Back to Journals » Nutrition and Dietary Supplements » Volume 18
Maternal Nutrition Security in Afghanistan: A Case Study in the Global Hunger Crisis
Authors Fayez SM ![]()
Received 19 February 2026
Accepted for publication 29 June 2026
Published 30 June 2026 Volume 2026:18 604269
DOI https://doi.org/10.2147/NDS.S604269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Mohammed S. Razzaque
Sayed Mortaza Fayez
Department of Nutrition, Medicine School, Kabul University of Medical Sciences Ali Ibn Sina, Kabul, Afghanistan
Correspondence: Sayed Mortaza Fayez, Email [email protected]
Abstract: Afghanistan’s maternal nutrition crisis epitomizes the intersection of conflict, systemic collapse, and entrenched gender inequality within the global hunger emergency. Nearly one‑third of Afghan women of reproductive age are underweight, while 45% of pregnant women suffer from anemia, driving one of the world’s highest child stunting rates at 41%. These stark figures reveal overlapping macronutrient and micronutrient deficiencies, compounded by food contamination, poor supplement quality, and restrictive socio‑cultural norms. The December 2022 ban on female NGO workers dismantled the primary channel of care delivery in a gender-segregated society; moreover, wider restrictions on women’s participation in civic space, education, and public life have further exacerbated humanitarian vulnerability and limited access to care. These interconnected rights restrictions underscore how systemic gender inequality intensifies humanitarian need. The human cost is measured in elevated maternal mortality, impaired child development, and communities locked in cycles of poverty and poor health. Evidence‑based interventions such as community‑based malnutrition management and fortified food distribution remain effective but are paralyzed by political and operational barriers. Afghanistan’s case highlights urgent lessons for global strategy: gender equality as foundational, systems strengthening as essential, food safety and quality as non-negotiable, and local data as critical for adaptation. Ultimately, maternal nutrition security in Afghanistan is both a humanitarian imperative and a critical measure of international resolve to confront structural barriers and uphold human rights in ending hunger.
Keywords: Afghanistan, maternal nutrition, food insecurity, hunger crisis, maternal health
Introduction
Hunger is a pervasive global crisis, but its most severe manifestations are acutely localized. Afghanistan exemplifies this reality, serving as a devastating microcosm of how conflict, systemic collapse, and gender inequality converge to catastrophically undermine food and nutrition security. The erosion of maternal nutrition in particular represents one of the world’s most severe humanitarian threats, driving intergenerational cycles of mortality, impaired development, and poverty.1,2 Climate-related shocks, including recurrent drought and food system disruptions, have further exacerbated food insecurity in Afghanistan.3,4 Additionally, mental health and psychosocial stress in conflict settings intensify maternal nutritional vulnerability, as chronic anxiety and depression can reduce dietary intake and care-seeking behavior.5
The objective of this paper is to examine Afghanistan’s maternal nutrition crisis as a case study within the global hunger emergency, identify the multifaceted structural drivers, and draw lessons for humanitarian policy and practice.
Methods
This manuscript is a narrative case study based on secondary analysis of existing literature, humanitarian reports, and publicly available nutrition surveys. No primary data collection or statistical analysis was conducted.
Data Sources and Search Strategy
We consulted peer-reviewed articles (via PubMed, Google Scholar, and Scopus), United Nations agency reports (FAO, WHO, UNICEF, WFP), and Afghan government health surveys (including the Afghanistan Demographic and Health Survey where available). The search focused on studies and reports published between 2015 and 2025, with priority given to Afghanistan-specific data. Search terms included combinations of the following keywords: “Afghanistan AND maternal nutrition”, “food insecurity AND women”, “anemia AND pregnancy AND Afghanistan”, “child stunting AND conflict”, “gender inequality AND humanitarian access”, and “nutrition interventions AND low-income countries”. A total of 47 reports and studies were screened; of these, 22 met inclusion criteria and were included in the synthesis. For conflicting evidence, priority was given to sources with larger sample sizes, more recent data collection, and transparent methodological reporting.
Inclusion Criteria
Sources were included if they reported quantitative nutrition indicators (eg, underweight, anemia, stunting) among Afghan women or children, described structural determinants (conflict, gender inequality, health system collapse), or evaluated nutrition interventions in similar settings.
Synthesis Approach
Data were extracted and organized thematically around prevalence estimates, causal factors (conflict, gender, food safety, cultural norms), intervention effectiveness, and barriers to implementation. The manuscript does not perform meta-analysis but instead synthesizes findings narratively to inform policy discussion.
