")
Back to Journals » Research and Reports in Urology » Volume 10
Mature teratoma of the bladder in adolescence: a case report and literature review
Authors Prihadi JC, Kusumajaya C
Received 8 March 2018
Accepted for publication 30 April 2018
Published 22 June 2018 Volume 2018:10 Pages 39—42
DOI https://doi.org/10.2147/RRU.S167683
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
Johannes Cansius Prihadi, Christopher Kusumajaya
Department of Surgery, Division of Urology, Faculty of Medicine, Atma Jaya Catholic University, Jakarta, Indonesia
Background: Teratomas are tumors consisting of two or three germ layers, seen commonly during childhood. Teratomas have been reported to occur in various sites and organs. Bladder teratoma is a very rare extragonadal tumor, moreover in adults. Although teratomas are known as benign lesions in childhood, they may act as malignant tumors when detected during adulthood. This requires total tumor resection, particularly in adult cases, and the addition of radiotherapy and chemotherapy in cases with the potential of malignancy.
Case presentation: A very rare case of teratoma of the bladder in a 17-year old Asian girl is presented. The patient had chief complaints of hematuria. The diagnosis was made on cystoscopy and confirmed histopathologically. Complete excision was possible. To the authors’ knowledge, this is the first such case reported from Indonesia and the South East Asian region.
Conclusion: A bladder teratoma mimics the presentation of a bladder stone, clinically and radiologically. A dermoid cyst should be considered as a differential diagnosis, especially when the stone appears to be confined to the bladder wall during examination.
Keywords: adolescence, bladder, teratoma, vesical
Introduction
Teratoma is a type I germ cell tumor, according to clinical presentation, pathology, and cytogenetics, just like yolk sac tumors, and is more frequent in extragonadal sites, especially in the midline and para-axial location; most of them are in the ovaries.1,2 Teratomas are considered as developmental anomalies, derived from all three primitive layers of the embryo. They may include elements of bone, cartilage, teeth, hair, and squamous epithelium (a fact that most likely explains the name teratoma, which roughly means “monster tumor” in Greek).3–5
Teratomas can cause various complications after growing to a significant size, according to the occupying organ, but they are primarily asymptomatic. Bladder teratomas have clinical manifestations ranging from irritative lower urinary tract symptoms up to urinary retention. They are usually found incidentally, during clinical examination, imaging studies, or nonrelated abdominal operations.4 The gross appearance of teratoma depends largely on the elements within it, with most tumors having solid and cystic areas.5,6 Teratomas are generally associated with normal serum tumor markers, but may cause mildly elevated serum alpha fetoprotein (AFP) levels.5
Teratomas are not infiltrative tumors, but are expansive. The primary approach is total removal of the tumor, other alternatives are radiotherapy and chemotherapy for the tumors that show malignant character.6 Primary urinary bladder germ cell tumors are exceedingly rare, this is the first case reported in Indonesia. We present here a case of a teratoma in the urinary bladder that was found in a 17-year-old girl.
Case report
A 17-year-old girl complained of episodes of gross hematuria and dysuria for the past 3 years. She had no other genitourinary or bowel complaints. There was no relevant past medical history of ovulation induction, nor any family history of ovarian or breast malignancies. She previously had a computed tomography (CT) scan and was diagnosed with cystitis and vesicolithiasis.
No remarkable findings were seen on physical examination. The clinical, routine blood and urine examinations were within normal limits, as well as all other routine laboratory work up. CT showed a well-defined lesion in the urinary bladder measuring 3.5×2.5×6 cm3, showing variegated attenuation of fat, soft tissue, and bone (Figure 1).
