Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Maternal Pre-Pregnancy Glycemic Status and Developmental Outcomes in Korean Children Aged 18–36 Months: A Nationwide Population-Based Cohort Study (2014–2021)
Authors Han Y ![]() , Park HW, Kim TE, Park S
, Park HW, Kim TE, Park S ![]() , Shin J
, Shin J ![]()
Received 4 September 2025
Accepted for publication 23 December 2025
Published 8 January 2026 Volume 2026:19 555935
DOI https://doi.org/10.2147/DMSO.S555935
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Yeeun Han,1 Hye Won Park,2,3 Tae-Eun Kim,4 Sanghyun Park,4 Jinyoung Shin1,3
1Department of Family Medicine, Konkuk University Medical Center, Seoul, Republic of Korea; 2Department of Pediatrics, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Republic of Korea; 3Konkuk University School of Medicine, Seoul, Republic of Korea; 4Department of Clinical Pharmacology, Konkuk University Medical Center, Seoul, Republic of Korea
Correspondence: Jinyoung Shin, Department of Family Medicine, Konkuk University Medical Center, Konkuk University School of Medicine, 120-1, Neungdong-ro, Gwangjin-gu, Seoul, 05030, Republic of Korea, Tel +82-2-2030-7698, Email [email protected]
Purpose: Maternal metabolic health is increasingly recognized as a critical factor influencing early childhood development. This study examined the relationship between maternal pre-pregnancy glycemic status and neurodevelopmental outcomes in early childhood using a large national cohort in Korea.
Patients and Methods: We conducted a population-based retrospective cohort study using national health examination and Korean Developmental Screening Test data from 2014 to 2021. Maternal fasting plasma glucose levels measured within one year prior to conception through delivery were used to classify women into normal, prediabetes, and diabetes mellitus (DM) groups. Neurodevelopmental outcomes were assessed at 18– 24 and 30– 36 months across six domains: gross motor, fine motor, cognition, language, sociality, and self-care. Inverse probability of treatment weighting was applied to adjust for baseline differences and weighted relative risks (RRs) and 95% confidence intervals (CIs) were estimated.
Results: Among 258,367 mother-child dyads, both prediabetes and DM were associated with significantly increased risks of developmental delays in multiple domains. Offspring of mothers with DM exhibited significantly increased risks of developmental delay across all domains at both 18– 24 and 30– 36 months, with the highest risk observed for self-care at 30– 36 months (RR 1.466, 95% CI 1.408– 1.525). Children of mothers with prediabetes also demonstrated increased risks in cognition (RR 1.061, 95% CI 1.008– 1.117) and self-care (RR 1.119, 95% CI 1.058– 1.184) at 18– 24 months. Additionally, statistically significant elevations were observed in gross motor (RR 1.101, 95% CI 1.037– 1.169), language (RR 1.058, 95% CI 1.019– 1.100), and sociality (RR 1.106, 95% CI 1.060– 1.154) skills at 30– 36 months.
Conclusion: Maternal pre-pregnancy glycemic abnormalities, even at the prediabetic level, were associated with an increased risk of developmental delays in early childhood. Optimizing maternal glycemic control prior to conception may promote more favorable developmental outcomes in offspring.
Keywords: glucose, child development, language development, personality development, administrative claims, health care
Introduction
Hyperglycemia is increasingly prevalent among young adults in their 20s and 30s globally, including in South Korea. In Korea, the prevalence of diabetes among women reached approximately 7.8% in 2021, with even higher rates observed in older age groups.1 Globally, the age-standardized prevalence of gestational diabetes mellitus (GDM) was 14.0% in 2019, with the highest prevalence reported in the South-East Asia region at 27.0%.2 As the average maternal age at childbirth continues to increase,3 there is a growing need to understand the implications of maternal hyperglycemia on offspring outcomes.
Previous cohort and case-control studies have reported that children born to mothers with either GDM or pregestational diabetes mellitus (DM) are at increased risk for delays in gross and fine motor development.4,5 A meta-analysis confirmed that children exposed to maternal DM demonstrate lower performance in motor milestones compared to their unexposed peers, with more pronounced effects observed in cases of pre-existing DM.4 Intrauterine exposure to hyperglycemia is thought to alter neuronal differentiation, synaptogenesis, and insulin dysregulation, which in turn increases the risk of neurocognitive and behavioral developmental disorders in offspring,6 including autism spectrum disorder, attention-deficit/hyperactivity disorder (ADHD) and general developmental delays.7–10
Unfortunately, most of these studies have focused on specific developmental domains or particular neurodevelopmental conditions rather than providing a comprehensive assessment of early childhood developmental outcomes. A large 29-year national cohort study of 3,407,961 Canadian mother–infant pairs reported that maternal DM was associated with higher long-term risks of cardiovascular disease, type 2 diabetes, and hypertension in the offspring, whereas no significant associations were observed with neurobehavioral outcomes.11 These discrepancies may be attributable to several methodological considerations. Many prior investigations included relatively small sample sizes or assessed developmental status at a single time point, thereby limiting the ability to evaluate developmental trajectories or capture domain-specific variations over time. Such variability underscores the need for large, longitudinal studies with repeated developmental assessments to clarify the true impact of maternal glycemia on offspring neurodevelopment.