Results
The Scale of the Crisis: Local Data, Global Patterns
The statistics from Afghanistan present a stark portrait of nutritional deprivation, mirroring trends seen in other crisis-affected states. Nationally, approximately 29% of women of reproductive age are underweight, a clear marker of chronic energy deficit.6 Nearly 45% of pregnant women suffer from anemia, predominantly due to iron deficiency, significantly increasing their risk of hemorrhage and death during childbirth.7 These deficiencies contribute directly to one of the world’s highest rates of child stunting at 41%, a physical testament to a malnourished foundation. These overlapping macronutrient and micronutrient shortfalls including vitamin A and iodine deficiencies are a pattern repeated across low-income and conflict-affected countries.8 These alarming statistics, however, reflect deeper structural and systemic factors that perpetuate nutritional deprivation. Summary of key nutritional indicators in Afghanistan was presented in (Table 1).
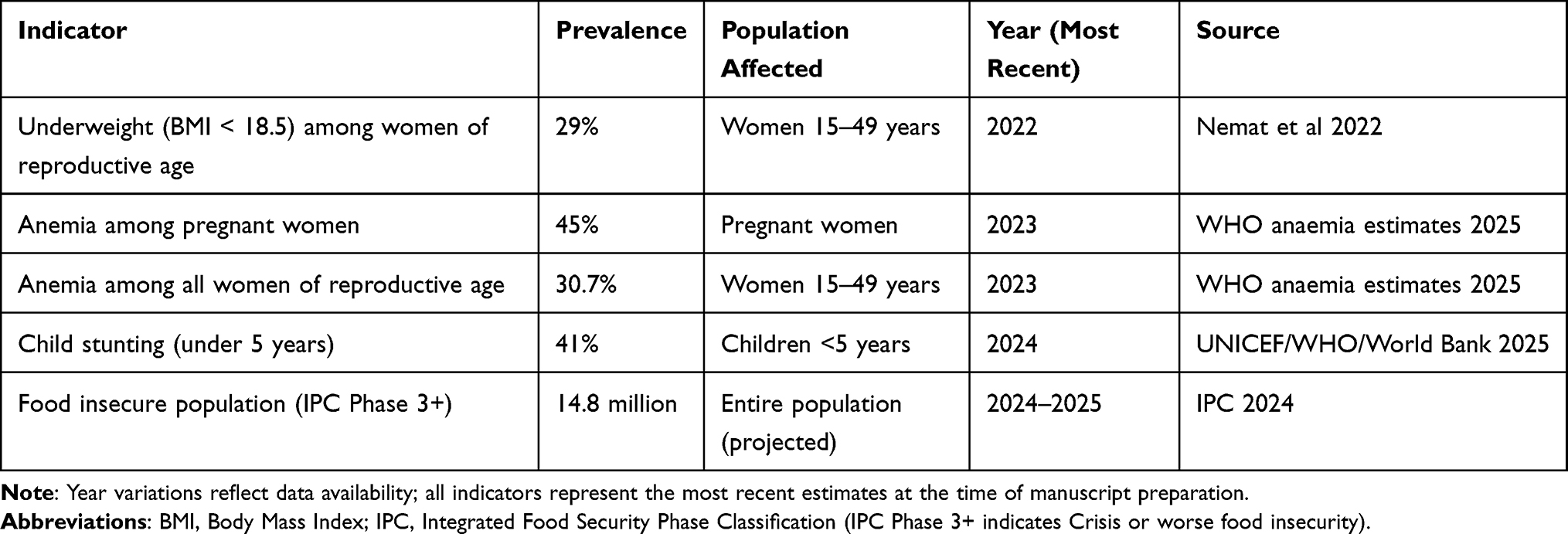 |
Table 1 Summary of Key Nutritional Indicators in Afghanistan |
Multifaceted Causes: A Syndemic of Risk
The drivers of this crisis are interconnected, reflecting global challenges:
Conflict and Systemic Collapse
Decades of war have decimated infrastructure. The political transition of August 2021 led to the collapse of a donor-dependent health system, gutting the implementation of policies like the National Nutrition Strategy.9,10 The December 2022 ban on female NGO workers severed the primary channel for delivering care to women in a gender-segregated society, a unique but instructive example of how rights restrictions exacerbate humanitarian need.
