Back to Journals » Risk Management and Healthcare Policy » Volume 16
Maternal Perception, Hesitancy, and Satisfaction Toward Childhood Immunization in Primary Health Centers, Hafr Al-Batin: A Multicenter Cross-Sectional Study from Eastern Saudi Arabia
Authors Thirunavukkarasu A, Falji A Alanazi M, Al-Hazmi AH, Farhan ALruwaili B, Awad Alsaidan A ![]() , Alshami M Alruwaili T, Abdulaziz M Algaed M, Kaseb Alsharari A, Alenazi RH, Alshalan AM, Alshalan SM
, Alshami M Alruwaili T, Abdulaziz M Algaed M, Kaseb Alsharari A, Alenazi RH, Alshalan AM, Alshalan SM
Received 3 February 2023
Accepted for publication 1 November 2023
Published 8 November 2023 Volume 2023:16 Pages 2357—2368
DOI https://doi.org/10.2147/RMHP.S406933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Ashokkumar Thirunavukkarasu,1 Mohammed Falji A Alanazi,2 Ahmad Homoud Al-Hazmi,1 Bashayer Farhan ALruwaili,1 Aseel Awad Alsaidan,1 Thamer Alshami M Alruwaili,3 Majed Abdulaziz M Algaed,4 Areej Kaseb Alsharari,4 Ragad Humaidi Alenazi,4 Amal Muteb Alshalan,5 Sultan Muteb Alshalan6
1Department of Family and Community Medicine, College of Medicine, Jouf University, Sakaka, Saudi Arabia; 2Department of Public Health, Hafr Al Batin Health Affairs, Hafr Al Batin, Saudi Arabia; 3Department of Pediatrics, College of Medicine, Jouf University, Sakaka, Saudi Arabia; 4College of Medicine, Jouf University, Sakaka, Saudi Arabia; 5Department of Medicine, King Abdulaziz Specialist Hospital, Sakaka, Saudi Arabia; 6Medical Department, North Medical Tower hospital, Arar, Saudi Arabia
Correspondence: Ashokkumar Thirunavukkarasu, Department of Family and Community Medicine, College of Medicine, Jouf University, Sakaka, 72388, Saudi Arabia, Tel +966-599739619, Email [email protected]
Background: Consumer perception of and satisfaction with vaccination services is a critical and commonly used indicator for evaluating the quality of services provided by concerned authorities. The present survey assessed maternal perceptions, hesitancy, satisfaction, and factors associated with childhood immunization services provided at the primary health centers (PHCs) of eastern Saudi Arabia.
Methods: The current analytical cross-sectional study included mothers of childhood vaccine beneficiaries attending PHCs in Hafr Al-Batin. We collected data related to mothers’ perceptions, hesitancy, and satisfaction using a validated Arabic version of the data collection tool. Factors associated with low and high satisfaction with the immunization services were evaluated using logistic regression analysis. We performed Spearman correlation test to identify the correlation between the perception and satisfaction scores.
Results: Of the 675 participants, 87.4% were satisfied with the immunization services provided at the PHCs. The participants’ satisfaction was significantly associated with the immunized child’s age group (adjusted odds ratio [AOR] = 1.89, 95% CI = 1.39– 2.89, p = 0.037) and occupation status (AOR = 1.42, 95% CI = 1.17– 1.74, p = 0.024). Vaccine hesitancy was significantly associated with the mother’s age group (AOR = 1.89, 95% CI of AR = 1.35– 3.39, P = 0.003) and number of children (AOR = 1.42, 95% CI of AR = 1.17– 1.74, P = 0.024), Additionally, we found a significant positive correlation (Spearman’s rho = 0.207, p < 0.001) between perception and satisfaction scores.
Conclusion: We recommend targeted health education programs for mothers to improve their perceptions and the importance of all recommended childhood vaccines. Additionally, we suggest continuing maternal satisfaction assessments to enhance and maintain the quality of vaccination services.
Keywords: childhood vaccines, adverse effect, satisfaction, hesitancy, perception, Saudi Arabia
Introduction
Immunization is one of the critical advancements in international health and development, saving millions of children worldwide.1,2 Currently, more than 20 serious diseases are under control due to immunization, enabling children and adults to live healthier and more productive lives.1,3 According to the United Nations Children’s Fund (UNICEF), immunizations has prevented over five deaths per minute and saved up to 3 million daily deaths, even before the COVID-19 pandemic.3 Childhood vaccinations are essential for protecting children against serious vaccine-preventable diseases, including measles, mumps, rubella, polio, diphtheria, pertussis, and tetanus. Childhood vaccination protects children and also helps in protecting other vulnerable groups.4
Despite the proven benefits of vaccination and the general acceptance of its efficacy, a small proportion of individuals refuse or delay vaccinations. Vaccine hesitancy can manifest as complete refusal, delayed acceptance, or acceptance accompanied by doubts about the process, influenced by factors such as decreased confidence in the vaccination process, underestimation of the risks associated with vaccine-preventable diseases, and limited accessibility and quality of services.5 A survey conducted by Lakunina in 2021 reported that more than 50% of parents were adequately informed about immunization. Parents often withhold vaccination due to concerns about potential behavioral and neurological issues emerging in children after vaccination.6 Similarly, a community-based survey conducted by GebreEyesus et al in 2020 using a cluster sampling method found that nearly one-third (68.2%) of mothers expressed satisfaction with childhood immunization services. They also found maternal satisfaction with childhood immunization services was significantly associated with education status, being divorced, and favorable health care providers.7 Another survey conducted in Egypt that evaluated maternal satisfaction with pediatric immunization services provided at primary health centers (PHCs) reported that most mothers had insufficient knowledge of childhood vaccination, but this was not statistically significant. The study recommended that clients’ needs are ever changing, and ongoing assessments of clients’ satisfaction are essential to improving childhood vaccination services.8
In the Kingdom of Saudi Arabia (KSA), PHCs are the first line of contact for the community in delivering healthcare services, including childhood immunizations, and are divided into two sections (one for men and the other for women).9,10 The immunization services are provided in the women’s section, where men are not allowed due to sociocultural restrictions implemented in the KSA. Consumer satisfaction with healthcare services serves as a crucial and commonly used indicator for evaluating the quality of services provided by relevant authorities, potentially influencing attitudes toward vaccination.11,12 This approach can also help policymakers gain insights into various domains of care and plan for necessary changes.13–15 In the KSA, a survey conducted by Alshammari TM et al assessed Saudi parents’ perceptions regarding childhood vaccinations. They revealed that most parents possessed a sound understanding of childhood vaccines, completed immunization as per the schedule for their children for up to five years and had easy accessibility to vaccine-related services.16
Despite these findings, a study from Saudi Arabia reported a 20% of vaccine hesitancy among parents.17 Decisions regarding vaccines include a complex array of elements that encompass emotional, cultural, social, spiritual and political domains.18 Considering the broad sociocultural diversity across different regions of the KSA, these findings cannot be generalized to the entire population. Continuous evaluation is imperative, especially given the changing epidemiological landscape related to vaccines, particularly post-pandemic.19,20 Furthermore, there exists a pressing need for region-specific data on this intricate subject to facilitate essential policy changes. Therefore, the present study aimed to assess the perceptions and hesitancy toward childhood immunization among mothers attending immunization services at Hafr Al-Batin, Saudi Arabia and to identify their satisfaction with the childhood immunization services provided at PHCs. Furthermore, we evaluated the correlation between maternal perceptions and satisfaction with the immunization services provided.