To address these gaps, the present study utilized data from the Korean Developmental Screening Test (K-DST) to assess neurodevelopmental outcomes at two time points—18–24 months and 30–36 months—allowing for a more longitudinal perspective. By examining multiple developmental domains, this study also offers a more comprehensive understanding of how maternal glycemic status may influence child development.
Therefore, this study aimed to investigate the association between maternal pre-pregnancy glycemic status and early childhood neurodevelopment across multiple developmental domains using a large nationwide cohort in Korea.
Materials and Methods
Study Data Sources and Participants
This retrospective cohort study utilized data from the National Health Examination jointly maintained by the National Health Insurance Service (NHIS) and the National Health Screening Program for Infants and Children (NHSPIC). The NHIS database offers extensive, population-wide data on diagnoses, procedures, and prescriptions in South Korea, coded according to the International Classification of Disease, Tenth Revision (ICD-10). Additionally, the NHIS administers biennial health screenings for individuals aged 20 years and older, collecting both self-reported health histories and anthropometric measurements. This deidentified dataset is considered nationally representative and has been widely employed in epidemiological research.
The study population was initially derived from 886,641 participants in the NHSPIC between 2014 and 2021 who underwent a health screening within one year prior to pregnancy. Among these, 779,091 mother–child pairs were linked using the family’s unique health insurance card number and the recorded delivery date in the NHIS system. Of these, a total of 258,367 mother–child dyads who completed developmental assessments using the K-DST at both the 18–24 months and 30–36 months screening periods were included in the final analysis (Figure 1).
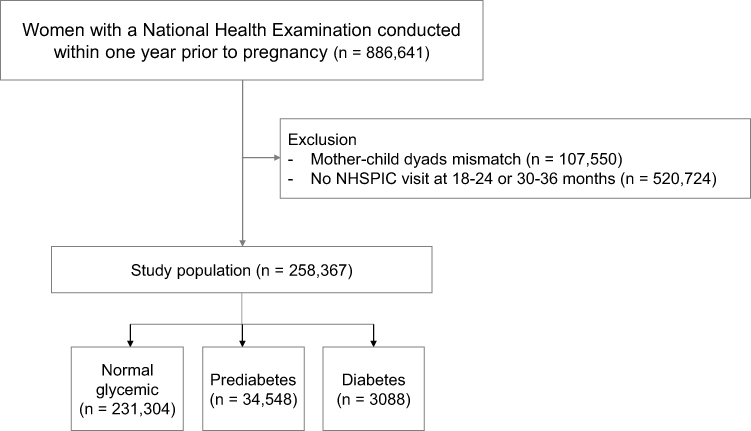 |
Figure 1 Study flow. |
The study was conducted in accordance with the Declaration of Helsinki. As the research used previously collected, fully anonymized data that are publicly available, the study protocol was exempted from full Institutional Review Board (IRB) review by the Konkuk University Medical Center (KUMC: 2025–06-023). The requirement for informed consent was also waived by the same IRB because the analysis involved only de-identified data and posed no potential risk to the participants.
Maternal Pre-Pregnancy Glycemic Status
Maternal glycemic status was assessed based on fasting plasma glucose levels obtained from national health screenings conducted one year prior to pregnancy. Due to data limitations, it was not possible to isolate glucose levels measured strictly before conception. However, given that pregnant women are typically transitioned to antenatal care under the Maternal and Child Health Act,12 and that national health screenings are not routinely advised during pregnancy, it is reasonable to infer that the majority of glucose values in this dataset represent pregestational levels.
Participants were classified into three groups according to their fasting glucose levels measured after at least 8 hours of fasting: normal (< 100 mg/dL), prediabetes (100–125 mg/dL), and DM (≥ 126 mg/dL or current use of antidiabetic medications).13 We obtained the pregestational DM as ICD-10 code (O24.0–O24.3, E100–E109, E110–E119, E120–E129, E130–E139, E140–E149).
Korean Developmental Screening Test (K-DST)
K-DST was developed within the framework of the NHSPIC, which began in 2007 to monitor growth and development, detect early abnormalities, and provide guidance to caregivers. The program schedules six routine health check-ups: the first at 4–6 months, the second at 9–12 months, the third at 18–24 months, the fourth at 30–36 months, the fifth at 42–48 months, the sixth at 54–60 months of age, and the seventh at 61–71 months of age. All examinations are conducted based on the child’s chronological age, not the corrected age. Each screening visit includes a medical history review, physical examinations, anthropometric assessments, visual screening, developmental evaluation using the K-DST, oral examination, and anticipatory guidance through structured questionnaires.