Food Safety and Quality
Beyond quantity, food quality is a critical issue. Staple crops are frequently contaminated with aflatoxins due to poor storage, posing chronic health risks.11 Even interventions are compromised; supply chain breakdowns lead to the distribution of expired or substandard iron-folic acid supplements.12
Socio-Cultural Norms
Deeply entrenched practices amplify biological risk. Intra-household food allocation often prioritizes men, directly disadvantaging women and girls. Early marriage, closely spaced pregnancies, and food taboos during pregnancy deplete maternal reserves, while low female literacy limits health information uptake.13
Impact: The Human Cost
The impact is measured in human suffering: increased maternal and infant mortality, children whose cognitive and physical potential is permanently diminished by stunting, and communities trapped in a cycle where malnutrition begets poverty and poor health. This dire outcome is not for lack of known solutions but because of barriers to their delivery.
Beyond immediate mortality, maternal malnutrition imposes long-term developmental consequences: children born to undernourished mothers have lower educational attainment and reduced lifetime earnings, perpetuating intergenerational poverty. The economic cost of stunting in Afghanistan is estimated at millions of dollars annually in lost productivity, though precise figures remain unavailable due to data gaps.
Discussion
The findings presented above demonstrate that maternal malnutrition in Afghanistan is not merely a consequence of food scarcity but a syndemic driven by conflict, gender inequality, health system collapse, and environmental shocks. These drivers do not operate in isolation; for example, the ban on female NGO workers directly prevents delivery of iron supplements to pregnant women, which in turn increases anaemia prevalence and post-partum haemorrhage risk. Biologically, chronic energy deficit among women of reproductive age reduces physiological reserves, raising maternal mortality by an estimated 20–30% in similar settings.14 Likewise, anaemia triples the risk of maternal death from haemorrhage. At the population level, stunting (41% prevalence) permanently lowers cognitive development and lifetime earnings, perpetuating intergenerational poverty.15
Climate change, specifically recurrent drought, has further reduced food availability and intensified displacement, as shown by the 2024–2025 IPC projections. Donor dependency and international sanctions have crippled the health system: by September 2023, the UN humanitarian appeal for Afghanistan was only 27% funded. These structural barriers are often overlooked in technical nutrition programmes.16,17
Long-term solutions require addressing political and gender-based barriers, not merely delivering supplements. The Afghan case offers transferable lessons for other conflict-affected settings: gender-sensitive humanitarian access, climate-adaptive food systems, and sustained funding regardless of political transitions.
Limitations
As a narrative review, this paper is subject to selection bias and does not provide causal inference. Where recent Afghanistan-specific data were unavailable (2019–2025), we note this as a gap. The search strategy, while systematic, may have missed relevant grey literature or non-English sources. Additionally, the rapidly evolving political situation in Afghanistan means that some findings may require updating as new data become available. Causal claims in this manuscript should therefore be interpreted cautiously.
Evidence-Based Solutions and Paralyzing Barriers
Past program data from Afghanistan and similar contexts shows that interventions like Community-Based Management of Acute Malnutrition (CMAM), fortified food distributions, and consistent antenatal supplementation are effective.18 However, their current feasibility is crippled by political and operational barriers. The central challenge is no longer what works, but how to deliver it safely and equitably to women when female workers are banned and health systems are fragmented.
Connecting to Global Action: Lessons for Worldwide Strategy
Afghanistan’s struggle underscores several non-negotiable principles for global hunger strategies:
- Gender Equality is Foundational: Protecting and enabling female health workers is not ancillary; it is central to effective humanitarian action in restrictive settings.
- Systems Strengthening is Key: Long-term nutrition security depends on resilient, integrated health, agriculture, and social protection systems.
- Safety & Quality Matter: Responses must address not just calorie counts but also food safety (eg, mycotoxin monitoring) and supplement quality.
- Local Data Drives Adaptation: Investing in context-specific operational research is essential to adapt interventions under severe constraints.
Conclusion
Maternal nutrition insecurity in Afghanistan is not solely the result of food scarcity but also of entrenched political instability, restricted humanitarian access, and systemic gender-based inequalities. The crisis highlights a broader global failure to protect vulnerable populations during prolonged conflict and economic collapse. While technical and nutritional interventions remain important, they cannot succeed without the political commitment necessary to safeguard human rights, ensure access to healthcare, and protect frontline humanitarian workers.
Governments, donors, and international organizations must therefore move beyond emergency food distribution toward comprehensive systems-based interventions that strengthen healthcare delivery, women’s education, economic participation, and community resilience. Policymakers should prioritize funding mechanisms that remain operational despite political transitions; humanitarian agencies must develop contingency protocols for delivering care when female workers are restricted; and donor governments should condition aid on the protection of women’s access to healthcare and nutrition services. Policies that empower women in decision-making processes and improve maternal access to essential health and nutrition services are fundamental to achieving sustainable outcomes for mothers and children.