Materials and Methods
Research Design and Setting
This analytical cross-sectional study was conducted from June 2022 to January 2023. We included mothers of childhood vaccine beneficiaries attending all PHCs in Hafr Al-Batin, which is situated in the Eastern province of the KSA. There are 73 PHCs in this region, serving approximately 600,000 people across 34 areas. The present study included mothers of childhood immunization beneficiaries (up to 6 years of age) and excluded participants other than mothers (relatives and caregivers).
Sampling Strategy
In this analytical cross-sectional study, we estimated the minimum number of vaccination beneficiaries (mothers) using Cochran’s formula (n=z2pq/e2). Given the wide range of satisfaction and hesitancy levels reported in previous studies, we considered 50% as the expected proportion (p). This choice aimed to provide the maximum number of required participants. Therefore, with an expected proportion of 50% at a 95% confidence interval (CI) and 5% margin of error, the measured sample size (minimum required) was 384, rounded to 390. However, the research team aimed to collect the data until reaching the minimum necessary sample size or the maximum duration allowed by the institutional review board, which resulted in data collection from 675 mothers who attended the PHCs of Hafr Al-Batin, KSA. Using consecutive sampling methods, all the mothers were invited to participate in the survey after their children got immunized at the PHCs. To ensure recruitment of participants over the study period, we limited the number of participants from each center to a maximum of 10 mothers per day.
Data Collection Procedure
The research team initiated the data collection process after getting ethical clearance from Hafr Al-Batin Health Affairs, KSA (Approval no:082, Dated: 21.06.22) and other necessary approvals from relevant health center officials. All participating mothers provided informed consent in line with the Declaration of Helsinki. The research team developed the data collection proforma based on the existing literature from PubMed, Web of Sciences, and other major databases and from the field of experts from pediatrics, public health, and family medicine.7,8,11,13,21 The prepared questionnaire was translated into Arabic, and the research team followed all the standard protocols during the translation process.22,23 Prior to the main data collection, a survey questionnaire was administered to 30 mothers who attended immunization session for their children. All the participated mothers gave feedback that the questionnaire was in simple language, clear, and easy to understand. The Cronbach’s alpha values for the perception and satisfaction sections were 0.78 and 0.91, respectively. All mothers communicated through q Google link by using the pretested and structured questionnaire. The data collection tool consists of three parts (refer to Appendix 1, data collection form, for detailed content). The first part included inquiries about sociodemographic characteristics such as the mother’s age, education, occupation, and residential status), and the second consists of 10 questions about the mother’s perception and hesitancy towards childhood vaccination. This section was based on the WHO vaccine hesitancy scale (VHS), commonly used in various sociocultural settings to assess participants’ perceptions and attitudes toward childhood vaccines that contribute to vaccine hesitancy.24–26 These 10 items were further divided into two domains that evaluated participants’ perceptions of vaccine efficacy and confidence in vaccine effects (Domain 1: Items 1, 2, 3, 4, 6, 7, and 8) and perceptions of vaccine risks (Domain 2: Items 5, 9, and 10).26,27 Higher scores in the domains and overall indicated lower hesitancy toward childhood vaccines. The final section comprised of 10 items related to participants’ satisfaction with the immunization services provided at the PHCs. The mothers responded on a 5-point Likert scale for both the perception and satisfaction sections. These 10 items evaluated the participants’ satisfaction related to immunization services regarding registration, healthcare providers’ role in care, and follow-up advice. The responses in the perception section ranged from strongly agree to strongly disagree, and we marked the score as 5 to 1. A reverse score (1 to 5) was assigned to the negative questions (Items 5, 7, 9, and 10). The responses in the satisfaction category ranged from very much satisfied to very much dissatisfied, and we marked the score from 5 to 1. We summed up all the responses scores to calculate the total scores.
Statistical Analysis
Descriptive data on background characteristics, perceptions, hesitancy, and satisfaction levels are presented as frequencies and proportions. The quantitative data, such as total scores, are presented as mean and standard deviation. We performed the Shapiro–Wilk normality test, and neither the satisfaction nor hesitancy scores met the normality assumption. Furthermore, we categorized the satisfaction scores into low and high using the demarcation threshold equation: (total highest score − total lowest score) / 2 + Total lowest scores.12,28,29 Using values from the present study, the cut-off value was set at 30 for satisfaction scores, categorizing them as low (≤30) and high (>30). The median value of the vaccine hesitancy scores assessed by the WHO-VHS was 37. We categorized them into less vaccine hesitancy (>37) and high vaccine hesitancy (≤37) groups based on the median value from this study. The associated factors for the low and high satisfaction with the immunization services and factors linked to low and high vaccine hesitancy were evaluated using binomial logistic regression analysis. Finally, we performed Spearman correlation test to identify the correlation between perception and satisfaction scores.
Results
Among the 675 participating mothers, the majority (48.3%) belonged to the age group of 25 to 35 years, and their immunized child age group was less than 12 months (45.0%). Furthermore, most mothers had an education level above high school (70.5%) and are currently married (96.1%). Concerning the source of information received about childhood vaccines, more than half (54.4%) of them received information from the Ministry of Health, KSA activities, and 24.4% received the same from media platforms (such as social media, TV, and radio) (Table 1).
