Back to Journals » International Medical Case Reports Journal » Volume 17
Massive Airway Bleeding Caused by Pulmonary Strongyloidiasis in a Patient with a Transplanted Kidney
Authors Zhu L ![]() , Zhang H, Fang J, Xiao S, Xiong F, Deng C
, Zhang H, Fang J, Xiao S, Xiong F, Deng C ![]() , Yang Q, Fu C, Pan Q, Zhao H
, Yang Q, Fu C, Pan Q, Zhao H ![]()
Received 29 October 2023
Accepted for publication 26 December 2023
Published 3 January 2024 Volume 2024:17 Pages 1—7
DOI https://doi.org/10.2147/IMCRJ.S442535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Longyin Zhu,1,* Huhai Zhang,1,* Jia Fang,1 Shuang Xiao,2 Fu Xiong,3 Caixia Deng,3 Qin Yang,1 Chunxiao Fu,1 Qianguang Pan,1 Hongwen Zhao1
1Department of Nephrology, the First Hospital Affiliated to Army Military Medical University (Southwest Hospital), Chongqing, 400038, People’s Republic of China; 2Department of Infectious Disease, the First Hospital Affiliated to Army Military Medical University (Southwest Hospital), Chongqing, 400038, People’s Republic of China; 3Department of Respiratory and Critical Care Medicine, the First Hospital Affiliated to Army Military Medical University (Southwest Hospital), Chongqing, 400038, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongwen Zhao; Qianguang Pan, Email [email protected]; [email protected]
Introduction: We report a fatal case of massive airway bleeding caused by pulmonary strongyloidiasis in a patient with a transplanted kidney.
Case Presentation: A 47-year-old male, regularly taking immunosuppressants post-kidney transplant, visited our hospital with symptoms of abdominal bloating, nausea, and emesis persisting for three days. After hospitalization, he developed a cough, hemoptysis, and respiratory failure. Sputum analysis confirmed an infestation with Strongyloides stercoralis. Despite receiving albendazole therapy and bronchoscopic management for bronchial hemorrhage, the patient ultimately died due to acute respiratory and circulatory collapse triggered by severe airway bleeding.
Conclusion: Patients undergoing immunosuppressive therapy following kidney transplantation are at increased risk for disseminated strongyloidiasis. Consequently, infectious disease screening prior to transplantation, along with essential preventive pharmacotherapy, is of paramount importance.
Keywords: strongyloides stercoralis, kidney transplantation, airway bleeding, disseminated infection
Introduction
Organ transplantation is an important pathway for the transmission and infection of parasites, yet it is frequently overlooked.1 The modes of transmission are primarily threefold: firstly, the donor infected with parasites, leading to transmission via transplantation; secondly, the recipient, due to extensive use of immunosuppressive therapy postoperatively, may have latent infections activated; and thirdly, reduced postoperative immunity can facilitate infection through animal contact.2 Strongyloidiasis, caused by the Strongyloides stercoralis, typically presents with concealed symptoms and lacks specificity. Normally, the immune response can confine the infection, allowing an asymptomatic latency period lasting for decades.3 However, diminished immune function can activate the infection, resulting in disseminated infection, with the mortality rate reaching up to 85%-100% in the absence of timely treatment.4 We report a fatal case of massive airway bleeding caused by pulmonary strongyloidiasis in a patient with a transplanted kidney.
Case Report
On August 4, 2023, a 47-year-old male patient was admitted to the hospital with symptoms of nausea, emesis, and abdominal bloating that had persisted for 3 days. The patient had been diagnosed with uremia for 13 years and underwent kidney transplantation two months prior. Post-transplant, he was taking prednisone (20 mg orally once daily), tacrolimus (3 mg orally every 12 hours), and mycophenolate mofetil (0.5 g orally every 12 hours) as anti-rejection treatment as per doctor’s instructions, but he had not received any prophylaxis for Pneumocystis jiroveci pneumonia (PJP). In February 2021, he traveled to Guangdong, an area previously reported to have cases of strongyloidiasis. After returning home, he reported no discomfort. However, in April 2021, his eosinophilia increased to 2.53×109/L and returned to normal over six months without treatment. The patient reports no additional medical history, medication use, or surgical interventions, and there are no relevant family medical history entries requiring mention.