The lessons from Afghanistan are clear: ending hunger requires global solidarity and coordinated action capable of confronting the political and gender-based barriers that transform scarcity into humanitarian catastrophe. Rebuilding maternal nutrition security in Afghanistan is therefore not only a humanitarian imperative but also a critical test of the international community’s commitment to achieving a world free from hunger.
Future research should prioritize context-specific operational studies that evaluate culturally adapted nutrition interventions, examine the long-term developmental impacts of maternal malnutrition, and assess the role of climate adaptation in strengthening food and nutrition security.
Funding
No Funding received.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Sotiraki M, Malliou A, Tachirai N, et al. Burden of childhood malnutrition: a roadmap of global and European policies promoting healthy nutrition for infants and young children. Children. 2022;9(8):1179. doi:10.3390/children9081179
2. Shruthi S, Govindarajan P, Shalini SR, Antony PJ, Uma AN, Rangarajan L. RISE: a novel unified framework for feature relevance in malnutrition analytics integrating statistical and expert insights. Front Public Health. 2025;13:1663373. doi:10.3389/fpubh.2025.1663373
3. Mobariz AH. Climatic Disaster Impacts on Displacement in Afghanistan. Washington, DC: Georgetown University; 2025.
4. Safi L, Mujeeb M, Sahak K, Mushwani H, Hashmi SK. Climate change impacts and threats on basic livelihood resources, food security and social stability in Afghanistan. GeoJournal. 2024;89(2):85. doi:10.1007/s10708-024-11077-8
5. Zahidi F, Khalid M, Surkan PJ, Azadbakht L. Associations between food insecurity and common mental health problems among reproductive-aged women in Kabul-Afghanistan. Front Nutr. 2022;8. doi:10.3389/fnut.2021.794607
6. Nemat O, Diwakar V, Ghafoori I, Azadmanesh S. Livelihoods and welfare amidst layered crises in Afghanistan. 2022.
7. World Health Organization. Report of the eleventh meeting of the WHO strategic and technical advisory group of experts for maternal, newborn, child, and adolescent health and nutrition. World Health Organization; 2025.
8. UNICEF. Malnutrition in Mothers soars by 25 percent in crisis-hit countries, putting women and newborn babies at risk. New York; 2023.
9. Salehi AS, Akseer N. Islamic Republic of Afghanistan Ministry of Public Health. 2020.
10. Azzahrah AK, Yumitro G. Analyzing the role of the United Nations in facing Taliban restriction women’s education in Afghanistan 2021. Indones J Int Relat. 2025;9(1):97–5. doi:10.32787/ijir.v9i1.599
11. Mesfin A, Lachat C, Vidal A, et al. Essential descriptors for mycotoxin contamination data in food and feed. Food Res Int. 2022;152:110883. doi:10.1016/j.foodres.2021.110883
12. Kim C, Mansoor GF, Paya PM, et al. Review of policies, data, and interventions to improve maternal nutrition in Afghanistan. Matern Child Nutr. 2020;16(4):e13003. doi:10.1111/mcn.13003
13. Handbook S. Humanitarian charter and minimum standards in humanitarian response. 2018.
14. Faizi A, Sohi P. The impact of prenatal care on maternal mortality among women aged 15 to 49 in Afghanistan. Int J Contemp Med Res. 2025;3(2):55.
15. Oresnik S, Moffat T, McKerracher L, Sloboda DM. A syndemic perspective on food insecurity, gestational diabetes, and mental health disorders during pregnancy. Soc Sci Med. 2025;373:117994. doi:10.1016/j.socscimed.2025.117994
16. Hadley K, Wheat S, Rogers HH, et al. Mechanisms underlying food insecurity in the aftermath of climate-related shocks: a systematic review. Lancet Planet Health. 2023;7(3):e242–e50. doi:10.1016/S2542-5196(23)00003-7
17. Network AA, van Bijlert M, Team A. Food Aid in a Collapsed Economy: relief, tensions and allegations. 2022.
18. Sharma J, Ludin H, Chauhan M, Zodpey S. Public health nutrition in Afghanistan-policies, strategies and capacity-building: current scenario and initiatives. East Mediterr Health J. 2021;27(7):728–737. doi:10.26719/emhj.21.043
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.