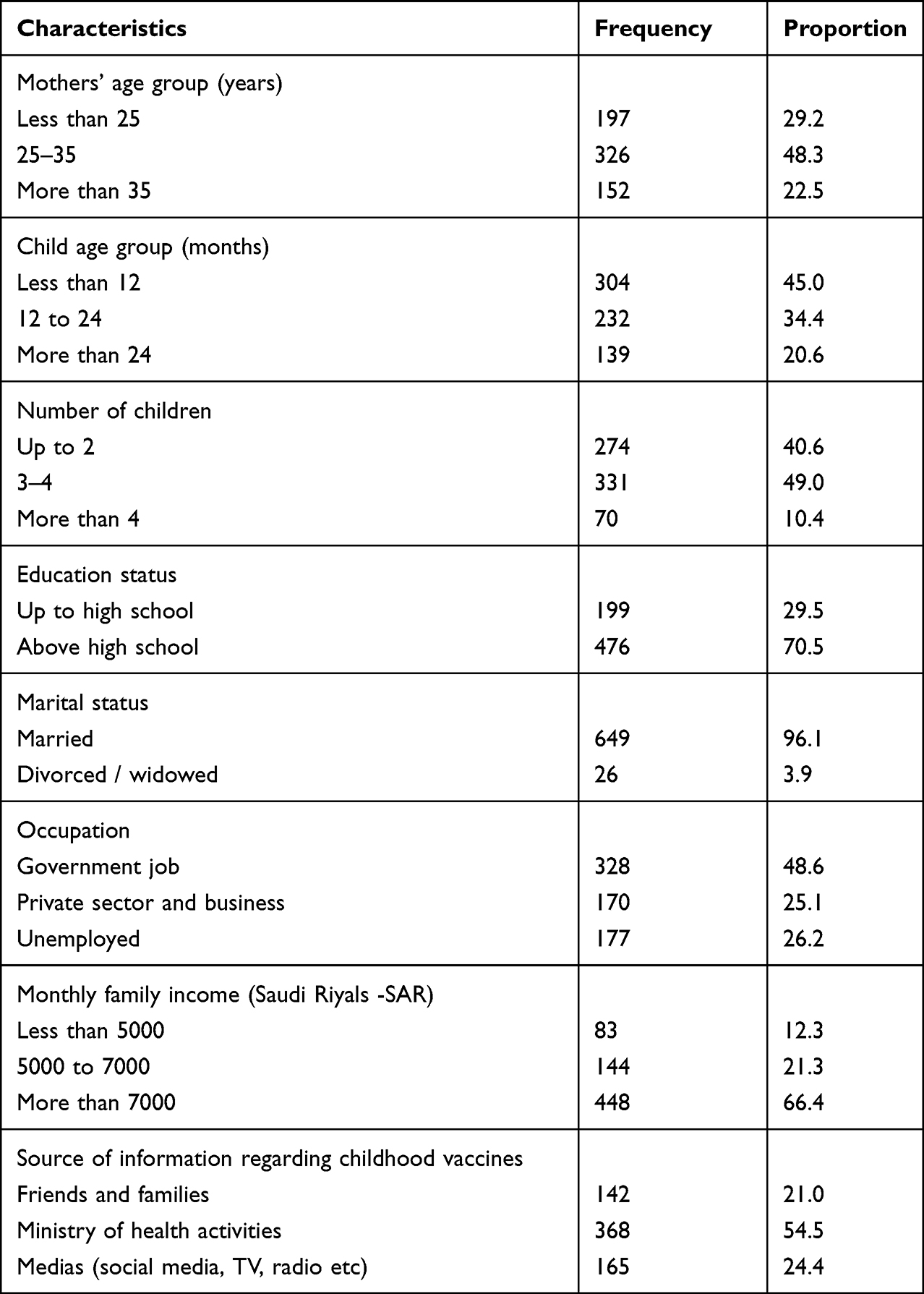 |
Table 1 Sociodemographic Characteristics of the Mothers (n = 675) |
Mothers’ perceptions regarding childhood vaccines and immunization services are detailed in Table 2. The majority of the mothers agreed that childhood vaccines are essential for their child’s health (91.3%) and prevent severe illness (87.4%) and having their child vaccinated is necessary for the health of others in the community (91.4%). Notably, approximately 36% of participants believed that newly approved vaccines carry more risk than older vaccines, and 35% were concerned about the adverse effects of childhood vaccines.
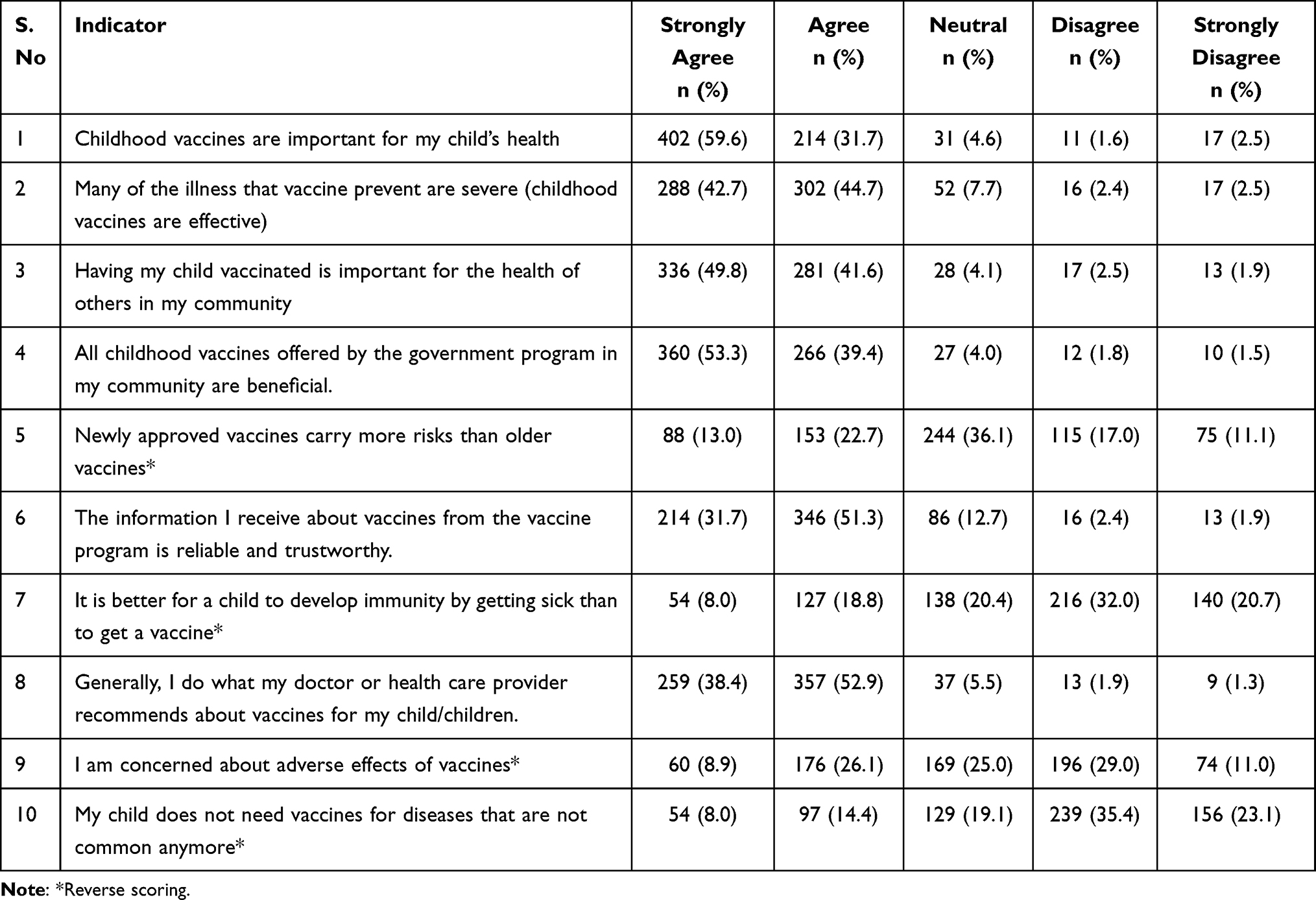 |
Table 2 Participants’ Perception and Hesitancy Towards Childhood Vaccines Provided at the Primary Health Centers (PHCs) of Hafr Al Batin (n = 675) |
Regarding participants’ satisfaction with immunization services, the highest satisfaction level (very much satisfied and satisfied) was observed in ease of registration and scheduling (85.9%), followed by the time spent by the healthcare providers upon my child having vaccinated (83.4%), and waiting time before getting vaccine services by the healthcare providers (79.8%). Conversely, the lowest satisfaction level was noted in follow-up advice on potential adverse effects and their management (64.3%) and the healthcare providers’ consideration of my concerns about vaccination (66.4%) (Table 3).
