rates may not accurately represent all elderly orthopedic patients. (3) We did not document postoperative wound assessments, wound-related complications, 30-day readmission rates and etc. These factors could influence anticoagulation regimen adjustments and potentially lead to underestimation of adverse events. (4) The lack of cost-effectiveness analysis warrants attention when considering widespread MDT model implementation. (5) The absence of long-term follow-up precludes comprehensive understanding of post-thrombosis outcomes. In future studies, we will expand the sample size, extend follow-up duration, and conduct prospective cohort research to further investigate the impact of multidisciplinary management on perioperative thrombotic and bleeding events.
Conclusion
This study rigorously evaluates the application of perioperative antithrombotic medications in elderly patients at a tertiary hospital, aiming to enhance clinical awareness and application of these critical interventions. By assessing clinical outcomes, including adverse thrombotic events, between groups managed with and without a MDT approach, the research highlights the benefits of MDT in the perioperative management of elderly patients. The findings clearly demonstrate that the MDT model significantly reduces adverse thrombotic events by enabling targeted and precise adjustments to antithrombotic therapies. Furthermore, this study establishes a foundation for future research, which should focus on broadening the evidence base through larger sample sizes, extended follow-up periods, and the implementation of prospective cohort studies. These efforts will provide deeper insights into the effectiveness of multidisciplinary management in mitigating perioperative thrombosis and bleeding risks, ultimately improving patient outcomes in complex clinical settings.
Acknowledgments
This study was supported by Guangdong Medical Science and Technology Research Fund (Grant Number: C2023050).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Onizuka N, Quatman C. Global barriers to Hip-fracture care. Lancet Healthy Longev. 2024;5(8):e510–e511.
2. Ho HH, Lau TW, Leung F, Tse HF, Siu CW. Peri-operative management of anti-platelet agents and anti-thrombotic agents in geriatric patients undergoing semi-urgent Hip fracture surgery. Osteoporos Int. 2010;21(Suppl 4):S573–7. doi:10.1007/s00198-010-1416-x
3. Lippi G, Cervellin G. Lippi G,Cervellin G.Aspirin for thromboprophylaxis in major orthopedic surgery: old drug, new tricks? Acta Biomed. 2018;89(1):31–33. doi:10.23750/abm.v89i1.7121
4. W Qin, Lu C, Shuai Z. Safety analysis of continuation of antithrombotic agents in patients with moderate or high thromboembolic risk undergoing Lichtenstein surgery during perioperative period. Chinese J of General Sur. 2022;4(31):490–496.
5. Csctva NSAB, Cccp CCOC, Cca CCA. Multidisciplinary Expert Consensus on Perioperative Management of Antithrombotic Drugs. Nat Med J China. 2020;39(100):3058–3074.
6. Al-Nasser B. Anticoagulant conversion in the elderly: pitfalls. J Clin Anesth. 2016;30:87–89. doi:10.1016/j.jclinane.2015.10.001
7. Association SBOS, Association CDBO, Association ABOS. Shanghai Expert Consensus on Perioperative Management of Patients Undergoing Non-Cardiac Surgery with Antithrombotic Therapy (2021 Edition). Chinese J Pract Sur. 2021;6(41):7.
8. Douketis JD, Spyropoulos AC, Spencer FA, et al. Perioperative management of antithrombotic therapy: antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e326S–e350S. doi:10.1378/chest.11-2298
9. Jaffer AK, Brotman DJ, Chukwumerije N. When patients on warfarin need surgery. Cleve Clin J Med. 2003;70(11):973–984. doi:10.3949/ccjm.70.11.973
10. Falck-Ytter Y, Francis CW, Johanson NA, et al. Prevention of VTE in orthopedic surgery patients: antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e278S–e325S.
11. Korte W, Cattaneo M, Chassot PG, et al. Peri-operative management of antiplatelet therapy in patients with coronary artery disease: joint position paper by members of the working group on Perioperative Haemostasis of the Society on Thrombosis and Haemostasis Research (GTH), the working group on Perioperative Coagulation of the Austrian Society for Anesthesiology, Resuscitation and Intensive Care (OGARI) and the Working Group Thrombosis of the European Society for Cardiology (ESC). Thromb Haemost. 2011;105(5):743–749. doi:10.1160/TH10-04-0217
12. Porres-Aguilar M, Ansell J, Mukherjee D, et al. Impact of Hospital-based Multidisciplinary Anticoagulation Stewardship Programs. Arch Med Res. 2023;54(1):1–6. doi:10.1016/j.arcmed.2022.11.016
13. Luepker RV, Steffen LM, Duval S, et al. Population Trends in Aspirin Use for Cardiovascular Disease Prevention 1980-2009: the Minnesota Heart Survey. J Am Heart Assoc. 2015;4(12). doi:10.1161/JAHA.115.002320.
14. Majeed A, Goldhaber SZ, Kakkar A, et al. Bleeding events with dabigatran or warfarin in patients with venous thromboembolism. Thromb Haemost. 2016;115(2):291–298. doi:10.1160/th15-04-0319
15. Douketis JD, Spyropoulos AC, Murad MH, et al. Executive Summary: perioperative Management of Antithrombotic Therapy: an American College of Chest Physicians Clinical Practice Guideline. Chest. 2022;162(5):1127–1139.