The K-DST is a parent-administered screening tool that evaluates six developmental domains: gross motor, fine motor, cognition, language, sociality, and self-care. Each domain comprises eight items scored from 0 to 3 with a maximum of 24 points per domain. The self-care domain is assessed only for children aged 18 months or older. Based on standard deviation cutoffs, developmental status is categorized as advanced (> +1 SD), age-appropriate (−1 to +1 SD), follow-up needed (−2 to −1 SD), or further evaluation needed (< −2 SD); the latter was defined as “abnormal” in this study.
The test was initially standardized in 2012–2014 using data from 3284 children aged 4–71 months, and was later re-standardized in 2015–2016 based on over 3 million children from the NHSPIC cohort, resulting in the current revised version.14
Statistical Analysis
Descriptive statistics were presented as mean ± standard deviation (SD) for continuous variables and as numbers with percentages for categorical variables. Baseline characteristics were compared across maternal glycemic groups using ANOVA and chi-square tests, as appropriate.
To minimize potential confounding across maternal glucose categories (normal, prediabetes, and DM), inverse probability of treatment weighting (IPTW) was applied using propensity scores (PS) estimated via multinomial logistic regression, with maternal characteristics as covariates. These covariates included maternal age (linear), comorbidities (hypertension [ICD-10 code: I10–I15, O10], pregnancy-induced hypertension [O12-15], and depression [F329, F332, and F530]), preterm birth, delivery method including normal delivery or cesarean section (O800-O809, O820-O829, R435, R436, RA314-318, RA36-38, RA43, R314, R450, R451, R452, and R500), multiple births, major anomalies, small for gestational age (SGA), birth-weight, sex, neonatal intensive care unit (NICU) admission (AJ101, AJ111, AJ121, AJ131, AJ144, AJ161, AJ201, AJ211, AJ221, AJ231, AJ244, AJ261, AJ301, AJ311, AJ321, AJ331, AJ351, AJ051~ AJ054), and gestational age. Covariate balance before and after IPTW was evaluated using absolute standardized differences (ASD). An ASD value <0.1 for all covariates was considered indicative of adequate balance across the three maternal glycemic groups, indicating that residual confounding was minimized after weighting. Stabilized IPTW were applied and the weights were truncated at the 1st and 99th percentiles to reduce the influence of extreme values. Outcome models were fitted using binomial generalized linear models with a log link and robust standard errors were calculated using the sandwich estimator.15
Subsequently, to examine the association between maternal glycemic status and developmental outcomes in offspring, weighted relative risks (RRs) and 95% confidence intervals (CIs) were estimated using generalized linear models after applying IPTW. The reference group was defined as mothers with normal fasting glucose levels (< 100 mg/dl). Developmental outcomes were assessed separately at 18–24 months and 30–36 months of age across six domains using the K-DST: gross motor, fine motor, cognition, language, sociality, and self-care. Developmental delay was defined as a score < −2 SD and the incidence of developmental delay was reported per 100 individuals.
All statistical analyses were conducted using SAS software (version 9.4; SAS Institute, Inc., Cary, NC, USA).
Results
We analyzed 258,367 mother–child pairs categorized by maternal fasting glucose into normal (n = 231,304), prediabetes (n = 23,975), and DM (n = 3088). IPTW was used to balance baseline covariates between groups (post-weighting absolute standardized differences < 0.1 for all variables; residual imbalances remained for BMI [ASD = 0.053], vaginal delivery [ASD = 0.073], and SGA [ASD = 0.050]; see Table 1).