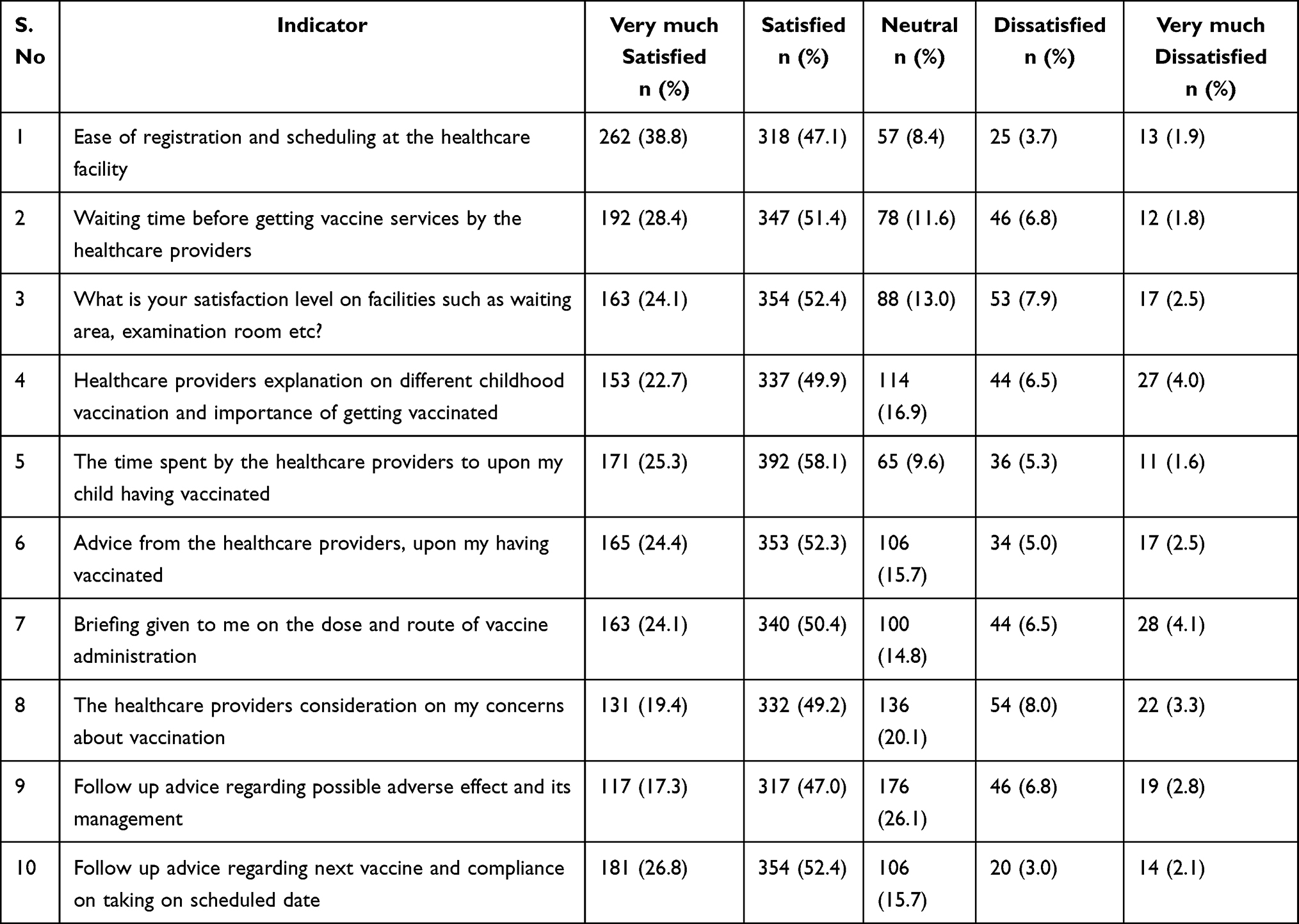 |
Table 3 Participants’ Satisfaction with Immunization Services Provided at the PHCs of Hafr Al Batin (n = 675) |
Categorizing vaccine hesitancy based on the study’s median score, 357 participants (52.9%) demonstrated less hesitancy, while 318 (47.1%) displayed high hesitancy. The binomial logistic regression, adjusted for the covariables of this survey, revealed a significant association between participants’ vaccine hesitancy and the mother’s age group (adjusted odds ratio [AOR] = 1.89, 95% CI of AR = 1.35–3.39, p = 0.003), number of children (AOR = 1.42, 95% CI of AR = 1.17–1.74, p = 0.024), education status (AOR = 1.71, 95% CI of AR = 1.23–2.94, p = 0.001), and source of information about immunization (AOR = 2.41, 95% CI of AR = 1.39–3.86, p = 0.004; Table 4).