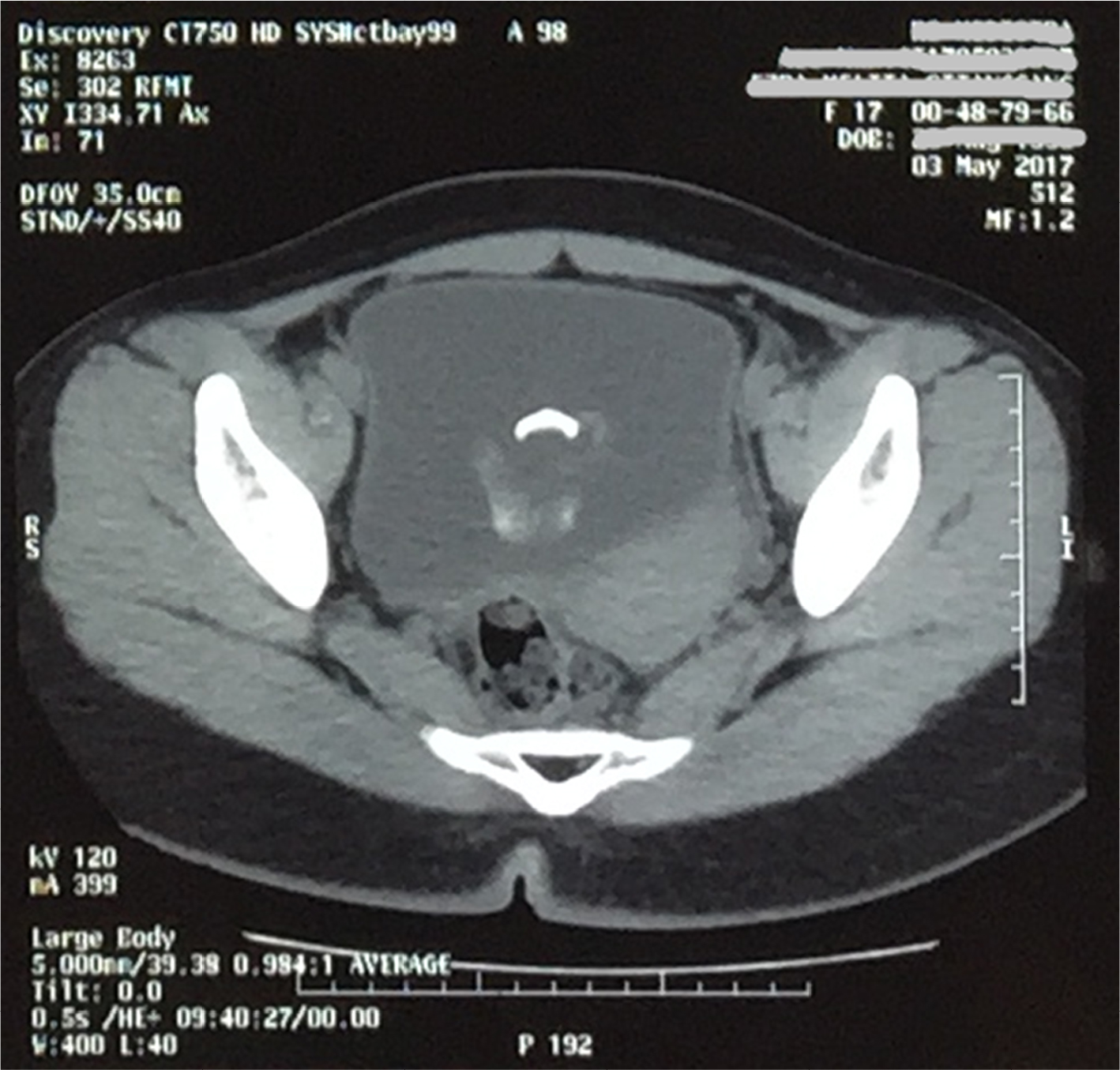 | Figure 1 CT scan showing a mass mimicking a stone in the bladder. Abbreviation: CT, computed tomography. |
The patient was hospitalized and planned for a cystoscopy and lithotripsy. Cystoscopy showed a calcified stone-like mass arising from the dome of the urinary bladder, with multiple hairs and debris projecting from it (Figure 2). A sample was taken for histopathology examination. The histopathology report showed a benign mature teratoma with ectodermal, mesodermal, and endodermal elements (Figure 3). The teratoma was reported to be confined to the bladder wall, with no extension outside. The patient was discharged and planned for surgical excision. Right now, the patient is symptom free and waiting to decide about the surgical excision.