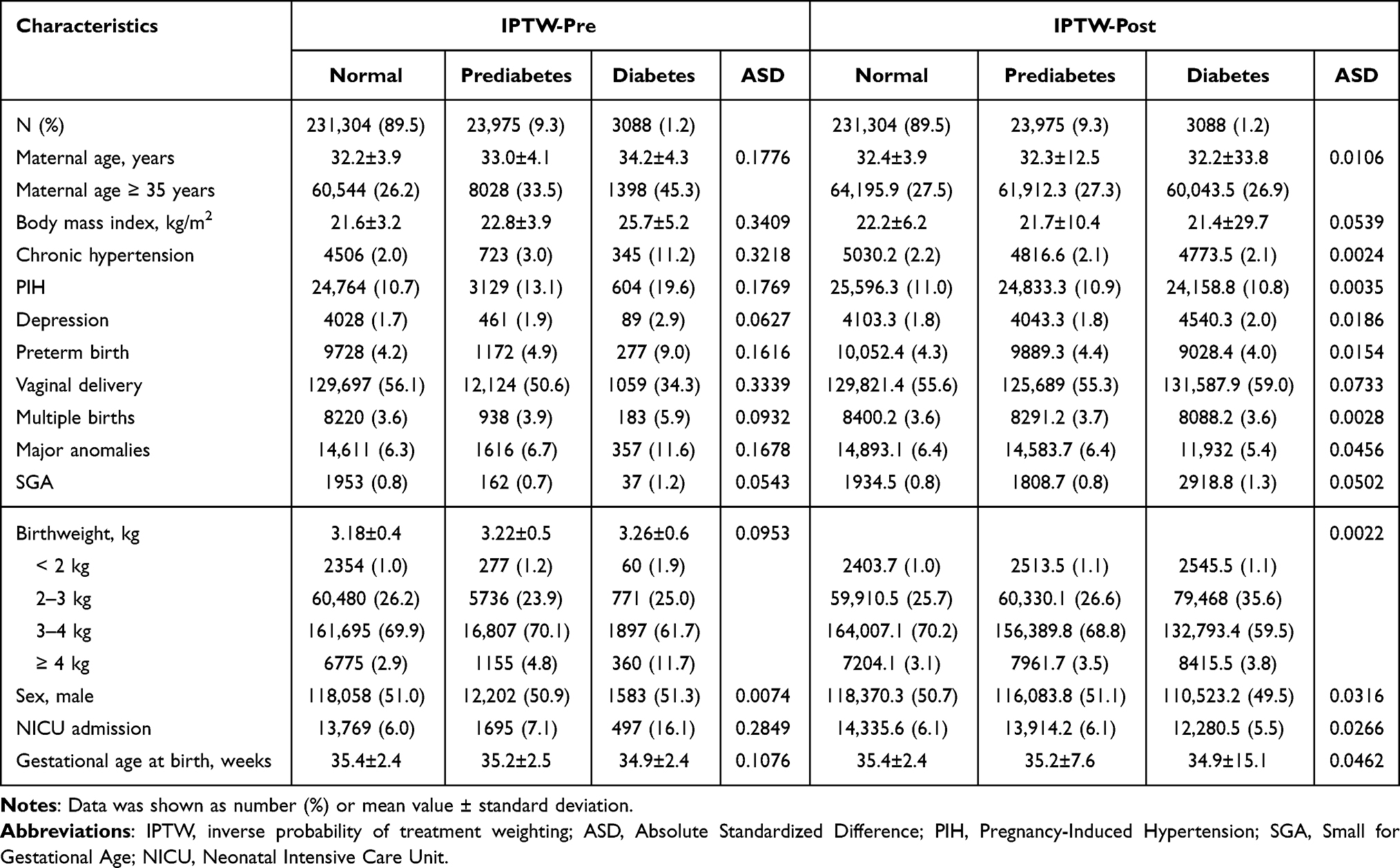 |
Table 1 Baseline Characteristics of Study Population According to the Glucose Status |
As presented in Table 1, baseline characteristics were assessed by maternal glycemic status prior to the application of IPTW. The normal glycemic group consisted of 231,304 individuals, the prediabetes group included 23,975 individuals, and the DM group comprised 3088 individuals. The mean maternal age was highest in the DM group at 34.17 years, with the highest proportion of mothers aged 35 years or older also observed in this group. Chronic hypertension, pregnancy-induced hypertension, and depression were most prevalent among the DM group. The incidence of preterm birth was also highest in the DM group. The rate of spontaneous vaginal delivery was highest in the normal group and lowest in the DM group, suggesting a higher likelihood of cesarean delivery among mothers with DM. The incidence of multiple births, major anomalies, and SGA was highest in DM group. The DM group also exhibited the greatest mean birth weight, as well as the highest prevalence of macrosomia (birth weight ≥ 4kg). Additionally, NICU admission rate was highest in the DM group, whereas the mean gestational age at birth was the lowest. While not shown in the table, the mean interval between childbirth and health screening was 1.39 ± 0.77 years for the normal group, 1.46 ± 0.70 years for the prediabetes group, and 1.36 ± 0.79 years for the DM group, indicating that most screenings were likely conducted prior to pregnancy.
Table 2 presents the associations between maternal glycemic status and the risk of developmental delay in offspring. Among children of mothers with DM, the risks of developmental delay at both 18–24 months and 30–36 months were consistently higher across all six K-DST domains compared with those of mothers with normal glucose levels. At 18–24 months, the weighted RRs for developmental delay in the DM group ranged from 1.107 (95% CI, 1.035–1.184) in gross motor to 1.348 (95% CI, 1.234–1.376) in sociality. For offspring of mothers with prediabetes at 18–24 months, significant increases were observed in cognition (RR 1.061; 95% CI, 1.008–1.117) and self-care (RR 1.119; 95% CI, 1.058–1.184). Other developmental domains showed modest elevations, although these did not reach statistical significance. At 30–36 months, maternal DM remained associated with elevated risks across all developmental domains, with weighted RRs ranging from 1.116 (95% CI, 1.075–1.158) in language to 1.466 (95% CI, 1.408–1.525) in self-care. A noteworthy finding is that children of mothers with prediabetes also exhibited modest but statistically significant increases in the risks of developmental delay at 30–36 months—particularly in gross motor, cognition, language, sociality, and self-care—compared with children of mothers with normal glycemic levels.