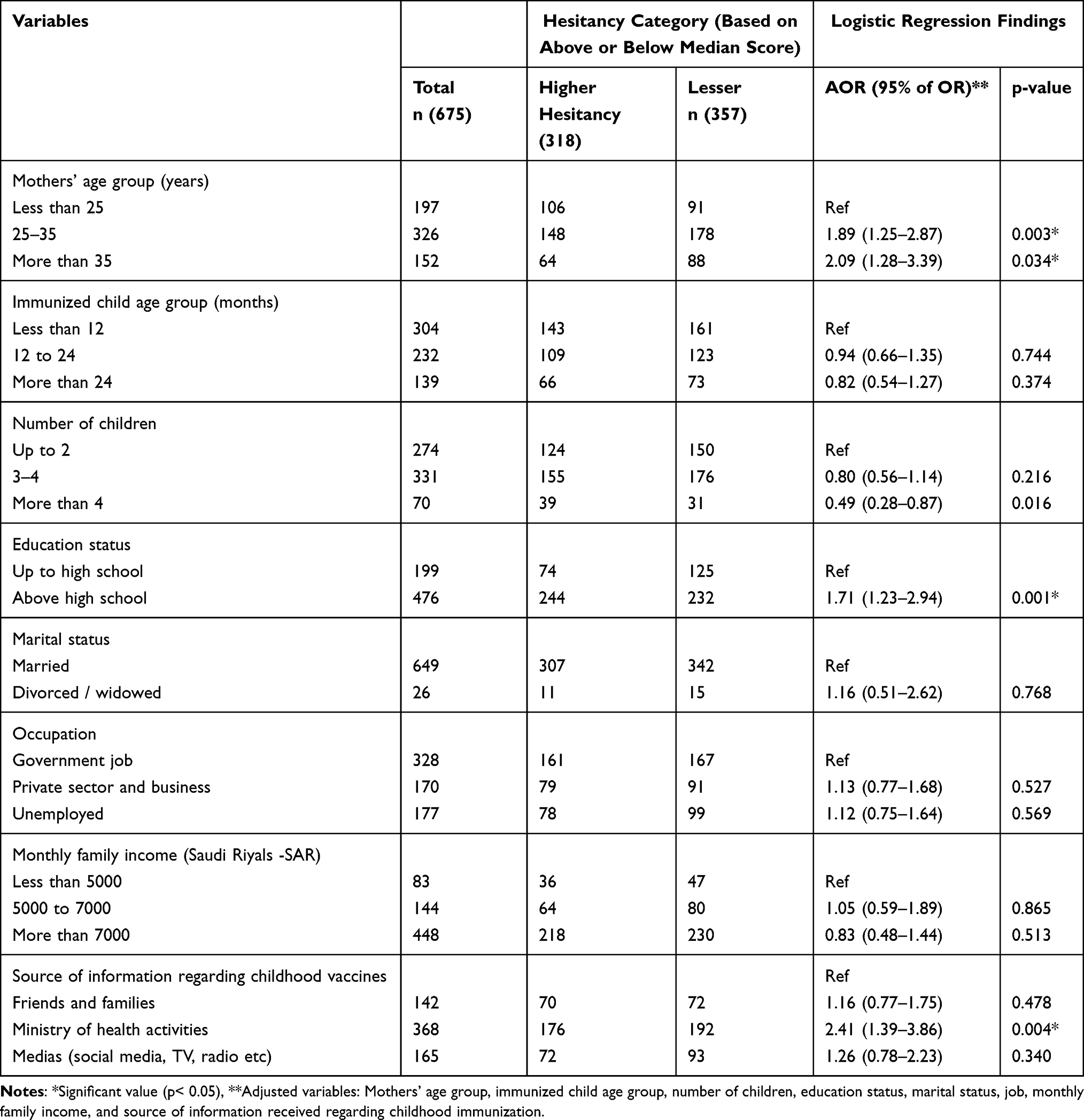 |
Table 4 The Associated Factors for the Vaccine Hesitancy Among the Mothers Attending PHCs of Hafr Al Batin (n = 675) |
Among the participants, 590 (87.4%) expressed satisfaction with the immunization services at the PHCs of Hafr Al-Batin, KSA. The binomial logistic regression, after adjusting with the covariables of this survey, we found that participants’ satisfaction was significantly associated with the immunized child age group AOR = 1.89, 95% CI of AR = 1.39–2.89, p = 0.037) and occupation status (AOR = 1.42, 95% CI of AR = 1.17–1.74, p = 0.024) (Table 5).
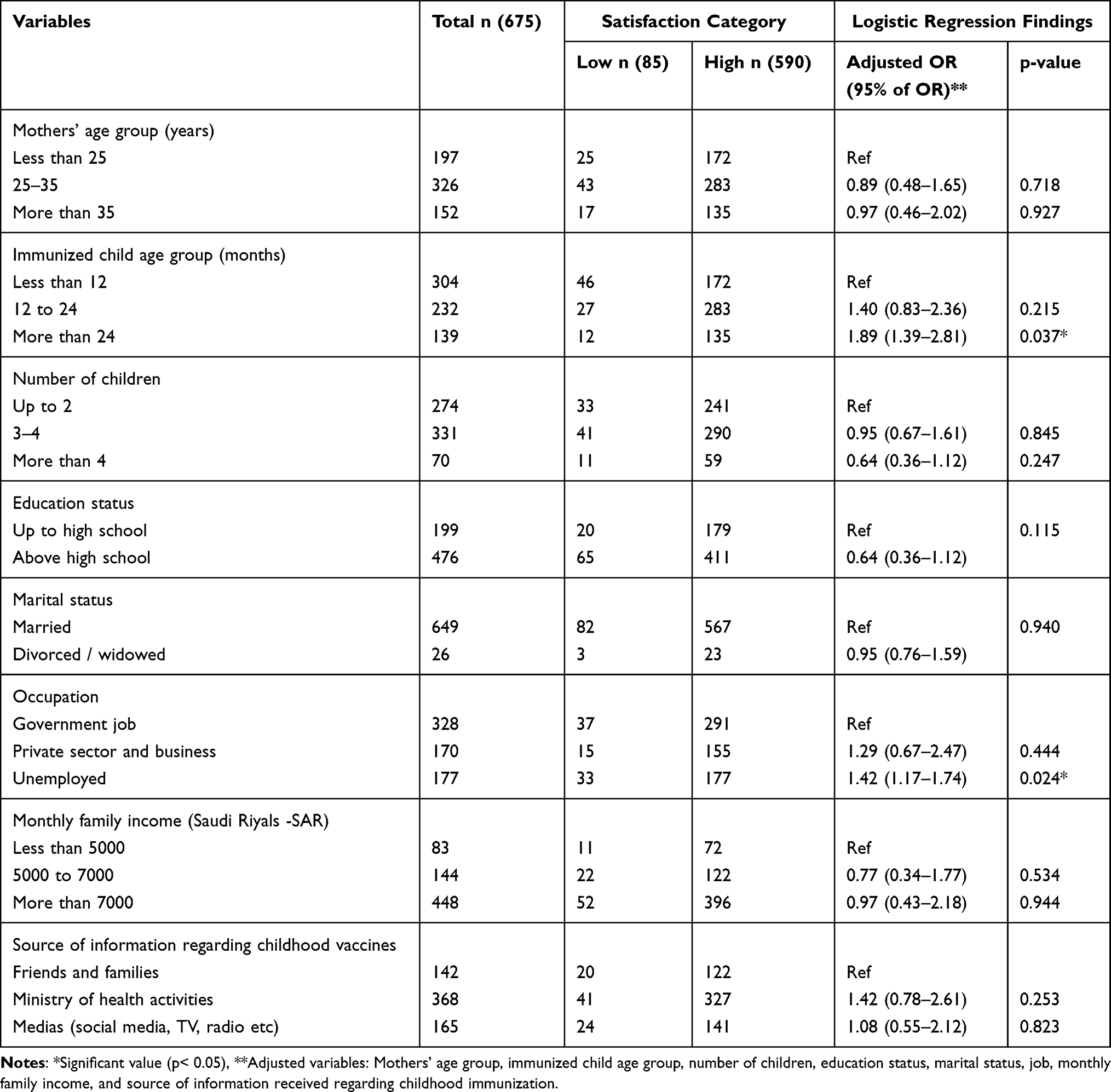 |
Table 5 The Associated Factors with the Immunization Services Provided at the PHCs of Hafr Al Batin (n = 675) |
Since neither the perception (test value = 0.931, p < 0.05) nor satisfaction (test value = 0.919, p < 0.05) scores met the normality assumption through the Shapiro–Wilk test. Hence, we executed the Spearman correlation test, and it revealed a significant positive correlation (Spearman’s rho = 0.207, p < 0.001) between perception and satisfaction scores (Table 6).
 |
Table 6 The Correlation Between Participants’ Perception and Satisfaction Scores |
Discussion
Mothers’ perceptions of childhood vaccines and their satisfaction with the immunization services provided by health authorities are a critical indicator for making policy decisions by the concerned authorities. In this context, we investigated Saudi mothers’ perceptions, hesitancy, and satisfaction concerning the childhood immunization provided at the PHCs of Hafr Al-Batin, KSA.