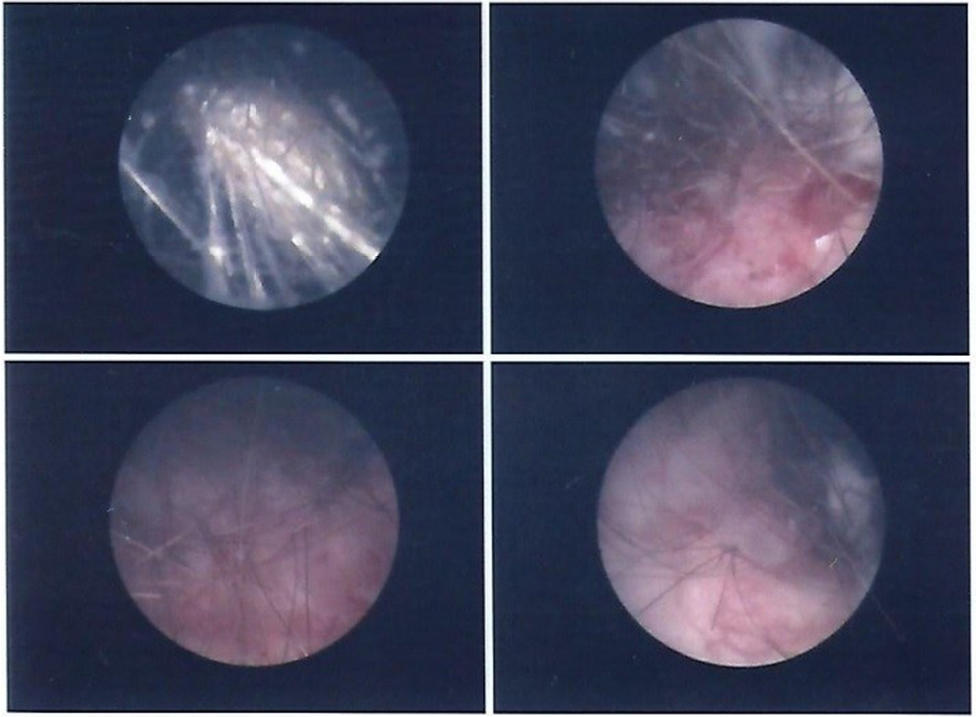 | Figure 2 Cystoscopy findings. |
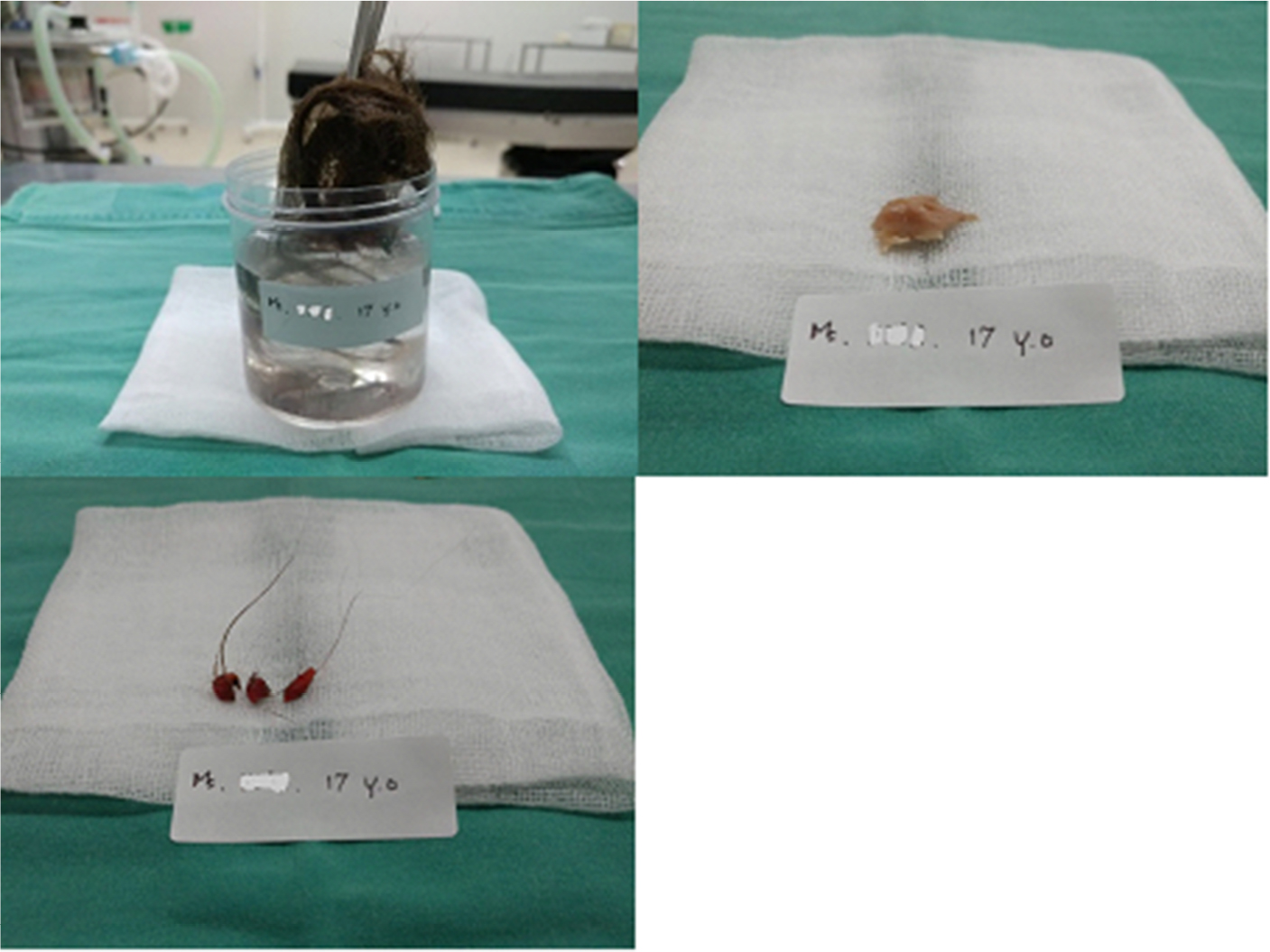 | Figure 3 (A) Hair, (B) teeth, and (C) biopsy sample taken during the cystoscopy. |
Discussion
Dermoid cysts or teratomas are the most nebulous and controversial member of germ cell tumors. The parthenogenetic theory, which suggests an origin from a primordial germ cell, is now the accepted pathogenesis theory.2,4 Well-differentiated tumors are benign and labeled mature teratomas.4,6 Teratomas are commonly found in pediatric subjects, arising from various sites, mostly sacrococcygeal and ovarian. Pilimiction, the passage of hair in urine, is a pathognomonic sign of urinary bladder dermoid.7 Our case is a 17-year-old girl with a bladder teratoma and a chief complaint of hematuria, which is a very rare entity and, therefore, can pose a diagnostic problem.
Imaging showed a mass, and it’s correlation with the adjacent viscera can help to identify any associated complications.4 CT and magnetic resonance (MR) imaging is fairly straightforward, as these modalities are more sensitive in the detection of fat attenuation within a cyst and calcifications of the wall.4 However, in our case, the CT findings showed a mass mimicking a stone in the bladder and, therefore, the typical cystoscopy findings help the diagnosis.