Upon admission, the patient exhibited stable vital signs, characterized by distinct coarse breath sounds in both lungs, slight tenderness in the upper left quadrant of the abdomen, and 7–8 bowel sounds per minute. No other positive signs were observed. The blood test showed the following: Complete blood count: white blood cell count was 5.34×109/L, hemoglobin was 91 g/L, lymphocyte count was 0.18×109/L, eosinophil count was 0.29×109/L; Procalcitonin level was 0.63 ng/mL; Renal function: Serum creatinine level was 283.4 μmol/L; No significant abnormalities were observed in liver function. The abdominal X-ray, conducted in both the standing and supine positions on August 4, indicated a partial accumulation of intestinal gas, with no other abnormalities detected. That same day, a chest computed tomography (CT) revealed widespread nodular opacities and patchy areas of increased density in both lungs (Figure 1A-D). Given the patient’s recent kidney transplantation and concurrent lung infection, the original medication was halted, and switched to Methylprednisolone (60 mg intravenously once daily) for anti-rejection, and Caspofungin (initial dose of 70 mg intravenously, followed by a maintenance dose of 50 mg daily) combined with Cefoperazone/Sulbactam (1.5 g intravenously every 12 hours) for anti-infection treatment was administered. Simultaneously, Omeprazole was used for gastric protection, and the patient’s gastrointestinal symptoms were alleviated on the same day.
 |
Figure 1 (A-D) Chest computed tomography revealed widespread nodular opacities and patchy areas of increased density in both lungs. |
However, on the night of August 4, the patient developed a cough, hemoptysis, but no symptoms such as chest pain, chest tightness, difficulty breathing, or fever. On August 5, the patient still had hemoptysis and developed symptoms of dyspnea and an elevated respiratory rate. Arterial blood gas (ABG) analysis showed a pH of 7.35, PaO2 at 71 mmHg, PCO2 at 29 mmHg, an oxygenation index of 192, and FiO2 at 37%, suggestive of respiratory failure. Consequently, non-invasive mechanical ventilation was initiated, employing Continuous Positive Airway Pressure (CPAP) mode. Combining the patient’s chest CT and medical history, it was considered that the patient could be suffering from PJP, thus sulfamethoxazole-trimethoprim (1.92g intravenously every 6 hours) for PJP was added to the treatment.
On August 7, sputum metagenomics next-generation sequencing (mNGS) revealed Escherichia coli with 40,668 sequence reads, Klebsiella pneumoniae with 3373 sequence reads, and Strongyloides stercoralis with 271,732 sequence reads (Figure 2). Simultaneously, Strongyloides stercoralis was seen in the sputum smear (Figure 3). Considering the patient’s chest CT more with Strongyloides stercoralis infection than with typical bacterial infection, and noting that neither white blood cell count nor procalcitonin levels showed significant elevation, it is believed that the primary concern is a Strongyloides stercoralis infection. Since Ivermectin was unavailable in the region, the patient was immediately given Albendazole (0.4g orally every 12 hours) for treatment, and the sulfamethoxazole-trimethoprim (0.96g orally once daily) dosage was adjusted to a preventive one. However, on the night of August 7th, the patient’s respiratory function deteriorated rapidly, with the oxygenation index dropping to 65. In order to administer effective oxygen therapy, the patient underwent tracheal intubation and invasive mechanical ventilation. After tracheal intubation, approximately 60 mL of bloody secretions were aspirated from the airway. We immediately performed a fiberoptic bronchoscopy and found a large amount of bloody secretions in the right bronchus, and partial blood clot blocking the bronchial lumen in the right lower lobe, suggesting active bleeding in the patient’s airway.