16. Xiaomeng W, Yingzhen N, Gang J. The interpretation of the guide for the prevention of venous thromboembolism with major orthopaedic surgery in China. Chin J Orthopaedics. 2017;10(37):636–640.
17. Baroni M, Serra R, Boccardi V, et al. The orthogeriatric comanagement improves clinical outcomes of Hip fracture in older adults. Osteoporos Int. 2019;30(4):907–916. doi:10.1007/s00198-019-04858-2
18. Rui Y, Qiu X, Zou J, et al. Clinical application of multidisciplinary team co-management in geriatric Hip fractures. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2019;33(10):1276–1282. doi:10.7507/1002-1892.201905017
19. Zhenwei W, Di A, Teng Z. Multidisciplinary team for treatment of Hip fracture in the elderly. Chin J Orthopaedic Trauma. 2020;3(22):6.
20. Yingjie N, Yunfeng R, Jianyue W. Application of Multidisciplinary Collaboration Diagnosis and Treatment in the Construction of Green Channel for Perioperative Period of Geriatric Hip Fracture. Chin J Bone Joint Injury. 2022;008:037.
21. Meloni M, Giurato L, Monge L, et al. Effect of a multidisciplinary team approach in patients with diabetic foot ulcers on major adverse limb events (MALEs): systematic review and meta-analysis for the development of the Italian guidelines for the treatment of diabetic foot syndrome. Acta Diabetol. 2024;61(5):543–553. doi:10.1007/s00592-024-02246-9
22. Lu Q, Bi Z, Tian Y, et al. Application study of multidisciplinary collaboration (MDT) integrated management model in perioperative management of patients with infectious nonunion. Front Surg. 2024;11:1335157. doi:10.3389/fsurg.2024.1335157
23. Dreijer AR, Kruip MJ, Diepstraten J, et al. Antithrombotic stewardship: a multidisciplinary team approach towards improving antithrombotic therapy outcomes during and after hospitalisation: a study protocol. BMJ Open. 2016;6(12):e011537. doi:10.1136/bmjopen-2016-011537
24. Dreijer AR, Kruip M, Diepstraten J, et al. Effect of antithrombotic stewardship on the efficacy and safety of antithrombotic therapy during and after hospitalization. PLoS One. 2020;15(6):e0235048. doi:10.1371/journal.pone.0235048
25. H BIN, Yawei L, Xingwen X. Application of Multidisciplinary Thrombosis Prevention and Treatment Model in Geriatric Unicompartmental Knee Replacement. Chin J Bone Joint Injury. 2020;8(35):3.
26. Wang C, Chang Y, Zheng Y, et al. Application of multidisciplinary doctor-nurse collaboration team on the perioperative management of geriatric Hip fractures. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2019;33(10):1283–1286. doi:10.7507/1002-1892.201805068
27. Gosch M, Hoffmann-Weltin Y, Roth T, et al. Orthogeriatric co-management improves the outcome of long-term care residents with fragility fractures. Arch Orthop Trauma Surg. 2016;136(10):1403–1409. doi:10.1007/s00402-016-2543-4
28. Walke LM, Rosenthal RA, Trentalange M, et al. Restructuring care for older adults undergoing surgery: preliminary data from the Co-Management of Older Operative Patients En Route Across Treatment Environments (CO-OPERATE) model of care. J Am Geriatr Soc. 2014;62(11):2185–2190. doi:10.1111/jgs.13098
29. Fairhall N, Sherrington C, Lord SR, et al. Effect of a multifactorial, interdisciplinary intervention on risk factors for falls and fall rate in frail older people: a randomised controlled trial. Age Ageing. 2014;43(5):616–622. doi:10.1093/ageing/aft204
30. Borui T, Zihui W, Huaguang W. Rationality Evaluation of Perioperative Antithrombotic Therapy in Orthopedic Patients with Long-term Use of Antiplatelet Drugs. Chinese J Pharmacoepidemiol. 2021;7(30):5.
31. Burnett AE, Ragheb B, Kaatz S. Perioperative consultative hematology: can you clear my patient for a procedure? Hematology Am Soc Hematol Educ Program. Hematology Am Soc Hematol Educ Program. 2022;2022(1):723. doi:10.1182/hematology.2022E01
32. Roberts HJ, Rogers SE, Ward DT, Kandemir U. Protocol-based interdisciplinary co-management for Hip fracture care: 3 years of experience at an academic medical center. Arch Orthop Trauma Surg. 2022;142(7):1491–1497. doi:10.1007/s00402-020-03699-7
33. Wu F, Hao X, Su J, Cao B. Efficacy Study of Multidisciplinary Team Participating in the Perioperative Administration for Elderly Patients With Intertrochanteric Fractures: a Prospective Randomized Controlled Trail. J Am Acad Orthop Surg. 2023;31(12):e540–e549. doi:10.5435/JAAOS-D-22-00929
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.