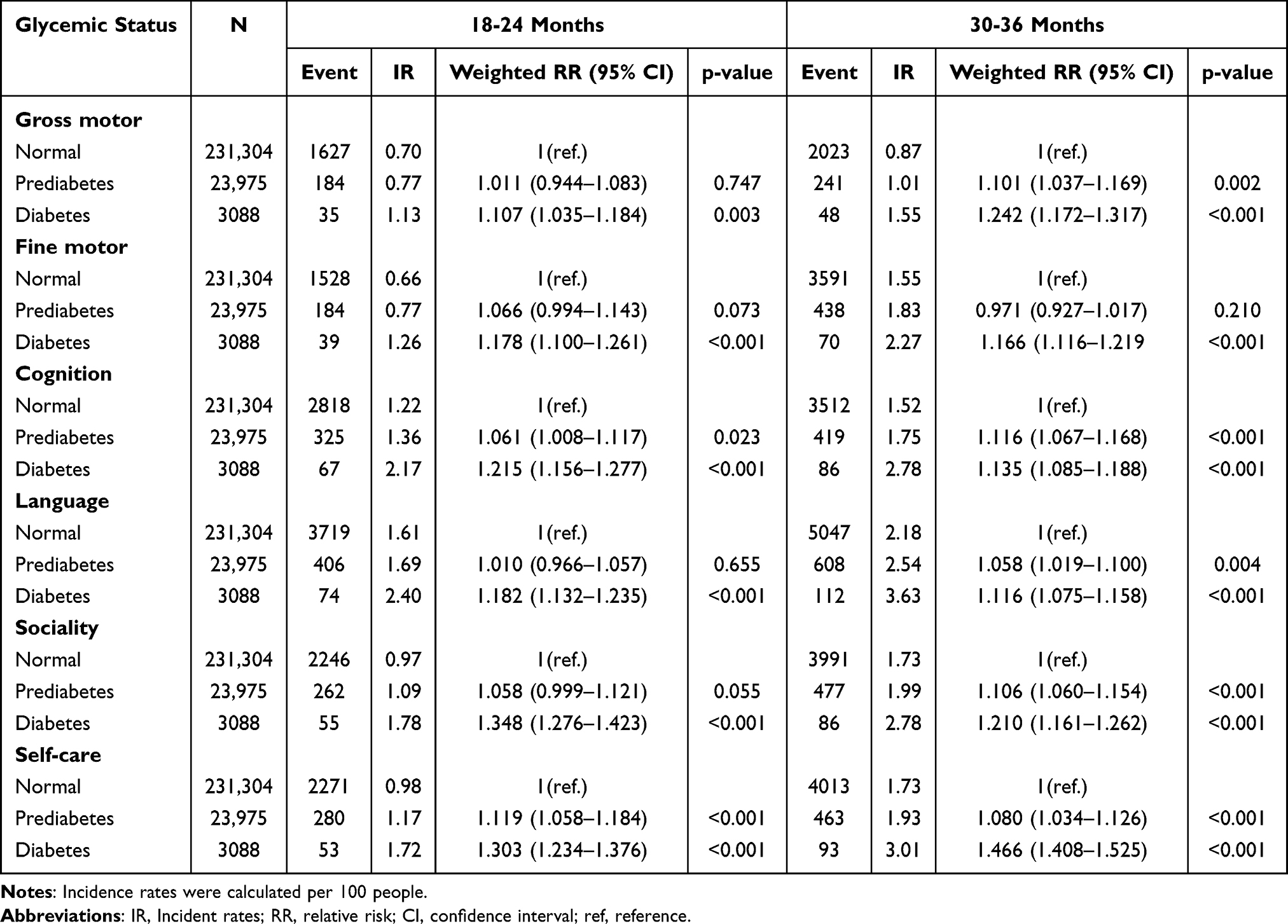 |
Table 2 The Risks of Developmental Assessment in Children of 18–24 Months or 30–36 Months According to the Maternal Glycemic Status |
Discussion
This study analyzed the association between maternal glycemic status and developmental delays in early childhood using a large-scale national cohort in Korea. Pregestational DM was associated with an increased risk of abnormal development for gross motor, fine motor, cognition, language, sociality, and self-care skills. Notably, even prediabetes was linked to an elevated risk of abnormal development in gross motor, cognitive, language, social, and self-care delays—particularly at 30–36 months—suggesting that maternal pre-pregnancy glucose status may have long-term consequences for developmental trajectories.