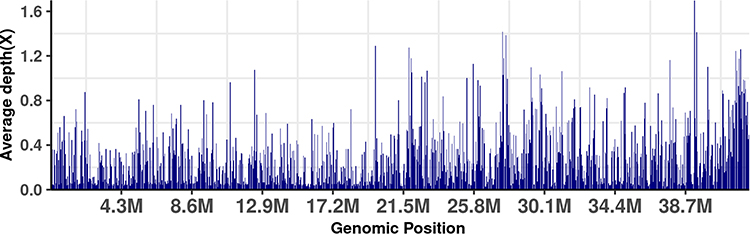 |
Figure 2 The coverage of Strongyloides stercoralis reads by metagenomics next-generation sequencing using sputum. |
 |
Figure 3 Microscopic examination of sputum shows Strongyloides stercoralis. Original magnification ×400. |
After successfully achieving hemostasis (a process involving the infusion of vasopressin and tranexamic acid, and the local instillation of a mixture of ice saline and adrenaline into the bleeding site under bronchoscopic guidance), the bronchial lumen was then cleared, with approximately 40 mL of bloody secretions removed. The hemoglobin level decreased from 75 g/L to 57 g/L. To address the anemia, 600 mL of red blood cells were transfused, and no fresh blood was observed flowing out on the same day.
However, on August 8th, approximately 60mL of bloody secretions were again aspirated from the patient’s airway. While supported by endotracheal mechanical ventilation (FIO2: 100%), the patient exhibited oxygen saturation levels fluctuating between 70% and 85%. Additionally, the patient’s heart rate fluctuated between 95 and 110 beats per minute, with a systolic blood pressure ranging from 80 to 100 mmHg and a diastolic blood pressure from 50 to 70 mmHg. These vital signs were observed while the patient was receiving norepinephrine at 1.5 µg/kg/min, epinephrine at 1 µg/kg/min, and metaraminol at 3 µg/kg/min. We suggested to the patient’s family that Extracorporeal Membrane Oxygenation (ECMO) treatment could be implemented. Due to financial constraints, the patient’s family declined further treatment, electing to proceed with same-day discharge. Unfortunately, follow-up data revealed that the patient experienced a rapid deterioration in health, leading to his demise at home on the day of discharge. The timeline illustrating progress of the case is shown in Figure 4.
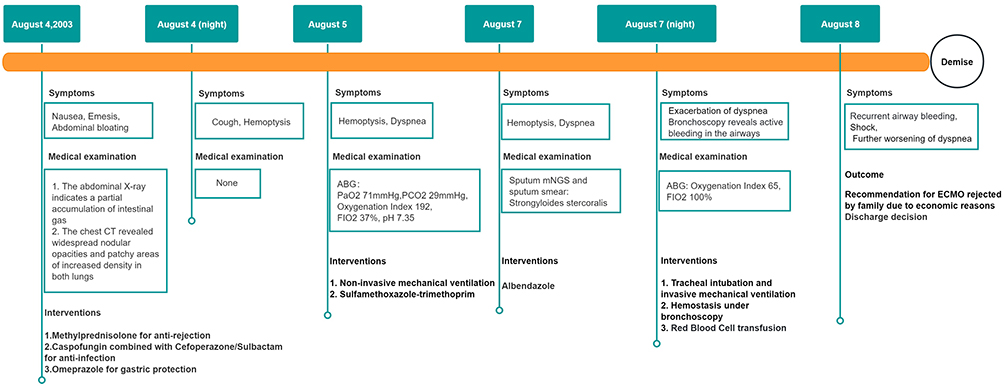 |
Figure 4 Case Progress Timeline. |
Discussion
Strongyloides stercoralis, a hermaphroditic parasite, primarily inhabits the small intestine of its host. Significantly, the parasite’s larvae can infiltrate various organs, including the lungs, brain, liver, and kidneys, thereby instigating strongyloidiasis.5 Markedly common in specific tropical and subtropical regions, this parasitic infection records morbidity rates near 30% in these endemic regions.6 While China has lower infection rates overall, cases have been documented in regions such as Guangdong, Guangxi, and Hainan.7,8 We document a case involving severe airway bleeding attributed to a Strongyloides stercoralis infection, ensuing two months subsequent to a kidney transplant. In the diagnosis and treatment of this case, precise and rapid diagnosis was made through mNGS, confirming the patient’s infection with Strongyloides stercoralis. However, due to the lack of ivermectin in the local area, which required ordering via express delivery taking three days to arrive, the patient could not receive first-line drug treatment in time. As a result, the patient’s condition rapidly deteriorated, leading to acute respiratory and circulatory failure. Due to financial reasons, the patient’s family ultimately gave up on further treatment.