Midline teratomas, along the embryonic fusion lines, resulted from abnormal germ cells when the neural tube closes at about the 3rd to 5th week of embryonic life.2 The midline position of the bladder mass in this patient was suggestive of a dermoid cyst. The histopathological findings (Figure 4) confirmed skin, adnexal structures (sweat glands, hair follicles), adipose, and fibroblastic tissue, which were consistent with those of a dermoid cyst. Transurethral resection of the mass has been reported for choice of treatment,3 but surgical excision of the lesion with a 1 cm rim of normal bladder mucosa and bladder repair is the definitive treatment.2,5
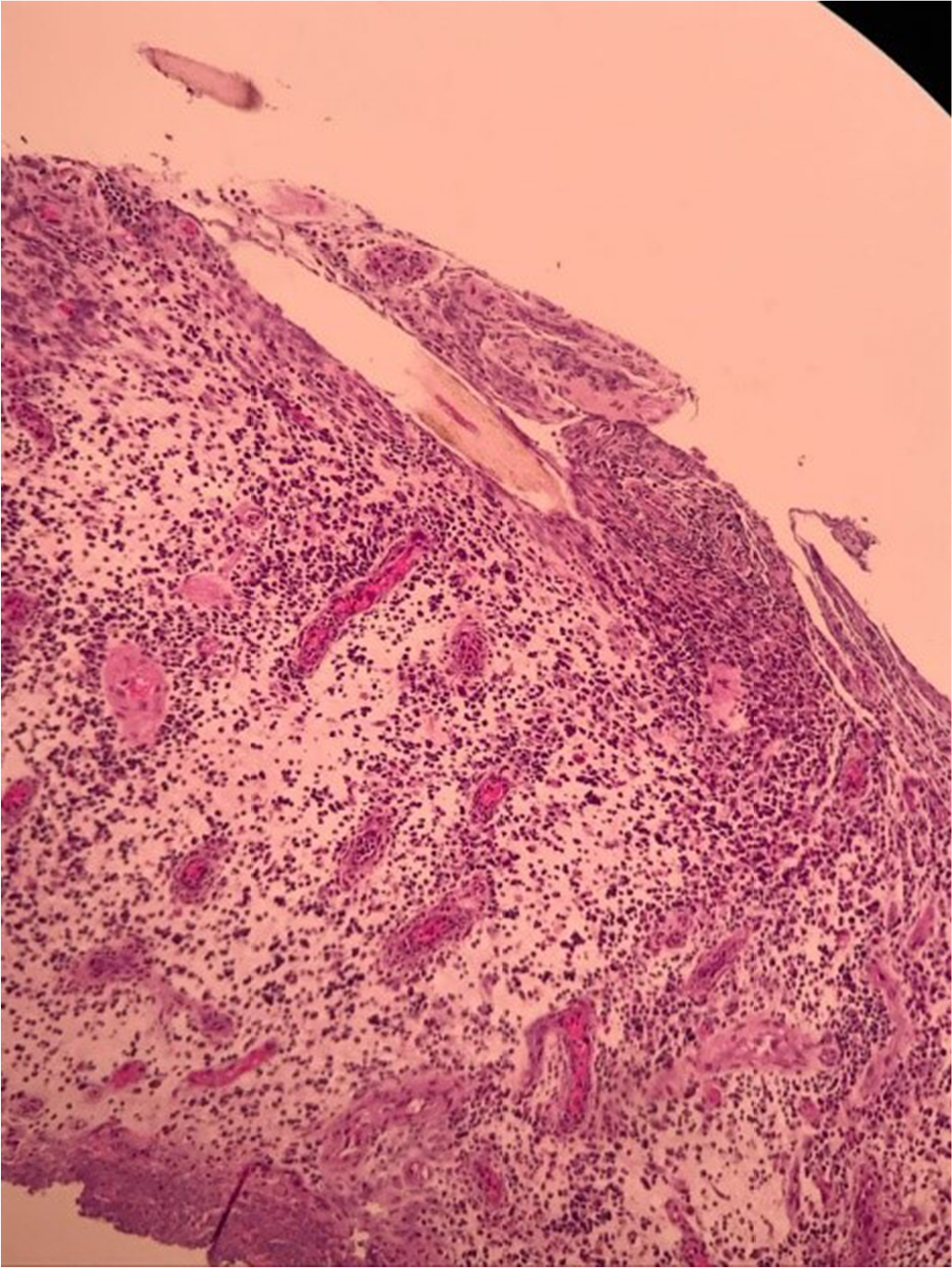 | Figure 4 Hair root, stromal edema background with acute and chronic inflammatory cells accompanied by small congestive blood vessel proliferation. |
A bladder teratoma can mimic the presentation of a bladder stone, clinically and radiologically. A dermoid cyst should be considered as a differential diagnosis, especially when the stone appears to be confined to the bladder wall during examination. The author hopes that the case report presented here has communicated some of the issues and concerns associated with teratoma in urinary bladder that are found in adults.
Acknowledgments
The authors sincerely acknowledge the advisers, Dr Yanto Budiman, Radiologist of Atma Jaya Catholic University, Jakarta, and Dr Renaningtyas Tambun, Pathologist of St. Carolus Hospital, Jakarta. Dr Johannes Cansius Prihadi is the head of the Surgery Department, Faculty