Mechanistically, the intrauterine environment shaped by maternal metabolic conditions plays a critical role in early brain development. Maternal hyperglycemia can induce inflammation, oxidative stress, placental vascular dysfunction, and fetal hypoxia during critical windows of neurogenesis.4 The resulting inflammatory environment increases placental vascular resistance and facilitates the transfer of pro-inflammatory cytokines to the fetus, altering neuroimmune development and increasing susceptibility to emotional and behavioral difficulties.16,17 Fetal hypoxia may impair neuronal survival and synaptogenesis, particularly in the hippocampus—an area crucial for learning and memory—potentially contributing to multi-domain developmental delays.18 Experimental studies further support these mechanisms, demonstrating neuronal apoptosis and delayed maturation in offspring exposed to diabetic intrauterine environments.19 In addition, compensatory fetal hyperinsulinemia may promote excessive fetal growth, consistent with our observation of a higher prevalence of macrosomia in infants of mothers with diabetes.20
Comparison with prior research highlights the importance of developmental timing and measurement approaches. While some studies, such as Nivins et al, reported null associations at early ages,21 others observed fluctuating motor development depending on the assessment period.22 These discrepancies underscore that early neurodevelopment is dynamic, potentially sensitive to both neuroplasticity and environmental enrichment such as caregiving and play-based stimulation.23 Our inclusion of two distinct time points and six developmental domains allowed us to capture age- and domain-specific variations that may have been missed in earlier studies.
Emerging evidence also indicates that the developmental impact of hyperglycemia differs by pregnancy trimester. Because routine clinical care typically evaluates maternal glucose levels in the second trimester, research on early-pregnancy hyperglycemia has remained limited. Recent studies, however, indicate that trimester-specific glycemic exposure may differentially influence neurodevelopment. For instance, in a Chinese cohort of 1888 mother–child pairs, first-trimester hyperglycemia (≤13 weeks) was associated with impaired cognitive development (OR 1.54, 95% CI 1.08–2.18).24 Early exposure may confer greater vulnerability due to critical periods of brain organogenesis, during which hyperglycemia can induce epigenetic alterations linked to neural tube defects and later neurodevelopmental disorders.25 Moreover, even within the non-diabetic range, elevated FPG levels in early pregnancy are consistently associated with a substantially increased risk of GDM and gestational hypertensive disorders, including preeclampsia and gestational hypertension.26 In contrast, a large US cohort of 322,323 births from the Kaiser Permanente Southern California hospitals reported that hyperglycemia identified after 26 weeks showed weak or null associations with neurodevelopmental delay (HR 0.98, 95% CI 0.84–1.15).27 However, conflicting results suggest that late-pregnancy hyperglycemia may still exert adverse effects. In the same Chinese cohort, hyperglycemia in late pregnancy and at full term was associated with increased risks of fine motor and social developmental delays—2.18-fold (95% CI 1.26–3.77) and 2.64-fold (95% CI 1.38–5.05), respectively—whereas early-pregnancy hyperglycemia was not.24 These mixed findings suggest that early-pregnancy hyperglycemia may be more detrimental to neurodevelopmental pathways, while mid- or late-pregnancy hyperglycemia more strongly reflects contemporaneous fetal growth conditions, contributing to outcomes such as large-for-gestational-age birth, macrosomia, preterm delivery, and cesarean section.28,29 These findings suggest that maternal glycemic trajectories across pregnancy influence neurodevelopmental pathways, although trimester-specific associations warrant further investigation.
The observed multi-domain associations in our study also reflect the interdependent nature of early childhood development. Gross motor skills facilitate environmental exploration, which supports cognitive and social development; fine motor skills contribute to problem-solving and self-regulation; and sociality and language domains are highly integrated through joint attention, emotional recognition, and communication.30,31 Our findings align with existing evidence linking maternal diabetes with neurodevelopmental disorders such as autism spectrum disorder and ADHD.8,9,20 These findings are consistent with ours and further support the hypothesis that maternal hyperglycemia negatively influences early neurodevelopment.
This study has several limitations. First, the K-DST is based on subjective responses from parents or caregivers, which may introduce reporting bias. However, in practice, pediatricians perform brief physical examinations (eg, walking, crawling) based on the questionnaires, lending credibility to results indicating “further evaluation needed”. Second, FPG values were measured within one year before pregnancy, and although women rarely undergo routine health examinations during pregnancy, the exact timing within the one-year window is not fully verifiable. Third, the DM group included both mothers on anti-diabetic medication and those with fasting glucose ≥ 126 mg/dL. Because we did not further classify these individuals according to their level of glycemic control, we were unable to assess how differences in glucose management may have influenced the risk of developmental delay. Finally, unmeasured confounders such as socioeconomic status could not be fully accounted for.
Despite these limitations, the study offers significant strengths. The use of a large nationwide cohort enhances generalizability and provides robust statistical power. The assessment of developmental outcomes at two time points provides longitudinal insight, while evaluation across six domains offers a comprehensive developmental profile. Importantly, the differentiation of maternal glycemic status into normal, prediabetes, and diabetes—rather than a binary classification of “normal vs DM”—allowed for the identification of developmental risks associated with prediabetes, a group often overlooked in previous research. Furthermore, by focusing on maternal glycemia prior to pregnancy rather than gestational diabetes alone, this study provides clearer insights into the preconception metabolic influences on offspring neurodevelopment.