Previous literature has reported cases of hemoptysis caused by hyperinfection.9–11 The patient in this case primarily exhibited gastrointestinal and respiratory symptoms, similar to those reported in previous cases.12,13 Notably, the initial symptoms of this patient included abdominal distension, nausea, and emesis. Unexpectedly, when respiratory symptoms developed, the gastrointestinal symptoms rapidly alleviated, a phenomenon not commonly seen in prior literature. The onset of airway bleeding might involve several mechanisms, which include both physical damage and inflammatory reactions caused by larvae in the pulmonary capillaries. Furthermore, the immune response induced by the Strongyloides stercoralis parasite in the host’s lungs can persist for an extended period, thereby constantly stimulating lung tissue to maintain an inflammatory reaction, resulting in continual damage.14 The onset of excessive hemoptysis could easily obstruct the airway, causing suffocation and presenting a life-threatening risk to the patient. As such, clinicians must pay close attention to such cases. We recommend including strongyloidiasis in the differential diagnosis of hemoptysis in patients who are on immunosuppressants, to allow timely implementation of appropriate interventions.
Due to the non-specific clinical manifestation of Strongyloides stercoralis infection, it is more likely to be overlooked when combined with other pathogen infections, thereby delaying diagnosis and treatment. For kidney transplant recipients presenting mainly with gastrointestinal and respiratory symptoms, vigilance for co-infection with Strongyloides stercoralis and cytomegalovirus is necessary.15 Although this co-infection is rare, its treatment mortality rate reaches 52.4%.15,16 Co-infection with cytomegalovirus may further suppress the immune system, exacerbating Strongyloides stercoralis infection.17 Therefore, when treating these patients, co-infection with pathogens like cytomegalovirus should be considered, with appropriate diagnostic and therapeutic measures taken. When kidney transplant recipients exhibit unexplained gastrointestinal and respiratory symptoms, clinicians should repeat sputum and stool smear tests. However, the diagnosis of Strongyloidiasis through conventional stool examination is often challenging due to low parasite load and irregular larval output.18 Simultaneous sputum and blood mNGS tests can assist in a timely diagnosis and treatment, thereby reducing the risk of developing a severe infection.