Favorable maternal perception and attitude toward childhood vaccines are crucial for ensuring complete immunization in children.30,31 Our study found that 91.3% of mothers agreed that childhood vaccines were vital for their child’s health. A recent survey from the Riyadh region of KSA reported a slightly higher proportion (93.7%) of mothers agreeing with the same statement32 which is quite similar to the findings of our the study. In contrast, a lower proportion of mothers (77.9%) reported positive perception in a recent study by Adedire et al in the Southwest Nigerian City33,34 Moreover another community-based, cross-sectional study conducted in Northeast Ethiopia found that mothers’ satisfaction with child immunization services was higher than that reported in earlier surveys21 However, a study in Egypt reported that most mothers had inadequate knowledge about childhood immunization, with only 0.3% reporting good knowledge.8 Similarly, a study conducted in rural areas of Nigeria aimed to assess how mothers perceived recovery and satisfaction levels following the treatment of childhood febrile conditions by patent medicine dealers, although the study did not place emphasis on childhood immunization.35 Therefore, it is important to note that parental education and practice play a significant role in vaccine hesitancy and acceptance.
These differences across studies could also be explained by population sociodemographic characteristics such as education and income. We found that nearly 90% of the participants believed that childhood vaccines prevent childhood diseases, especially severe illnesses. Our results are supported by studies by Kuruvilla et al in India and other authors.32,36,37 On the other hand, more than one-third of participants expressed concerns about the side effects of childhood vaccines, and only 58.5% disagreed with the negative statement, “children do not need a vaccine for diseases that are not common anymore”. Some researchers have reported the re-emergence of previously controlled severe and deadly vaccine-preventable diseases, including in developed nations, where efficient vaccination facilities are available.38–40 Possible reasons for this trend could include anti-vaccine beliefs, vaccine hesitancy, increased travel across countries, and varying perceptions toward vaccines.31,40,41 The critical negative perception identified regarding the necessity of vaccines for well-controlled diseases could potentially lead to mothers and caretakers delaying or avoiding the vaccines against the diseases, that are not currently common in the KSA.
Our present study revealed that vaccine hesitancy was significantly associated with the mother’s age, education, and the source of immunization information received. Similar to the results of our study, Aldakhil et al reported that education was a significant predictor of vaccine hesitancy. The authors also found that the source of information was another factor associated with vaccine hesitancy. A qualitative study conducted by Dube et al in Canada reported that nearly half of the participants were hesitant about vaccines. Although they decided to proceed with their children’s vaccination according to the schedule, they continued to question the effectiveness and consequences of the vaccine.42 In Singapore, the level of trust in children’s doctors was identified as the most influential factor in determining vaccine hesitancy among parents. A multinomial logistic regression model that examined variables such as sex, household income status, and vaccine history enabled the prediction of vaccine hesitancy in parents with a 70% accuracy rate, while non-vaccine hesitancy could be predicted with an accuracy rate of 92.4%.43
Client satisfaction is vital for the utilization of health services, including vaccination services provided at healthcare facilities. The present study found that 87.4% of the participants were satisfied with the immunization services provided at the PHCs of Hafr Al Batin, KSA. Similar to the present study, a survey conducted by El Gammal in Egypt and Schempf et al in the USA reported high levels of satisfaction.8,44 However, some surveys conducted in developing and underdeveloped countries have reported lower satisfaction among beneficiaries.12,21,45 Interestingly a lower proportion (75.9%) of satisfaction (partially and fully) was observed by Shati et al in 2021 among parents attending the well-baby clinic (including the immunization clinic) at the PHCs of Abha city, KSA.46 We also found that participants’ satisfaction was significantly associated with the age group of immunized and the mother’s occupational status. Furthermore, we found a positive correlation with mothers’ attitude with the satisfaction score (p <0.001). Similar to the present study, Debela et al found that mothers with favorable attitude and perceptions demonstrated a significantly higher level of satisfaction with the immunization services provided at the PHCs.21 Healthcare providers play a significant role in vaccine administration and in communicating the benefits, potential side effects, and follow-up advice for childhood vaccines, as stated by the Centers for Disease Control and Prevention, USA.47 The present study found that the lowest level of satisfaction was noted for follow-up advice regarding potential adverse effects and their management by healthcare providers, as well as for healthcare providers’ consideration of mothers’ concerns about vaccination. Considering that more than half (54.5%) of the participants in our study received childhood vaccination-related information from the healthcare providers through the Ministry of Health activities, the low level of satisfaction is vital for the policymakers to consider necessary proactive measures. Our study findings are supported by a recent mixed-method survey conducted by Ebi et al in Switzerland.13 Furthermore, a study found that an overwhelming majority of the participants (90%) recognized the importance of receiving the recommended vaccines for themselves and their children (p < 0.001). Additionally, 92% expressed confidence in the safety of vaccines for their children (p < 0.001), and 91% were willing to ensure that their newborns received all the recommended vaccine doses (p < 0.001). Moreover, 86% of the participants welcomed mass/school vaccination campaigns (p < 0.001), and 81% were willing to pay for additional vaccines for both themselves and their children (p < 0.001).18 These findings are consistent with our study’s findings, indicating a low level of vaccine hesitancy in Saudi Arabia, with a predominantly positive attitude toward vaccination among the participants. This study found a significant positive relationship (Spearman’s rho = 0.207, p < 0.001) between perception and satisfaction scores. However, 20.7% of the participants exhibited hesitancy regarding the provision of recommended childhood vaccines. Therefore, two major recommendations are emerged: to enhance communication and education efforts tailored to different age groups to bolster parental satisfaction with immunization services, and to implement targeted interventions to address vaccine hesitancy and its underlying causes, promoting informed decision-making among parents.
Strengths and Limitations of the Study
The present study is one of the first of its kind in the eastern province of the KSA. We employed a standardized and validated data collection tool gathering insights from 675 participants to analyze and report the findings. Nonetheless, it is essential to acknowledge some limitations of this study that need to be noted while interpreting our findings. Firstly, the current satisfaction survey was conducted exclusively among mothers in the eastern province of the KSA. Therefore, it is not possible to generalize the results to the entire KSA or other middle east countries. Secondly, this cross-sectional study sought to establish associations between maternal satisfaction and other factors, not causation. Finally, the potential for biases associated with self-reported surveys cannot be overlooked.
Conclusion
In general, mothers in eastern Saudi Arabia exhibited high levels of satisfaction with the immunization services provided at the PHCs. However, a lower level of satisfaction was observed concerning follow-up advice and concerns regarding potential side effects. Maternal perceptions regarding childhood vaccines displayed a positive correlation with the vaccination services provided at the PHCs. Notably, we identified a higher level of disagreement concerning the necessity of vaccines given by the Ministry of Health for diseases that are currently well-controlled. Hence, we recommend focused programs aimed at educating mothers about the importance of all childhood vaccines recommended by the Ministry of Health, KSA. The present survey findings underscore the necessity of regular training programs for healthcare providers operating at vaccination centers. Finally, there is a clear necessity for an exploratory, mixed-method survey focusing on childhood immunization satisfaction in other regions of the KSA.