Conclusion
Maternal glycemic abnormalities, even at the prediabetic level, were associated with an increased risk of developmental delays in early childhood. From the preconception period onward, continuous glycemic screening and intervention should be considered as part of early childhood developmental strategies. Although associations between maternal pre-pregnancy FPG and key developmental and birth outcomes are becoming clearer, the broader implications for other obstetric and neonatal risks remain uncertain. To better understand these relationships, future large-scale longitudinal studies with repeated maternal glycemic assessments across pregnancy are needed. In addition, intervention studies focused on improving maternal glycemic control—through lifestyle modification, early screening, or targeted metabolic management—will be essential to determine whether reducing maternal hyperglycemia can mitigate adverse neurodevelopmental and perinatal outcomes.
Data Sharing Statement
The data supporting this article are accessible from the National Health Insurance Service Open Data Portal (https://nhiss.nhis.or.kr/). Deidentified data used in this study are available upon reasonable request and approval by the NHIS. Study-related documents (eg, analytic code or data dictionaries) are available from the corresponding author upon reasonable request.
Author Contributions
YH – Conceptualization, Methodology, Writing – original draft. HWP – Conceptualization, Methodology, Writing – review & editing. TEK – Conceptualization, Methodology, Writing – review & editing. SHP – Conceptualization, Methodology, Formal analysis, Writing – review & editing. JS – Conceptualization, Methodology, Funding acquisition, Writing – review & editing.
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Konkuk University Medical Center Research Grant 2025.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Korea Disease Control and Prevention Agency. Trends in prevalence of diabetes, 2011-2021. Public Health Wkly Rep. 2023;16(43):1488–9. doi:10.56786/PHWR.2023.16.43.3
2. Wang H, Li N, Chivese T, et al. IDF diabetes atlas: estimation of global and regional gestational diabetes mellitus prevalence for 2021 by international association of diabetes in pregnancy study group’s criteria. Diabetes Res Clin Pract. 2022;183:109050. doi:10.1016/j.diabres.2021.109050
3. Mean age of women at childbirth by birth order. Statistics Korea. Available from: https://www.index.go.kr/unity/potal/indicator/IndexInfo.do?cdNo=260&clasCd=12&idxCd=H0025&upCd=1.
4. Arabiat D, AL Jabery M, Kemp V, Jenkins M, Whitehead LC, Adams G. Motor developmental outcomes in children exposed to maternal diabetes during pregnancy: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(4):1699. doi:10.3390/ijerph18041699
5. Saito Y, Kobayashi S, Ito S, et al. Neurodevelopmental delay up to the age of 4 years in infants born to women with gestational diabetes mellitus: the Japan environment and children’s study. J Diabetes Invest. 2022;13(12):2054–2062. doi:10.1111/jdi.13907
6. Rodolaki K, Pergialiotis V, Iakovidou N, Boutsikou T, Iliodromiti Z, Kanaka-Gantenbein C. The impact of maternal diabetes on the future health and neurodevelopment of the offspring: a review of the evidence. Front Endocrinol. 2023;14:1125628. doi:10.3389/fendo.2023.1125628
7. Chen S, Zhao S, Dalman C, Karlsson H, Gardner R. Association of maternal diabetes with neurodevelopmental disorders: autism spectrum disorders, attention-deficit/hyperactivity disorder and intellectual disability. Int J Epidemiol. 2021;50(2):459–474. doi:10.1093/ije/dyaa212
8. Ornoy A, Becker M, Weinstein-Fudim L, Ergaz Z. Diabetes during pregnancy: a maternal disease complicating the course of pregnancy with long-term deleterious effects on the offspring. a clinical review. Int J Mol Sci. 2021;22(6):2965. doi:10.3390/ijms22062965
9. Chen KR, Yu T, Lien YJ, Chou YY, Kuo PL. Childhood neurodevelopmental disorders and maternal diabetes: a population-based cohort study. Dev Med Child Neurol. 2023;65(7):933–941. doi:10.1111/dmcn.15488
10. Garza-Martínez MJ, ÁH-M J, Hurtado-Salgado EM, Cupul-Uicab LA. Maternal diabetes during pregnancy and offspring’s risk of autism spectrum disorder: a systematic review and meta-analysis. J Psychiatr Res. 2025;182:100–115. doi:10.1016/j.jpsychires.2025.01.003
11. Feig DS, Artani A, Asaf A, Li P, Booth GL, Shah BR. Long-term neurobehavioral and metabolic outcomes in offspring of mothers with diabetes during pregnancy: a large, population-based cohort study in Ontario, Canada. Diabetes Care. 2024;47(9):1568–1575. doi:10.2337/dc24-0108