of Medicine, Atma Jaya Catholic University. An informed consent letter by the patient’s parents has been documented which stated agreement and no objection to the publication of their daughter’s case for scientific and educational purposes.
Disclosure
The authors report no conflicts of interest in this work.
References
Mui WH, Lee KC, Chiu SC, et al. Primary yolk sac tumour of the urinary bladder: a case report and review of the literature. Oncol Lett. 2014;7(1):199–202. | ||
Okeke LI, Ogun GO, Etukakpan BR, Iyama A, Adeoye AO, Duduyemi BM. Dermoid cyst of the urinary bladder as a differential diagnosis of bladder calculus: a case report. J Med Case Rep. 2007;1:32. | ||
Agrawal S, Khurana N, Mandhani A, Agrawal V, Jain M. Primary bladder dermoid: a case report and review of the literature. Urol Int. 2006;77:279–280. | ||
Omar M, El-Gharabawy M, Samir A, El Sherif E, Monga M. Mature cystic teratoma of the bladder masquerading as a distal ureteral stone. Urol Case Rep. 2017;13:94–96. | ||
Vera, Safriadi F. Mature (benign) cystic retrovesical teratoma in a 49-year-old male: a case report and literature review. AJMCR. 2016;4(5):153–157. | ||
Onen MR, Kayalar AE, Kilic A, Kir G, Naderi S. Adult sacrococcygeal teratoma: a case report. WScJ. 2012;3(2):67–70. | ||
Jain SK, Kaza RC, Vindal A, Bains L. Vesical dermoid: an unusual presentation. Int J Urol. 2010;17(9):824–825. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.