Acknowledgments
We wish to thank the mothers for participating in the survey. We extend our sincere thanks to the Hafr Al Batin Health Affairs for their immense support to complete the research. We extend Dr.Ibtisam Qazi, Jouf University for her support in completing survey.
Funding
This work was funded by the Deanship of Scientific Research at Jouf University through the Fast-track Research Funding Program.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Vaccines and immunization. World Health Organization; 2022. Available from: https://www.who.int/health-topics/vaccines-and-immunization.
2. Greenwood B. The contribution of vaccination to global health: past, present and future. Philos Trans R Soc Lond B Biol Sci. 2014;369(1645):20130433. doi:10.1098/rstb.2013.0433
3. UNICEF. Immunization Programme. United Nations Children’s Fund; 2022. Available from: https://www.unicef.org/immunization.
4. Nandi A, Shet A. Why vaccines matter: understanding the broader health, economic, and child development benefits of routine vaccination. Hum Vaccin Immunother. 2020;16(8):1900–1904. doi:10.1080/21645515.2019.1708669
5. MacDonald NE. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–4164. doi:10.1016/j.vaccine.2015.04.036
6. Lakunina S. 1036 Parental Perception of Childhood Vaccinations. BMJ Publishing Group Ltd and Royal College of Paediatrics and Child Health. https://adc.bmj.com/content/106/Suppl_1/A201.1.citation-tools.
7. GebreEyesus FA, Assimamaw NT, GebereEgziabher NT, Shiferaw BZ. Maternal satisfaction towards childhood immunization service and its associated factors in Wadla District, North Wollo, Ethiopia, 2019. Int J Pediatr. 2020;3715414. doi:10.1155/2020/3715414
8. El Gammal HA. Maternal satisfaction about childhood immunization in primary health care center, Egypt. Pan Afr Med J. 2014;18:157. doi:10.11604/pamj.2014.18.157.1773
9. Al Saffer Q, Al-Ghaith T, Alshehri A, et al. The capacity of primary health care facilities in Saudi Arabia: infrastructure, services, drug availability, and human resources. BMC Health Serv Res. 2021;21(1):365. doi:10.1186/s12913-021-06355-x
10. Al Asmri M, Almalki MJ, Fitzgerald G, Clark M. The public health care system and primary care services in Saudi Arabia: a system in transition. East Mediterr Health J. 2020;26(4):468–476. doi:10.26719/emhj.19.049
11. Thirunavukkarasu A, Alotaibi NH, Al-Hazmi AH, et al. Patients’ perceptions and satisfaction with the outpatient telemedicine clinics during COVID-19 Era in Saudi Arabia: a cross-sectional study. Healthcare. 2021;9(12). doi:10.3390/healthcare9121739
12. Dana E, Asefa Y, Hirigo AT, Yitbarek K. Satisfaction and its associated factors of infants’ vaccination service among infant coupled mothers/caregivers at Hawassa city public health centers. Hum Vaccin Immunother. 2021;17(3):797–804. doi:10.1080/21645515.2020.1790278
13. Ebi SJ, Deml MJ, Jafflin K, et al. Parents’ vaccination information seeking, satisfaction with and trust in medical providers in Switzerland: a mixed-methods study. BMJ Open. 2022;12(2):e053267. doi:10.1136/bmjopen-2021-053267
14. Prakash B. Patient satisfaction. J Cutan Aesthet Surg. 2010;3(3):151–155. doi:10.4103/0974-2077.74491
15. Gonzalez ME. Improving customer satisfaction of a healthcare facility: reading the customers’ needs. Benchmark Inter J. 2019;26(3):854–870. doi:10.1108/BIJ-01-2017-0007
16. Alshammari TM, Subaiea GM, Hussain T, Moin A, Yusuff KB. Parental perceptions, attitudes and acceptance of childhood immunization in Saudi Arabia: a cross sectional study. Vaccine. 2018;36(1):23–28. doi:10.1016/j.vaccine.2017.11.050
17. Alsubaie SS, Gosadi IM, Alsaadi BM, et al. Vaccine hesitancy among Saudi parents and its determinants: result from the WHO SAGE working group on vaccine hesitancy survey tool. Saudi Med J. 2019;40(12):1242. doi:10.15537/smj.2019.12.24653
18. Alaamri O, Okmi EA, Suliman Y. Vaccine hesitancy in Saudi Arabia: a cross-sectional study. Tropical Medicine Infect Dis. 2022;7(4):60. doi:10.3390/tropicalmed7040060
19. Alsuhebany N, Alowais SA, Aldairem A, et al. Identifying gaps in vaccination perception after mandating the COVID-19 vaccine in Saudi Arabia. Vaccine. 2023;41(24):3611–3616. doi:10.1016/j.vaccine.2023.04.057
20. UNICEF. New data indicates declining confidence in childhood vaccines of up to 44 percentage points in some countries during the COVID-19 pandemic; 2023. Available from: https://www.unicef.org/rosa/press-releases/new-data-indicates-declining-confidence-childhood-vaccines-44-percentage-points-some.