The patient had a history of residing in an epidemic area in February 2021. We speculate that during this period, the patient might have been exposed to Strongyloides stercoralis. Due to their normal immune response, the patient did not exhibit any clinical symptoms. In May 2023, the patient underwent an allogeneic kidney transplant. Before the surgery, the patient underwent a comprehensive infection screening, including chest CT, abdominal CT, 1,3-β-D-glucan test, Galactomannan test, Epstein-Barr virus polymerase chain reaction (PCR), Cytomegalovirus PCR, Syphilis spirochete antibody, Hepatitis C antigen, Human Immunodeficiency Virus antibody, Hepatitis B surface antigen, tuberculin test, and stool examination for parasites (including eggs of Ascaris, hookworms, whipworms, roundworms, liver flukes, lung flukes, or tapeworms). All results were negative. Therefore, the patient did not receive any prophylactic antiparasitic drug treatment before or after the surgery. The patient had been taking potent immunosuppressive drugs orally since his operation, which led to a lower immunity in his body. As a result, the asymptomatic latent infection was activated, which led to a fatal disseminated infection. Literature reports that in the presence of chronic Strongyloides stercoralis infections, whether symptomatic or not, eosinophilia can be observed in approximately two-thirds of cases.13 The patient’s eosinophil count did not increase after this admission, which we consider to be related to the inhibition of eosinophil production under a low immune state. In addition, an increase in peripheral blood eosinophil count during a hyperinfection period may indicate a better prognosis.12,13
The patient, who predominantly resided in a non-endemic area of infection, had a history of travel to epidemic areas. Unfortunately, this information was overlooked during the medical history interview conducted before the kidney transplant surgery. Consequently, no effective anti-infection treatment was administered, raising potential risks. Therefore, essential infection assessments should be conducted before any solid organ transplant. This assessment must evaluate several aspects: exposure history, past infection history, colonization culture, early exposure serological tests, and vaccination status.19 Should their serological test results be positive, patients must be treated before the transplantation. In addition, empirical treatments are often necessary for those with potential exposure history, such as those residing in endemic areas. Ivermectin is typically the first-choice drug in these scenarios.20 For clinicians who usually practice in non-epidemic areas, it is often easy to overlook a patient’s travel history to epidemic areas, which deserves special attention. Therefore, we should place particular emphasis on this aspect during the collection and assessment of medical histories. Correctly identifying and managing this key information is crucial for preventing potential infection risks and improving the treatment outcomes of patients after transplantation.
Summary
The reported rate of Strongyloides stercoralis infection has been gradually increasing in recent years. Patients who undergo immunosuppressive therapy after a kidney transplant are more susceptible to disseminated infections. Thus, conducting appropriate infection assessments before transplantation and necessary preventive medication treatment is crucial. In cases where a kidney transplant recipient experiences unexplained abdominal pain, bloating, nausea, emesis, cough, hemoptysis or difficulty breathing, the possibility of this disease should be considered. Promptly completing a Strongyloides stercoralis infection screening and formulating a targeted treatment plan are key for a good prognosis of the disease.
Ethical Approval
Ethical approval was not needed by local ethical committee, as this is a case report. The patient’s family provided written informed consent to publish details of this case. A copy of the consent form is available for review by the Editor of this journal.
Consent to Participate
The patient’s family has given its consent to participate in this case report.
Consent to Publish
The authors hereby confirm that the kidney donation was conducted voluntarily, with written informed consent, and it was in adherence with the Declaration of Istanbul. All authors confirm that they had full access to all the data in the study and accept responsibility to submit for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Article publishing charge provided by Clinical Technological Innovation Training Project of Army Medical University (CX2019LC104).
Disclosure
None of the authors have any competing interests to declare.