12. Enforcement rule of the mother and child health act. Available from: https://www.law.go.kr/.
13. Choi JH, Lee KA, Moon JH, et al. 2023 clinical practice guidelines for diabetes mellitus of the Korean diabetes association. Diabetes Metab J. 2023;47(5):575–594. doi:10.4093/dmj.2023.0282
14. Chung HJ, Yang D, Kim GH, et al. Development of the Korean Developmental Screening Test for infants and children (K-DST). Clin Exp Pediatr. 2020;63(11):438–446. doi:10.3345/cep.2020.00640
15. Kreif N, Gruber S, Radice R, Grieve R, Sekhon JS. Evaluating treatment effectiveness under model misspecification: a comparison of targeted maximum likelihood estimation with bias-corrected matching. Stat Methods Med Res. 2016;25(5):2315–2336. doi:10.1177/0962280214521341
16. Kawaguchi C, Ishikuro M, Saito R, et al. Maternal fasting plasma glucose level in early gestation and developmental delay in 2-year-old children. J Clin Endocrinol Metab. 2025;110(10):e3425–e3432. doi:10.1210/clinem/dgae825
17. Gumusoglu SB, Stevens HE. Maternal inflammation and neurodevelopmental programming: a review of preclinical outcomes and implications for translational psychiatry. Biol. Psychiatry. 2019;85(2):107–121. doi:10.1016/j.biopsych.2018.08.008
18. Rubin RD, Watson PD, Duff MC, Cohen NJ. The role of the hippocampus in flexible cognition and social behavior. Front Human Neurosci. 2014;8:742. doi:10.3389/fnhum.2014.00742
19. Zhao J, Hakvoort TBM, Ruijter JM, et al. Maternal diabetes causes developmental delay and death in early-somite mouse embryos. Sci Rep. 2017;7(1):11714. doi:10.1038/s41598-017-11696-x
20. Krakowiak P, Walker CK, Bremer AA, et al. Maternal metabolic conditions and risk for autism and other neurodevelopmental disorders. Pediatrics. 2012;129(5):e1121–8. doi:10.1542/peds.2011-2583
21. Nivins S, Giesbrecht GF, Tomfohr-Madsen L, Lebel C. Prenatal maternal diabetes, comorbidities, and risk for neurodevelopmental impairment in the first two years. Pediatr Res. 2025;97(5):1612–1622. doi:10.1038/s41390-024-03620-7
22. Ornoy A, Ratzon N, Greenbaum C, Peretz E, Soriano D, Dulitzky M. Neurobehaviour of school age children born to diabetic mothers. Arch Dis Child Fetal Neonatal Ed. 1998;79(2):F94–9. doi:10.1136/fn.79.2.f94
23. Corsi C, Santos MM, Marques LA, Rocha NA. [Impact of extrinsic factors on fine motor performance of children attending day care]. Repercussões de fatores extrínsecos no desempenho motor fino de crianças frequentadoras de creches. Rev Paulista Pediatria. 2016;34(4):439–446. doi:10.1016/j.rpped.2016.01.005
24. Yuan Z, Su T, Yang L, Xi L, Wang HJ, Ji Y. Maternal glycemia and its pattern associated with offspring neurobehavioral development: a chinese birth cohort study. Nutrients. 2025;17(2):257. doi:10.3390/nu17020257
25. Banik A, Kandilya D, Ramya S, Stünkel W, Chong YS, Dheen ST. Maternal factors that induce epigenetic changes contribute to neurological disorders in offspring. Genes. 2017;8(6):150. doi:10.3390/genes8060150
26. Tong JN, Wu LL, Chen YX, et al. Fasting plasma glucose in the first trimester is related to gestational diabetes mellitus and adverse pregnancy outcomes. Endocrine. 2022;75(1):70–81. doi:10.1007/s12020-021-02831-w
27. Xiang AH, Wang X, Martinez MP, et al. Association of maternal diabetes with autism in offspring. JAMA. 2015;313(14):1425–1434. doi:10.1001/jama.2015.2707
28. Yang Y, Lin Q, Ma L, et al. Maternal fasting glucose levels throughout the pregnancy and risk of adverse birth outcomes in newborns: a birth cohort study in Foshan city, Southern China. Eur J Endocrinol. 2023;188(1):101–108. doi:10.1093/ejendo/lvac019
29. Wang N, Han B, Hong S, et al. Association between maternal plasma glucose levels during pregnancy and risk of preterm birth: a retrospective study. BMC Pregnancy Childbirth. 2025;25(1):1242. doi:10.1186/s12884-025-08309-1
30. Capio CM, Mendoza NB, Jones RA, Masters RSW, Lee K. The contributions of motor skill proficiency to cognitive and social development in early childhood. Sci Rep. 2024;14(1):27956. doi:10.1038/s41598-024-79538-1
31. Krombholz H. Gross and fine motor milestones in the first two years of life - representative data for Germany. Global Pediatrics. 2025;12:100254. doi:10.1016/j.gpeds.2025.100254
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.