21. Debela BG, Negassa B, Hareru HE, Sisay D, Soboksa NE. Maternal satisfaction on child immunization services of rural health extension workers in Dawie Harewa district, Northeast Ethiopia: a community based cross-sectional study. Envir Chall. 2022;7:100455. doi:10.1016/j.envc.2022.100455
22. Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesth. 2017;11(Suppl 1):S80–s89. doi:10.4103/sja.SJA_203_17
23. AlAjmi M, Al-Ghamdi S. Translation and validation of the Arabic version of the osteoarthritis quality of life questionnaire (OAQoL) in Saudi patients with osteoarthritis. Health Qual Life Outcomes. 2021;19(1):91. doi:10.1186/s12955-021-01741-9
24. Domek GJ, O’Leary ST, Bull S, et al. Measuring vaccine hesitancy: field testing the WHO SAGE working group on vaccine hesitancy survey tool in Guatemala. Vaccine. 2018;36(35):5273–5281. doi:10.1016/j.vaccine.2018.07.046
25. Shapiro GK, Tatar O, Dube E, et al. The vaccine hesitancy scale: psychometric properties and validation. Vaccine. 2018;36(5):660–667. doi:10.1016/j.vaccine.2017.12.043
26. Nour R, Powell L, Alnakhi WK, et al. Adult vaccine hesitancy scale in Arabic and French: protocol for translation and validation in the world health organization eastern Mediterranean region. JMIR Res Protoc. 2019;11(4):e36928. doi:10.2196/36928
27. Aldakhil H, Albedah N, Alturaiki N, Alajlan R, Abusalih H. Vaccine hesitancy towards childhood immunizations as a predictor of mothers’ intention to vaccinate their children against COVID-19 in Saudi Arabia. J Infect Public Health. 2021;14(10):1497–1504. doi:10.1016/j.jiph.2021.08.028
28. Thirunavukkarasu A, Alharbi MS, Salahuddin M, et al. Evaluation of oral health-related quality of life and its association with mental health status of patients with type 2 diabetes mellitus in the post-COVID-19 pandemic era: a study from Central Saudi Arabia. Front Public Health. 2023;11:1158979. doi:10.3389/fpubh.2023.1158979
29. Rodríguez-Herrera C, López-Jiménez JJ, Del Toro-Valero A, et al. The Newcastle satisfaction with nursing scales in a Mexican oncology hospital. Afr Health Sci. 2021;21(1):60–66. doi:10.4314/ahs.v21i1.10
30. Fakonti G, Hadjikou A, Tzira E, Kyprianidou M, Giannakou K. Attitudes and perceptions of mothers towards childhood vaccination in Greece: lessons to improve the childhood COVID-19 vaccination acceptance. Front Pediatr. 2022;10:951039. doi:10.3389/fped.2022.951039
31. Bussink-Voorend D, Hautvast JLA, Vandeberg L, Visser O, Mejl H. A systematic literature review to clarify the concept of vaccine hesitancy. Nature Hum Behav. 2022;6(12):1634–1648. doi:10.1038/s41562-022-01431-6
32. Alshammari SZ, AlFayyad I, Altannir Y, Al-Tannir M. Parental awareness and attitude about childhood Immunization in Riyadh, Saudi Arabia: a cross-sectional study. Int J Environ Res Public Health. 2021;18(16):8455. doi:10.3390/ijerph18168455
33. Adedire EB, Ajumobi O, Bolu O, Nguku P, Ajayi I. Maternal knowledge, attitude, and perception about childhood routine immunization program in Atakumosa-west Local Government Area, Osun State, Southwestern Nigeria. Pan Afr Med J. 2021;40(Suppl 1):8. doi:10.11604/pamj.supp.2021.40.1.30876
34. GebreEyesus FA, Assimamaw NT, GebereEgziabher NT, Shiferaw BZ. Maternal satisfaction towards childhood immunization service and its associated factors in Wadla District. North Wollo Ethiopia. Int J Pediatr. 2019;2019:1–13.
35. Ibeneme GC, Nwaneri AC, Ibeneme SC, et al. Mothers’ perception of recovery and satisfaction with patent medicine dealers’ treatment of childhood febrile conditions in rural communities. Malar J. 2016;15(1):1–9. doi:10.1186/s12936-016-1384-5
36. Kuruvilla BS, Cherian V, Thomas AM, Rose BM, John A. Perceptions regarding childhood immunization among mothers in Kunnukara Panchayat, North Paravur, Ernakulam, Kerala. Int j Community Med Public Health. 2021;8(7):3506. doi:10.18203/2394-6040.ijcmph20212610
37. McNeil DA, Mueller M, MacDonald S, et al. Maternal perceptions of childhood vaccination: explanations of reasons for and against vaccination. BMC Public Health. 2019;19(1):49. doi:10.1186/s12889-018-6338-0
38. Raslan R, El Sayegh S, Chams S, Chams N, Leone A, Hajj Hussein I. Re-emerging vaccine-preventable diseases in war-affected peoples of the eastern Mediterranean region-an update. Front Public Health. 2017;5:283. doi:10.3389/fpubh.2017.00283
39. Dixon MG, Ferrari M, Antoni S, et al. Progress toward regional measles elimination—worldwide, 2000–2020. MMWR. 2021;70(45):1563. doi:10.15585/mmwr.mm7045a1
40. Hotez P. America and Europe’s new normal: the return of vaccine-preventable diseases. Pediatr Res. 2016;85(7):912–914. doi:10.1038/s41390-019-0354-3
41. Feldman AG, O’Leary ST, Danziger-Isakov L. The risk of resurgence in vaccine-preventable infections due to coronavirus disease 2019-related gaps in immunization. Clin Infect Dis. 2021;73(10):1920–1923. doi:10.1093/cid/ciab127
42. Dubé E, Vivion M, Sauvageau C, Gagneur A, Gagnon R, Guay M. “Nature does things well, why should we interfere?”: Vaccine hesitancy among mothers. Qual Health Res. 2016;26(3):411–425. doi:10.1177/1049732315573207
43. Low JM, Soo CWT, Phuong T, Zhong Y, Lee LY. Predicting vaccine hesitancy among parents towards COVID-19 vaccination for their children in Singapore. Front Pediatr. 2022;10:994675. doi:10.3389/fped.2022.994675
44. Schempf AH, Minkovitz CS, Strobino DM, Guyer B. Parental satisfaction with early pediatric care and immunization of young children: the mediating role of age-appropriate well-child care utilization. Arch Pediatr Adolesc Med. 2007;161(1):50–56. doi:10.1001/archpedi.161.1.50
45. Hussain A, Zahid A, Malik M, et al. Assessment of parents’ perceptions of childhood immunization: a cross-sectional study from Pakistan. Children. 2021;8(11):1007. doi:10.3390/children8111007
46. Shati AA, Al-Saleh MM, Al-Asmari BA, et al. Awareness and perception of parents regarding well baby clinic in primary health care centres in Abha City, Southwestern Saudi Arabia. J Family Med Prim Care. 2021;10(9):3464–3469. doi:10.4103/jfmpc.jfmpc_871_21
47. CDC. Provider’s role in importance of vaccine administration and storage. Centers for Disease Control and Prevention; 2022. Available from: https://www.cdc.gov/vaccines/hcp/admin/storage/providers-role-vacc-admin-storage.html.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Job Motivation and Satisfaction Among Female Pharmacists Working in Private Pharmacy Professional Sectors in Saudi Arabia
Al-Omar HA, Khurshid F, Sayed SK, Alotaibi WH, Almutairi RM, Arafah AM, Mansy W, Alshathry S
Risk Management and Healthcare Policy 2022, 15:1383-1394
Published Date: 21 July 2022
Patients’ Perceptions on Community Pharmacy Services of a Ward (10) of Kathmandu Metropolitan
Ojha A, Bista D, KC B
Patient Preference and Adherence 2023, 17:1487-1499
Published Date: 21 June 2023
Saudi Women’s Views on Healthcare Leadership in the Era of Saudi 2030 Health Transformation
Aldekhyyel RN, Alhumaid N, Alismail DS
Journal of Multidisciplinary Healthcare 2024, 17:237-249
Published Date: 16 January 2024
Knowledge and Perception Towards Psychotropic Drugs Among the General Population in Saudi Arabia
Al-Shareef EM, Kadah Salim AM, Al-Farrah NM, Al-Murad BM, Moallem AA, Radwan MA, Hakami S, Alshanberi AM, Shaikhomer M, Alsanosi SM
Psychology Research and Behavior Management 2024, 17:3543-3553
Published Date: 15 October 2024
Privatization of Healthcare Services from the Nursing Perspective in the Kingdom of Saudi Arabia: A Cross-Sectional Study
Al-Sadoun AS, Al-Otaibi NO, Al-Ahmari HH, Adawi DO, Al-Dalbahi LM, Tumala RB
Journal of Multidisciplinary Healthcare 2025, 18:5817-5831
Published Date: 13 September 2025