References
1. Coster LOB. Parasitic Infections in Solid Organ Transplant Recipients[J]. Infect Dis Clin North Am. 2013;27(2):395–427. doi:10.1016/j.idc.2013.02.008
2. Deng H, Zhang W. Nursing care for a case of severe disseminated Strongyloides stercoralis infection after renal transplantation[J]. J Nurses Training. 2018;33(19):1818–1819. doi:10.16821/j.cnki.hsjx.2018.19.029
3. Upadhyay D, Corbridge T, Jain M, et al. Pulmonary hyperinfection syndrome with Strongyloides stercoralis[J]. Am J Med. 2001;111(2):167–169. doi:10.1016/s0002-9343(01)00708-2
4. Krolewiecki A, Nutman TB. Strongyloidiasis: a Neglected Tropical Disease[J]. Infect Dis Clin North Am. 2019;33(1):135–151. doi:10.1016/j.idc.2018.10.006
5. Karanam LS, Basavraj GK, Papireddy C. Strongyloides stercoralis Hyper infection Syndrome[J]. Indian J Surg. 2021;83(Suppl 3):582–586. doi:10.1007/s12262-020-02292-x
6. Munisankar S, Rajamanickam A, Balasubramanian S, et al. Seroprevalence of Strongyloides stercoralis infection in a South Indian adult population[J]. PLoS Negl Trop Dis. 2022;16(7):e0010561. doi:10.1371/journal.pntd.0010561
7. Kangxia L, Haijun L, Jian’er Z, et al. Strongyloidiasis infection after glucocorticoid usage: a case report and literature review [J]. Chine J Front Med Sci. 2022;14(08):59–64. doi:10.12037/YXQY.2022.08-11
8. Rongxin C, Lei Z, Jiali F, et al. Infection of Strongyloides stercoralis in two kidney transplant recipients. Chine J Organ Transpl. 2021;42(10):621–623. doi:10.3760/cma.j.cn421203-20210325-00109
9. Kim EJ. Acute Respiratory Distress Syndrome With Alveolar Hemorrhage due to Strongyloidiasis Hyperinfection in an Older Patient[J]. Ann Geriatric Med Res. 2018;22(4):200–203. doi:10.4235/agmr.18.0041
10. El-Sameed YA, Beejay N, Al MR. Diffuse alveolar haemorrhage and severe hypoxemia from Strongyloides stercoralis hyperinfection syndrome[J]. Clin Respir J. 2015;9(4):489–492. doi:10.1111/crj.12169
11. Gonzalez-Ibarra F, Chevli P, Schachter L, et al. Strongyloidiasis and Diffuse Alveolar Hemorrhage in a Patient with Systemic Lupus Erythematosus[J]. Case Rep Med. 2014;2014:1–3. doi:10.1155/2014/278390
12. Osiro S, Hamula C, Glaser A, et al. A case of Strongyloides hyperinfection syndrome in the setting of persistent eosinophilia but negative serology[J]. Diagn Microbiol Infect Dis. 2017;88(2):168–170. doi:10.1016/j.diagmicrobio.2017.02.016
13. Geri G, Rabbat A, Mayaux J, et al. Strongyloides stercoralis hyperinfection syndrome: a case series and a review of the literature[J]. Infection. 2015;43(6):691–698. doi:10.1007/s15010-015-0799-1
14. Morrell MR, Dallas J, Kollef MH. A 50-year-old woman with abdominal pain and respiratory failure 3 months after kidney transplantation[J]. Chest. 2008;134(2):442–446. doi:10.1378/chest.07-2754
15. Lupia T, Crisa E, Gaviraghi A, et al. Overlapping Infection by Strongyloides spp. and Cytomegalovirus in the Immunocompromised Host: a Comprehensive Review of the Literature[J]. Trop Med Infect Dis. 2023;8(7). doi:10.3390/tropicalmed8070358
16. A FM, T RN, Vahhab E, et al. Strongyloides stercoralis and cytomegalovirus coinfection in a patient with a transplanted kidney[J]. Baylor Univ Med Center Proce. 2022;35(2):190–192. doi:10.1080/08998280.2021.1997262
17. R CB, M DS, Serrano A, et al. Strongyloides stercoralis Hyperinfection and Concomitant Cytomegalovirus Gastroenteritis in an Immunocompromised Host[J]. ACG Case Reports J. 2019;6(7):e00135. doi:10.14309/crj.0000000000000135
18. Siddiqui AA, Berk SL. Diagnosis ofStrongyloides stercoralis Infection[J]. Clinl Infect Dis. 2001;33(7):1040–1047. doi:10.1086/322707
19. Fishman JA. Infection in Organ Transplantation[J]. Am J Transplant. 2017;17(4):856–879. doi:10.1111/ajt.14208
20. Roxby AC, Gottlieb GS, Limaye AP. Strongyloidiasis in transplant patients[J]. Clin Infect Dis. 2009;49(9):1411–1423. doi:10.1086/630201
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.